Effects of Effects of Dihydrocapsiate on Dihydrocapsiate on Adaptive and Diet- Adaptive and Diet- Induced Thermogenesis Induced Thermogenesis with High Protein Very with High Protein Very Low Calorie Diet Low Calorie Diet TY Amy Lee MD TY Amy Lee MD Zhaoping Li MD, PhD Zhaoping Li MD, PhD Alona Zerlin RD Alona Zerlin RD Susan Bowerman RD Susan Bowerman RD Gail Thames Gail Thames David Heber MD, PhD David Heber MD, PhD Center for Human Nutrition, David Geffen School of Center for Human Nutrition, David Geffen School of Medicine, University of California Medicine, University of California Los Angeles, California Los Angeles, California [email protected] [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Effects of Dihydrocapsiate on Effects of Dihydrocapsiate on Adaptive and Diet-Induced Adaptive and Diet-Induced Thermogenesis with High Thermogenesis with High
Protein Very Low Calorie DietProtein Very Low Calorie DietTY Amy Lee MDTY Amy Lee MD
Zhaoping Li MD, PhDZhaoping Li MD, PhDAlona Zerlin RDAlona Zerlin RD
Susan Bowerman RDSusan Bowerman RDGail ThamesGail Thames
David Heber MD, PhDDavid Heber MD, PhDCenter for Human Nutrition, David Geffen School of Center for Human Nutrition, David Geffen School of
Medicine, University of CaliforniaMedicine, University of CaliforniaLos Angeles, CaliforniaLos Angeles, California
[email protected]@mednet.ucla.edu

Dihydrocapsiate (DCT)Dihydrocapsiate (DCT) Capsicum annuum L. Capsicum annuum L.
CH-19 SweetCH-19 Sweet NaturalNatural
Increases sympathetic Increases sympathetic nervous systemnervous system
Acts Transient Receptor Acts Transient Receptor Potential Vanilloid 1 Potential Vanilloid 1 (TRPV1)(TRPV1)
Good alternative to the Good alternative to the pungent chili pepperspungent chili peppers

MechanismsMechanisms
CapsaicinCapsaicin– TRPV1TRPV1
Tongue, gut, othersTongue, gut, others
Peripheral Peripheral vasodilationvasodilation
Sympathetic activitySympathetic activity Increase Increase
thermogenesisthermogenesis
CapsinoidsCapsinoids– TRPV1TRPV1
Doesn’t reach the Doesn’t reach the tongue due to structural tongue due to structural differencedifference
10001000thth x less potent x less potent Sympathetic activitySympathetic activity Increase thermogenesisIncrease thermogenesis

ObjectivesObjectives
Examine the effects of DCT on both Examine the effects of DCT on both adaptive thermogenesis as the result adaptive thermogenesis as the result of caloric restriction with a high of caloric restriction with a high protein, very low calorie dietprotein, very low calorie diet
Determine whether DCT would Determine whether DCT would increase post-prandial energy (PPEE) increase post-prandial energy (PPEE) in response to 400 calories/ 60 in response to 400 calories/ 60 grams protein liquid mealgrams protein liquid meal

Inclusion Criteria:Inclusion Criteria:
Men over age of 30 and Men over age of 30 and postmenopausal womenpostmenopausal women
Nonsmoker or smoke less than 1 Nonsmoker or smoke less than 1 cigarette a daycigarette a day
Subject willing to go on a VLCD as Subject willing to go on a VLCD as meal replacementmeal replacement
Can sign the IRB/ informed consentCan sign the IRB/ informed consent

Exclusion CriteriaExclusion Criteria More than 30 minutes of exercise/ More than 30 minutes of exercise/
weekweek Diabetes, uncontrolled BP (>160/95), Diabetes, uncontrolled BP (>160/95),
eating disorders, chronic infections, eating disorders, chronic infections, malignancymalignancy
Major surgeries in past 12 weeksMajor surgeries in past 12 weeks > 1 alcohol beverage/ day or tobacco> 1 alcohol beverage/ day or tobacco Antidepressants or weight loss Antidepressants or weight loss
supplementsupplement Allergy to chili peppersAllergy to chili peppers

Methods Methods
VLCD 800 cal/120g VLCD 800 cal/120g proteinprotein
Capsiate capsulesCapsiate capsules– Placebo, 3mg, 9mgPlacebo, 3mg, 9mg
Body compositionBody composition Indirect calorimetryIndirect calorimetry

