Journal of Steroid Biochemistry & Molecular Biology 111 (2008) 178–194 Contents lists available at ScienceDirect Journal of Steroid Biochemistry and Molecular Biology journal homepage: www.elsevier.com/locate/jsbmb Effect of intravaginal DHEA on serum DHEA and eleven of its metabolites in postmenopausal women Fernand Labrie ∗ , Leonello Cusan, José Luis Gomez, Isabelle Côté, René Bérubé, Patrick Bélanger, Céline Martel, Claude Labrie Oncology and Molecular Endocrinology Research Center, Laval University Hospital Research Center (CRCHUL) and Laval University, 2705 Laurier Boulevard, Quebec City, Quebec G1V 4G2, Canada article info Article history: Received 17 January 2008 Received in revised form 4 June 2008 Accepted 5 June 2008 Keywords: DHEA Menopause Vaginal atrophy Intracrinology Maturation index Maturation value Vaginal pH abstract The primary objective of this study was measurement of the systemic bioavailability of DHEA and its metabolites following daily intravaginal application of the sex steroid precursor. Forty postmenopausal women were randomized to receive a daily dose of one ovule of the following DHEA concentrations: 0.0%, 0.5%, 1.0% or 1.8%. After only 7 days of treatment, the maturation value of the vaginal epithelial cells was significantly increased while the vaginal pH was significantly decreased at all DHEA doses. These important local effects were observed while the serum concentrations of estradiol and testosterone remained within the values found in normal postmenopausal women at all DHEA doses. Similar observations were made for serum androstenedione, estrone, estrone-sulfate and DHEA-sulfate. Even at the highest 1.8% DHEA dose, serum DHEA was increased at the levels found in normal premenopausal women. The present data show that the intravaginal administration of DHEA permits to rapidly achieve the local beneficial effects against vaginal atrophy without significant changes in serum estrogens, thus avoiding the increased risk of breast cancer associated with the current intravaginal or systemic estrogenic formulations. In addition, the recent observation that DHEA is transformed into both androgens and estrogens in the vagina permits to exert benefits on all the three layers of the vaginal wall. © 2008 Elsevier Ltd. All rights reserved. 1. Introduction Vaginal dryness affects about 50% of postmenopausal women at the age of 50–60 years and 72% after 70 years [1]. Of these women, about 80% experience urogenital disorders [2]. In fact, vaginal dryness or atrophic vaginitis, also referred to as urogenital atrophy accompanied by sexual dysfunction is a common problem in postmenopausal women [3–11]. The most common symptoms are dryness, burning, pruritus, infection, irritation and dyspareunia, thus leading to decreased libido, sexual dysfunction and quality of life [12]. Since the problems of vaginal atrophy are believed to be largely related to the deprivation of sex steroids, appropriate hormonal replacement therapy is a reasonable and efficient approach. Based upon knowledge of the cessation of ovarian estrogen secretion at menopause, intravaginal and systemic estrogens have been the standard therapy [5,8–10]. However, recent data show that post- menopausal women are not only deficient in estrogens at time of menopause, but that they are also deprived, starting in the thir- ∗ Corresponding author. Tel.: +1 418 654 2704; fax: +1 418 654 2735. E-mail address: [email protected] (F. Labrie). ties, of the androgens originating from the peripheral intracrine transformation of dehydroepiandrosterone (DHEA) into androgens [13–15]. In fact, serum DHEA and DHEA-sulfate (DHEA-S) progres- sively decrease from the age of 30 years [15–17]. At menopause, serum DHEA has already decreased by 60% [18]. Since serum DHEA is the predominant source of androgens in women, the 60% decrease in circulating DHEA leads to a similar 60% decrease in the total androgen pool in women by time of menopause [18]. Although intravaginal estrogen formulations were developed to avoid systemic exposure to estrogens, a series of studies have clearly demonstrated that such preparations intended for exclusive local action lead to relatively high serum estrogen levels [19–22] clearly indicating that their use is an issue related to an increased risk of breast and possibly also uterine cancer [23–27]. It is well known that atrophic vaginitis in postmenopausal women can be worsened or induced by the use of aromatase inhibitors for the treatment of breast cancer. In fact, these drugs exert their benefits on breast cancer by decreasing E 2 biosyn- thesis, thus increasing the frequency and severity of menopausal symptoms [28,29]. In a recent study where seven breast cancer patients treated with aromatase inhibitors received Vagifem (estra- diol tablet) at a daily dose of 25 g for 2 weeks and then, thereafter, twice weekly, serum estradiol (E 2 ) rose from a median of 3 to 0960-0760/$ – see front matter © 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.jsbmb.2008.06.003

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Journal of Steroid Biochemistry & Molecular Biology 111 (2008) 178–194
Contents lists available at ScienceDirect
Journal of Steroid Biochemistry and Molecular Biology
journa l homepage: www.e lsev ier .com/ locate / j sbmb
Effect of intravaginal DHEA on serum DHEA and eleven of its metabolitesin postmenopausal women
Fernand Labrie ∗, Leonello Cusan, José Luis Gomez, Isabelle Côté, René Bérubé,Patrick Bélanger, Céline Martel, Claude LabrieOncology and Molecular Endocrinology Research Center, Laval University Hospital Research Center (CRCHUL) and Laval University,2705 Laurier Boulevard, Quebec City, Quebec G1V 4G2, Canada
a r t i c l e i n f o
Article history:Received 17 January 2008Received in revised form 4 June 2008Accepted 5 June 2008
Keywords:DHEAMenopauseVaginal atrophyIntracrinologyMaturation index
a b s t r a c t
The primary objective of this study was measurement of the systemic bioavailability of DHEA and itsmetabolites following daily intravaginal application of the sex steroid precursor. Forty postmenopausalwomen were randomized to receive a daily dose of one ovule of the following DHEA concentrations: 0.0%,0.5%, 1.0% or 1.8%. After only 7 days of treatment, the maturation value of the vaginal epithelial cells wassignificantly increased while the vaginal pH was significantly decreased at all DHEA doses. These importantlocal effects were observed while the serum concentrations of estradiol and testosterone remained withinthe values found in normal postmenopausal women at all DHEA doses. Similar observations were madefor serum androstenedione, estrone, estrone-sulfate and DHEA-sulfate. Even at the highest 1.8% DHEAdose, serum DHEA was increased at the levels found in normal premenopausal women. The present datashow that the intravaginal administration of DHEA permits to rapidly achieve the local beneficial effects
Maturation valueVaginal pH
against vaginal atrophy without significant changes in serum estrogens, thus avoiding the increased riskof breast cancer associated with the current intravaginal or systemic estrogenic formulations. In addition,
t DHEthre
1
awvaiatl
rrumsmm
tt[ssDdt
adaib
0d
the recent observation thato exert benefits on all the
. Introduction
Vaginal dryness affects about 50% of postmenopausal woment the age of 50–60 years and 72% after 70 years [1]. Of theseomen, about 80% experience urogenital disorders [2]. In fact,
aginal dryness or atrophic vaginitis, also referred to as urogenitaltrophy accompanied by sexual dysfunction is a common problemn postmenopausal women [3–11]. The most common symptomsre dryness, burning, pruritus, infection, irritation and dyspareunia,hus leading to decreased libido, sexual dysfunction and quality ofife [12].
Since the problems of vaginal atrophy are believed to be largelyelated to the deprivation of sex steroids, appropriate hormonaleplacement therapy is a reasonable and efficient approach. Basedpon knowledge of the cessation of ovarian estrogen secretion at
enopause, intravaginal and systemic estrogens have been thetandard therapy [5,8–10]. However, recent data show that post-enopausal women are not only deficient in estrogens at time ofenopause, but that they are also deprived, starting in the thir-
∗ Corresponding author. Tel.: +1 418 654 2704; fax: +1 418 654 2735.E-mail address: [email protected] (F. Labrie).
wietspdt
960-0760/$ – see front matter © 2008 Elsevier Ltd. All rights reserved.oi:10.1016/j.jsbmb.2008.06.003
A is transformed into both androgens and estrogens in the vagina permitse layers of the vaginal wall.
© 2008 Elsevier Ltd. All rights reserved.
ies, of the androgens originating from the peripheral intracrineransformation of dehydroepiandrosterone (DHEA) into androgens13–15]. In fact, serum DHEA and DHEA-sulfate (DHEA-S) progres-ively decrease from the age of 30 years [15–17]. At menopause,erum DHEA has already decreased by 60% [18]. Since serumHEA is the predominant source of androgens in women, the 60%ecrease in circulating DHEA leads to a similar 60% decrease in theotal androgen pool in women by time of menopause [18].
Although intravaginal estrogen formulations were developed tovoid systemic exposure to estrogens, a series of studies have clearlyemonstrated that such preparations intended for exclusive localction lead to relatively high serum estrogen levels [19–22] clearlyndicating that their use is an issue related to an increased risk ofreast and possibly also uterine cancer [23–27].
It is well known that atrophic vaginitis in postmenopausalomen can be worsened or induced by the use of aromatase
nhibitors for the treatment of breast cancer. In fact, these drugsxert their benefits on breast cancer by decreasing E2 biosyn-
hesis, thus increasing the frequency and severity of menopausalymptoms [28,29]. In a recent study where seven breast canceratients treated with aromatase inhibitors received Vagifem (estra-iol tablet) at a daily dose of 25 �g for 2 weeks and then, thereafter,wice weekly, serum estradiol (E2) rose from a median of 3 to
istry &
7eaA8flaiotcwa
Etwaeaisamwtmawt
oicawit
amdvia
2
tpd0TaIL
-
-
--
------
-
--
------------
•
•
• At least a 4-week washout period for locally delivered hormonereplacement therapy for vaginal dryness (rings, creams, gels ortablets).
F. Labrie et al. / Journal of Steroid Biochem
2 pmol/l, at 2 weeks (range 3–232 pmol/l) [30]. Serum E2 lev-ls generally decreased thereafter to values of 40 pmol/l or lesslthough values of 137 and 219 pmol/l were found at weeks 7–10.
patient who received Premarin cream had serum E2 levels of3 pmol/l at 2 weeks. It should be mentioned that blood samplingor E2 measurement was done at time of patient’s visit, a timing notikely to correspond to the highest levels of serum E2 after Vagifemdministration. It is thus more than likely that the values reportedn [30] underestimate, up to an unknown extent, the true elevationf serum E2 after Vagifem administration. The authors concludedhat the use of Vagifem with aromatase inhibitors is contraindi-ated. These findings obtained in breast cancer women treatedith aromatase inhibitors raise a serious issue about the use of
ny vaginal estrogen preparation in postmenopausal women.In previous studies with Vagifem, maximal and mean 24 h serum
2 concentrations were measured at 180 ± 99 and 84 pmol/l forhe 25 �g dose while values of 81 ± 62 and 40 pmol/l, respectively,ere found for the 10 �g dose [30]. Other vaginal estrogen tablets
nd creams have led to high or even higher serum estrogen lev-ls [31–33]. In agreement with the role of both estrogens andndrogens in vaginal atrophy, the morphological changes observedn the rat vagina after DHEA treatment reflect its local conver-ion into active sex steroids having androgenic and/or estrogenicction through intracrine mechanisms [13]. These changes includearked epithelial mucification, high compactness of delicate, finelyoven lamina propria collagen fibers and moderate muscularis
hickness increase when compared to ovariectomized (OVX) ani-als. The first and the second morphological changes are typical of
n androgenic effect while the third shows an estrogen-like activity,hich is further supported by a concomitant increase in proges-
erone receptor expression in the muscularis layer [34].The primary objective of the present study was the evaluation
f the systemic bioavailability of DHEA and its metabolites follow-ng daily intravaginal application of ovules at four different DHEAoncentrations. This study was a randomized, placebo-controllednd double-blind trial. The maturation index as well as vaginal pHere measured at pretreatment as well as after 7 days of treatment
n order to obtain an indication of the local effect of DHEA duringhat short period.
The present data show that, at the doses used, the intravaginaldministration of DHEA already exerts a significant effect on theaturation value of the vaginal epithelial cells and significantly
ecreases the pH while maintaining serum estrogens within thealues found in normal postmenopausal women, thus avoiding thencreased risk of breast cancer found with any estrogen preparationdministered intravaginally or systemically.
. Subjects and methods
This study is a randomized, placebo-controlled, double-blindrial of 10 subjects per arm (for a total of 40 subjects). Fortyostmenopausal women were thus randomized to receive a dailyose of one ovule of the following DHEA concentrations: 0.0%,.5% (6.5 mg DHEA), 1.0% (13 mg DHEA) or 1.8% (23.4 mg DHEA).he study was divided into two phases, a screening period andtreatment period of 1 week. The protocol was approved by the
nstitutional Review Board of the Centre Hospitalier de l’Universitéaval.
