Early maternal separation and the trajectory of borderline personality disorder symptoms THOMAS N. CRAWFORD, PATRICIA R. COHEN, HENIAN CHEN, DEIDRE M. ANGLIN, AND MIRIAM EHRENSAFT New York State Psychiatric Institute Abstract Extended maternal separations before age 5 were evaluated as a predictor of long-term risk for offspring borderline personality disorder (BPD) symptoms in longitudinal data from a large random community sample. Early separations from mother predicted elevations in BPD symptoms assessed repeatedly from early adolescence to middle adulthood. Early separations also predicted a slower than normal rate of decline in symptoms with age. Other theoretically grounded risks were examined and shown to predict elevated BPD symptoms over the developmental trajectory. Long-term effects of early separations were largely independent of childhood temperament, child abuse, maternal problems, and parenting risks. These data provide the first prospectively collected data on the developmental course of BPD symptoms and suggest a series of environmental and other influences on these very disabling problems. Borderline personality disorder (BPD) is a seri- ous psychiatric disturbance characterized by emo- tional lability, poor impulse control, and angry outbursts. In addition to core disturbances in affect regulation, BPD also manifests in chaotic interpersonal relationships, unstable identity, suicide attempts, self-mutilation, and other self- destructive behaviors (Skodol et al., 2002). The prevalence of BPD is 1–2% in the community, 10% in outpatient psychiatric clinics, and 20% in inpatient psychiatric settings (Gross et al., 2002; Lenzenweger, Loranger, Korfine, & Neff, 1997; Torgersen, Kringlen, & Cramer, 2001). Al- though women present with BPD more often than men in clinical settings (Skodol & Bender, 2003), gender differences in prevalence have not been observed in population-based epidemiological research (Torgersen et al., 2001; Winograd, Co- hen, & Chen, 2008). Approximately 3% to 10% of patients with BPD commit suicide (McGlas- han, 1986; Paris, Brown, & Nowlis, 1987; Stone, Hurt, & Stone, 1987), thus making it a serious concern for the public health. Despite widespread interest in BPD, relatively little empirical research has investigated its course and developmental origins in prospective data first gathered in childhood (Cohen, 2008). Longitudinal data from a community sample show that average symptom levels are highest in early adolescence and then decline over time (Co- hen et al., 2008; Johnson, Cohen, Kasen, Skodol, & Brook, 2000), probably because of maturation and socialization effects. Symptom levels in adult patients in clinical settings also tend to decline over time (Shea et al., 2002). Given parallel find- ings in community and clinical data, it is impor- tant to identify childhood risks that lead to early elevations in BPD symptoms but also to clarify developmental processes that delay or otherwise interfere with their usual developmental decline. The limited data on etiology show that BPD is associated with childhood histories of abuse, Address correspondence and reprint requests to: Thomas N. Crawford, Children in the Community Study, New York State Psychiatric Institute, 100 Haven Avenue, Suite 31F, New York, NY 10032; E-mail: [email protected]. columbia.edu This research was supported by NIMH Grants MH-49191 and MH-36971 and by National Institute on Drug Abuse Grant DA-03188. Development and Psychopathology 21 (2009), 1013–1030 Copyright # 2009 Cambridge University Press Printed in the United States of America doi:10.1017/S0954579409000546 1013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Early maternal separation and the trajectoryof borderline personality disorder symptoms
THOMAS N. CRAWFORD, PATRICIA R. COHEN, HENIAN CHEN,DEIDRE M. ANGLIN, AND MIRIAM EHRENSAFTNew York State Psychiatric Institute
Abstract
Extended maternal separations before age 5 were evaluated as a predictor of long-term risk for offspring borderlinepersonality disorder (BPD) symptoms in longitudinal data from a large random community sample. Early separationsfrom mother predicted elevations in BPD symptoms assessed repeatedly from early adolescence to middle adulthood.Early separations also predicted a slower than normal rate of decline in symptoms with age. Other theoretically groundedrisks were examined and shown to predict elevated BPD symptoms over the developmental trajectory. Long-termeffects of early separations were largely independent of childhood temperament, child abuse, maternal problems, andparenting risks. These data provide the first prospectively collected data on the developmental course of BPD symptomsand suggest a series of environmental and other influences on these very disabling problems.
Borderline personality disorder (BPD) is a seri-ous psychiatric disturbance characterizedbyemo-tional lability, poor impulse control, and angryoutbursts. In addition to core disturbances inaffect regulation, BPD also manifests in chaoticinterpersonal relationships, unstable identity,suicide attempts, self-mutilation, and other self-destructive behaviors (Skodol et al., 2002). Theprevalence of BPD is 1–2% in the community,10% in outpatient psychiatric clinics, and 20%in inpatient psychiatric settings (Gross et al.,2002; Lenzenweger, Loranger, Korfine, & Neff,1997; Torgersen, Kringlen,&Cramer, 2001). Al-thoughwomenpresentwithBPDmore often thanmen in clinical settings (Skodol&Bender, 2003),gender differences in prevalence have not beenobserved in population-based epidemiological
research (Torgersen et al., 2001; Winograd, Co-hen, & Chen, 2008). Approximately 3% to 10%of patients with BPD commit suicide (McGlas-han, 1986; Paris, Brown, & Nowlis, 1987; Stone,Hurt, & Stone, 1987), thus making it a seriousconcern for the public health.
Despitewidespread interest in BPD, relativelylittle empirical research has investigated itscourse and developmental origins in prospectivedata first gathered in childhood (Cohen, 2008).Longitudinal data from a community sampleshow that average symptom levels are highest inearlyadolescence and then decline over time (Co-hen et al., 2008; Johnson, Cohen, Kasen, Skodol,& Brook, 2000), probably because of maturationand socialization effects. Symptom levels in adultpatients in clinical settings also tend to declineover time (Shea et al., 2002). Given parallel find-ings in community and clinical data, it is impor-tant to identify childhood risks that lead to earlyelevations in BPD symptoms but also to clarifydevelopmental processes that delay or otherwiseinterfere with their usual developmental decline.
The limited data on etiology show that BPDis associated with childhood histories of abuse,
Address correspondence and reprint requests to:Thomas N. Crawford, Children in the Community Study,New York State Psychiatric Institute, 100 Haven Avenue,Suite 31F, New York, NY 10032; E-mail: [email protected]
This research was supported by NIMH Grants MH-49191and MH-36971 and by National Institute on Drug AbuseGrant DA-03188.
Development and Psychopathology 21 (2009), 1013–1030Copyright # 2009 Cambridge University PressPrinted in the United States of Americadoi:10.1017/S0954579409000546
1013

neglect, orother relationship-related risks reportedby clinical patients (Links, Steiner, Offord, & Ep-pel, 1988; Zanarini et al., 2002). People in thecommunity with elevated BPD symptoms oftencome from families with lower socioeconomicstatus (SES); those exposed to serious life eventsand problematic parenting also have higher riskfor BPD (Cohen et al., 2008). In absence of moreempirical data, theoretical models have hypothe-sized that childhood temperament may predis-pose young people to the affective instability, im-pulsivity, and aggression associated with BPD(Siever & Davis, 1991). Other models hypothe-size that relational factors such as insecure parent–child attachment increase risk for BPD (Agrawal,Gunderson, Holmes, & Lyons-Ruth, 2004). Thepresent study investigates whether BPD is associ-ated with extended maternal separations beforeage 5 based on expectations that they have detri-mental effects on parent–child attachment or re-flect or cause other problems in the parent–childrelationship.
Bowlby (1969, 1973, 1980) identified earlyseparations as significant threats to emotional de-velopment while working in a pediatric hospitalduring World War II. He observed how infantswere severely traumatized when separated frommother, first calling out frantically and then even-tually falling into long periods of despair. Bowlbyhypothesized that extended separations under-mine the emotional security infants or toddlersnormally experience when they are closely at-tached to primary caregivers. Young childrenrely heavily on caregivers to be available, sensi-tive, and responsive to their needs, especially inso-far as their own coping resources are developmen-tally immature. As such, separations from a parentare not just alarming in early childhood; that dis-tress is compounded when infants and toddlershave limited ability to modulate potentially over-whelming emotions on their own. Subsequent re-search confirmed that childhood separations areassociated with lasting attachment insecurity(Moss, Cyr, Bureau, Tarabulsy, & Dubois-Com-tois, 2005; Waters, Merrick, Treboux, Crowell,& Albersheim, 2000). The link between insecureattachment and early separation is important, inturn, because insecure attachment is stronglyasso-ciated with a wide range of psychopathology inyoung children, adolescents, and adults (see Mi-kulincer & Shaver, 2007, for a review).
Insecure attachment plays an especially salientrole in BPD (Agrawal et al., 2004; Bartholomew,Kwong, &Hart, 2001). As detailed in a recent re-view (Levy, 2005), there is a robust link betweenBPD diagnoses and insecurely attached adultsidentified with the Adult Attachment Interview(AAI; George, Kaplan, & Main, 1985), whichelicits thoughts, feelings, and memories aboutchildhood attachment experiences with care-givers. BPD is also robustly associatedwith a dif-ferent domain of attachment insecurity measuredwith self-report questionnaires assessing close re-lationships between adolescents or adults (Bren-nan & Shaver, 1998). However attachment inse-curity is conceptualized or measured, it is closelylinked with BPD and may even mediate associa-tions between extended separations in childhoodand subsequent personality disorder in adults.Attachment insecurity in adolescence and earlyadulthood also could maintain BPD symptomsat elevated levels during development whenthese symptoms normally subside.
Bradley (1979) investigated childhood his-tories of separation from mother before age 10in child and adolescent patients (n ! 14) diag-nosed with BPD and compared them with var-ious control samples. Separations before age 5occurred more frequently among BPD patientsthan they did among psychotic, nonpsychoticpsychiatric, and nonpsychiatrically referred de-linquent youth. In contrast, there were no differ-ences in number of separations between ages 5and 10 recorded for BPD patients and the re-maining groups. Subsequent studies investigat-ing adult patients found significant associationsbetween BPD and childhood histories of sepa-ration (Bandelow et al., 2005; Links et al.,1988; Reich & Zanarini, 2001; Soloff & Mill-ward, 1983). Data on early separations (paren-tal divorce, childhood hospitalizations, parentalhospitalization) were drawn from chart reviews,retrospective self-reports from patients, or insome cases from family informants. When pa-rental death was used to operationalize earlyseparations, it was not associated with BPD inadults (e.g., Brennan & Shaver, 1998; Paris,Zweig, & Gruzder, 1994).
Most of the available literature is limited byreliance on retrospective self-reports by adults,typically patients from clinical samples. First,childhood amnesia prevents adult recall of experi-
T. N. Crawford et al.1014

