顎関節雑音のフーリエスペクトル解析 花輪小百合 1§ 池 真樹子 1 花輪 浩司 2 奥村 泰彦 2 1 明海大学大学院歯学研究科歯学専攻 2 明海大学歯学部病態診断治療学講座歯科放射線学分野 要旨:顎関節症は歴史的に非常に古くから多くの研究が行われてきた.しかし,病態はある程度判明してきたものの, 今日までまだ病因の解明に至っていないのが現状である. 本研究は顎関節雑音に的を絞り,その発生機序の解明を最終目標に解析を行った.顎関節雑音の採取には,聴診器とマ イクロホンを組み合わせた聴音器を作製し,それを用いて波形とスペクトル解析を行った結果,以下の結論を導くことが できた. 1 .クリック音は,スペクトル上と周波数により単峰性,2 峰性,多峰性に,クレピタス音は 2 峰性と多峰性に分類する ことができた. 2 .クリック音,クレピタス音共に,主たる周波数は 50 Hz から 200 Hz の間に存在した. 3 .顎関節雑音の持続時間は,クリック音では 120 ms 以下,クレピタス音では 200 ms 以上であった. 4 .顎関節雑音は一定した周波数ではなく,発生時ごとにスペクトルが変化する非常に不安定な音であることがわかっ た. 5 .顎関節雑音の発生は,開閉口時に顎関節内で起こるインパルスによって顎顔面頭蓋内の特定部位で共振が惹起され, これが顎関節雑音として採取されることが判明した. 6 .インパルスは,クリック音の場合は円板前方転位にともなう相反性クリックに起因するものであり,クレピタス音で は骨性アルスローシスに起因するものであろうと推測された. 7 .クリック音が単発の大きなインパルスによって発生するのに対して,クレピタス音が小さなインパルスの連続したも のによって発生すると推測できた. 8 .顎関節雑音が発生時ごとに変化するのは,インパルスの発生部位,方向,大きさなどの違いから,種々の部位の固有 振動が惹起され,さらにその共振の大きさが雑音発生のたびに異なるためと推測された. 索引用語:顎関節症,顎関節雑音,FFT Fast Fourier Transform Analysis of Temporomandibular Sounds Sayuri HANAWA 1§ , Makiko IKE 1 , Koji HANAWA 2 and Yasuhiko OKUMURA 2 1 Meikai University Graduate School of Dentistry 2 Division of Dental Radiology, Department of Diagnostic & Therapeutic Sciences, Meikai University School of Dentistry Abstract : Temporomandibular joint (TMJ) disorder is not a new condition. However, although these investigations have afforded a reasonably accurate assessment regarding the symptoms, we have not attained the same level of success in terms of learning how and why TMJ disorder occurs. This study, which focused on the actual sounds produced in patients with TMJ disorder, attempted to examine the mechanism of their occurrence. An apparatus was constructed employing a stethoscope combined with a microphone to ac- quire TMJ sound data. Spectrum analyses as well as evaluation of the shape of specific sound waves were conducted on the collected samples. The conclusions are as follows : 明海歯学(J Meikai Dent Med )37 (2) , 81-100, 2008 81

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

顎関節雑音のフーリエスペクトル解析
花輪小百合1§ 池 真樹子1 花輪 浩司2 奥村 泰彦2
1明海大学大学院歯学研究科歯学専攻2明海大学歯学部病態診断治療学講座歯科放射線学分野
要旨:顎関節症は歴史的に非常に古くから多くの研究が行われてきた.しかし,病態はある程度判明してきたものの,今日までまだ病因の解明に至っていないのが現状である.本研究は顎関節雑音に的を絞り,その発生機序の解明を最終目標に解析を行った.顎関節雑音の採取には,聴診器とマイクロホンを組み合わせた聴音器を作製し,それを用いて波形とスペクトル解析を行った結果,以下の結論を導くことができた.1.クリック音は,スペクトル上と周波数により単峰性,2峰性,多峰性に,クレピタス音は 2峰性と多峰性に分類することができた.
2.クリック音,クレピタス音共に,主たる周波数は 50 Hz から 200 Hz の間に存在した.3.顎関節雑音の持続時間は,クリック音では 120 ms 以下,クレピタス音では 200 ms 以上であった.4.顎関節雑音は一定した周波数ではなく,発生時ごとにスペクトルが変化する非常に不安定な音であることがわかった.
5.顎関節雑音の発生は,開閉口時に顎関節内で起こるインパルスによって顎顔面頭蓋内の特定部位で共振が惹起され,これが顎関節雑音として採取されることが判明した.
6.インパルスは,クリック音の場合は円板前方転位にともなう相反性クリックに起因するものであり,クレピタス音では骨性アルスローシスに起因するものであろうと推測された.
7.クリック音が単発の大きなインパルスによって発生するのに対して,クレピタス音が小さなインパルスの連続したものによって発生すると推測できた.
8.顎関節雑音が発生時ごとに変化するのは,インパルスの発生部位,方向,大きさなどの違いから,種々の部位の固有振動が惹起され,さらにその共振の大きさが雑音発生のたびに異なるためと推測された.
索引用語:顎関節症,顎関節雑音,FFT
Fast Fourier Transform Analysis of Temporomandibular Sounds
Sayuri HANAWA1§, Makiko IKE1, Koji HANAWA2
and Yasuhiko OKUMURA2
1Meikai University Graduate School of Dentistry2Division of Dental Radiology, Department of Diagnostic & Therapeutic Sciences, Meikai University School of Dentistry
Abstract : Temporomandibular joint(TMJ)disorder is not a new condition. However, although these investigations have
afforded a reasonably accurate assessment regarding the symptoms, we have not attained the same level of success in terms
of learning how and why TMJ disorder occurs.
This study, which focused on the actual sounds produced in patients with TMJ disorder , attempted to examine the
mechanism of their occurrence. An apparatus was constructed employing a stethoscope combined with a microphone to ac-
quire TMJ sound data. Spectrum analyses as well as evaluation of the shape of specific sound waves were conducted on the
collected samples. The conclusions are as follows :
明海歯学(J Meikai Dent Med)37(2), 81−100, 2008 81

緒 言
顎関節症と呼ばれる疾患名は,1956年,上野ら1)によ
り下顎運動時に顎関節部の疼痛,雑音発生,開口障害等
の症状を伴う慢性疾患の臨床診断名として提唱されたこ
とに始まる.1996年,日本顎関節学会2)は,顎関節症の
疾患概念を明らかにし「顎関節症とは,顎関節や咀嚼筋
の疼痛,関節雑音,開口障害または顎運動異常を主要症
候とする慢性疾患の総括的診断名であり,その病態には
咀嚼筋障害,関節包・靭帯障害,関節円板障害,変形性
関節症などが含まれる.」と定義した.さらに症型とし
て蠢型~蠹型に分類されている.国際的には顎関節症に
相当する疾患は,temporomandibular disorder(TMD)と
して顎関節,咀嚼筋を包含する臨床的異常の一つとして
表わされている3).
TMD は歴史的にみると古代エジプト時代からみら
れ4),当時は徒手的に顎の位置を治していた.その後外
科的手術や関節円板の整復5),また関節円板の除去が行
われ6−8),TMD の症状に有効な治療法であることが報告
された.しかし,これらの治療は TMD の治療や症状の
改善にはなったが,TMD 発症の原因が明らかにされ,
それに沿った治療法ではなかった.
Costen9, 10)は,歯の欠損や咬耗によって咬合が低位と
なり,これによって下顎頭の位置が変化し,頭部や顎関
節部の症状が発生することを報告し,臼歯部の咬合の低
下とこの疾患の関係を報告した.さらに咬合論11, 12)が論
じられるようになり,咬合の概念が明らかになるにつれ
て TMD と咬合との因果関係が論じられるようになっ
た.また,咬合病という考え方が提唱されたことによ
り13),咬合と TMD とが関連付けられ,咬合改善や,咬
合の再構築がナソロジー学派の人々によって行われるよ
うになった.しかし,その後このナソロジーの考え方で
は TMD は治癒しないことが明らかとなり,同時に咬合
病は,顎関節症の単一の病因ではないと考えられるよう
になってきた.
その後,MPD 症候群(myofascial pain dysfunction syn-
drome)14)が顎関節症に導入され,治療法として薬物や行
動療法,そしてスプリント療法が用いられるようになっ
た.顎関節症はこの頃から単一病因説から多因子の考え
方に変わり,ここにストレスとの関連が認知されるよう
になり今日に至っている14−18).
顎関節症の研究は,最初の文献19)以降,大きく 3種の
アプローチの仕方があった.その 1つは X 線学的に追
及するものである.当初はセファログラム,Schüller
法,パルマ法などの撮影20)によるものであった.その
後,顎関節造影法21, 22)が開発され,現在では CT23)や
MRI24)による撮影が行われるようになり,円板と顎関節
内障との関係が明らかとなってきている.
1. In terms of frequency, TMJ clicking was categorized into three types : unimodal(single-peaked),bimodal(double-
peaked)and multimodal(peaked in three or more locations).Crepitation was classified as bimodal and multimodal.
2. The majority of frequencies of both clicking and crepitation occurred between 50 Hz and 200 Hz.
3. The duration of sound was 120 ms or less with respect to clicking and 200 ms or greater in terms of crepitation.
4. The spectra of TMJ sound differed in each occurrence, indicating that unsteady frequency is a characteristic of TMJ
sound.
5. TMJ sounds collected were a result of resonance in certain parts of the mandible and craniofacial area, which was trig-
gered by an impulse occurring in the temporomandibular joint during opening and closing.
6. Impulses in the case of clicking were believed to be due to reciprocal clicksassociated with anterior displacement.In the
case of crepitation, impulses were thought to be attributable to osteoarthrosis.
7. Clicking is caused by a single, isolated strong impulse. On the other hand, crepitation is caused by a series of minor im-
pulses. Although their symptoms differ, an impulse is instrumental in the fundamental mechanism of both types of sound.
8. TMJ sound may differ in each occurrence due to variables such as the origin of the impulse, its direction or intensity and
the manner in which generated vibrations are transmitted from the various parts of the joint. Moreover, variations in the
manner of how individual vibrations resonate with respect to one another may contribute to the non-uniformity in TMJ
sound patterns.