The inclusion criteria were the following:
Postmenopausal women who satisfy either a or b or c:a. No menses for at least 1 year, or;b. FSH levels ≥40 IU/L (within 60 days prior to day 1) in women
with no menses ≥6 months but <12 months, or hysterec-
•
••
Molecular Biology 111 (2008) 178–194 179
tomized women who were premenopausal at the time ofhysterectomy, with unknown ovarian status or;
c. Six weeks or more following bilateral oophorectomy with orwithout hysterectomy.
Women who have self-identified at least one moderate to severeof the following symptoms:• Vaginal dryness (none, mild, moderate or severe).• Vaginal and/or vulvar irritation/itching (none, mild, moderate
or severe).• Dysuria (none, mild, moderate or severe).• Vaginal pain associated with sexual activity (none, mild, mod-
erate or severe).• Vaginal bleeding associated with sexual activity (none, mild,
moderate or severe).Women between 40 and 75 years of age.Women having a low maturation index (no greater part of guid-ance than 5% of superficial cells on vaginal smear).Women having a vaginal pH above 5.Normal mammography within 24 months of enrolment.Normal breast examination.Willing to participate in the study and sign an informed consent.No former or present narcotic addiction or alcoholism.Body weight within the range of 18.5 and 29.9 of ideal body weightaccording to body mass index (BMI) (WHO).No hepatic or renal impairment or condition known to affect drugor steroid metabolism.Normal baseline hematology, clinical chemistry, and urinalysis.Endometrial thickness of 4 mm or less at transvaginal ultrasonog-raphy.
The exclusion criteria were:
Undiagnosed abnormal genital bleeding.Previous diagnosis of cancer, except skin cancer (non-melanoma).History of hormone-dependant cancer (uterus, breast).Active or history of thromboembolic disease.Significant metabolic or endocrine disease.Clinically significant gastrointestinal, liver or gallbladder disease.Migraine headache.Diabetes mellitus not controlled by conventional therapy.Eczema, cutaneous allergies.Significant complication on previous hormonal therapy.Use of hormonal implants within 6 months prior to study entry.Any oral estrogen, progestin or DHEA exposure (HRT and vaginalcreams) or use of natural estrogens (phytoestrogens) or herbalproducts to treat postmenopausal symptoms in the 8 weeks priorto baseline assessments.
Patients could washout as follows:
At least an 8-week washout period for prior oral estrogen, DHEAand/or progestin therapy, including oral contraceptives.At least a 4-week washout period for prior transdermal hormonetherapy.
At least 6 months for prior estrogen pellet therapy or progestininjectable drug therapy.Eight weeks or longer for prior intrauterine progestin therapy.Three months or longer for prior progestin implants and estrogenalone injectable drug therapy.
1 istry &
-
---
-
-
-
--
--
--
-
2
thlrgaeo
2
pwwwld(c3Ed
oat1
2
2e
G0d
fa
sAs0a
mamvarc
4oa
2
adprtHcp5i
2
diaitit
2
t(0ae
23
2e
ms
80 F. Labrie et al. / Journal of Steroid Biochem
Corticosteroid treatment (including topical, intranasal, oral, etc.)within 6 weeks of study entry.No chronic use of corticosteroids allowed.Cardiac failure or manifest coronary heart disease.Hypertension equal to or above 150/95 mmHg or not controlledby standard therapy.Confirmed clinically significant depression or confirmed historyof severe psychiatric disturbance.The administration of any investigational drug within 30 days ofscreening visit.Previous treatment with androgens or anabolic steroids within 3months prior to screening visit.Clinically relevant abnormal serum biochemistry or hematology.Baseline cervical cytology showing low-grade squamous intraep-ithelial lesion (LGISIL) or worse.Presence of any manifest premalignant or malignant disease.Exposure to or use of antidepressants, psychologic medication,narcotic analgesics or tranquilizers within 30 days prior to enrol-ment.Smoking: any number of cigarettes is an exclusion criteria.Drugs that interfere with the metabolism of estrogen (e g , keto-conazole, steroid formation or action inhibitors, and alternativemedicines) are not allowed.Clonidine or methyldopa is not allowed.
.1. Informed consent
A written informed consent was obtained from all subjects prioro the performance of any study-related procedures. The subjectsad a medical history and a medical exam. A complete gyneco-
ogical exam had to be documented within three months prior toandomization or performed as part of the physical exam. A partialynecological exam to evaluate the aspect of the mucosa and toler-nce of the ovules was done at screening (if complete gynecologicalxam had been performed within 3 months), day 1 and at the endf study.
.2. Laboratory tests
The usual laboratory tests, namely hematology (including com-lete blood count and coagulation), blood chemistry and urinalysisere performed. Serum FSH had to be measured only in womenho had no menses for ≥6 months but <12 months or whoere premenopausal at the time of hysterectomy. Serum steroid
evels of DHEA, DHEA-S, androst-5-ene-3�, 17�-diol, (5-diol),ihydrotestosterone (DHT), testosterone (testo), androstenedione4-dione), estradiol (E2), estrone (E1), E1-S, androsterone glu-uronide (ADT-G), androstane-3�, 17�-diol-3G (3�-diol-3G) and�-diol-17G were measured at the Laboratory of Molecularndocrinology, CHUL Research Center by mass spectrometry asescribed [18].
Pharmacokinetic measurements of serum steroids were maden day 1 (first administration of a DHEA ovule) and day 7 (7thdministration of a DHEA ovule). Blood samplings were made atime zero (time of ovule administration) as well as 0.5, 1, 2, 4, 6, 8,2, 18 and 24 h after DHEA ovule administration.
.3. Analysis of non-conjugated steroids
.3.1. Preparation of calibration curve of standard samples and
xtraction of steroids from human serumDHEA, 5-diol, 4-dione, testo, DHT, E1 and E2 were analyzed byC/MS. On each day of analysis, calibration standards ranging from.2 to 20 ng/ml for DHEA and 5-diol, from 0.05 to 10 ng/ml for 4-ione and testo, from 0.02 to 4 ng/ml for DHT, from 8 to 400 pg/ml
tm
tt
Molecular Biology 111 (2008) 178–194
or E1 and from 2 to 400 pg/ml for E2 are prepared using charcoal-dsorbed human serum.
For the extraction of steroids, 500 �l of a 0.5 M sodium acetateolution is added to each tube (1.0 ml for calibration standards).methanolic solution (50 �l), containing a mixture of deuterated
teroid internal standards, is then added to each tube. Aliquots of.75 ml of study samples (0.25 ml for calibration standards) aredded and tubes are vortexed for ca. 1 min.
1-Chlorobutane (3 ml) is then added to each tube andixed. After centrifugation, the organic extracts are collected
nd purified on LC–Si SPE columns. Columns and the adsorbedaterial are washed with ethyl acetate:hexane (ca. 6 ml; 1:9,
:v). The analytes of interest are then eluted using 4 ml ethylcetate:hexane (50:50, v:v) which is evaporated at 50 ◦C. The driedesidue is reconstituted in 0.5 ml ethyl acetate and vortexed fora. 15 s.
An aliquot of 100 �l is transferred to a glass tube for the assay of-dione and the remaining extract is kept in the tube for the assayf DHEA, 5-diol, testo, DHT, E1 and E2. Both extracts are evaporatedt 50 ◦C.
.3.2. Derivatization of DHEA, 5-diol, testo, DHT, E1 and E2Pentafluorobenzoylchloride in ethyl acetate (50 �l; 1/10, w/v)
nd pyridine in ethyl acetate (500 �l; 1:99, v:v) are added to theried residue of DHEA, 5-diol, testo, DHT, E1 and E2 and the sam-les are incubated for ca. 30 min at 60 ◦C. After evaporation of theeagent mixture, a solution of 0.5 M NaHCO3 (1.0 ml) is added to theubes, which are then left to react for 15 min at room temperature.exane (2 ml) is then added to the tubes, which are vortexed fora. 2 min and left at room temperature for ca. 10 min. The organichase is evaporated at 50 ◦C and the final extract reconstituted in0 �l isooctane and then transferred into a conical vial for injection
nto the GC/MS.
.3.3. Derivatization of 4-dioneA solution of 1 mg pentafluorobenzylhydroxylamine/ml pyri-
ine (100 �l) is added to the 4-dione extract and the tubes arencubated for ca. 30 min at 60 ◦C. After derivatization, the tubesre left to cool at room temperature for ca. 5 min and hexane (3 ml)s added to the samples. The mixtures are vortexed for ca. 5 s andhen evaporated at 50 ◦C. The final extract is reconstituted in 50 �lsooctane and then transferred into a conical vial for injection intohe GC/MS system.
.3.4. Analysis by GC/MSThe GC/MS system for the analysis of DHEA, 5-diol, 4-dione,
esto, DHT, E1 and E2 uses a 50% phenyl–methyl polysiloxaneDB-17HT) capillary column (30 m × 0.25 mm internal diameter,.15 �m film thickness) with helium as the carrier gas. The analytesnd IS are detected using a HP5973 quadrupole mass spectrometerquipped with a chemical ionization source.
.4. Analysis of the conjugated steroids—ADT-G, 3˛-diol-3G and˛-diol-17G
.4.1. Preparation of calibration curve of standard samples andxtraction from human serum
ADT-G, 3�-diol-3G and 3�-diol-17G are analyzed by a LC/MS/MSethod using TurboIonSpray. On each day of analysis, calibration
tandards ranging from 2 to 200 ng/ml for ADT-G and from 0.50
o 50 ng/ml for 3�-diol-3G and 3�-diol-17G are prepared using aixture of charcoal-adsorbed serum:water (1:1, v:v).For extraction from serum, 500 �l of serum sample is transferred
o each tube. Water (500 �l) is added and the tubes are then vor-exed. A methanolic solution (100 �l) containing the deuterated
istry & Molecular Biology 111 (2008) 178–194 181
sov
u(satma
2
sAAT
Table 1Intra- and inter-assay coefficients of variation (%) for 12 steroids measured by GC/MSand LC–MS/MS in human samples (endogenous steroids)
Steroid LLOQ ng/ml Conc ng/ml Coefficient of variation
Within runs Between runs
DHEAa 0.20 2.44 2.0 1.9DHEA-Sb 75.0 593 5.2 6.35-Diola 0.20 0.91 9.5 13.14-Dionea 0.05 0.62 3.7 4.2Testoa 0.05 0.48 2.9 3.4DHTa 0.02 0.11 3.1 4.1ADT-Gb 2.00 22.8 3.1 3.73�-Diol-3Gb 0.50 0.79 10.3 10.73�-Diol-17Gb 0.50 1.65 4.6 5.3E1a 8.00c 60.8c 1.8 1.8
Fo
F. Labrie et al. / Journal of Steroid Biochem
teroid internal standard is then added to each tube. A solutionf NaH2PO4/citric acid buffer (1.5 ml) is added and the tubes areortexed again.
Samples are transferred to the C-18 SPE columns. Each col-mn is then washed with water and a solution of methanol:water50:50, v:v). The analytes of interest are then eluted using aolution (4 ml) of methanol:water (80:20, v:v), containing 10 mMmmonium acetate. The eluates are evaporated at 45 ◦C andhe dried residue is reconstituted in a solution (100 �l) of
ethanol:water (50:50, v:v) containing 0.01% acetic acid prior tonalysis.
.4.2. Analysis by LC/MS/MS
The HPLC system uses a 150 mm × 4.6 mm, 4-�m particleize Synergy Hydro-RP column at a flow rate of 1.0 ml/min.DT-G, 3�-diol-3G and 3�-diol-17G are detected using a SciexPI 3000 triple quadrupole mass spectrometer, equipped withurboIonSprayTM.
E2a 2.00c 19.2c 3.5 3.7E1-Sb 75.0c 279c 4.5 6.0
a GC/MS.b LC–MS/MS.c Values in pg/ml.