ences before age 4 or 5, thereby raising questionsabout childhood risks before that age. Second,retrospectively gathered data are often distortedby memory and reporting biases (Maughan &Rutter, 1997). Adults in emotional distress maybe more ready and willing to report earlier child-hood adversity; those who are functioning rela-tivelywell often underreport it instead (Maughan,Pickles, & Quinton, 1995; Robins et al., 1985).This reporting bias may artificially increase theassociation between early risks and adult out-comes.
Because developmental findings are morereliable when based on repeated assessmentsover a range of ages, the present study investi-gated the association between early separationsand BPD symptom trajectories in 766 youthsfrom the Children in the Community (CIC)Study (Cohen, Crawford, Johnson, & Kasen,2005). This ongoing longitudinal study hastracked the course of childhood and adolescentpsychiatric disorders and a wide array of devel-opmental risks for over 30 years. Mothers pro-vided initial data on early separations in 1975when children were on average 5 years old. Al-though reported retrospectively, the intervalbetween childhood separation and maternal re-ports was far less than the longer intervals asso-ciated with self-report data typically gatheredfrom adults. In addition, mother reports arepreferable to self-reports because they are notsubject to childhood amnesia that limits long-term recall in adults. BPD and other psychiatricdisorders were recorded in follow-up assess-ments of the children 8 years later and at threesubsequent data intervals over the next 20years. The present study focuses on separationslasting 1month or longer before the child’s fifthbirthday to determine if they predict the courseof BPD during adolescence and adulthood.
Despite its conceptual relevance, parent–child attachment security could not be evalu-ated in this study because it was not measuredin 1975 when the sample was already betweenthe ages of 1 and 10, and data came only frommaternal interviews. However, self-reported at-tachment insecurity was measured at subse-quent data intervals, thus making it possibleto examine its association with the trajectoryof BPD symptoms and to determine if it me-diates the effects of early separation. Although
the self-reported data used here pertain to inse-cure attachment in adolescence and adulthoodmore than early childhood (for differences inhow insecure attachment has been conceptual-ized and measured, see Belsky, 2002; Shaver&Mikulincer, 2002), they were tested primarilyto determine if they maintain elevations in BPDsymptoms over time.
From a developmental psychopathology per-spective (Cicchetti & Cohen, 2006a, 2006b; Rut-ter & Sroufe, 2000), it is important to evaluateearlyseparations in the context of other childhoodrisks. For instance, BPD may be associated withgeneticallymediated differences in temperament,especially differences in affect dysregulation andimpulsive aggression (Siever & Davis, 1991).Heritable vulnerabilities sometimes interact withchildhood adversity, thereby making some peo-plemore reactive to early stressors than others ex-posed to the same risks (e.g. Caspi et al., 2003;Fox et al., 2005; Kaufman et al., 2004, 2006). Re-search on infant attachment has recently shownthat heritable differences in the serotonin trans-porter gene increased risk for attachment insecur-ity, but only when combined with unresponsiveor insensitive caregiving (Barry, Kochanska, &Philibert, 2008). In research on rhesus monkeys,variations in the serotonin transporter gene inter-actedwith early separations frommothers inwaysthat increased fearful and aggressive behavior inmonkeys (Suomi, 2006). Although genetic dataare not as yet available for this sample, constitu-tional differences reflected in childhood tem-perament may mediate or moderate long-termassociations between early separation and BPDsymptoms from adolescence to adulthood.
Other family risks could render children morevulnerable to lasting effects of early separation.Childhood histories of abuse and neglect arelinked with insecure attachment and BPD(Stalker & Davies, 1995; Zanarini et al., 2002).At present, it is unknownwhether effects of thesedevelopmental risks combine in a simple additivemanner or interact in more complex ways to in-crease risk for BPD. Accordingly, we examinethe potential impact of later assessed risks onlong-term associations of early separation andother potential early risks for BPD.These includematernal characteristics and behavior reflectedin interpersonal difficulties and marital conflict,maternal consistency in childrearing practices,
Early separations and borderline personality 1015

and mother’s overall satisfaction with the child.Inconsistent parenting was selected based on itsempirical association with BPD (Bezirganian,Cohen, & Brook, 1993; Cohen et al., 2008). Ma-ternal interpersonal difficulties (having troublefeeling close, blaming others, getting angry withothers) was selected for its overlap with border-line symptoms, and thus a potential genetic ormodeling effect on offspring. Insofar as parentsmay provide a dysfunctional model of interper-sonal relationships, an essential aspect of BPD,we also tested whether marital conflict wouldpredict BPD and potentiallymediate its associa-tion with early separation. Maternal dissatisfac-tion with the child reflects both potentially harshassessment andways inwhich amother may dis-tance herself from her child. In addition to exam-ining the potential influence of these variables onthe BPD symptom trajectory, these variableswere tested to determine if they reinforce or evenpotentiate effects of early separations.
Finally, we examined the impact of comorbidschizotypal personality disorder symptoms onthe overall trajectory model because of knowncorrelation and comorbidity with BPD (Cohenet al., 2008; Kavoussi & Siever, 1992) and recentfindings linking it with early separations in thiscohort (Anglin, Cohen, & Chen, 2008). Ratherthan looking formediating ormoderating effects,this variablewas included to rule out the possibil-ity that it might explain an association found be-tween early separation and BPD.
Improving Our Understandingof Developmental Data
Here we present data on factors affecting the de-velopmental trajectory of BPD symptoms as-sessed four times over two decades, beginningwith early childhood risks. It is worth presentingour view of an important aspect of such data pre-sentation that is not often present, we admit,previously not even always in the data from thecohort studyonwhich this investigation of devel-opment is based. Of course, much developmentalresearch is cross-sectional, perhaps with retro-spective reports or other data about past expo-sures to experiences that are likely to have an in-fluence on the measure on which the currentfocus is being placed. When data are collectedrepeatedly, the most common number of times
is two, often within a single school year, orover 2 consecutive years. Nevertheless, the issuewe address remains: it is informative to presentdata in such away that themagnitude of develop-mental changes in measured data is understand-able, and the magnitude of other influences onthese variables, including on their developmentalchanges, can similarly be understood in a com-mon frame.
There are two complications with this other-wise easily accomplished goal: one is problemswith the reliability of the variables included inthe developmental trajectories and of the predic-tors of potential influences on the developmentalpath. Estimates of the “true” or valid aspects orinfluences of many of the scaled variables we as-sess require multiple measures of the componentconstructs, latent variable techniques, and validinterpretations of the meaning of changes incoefficients. For multiple time point measuresthese can get quite complicated, but are very use-ful when assumptions can bemet. Suchmethodsare almost never used for more than two or threetime points, to our knowledge. Those of us whohave been usingmultiple time-point assessmentshave gradually realized a delicious surprise: anykind of multiple assessments of a variable, in-cluding those taking place over a number ofyears, improve the reliabilityandprobable validityof their overall average and, given more than twoassessments, of their trajectory. In other words,problems of reliability/validity of a trajectory ofsuch repeated assessments are diminished, prob-ably substantially, relative to single assessments.
The other problem is how to scale variablesso that there can be a common understanding ofthe magnitude of impact of a given influence ona developmental trajectory over two or more as-sessments. An elegant and familiar solution, ifslightly more complicated than coping with asingle variable, is standardization across the tra-jectory. This is accomplished by the followingsimple process. First, a preparation for an anal-ysis of a trajectory requires “stacking” of thedata, so that for each unit being studied (usuallya person with a particular identifying number)the data are rearranged so that every assessmentof a given variable (each measure that is remea-sured over time) for each ID is in a single col-umn of data. Which assessment each variablevalue comes from is identified by some other
T. N. Crawford et al.1016