Key words : TMJ disorder, TMJ sounds, FFT
─────────────────────────────§別刷請求先:花輪小百合,〒350-0283埼玉県坂戸市けやき台 1-1明海大学歯学部病態診断治療学講座歯科放射線学分野(現所属)
82 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008

Stethoscope(Littman Brand, ClassicⅡS.E.Stethoscope)
Multimixer(Audio-technica,AT-PMX5P)
Line IN
LineOUT
Gain control
Data memoryWave
analysis
Digital Oscilloscope(Iwatsu,DS-5100)
Multimixer
Line IN
LineOUT
Gain control
Data memoryWave
analysis
L 1ch
R 2ch
L
R
Bone conductionmicrophone
(Sony,ECM-TL1)
Line IN
LineOUT
Gain control
Line IN
LineOUT
Gain control
Data memory
(Buffalo,USB2.0 Flash Drive)
Waveanalysis
(Dell Optiplex GX60)Flash memory P.C
次のアプローチは顎関節雑音(以後雑音と略す)をマ
イクロホンを介して採取し,波形解析によって診断しよ
うとするものである.Nanthaviroj ら25)は雑音と筋電計を
組合せて測定した結果を報告し,Rohlin ら26)は新鮮な死
体からブロックとして切り出した 55個の顎関節から雑
音の有無と顎関節の病態を検索した.雑音に関する音響
学的研究は,今日まで多数みられる27−34).
もう一つのアプローチは筋電図35−40)による解析であ
る.Tsolka と Preiskel41)は,顎関節症 51名の患者を 2つ
に分け,咬合調整,疑似咬合調整を行い比較したとこ
ろ,筋活動や顎運動所見に両者の差のないことを報告
し,顎関節症は咬合異常に原因するという病因説を否定
した.
これまでの顎関節症の研究は,様々な方法を用いて行
われているが,研究成果をまとめると,クリック音の発
生は関節円板の前方転位に起因する相反性クリックであ
り,クレピタス音は骨性アルスローシスによる音42, 43)で
あると推測されているのみである.では円板の前方転位
はなぜ起こるのか,クレピタス音を発するようになるの
はなぜかという顎関節症の真の原因を解明するまでに至
っていないのが現状である.また治療法に関してもスプ
リント療法が 1次選択肢として提唱されているものの,
その後の治療法は確立されていない.
そこで本研究は,顎関節症の病因解明を最終目標に,
その第一歩として雑音に的を絞り,これを音響学的に採
取解析し,そこから雑音の特徴を描出することによっ
て,雑音発生の機序の解明を目的とした.
マイクロホンから雑音を採取し音響学的に分析する方
法は,1952年に Ekensten27)が報告したのが最初である.
その後,電子機器の発達によって,より高感度で S/N
の良い高精度な記録系を用いて多数の研究がみられるよ
うになった.1966年,Watt32)は雑音波形の分析から,雑
音をクリック音とクレピタス音に分類しているが,両者
を明確に分けることは難しく,今日ではその複合した波
形が注目されるようになっている.
波形解析には一般的に周波数分析44)が行われている.
これまでの分析をみると,雑音の発生と開閉口運動時と
の関係や,雑音の構成周波数等は求められている.しか
し,その周波数は雑音の発生時ごとに変化したり,また
マイクロホンの設置位置によって異なって出現したりす
るなど非常に不安定な一面がある.この不安定な周波数
と雑音波形を関連付けて解析したものは,著者の知る限
りではまだ報告されていない.
本研究は,この不安定な雑音波形発生の本質の解明を
目的に実験を行った.その結果,雑音は,円板前方転位
にともなう相反性クリックであれ,骨性アルスローシス
によるクレピタスであれ,そこに発生するインパルスに
よる顎顔面頭蓋の共振音であることが証明された.そし
て雑音波形が発生時ごとに異なるのは,インパルスの発
生位置や形状,大きさなどに原因することがわかり,雑
音発生の機序を明らかにすることができた.ここにその
実験の詳細を報告する.
材料と方法
1.測定系の設計と雑音波形の解析
通常顎関節雑音の診断は,歯科医が患者の顎関節上の
皮膚面に指を置き,開閉口運動にともなう関節部に発生
する雑音による振動を触診する.そして指先の感覚や発
生音,さらに患者からの雑音の表現などを統合して,ク
リック音やクレピタス音の診断が行われている.本研究
は,この雑音を音響学的に採取記録し,定量性のある解
析を行うための測定系を設計し作製した.
実験装置のブロックダイアグラムを Fig 1に,装置を
Fig 2に示す.この装置の概要を示すと,雑音を採取す
るために聴診器 Littman Classic蠡 S E Stethoscope(3 M,
Neuss, Germany)と骨伝導マイクロホン ECM-TL 1(ソ
ニー,東京)を組み合わせた雑音採取器(聴音器 Gnatho-
soundscope,以後聴音器と呼ぶ)を作製した.聴音器に
よって電気信号に変換された雑音はマルチミキサー AT-
PMX 5 P(オーディオテクニカ,町田,東京)で増幅さ
れ,デジタルオシロスコープ DS-5100(岩崎通信機,東
京)で波形として記録観察できるようにした.オシロス
コープに記録された波形をフラッシュメモリーに記録保
存し,これをパーソナルコンピュータ Optiplex GX 60
(DELL,川崎,神奈川)につなぎ,Microsoft Office Ex-
Fig 1 Blockdiagram of apparatus for TMJ sound analysis.
顎関節雑音のフーリエスペクトル解析 83

Digital Oscilloscope
MultimixerOscilloscope and multimixer Gnathosoundscope
Bone conductionmicrophone
Stethoscope
Original soundwave
5point smoothing
R O I
F F T
Out put
Out put
Hamming window function
Speaker(FOSTEX FE133)
Gnathosoundscope
0.5m
Frequencygenerator(WAVETEKMODEL 19)
Noisemeter
(RION SA-78)
TMJ sound analyzer
Microphone
cel 2003で波形解析を行った.
雑音の採取条件としては,開閉口運動の周期を一定に
しておくことが必要である.本研究では開口から閉口ま
での 1周期を約 2秒とし,メトロノームに合わせて開閉
口運動の訓練を行い,スピードが安定した時点で雑音採
取を行なうようにした.データの採取条件としては,ク
リック音の場合サンプリングレートを 10 ms/div,クレ
ピタス音の場合 50 ms/div とした.これをサンプリング
ピッチに変換すると,それぞれ 50 µs と 117.2 µs とな
る.サンプリングの総数はいずれも 5,120点である.
波形解析は,Fig 3に示すように聴音器から採取され
たオリジナル波形に,前処理としてまず 5点スムージン
グ処理を行った.この処理波形をアウトプットして評価
波形とした.次に波形内に関心領域(以後 ROI とす
る)を設定しこれを切り出した.ROI のサンプル数
は,クリック音では 1,024点,クレピタス音では 2,048
点とした.切り出した波形についてウインドウ関数とし
てハミング関数処理を行い,次いで Fast Fourier Trans-
form(以後 FFT とする)を行った.フーリエスペクト
ル(以後スペクトルと略す)は FFT の絶対値で表示し
た.スペクトルは既存の FFT ソフトを用いて解析した.
2.測定系の音響学的特性
1)入出力特性
顎関節内で発生した雑音を,皮膚面上から聴音器を介
して採取する場合に,聴音器を含めた測定系に入力され
る音の強さ,すなわち音圧レベルと出力される信号強度
の音響学的特性を測定した.
測定は Figs 4, 5に示すように,周波数ジェネレータ
ー MODEL 19(WAVETEK, San Diego, CA, USA)から
発せられる正弦波波形をスピーカ FE 133(FOSTEX,
昭島,東京)を通して音に変換した.このスピーカから
Fig 2 Apparatus for TMJ sound recording.
Fig 3 Flow chart of TMJ sound analysis.
Fig 4 Block diagram for frequency characteristic measurement.
84 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008

Experimental arrangement Gnathosoundscope and microphone of noise meter
0.5 m 離れた位置に音圧レベルを測定する騒音計 2 ch
FFT ANALYZER(リオン,東京)のマイクロホンと聴
音器を配置した.測定は種々の音圧レベルと出力信号の
関係を計測した.測定には 300 Hz の周波数を使用した.
2)周波数特性
実験は測定系の周波数特性について測定した.方法は
前実験 2-1)と同じ,実験配置を使用した.
測定は以前の報告45)にあるように 50 Hz から 1,000 Hz
まで,種々の周波数の一定音圧レベルに対する出力特性
について測定した.測定時の周波数間隔は 100 Hz と
し,音圧レベルは 55 dB と一定にした.
3.左右聴音器による雑音波形の採取と解析
被験者から雑音の採取にあたっては,以前の報告44, 45)
にみられるように,聴音器を左右顎関節上の皮膚面に置
き雑音を採取するようにした.聴音器の固定は,被験者
が自身の指で聴音器を押さえるようにした(Fig 6).
雑音は左右側同時系列に記録しその波形とスペクトル
解析を行った.雑音解析はクリック音とクレピタス音の
2種について検討した.
以後,被験者を用いた実験に関しては,各被験者に対
し実験の旨を説明し,インフォームドコンセントを行い
承諾を得た.
4.雑音波形の再現性
1)聴音器の位置と雑音波形の変化
実験は,聴音器をあてる皮膚面上の位置の違いが雑音
波形の変化におよぼす影響について検討した.
聴音器の位置付けは Fig 7に示すように A~D の 4位
置とした.A は聴音器の中央が顎関節部の真上の位
置,B は聴音器の後縁が顎関節部にあたる前方位置,C
は聴音器の下縁が顎関節部にあたる上方位置,D は聴
音器の上縁が顎関節部にあたる下方位置とした.
雑音はクリック音とした.雑音波形の採取にあたって
は,4位置とも同じ雑音の発生状態で採取するため,反
対側の顎関節上においた聴音器で雑音波形をモニタリン
グした.モニタリングによるクリック音波形が,同じ波
形を呈したときの発生側の波形を採取記録した.同じ波
形である条件は,モニタ上で波形の振幅,形状そしてス
ペクトルによる解析が同じ状態を呈した場合の波形をい
い,そのような波形を呈したときの雑音波形を採取し試
料とした.
2)雑音波形の経日的変化
顎関節症の治療は,長期間にわたり,患者によっては
Fig 6 Holding of gnathosoundscope.