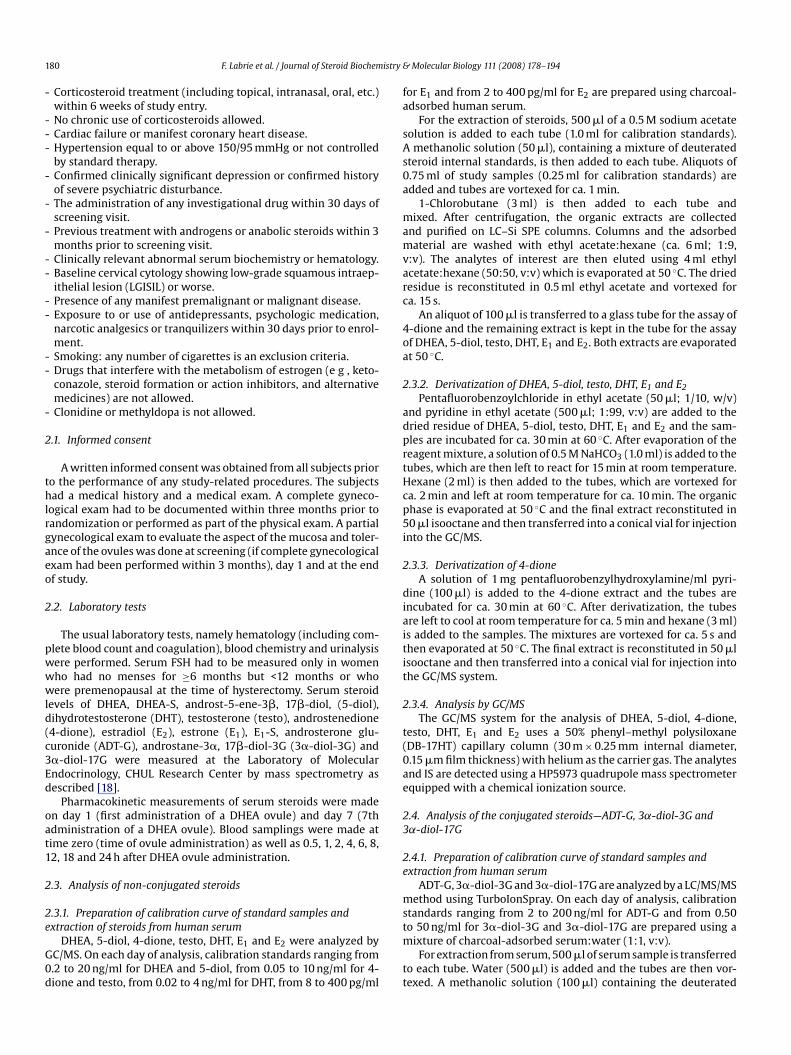
ig. 1. Serum levels of DHEA and 5-diol on days 1 and 7 in 40–75-year-old postmenopausal women following daily administration of vaginal ovules containing 0%, 0.5%, 1.0%r 1.8% DHEA. Data are expressed as means ± S.E.M. (n = 9 or 10).

1 istry &
2a
2e
bfE
fmnoaea(svff
2
5fl3w1u3w
2s
3aa
2
stcsca
tiTosPwfi
2
m
itffsf
2
aw
•
••
2
svdacCbdef
3
clua114Dowui
isti(Ds1t
82 F. Labrie et al. / Journal of Steroid Biochem
.5. Analysis of the conjugated steroids DHEA-sulfate (DHEA-S)nd E1-S
.5.1. Preparation of calibration curve standard samples andxtraction from human serum
DHEA-S and E1-S are analyzed by a LC/MS/MS method using Tur-oIonspray. On each day of analysis, calibration standards rangingrom 0.075 to 10 �g/ml for DHEA-S and from 0.075 to 10 ng/ml for1-S are prepared using PBS:charcoal-adsorbed serum (1:1, v:v).
For extraction from serum, 100 �l of the serum sample is trans-erred to individual tubes and 2 ml of PBS buffer is added. A
ethanolic solution (50 �l) containing the deuterated steroid inter-al standard is then added to each tube. Samples are transferredn Oasis HLB SPE columns and each column is washed with waternd methanol:water (10:90, v:v). The analytes of interest are thenluted with 4 ml of methanol. Methanol is evaporated at 35 ◦Cnd the dried residue reconstituted in 125 �l of methanol:water50:50, v:v) and then filtered on 0.2 �m nylon filter. Part of thisolution (20 �l) is diluted in 0.5 ml of methanol:water (50:50,:v) containing 5 mM ammonium acetate and 0.01% acetic acidor the DHEA-S analysis. The remaining part is used directlyor E1-S analysis.
.5.2. Analysis by LC/MS/MSFor DHEA-S analysis, the HPLC system uses a 100 mm × 3.2 mm,
-�m particle size, Phenomenex Columbus C18 column at aow rate of 0.5 ml/min. DHEA-S is detected using a Sciex API00 or API 3000 triple quadrupole mass spectrometer equippedith TurboIonsprayTM. For E1-S analysis, the HPLC system uses a
00 mm × 4.6 mm, 35 �m particle size Phenomenex Luna C18 col-mn at a flow rate of 1.0 ml/min. E1-S is detected using a Sciex API65 or API 3000 triple quadrupole mass spectrometer, equippedith Turbolonspray.
.6. Coefficients of variation of steroid assays by masspectrometry
The intra- and inter-assay coefficients of variation obtained fromdifferent assays performed with 6 replicates in each assay as well
s the lower limit of quantification (sensitivity) for steroid assaysre indicated on Table 1.
.7. Vaginal pH and cytology
For the vaginal pH, maturation index and Papanicolaou (PAP)mear, all samples were examined by a cytopathologist blindedo the treatment regimens. A 100-cell count was performed tolassify cells as superficial (S), intermediate (I) and parabasal (P)quamous cell types. The vaginal maturation value (VMV) was cal-ulated using the equation (1 × S) + (0.5 × I) + (0 × P). The VMV hasrange of 0–100 [35,36].
Vaginal smears were obtained by scraping the middle third ofhe side wall of the vagina using a plastic or wooden spatula thats applied to a glass slide and immediately fixed with Spray-Cyte.hese samples were sent to a central laboratory for determinationf the maturation index. Vaginal pH was measured by applying a pHtrip directly to the lateral wall of the vagina with a forceps. For theapanicolaou smear, if not done in the last 12 months, specimensere obtained from the endocervix and exocervix and immediatelyxed with cytospray.
.8. Mammography
Mammography was done if not available during the last 12onths. A transvaginal ultrasonography was performed at screen-
id
ai
Molecular Biology 111 (2008) 178–194
ng to assess the endometrial thickness. The uterus was examinedo determine the endometrial thickness in the long axis projectionrom one endometrial/myometrial interface to the opposite inter-ace. In the case of an endometrial thickness of more than 4 mm atcreening, the woman was not to be admitted in the study and wasollowed according to medical practice.
.9. Medication
The medication necessary for the patient’s well-being wasllowed (including: treatment of hypertension and thyroid disease)ith the exception of:
Any systemic estrogen or progestin exposure (HRT and vaginalcreams) or use of natural estrogen (phytoestrogens) contained infoods or as food supplements or alternative medicines to treatpostmenopausal symptoms was not allowed.Any other investigational drug was not allowed.Cigarette smoking was not allowed.
.10. Statistics
Descriptive statistics were reported per treatment group forerum DHEA and its metabolites and for vaginal pH and maturationalue. Pharmacokinetic parameters were calculated on day 1 anday 7, including the area under the curve from 0 to 24 h (AUC0–24 h)nd Cmax, and summarized using means and S.E.M. AUCs werealculated by a linear trapezoidal method (model-independent).onfidence intervals (95% two-tailed) were calculated for AUC0–24 h,asal and average serum steroid levels. Statistical analysis of theay 7 − day 1 differences was performed using paired t-tests withinach treatment group. Paired t-tests were used without adjustmentor multiple comparisons.
. Results
As illustrated in Fig. 1B, Tables 2 and 3, daily intravaginal appli-ation of a 1.3 ml ovule containing 0.0%, 0.5%, 1.0% or 1.8% DHEAed to a progressive increase in serum DHEA with AUC0–24 h val-es on day 7 of 24.8 ± 4.8, 56.2 ± 8.9 (p < 0.05), 76.2 ± 10.3 (p < 0.01)nd 114.3 ± 9.97 ng h/ml (p < 0.01), respectively. There was thus27%, 207% and 361% increases over control at the 0.5%, 1.0% and.8% doses of DHEA, respectively.The average 24 h serum value of.76 ± 0.42 ng/ml of DHEA following treatment with the highestHEA dose (Table 3) is similar to the value of 4.47 ± 2.19 ng/mlbserved in forty-seven 30–35-year-old premenopausal normalomen [18]. That serum DHEA following any of the doses of DHEAsed remains within the limits of normal premenopausal women
s well illustrated in Fig. 7A.As observed previously following oral or percutaneous admin-
stration of DHEA [37], serum 5-diol follows a pattern almostuperimposable to that of DHEA, although at much lower concen-rations. In fact, the AUC0–24 h value goes from 5.60 ± 0.60 ng h/mln the placebo group on day 7 to 9.83 ± 1.14 (p < 0.05), 13.8 ± 1.87p < 0.01) and 21.0 ± 1.66 (p < 0.01) at the 0.5%, 1.0% and 1.8%HEA doses, respectively (Fig. 1D, Table 2). Such changes corre-
pond to 75%, 147% and 276% increases over control. Only the.8% DHEA dose causes an increase in serum 5-diol exceedinghe values found in normal premenopausal women (Fig. 7B) dur-
ng the 24 h following intravaginal administration of DHEA onay 7.The AUC0–24 h value of serum testo shows no significant changet the 0.5% dose (2.79 ± 0.30 ng h/ml on day 7 vs. 2.58 ± 0.33 ng h/mln the placebo group) (Fig. 2B, Table 2). At the 1.0% and 1.8% doses,
F.Labrieet
al./JournalofSteroidBiochem
istry&
Molecular
Biology111
(2008)178–194
183
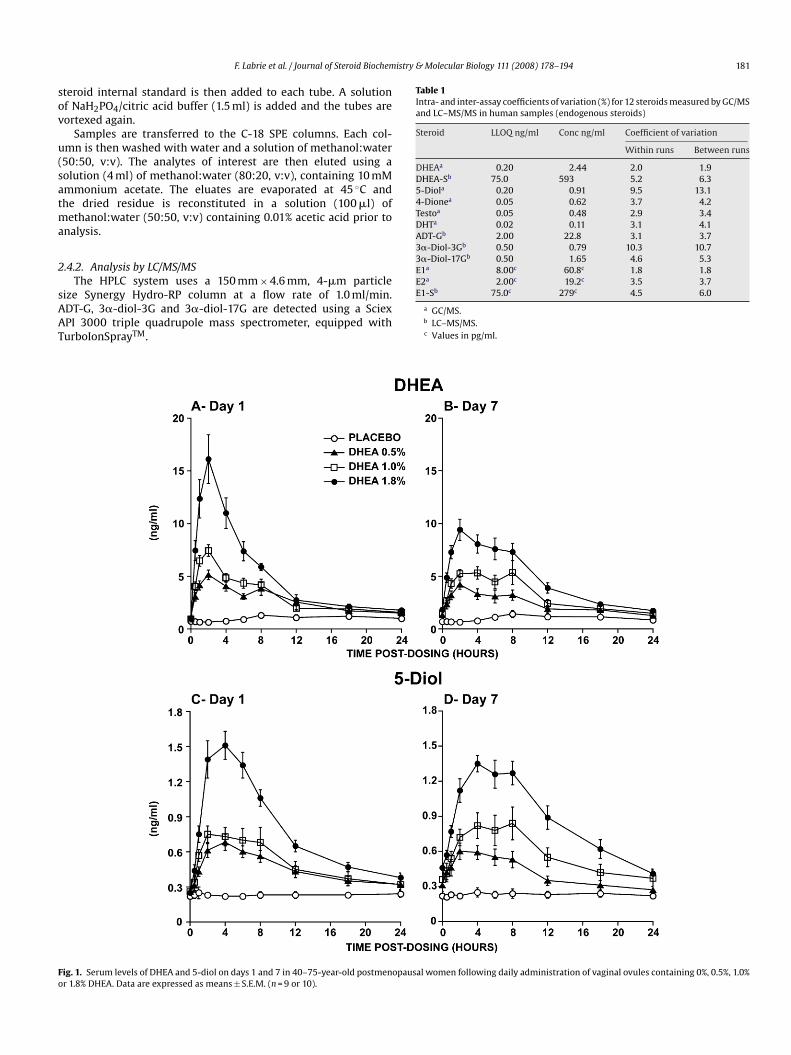
Table 2Areas under the curve (AUC0–24 h) values of DHEA and eleven of its metabolites on days 1 and 7 of daily administration of intravaginal DHEA ovules to 40-75-year-old postmenopausal women with vaginal atrophy
Group Value DHEA 5-Diol Testo DHT E1 E2
Day 1(ng h/ml)
Day 7(ng h/ml)
Day 1(ng h/ml)
Day 7(ng h/ml)
Day 1(ng h/ml)
Day 7(ng h/ml)
Day 1(ng h/ml)
Day 7(ng h/ml)
Day 1(pg h/ml)
Day 7(pg h/ml)
Day 1(pg h/ml)
Day 7(pg h/ml)
Placebo Mean 24.47 24.82 5.55 5.60 2.71a 2.58a 0.61 0.58 305.58 301.92 69.51 66.49S.E.M. 4.80 4.77 0.59 0.60 0.34 0.33 0.08 0.07 34.56 33.77 7.63 6.90
DHEA 0.5% Mean 65.49 56.17 10.91 9.83 2.79 2.79 0.91 0.93 336.52 369.69 87.79 96.93S.E.M. 7.80 8.94 1.03 1.14 0.29 0.30 0.10 0.11 37.96 48.86 11.34 16.46
DHEA 1.0% Mean 74.82 76.22 12.09 13.84 3.79 4.54 1.11 1.31 418.08 578.59 101.57 144.34S.E.M. 6.71 10.28 1.66 1.87 0.70 0.91 0.23 0.26 70.91 84.90 22.97 31.47
DHEA 1.8% Mean 123.52 114.30 18.98 21.04 5.13 5.97 1.62 1.93 433.74 600.93 89.76 136.28S.E.M. 9.43 9.96 1.05 1.66 0.72 0.69 0.19 0.23 37.68 68.35 11.65 20.27
Group Value E1-S DHEA-S 4-Dione ADT-G 3�-Diol-3G 3�-Diol-17G
Day 1(ng h/ml)
Day 7(ng h/ml)
Day 1(�g h/ml)
Day 7(�g h/ml)
Day 1(ng h/ml)
Day 7(ng h/ml)
Day 1(ng h/ml)
Day 7(ng h/ml)
Day 1(ng h/ml)
Day 7(ng h/ml)
Day 1(ng h/ml)
Day 7(ng h/ml)
Placebo Mean 3.15 2.93 8.71 8.35 6.23 6.34 176.53 167.39 12.00 12.00 12.53 12.20S.E.M. 0.62 0.47 2.41 2.22 0.71 0.80 30.86 28.87 0.00 0.00 0.53 0.20
DHEA 0.5% Mean 3.19 3.24 13.59 13.29 9.03 8.71 474.10 461.15 16.01 16.73 24.68 26.74S.E.M. 0.60 0.63 3.42 3.16 0.98 0.84 126.99 95.77 2.02 1.97 4.70 5.02
DHEA 1.0% Mean 3.14 4.37 14.42 16.49 10.28 11.06 417.73 471.54 17.12 20.14 20.88 24.94S.E.M. 0.44 0.60 3.07 2.71 1.35 1.51 66.09 59.54 2.28 3.26 4.42 4.75
DHEA 1.8% Mean 4.23 5.93 14.99 19.33 10.61 11.94 510.77 617.73 20.36 26.02 22.00 32.23S.E.M. 0.76 1.11 2.62 3.59 0.63 0.81 52.78 69.01 2.31 3.38 2.68 4.35
a Data from one patient were excluded.