time-indicating variable, stacked in parallel (e.g.,age, date, wave of data assessment). Any “time-varying” predictors to be employed in the analy-sis may also be stacked in the file.
The next step is quick and easy: simply stan-dardize the column of data that includes the entireset of measures of your dependent variable. Sec-ond, when your main interest is developmentalchange, center your measure of age (or time) atthemeanvalue across the trajectory data. In conse-quence, there will be two large advantages: first,themagnitudeof the rate of developmental changein the dependent variable will be easily under-stood. Whether the time units are dates, ages, orwaves, analyses using this variable as a trajectorypredictor will estimate the mean developmentalchange per time unit expressed in standard devia-tions. Second, the estimated effects of all predic-tors can be separated into effects on the overalllevel estimated at the average age and effect onthe rate of change, estimated by the product of thepredictor and the time variable (e.g., age). Morecomplex analyses can investigate nonlinear devel-opmental changes, forwhich appropriate transfor-mations of the time variable may be complex.
Having accomplished this transformation,additional understanding of effect magnitudeswill come by standardizing predictors that arenot scaled in understood units, such as a num-ber of something, or no or yes. Doing so willenable comparison of the effects of differentmeasures on the trajectory mean, and better un-derstanding of the magnitude of potential me-diation effects when variables are combined intrajectory-predicting equations.
In this paper our focus will naturally fall on thesubstantive issues, but we will try throughout tomake clear our interpretation of the magnitude ofsignificant effects as assessed, in keeping withour belief that we must ultimately know not onlywhat influencesdevelopment, but also accumulateevidence about magnitudes of such influences.
Method
Participants
The CIC sample is a cohort of children origi-nally drawn in 1975 from randomly sampledfamily households in rural, suburban, city, andcentral city areas in two counties in upstate
NewYork, picked for demographic resemblanceto the full US population (prior to large-scale im-migration from Latin America). The initial inter-views of 976 mothers related to one child be-tween ages 1 and 10 randomly selected fromage-eligible children in the household. Inter-views covered a wide array of issues related tooffspringwell-being including the child’s health,temperament, attitudes, behavior, relationshipwith parents, and social environment, includingparental problems, and significant events suchas extended separations, divorce, and deaths offamilymembers. Eighty-five percent of the origi-nal families were identified and relocated in1983, and 78% agreed to participate in a fol-low-up interview with the mother and/or a sepa-rate interview with the sample child. Many fam-ilies living in poor urban areas could not belocated because whole neighborhoods had beentorn down for urban renewal. To replace theseyoung, urban, and poor families excessivelylost to follow-up, this sample was supplementedwith 54 families from comparable areas of urbanpoverty within the sampled region who hadchildren between ages 9 and 12 years. The sam-ple’s racial distribution (91% Caucasian, 8%African American) and SES (21% with familyincome below the poverty line at some time inchildhood, 25% with upper middle class educa-tional and income) were representative of thetwo counties.
Data for the present study were drawn from766 youth who participated in two or more fol-low-up interviews conducted in 1983 (N ! 756;mean age ! 13.7, SD ! 2.6 years), 1985–1986(N ! 746; mean age ! 16.1, SD ! 2.8 years),1991–1993 (N ! 749: 717 with complete infor-mation; mean age ! 22.0, SD ! 2.7 years), and2001–2004 (N ! 678; mean age ! 33.1, SD !2.8 years).Aftermaintaining youth retention ratesexceeding 90% through the 1991–1993 assess-ment, participation dropped to about 84% in the2001–2004 assessment. Similar problemsof attri-tion have been observed in other recent longitu-dinal studies of community and clinical samplesand reflect loss because of unknown relocationand failure to respond to study communications.Men surveyed in adolescence have been lesslikely than women to participate in adulthood, al-though there have been very few respondentswho have declined to continue in the study.
Early separations and borderline personality 1017

Race, SES, and psychiatric disorder have notbeen related to attrition.
This cohort study includes participants bornover a full decade. In consequence at every agebetween 9 and 39 a number of assessmentswere available for these analyses, easing concernsabout potential nonlinear changes thatmight havetaken place in the years between assessments.Additional details about this community sampleare available on the study Website (http://nyspi.org/childcom). Informed consent or assent wasobtained for all interviews and a NIH Certificateof Confidentiality exists for these data.
Measures
BPD. There were no existing measures of Diag-nostic and Statistical Manual of Mental Disor-ders (DSM) personality disorders for adolescentswhen this cohort was first followed up in 1983.Items were drawn from the Personality Diagnos-tic Questionnaire (Hyler, Rieder, Spitzer, &Wil-liams, 1982; Hyler, Skodol, Kellman, Oldham,& Rosnick, 1990) and adapted as necessary tomake them age appropriate. Additional itemshave been selected from the CIC protocol to pro-duce measures that closely correspond to DSM-IV (American Psychiatric Association, 1994) di-agnostic criteria. The present report used BPDsymptom scales based on 15 youth-reporteditems assessed at mean ages 13.7, 16.1, 22.0,and 33.1 (mean Cronbach a ! .74).1 Items inthe BPD scale (measured on Likert scales mostlyranging from 1 to 4) were summed and standard-ized as described above, thus making develop-mental change easier to interpret. Convergent
validity for the BPD scale at mean age 33 is good;it is positively correlated with the BPD self-report scale on the Structured Clinical Interviewfor DSM-IV (SCID-II; First, Gibbon, Spitzer,Williams,&Benjamin, 1997) PersonalityQuestion-naire (r ! .74, p , .001). By comparison, themedian correlation between self-report BPDscales was only .41 when agreement was as-sessed in 13 other studies (Modestin, Ern, &Oberson, 1998). TheBPDscalewas stable across11 years from mean ages 22 to 33 (r ! .51, p,.01), and predicted a clinician’s assessment ofglobal functioning after completion of a clinicalinterview (Crawford et al., 2005). This measurehas been validated in additional longitudinal re-search showing that adolescent BPD is associ-atedwith adult borderline symptoms and diagno-ses, lower academic and occupational attainment,higher need for services at mean age 33 (Wino-grad et al., 2008), higher partner conflict (Chenet al., 2004), and long-term reductions in qualityof life (Chen et al., 2006).
Maternal separation. Mothers provided dataabout early separations in 1975 and at follow-upin 1983.Motherswere initially asked, “Have therebeen any times since (CHILD) was born that youhave been separatedmore than a month either be-cause you were away or because (CHILD) wasaway from home?” In 1983 mothers were asked,“Howmany times since 1975haveyoubeen sepa-rated from (CHILD) for more than a month?” Inboth cases positive responses were followed upwith questions about the duration, timing, and rea-son for the separation. Based on Bradley’s (1979)finding that early separations increased risk forBPD, we identified participants who were sepa-rated from mother for at least one month beforeage 5. This age was also selected as a reasonablecutoff becausematernal separations becomemorenormative after age 5 (e.g., enrollment in primaryeducation, going away to summer camp, etc.). Al-together, 35 children (4% of the sample) were ex-posed to this operational definition of early sep-arations. Five children were separated becauseof childhood hospitalization or illness, 13 had ex-tended separations because of maternal hospitali-zation or illness, and 17 were separated for otherreasons. These other separations included ex-tended visits to a relative, or the mother’s depar-ture for personal, educational, or professional
1. Earlier published reports on personality disorders in thiscohort have employed combined maternal–child re-ported symptoms using DSM-III (American PsychiatricAssociation, 1980) andDSM-IV criteria. Evidence basedon the longitudinal data suggests that youth self-reportmay predict prognosis and dysfunction better, and recentreports have employed these measures. We have pub-lished data elsewhere on a 22-item self-report BPD scale(Crawford et al., 2005), which used 7 additional itemsavailable only in the last two data waves. The abbrevi-ated 15-item scale was used here because it provides aconsistent repeated measure at all four data intervalsfrom adolescence into adulthood, including the adoles-cent assessments at mean ages 13.7 and 16.3. The corre-lation between the abbreviated and complete BPD scaleis .97.
T. N. Crawford et al.1018

reasons. We used the length of separations (mean! 15.7 weeks, range ! 4–59 weeks) as a scaledmeasure for statistical analyses.
No early separationswere attributable to fostercare placement. To determine if early parentaldeath increased risk for BPD, we identified 11children whose mother or father died before age5. However, early parental death was not associ-atedwith BPD in any statistical analyses. Parentaldivorces that occurred before the child turned 10were also not predictive of BPD symptoms in theoffspring. Based on these findings, we did not in-clude parental death or divorce in this paper.
Demographic factors. SES was measured as astandardized sum of standardized measures ofyears of maternal and paternal education, occu-pational status, and family income. SES variesinversely with BPD symptoms (Cohen et al.,2008). Gender and race (White vs. not White)were not associated with BPD in this communitysample. Despite higher rates of women in BPDclinical populations, recent evidence stronglysuggests that this differential may be because ofbiases in diagnosing practice (Skodol & Bender,2003).
Child risk factors. Mothers were asked abouttheir child’s temperament in 1975 using itemsadapted from the Thomas and Chess longitu-dinal study that tracked temperament fromchildhood to adolescence (Chess & Thomas,1978; Thomas & Chess, 1977; Thomas, Chess,& Birch, 1970). Although items varied by age,a fixed set of items covered ages 4 to 10. Eightyears later newly recruited mothers with chil-dren ages 9 to 12 and mothers of childrenfrom the original sample who were then 9 to12 were administered the same items. To mini-mize age effects, the assessment closest to age 9was selected for each child and then adjustedfor sex-specific age changes, converting thedata covering ages 6 to 12 to estimates at a con-stant age 9. Two temperament scales were se-lected as predictors based on correlations withearly separation. The “crying/demanding” scaleuses seven items (Cronbach a ! .68) to assessfrequency of crying, mood reactivity, and de-mands for attention. Two additional items inthe scale asked whether the child’s crying an-noyed mother and father. The “crying/demand-
ing” scale corresponds to early measures of“difficult” temperament (Thomas & Chess,1977; Thomas, Chess, & Korn, 1982). The “an-gry/tantrum” scale uses four items (a ! .47) toassess how frequently the child cries or com-plains loudly, screams when angry, kicks andthrows things, and has temper tantrums. Theseitems resemble those in the “frustration” scalesof the Children’s Behavior Questionnaire(Rothbart, Ahadi, Hershey, & Fisher, 2001).
Maternal risk factors. Maternal interpersonaldifficulties, marital conflict, inconsistency inchild rearing, and dissatisfaction with the childwere reported by mothers when children wereon average 13.7 years old (age range ! 9.1–18.6 years). Maternal interpersonal difficultieswere measured with five items (a! .73) adaptedfrom the System Checklist–90 (Derogatis, Lip-man, Rickles, Uhlenhuth, & Covi, 1974) that as-sess problems getting close to others, havingtemper outbursts, feeling tense or anxious, feel-ing easily annoyed, and blaming others. TheMarital Conflict Scale is a three-item index (a! .58) that assesses three components Finchamand Osborne (1993) identified as important sub-dimensions of marital conflict: (a) the frequency,(b) their average intensity (calm to potential vio-lence), and (c) whether the differences end up innegotiated agreement or ongoing disagreement.Marital conflict has been linked to problematicoffspring emotional security (Davies & Cum-mings, 1994), a component of BPD symptoms.
Maternal inconsistency (a ! .63) was mea-sured with three mother-reported items adaptedfrom a maternal inconsistency scale (Schaefer,1965) and two items from a separate rule scale(Jessor,Graves,Hanson,& Jessor, 1968). Sampleitems include “How consistent are you in the wayyou handle your child?” and “I often change therules that my child is supposed to follow.”Mater-nal dissatisfaction wasmeasured with six originalitems (a ! .81) that assess maternal satisfaction/dissatisfaction with the child’s physical appear-ance, intellectual and interpersonal ability, moraland emotional behavior, and achievement inschool. Prior research has supported the validityand predictive utility of these three measures(Berenson, Crawford, Cohen, & Brook, 2005;Bezirganian et al., 1993; Cohen, 1996; Cohen &Cohen, 1996; Crawford, Cohen, Midlarsky, &
Early separations and borderline personality 1019