Fig 5 Apparatus for frequency characteristic.
顎関節雑音のフーリエスペクトル解析 85

数年の治療期間を要することがある.従ってこの期間の
雑音波形の変化を記録することが必要となる.
雑音波形の記録では,雑音の強度や波形形状の変化等
が,顎関節症の回復の指標になると考えられる.そこ
で,長期間にわたり雑音を安定的に採取記録するには,
聴音器の固定ならびに音響系や電気系の記録条件がいつ
も一定していることが求められる.
本実験は同一被験者について,同じ採取条件で経日的
に記録し,同じ雑音波形が採取出来るかどうかを検討し
た.実験は,前実験 4-1)の被験者について最初の検査
日と 1週間の間隔をおいて採取した 2回の波形について
比較検討した.聴音器の固定位置は,顎関節上の中央部
とし,ミキシングのレベルは 3とし一定にした.また雑
音採取に際し,反対側の聴音器から採取された雑音波形
をモニタリングし,モニタ波形が初回時と同一波形の得
られた場合の波形を記録し試料とした.雑音波形はクリ
ック音とした.
5.クリック音波形の特徴抽出
1)クリック音波形の振幅が変化する場合の特徴
クリック音波形を採取すると,採取時に雑音の大きい
場合,すなわち振幅強度の大きいときと,比較的小さな
音でしか発生しないときがある.このときクリック音波
形はどのような形状を呈するのか,またそのスペクトル
はどのような変化を示すのかをあらかじめ検討しておく
必要がある.
本実験は,クリック音波形で振幅強度が変化する被験
者について検討した.
クリック音波形の採取にあたっては,実験 2-1)で求
めた入出力特性において,線型性の成立する範囲内で 3
段階の振幅強度を設定し,それぞれの波形形状ならびに
スペクトルを比較した.
2)クリック音波形の形状が変化する場合の特徴
クリック音波形の採取時には,実験 5-1)のような強
度変化だけでなく,雑音に音の変化,すなわち波形形状
に変化が見られることがある.
本実験は開閉口運動を行ううちに波形形状に変化の見
られた一被験者について,1回目から 10回目の 10波形
を記録し,その形状の変化ならびにスペクトルの変化に
ついて検討した.各開閉口運動の間隔は 1分とした.
3)クリック音を複数回発生する場合の波形の特徴
クリック音は,開口時に一回発生すると閉口時には多
少位置は異なるが,ほぼ同位置で一回発生する場合が一
般的である.しかし開口時か閉口時にしか発生しない場
合や,開閉口時に複数回発生するものも観察される.
そこで本実験は,開口時にクリック音を 2回発生する
被験者について,波形とスペクトルを求め検討した.
6.クレピタス音波形の特徴抽出
1)クレピタス音波形の振幅が変化する場合の特徴
クレピタス音もクリック音と同様に,発生時に振幅強
度が大きかったり比較的小さな音で発生したりすること
が確認された.そこでクリック音の場合と同じ様に,同
一被験者でクレピタス音波形の振幅強度の異なる 3波形
を採取し,波形形状ならびにスペクトルについて検討し
た.
2)クレピタス音波形の形状が変化する場合の特徴
クレピタス音の発生時ごとに得られる波形を解析し
た.実験はクレピタス音を有する一被験者についてクリ
ック音波形採取の場合と同じように,波形形状の異なる
3種のクレピタス音波形を採取した.これらのクレピタ
ス音波形の形状ならびにスペクトルについて検討した.
7.クリック音の分類
クリック音を有する被験者 15名について,クリック
音を採取し,その波形形状,スペクトルならびにクリッ
ク音の持続時間について検討した.またクリック音の分
類を行った.
8.クレピタス音の分類
クレピタス音を有する被験者 13名について,クレピ
タス音を採取し,その波形形状,スペクトルならびに持
Fig 7 Various holding positions of gnathosoundscope.
86 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008

-2
-1
0
1
2
0 50 100 150 200 250
Voltage [V]
Time [ms]
-2
-1
0
1
2
0 50 100 150 200 250
Voltage [V]
Time [ms]
Left side Right side
0.01
0.1
1
50 60 70 80 90
Input [dB]
Out put [V]
0
0.1
0.2
0.3
0.4
0.5
0 200 400 600 800 1000 1200
Frequency [Hz]
Voltage [V]
続時間を求め,それらの特徴からクレピタス音の分類を
行った.
結 果
1.測定系の設計と雑音波形の解析
Fig 8に左右聴音器から採取した一被験者のクリック
音波形を示す.図は,歯科医が顎関節上の皮膚面におけ
る触診で,かすかなクリック音を感知できる程度の音
を,左右の聴音器から採取したものを波形として表示し
たものである.
本装置では触診で感知できるクリック音は確実にこれ
をオシロスコープ上で波形として表示することができ
た.しかし,被験者ではクリック音を自覚するが,外部
からの触診で感知できないものは,この聴音器において
も採取することはできなかった.
2.測定系の音響学的特性
1)入出力特性
300 Hz の一定周波数における,種々の音圧レベルの
入力に対する出力信号強度の関係を Fig 9に示す.本実
験で作製した測定系の入出力特性は,58 dB から 84 dB
の間で線型性を示していた.
2)測定系の周波数特性
Fig 10に測定系の周波数特性を示す.出力特性をみる
と測定範囲の 50 Hz から 1000 Hz 間では 0.1 V~0.2 V 内
に位置し,ほぼ一定の値を示していた.
3.左右聴音器による雑音波形の採取と解析
1)クリック音の採取
Fig 11にクリック音を左右の聴音器から同時に採取し
た波形とスペクトルを示す.被験者は左側顎関節にクリ
ック音を発生する.
左右の波形を比較すると,クリック音を有する左側で
は,振幅強度が右側より大きく記録されていた.
左右のスペクトルを比較すると,左側のクリック音波
形のスペクトルに比べて,右側のスペクトルは多少大き
な裾広がりを示すものの,メインの周波数は 100 Hz 前
後で同一であった.このことは,この被験者の左右聴音
Fig 8 Clicking sound waves by right and left gnathosoundscope.
Fig 10 Frequency characteristic.
Fig 9 Characteristic of input output relation.
顎関節雑音のフーリエスペクトル解析 87

-3
-2
-1
0
1
2
3
0 50 100 150 200 250
Time [ms]
Voltage [V]
Left side
0
0.2
0.4
0.6
0.8
1
0 500 1000
Frequency [Hz]
Relative intensity
-3
-2
-1
0
1
2
3
Voltage [V]
0
0.2
0.4
0.6
0.8
1
Relative intensity
Left side
50 100 150 200 250
Time [ms]
Right side
0 500 1000
Frequency [Hz]
Right side
Normal sideDisorder side
-2
-1
0
1
2
0 100 200 300 400 500 600 0 100 200 300 400 500 600
Time [ms]
Voltage [V]
Left side
0
0.2
0.4
0.6
0.8
1
0 500 1000
Frequency [Hz]
Relative intensity
-2
-1
0
1
2
Voltage [V]
0
0.2
0.4
0.6
0.8
1
Relative intensity
Left side
Time [ms]
Right side
0 500 1000
Frequency [Hz]
Right side
Normal sideDisorder side
Fig 11 Clicking sound waves and spectra from right and left gnathosoundscope.
Fig 12 Crepitation sound waves and spectra from right and left gnathosoundscope.
88 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008
-1.5
-1
0
0.5
1.5
1
-0.5
0 50 100 150 200 250 0 50 100 150 200 250
Time [ms]
Voltage [V]
-1.5
-1
0
0.5
1.5
1
-0.5
Voltage [V]
Time [ms]
-1.5
-1
0
0.5
1.5
1
-0.5
0 50 100 150 200 250 0 50 100 150 200 250
Time [ms]
Voltage [V]
-1.5
-1
0
0.5
1.5
1
-0.5
Voltage [V]
Time [ms]
A position B position
C position D position
器から採取されたクリック音波形は,左右側で全く同一
の振動波形であると判断することができた.しかし別の
被験者では左右全く異なる振動波形を呈する場合もあっ
た.
クリック音の持続時間については,左右側で近似し 60
ms であった.
2)クレピタス音の採取
Fig 12に左右聴音器から同時に採取されたクレピタス
音波形とスペクトルの比較を示す.被験者は左側顎関節
にクレピタス音を発生する.両側の波形を比較すると,
左側波形の振幅が右側より大きく記録されている.両波
形はクリック音の場合と異なり,全く形状を異にするこ
とがわかった.
スペクトルでは左側聴音器からの波形は 50 Hz 前後の
単峰性であるのに対し,右側のスペクトルは 50 Hz と
100 Hz 前後の 2峰性を呈し,明らかにスペクトルでも
両波形に差がみられた.クレピタス音の持続時間は左右
側で近似し 200 ms であった.