184F.Labrie
etal./JournalofSteroid
Biochemistry
&M
olecularBiology
111(2008)
178–194Table 3Average serum steroid levels of DHEA and eleven of its metabolites on day 1 and 7 of daily administration of intravaginal DHEA ovules to 40–75-year-old postmenopausal women with vaginal atrophy
Group Value DHEA 5-Diol Testo DHT E1 E2
Day 1(ng/ml)
Day 7(ng/ml)
Day 1(ng/ml)
Day 7(ng/ml)
Day 1(ng/ml)
Day 7(ng/ml)
Day 1(ng/ml)
Day 7(ng/ml)
Day 1(pg/ml)
Day 7(pg/ml)
Day 1(pg/ml)
Day 7(pg/ml)
Placebo Mean 1.02 1.03 0.23 0.23 0.11a 0.11a 0.026 0.024 12.73 12.58 2.90 2.77S.E.M. 0.20 0.20 0.02 0 02 0 01 0.01 0.003 0.003 1.44 1.41 0.32 0.29
DHEA 0.5% Mean 2.73 2.34 0.45 0.41 0.12 0.12 0.038 0.039 14.02 15.40 3.66 4.04S.E.M. 0.33 0.37 0.04 0.05 0.01 0.01 0.004 0.004 1.58 2.04 0.47 0.69
DHEA 1.0% Mean 3.12 3.18 0.50 0.58 0.16 0.19 0.046 0.055 17.42 24.11 4.23 6.01S.E.M. 0.28 0.43 0.07 0.08 0.03 0.04 0.010 0.011 2.95 3.54 0.96 1.31
DHEA 1.8% Mean 5.15 4.76 0.79 0.88 0.21 0.25 0.068 0.081 18.07 25.04 3.74 5.68S.E.M. 0.39 0.42 0.04 0.07 0.03 0.03 0.008 0.010 1.57 2.85 0.49 0.84
30–35-year-old premenopausalwomen (n = 47)
Mean 4.47 0.49 0.18 0.07 53.96 82.05S.D. 2.19 0.20 0.07 0.03 23.28 42.19Median 4.14 0.44 0.17 0.07 49.47 71.385th–95th centiles 1.53–9.14 0.25–0.84 0.06–0.31 0.03–0.14 23.74–87.46 22.00–159.97(Min-max) (1.41–10.37) (0.25–0.96) (0.05–0.32) (0.03–0.17) (18.27–123.50) (17.71–181.14)
55–65-year-old postmenopausalwomen (n = 377)
Mean 1.95 0.27 0.14 0.04 17.78 4.17S.D. 1.18 0.15 0.07 0.03 10.04 3.29Median 1.72 0.25 0.13 0.03 15.58 3.445th–95th centiles 0.56–3.99 0.1–0.54 0.06–0.26 0.01–0.07 7.57–34.77 1.0–9.27(Min-max) (0.1–11.19) (0.1–0.85) (0.03–0.57) (0.01–0.29) (4.0–103.06) (1.0–30.02)
Group Value E1-S DHEA-S 4-Dione ADT-G 3�-Diol-3G 3�-Diol-17G
Day 1(ng/ml)
Day 7(ng/ml)
Day 1(�g/ml)
Day 7(�g/ml)
Day 1(ng/ml)
Day 7(ng/ml)
Day 1(ng/ml)
Day 7(ng/ml)
Day 1(ng/ml)
Day 7(ng/ml)
Day 1(ng/ml)
Day 7(ng/ml)
Placebo Mean 0.13 0.12 0.36 0.35 0.26 0.26 7.36 6.97 0.50 0.50 0.52 0.51S.E.M. 0.03 0.02 0.10 0.09 0.03 0.03 1.29 1.20 0.00 0.00 0.02 0.01
DHEA 0.5% Mean 0.13 0.13 0.57 0.55 0.38 0.36 19.75 19.21 0.67 0.70 1.03 1.11S.E.M. 0.02 0.03 0.14 0.13 0.04 0.03 5.29 3.99 0.08 0.08 0.20 0.21
DHEA 1.0% Mean 0.13 0.18 0.60 0.69 0.43 0.46 17.41 19.65 0.71 0.84 0.87 1.04S.E.M. 0.02 0.03 0.13 0.11 0.06 0.06 2.75 2.48 0.10 0.14 0.18 0.20
DHEA 1.8% Mean 0.18 0.25 0.62 0.81 0.44 0.50 21.28 25.74 0.85 1.08 0.92 1.34S.E.M. 0.03 0.05 0.11 0.15 0.03 0.03 2.20 2.88 0.10 0.14 0.11 0.18
30–35-year-old premenopausalwomen (n = 47)
Mean 1.19 1.27 0.96 40.21 1.21 1.43S.D. 0.93 0.62 0.35 29.31 0.83 0.93Median 0.87 1.04 0.92 31.62 1.06 1.355th–95th centiles 0.31–3.50 0.56–2.65 0.45–1.64 12.17–118.2 0.25–2.78 0.25–2.56(Min-max) (0.21–4.4) (0.45–2.71) (0.31–1.77) (6.86–132.6) (0.25-4.33) (0.25–5.71)
55-65-year-old postmenopausalwomen (n = 377)
Mean 0.22 0.59 0.40 15.83 0.64 0.57S.D. 0.21 0.36 0.18 12.46 0.52 0.47Median 0.17 0.55 0.37 13.11 0.55 0.255th–95th centiles 0.04–0.59 0.15–1.24 0.17–0.71 3.27–41.72 0.25-1.69 0.25–1.54(Min–max) (0.04–2.0) (0.04–2.44) (0.1–1.37) (1.0–79.4) (0.25-3.48) (0.25–3.56)
The values were obtained by dividing the AUC0–24 h values measured on days 1 and 7 by 24, thus yielding the average serum concentration of each steroid over the 24-h period. Serum steroid concentrations measured in30–35-year-old premenopausal (n = 47) and 55–65-year-old postmenopausal (n = 377) women are added as reference data [18].
a One patient excluded from the group.
istry &
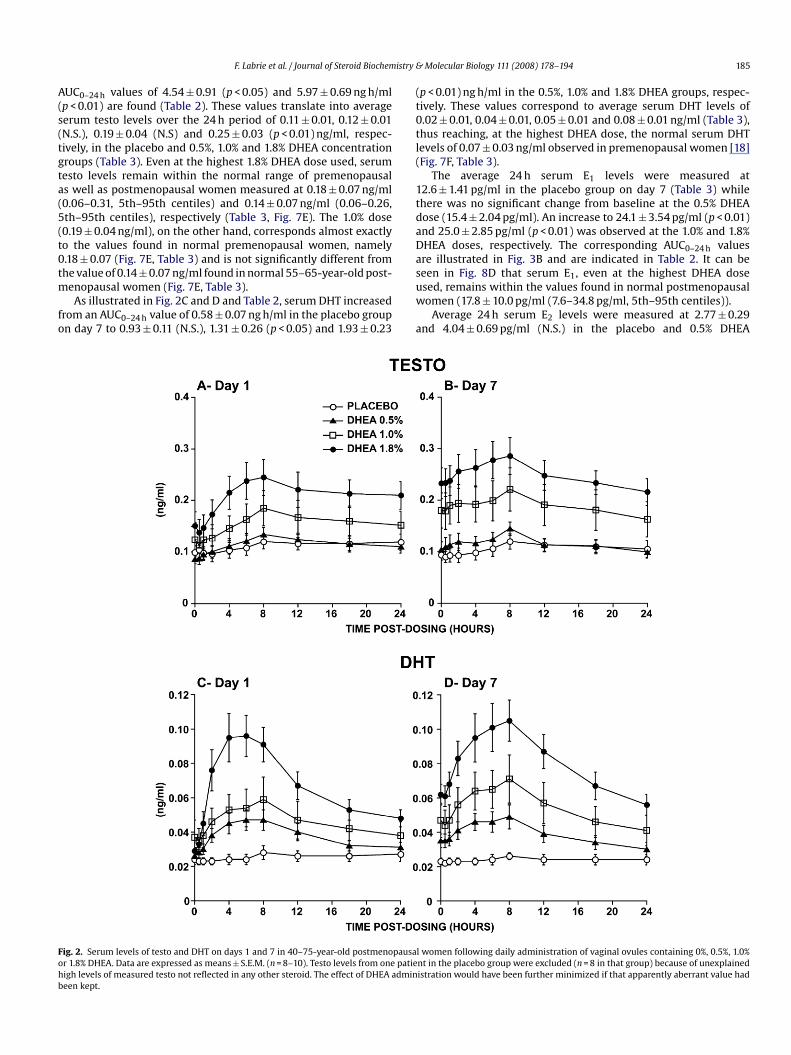
A(s(tgta(5(t0tm
fo
(t0tl(
1tdaDas
Fohb
F. Labrie et al. / Journal of Steroid Biochem
UC0–24 h values of 4.54 ± 0.91 (p < 0.05) and 5.97 ± 0.69 ng h/mlp < 0.01) are found (Table 2). These values translate into averageerum testo levels over the 24 h period of 0.11 ± 0.01, 0.12 ± 0.01N.S.), 0.19 ± 0.04 (N.S) and 0.25 ± 0.03 (p < 0.01) ng/ml, respec-ively, in the placebo and 0.5%, 1.0% and 1.8% DHEA concentrationroups (Table 3). Even at the highest 1.8% DHEA dose used, serumesto levels remain within the normal range of premenopausals well as postmenopausal women measured at 0.18 ± 0.07 ng/ml0.06–0.31, 5th–95th centiles) and 0.14 ± 0.07 ng/ml (0.06–0.26,th–95th centiles), respectively (Table 3, Fig. 7E). The 1.0% dose0.19 ± 0.04 ng/ml), on the other hand, corresponds almost exactlyo the values found in normal premenopausal women, namely.18 ± 0.07 (Fig. 7E, Table 3) and is not significantly different fromhe value of 0.14 ± 0.07 ng/ml found in normal 55–65-year-old post-
enopausal women (Fig. 7E, Table 3).As illustrated in Fig. 2C and D and Table 2, serum DHT increased
rom an AUC0–24 h value of 0.58 ± 0.07 ng h/ml in the placebo groupn day 7 to 0.93 ± 0.11 (N.S.), 1.31 ± 0.26 (p < 0.05) and 1.93 ± 0.23
uw
a
ig. 2. Serum levels of testo and DHT on days 1 and 7 in 40–75-year-old postmenopausar 1.8% DHEA. Data are expressed as means ± S.E.M. (n = 8–10). Testo levels from one patieigh levels of measured testo not reflected in any other steroid. The effect of DHEA admineen kept.