Brook, 2001; Johnson, Cohen, Kasen, Ehrensaft,& Crawford, 2006; Schaefer, 1965).
Child maltreatment. Official records identified37 participants who met legal criteria for sexualabuse, physical abuse, or neglect.
Insecure attachment. Self-reported attachmentinsecurity was assessed at mean age 16.1 withthe CIC attachment scales (Crawford et al., 2006)using 13 items (a ! .87) to measure attachmentanxiety (fears of abandonment) and 14 items (a! .87) tomeasure attachment avoidance (discom-fort with intimacy). These scales assess the sameattachment dimensions as theExperience inCloseRelationships Inventory (ECR;Brennan,Clark,&Shaver, 1998), awidely used instrument first pub-lished after adolescents in the CIC study were al-ready interviewed. Item content in these scales fo-cused on how respondents felt about their closestrelationships at the time of assessment. Correla-tions between anxious attachment scales on CICand ECRmeasures (r! .70) and associations be-tween corresponding avoidant attachment scales(r ! .71) were reasonably high in a separate col-lege validation sample (N! 307), thus supportingthe convergent validity of these scales.
Additional risks. Schizotypal personality disor-der symptoms correlatewith BPD symptoms (Co-hen et al., 2008) and have recently been linkedwith early separations (Anglin et al., 2008). Ac-cordingly, schizotypal symptomsassessed inearlyadolescencewere examined to control for their po-tentially confounding effect on risks for BPD, es-pecially early separation. Schizotypal symptomswere measured with self-report items from theCIC protocol that match DSM diagnostic criteria(Crawford et al., 2005). The internal consistencyof this 16-item scale was acceptable (mean a !.61). The same scale correlated .49 with theSchizotypal Scale on the StructuredClinical Inter-val for DSM-III-R (SCID-II) Personality Ques-tionnaire and2.46 with clinician reported GlobalAssessment of FunctioningScale (Crawford et al.,2005).
Data analyses
Hierarchical linear regression modeling (HLM)was used to investigate associations between
early separations and age trajectories for BPDsymptoms from age 9 to 39. The SAS PROCMIXED program generated maximum likeli-hood estimates of fixed effects (average) and ran-dom effects (differences between participants)associated with each study variable. Linear tra-jectories were assessed in all HLMmodels repre-sented by the age variable. Age was centered atage 20: here the (!0) intercept equals the meanlevel of BPD symptoms at age 20 when all otherpredictors equal zero.
Initial analyses examined the effects of earlyseparation on trajectory of BPD symptoms aswell as the reasons given for those separations.Subsequent analyses added the covariates speci-fied above to determine if they mediate, moder-ate, or confound the effects of early separationson subsequentBPDsymptoms.To facilitatecom-parisons of effect sizes across models, all scaledpredictors (except weeks of separation and age)were standardized. (For interested readers, equa-tions used in HLM analyses are available fromthe author upon request.)
Results
HLMmodels confirmed that extended separationsfrom mother before age 5 were associated withBPD symptoms in adolescence and adulthood.Table 1 shows that children with early separationshad significantly higher BPD symptoms, 0.0172SD/week of separation, than children not separa-ted from mother. At the average separation dura-tion of 15.7 weeks, we find the effect ! 15.7"0.0172! 0.27 SD, a surprisingly large effect con-sidering the elapsed time between the early child-hood risk and the average age 20 when BPDsymptoms were assessed. As expected, BPDsymptoms decreased with age (20.0341 SD/year), thus reflecting normal declines observedacross adolescence and early adulthood. How-ever, the level of BPD symptoms declined lessover the full trajectory for thosewho had extendedearly separations (see Figure 1 for the estimate forthe average 15.7-week separation). On average,young people from families with lower SES hadsignificantly higher risk for BPD.
Dummy variables were used to parse theseparation variable into three independent vari-ables based on reasons why mother and childwere separated: mother’s illness (n ! 13),
T. N. Crawford et al.1020
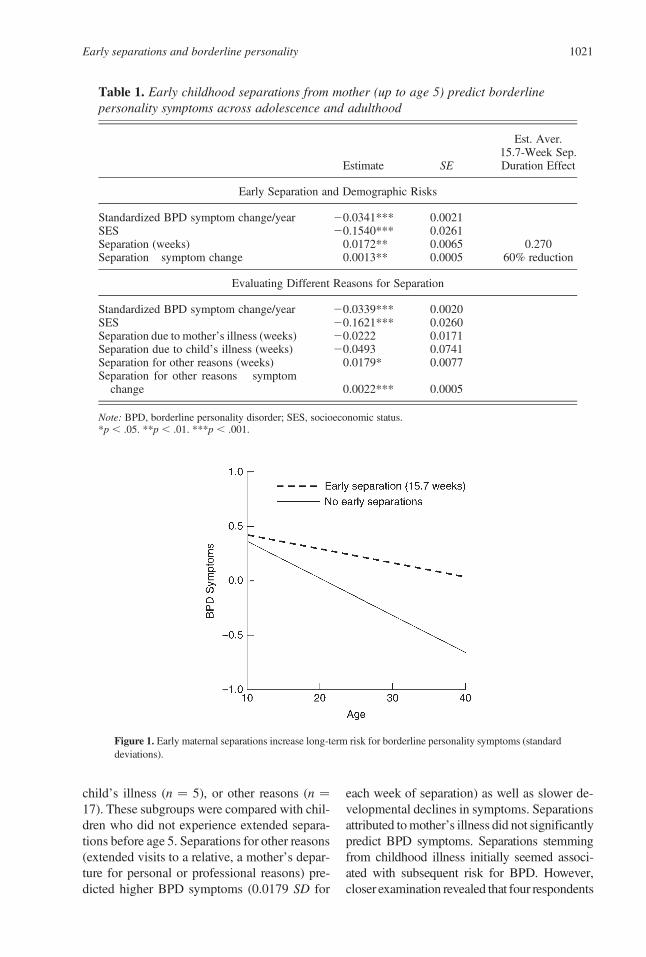
child’s illness (n ! 5), or other reasons (n !17). These subgroups were compared with chil-dren who did not experience extended separa-tions before age 5. Separations for other reasons(extended visits to a relative, a mother’s depar-ture for personal or professional reasons) pre-dicted higher BPD symptoms (0.0179 SD for
each week of separation) as well as slower de-velopmental declines in symptoms. Separationsattributed tomother’s illness did not significantlypredict BPD symptoms. Separations stemmingfrom childhood illness initially seemed associ-ated with subsequent risk for BPD. However,closer examination revealed that four respondents
Table 1. Early childhood separations from mother (up to age 5) predict borderlinepersonality symptoms across adolescence and adulthood
Estimate SE
Est. Aver.15.7-Week Sep.Duration Effect
Early Separation and Demographic Risks
Standardized BPD symptom change/year 20.0341*** 0.0021SES 20.1540*** 0.0261Separation (weeks) 0.0172** 0.0065 0.270Separation! symptom change 0.0013** 0.0005 60% reduction
Evaluating Different Reasons for Separation
Standardized BPD symptom change/year 20.0339*** 0.0020SES 20.1621*** 0.0260Separation due to mother’s illness (weeks) 20.0222 0.0171Separation due to child’s illness (weeks) 20.0493 0.0741Separation for other reasons (weeks) 0.0179* 0.0077Separation for other reasons ! symptom
change 0.0022*** 0.0005
Note: BPD, borderline personality disorder; SES, socioeconomic status.*p , .05. **p , .01. ***p , .001.
Figure 1. Early maternal separations increase long-term risk for borderline personality symptoms (standarddeviations).
Early separations and borderline personality 1021