Method Method Week 1Week 1
– Safety blood, weigh in, BodPodSafety blood, weigh in, BodPod– Baseline Vmax (1)Baseline Vmax (1)– 400 calories/ 60 g protein400 calories/ 60 g protein– Vmax (2- 4)Vmax (2- 4)
Week 2, 3Week 2, 3– Safety blood, weigh in, BodPodSafety blood, weigh in, BodPod– 800 calories/ 120 g protein800 calories/ 120 g protein– DCT capsules (placebo, 3mg or 9 mg)DCT capsules (placebo, 3mg or 9 mg)
Week 4Week 4– Repeat of week oneRepeat of week one– 400 calories/ 60 g protein400 calories/ 60 g protein– 9 capsules of group 9 capsules of group

Placebo 3 mg 9mg
Subject number
Age (y) 50±11.78 54.58±9.33 54.22±11.872
Females (%) 70 53 44
Body Mass (kg) 91.8±14.6 86.3±19.6 92.9±16.9
BMI (kg/m2) 31.22±3.38 30.33±2.99 31.77±3.59
Fat Free Mass (kg) 57.6±11.8 51.1±14.6 52.5±15.6
REE (kcal/d) 1431.4±276.8 1377.9±314.7 1397.6±282.2
Baseline Characteristics

SafetySafety
No severe adverse Events
Adverse events from VLCD
No significant change of chemistry, liver function tests

ResultsResults
CAPSINOIDs PLACEBO TOTAL
Study group (randomized) 32 15 47
Screened but never started 0 0 3
Had at least one dose 0 0 0
Stopped at 1 week 1 1 2
Stopped at 2 week 8 3 13
Stopped at 3 week 0 0 0
Completed 4 weeks 15 18 33

Change of Body WeightChange of Body Weight

Resting Metabolic RateResting Metabolic Ratekcal/
day

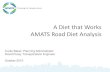
Figure 1 Changes of average of energy expenditure adjusted by fat free mass (EE/FFM) from 1h to 4h during diet induced thermogenesis at Day 28. FFM was determined by BODPOD. Values are shown mean and SE. *; P<0.05 vs placebo.
placebo 9 mg 3 mg
Ch
an
ge o
f E
E/F
FM
( kc
al/d
ay/
kg)
0.0
2.0
4.0
6.0
8.0 *
Postprandial Energy Expenditure

Ch
an
ge
of
RQ
-0.02
0.00
0.02
0.04
0.06
Figure 2 Changes of average of respiratory quotient (RQ) from 1h to 4h during diet induced thermogenesis at Day 28. Values are shown mean and SE. *; P<0.05 vsplacebo.
placebo 9 mg 3 mg
**

ConclusionsConclusions
We did not see any significant change We did not see any significant change of the adaptive thermogenesis with the of the adaptive thermogenesis with the VLCD program. VLCD program.
DCT significantly increased DCT significantly increased postprandial energy expenditure. postprandial energy expenditure.
DCT significantly increased fat DCT significantly increased fat oxidation.oxidation.

InterpretationInterpretation No weight change was detected in this 4 No weight change was detected in this 4
week study.week study. This may have been due to the effects of the This may have been due to the effects of the
VLCD on weight change in an outpatient VLCD on weight change in an outpatient setting overwhelming the effects of the DCT. setting overwhelming the effects of the DCT.
Increased fat metabolism was observed with Increased fat metabolism was observed with an increase of RQ after the 400 cal/ 60 g an increase of RQ after the 400 cal/ 60 g protein test meal challenge but there was no protein test meal challenge but there was no interference with the adaptive decrease interference with the adaptive decrease in thermogenesis seen with VLCD.in thermogenesis seen with VLCD.

DiscussionDiscussion
DCT stimulate thermogenesis in DCT stimulate thermogenesis in animals, and activate the neuronal animals, and activate the neuronal TRPV1 receptors on vagal afferent TRPV1 receptors on vagal afferent nerves in the intestine leading to nerves in the intestine leading to increased SNS activity with uncoupling increased SNS activity with uncoupling of oxidative phosphorylation leading of oxidative phosphorylation leading to heat production.to heat production.
PPEE was also observed in this study PPEE was also observed in this study after subjects took in 400 calories / 60 after subjects took in 400 calories / 60 g proteing protein

Future Research Directions
Need longer term studies with a less intensive diet to detect the effects of 9 mg of dihydrocapsiate per day vs. placebo on weight and obesity-associated co-morbidities.

DropsDrops 51 enrolled51 enrolled 33 completed33 completed
PlaceboPlacebo– 3 males, 1 female3 males, 1 female– NoncomplianceNoncompliance– Feeling weakFeeling weak
3 mg3 mg– 3 males3 males– NoncomplianceNoncompliance– Uncontrolled BPUncontrolled BP
9 mg9 mg– 3 males, 3 females3 males, 3 females– NoncomplianceNoncompliance– ConstipationConstipation– Feeling weakFeeling weak– Low glucoseLow glucose

Thank you!Thank you!
Thank Thank you!you!
Related Documents