Molecular Biology 111 (2008) 178–194 185
p < 0.01) ng h/ml in the 0.5%, 1.0% and 1.8% DHEA groups, respec-ively. These values correspond to average serum DHT levels of.02 ± 0.01, 0.04 ± 0.01, 0.05 ± 0.01 and 0.08 ± 0.01 ng/ml (Table 3),hus reaching, at the highest DHEA dose, the normal serum DHTevels of 0.07 ± 0.03 ng/ml observed in premenopausal women [18]Fig. 7F, Table 3).
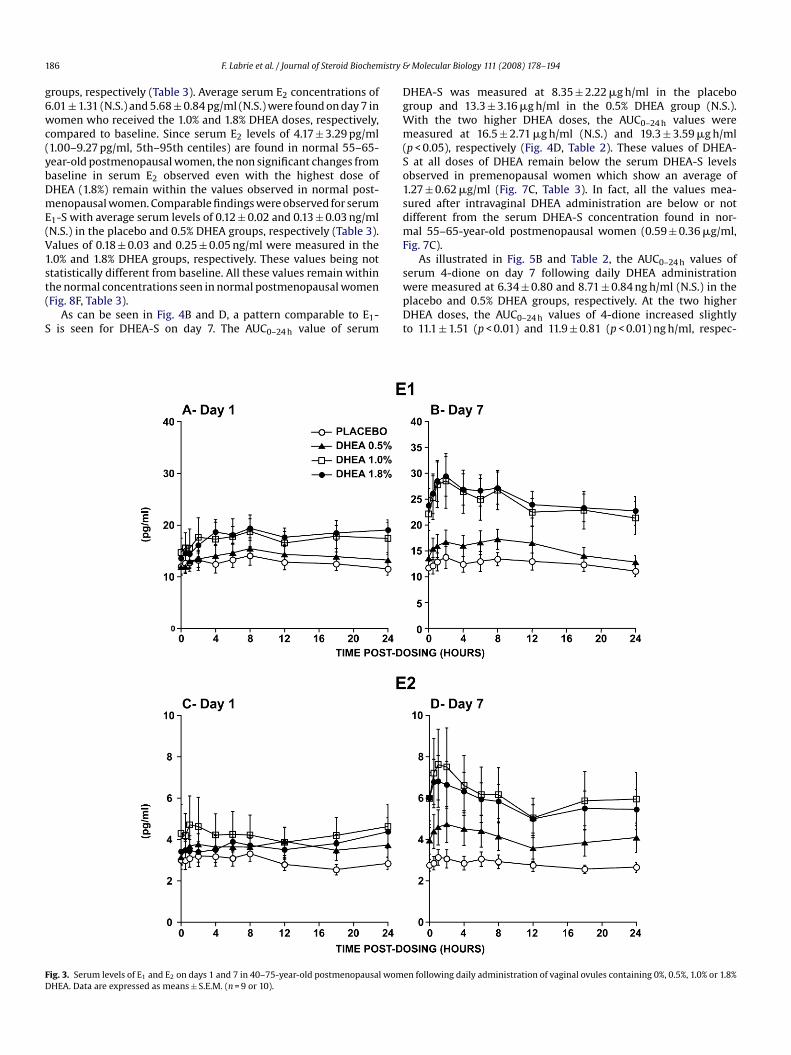
The average 24 h serum E1 levels were measured at2.6 ± 1.41 pg/ml in the placebo group on day 7 (Table 3) whilehere was no significant change from baseline at the 0.5% DHEAose (15.4 ± 2.04 pg/ml). An increase to 24.1 ± 3.54 pg/ml (p < 0.01)nd 25.0 ± 2.85 pg/ml (p < 0.01) was observed at the 1.0% and 1.8%HEA doses, respectively. The corresponding AUC0–24 h valuesre illustrated in Fig. 3B and are indicated in Table 2. It can beeen in Fig. 8D that serum E1, even at the highest DHEA dose
sed, remains within the values found in normal postmenopausalomen (17.8 ± 10.0 pg/ml (7.6–34.8 pg/ml, 5th–95th centiles)).Average 24 h serum E2 levels were measured at 2.77 ± 0.29nd 4.04 ± 0.69 pg/ml (N.S.) in the placebo and 0.5% DHEA
l women following daily administration of vaginal ovules containing 0%, 0.5%, 1.0%nt in the placebo group were excluded (n = 8 in that group) because of unexplainedistration would have been further minimized if that apparently aberrant value had
1 istry &
g6wc(ybDmE(V1st(
S
DgWm(So1sdmF
FD
86 F. Labrie et al. / Journal of Steroid Biochem
roups, respectively (Table 3). Average serum E2 concentrations of.01 ± 1.31 (N.S.) and 5.68 ± 0.84 pg/ml (N.S.) were found on day 7 inomen who received the 1.0% and 1.8% DHEA doses, respectively,
ompared to baseline. Since serum E2 levels of 4.17 ± 3.29 pg/ml1.00–9.27 pg/ml, 5th–95th centiles) are found in normal 55–65-ear-old postmenopausal women, the non significant changes fromaseline in serum E2 observed even with the highest dose ofHEA (1.8%) remain within the values observed in normal post-enopausal women. Comparable findings were observed for serum
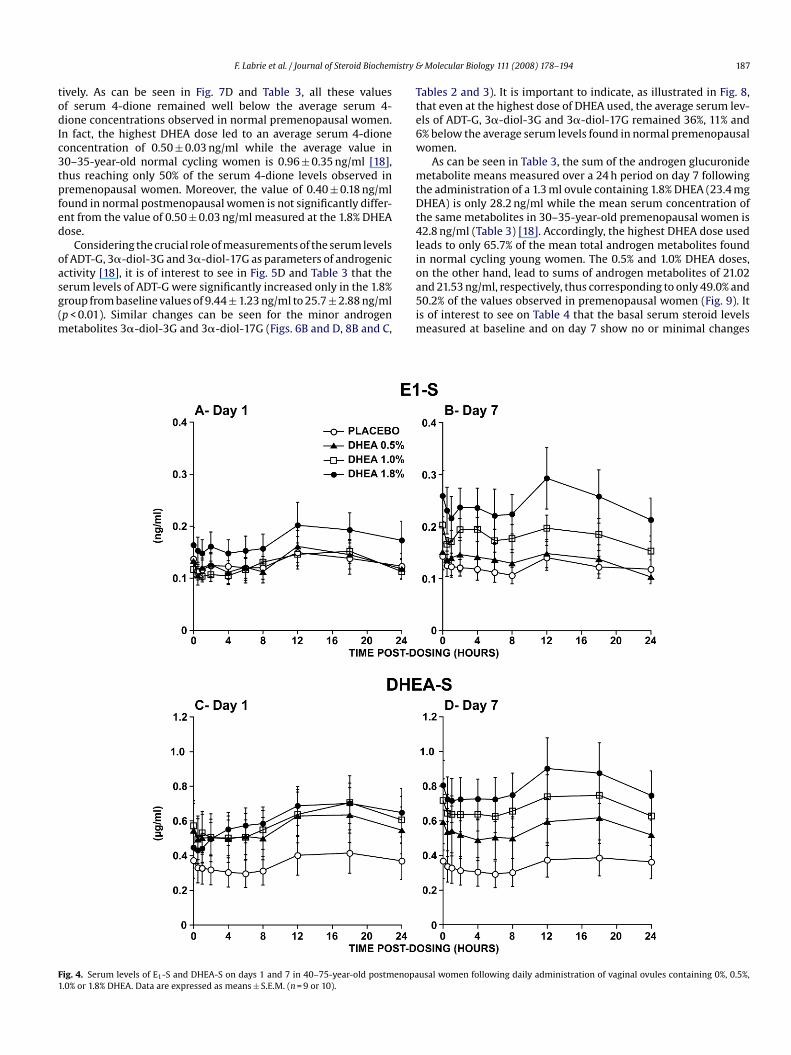
1-S with average serum levels of 0.12 ± 0.02 and 0.13 ± 0.03 ng/mlN.S.) in the placebo and 0.5% DHEA groups, respectively (Table 3).alues of 0.18 ± 0.03 and 0.25 ± 0.05 ng/ml were measured in the.0% and 1.8% DHEA groups, respectively. These values being not
tatistically different from baseline. All these values remain withinhe normal concentrations seen in normal postmenopausal womenFig. 8F, Table 3).As can be seen in Fig. 4B and D, a pattern comparable to E1-is seen for DHEA-S on day 7. The AUC0–24 h value of serum
swpDt
ig. 3. Serum levels of E1 and E2 on days 1 and 7 in 40–75-year-old postmenopausal womHEA. Data are expressed as means ± S.E.M. (n = 9 or 10).
Molecular Biology 111 (2008) 178–194
HEA-S was measured at 8.35 ± 2.22 �g h/ml in the placeboroup and 13.3 ± 3.16 �g h/ml in the 0.5% DHEA group (N.S.).ith the two higher DHEA doses, the AUC0–24 h values wereeasured at 16.5 ± 2.71 �g h/ml (N.S.) and 19.3 ± 3.59 �g h/ml
p < 0.05), respectively (Fig. 4D, Table 2). These values of DHEA-at all doses of DHEA remain below the serum DHEA-S levels
bserved in premenopausal women which show an average of.27 ± 0.62 �g/ml (Fig. 7C, Table 3). In fact, all the values mea-ured after intravaginal DHEA administration are below or notifferent from the serum DHEA-S concentration found in nor-al 55–65-year-old postmenopausal women (0.59 ± 0.36 �g/ml,
ig. 7C).As illustrated in Fig. 5B and Table 2, the AUC0–24 h values of
erum 4-dione on day 7 following daily DHEA administrationere measured at 6.34 ± 0.80 and 8.71 ± 0.84 ng h/ml (N.S.) in thelacebo and 0.5% DHEA groups, respectively. At the two higherHEA doses, the AUC0–24 h values of 4-dione increased slightly
o 11.1 ± 1.51 (p < 0.01) and 11.9 ± 0.81 (p < 0.01) ng h/ml, respec-
en following daily administration of vaginal ovules containing 0%, 0.5%, 1.0% or 1.8%
istry &
todIc3tpfed
oasg(m
Tte6w
mtDt4li
F1
F. Labrie et al. / Journal of Steroid Biochem
ively. As can be seen in Fig. 7D and Table 3, all these valuesf serum 4-dione remained well below the average serum 4-ione concentrations observed in normal premenopausal women.
n fact, the highest DHEA dose led to an average serum 4-dioneoncentration of 0.50 ± 0.03 ng/ml while the average value in0–35-year-old normal cycling women is 0.96 ± 0.35 ng/ml [18],hus reaching only 50% of the serum 4-dione levels observed inremenopausal women. Moreover, the value of 0.40 ± 0.18 ng/mlound in normal postmenopausal women is not significantly differ-nt from the value of 0.50 ± 0.03 ng/ml measured at the 1.8% DHEAose.