had hospitalizations that were similar in duration(4–6 weeks) and one had a much longer hospitalstay (26 weeks). When this outlier was removed,the association between BPD and separations at-tributed to childhood illness disappeared. Toavoid reporting unreliable results, findings in Ta-ble 1were based on the samplewithout the singleoutlier. Nevertheless, because these analyses ofcause-specific separation may have missed trueassociations with later BPD symptoms becauseof very small numbers of children in subgroups,we carried out subsequent HLM analyses forthe full set of children who experienced extendedseparation from their mothers regardless of rea-son.We employedweeks of separation as the pre-dictor in all subsequent analyses.
Table 2 reports analyses that examined the cu-mulating andmediating effects of other risks, en-tered in the sequence that they took place or werefirst measured. Thus, we can examine the media-tion of the association of early risks, includingearly separation, on the developmental trajectoryof BPD symptoms by later risks.
The baseline model specified childhood sep-arations as a predictor of both mean and slope(linear change with age) of BPD symptom trajec-tory. Overall estimates of the effects of early sepa-rationwere calculatedbymultiplying the estimatedeffect per week by themean separation duration!15.7 weeks (reported in the third column of Ta-ble 2). Estimates of the effects on BPD symptomchange per year are similarlymade bymultiplyingthe weekly effect by the mean number of weeksand dividing this estimate by the reference annualmean change from the same equation.
Subsequent models identify later trajectorypredictors and enable estimation of potentialmeditational effects of these predictors on the as-sociation between early separation and the BPDsymptom trajectory. Moderating effects of laterrisks on the early separation effects were testedby adding products of these variables to the pre-diction equations, but none were statistically sig-nificant. We also did not find a later risk that wasrelated to the slope (change per year) of the tra-jectory of BPD symptoms, and therefore, theseare not included in the table.
In the baseline model, the average effect ofearly separations (mean ! 15.7 weeks) was as-sociated with increases in BPD symptoms thatwere over 0.25 SD in magnitude, a rather sub-
stantial effect over a 15- to 19-year period. Inthe baseline model we see that annual symptomdecline is estimated to be 65% slower for thoseat the average number of separated weeks.
Model 1 in Table 2 adds child temperamentrisks estimated at age 9. Each standard devia-tion increase in angry temperament was associ-ated with a 0.0951 SD increase in BPD symp-toms. Each standard deviation increase incrying/demanding temperament was indepen-dently associated with a 0.1054 SD increase.Parameter estimates for differences in symptommean and symptom trajectory associated withearly separation changed little when tempera-ment risks were added to the model. Thus, ma-ternal reports of child temperament did not me-diate early separation effects onBPD, indicatingindependence of these risks.
Model 2 shows that a documented history ofabuse was associated with a 0.5603 SD increasein risk for BPD symptoms, an estimate consistentwith previous evidence of the history of abuse re-ported by BPD patients. However, abuse did notsubstantially mediate the early separation effectson the BPD symptom trajectory.
Model 3 adds parental variables to the po-tential predictors, all assessed at the sametime as the first offspring report of BPD symp-toms (mean age ! 13.7). We see that inconsis-tent mothering and low maternal satisfactionwith the child were significant predictors ofhigher BPD symptoms. For each standard de-viation decrease in maternal satisfaction, therewas a 0.1579 SD increase in BPD symptoms.Inconsistent mothering had a much smaller in-dependent effect. These mother-reported vari-ables also partially mediated the effects of herearlier reports of her child’s temperament. Theindependent effect of crying–demanding wasno longer statistically significant, and the effectof angry temperament was lowered almost 40%.Maternal interpersonal difficulties and parentalconflict did not significantly predict offspringBPD symptoms independently of other varia-bles in the model.
Model 4 adds anxious and avoidant attach-ment measured in middle adolescence. Foreach standard deviation increase in attachmentanxiety, there was a notably large elevation inBPD symptoms over the trajectory (0.3756 SD):independent effects of attachment avoidance
T. N. Crawford et al.1022

Table 2. Estimated standardized effects of risks on the trajectory of borderlinedisorder symptoms from early adolescence to 20 years later as adults
Estimate SE
Est. Aver.15.7-Week Sep.Duration Effect
Baseline Comparison Model
BPD symptom change/year 20.0341*** 0.0021Separation (weeks) 0.0201** 0.0067 0.270 SDSeparation! symptom change 0.0014** 0.0005 65% reduction
Model 1: Separation and Childhood Temperament Risks
BPD symptom change/year 20.0340*** 0.0021Separation (weeks) 0.0157* 0.0065 0.246 SD*Separation! symptom change 0.0014** 0.0005 65% reductionAngry temperament (age 9) 0.0951** 0.0284Crying/demanding (age 9) 0.1054** 0.0289
Model 2: Adding Abuse History
BPD symptom change/year 20.0339*** 0.0021Separation (weeks) 0.0130* 0.0064 0.204 SD*Separation! symptom change 0.0014** 0.0005 65% reductionAngry temperament age 9 0.0970*** 0.0280Crying/demanding age 9 0.0951*** 0.0285Abuse record 0.5603*** 0.1149
Model 3: Adding Maternal Risk and Parenting
BPD symptom change/year 20.0340*** 0.0209Separation (weeks) 0.0106 0.0062 0.166 SDSeparation! symptom change 0.0014** 0.0005 65% reduction*Angry temperament age 9 0.0597* 0.0276Crying/demanding age 9 0.0500 0.0288Abuse 0.5131*** 0.1127Parental conflict 0.0000 0.0274Maternal interpersonal difficulty 0.0365 0.0302Inconsistent mothering 0.0555* 0.0273Maternal satisfaction with child 20.1579*** 0.0298
Model 4: Adding Adolescent Attachment
BPD symptom change/year 20.0340*** 0.0020Separation (weeks) 0.0079 0.0053 0.141 SDSeparation! symptom change 0.0015* 0.0005 69% reduction*Angry temperament age 9 0.0606** 0.0235Crying/demanding age 9 0.0294 0.0245Abuse 0.4249*** 0.0959Inconsistent mothering 0.0236 0.0232Maternal satisfaction with child 20.1313*** 0.0253Anxious attachment in adolescence 0.3756*** 0.0225Avoidant attachment in adolescence 0.0934*** 0.0220
Note: BPD, borderline personality disorder.*p , .05. **p , .01. ***p , .001.
Early separations and borderline personality 1023

were also significant but much less dramatic(0.0934 SD). In this model the (modest) esti-mated effects of maternal inconsistency wereno longer statistically significant, and nearly20% of the association of abuse history wasmediated by these variables. However, the ef-fect of early separation on the lesser declineof BPD symptoms with age remained robust,and is nearly 70% less per year than estimatedin those participants without these risks.
In separate models (not shown in Table 2) weaddedschizotypalPDsymptomsassessed in the in-itial assessment (mean age! 13.7) to these predic-tors. This inclusion did not affect the estimates ofearly separation effects on the BPD symptom tra-jectory, and only the effect of avoidant attachmentin adolescence was changed from marginal to notsignificant in this model. Schizotypal symptomsare not viewed as an unambiguous “mediator” be-cause the causal direction between symptoms ofthese two disorders is not known. However, wealso evaluated the trajectory of schizotypal symp-toms (measured as a time-varying covariate fromearly adolescence to middle adulthood) to deter-mine if its own associations with early separations(Anglin et al., 2008) and co-occurring BPD symp-toms (Cohen et al., 2008)might account for the ef-fects observed here. The estimated effect of earlyseparation on the trajectory of BPD symptomsdid not change when co-occurring schizotypalsymptoms were added to the model.
Discussion
Associations between early childhood risks andadult psychopathology are often hypothesizedbut seldom observed. This outcome stems notjust from a shortage of longitudinal data; moresubstantively, it reflects how individual trajec-tories are affected by many factors throughoutdevelopment (e.g., heritable vulnerability or re-siliency factors, stability or change in familycomposition, exposure to new relationshipsoutside the family, etc.) that influence whetheror not early risks eventually manifest as psy-chopathology in adults. In this context, it isnoteworthy that extended childhood separationfrom mother before age 5 was associated withBPD symptom trajectory up to 30 years later.
The present study reinforces prior researchlinking early separation and BPD in children
and adolescents (Bradley, 1979). Our findingsalso reinforce studies that found associationsbetween BPD in adults and early separationsbased on retrospectively reported data (Bande-low et al., 2005; Links et al., 1988; Reich &Zanarini, 2001; Soloff&Millward, 1983), espe-cially insofar as our prospective data are lesslikely to be distorted by memory and reportingbiases. Not only were BPD symptoms higher onaverage among children with early separations,the same symptoms declined at significantlyslower rates than those observed in young peo-ple without early separations. In most cases,elevated personality disorder symptoms de-crease in adolescence because of normativematuration and socialization processes (Cohen& Crawford, 2005). Slower declines in youngpeople with early separations suggest that theiremotional development lags behind age peersduring adolescence and early adulthood.
Childhood separations by themselvesmay notincrease long-term risk for BPD. Early separa-tions attributed to extended child ormaternal hos-pitalization were not associated with the BPDsymptoms or their developmental trajectory. De-finitive results, however,will require longitudinaldata on more cases than those available here.These findings contrast with those observedwhen 66 adult patients with BPDwere comparedwith 109 nonpsychiatric controls (Bandelowet al., 2005). Patients hadmore retrospectively re-ported childhood hospitalizations than healthycontrols (72.7% vs. 37.6%, p , .001), althoughthese hospitalizations were not limited to thetime between birth and age 5. Adults with BPDalso reported more childhood separations be-cause of maternal hospitalizations than controls(65.6%vs. 34.9%, p, .001).Different outcomesmay stem from differences between clinical andcommunity samples. Each childhood risk in-creases not just the likelihood of psychopathol-ogy; as risks and psychopathology accumulatethey also increase the likelihood of treatmentseeking, thereby resulting in an ascertainmentbias in clinical samples that may artificially in-flate associations between BPD and childhoodand maternal hospitalizations. Recall biases inretrospectively reported data may also inflate as-sociations observed by Bandelow et al. (2005).
Long-term risk for BPD in our communitysample was more reliably associated with
T. N. Crawford et al.1024