4.雑音波形の再現性
1)聴音器の位置と雑音波形の変化
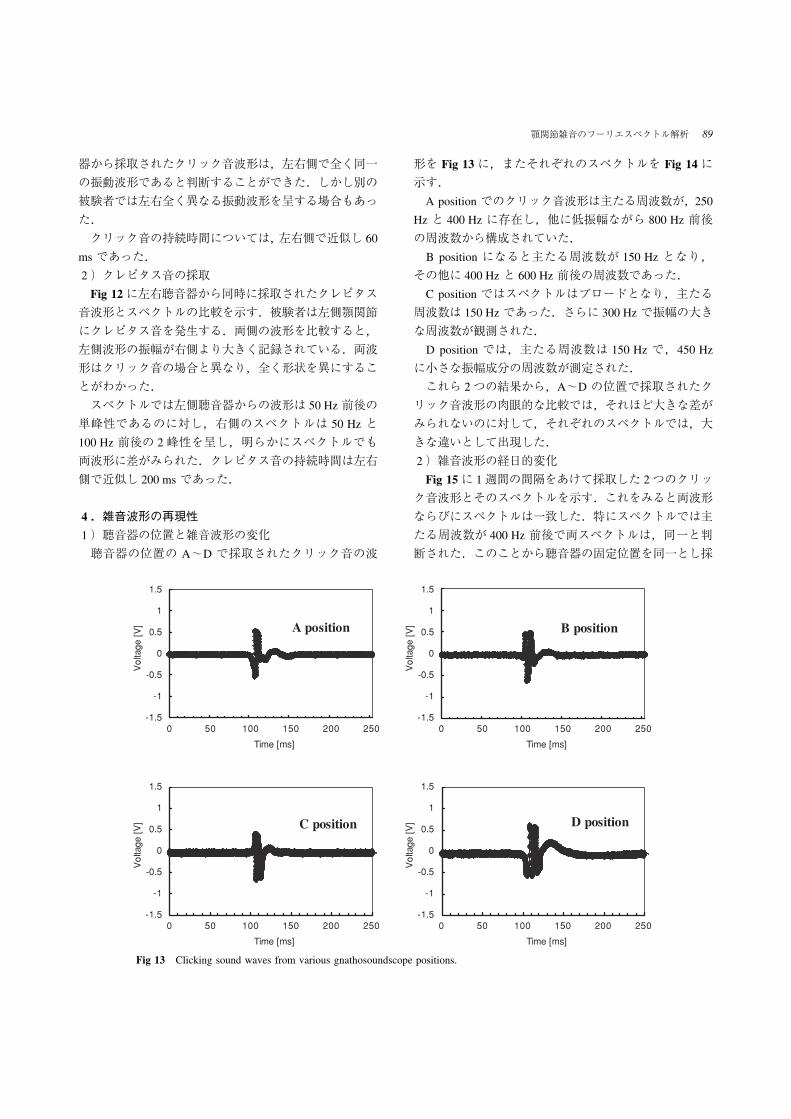
聴音器の位置の A~D で採取されたクリック音の波
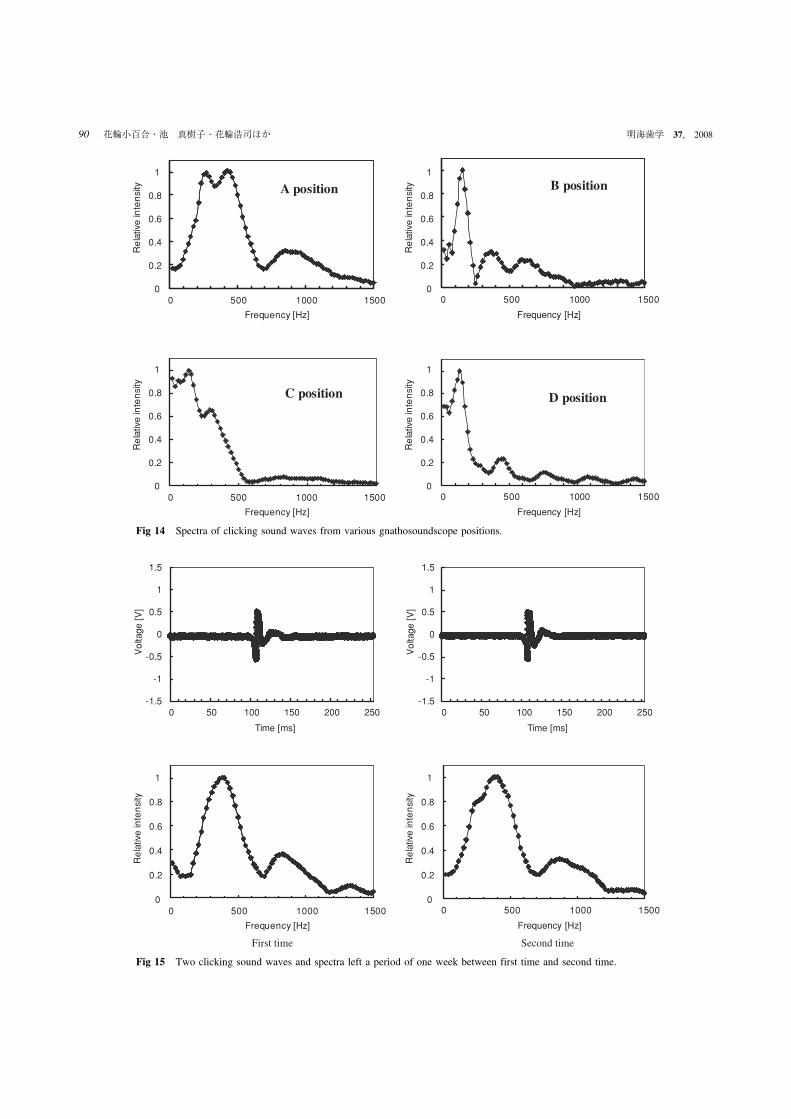
形を Fig 13に,またそれぞれのスペクトルを Fig 14に
示す.
A position でのクリック音波形は主たる周波数が,250
Hz と 400 Hz に存在し,他に低振幅ながら 800 Hz 前後
の周波数から構成されていた.
B position になると主たる周波数が 150 Hz となり,
その他に 400 Hz と 600 Hz 前後の周波数であった.
C position ではスペクトルはブロードとなり,主たる
周波数は 150 Hz であった.さらに 300 Hz で振幅の大き
な周波数が観測された.
D position では,主たる周波数は 150 Hz で,450 Hz
に小さな振幅成分の周波数が測定された.
これら 2つの結果から,A~D の位置で採取されたク
リック音波形の肉眼的な比較では,それほど大きな差が
みられないのに対して,それぞれのスペクトルでは,大
きな違いとして出現した.
2)雑音波形の経日的変化
Fig 15に 1週間の間隔をあけて採取した 2つのクリッ
ク音波形とそのスペクトルを示す.これをみると両波形
ならびにスペクトルは一致した.特にスペクトルでは主
たる周波数が 400 Hz 前後で両スペクトルは,同一と判
断された.このことから聴音器の固定位置を同一とし採
Fig 13 Clicking sound waves from various gnathosoundscope positions.
顎関節雑音のフーリエスペクトル解析 89
0
0.2
0.4
0.6
0.8
1
0 500 15001000
Frequency [Hz]
Relative intensity
0
0.2
0.4
0.6
0.8
1
Relative intensity
0 500 15001000
Frequency [Hz]
0
0.2
0.4
0.6
0.8
1
0 500 15001000
Frequency [Hz]
Relative intensity
0
0.2
0.4
0.6
0.8
1
Relative intensity
0 500 15001000
Frequency [Hz]
A position B position
C position D position
-1.5
-1
-0.5
0
1
0.5
1.5
0 10050 150 200 250-1.5
-1
-0.5
0
1
0.5
1.5
0 10050 150 200 250
Time [ms]
Voltage [V]
0
0.2
0.4
0.6
0.8
1
Frequency [Hz]
Relative intensity
Voltage [V]
0
0.2
0.4
0.6
0.8
1
Relative intensity
Time [ms]
0 500 15001000 0 500 15001000
Frequency [Hz]
Second timeFirst time
Fig 14 Spectra of clicking sound waves from various gnathosoundscope positions.
Fig 15 Two clicking sound waves and spectra left a period of one week between first time and second time.
90 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008

-2
-1
0
1
2
0 50 100 150 200 250
Time [ms]
Voltage [V]
Maximum amplitude
+1.12V
-1.82V
-2
-1
0
1
2
0 50 100 150 200 250
Time [ms]
Voltage [V]
Medium amplitude
+0.97V
-1.25V
-2
-1
0
1
2
0 50 100 150 200 250
Time [ms]
Voltage [V]
Minimum amplitude
-0.76
+0.53V
0 500 1000 1500
Frequency [Hz]
Relative intensity
Maximum amplitude
0
0.2
0.4
0.6
0.8
1
0 500 1000 1500
Frequency [Hz]
Relative intensity
Medium amplitude
0
0.2
0.4
0.6
0.8
1
0 500 1000 1500
Frequency [Hz]
Relative intensity
Minimum amplitude
0
0.2
0.4
0.6
0.8
1
-2
-1
0
2
1
0 50 100 150 200 250 0 50 100 150 200 250
Time [ms]
Voltage [V]
-2
-1
0
2
1
Voltage [V]
Time [ms]
-2
-1
0
2
1
0 50 100 150 200 250 0 50 100 150 200 250
Time [ms]
Voltage [V]
-2
-1
0
2
1
Voltage [V]
Time [ms]
6th ~10th time4th, 5th time
3rd time1st, 2nd time
取条件を同じとすれば,かなりの精度で同じ形状が採取
されることが確認された.
5.クリック音波形の特徴抽出
1)クリック音波形の振幅が変化する場合の特徴
クリック音の発生時ごとに,波形の振幅変化を呈する
Fig 16 Different amplitude waves of clicking sound and spectra from the same parson.
Fig 17 Change of clicking sound wave during opening and closing movement.
顎関節雑音のフーリエスペクトル解析 91
0
0.2
0.4
0.6
0.8
1
0 500 1000
Frequency [Hz]
Relative intensity
0
0.2
0.4
0.6
0.8
1
Relative intensity
0 500 1000
Frequency [Hz]
0
0.2
0.4
0.6
0.8
1
0 500 1000
Frequency [Hz]
Relative intensity
0
0.2
0.4
0.6
0.8
1
Relative intensity
0 500 1000
Frequency [Hz]
6th ~10th time4th, 5th time
3rd time1st, 2nd time
被験者について,3つの振幅強度の異なるクリック音波
形を採取し,その波形とスペクトルを Fig 16に示す.
原波形について比較すると振幅強度に変化はみられる
が,波形全体は同じような形状を呈していた.最も振幅
の大きい+1.12 V~-1.82 V を呈する波形のスペクトル
ではメインの周波数が 100 Hz と 500 Hz の 2峰性を呈し
ていた.中等度の振幅である+0.97 V~-1.25 V の波形
でも全く同じ周波数で 2峰性のスペクトルを呈し,この
2つの波形の差異はないものと判断された.さらに振幅
が小さく+0.53 V~-0.76 V になると,2峰性の周波数
成分のうち高周波数の 500 Hz の周波数の振幅が相対的
に小さくなり,さらに 400 Hz の周波数成分の出現がみ
られた.
つまり,3つのクリック音波形のうち,ある程度の振
幅強度を有する場合は同一の波形と考えることができる
が,振幅の小さい場合は別の波形と判断しなければなら
ないことがわかった.