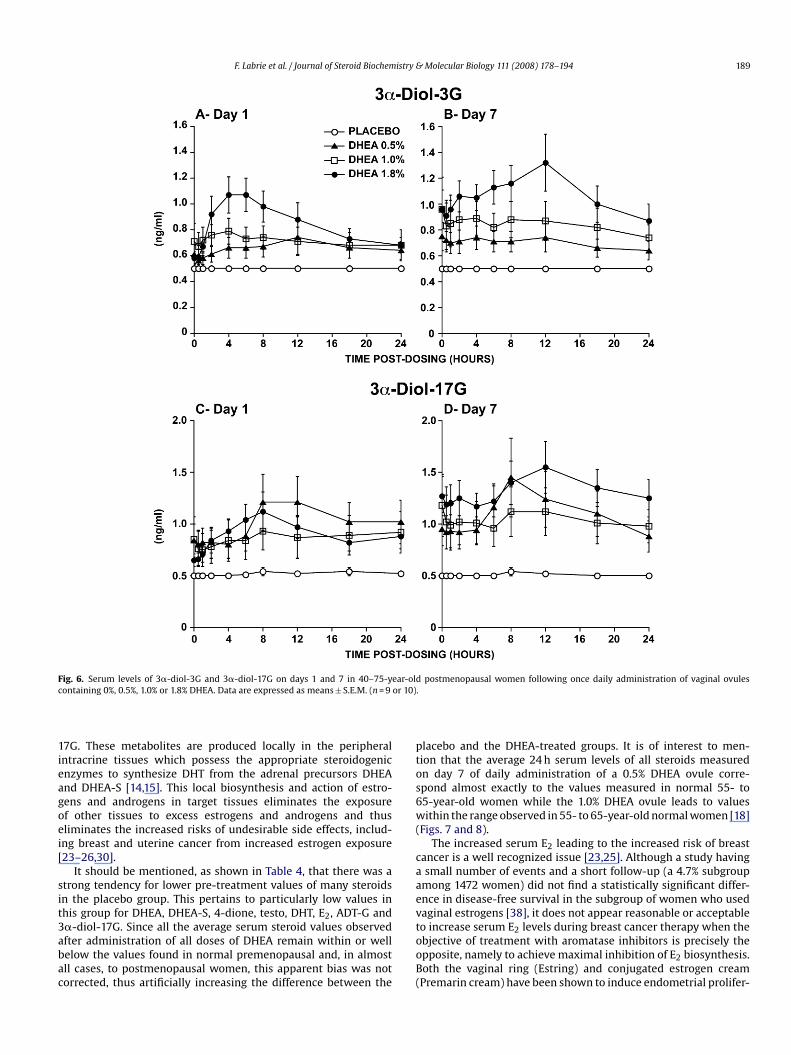
Considering the crucial role of measurements of the serum levelsf ADT-G, 3�-diol-3G and 3�-diol-17G as parameters of androgenic
ctivity [18], it is of interest to see in Fig. 5D and Table 3 that theerum levels of ADT-G were significantly increased only in the 1.8%roup from baseline values of 9.44 ± 1.23 ng/ml to 25.7 ± 2.88 ng/mlp < 0.01). Similar changes can be seen for the minor androgenetabolites 3�-diol-3G and 3�-diol-17G (Figs. 6B and D, 8B and C,
oa5im
ig. 4. Serum levels of E1-S and DHEA-S on days 1 and 7 in 40–75-year-old postmenopa.0% or 1.8% DHEA. Data are expressed as means ± S.E.M. (n = 9 or 10).
Molecular Biology 111 (2008) 178–194 187
ables 2 and 3). It is important to indicate, as illustrated in Fig. 8,hat even at the highest dose of DHEA used, the average serum lev-ls of ADT-G, 3�-diol-3G and 3�-diol-17G remained 36%, 11% and% below the average serum levels found in normal premenopausalomen.
As can be seen in Table 3, the sum of the androgen glucuronideetabolite means measured over a 24 h period on day 7 following
he administration of a 1.3 ml ovule containing 1.8% DHEA (23.4 mgHEA) is only 28.2 ng/ml while the mean serum concentration of
he same metabolites in 30–35-year-old premenopausal women is2.8 ng/ml (Table 3) [18]. Accordingly, the highest DHEA dose used
eads to only 65.7% of the mean total androgen metabolites foundn normal cycling young women. The 0.5% and 1.0% DHEA doses,
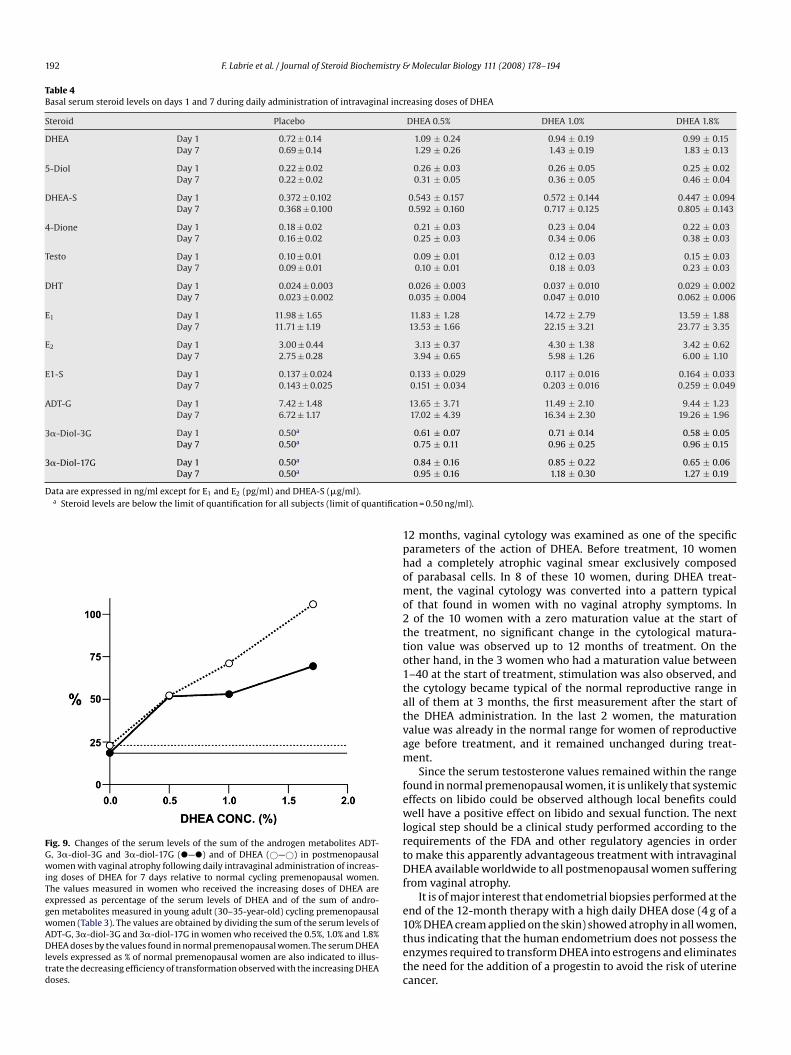
n the other hand, lead to sums of androgen metabolites of 21.02nd 21.53 ng/ml, respectively, thus corresponding to only 49.0% and0.2% of the values observed in premenopausal women (Fig. 9). Its of interest to see on Table 4 that the basal serum steroid levelseasured at baseline and on day 7 show no or minimal changes
usal women following daily administration of vaginal ovules containing 0%, 0.5%,

1 istry &
ww
n(rf(tmb
4
nit
lw[
ppagscltt
F1
88 F. Labrie et al. / Journal of Steroid Biochem
ith values within the range found in normal postmenopausalomen.
After only 1 week of daily administration of the DHEA intravagi-al ovules, the maturation value increased by 107% (p < 0.01), 75%p < 0.05) and 150% (p < 0.01) in the 0.5%, 1.0% and 1.8% DHEA groups,espectively (Fig. 10A). Vaginal pH, on the other hand, decreasedrom 6.29 ± 0.21 to 5.75 ± 0.27 (p < 0.05), 6.47 ± 0.23 to 5.76 ± 0.22p < 0.01) and 6.53 ± 0.25 to 5.86 ± 0.28 (p < 0.05), respectively, inhe 0.5%, 1.0% and 1.8% DHEA groups (Fig. 10B). No change of the
aturation value or vaginal pH was observed in the placebo groupetween days 1 and 7.
. Discussion
The present data show for the first time that the intravagi-al administration of DHEA can rapidly increase the maturation
ndex and decrease the pH in vaginal atrophy. Most impor-antly, this effect is achieved while maintaining serum estrogen
cv[om
ig. 5. Serum levels of 4-dione and ADT-G on days 1 and 7 in 40–75-year-old postmenop.0% or 1.8% DHEA. Data are expressed as means ± S.E.M. (n = 9 or 10).
Molecular Biology 111 (2008) 178–194
evels within the values found in normal postmenopausalomen, thus avoiding the risk of breast or uterine cancer
23–26].As well demonstrated in our previous studies [13–15,37], sup-
lementation with physiological amounts of exogenous DHEAermits the biosynthesis of androgens and estrogens only in theppropriate target tissues which contain the required steroido-enic enzymes [14]. The active androgens and estrogens thusynthesized in peripheral tissues exert their action in the sameells where their formation takes place. Most importantly, veryittle leakage of the active sex steroids into the circulationakes place, thus explaining the beneficial effects observed inhe vagina in the present study with no significant change in
irculating estrogens or androgens. In fact, as observed pre-iously following oral or percutaneous DHEA administration18,37], the most striking effects of DHEA administration aren the circulating levels of the glucuronide derivatives of theetabolites of DHT, namely ADT-G, 3�-diol-3G, and 3�-diol-ausal women following daily administration of vaginal ovules containing 0%, 0.5%,
F. Labrie et al. / Journal of Steroid Biochemistry & Molecular Biology 111 (2008) 178–194 189
F ar-oldc or 10)
1ieagoei[
sit3abac
ptos6w(
caaev
ig. 6. Serum levels of 3�-diol-3G and 3�-diol-17G on days 1 and 7 in 40–75-yeontaining 0%, 0.5%, 1.0% or 1.8% DHEA. Data are expressed as means ± S.E.M. (n = 9
7G. These metabolites are produced locally in the peripheralntracrine tissues which possess the appropriate steroidogenicnzymes to synthesize DHT from the adrenal precursors DHEAnd DHEA-S [14,15]. This local biosynthesis and action of estro-ens and androgens in target tissues eliminates the exposuref other tissues to excess estrogens and androgens and thusliminates the increased risks of undesirable side effects, includ-ng breast and uterine cancer from increased estrogen exposure23–26,30].
It should be mentioned, as shown in Table 4, that there was atrong tendency for lower pre-treatment values of many steroidsn the placebo group. This pertains to particularly low values inhis group for DHEA, DHEA-S, 4-dione, testo, DHT, E2, ADT-G and
�-diol-17G. Since all the average serum steroid values observedfter administration of all doses of DHEA remain within or wellelow the values found in normal premenopausal and, in almostll cases, to postmenopausal women, this apparent bias was notorrected, thus artificially increasing the difference between thetooB(
postmenopausal women following once daily administration of vaginal ovules.