childhood separations attributed to other rea-sons: mothers leaving for personal reasons, re-locating for professional or educational pur-poses, or children going away for extendedvisits to a relative. Although we lack detailedinformation about what motivated these separa-tions, parents who sent children to live with rel-atives may have done so because of the child’sbehavioral problems that were difficult to toler-ate or manage. In other cases, mothers mayhave placed a higher priority on educational,professional, or personal goals than on parent-ing responsibilities, at least for the duration oftheir absence. Extended separation thus couldbe a long-term risk only insofar as they reflecta lack of maternal investment in caregiving.
Such separations may be difficult for youngchildren to understand, perhaps leading them toblame themselves for mother’s absence. Thesecognitions may have a harmful impact on thechild’s mental representations of self and other:the “internal working models” emphasized inBowlby’s theory (Bowlby, 1969, 1973, 1980;Bretherton & Munholland, 1999). If childrenbelieve that their mother did not want to bewith them or care about their needs, they mayform mental representations of themselves asbeing unworthy of love and expect significantothers to be uninterested or rejecting. To the ex-tent that such affectively laden representationsundermine attachment security, they may alsoincrease risk for psychopathology. In theseanalyses we find that the elevation of BPDsymptoms at the trajectory mean age was about0.25 SD for separations of the average length, asmall to medium effect when considered overthis extended period. Perhaps more impressiveis the impact on the normative annual BPDsymptom decline, running at about one-thirdthe rate experienced by those without early sep-aration. This effect was essentially unmediatedby any of the measured later risks.
Maternal reports of childhood temperamentpredicted higher BPD symptoms at the trajec-tory mean, with about a 0.1 SD increase insymptoms per standard deviation increase. As-sociations between childhood temperament andBPD specifically support Siever and Davis’s(1991) model of this disorder. The impulsiveaggression hypothesized in their model, in-dexed here by angry tantrums at mean age 9,
predicted BPD symptoms in adolescence andadulthood. BPD was also associated with fre-quent crying, mood reactivity, and demandsfor attention at mean age 9, which may reflectthe heritable predisposition to affective instabil-ity Siever and Davis hypothesize in their model.The childhood temperament variables mediatedalmost 20% of the early separation associationwith mean BPD symptoms over the trajectory(reduction from .0201 to .0157 per week) butdid not mediate the impact of early separationon estimated annual decline in symptoms. As-sociations between childhood temperamentand BPD are noteworthy in themselves becausethey extend well into adulthood and have notbeen examined previously in developmentaldata. Of course, variables measuring angry tan-trums and crying/demanding behaviors couldalso stem from family disturbances instead ofgenetically mediated differences in tempera-ment: as noted below, the effects of the tem-perament variables were mediated primarilyby the maternal parenting risks.
A recorded history of child abuse had the ex-pected very large association with BPD symp-tom mean over the trajectory (increase of .0.5SD for those with such a history), but very mod-est mediation effect on early separation relation-ship with this mean and none on the trajectoryslope or on the temperament effects. Severeabuse has been linked with lasting disruptionsof the hypothalamic–pituitary–adrenal system,which regulates the release of glucocorticoid hor-mones into the bloodstream in normal daily cy-cles but also in response to stress (Smith &Vale, 2006; Van Voorhees & Scarpa, 2004). Se-vere or prolonged stress from familial adversityin early development may result in hyperactiva-tion of the hypothalamic–pituitary–adrenal sys-tem (hypercortisolism) and amygdala hyper-function (fear reaction; Charmandari, Kino,Souvatzoglou, & Chrousos, 2003; Heim & Ne-meroff, 2001; Tarullo & Gunnar, 2006). Addi-tional research is needed to determine if thisphysiological mechanism mediates associationsbetween early risks and BPD (Garner et al.,2007; Lieb et al., 2004).
Maternal interpersonal difficulties did not re-late to offspring BPD symptoms, nor did paren-tal conflict. These findings surprised us becausewe anticipated that maternal behaviors reflecting
Early separations and borderline personality 1025

some of the serious aspects of BPD symptomswould have presented a “model” of expected ornormative behavior to her child, as conflict be-tween the parents might also have done. Theymight even have reflected a component of poten-tial genetic transmission. However, inconsistentparenting and to a much larger degree her dissat-isfaction with her child as reported to a stranger(the interviewer) did predict subsequent BPDsymptoms over the trajectory. These predictionsmediated the effect of early separation enough toreduce the estimated independent effect on meansymptoms to a level that is no longer statisticallysignificant. Although maternal dissatisfactioncould plausibly amplify an existing risk fromearly separation (e.g., by reinforcing internalworking models that make the child feel unwor-thyof love),nomoderatingeffectswereobserved.In addition, these parent variables did not medi-ate the lesser decline in BPD symptoms with agein those who had experienced such separations.
We have long viewed very low scores on thesatisfaction variable as a representation of nearhostility of the mother toward the child: consis-tent dissatisfaction of her child’s appearance, in-telligence, relationships, emotional behavior,achievement, and moral behavior. We also notethat, although temperament risks were not medi-ated by abuse records, they were substantiallymediated by inconsistent mothering and mater-nal satisfaction with the child (both mother re-ported). This pattern, if accepted as measuredin these data, suggests that even very problematic“difficult” childrenmay turn out to be fairlywell-adjusted adults if accepted and managed wiselyby parents (Thomas & Chess, 1978).
Risk associated with early separation was in-dependent of self-reported attachment anxiety(abandonment fears) and avoidance (discom-fort with intimacy) experienced in close rela-tionships in mid to late adolescence. Attach-ment anxiety in close/romantic relationshipswas notably more associated with higher BPDsymptoms (over 0.5 SD of BPD symptoms forevery standard deviation of anxious attach-ment) than was avoidant attachment (about0.125 SD of BPD symptoms for every standarddeviation of avoidant attachment). This highrelationship is consistent with the salience ofabandonment fears in BPD reported elsewherein the literature (for a review, see Levy,
2005). The association with attachment avoid-ance and BPD has been more variable, some-times showing positive associations and othertimes inverse associations with BPD. Thisvariability may reflect differences in how peo-ple defend against high attachment anxiety,some by distancing themselves from close rela-tionships (high avoidance), others by clingingto close friends or romantic partners instead(low avoidance). Some variability may alsoreflect differences in sample composition; onaverage, treatment-seeking individuals in clini-cal samples may experience less avoidance, andpeople selected at random for community sam-ples may report higher avoidance instead.
Contrary to expectations, self-reported at-tachment anxiety and avoidance did not medi-ate the association between early separationand BPD symptoms. Indeed, the available at-tachment variables were not significantly asso-ciated with early separations, probably becauseself-report attachment questionnaires focus onclose relationships between adolescents oradults, not the parent–child relationships stud-ied in the childhood attachment literature. Theestimated effects of inconsistent parentingwere somewhat mediated by the adolescent at-tachment variables in this model.
Instead, the self-reported attachment variablesreduced the estimated impact of child abuse his-tory on BPD symptoms by about 20%. To the ex-tent that child abuse increases attachment insecur-ity during adolescence and adulthood, it mayinstill ongoing attachment anxiety that is stronglyassociated with BPD. If so, attachment anxietymay play a key role in maintaining elevated BPDsymptoms across adolescent and early adult de-velopment when these symptoms might other-wise subside.
Child maltreatment by primary caregivershas also been linked with “disorganized attach-ment” (Solomon & George, 1999), which oftenoccurs when maltreated children seek comfortfrom primary caregivers who have abusedthem in the past. When young children feartheir primary caregiver, or when the caregiverherself is afraid, children experience approach/avoidance conflicts and often have dazed disso-ciative responses on reunion following a briefseparation. When the effects of childhood mal-treatment and disorganized attachment persist
T. N. Crawford et al.1026

into adulthood, they are thought to increase riskfor BPD (Fonagy, Gergely, Jurist, & Target,2002; Holmes, 2004; Salzman, Salzman, &Wolfson, 1997).
Finally, the link between early separation andBPD cannot be attributed to schizotypal person-ality disorder symptoms, which were found to beassociated with early separations in this cohort(Anglin et al., 2008). Although borderline andschizotypal PD are correlated (Cohen et al.,2008; Kavoussi & Siever, 1992), they are never-theless distinct forms of personality pathology(Sanislow et al., 2002). These associations be-tween early separation and two distinct personal-ity disorders indicate that this developmentalrisk is not unique to BPD. Consistent with theprincipal of multifinality (Cicchetti & Rogosch,1996), early separations may lead to develop-mental trajectories associated with a wider rangeof psychopathology.
Associations between early separations anddistinct personality disorders or other forms ofmental illness may reflect different underlyingmechanisms. In fact, the association with theschizotypal symptom trajectory was limited tothose children who had both experienced theseearly separations and had high angry tempera-ment as assessed here at age 9 (Anglin et al.,2008), whereas in these data there were no iden-tifiedmoderating effects of other risks. Althoughmechanisms remain unclear, early separation incombination with an angry temperamentmay in-crease risk for the cognitive and perceptual dis-turbances that are more characteristic of schizo-typal pathology. Increased risk for BPD maybe more specifically linked with affect dysregu-lation. Future developmental investigations mayaid understanding of mechanisms of this risk byexamining early separation as a risk for other dis-orders (e.g., depression, anxiety, and disruptivebehavior disorders), alternative dimensionalconceptualizations of psychopathology (inter-nalizing and externalizing symptoms), or specifichigh-risk behaviors (e.g., suicide attempts).
Significance and Limitations
Perhaps it is most significant that early separa-tions had enduring effects on the develop-mental trajectory of BPD symptoms that wereindependent of a range of other risks that could
plausibly be outcomes of those early separa-tions. Some of these risks mediated the effectsof other risks but none accounted for the asso-ciation of early separation with failure to “ma-ture out of” BPD symptoms with age. Althoughit is noteworthy that this early experience hadsuch an enduring effect, we note no singlerisk is insufficient on its own to cause BPDand particularly look forward to the genetic in-formation now being gathered on this cohort todetermine its potential role in these develop-mental outcomes.
The longitudinal data in this study represent animportant strength. Early separations were re-ported by mothers when the children were stillyoung. Mothers also reported on childhood tem-perament when children were on average 9 yearsold and maternal characteristics and behaviorwhen children were on average 13.7 years old.As such, the developmental data here are unlikelyto be distorted by memory and reporting biasesassociated with self-reported data on childhoodgathered retrospectively from adults. Repeatedassessments of self-reported BPD symptomsalso provide a more reliable and probably morevalid measure of this personality disorder in ado-lescence and adulthood. All data were gatheredfrom two independent informants, mother andchild, in in-home or (rarely) telephone interviewsor (recently) on-line responses. Nevertheless, thedata do not include the structured observationsthat would strengthen the objectivity of assess-ments. Further, the principal investigator’s inter-est in a broad range of emotional/cognitive prob-lems and risks led to less intense assessment ofindividual variables than would usually charac-terize a cross-sectional or laboratory-based study.
Insofar as our attempt to understand themechanisms of early separation effects drawsheavily on attachment theory, it is limitedby its lack of any observational or interviewmeasure of attachment in the parent–child rela-tionship. Without such a measure, it remainsunclear whether attachment insecurity experi-enced in childhood mediates long-term associa-tion between early separation and subsequentBPD. Although inclusion of self-reported at-tachment scales provides relevant information,these measures focus on close relationships inadolescence and adulthood, and thus differfrom measures focusing on parent–child attach-
Early separations and borderline personality 1027