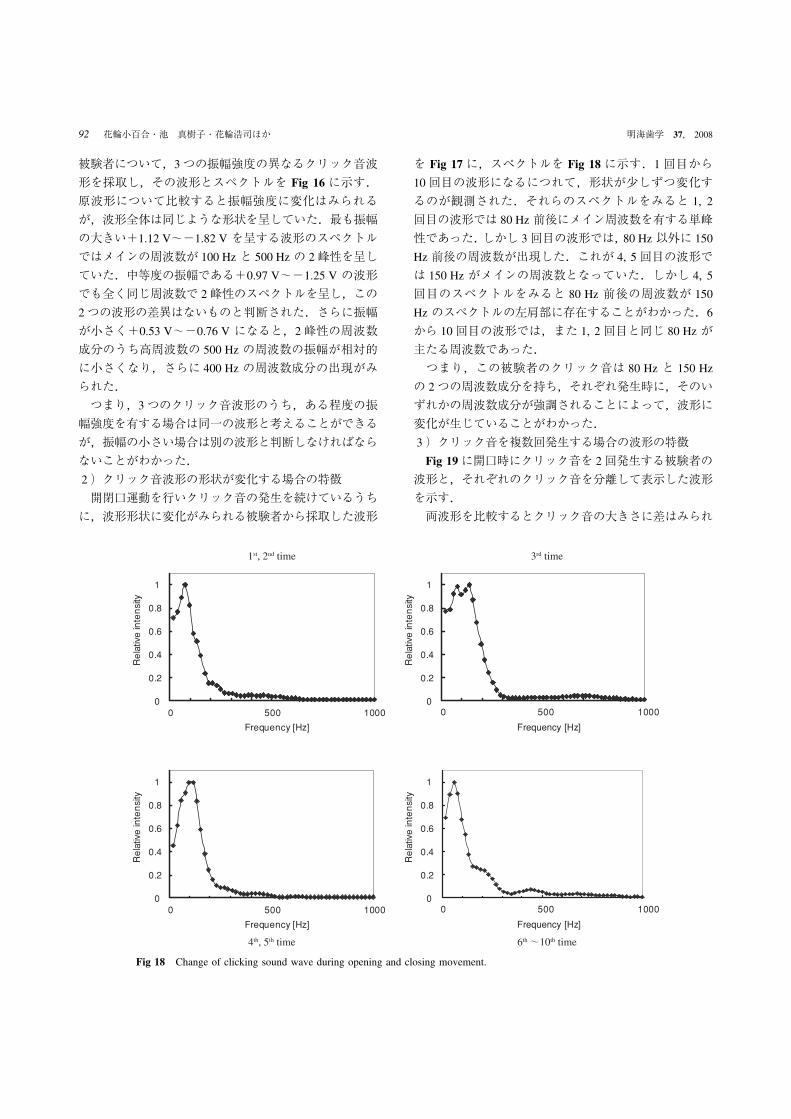
2)クリック音波形の形状が変化する場合の特徴
開閉口運動を行いクリック音の発生を続けているうち
に,波形形状に変化がみられる被験者から採取した波形
を Fig 17に,スペクトルを Fig 18に示す.1回目から
10回目の波形になるにつれて,形状が少しずつ変化す
るのが観測された.それらのスペクトルをみると 1, 2
回目の波形では 80 Hz 前後にメイン周波数を有する単峰
性であった.しかし 3回目の波形では,80 Hz 以外に 150
Hz 前後の周波数が出現した.これが 4, 5回目の波形で
は 150 Hz がメインの周波数となっていた.しかし 4, 5
回目のスペクトルをみると 80 Hz 前後の周波数が 150
Hz のスペクトルの左肩部に存在することがわかった.6
から 10回目の波形では,また 1, 2回目と同じ 80 Hz が
主たる周波数であった.
つまり,この被験者のクリック音は 80 Hz と 150 Hz
の 2つの周波数成分を持ち,それぞれ発生時に,そのい
ずれかの周波数成分が強調されることによって,波形に
変化が生じていることがわかった.
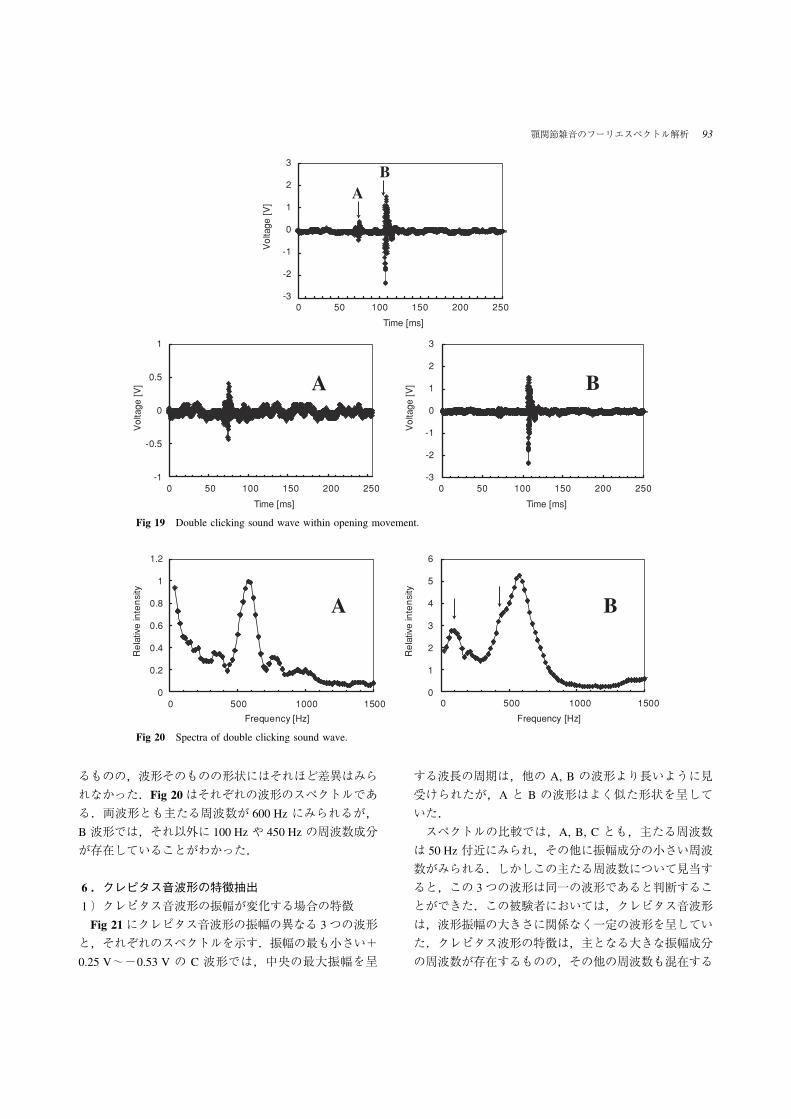
3)クリック音を複数回発生する場合の波形の特徴
Fig 19に開口時にクリック音を 2回発生する被験者の
波形と,それぞれのクリック音を分離して表示した波形
を示す.
両波形を比較するとクリック音の大きさに差はみられ
Fig 18 Change of clicking sound wave during opening and closing movement.
92 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008
-3
-1
0
3
1
0 50 100 150 200 250
Time [ms]
Voltage [V]
-1
-0.5
0
1
0 50 100 150 200 250 0 50 100 150 200 250
Time [ms]
Voltage [V]
-3
-2
-2
-1
0
3
2
0.52
1
Voltage [V]
Time [ms]
A B
AB
0
0.2
0.4
0.6
0.8
1
1.2
Frequency [Hz]
Relative intensity
0
2
1
3
4
5
6
Relative intensity
0 500 15001000 0 500 15001000
Frequency [Hz]
A B
るものの,波形そのものの形状にはそれほど差異はみら
れなかった.Fig 20はそれぞれの波形のスペクトルであ
る.両波形とも主たる周波数が 600 Hz にみられるが,
B 波形では,それ以外に 100 Hz や 450 Hz の周波数成分
が存在していることがわかった.
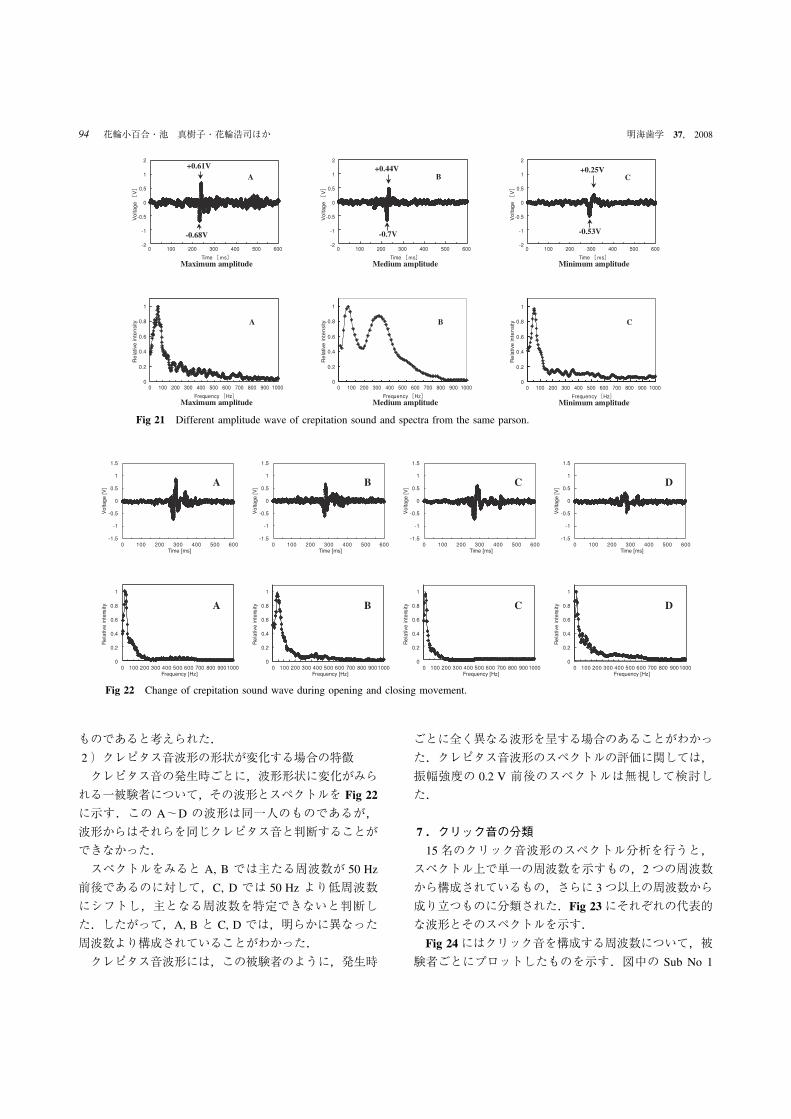
6.クレピタス音波形の特徴抽出
1)クレピタス音波形の振幅が変化する場合の特徴
Fig 21にクレピタス音波形の振幅の異なる 3つの波形
と,それぞれのスペクトルを示す.振幅の最も小さい+
0.25 V~-0.53 V の C 波形では,中央の最大振幅を呈
する波長の周期は,他の A, B の波形より長いように見
受けられたが,A と B の波形はよく似た形状を呈して
いた.