lacebo and the DHEA-treated groups. It is of interest to men-ion that the average 24 h serum levels of all steroids measuredn day 7 of daily administration of a 0.5% DHEA ovule corre-pond almost exactly to the values measured in normal 55- to5-year-old women while the 1.0% DHEA ovule leads to valuesithin the range observed in 55- to 65-year-old normal women [18]
Figs. 7 and 8).The increased serum E2 leading to the increased risk of breast
ancer is a well recognized issue [23,25]. Although a study havingsmall number of events and a short follow-up (a 4.7% subgroup
mong 1472 women) did not find a statistically significant differ-nce in disease-free survival in the subgroup of women who usedaginal estrogens [38], it does not appear reasonable or acceptable
o increase serum E2 levels during breast cancer therapy when thebjective of treatment with aromatase inhibitors is precisely thepposite, namely to achieve maximal inhibition of E2 biosynthesis.oth the vaginal ring (Estring) and conjugated estrogen creamPremarin cream) have been shown to induce endometrial prolifer-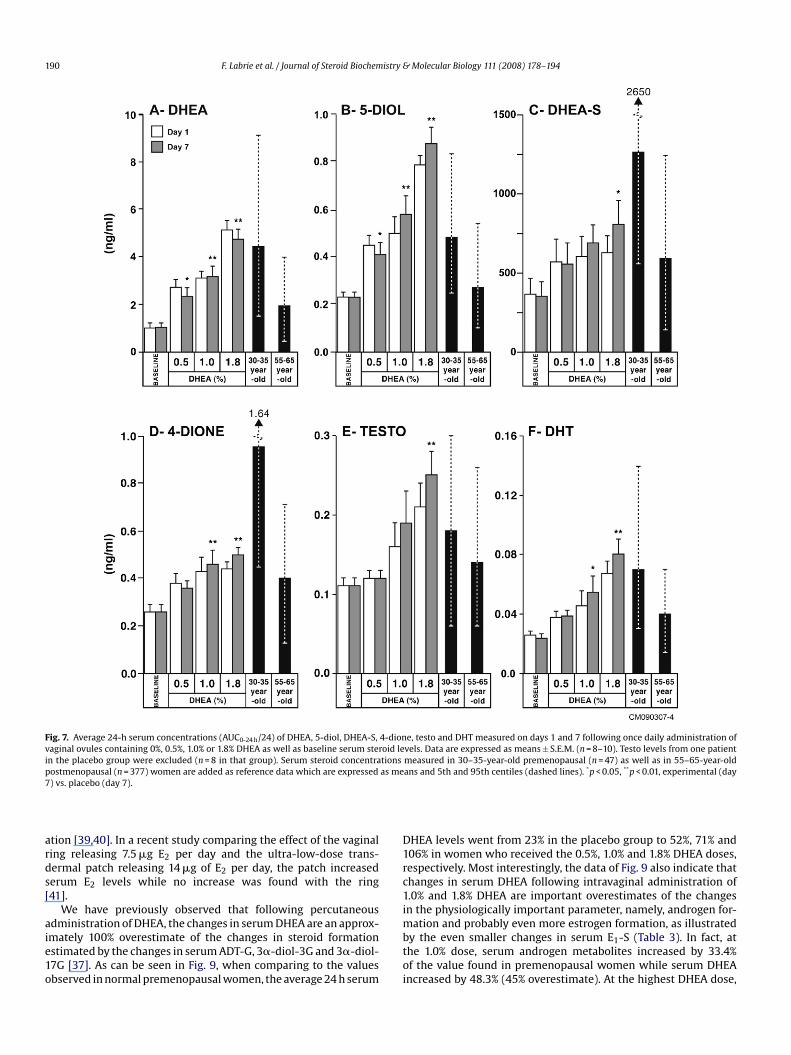
190 F. Labrie et al. / Journal of Steroid Biochemistry & Molecular Biology 111 (2008) 178–194
Fig. 7. Average 24-h serum concentrations (AUC0-24 h/24) of DHEA, 5-diol, DHEA-S, 4-dione, testo and DHT measured on days 1 and 7 following once daily administration ofvaginal ovules containing 0%, 0.5%, 1.0% or 1.8% DHEA as well as baseline serum steroid levels. Data are expressed as means ± S.E.M. (n = 8–10). Testo levels from one patientin the placebo group were excluded (n = 8 in that group). Serum steroid concentrations measured in 30–35-year-old premenopausal (n = 47) as well as in 55–65-year-oldp as me * **
7
ards[
aie1o
D1rc1i
ostmenopausal (n = 377) women are added as reference data which are expressed) vs. placebo (day 7).
tion [39,40]. In a recent study comparing the effect of the vaginaling releasing 7.5 �g E2 per day and the ultra-low-dose trans-ermal patch releasing 14 �g of E2 per day, the patch increasederum E2 levels while no increase was found with the ring41].
We have previously observed that following percutaneous
dministration of DHEA, the changes in serum DHEA are an approx-mately 100% overestimate of the changes in steroid formationstimated by the changes in serum ADT-G, 3�-diol-3G and 3�-diol-7G [37]. As can be seen in Fig. 9, when comparing to the valuesbserved in normal premenopausal women, the average 24 h serummbtoi
ans and 5th and 95th centiles (dashed lines). p < 0.05, p < 0.01, experimental (day
HEA levels went from 23% in the placebo group to 52%, 71% and06% in women who received the 0.5%, 1.0% and 1.8% DHEA doses,espectively. Most interestingly, the data of Fig. 9 also indicate thathanges in serum DHEA following intravaginal administration of.0% and 1.8% DHEA are important overestimates of the changesn the physiologically important parameter, namely, androgen for-
ation and probably even more estrogen formation, as illustratedy the even smaller changes in serum E1-S (Table 3). In fact, athe 1.0% dose, serum androgen metabolites increased by 33.4%f the value found in premenopausal women while serum DHEAncreased by 48.3% (45% overestimate). At the highest DHEA dose,

F. Labrie et al. / Journal of Steroid Biochemistry & Molecular Biology 111 (2008) 178–194 191
Fig. 8. Average 24-h serum concentrations (AUC0-24 h/24) of ADT-G, 3�-diol-3G, 3�-diol-17G, E1, E2 and E1-S measured on days 1 and 7 following daily administration ofvaginal ovules containing 0%, 0.5%, 1.0% or 1.8% DHEA as well as baseline serum steroid levels. Data are expressed as means ± S.E.M. (n = 9 or 10). Serum steroid concentrationsmeasured in 30–35-year-old premenopausal (n = 47) and 55–65-year-old postmenopausal (n = 377) women are added as reference data which are expressed as means and5th and 95th centiles (dashed lines). *p < 0.05, **p < 0.01, experimental (day 7) vs. placebo (day 7).
sDlt[
Dhmccwme
eocgr(ieD
erum androgen metabolites increased by only 49.7% while serumHEA increased by 83.7% (68% overestimate). Since serum E1-S is
ikely to reflect total estrogen formation, the present data confirmhat very little estrogen formation follows DHEA administration14].
The morphological changes observed in the rat vagina afterHEA treatment reflect its local conversion into active sex steroidsaving androgenic and/or estrogenic action through intracrineechanisms [13]. These changes include marked epithelial mucifi-
ation, high compactness of delicate, finely woven lamina propriaollagen fibers and a moderate muscularis thickness increasehen compared to ovariectomized (OVX) animals [34]. Theseorphological changes are typical of androgenic effects. In the
pithelium treated with DHEA, there is appearance of many lay-
e
law
rs of large mucous cells with the presence of large vacuolesverlaying a few layers of squamous epithelium and a basalell layer. In the lamina propria, fine newly synthesized colla-en fibers are seen near the epithelium. Labeling of the androgeneceptor is increased by about 3-fold in the three vaginal layersepithelium, lamina propria and muscularis) after DHEA admin-stration [34]. It is thus most likely that the rapid beneficialffects observed within a week of treatment with intravaginalHEA result from a combination of estrogenic and androgenic
ffects.The beneficial effects of DHEA on the vaginal atrophic epithe-ium have been previously observed in postmenopausal womenfter percutaneous administration of DHEA [42]. In that studyhere women received DHEA by percutaneous administration for
192 F. Labrie et al. / Journal of Steroid Biochemistry & Molecular Biology 111 (2008) 178–194
Table 4Basal serum steroid levels on days 1 and 7 during daily administration of intravaginal increasing doses of DHEA
Steroid Placebo DHEA 0.5% DHEA 1.0% DHEA 1.8%
DHEA Day 1 0.72 ± 0.14 1.09 ± 0.24 0.94 ± 0.19 0.99 ± 0.15Day 7 0.69 ± 0.14 1.29 ± 0.26 1.43 ± 0.19 1.83 ± 0.13
5-Diol Day 1 0.22 ± 0.02 0.26 ± 0.03 0.26 ± 0.05 0.25 ± 0.02Day 7 0.22 ± 0.02 0.31 ± 0.05 0.36 ± 0.05 0.46 ± 0.04
DHEA-S Day 1 0.372 ± 0.102 0.543 ± 0.157 0.572 ± 0.144 0.447 ± 0.094Day 7 0.368 ± 0.100 0.592 ± 0.160 0.717 ± 0.125 0.805 ± 0.143
4-Dione Day 1 0.18 ± 0.02 0.21 ± 0.03 0.23 ± 0.04 0.22 ± 0.03Day 7 0.16 ± 0.02 0.25 ± 0.03 0.34 ± 0.06 0.38 ± 0.03
Testo Day 1 0.10 ± 0.01 0.09 ± 0.01 0.12 ± 0.03 0.15 ± 0.03Day 7 0.09 ± 0.01 0.10 ± 0.01 0.18 ± 0.03 0.23 ± 0.03
DHT Day 1 0.024 ± 0.003 0.026 ± 0.003 0.037 ± 0.010 0.029 ± 0.002Day 7 0.023 ± 0.002 0.035 ± 0.004 0.047 ± 0.010 0.062 ± 0.006
E1 Day 1 11.98 ± 1.65 11.83 ± 1.28 14.72 ± 2.79 13.59 ± 1.88Day 7 11.71 ± 1.19 13.53 ± 1.66 22.15 ± 3.21 23.77 ± 3.35
E2 Day 1 3.00 ± 0.44 3.13 ± 0.37 4.30 ± 1.38 3.42 ± 0.62Day 7 2.75 ± 0.28 3.94 ± 0.65 5.98 ± 1.26 6.00 ± 1.10
E1-S Day 1 0.137 ± 0.024 0.133 ± 0.029 0.117 ± 0.016 0.164 ± 0.033Day 7 0.143 ± 0.025 0.151 ± 0.034 0.203 ± 0.016 0.259 ± 0.049
ADT-G Day 1 7.42 ± 1.48 13.65 ± 3.71 11.49 ± 2.10 9.44 ± 1.23Day 7 6.72 ± 1.17 17.02 ± 4.39 16.34 ± 2.30 19.26 ± 1.96
3�-Diol-3G Day 1 0.50a 0.61 ± 0.07 0.71 ± 0.14 0.58 ± 0.05Day 7 0.50a 0.75 ± 0.11 0.96 ± 0.25 0.96 ± 0.15
3�-Diol-17G Day 1 0.50a 0.84 ± 0.16 0.85 ± 0.22 0.65 ± 0.06Day 7 0.50a
Data are expressed in ng/ml except for E1 and E2 (pg/ml) and DHEA-S (�g/ml).a Steroid levels are below the limit of quantification for all subjects (limit of quantificat
Fig. 9. Changes of the serum levels of the sum of the androgen metabolites ADT-G, 3�-diol-3G and 3�-diol-17G (�—�) and of DHEA (©—©) in postmenopausalwomen with vaginal atrophy following daily intravaginal administration of increas-ing doses of DHEA for 7 days relative to normal cycling premenopausal women.The values measured in women who received the increasing doses of DHEA areexpressed as percentage of the serum levels of DHEA and of the sum of andro-gen metabolites measured in young adult (30–35-year-old) cycling premenopausalwomen (Table 3). The values are obtained by dividing the sum of the serum levels ofADT-G, 3�-diol-3G and 3�-diol-17G in women who received the 0.5%, 1.0% and 1.8%DHEA doses by the values found in normal premenopausal women. The serum DHEAlevels expressed as % of normal premenopausal women are also indicated to illus-trate the decreasing efficiency of transformation observed with the increasing DHEAdoses.
1phomo2tto1tatvam
fewlrtDf
e1tetc
0.95 ± 0.16 1.18 ± 0.30 1.27 ± 0.19
ion = 0.50 ng/ml).