ment (Bartholomew & Shaver, 1998; Shaver &Mikulincer, 2004). At present, the causal direc-tion of effects linking self-reported attachmentand BPD symptoms is unclear; both may be in-fluenced by common interpersonal experience.New investigations of the long-term relationship
between early separation, childhood attachmentinsecurity, and adult BPD are needed and maybe more feasible now that a sufficient numberof children assessed with the Strange Situationprocedure have reached adulthood (Waters et al.,2000; Weinfeld, Sroufe, & Egeland, 2000).
References
Agrawal,H.R.,Gunderson, J.,Holmes, B.M.,&Lyons-Ruth,K. (2004). Attachment studies with borderline patients:A review. Harvard Review of Psychiatry, 12, 94–104.
American Psychiatric Association. (1980). Diagnostic andstatistical manual of mental disorders (3rd ed.). Wash-ington, DC: Author.
American Psychiatric Association. (1994). Diagnostic andstatistical manual of mental disorders (4th ed.). Wash-ington, DC: Author.
Anglin, D.M., Cohen, P. R., &Chen, H. (2008). Duration ofearly maternal separation and prediction of schizotypalsymptoms from early adolescence to midlife. Schizo-phrenia Research, 103, 143–150.
Bandelow, B., Krause, J., Wedekind, D., Broocks, A., Ha-jak, G., & Ruther, E. (2005). Early traumatic life events,parental attitudes, family history, and birth risk factorsin patients with borderline personality disorder andhealthy controls. Psychiatry Research, 134, 169–179.
Barry, R. A., Kochanska, G., & Philibert, R. A. (2008). G"E interaction in the organization of attachment:Mothers’ responsiveness as a moderator of children’sgenotypes. Journal of Child Psychology and Psychia-try, 49, 1313–1320.
Bartholomew, K., Kwong, M. J., & Hart, S. D. (2001). At-tachment. In W. J. Livesley (Ed.),Handbook of person-ality disorders (pp. 196–230). New York: GuilfordPress.
Bartholomew, K., & Shaver, P. R. (1998). Methods of as-sessing adult attachment: Do they converge? In J. A.Simpson & W. S. Rholes (Eds.), Attachment theoryand close relationships (pp. 25–45). New York: Guil-ford Press.
Belsky, J. (2002). Developmental origins of attachmentstyles. Attachment and Human Development, 4, 166–170.
Berenson, K. R., Crawford, T. N., Cohen, P., & Brook, J.(2005). Implications of identification with parents andparents’ acceptance for adolescent and young adultself-esteem. Self and Identity, 4, 289–301.
Bezirganian, S., Cohen, P., & Brook, J. (1993). The impactof mother–child interaction on the development of bor-derline personality disorder. American Journal of Psy-chiatry, 150, 1836–1842.
Bowlby, J. (1969).Attachment and loss: Vol. 1. Attachment.New York: Basic Books.
Bowlby, J. (1973). Attachment and loss: Vol. 2. Separation.New York: Basic Books.
Bowlby, J. (1980). Attachment and loss: Vol. 3. Loss, sad-ness, and depression. New York: Basic Books.
Bradley, S. J. (1979). The relationship of earlymaternal sep-aration to borderline personality in children and adoles-cents: A pilot study. American Journal of Psychiatry,136, 424–426.
Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult attachment: An integrative
approach. In J. A. Simpson & W. S. Rhodes (Eds.), At-tachment theory and close relationships (pp. 46–76).New York: Guildford Press.
Brennan,K.A.,&Shaver, P. R. (1998). Attachment styles andpersonality disorders: Their connection to each other andparental divorce, parental death, and perceptionof parentalcaregiving. Journal of Personality, 66, 835–878.
Bretherton, I., & Munholland, K. A. (1999). Internal work-ing models in attachment relationships: A construct re-visited. In J. Cassidy & P. R. Shaver (Eds.), Handbookof attachment: Theory, research, and clinical applica-tions (pp. 89–111). New York: Guilford Press.
Caspi, A., Sugden, K., Moffitt, T. E., Taylor, A., Craig, I.W., Harrington, H. L., et al. (2003). Influence of lifestress on depression: Moderation by a polymorphismin the 5-HTT gene. Science, 301, 386–389.
Charmandari, E., Kino, T., Souvatzoglou, E., & Chrousos,G. P. (2003). Pediatric stress: Hormonal mediators andhuman development.Hormone Research, 59, 161–179.
Chen, H., Cohen, P., Crawford, T. N., Kasen, S., Johnson, J.G., & Berenson, K. (2006). Relative impact of youngadult personality disorders on subsequent quality oflife: Findings of a community-based longitudinal study.Journal of Personality Disorders. 20, 510–523.
Chen, H., Cohen, P., Johnson, J. G., Kasen, S., Sneed, J. R.,& Crawford, T. N. (2004). Adolescent personality dis-orders and conflict with romantic partners during thetransition to adulthood. Journal of Personality Disor-ders, 18, 507–525.
Chess, S., & Thomas, A. (1978). Temperamental individu-ality from childhood to adolescence. Annual Progressin Child Psychiatry and Child Development, 223–244.
Cicchetti D., & Cohen D. (Eds.). (2006a). Developmentalpsychopathology: Vol. 1. Theory and method (2nd ed.).New York: Wiley.
Cicchetti D., & Cohen D. (Eds.). (2006b). Developmentalpsychopathology: Vol. 3. Risk, disorder, and adaptation(2nd ed.). New York: Wiley.
Cicchetti, D., & Rogosch, F. A. (1996). Equifinality andmultifinality in developmental psychopathology. De-velopment and Psychopathology, 8, 597–600.
Cohen, P. (1996). Childhood risks for young adult symp-toms of personality disorder: Method and substance.Multivariate Behavioral Research, 31, 121–148.
Cohen, P. (2008). Child development and personality disor-der. Psychiatric Clinics of North America, 31, 477–493.
Cohen, P., Chen, H., Gordon, K., Johnson, J., Brook, J., &Kasen, S. (2008). Socioeconomic background andthe developmental course of schizotypal and border-line personality disorder symptoms. Development andPsychopathology, 20, 633–650.
Cohen, P., & Cohen, J. (1996). Life values and adolescentmental health. Mahwah, NJ: Erlbaum.
Cohen, P., & Crawford, T. N. (2005). Developmental issues.In J. M. Oldham, A. E. Skodol, & D. S. Bender (Eds.),
T. N. Crawford et al.1028

Textbook of personality disorders (pp. 171–185). Wash-ington, DC: American Psychiatric Publishing.
Cohen, P., Crawford, T. N., Johnson, J. G., & Kasen, S.(2005). The Children in the Community Study of devel-opmental course of personality disorder. Journal ofPersonality Disorders, 19, 466–486.
Crawford, T. N., Cohen, P., Johnson, J. G., Kasen, S., First,M. B., Gordon, K., et al. (2005). Self-reported person-ality disorder in the Children in the Community sample:Convergent and prospective validity in late adolescenceand adulthood. Journal of Personality Disorders, 19,30–52.
Crawford, T. N., Cohen, P., Midlarsky, E., & Brook, J. S.(2001). Internalizing symptoms in adolescents: Genderdifferences in vulnerability to parental distress and dis-cord. Journal of Research on Adolescence, 11, 85–119.
Crawford, T. N., Shaver, P. R., Cohen, P., Pilkonis, P. A., Gil-lath, O., &Kasen, S. (2006). Self-reported attachment, in-terpersonal aggression, and personality disorder in a pro-spective community sample of adolescents and adults.Journal of Personality Disorders, 20, 331–353.
Davies, P. T., & Cummings, E. M. (1994). Marital conflictand child adjustment: An emotional security hypoth-esis. Psychological Bulletin, 116, 387–411.
Derogatis, L. R., Lipman, R. S., Rickles, K., Uhlenhuth, E.H., & Covi, L. (1974). The Hopkins Symptom Check-list (HSCL). Behavioral Science, 19, 1–15.
Fincham, F. D., & Osborne, L. N. (1993). Marital conflictand children: Retrospect and prospect. Clinical Psy-chology Review, 13, 75–88.
First, M. B., Gibbon, M., Spitzer, R. L., &Williams, J. B. W.(1997). Structured Clinical Interview for DSM-IVAxis IIpersonality disorders (SCID-II). Arlington, VA: Ameri-can Psychiatric Publishing.
Fonagy, P., Gergely, G., Jurist, E. L., & Target, M. (2002).Affect regulation, mentalization, and the development ofthe self. New York: Other Press.
Fox, N. A., Nichols, K. E., Henderson, H. A., Rubin, K.,Schmidt, L., Hamer, D., et al. (2005). Evidence for agene–environment interaction in predicting behavioralinhibition in middle childhood. Psychological Science,16, 921–926.
Garner, B., Chanen, A. M., Phillips, L., Velakoulis, D.,Wood, S. J., Jackson, H. J., et al. (2007). Pituitary vol-ume in teenagers with first-presentation borderline per-sonality disorder. Psychiatry Research, 156, 257–261.
George, C., Kaplan, N., & Main, M. (1985). The BerkeleyAdult Attachment Interview. Unpublished manuscript,University of California, Berkeley.
Gross, R., Olfson, M., Gameroff, M., Shea, S., Feder, A.,Fuentes, M., et al. (2002). Borderline personality disor-der in primary care. Archives of Internal Medicine, 162,53–60.
Heim, C., & Nemeroff, C. (2001). The role of childhoodtrauma in the neurobiology of mood and anxiety disor-ders: Preclinical and clinical studies. Biological Psy-chiatry, 49, 1023–1039.
Holmes, J. (2004). Disorganized attachment and borderlinepersonality disorder: A clinical perspective. Attachmentand Human Development, 6, 181–190.
Hyler, S. E., Rieder, R., Spitzer, R., & Williams, J. (1982).The Personality Diagnostic Questionnaire (PDQ).New York: New York State Psychiatric Institute.
Hyler, S. E., Skodol, A. E., Kellman, H. D., Oldham, J. M.,& Rosnick, L. (1990). Validity of the Personality Diag-nostic Questionnaire—Revised: Comparison with twostructured interviews. American Journal of Psychiatry,47, 1043–1048.
Jessor, R., Graves, T. D., Hanson, R. C., & Jessor, S. L.(1968). Society, personality, and deviant behavior: Astudy of a tri-ethnic community. NewYork:Holt, Rinehart& Wilson.
Johnson, J. G., Cohen, P., Kasen, S., Skodol, A., & Brook,J. (2000). Age-related change in personality disordertrait levels between early adolescence and adulthood:A community-based longitudinal investigation. ActaPsychiatrica Scandinavica, 102, 265–275.
Johnson, J. G., Cohen, P., Kasen, S., Ehrensaft, M. K., &Crawford, T. N. (2006). Associations of parental per-sonality disorders and Axis I disorders with childrearingbehavior. Psychiatry: Interpersonal and BiologicalProcesses, 69, 336–350.
Kaufman, J., Yang, B., Douglas-Palumberi, H., Grasso, D.,Lipschitz, D., Houshyar, S., et al. (2006). Brain-derivedneurotrophic factor–5-HTTLPR gene interactions andenvironmental modifiers of depression in children. Bio-logical Psychiatry, 59, 673–680.
Kaufman, J., Yang, B., Douglas-Palumberi, H., Houshyar,S., Lipschitz, D., Krystal, J. H., et al. (2004). Social sup-ports and serotonin transporter gene moderate depres-sion in maltreated children. Proceedings of the NationalAcademy of Sciences of the United States of America,101, 17316–17321.
Kavoussi, R. J., & Siever, L. J. (1992). Overlap betweenborderline and schizotypal personality disorders. Com-prehensive Psychiatry, 33, 7–12.
Lenzenweger, M., Loranger, A., Korfine, L., & Neff, C.(1997). Detecting personality disorders in a nonclinicalpopulation: Application of a 2-stage for case identifica-tion. Archives of General Psychiatry, 54, 345–351.
Levy, K. N. (2005). The implications of attachment theoryand research for understanding borderline personality dis-order. Development and Psychopathology, 17, 959–986.
Lieb, K., Rexhausen, J. E., Kahl, K. G., Schweiger, U., Phil-ipsen, A., Hellhammer, D. H., et al. (2004). Increaseddiurnal salivary cortisol in women with borderline per-sonality disorder. Journal of Psychiatric Research, 38,559–565.
Links, P. S., Steiner, M., Offord, D. R., & Eppel, A. B.(1988). Characteristics of borderline personality disor-der: ACanadian study.Canadian Journal of Psychiatry,33, 336–340.
Maughan, B., Pickles, A., & Quinton, D. (1995). Parentalhostility, childhood behavior and adult social function-ing. In J. McCord (Ed.), Coercion and punishment inlong term perspectives (pp. 34–58). New York: Cam-bridge University Press.
Maughan, B., & Rutter, M. (1997). Retrospective reportingof childhood adversity: Issues in assessing long-term re-call. Journal of Personality Disorders, 11, 19–33.
McGlashan, T. (1986). The Chestnut Lodge Follow-UpStudy, Part III: Long-term outcome of borderline per-sonalities. Archives of General Psychiatry, 42, 20–30.
Mikulincer, M., & Shaver, P. R. (2007). Attachment in adult-hood: Structure, dynamics, and change. NewYork: Guil-ford Press.
Modestin, J., Ern, T., & Oberson, B. (1998). A comparisonof self-report and interview diagnoses of DSM-III-Rpersonality disorders. European Journal of Personality,12, 445–455.
Moss, E., Cyr, C., Bureau, J.-F., Tarabulsy, G. M., &Dubois-Comtois,K. (2005).Stabilityof attachment during thepre-school period. Developmental Psychology, 41, 773–783.
Paris, J., Brown, R., & Nowlis, D. (1987). Long-term fol-low-up of borderline patients in a general hospital.Comprehensive Psychiatry, 28, 530–535.
Early separations and borderline personality 1029