スペクトルの比較では,A, B, C とも,主たる周波数
は 50 Hz 付近にみられ,その他に振幅成分の小さい周波
数がみられる.しかしこの主たる周波数について見当す
ると,この 3つの波形は同一の波形であると判断するこ
とができた.この被験者においては,クレピタス音波形
は,波形振幅の大きさに関係なく一定の波形を呈してい
た.クレピタス波形の特徴は,主となる大きな振幅成分
の周波数が存在するものの,その他の周波数も混在する
Fig 19 Double clicking sound wave within opening movement.
Fig 20 Spectra of double clicking sound wave.
顎関節雑音のフーリエスペクトル解析 93
-2
-0.5
-1
0
1
2
0.5
0 100 200 300 400 500 600
Time [ms]
Voltage [V]
Maximum amplitude
+0.61V
-0.68V
A
-2
-0.5
-1
0
1
2
0.5
0 100 200 300 400 500 600
Time [ms]
Voltage [V]
Medium amplitude
+0.44V
-0.7V
B
-2
-0.5
-1
0
1
2
0.5
0 100 200 300 400 500 600
Time [ms]
Voltage [V]
Minimum amplitude
+0.25V
-0.53V
C
0 100 200 300 400 500 600 700 800 900 1000
Frequency [Hz]
Relative intensity
Maximum amplitude
0
0.2
0.4
0.6
0.8
1
A
0 100 200 300 400 500 600 700 800 900 1000
Frequency [Hz]
Relative intensity
Medium amplitude
0
0.2
0.4
0.6
0.8
1
B
0 100 200 300 400 500 600 700 800 900 1000
Frequency [Hz]
Relative intensity
Minimum amplitude
0
0.2
0.4
0.6
0.8
1
C
-1.5
-1
-0.5
0
0.5
1
1.5
0 100 200 300 400 500 600Time [ms]
Voltage [V]
A
-1.5
-1
-0.5
0
0.5
1
1.5
0 100 200 300 400 500 600Time [ms]
Voltage [V]
B
-1.5
-1
-0.5
0
0.5
1
1.5
0 100 200 300 400 500 600Time [ms]
Voltage [V]
C
-1.5
-1
-0.5
0
0.5
1
1.5
0 100 200 300 400 500 600Time [ms]
Voltage [V]
D
0
0.2
0.4
0.6
0.8
1
0 100 200 300 400 500 600 700 800 9001000Frequency [Hz]
Relative intensity A
0
0.2
0.4
0.6
0.8
1
0 100 200 300 400 500 600 700 800 9001000Frequency [Hz]
Relative intensity B
0
0.2
0.4
0.6
0.8
1
0 100 200 300 400 500 600 700 800 9001000Frequency [Hz]
Relative intensity C
0
0.2
0.4
0.6
0.8
1
0 100 200 300 400 500 600 700 800 9001000Frequency [Hz]
Relative intensity D
ものであると考えられた.
2)クレピタス音波形の形状が変化する場合の特徴
クレピタス音の発生時ごとに,波形形状に変化がみら
れる一被験者について,その波形とスペクトルを Fig 22
に示す.この A~D の波形は同一人のものであるが,
波形からはそれらを同じクレピタス音と判断することが
できなかった.
スペクトルをみると A, B では主たる周波数が 50 Hz
前後であるのに対して,C, D では 50 Hz より低周波数
にシフトし,主となる周波数を特定できないと判断し
た.したがって,A, B と C, D では,明らかに異なった
周波数より構成されていることがわかった.
クレピタス音波形には,この被験者のように,発生時
ごとに全く異なる波形を呈する場合のあることがわかっ
た.クレピタス音波形のスペクトルの評価に関しては,
振幅強度の 0.2 V 前後のスペクトルは無視して検討し
た.
7.クリック音の分類
15名のクリック音波形のスペクトル分析を行うと,
スペクトル上で単一の周波数を示すもの,2つの周波数
から構成されているもの,さらに 3つ以上の周波数から
成り立つものに分類された.Fig 23にそれぞれの代表的
な波形とそのスペクトルを示す.
Fig 24にはクリック音を構成する周波数について,被
験者ごとにプロットしたものを示す.図中の Sub No 1
Fig 21 Different amplitude wave of crepitation sound and spectra from the same parson.
Fig 22 Change of crepitation sound wave during opening and closing movement.
94 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008

-2
-1
0
1
2
0 50 100 150 200 250
Time [ms]
Voltage [V]
A
-2
-1
0
1
2
0 50 100 150 200 250
Time [ms]
Voltage [V]
B
-2
-1
0
1
2
0 50 100 150 200 250
Time [ms]
Voltage [V]
C
0 100 200 300 400 500 600 700 800 900 1000
Frequency [Hz]
Relative intensity
0
0.2
0.4
0.6
0.8
1
A
0 500 1000 1500 2000 2500 3000
Frequency [Hz]
Relative intensity
0
0.2
0.4
0.6
0.8
1
B
0 500 1000 1500 2000 2500 3000
Frequency [Hz]
Relative intensity
0
0.2
0.4
0.6
0.8
1
C
0
100
200
300
400
500
600
700
800
900
1000
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Sub. No
Frequency [Hz]
Single-peakgroup
Two-peakgroup
Multi-peak group
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Sub. No
Time [ms]
0
20
40
60
80
100
120
~8は単峰性,No 9~14は 2峰性,No 15は 1例であっ
たが多峰性を示す.
クリック音に関して周波数分析上の一般的な特徴は,
主たる第 1周波数が 50~200 Hz 前後にみられること,
第 2周波数が 400~600 Hz にみられることであった.た
だこれらの周波数を逸脱して第 1周波数が 400 Hz や,
第 3周波数が 900 Hz などを呈するものも一部にみられ
た.
クリック音の持続時間をみると,Fig 25 に示すよう
に,すべて 120 ms 以内であった.
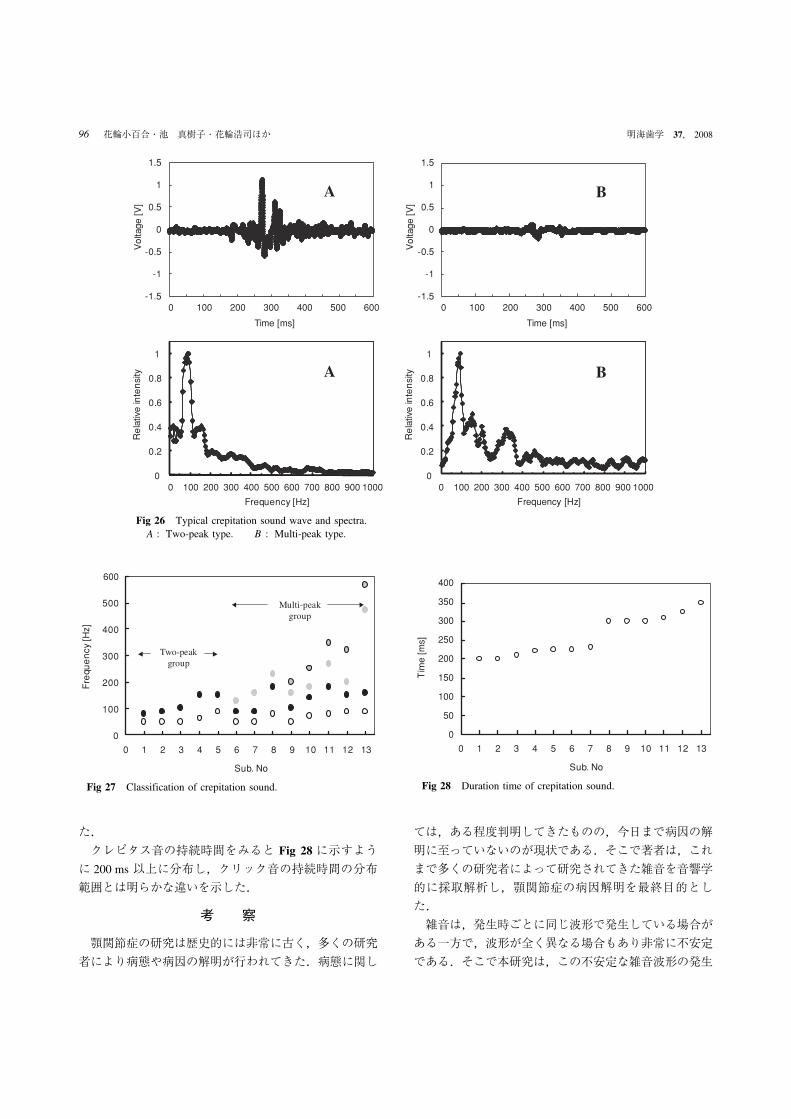
8.クレピタス音の分類
13例のクレピタス音を分類した結果,クレピタス音
ではクリック音のような単峰性を呈するものはみられ
ず,2峰性と多峰性に分類された.
Fig 26に 13名クレピタス音を発する被験者のうち,
代表的な 2峰性と多峰性の波形,そしてそれぞれのスペ
クトルを示す.
クレピタス音の分類では 2峰性と多峰性の差はクリッ
ク音ほど,大きな違いは見られなかった.どちらかとい
えば主たる周波数を単一とする波形,すなわち第 2周波
数のピークが小さく,単一周波数と考えられるようなス
ペクトルであった.また Fig 27には 13名の被験者の主
たる周波数をまとめたものを示す.クレピタス音の周波
数の特徴は,主の第 1周波数は 50 Hz~200 Hz の間に分
布し,第 2周波数は 100~400 Hz の間に分布する結果で
あった.しかし,一部に 500~600 Hz の高周波数もみら
れた.これらの周波数帯はクリック音と全く同一であっ
Fig 24 Classfication of clicking sound. Fig 25 Duration time of clicking sound.