2 months, vaginal cytology was examined as one of the specificarameters of the action of DHEA. Before treatment, 10 womenad a completely atrophic vaginal smear exclusively composedf parabasal cells. In 8 of these 10 women, during DHEA treat-ent, the vaginal cytology was converted into a pattern typical
f that found in women with no vaginal atrophy symptoms. Inof the 10 women with a zero maturation value at the start of
he treatment, no significant change in the cytological matura-ion value was observed up to 12 months of treatment. On thether hand, in the 3 women who had a maturation value between–40 at the start of treatment, stimulation was also observed, andhe cytology became typical of the normal reproductive range inll of them at 3 months, the first measurement after the start ofhe DHEA administration. In the last 2 women, the maturationalue was already in the normal range for women of reproductivege before treatment, and it remained unchanged during treat-ent.Since the serum testosterone values remained within the range
ound in normal premenopausal women, it is unlikely that systemicffects on libido could be observed although local benefits couldell have a positive effect on libido and sexual function. The next
ogical step should be a clinical study performed according to theequirements of the FDA and other regulatory agencies in ordero make this apparently advantageous treatment with intravaginalHEA available worldwide to all postmenopausal women suffering
rom vaginal atrophy.It is of major interest that endometrial biopsies performed at the
nd of the 12-month therapy with a high daily DHEA dose (4 g of a
0% DHEA cream applied on the skin) showed atrophy in all women,hus indicating that the human endometrium does not possess thenzymes required to transform DHEA into estrogens and eliminateshe need for the addition of a progestin to avoid the risk of uterineancer.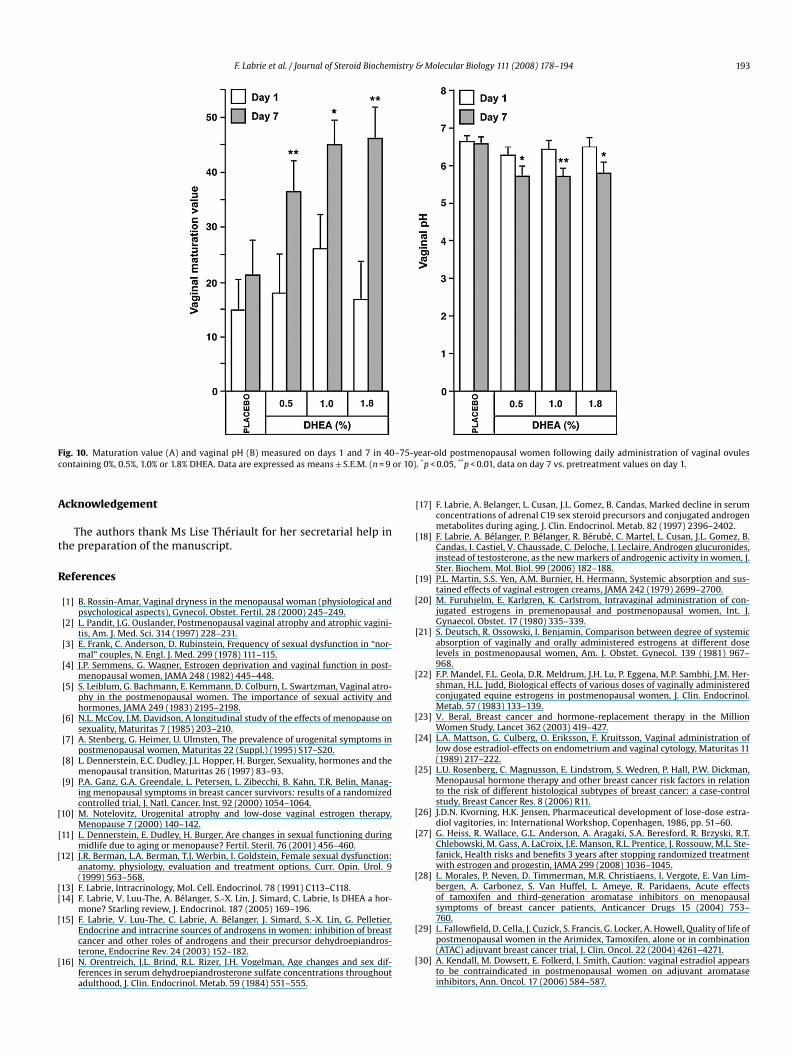
F. Labrie et al. / Journal of Steroid Biochemistry & Molecular Biology 111 (2008) 178–194 193
F –75-yc or 10)
A
t
R
[
[
[
[[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ig. 10. Maturation value (A) and vaginal pH (B) measured on days 1 and 7 in 40ontaining 0%, 0.5%, 1.0% or 1.8% DHEA. Data are expressed as means ± S.E.M. (n = 9
cknowledgement
The authors thank Ms Lise Thériault for her secretarial help inhe preparation of the manuscript.
eferences
[1] B. Rossin-Amar, Vaginal dryness in the menopausal woman (physiological andpsychological aspects), Gynecol. Obstet. Fertil. 28 (2000) 245–249.
[2] L. Pandit, J.G. Ouslander, Postmenopausal vaginal atrophy and atrophic vagini-tis, Am. J. Med. Sci. 314 (1997) 228–231.
[3] E. Frank, C. Anderson, D. Rubinstein, Frequency of sexual dysfunction in “nor-mal” couples, N. Engl. J. Med. 299 (1978) 111–115.
[4] J.P. Semmens, G. Wagner, Estrogen deprivation and vaginal function in post-menopausal women, JAMA 248 (1982) 445–448.
[5] S. Leiblum, G. Bachmann, E. Kemmann, D. Colburn, L. Swartzman, Vaginal atro-phy in the postmenopausal women. The importance of sexual activity andhormones, JAMA 249 (1983) 2195–2198.
[6] N.L. McCoy, J.M. Davidson, A longitudinal study of the effects of menopause onsexuality, Maturitas 7 (1985) 203–210.
[7] A. Stenberg, G. Heimer, U. Ulmsten, The prevalence of urogenital symptoms inpostmenopausal women, Maturitas 22 (Suppl.) (1995) S17–S20.
[8] L. Dennerstein, E.C. Dudley, J.L. Hopper, H. Burger, Sexuality, hormones and themenopausal transition, Maturitas 26 (1997) 83–93.
[9] P.A. Ganz, G.A. Greendale, L. Petersen, L. Zibecchi, B. Kahn, T.R. Belin, Manag-ing menopausal symptoms in breast cancer survivors: results of a randomizedcontrolled trial, J. Natl. Cancer. Inst. 92 (2000) 1054–1064.
10] M. Notelovitz, Urogenital atrophy and low-dose vaginal estrogen therapy,Menopause 7 (2000) 140–142.
11] L. Dennerstein, E. Dudley, H. Burger, Are changes in sexual functioning duringmidlife due to aging or menopause? Fertil. Steril. 76 (2001) 456–460.
12] J.R. Berman, L.A. Berman, T.J. Werbin, I. Goldstein, Female sexual dysfunction:anatomy, physiology, evaluation and treatment options, Curr. Opin. Urol. 9(1999) 563–568.
13] F. Labrie, Intracrinology, Mol. Cell. Endocrinol. 78 (1991) C113–C118.14] F. Labrie, V. Luu-The, A. Bélanger, S.-X. Lin, J. Simard, C. Labrie, Is DHEA a hor-
mone? Starling review, J. Endocrinol. 187 (2005) 169–196.15] F. Labrie, V. Luu-The, C. Labrie, A. Bélanger, J. Simard, S.-X. Lin, G. Pelletier,
Endocrine and intracrine sources of androgens in women: inhibition of breastcancer and other roles of androgens and their precursor dehydroepiandros-terone, Endocrine Rev. 24 (2003) 152–182.
16] N. Orentreich, J.L. Brind, R.L. Rizer, J.H. Vogelman, Age changes and sex dif-ferences in serum dehydroepiandrosterone sulfate concentrations throughoutadulthood, J. Clin. Endocrinol. Metab. 59 (1984) 551–555.
[
[
ear-old postmenopausal women following daily administration of vaginal ovules. *p < 0.05, **p < 0.01, data on day 7 vs. pretreatment values on day 1.
17] F. Labrie, A. Belanger, L. Cusan, J.L. Gomez, B. Candas, Marked decline in serumconcentrations of adrenal C19 sex steroid precursors and conjugated androgenmetabolites during aging, J. Clin. Endocrinol. Metab. 82 (1997) 2396–2402.
18] F. Labrie, A. Bélanger, P. Bélanger, R. Bérubé, C. Martel, L. Cusan, J.L. Gomez, B.Candas, I. Castiel, V. Chaussade, C. Deloche, J. Leclaire, Androgen glucuronides,instead of testosterone, as the new markers of androgenic activity in women, J.Ster. Biochem. Mol. Biol. 99 (2006) 182–188.
19] P.L. Martin, S.S. Yen, A.M. Burnier, H. Hermann, Systemic absorption and sus-tained effects of vaginal estrogen creams, JAMA 242 (1979) 2699–2700.
20] M. Furuhjelm, E. Karlgren, K. Carlstrom, Intravaginal administration of con-jugated estrogens in premenopausal and postmenopausal women, Int. J.Gynaecol. Obstet. 17 (1980) 335–339.
21] S. Deutsch, R. Ossowski, I. Benjamin, Comparison between degree of systemicabsorption of vaginally and orally administered estrogens at different doselevels in postmenopausal women, Am. J. Obstet. Gynecol. 139 (1981) 967–968.
22] F.P. Mandel, F.L. Geola, D.R. Meldrum, J.H. Lu, P. Eggena, M.P. Sambhi, J.M. Her-shman, H.L. Judd, Biological effects of various doses of vaginally administeredconjugated equine estrogens in postmenopausal women, J. Clin. Endocrinol.Metab. 57 (1983) 133–139.
23] V. Beral, Breast cancer and hormone-replacement therapy in the MillionWomen Study, Lancet 362 (2003) 419–427.
24] L.A. Mattson, G. Culberg, O. Eriksson, F. Kruitsson, Vaginal administration oflow dose estradiol-effects on endometrium and vaginal cytology, Maturitas 11(1989) 217–222.
25] L.U. Rosenberg, C. Magnusson, E. Lindstrom, S. Wedren, P. Hall, P.W. Dickman,Menopausal hormone therapy and other breast cancer risk factors in relationto the risk of different histological subtypes of breast cancer: a case-controlstudy, Breast Cancer Res. 8 (2006) R11.
26] J.D.N. Kvorning, H.K. Jensen, Pharmaceutical development of lose-dose estra-diol vagitories, in: International Workshop, Copenhagen, 1986, pp. 51–60.
27] G. Heiss, R. Wallace, G.L. Anderson, A. Aragaki, S.A. Beresford, R. Brzyski, R.T.Chlebowski, M. Gass, A. LaCroix, J.E. Manson, R.L. Prentice, J. Rossouw, M.L. Ste-fanick, Health risks and benefits 3 years after stopping randomized treatmentwith estrogen and progestin, JAMA 299 (2008) 1036–1045.
28] L. Morales, P. Neven, D. Timmerman, M.R. Christiaens, I. Vergote, E. Van Lim-bergen, A. Carbonez, S. Van Huffel, L. Ameye, R. Paridaens, Acute effectsof tamoxifen and third-generation aromatase inhibitors on menopausalsymptoms of breast cancer patients, Anticancer Drugs 15 (2004) 753–760.
29] L. Fallowfield, D. Cella, J. Cuzick, S. Francis, G. Locker, A. Howell, Quality of life ofpostmenopausal women in the Arimidex, Tamoxifen, alone or in combination(ATAC) adjuvant breast cancer trial, J. Clin. Oncol. 22 (2004) 4261–4271.
30] A. Kendall, M. Dowsett, E. Folkerd, I. Smith, Caution: vaginal estradiol appearsto be contraindicated in postmenopausal women on adjuvant aromataseinhibitors, Ann. Oncol. 17 (2006) 584–587.

1 istry &
[
[
[
[
[[
[
[
[
[
[
94 F. Labrie et al. / Journal of Steroid Biochem
31] I. Schiff, D. Tulchinsky, K.J. Ryan, Vaginal absorption of estrone and 17beta-estradiol, Fertil. Steril. 28 (1977) 1063–1066.
32] J.E. Rioux, C. Devlin, M.M. Gelfand, W.M. Steinberg, D.S. Hepburn, 17beta-estradiol vaginal tablet versus conjugated equine estrogen vaginal cream torelieve menopausal atrophic vaginitis, Menopause 7 (2000) 156–161.
33] M. Notelovitz, S. Funk, N. Nanavati, M. Mazzeo, Estradiol absorption from vagi-nal tablets in postmenopausal women, Obstet. Gynecol. 99 (2002) 556–562.
34] L. Berger, M. El-Alfy, C. Martel, F. Labrie, Effects of dehydroepiandrosterone,Premarin and Acolbifene on histomorphology and sex steroid receptors in therat vagina, J. Steroid. Biochem. Mol. Biol. 96 (2005) 201–215.
35] A. Meisels, The maturation value, Acta Cytol. 11 (1967) 249.36] G.L. Wied, Industrial developments in automated cytology as submitted by their
developers, Anal. Quant. Cytol. Histol. 15 (1993) 358–370.37] F. Labrie, A. Belanger, C. Labrie, B. Candas, L. Cusan, J.L. Gomez, Bioavailability
and metabolism of oral and percutaneous dehydroepiandrosterone in post-menopausal women, J. Steroid Biochem. Mol. Biol. 107 (2007) 57–69.
[
Molecular Biology 111 (2008) 178–194
38] J.E. Dew, B.G. Wren, J.A. Eden, A cohort study of topical vaginal estrogen therapyin women previously treated for breast cancer, Climacteric 6 (2003) 45–52.
39] R.A. Ayton, G.M. Darling, A.L. Murkies, E.A. Farrell, E. Weisberg, I. Selinus, I.D.Fraser, A comparative study of safety and efficacy of continuous low doseoestradiol released from a vaginal ring compared with conjugated equineoestrogen vaginal cream in the treatment of postmenopausal urogenital atro-phy, Br. J. Obstet. Gynaecol. 103 (1996) 351–358.
40] L.E. Nachtigall, Clinical trial of the estradiol vaginal ring in the U.S., Maturitas22 (Suppl.) (1995) S43–47.
41] P. Gupta, B. Ozel, F.Z. Stanczyk, J.C. Felix, D.R. Mishell Jr., The effect of transdermal
and vaginal estrogen therapy on markers of postmenopausal estrogen status,Menopause 15 (2008) 94–97.42] F. Labrie, P. Diamond, L. Cusan, J.L. Gomez, A. Belanger, B. Candas, Effect of12-month dehydroepiandrosterone replacement therapy on bone, vagina, andendometrium in postmenopausal women, J. Clin. Endocrinol. Metab. 82 (1997)3498–3505.
Related Documents