Paris, J., Zweig–Frank,H.,&Guzder, J. (1994). Psychologicalrisk factors for borderline personality disorder in femalepatients. Comprehensive Psychiatry, 35, 301–305.
Reich, B., & Zanarini, M. C. (2001). Developmental as-pects of borderline personality disorder. Harvard Re-view of Psychiatry, 9, 294–301.
Robins, L. N., Schoenberg, S. P., Holmes, S. J., Ratcliff, K.S., Benham, A., & Works, J. (1985). Early home envi-ronment and retrospective recall: A test for concordancebetween siblings with and without psychiatric disor-ders. American Journal of Orthopsychiatry, 55, 27–41.
Rothbart, M. K., Ahadi, S. A., Hershey, K. L., & Fisher, P.(2001). Investigations of temperament at three to sevenyears: The Children’s Behavior Questionnaire. ChildDevelopment, 72, 1394–1408.
Rutter, M., & Sroufe, L. A. (2000). Developmental psycho-pathology: Concepts and challenges. Development andPsychopathology, 12, 265–296.
Salzman, J. P., Salzman, C., & Wolfson, A. N. (1997). Re-lationship of childhood abuse and maternal attachmentto the development of borderline personality disorder.In M. C. Zanarini (Ed.), Role of sexual abuse in theetiology of borderline personality disorder (pp. 71–91).Washington, DC: American Psychiatric Press.
Sanislow, C. A., Morey, L. C., Grilo, C. M., Gunderson, J.G., Shea, M. T., Skodol, A. E., et al. (2002). Confirma-tory factor analysis of DSM-IV borderline, schizotypal,avoidant and obsessive–compulsive personality disor-ders: Findings from the Collaborative Longitudinal Per-sonality Disorders Study. Acta Psychiatrica Scandina-vica, 105, 28–36.
Schaefer, E. (1965). Children’s reports of parental behavior:An inventory. Child Development, 36, 413–424.
Shaver, P. R., & Mikulincer, M. (2002). Attachment-relatedpsychodynamics. Attachment and Human Development,4, 133–161.
Shaver, P. R., &Mikulincer, M. (2004).What do self-reportattachment measures assess? In W. S. Rholes & J. A.Simpson (Eds.), Adult attachment: Theory, research,and clinical implications (pp. 17–54). New York: Guil-ford Press.
Shea, M. T., Stout, R., Gunderson, J., Morey, L. C., Grilo,C. M., McGlashan, T., et al. (2002). Short-term diag-nostic stability of schizotypal, borderline, avoidant,and obsessive–compulsive personality disorders. Amer-ican Journal of Psychiatry, 159, 2036–2041.
Siever, L. J., & Davis, K. L. (1991). A psychobiologicalperspective on the personality disorders. AmericanJournal of Psychiatry, 148, 1647–1658.
Smith, S. M., & Vale, W. W. (2006). The role of the hypo-thalamic–pituitary–adrenal axis in neuroendocrine re-sponses to stress. Dialogues in Clinical Neuroscience,8, 383–395.
Skodol, A. E., & Bender, D. S. (2003). Why are women di-agnosed borderline more than men? Psychiatric Quar-terly, 74, 349–360.
Skodol, A. E., Gunderson, J. G., Livesley, W. J., Pfohl, B.,Siever, L. J., & Widiger, T. A. (2002). The borderlinediagnosis from the perspectives of psychopathology,comorbidity, personality structure, biology, genetics,and course. Biological Psychiatry, 51, 936–950.
Soloff, P. H., &Millward, J. W. (1983). Developmental his-tories of borderline patients.Comprehensive Psychiatry,24, 574–588.
Solomon, J., & George, C. (1999). Attachment disorganiza-tion. New York: Guilford Press.
Stalker, C. A., & Davies, F. (1995). Attachment organiza-tion and adaptation in sexually-abused women. Cana-dian Journal of Psychiatry, 40, 234–240.
Stone, M. H., Hurt, S. W., & Stone, D. K. (1987). The P.I.-500: Long-term follow-up of borderline inpatientsmeeting DSM-III criteria: I. Global outcome. Journalof Personality Disorders, 1, 291–298.
Suomi, S. J. (2006). Risk, resilience, and Gene"Environ-ment interactions in rhesus monkeys. Annals of theNew York Academy of Sciences, 1094, 52–62.
Tarullo, A. R., & Gunnar, M. R. (2006). Child maltreatmentand the developing HPA axis.Hormones and Behavior,50, 632–639.
Thomas, A., & Chess, S. (1977). Temperament and devel-opment. Oxford: Brunner/Mazel.
Thomas, A., Chess, S., & Birch, H. G. (1970). The origin ofpersonality. Scientific American, 223, 102–109.
Thomas, A., Chess, S., &Korn, S. J. (1982). The reality of dif-ficult temperament.Merrill–Palmer Quarterly, 28, 1–20.
Torgersen, S., Kringlen, E., & Cramer, V. (2001). The prev-alence of personality disorders in a community sample.Archives of General Psychiatry, 58, 590–596.
Van Voorhees, E., & Scarpa, A. (2004). The effects of childmaltreatment on the hypothalamic–pituitary–adrenalaxis. Trauma Violence and Abuse, 5, 333–352.
Waters, E., Merrick, S., Treboux, D., Crowell, J., & Alber-sheim, L. (2000). Attachment security in infancy andearly adulthood: A twenty-year longitudinal study.Child Development, 71, 684–689.
Weinfeld, N. S., Sroufe, L. A., & Egeland, B. (2000). At-tachment from infancy to early adulthood in a high-risk sample: Continuity, discontinuity, and their corre-lates. Child Development, 71, 695–702.
Winograd, G., Cohen, P., & Chen, H. (2008). Adolescentborderline symptoms in the community: Prognosis forfunctioning over 20 years. Journal of Child Psychologyand Psychiatry, 49, 933–941.
Zanarini, M. C., Yong, L., Frankenburg, F. R., Hennen, J.,Reich, D. B., Marino, M. F., & Vujanovic, A. A. (2002).Severity of reported childhood sexual abuse and its rela-tionship to severity of borderline psychopathology andpsychosocial impairment among borderline inpatients.Journal of Nervous and Mental Disease, 190, 381–387.
T. N. Crawford et al.1030
Related Documents