Fig 23 Typical clicking sound waves and spectra.A : Single-peak type. B : Two-peak type. C : Multi-peak type.
顎関節雑音のフーリエスペクトル解析 95
-1.5
-1
-0.5
0
1
0.5
1.5
0 200100 300 400 600500-1.5
-1
-0.5
0
1
0.5
1.5
0 200100 300 400 600500
Time [ms]
Voltage [V]
0
0.2
0.4
0.6
0.8
1
Frequency [Hz]
Relative intensity
Voltage [V]
0
0.2
0.4
0.6
0.8
1
Relative intensity
Time [ms]
0 1000900800700600500400300200100 0 1000900800700600500400300200100
Frequency [Hz]
A B
A B
0
100
200
300
400
500
600
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Sub. No
Frequency [Hz]
Two-peakgroup
Multi-peakgroup
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Sub. No
Time [ms]
0
400
350
300
250
200
150
100
50
た.
クレピタス音の持続時間をみると Fig 28に示すよう
に 200 ms 以上に分布し,クリック音の持続時間の分布
範囲とは明らかな違いを示した.
考 察
顎関節症の研究は歴史的には非常に古く,多くの研究
者により病態や病因の解明が行われてきた.病態に関し
ては,ある程度判明してきたものの,今日まで病因の解
明に至っていないのが現状である.そこで著者は,これ
まで多くの研究者によって研究されてきた雑音を音響学
的に採取解析し,顎関節症の病因解明を最終目的とし
た.
雑音は,発生時ごとに同じ波形で発生している場合が
ある一方で,波形が全く異なる場合もあり非常に不安定
である.そこで本研究は,この不安定な雑音波形の発生
Fig 26 Typical crepitation sound wave and spectra.A : Two-peak type. B : Multi-peak type.
Fig 27 Classification of crepitation sound. Fig 28 Duration time of crepitation sound.
96 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008
原因を解明することをねらいとした.
雑音採取の音響学的装置の作製では,これまで多くの
研究者はコンデンサータイプのマイクロホン26, 46)を使用
したり,加速度計47, 48)を用いていた.今回著者は,骨伝
導マイクロホンを使用した.このマイクロホンは空気に
よる伝搬音だけでなく,骨伝導による音も採取できる特
性を有しているため,より情報量の多い雑音が採取でき
ると考えた.これを聴診器と組み合わせて雑音採取器を
作製した.
実験結果から,測定系の入出力特性ならびに周波数特
性では,雑音測定上障害となるような問題点はなかっ
た.特に周波数特性に関しては,聴診器と組み合わせた
ことから,特性の変化が危惧されたが,測定結果では 100
Hz から 1,000 Hz まで雑音測定の周波数帯域において一
定の特性を有することがわかり,聴診器の影響はなかっ
たと考えられた.
測定系による雑音採取の感度に関しては,外部からの
触診でクリック音を感知できるものはすべて波形として
描出することはできたが,触診できず被験者のみが自覚
するような,かすかなクリック音は描出することができ
なかった.そこでできるだけ感度を上げる実験を行った
ため,採取された波形データにノイズを含む結果となっ
た.ノイズの少ない波形描出については,今後研究して
いく必要がある.
クリック音やクレピタス音の採取時に,発生側だけで
なく反対側の聴音器から同時に両者の音が採取されるこ
とが確認された.そしてその波形の振幅は必ずしも発生
側が大きいとは限らず,反対側で大きく採取されること
があった.
両側から採取された波形を詳細に観察すると,波形の
立ち上がりで位相が π だけずれていること,波形は減衰振動を呈していることが確認された.この結果から,
雑音は顎顔面頭蓋部で共振音として振動していると推察
された.
雑音は左右いずれかで発生しているので,これを左右
聴音器の波形から,発生側を特定しようとしたが両者の
分離は困難であった.実験は雑音発生部位の特定を目的
に含めていないため,雑音波形は発生側のみから採取す
ることとした.反対側から得られる雑音波形は,同じ雑
音が発生しているのか否かを判定するためのモニタとし
て使用するにとどめた.また,スペクトル上で波形を構
成する周波数成分として計測する周波数は,主たる周波
数(以後第 1周波数と呼ぶ)の振幅成分に対し 0.2 V 以
上の大きさのピークを有する振幅成分(以後第 2,第 3
周波数と呼ぶ)とした.その理由は 0.2 V 以下ではノイ
ズ成分の混入があるからである.
聴音器の位置付けと得られた雑音波形の変化に関して
行った実験をみると,位置のわずかな変化でスペクトル
が大きく異なることが判明した.これは聴音器の位置が
変わることによって,顎顔面頭蓋内の共振部位との位置
関係や,音の伝搬に差が生じ,雑音波形が変化したこと
によるものと推測された.雑音が発生しながら伝搬し,
その経路の影響を受け聴音器で採取されることから得ら
れた雑音波形の変化と経路の共振部位を特定する必要が
あるか,今後の課題とした.
雑音波形の振幅が変化する場合や,波形の形状が発生
時ごとに変化する実験から推測されることは,クリック
音の発生には,共振音を惹起させるインパルスが引き金
として存在するということである.雑音の発生は,顎顔
面頭蓋内に入ったインパルスがその大きさ,形状,そし
て方向によってある部位が共振し,その部位固有の振動
数で発振している音であり,それを外部から雑音と認識
しているということが判明した.したがって,クリック
音の場合は,相反性クリックによってインパルスと呼ば
れる衝撃波が引き起こされる.次にこのインパルスによ
りある部位が共振し,その部位特有の固有振動が惹起さ
れ,これがクリック音として外部から採取されることが
判明した.この共振部位が同じ位置である場合は,クリ
ック音を 2回発生する被験者からのデータが,両方とも
600 Hz で同一であることから確認することができた.
この被験者より得られた 100 Hz と 450 Hz の周波数は,
B 波形の振幅が A 波形より約 5倍程度大きいことによ
って,種々の部位の共振を惹起し,これが混入したもの
と思われる.基本的にはこの被験者の 2回のクリック音
の主たる周波数は,ともに変わらず 600 Hz 前後にある
ものと判断した.したがって,クリック音を複数回発生
する被験者でも主となる周波数は 1つであると考えられ
たからである.
しかし発生時ごとに波形が異なる場合は,同一測定部
位であっても共振の程度に違いが生じたり,異なる部位
の共振が混入したりするためと考えられる.
クリック音の分類では,スペクトルからみると単峰
性,2峰性さらに多峰性に分類することができた.この
内主たる第 1周波数は,50~200 Hz 前後に存在し,ほ
ぼ 1 kHz 以内にその他の周波数が存在した.この数値は
Ciancaglini ら46),Gay and Bertolami47, 48),鈴木ら49, 50),堀
内ら51)のデータと一致した.
クレピタス音の分類では,周波数は 2峰性以上となる
顎関節雑音のフーリエスペクトル解析 97

結果であったが,2峰性と多峰性はクリック音ほど明確
な差はなかった.主となる第 1周波数はやはり 50~200
Hz 前後にみられ,クリック音の場合と同じ結果であっ
た.この結果から,クレピタス音も顎顔面頭蓋の共振音
であることが考えられた.また Fig 26に示すクレピタ
ス音波形を観察すると,この波形中に振幅の大きなクリ
ック様の波形を呈する部分が存在する.これは骨性アル
スローシス中にみられるクリック音と考えることもでき
る.すなわち,クレピタス音波形とは,“メキメキ”と
か“ミシミシ”という音で表現されるが,それは振幅の
小さなインパルスの連続した状態であり,その中で時折
クリック音に相当する短時間で振幅の大きなインパルス
が存在するものと考えられる.これは下顎窩と下顎頭の
骨表面の粗造性に原因しているものと考えられる.ま
た,クレピタス音の採取においても,発生側以外の反対
側でクレピタス音波形が採取されることが判明した.し
たがって,クレピタス音の解析は発生側の聴音器から採
取された波形をもって行った.
クリック音とクレピタス音の持続時間をみると,クリ
ック音の場合は 120 ms 以下であるのに対し,クレピタ
ス音は 200 ms 以上であった.これはそれぞれの発生理
由から短いインパルスと持続したインパルスとの違いに
よると考えられる.
本研究から明らかになったことは,雑音の中でクリッ
ク音やクレピタス音は,関節円板の前方転位や骨性アル
スローシスを原因として,開閉口運動時にインパルスが
発生し,これが顎顔面頭蓋内で共振を惹起させること,
この共振は顎顔面頭蓋を一つとした共振体ではなく,顎
顔面頭蓋内には種々の固有振動数を有する共振部位が存
在することが実験を通して明らかとなった.そして雑音
の発生時ごとに波形が変化するのは,共振部位が異なっ
たり,それぞれの部位で共振の大きさに差異が生じたり
するためと推測された.それを起こす原因は,雑音発生
時のインパルスの発生の位置,方向,大きさ,形状など
によって惹起される共振部位や大きさが異なることによ
るものと考えられる.
この不安定な雑音波形をいかに忠実に安定して採取す
るかという問題に関しては,まず第一に雑音採取方法を
根本的に見直すこと,第二は音響学的にノイズの少ない
S/N のよい高感度の測定系を開発することが必要であ
る.本実験で作製した聴音器は皮膚面に接触するため,
接触位置によって採取される雑音波形が変化することで
ある.雑音採取にあたり,聴音器の位置が,波形形状な
らびにスペクトルに大きな影響を与えることがわかっ
た.長い治療期間にわたり安定して雑音波形を採取する
には,聴音器をいかに同じ位置に固定するかが重要な要
件となり,測定される波形の定量評価の信頼性を決定す
る鍵となると考えられる.採取される雑音には共振音が
含まれていることから,種々の部分で発生している共振
音を,すべて確実に採取されれば,より診断情報として
の寄与は大きくなるはずである.その理由は周波数によ
って共振部位が特定でき,その部位の共振を起こすには
どこからインパルスが入力したかが推測できる可能性が
あるからである.さらに音の変化が顎関節症の治療効果
の指標となると考えられる.これらの事項が解決されて
はじめて,顎関節症の診断器として雑音を用いることが
可能になると考える.
結 論
本研究は顎関節症にみられる顎関節雑音について,そ
の発生メカニズムの解明を目的に,聴診器とマイクロホ
ンを組み合わせた聴音器を作製し,雑音の採取を行っ
た.そして,その波形とスペクトルの解析から次のよう
な結論を導くことができた.
1.顎関節雑音のうちクリック音は,スペクトル上から
みると単一周波数からなる単峰性,2つの周波数から
なる 2峰性,多峰性に分類することができた.
2.クリック音を構成する周波数のうち主たる周波数は
最も低周波数にあり,これらの周波数は,大部分の被
験者で 50 Hz から 200 Hz の間に存在した.
3.クレピタス音のスペクトルでは 2峰性と多峰性に分
類された.
4.クレピタス音の主たる周波数は 50 Hz から 200 Hz
の間に分布し,そのスペクトルはクリック音と同一で
あった.
5.顎関節雑音の持続時間は,クリック音では 120 ms
以下,クレピタス音では 200 ms 以上であった.
6.顎関節雑音は一定した周波数ではなく,発生時ごと
にスペクトルが変化する非常に不安定な音であること
がわかった.
7.顎関節雑音の発生メカニズムは,開閉口時に顎関節
内で起こるインパルスによって顎顔面頭蓋内の特定部
位で共振が惹起され,これが顎関節雑音として採取さ
れることが判明した.
8.このインパルスはクリック音の場合は,円板前方転
位にともなう相反性クリックであり,クレピタス音で
は骨性アルスローシスであろうと推測された.
9.クリック音は単発の大きなインパルスによって発生
98 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008

するのに対して,クレピタス音は小さなインパルスの
連続したものによって発生すると推測できた.
10.顎関節雑音が発生時ごとに変化するのは,インパル
スの発生部位,方向,そして大きさなどの違いから,
種々の部位の固有振動が惹起され,さらにその共振の
大きさが雑音発生のたびに異なるためと推測された.
引用文献
1)上野 正,岡 達,中村允也:顎関節症の研究(第一報).日口腔科会誌 5, 284, 1956
2)日本顎関節学会編:顎関節疾患および顎関節症の分類.日顎関節会誌 8(2),113−117, 1996
3)Foged J : Temporomandibular arthrosis. Lancet 254, 1209−1211, 1949
4)McNeill C : History and evolution of TMD concepts . OralSurg Oral Med Oral Pathol Oral Radiol Endod 83, 51−60, 1997
5)Annandale T : Displacement of the inter-articular cartilage ofthe lower jaw and its treatment by operation. Lancet 129, 411,1887
6)Lanz A : Discitis mandibularis. Zentralbl Chir 9, 289−291,1909
7)Wakeley C : The causation and treatment of displaced mandi-bular cartilage. Lancet 214, 543, 1929
8)Pringle J : Displacement of the mandibular meniscus and itstreatment. Br J Surg 6, 385−389, 1918
9)Costen JB : A syndrome of ear and sinus symptoms dependentupon disturbed function of the temporomandibular joint . AnnOtol Rhinol Laryngol 43, 1−15, 1934
10)Costen JB : Some features of the mandibular articulation as itpertains to medical diagnosis, especially in otolaryngology. J AmDent Assoc 24, 1507−1511, 1937
11)Hanau RL : Articulation defined, analyzed and formulated. JAm Dent Assoc 13, 1694−1709, 1926
12)Gysi A : Zahnersatzkunde. In : Handbuch der Zahnheilkunde.Bd IV, Urban & Schwarzenberg, Berlin, pp7−41, 1929
13)Guichet NF : Occlusal disease. In : Occlusion. Denar, Ana-heim, pp31−36, 1970
14)Laskin DM : Etiology of the pain-dysfunction syndrome. J AmDent Assoc 79, 147−153, 1969
15)Moulton MD : Psychiatric considerations in maxillofacial pain.J Am Dent Assoc 51, 408−414, 1955
16)Greene CS and Laskin DM : Long-term evaluation of conser-vative treatment for myofascial pain-dysfunction syndrome. J AmDent Assoc 89, 1365−1368, 1974
17)Rugh JD and Solberg WK : Psychological implications in tem-poromandibular pain and dysfunction . Oral Sci Rev 7, 3 − 30,1976
18)Dworkin SF, LeResche L, DeRouen T and Von Korff M : As-sessing clinical signs of temporomandibular disorders : reliabilityof clinical examiners. J Prosthet Dent 63, 574−579, 1990
19)遠藤至六郎:下顎関節の炎症性疾患.In:口腔外科通論及手術学.複製版,医学書房,東京,pp366−368, 1968
20)Lindblom G : Anatomy of the temporomandibular joint. ActaOdontol Scand 17(Suppl 28), 23−39, 1960
21)大西正俊:顎関節腔内穿刺法とその応用に関する臨床的研究.口腔病会誌 37, 178−207, 1970
22)Westesson PL, Omnell KA and Rohlin M : Double-contrast to-mography of the temporomandibular joint. Acta Radiol Diagn 21,777−784, 1980
23)東 与光,鹿島勇一,井口雅夫,閑野政則:CT スキャンの口腔領域への応用.歯界展望 53, 357−369, 1979
24)Westesson PL , Katzberg RW , Tallents RH , Sanchez-Woodworth RE, Svensson SA and Espeland MA : Temporoman-dibular joint : comparison of MR images with cryosectional anat-omy. Radiology 164, 59−64, 1987
25)Nanthaviroj S, Omnell KA, Randow K and Oberg T : Clickingand temporary“locking”in the temporomandibular joint.A clini-cal, radiographical and electromyographical study. Dentomaxillo-fac Radiol 5, 33−38, 1976
26)Rohlin M, Westesson PL and Eriksson L : The correlation oftemporomandibular joint sounds with joint morphology in fifty-five autopsy specimens. J Oral Maxillofac Surg 43, 194−200,1985
27)Ekensten B : Phonograms of anomalies of the temporomandi-bular joint in motion. Odontol Tidskr 60, 235−242, 1952
28)Findlay IA and Kilpatrick SJ : An analysis of the sounds pro-duced by the mandibular joint. J Dent Res 39, 1163−1171, 1960
29)風間栄輔,平野秀利,石岡 靖:顎関節音に関する研究第 1報.新潟歯会誌 2(2),27−35, 1972
30)Quellette PL : TMJ sound prints : electronic auscultation andsonagraphic audiospectral analysis of the temporomandibularjoint. J Am Dent Assoc 89, 623−628, 1974
31)Watt DM : A preliminary report on the auscultation of themasticatory mechanism. Dent Pract Dent Rec 14, 27−30, 1963
32)Watt DM : Clinical applications of gnathosonics. J ProsthetDent 16, 83−95, 1966
33)Watt DM : Gnathosonics-A study of sounds produced by themasticatory mechanism. J Prosthet Dent 16, 73−82, 1966
34)Watt DM and Hedegard B : The stereostethoscope-an instru-ment for clinical gnathosonics . J Prosthet Dent 18, 458 − 464,1967
35)Widmer CG, Lund JP and Feine JS : Evaluation of diagnostictests for TMD. J Calif Dent Assoc 18(3), 53−60, 1990
36)Mohl ND, McCall WD Jr, Lund JP and Plesh O : Devices forthe diagnosis and treatment of temporomandibular disorders. PartI : Introduction, scientific evidence, and jaw tracking. J ProsthetDent 63, 198−201, 1990
37)Lund JP and Widmer CG : Evaluation of the use of surfaceelectromyography in the diagnosis, documentation, and treatmentof dental patients. J Craniomandib Disord 3, 125−137, 1989
38)Farrar WB and McCarty WL Jr : Inferior joint space arthrogra-phy and characteristics of condylar paths in internal derangementsof the TMJ. J Prosthet Dent 41, 548−555, 1979
39)Farrar WB : Characteristics of the condylar path in internal de-rangements of the TMJ. J Prosthet Dent 39, 319−323, 1978
40)Ramfjord SP and Ash MM Jr : Physiology occlusion. In : Oc-clusion. 2nd ed, Saunders, Philadelphia, pp67−111, 1971
41)Tsolka P and Preiskel HW : Kinesiographic and electro-myographic assessment of the effects of occlusal adjustment ther-apy on craniomandibular disorders by a double-blind method. JProsthet Dent 69, 85−92, 1993
顎関節雑音のフーリエスペクトル解析 99

42)Hansson T and Nilner M : A study of the occurrence of symp-toms of diseases of the temporomandibular joint masticatory mus-culature and related structures. J Oral Rehabil 2, 313−324, 1975
43)米津博文:X 線テレビシステムを用いる上下関節造影検査による顎関節症患者の関節円板動態異常に関する研究.歯科学報 87, 1613−1639, 1987
44)永田和裕,旗手 敏:周波数解析を用いた顎関節音の定量的な解析法に関する研究 第 1報.日補綴歯会誌 39, 881−890, 1995
45)黒田 勝,奥村泰彦:打診音解析による口腔疾患の診断-下顎骨における打診音の発生機序-.歯放線 27, 105−120, 1987
46)Ciancaglini R, Sorini M, De Cicco L and Brodoloni F : Digitalphonoarthrometry of temporomandibular joint sounds : a prelimi-
nary report. J Oral Rehabil 14, 385−392, 198747)Gay T and Bertolami CN : The spectral properties of temporo-
mandibular joint sounds. J Dent Res 66, 1189−1194, 198748)Gay T and Bertolami CN : The acoustical characteristics of the
normal temporomandibular joint. J Dent Res 67, 56−60, 198849)鈴木 博:顎関節雑音の音響学的研究.口腔病会誌 57,
156−174, 199050)鈴木 博,半田秀穂,三浦不二夫:顎関節雑音と顎口腔機能との関連性について.日顎関節会誌 2, 37−47, 1990
51)堀内和夫,真下宏枝,山田 博:顎関節のドップラー聴診音とその周波数分析-歯科矯正診断への応用の可能性について-.バイオプログレ・スタディ会誌 8, 45−59, 1994
(受付日:2008年 4月 18日 受理日:2008年 5月 24日)
100 花輪小百合・池 真樹子・花輪浩司ほか 明海歯学 37, 2008
Related Documents











