Psychopathology: Theory and Practice Borderline Personality Disorder The term - Borderline Personality Disorder - has a long history, dating back to 1938 and Adolf Stern's definitive paper (although it has recently been supplanted in the psychiatric field by the term Emotionally Unstable Personality Disorder). In this lecture, Marcus West will be tracing some of the ways the concept has been understood in both psychiatric and analytic fields, particularly focusing on Kernberg's and Fonagy's conceptualisations and contemporary attachment and trauma theories, which have afforded us further, and now widely accepted, ways of looking at the phenomena. West will explore the overlap between borderline and narcissistic organisations and ways of functioning, before focusing on the powerful and profoundly distressing clinical phenomena as they occur in the consulting room, understood primarily as sometimes near-unbearable (for both patient and analyst) co-constructions in the analytic relationship of early relational trauma. The clinical challenges, as well as the opportunities, opened up by these co-constructions will be explored using, amongst other things, a developed understanding of Jung's concept of the traumatic complex.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Psychopathology: Theory and Practice
Borderline Personality Disorder
The term - Borderline Personality Disorder - has a long history, dating back
to 1938 and Adolf Stern's definitive paper (although it has recently been
supplanted in the psychiatric field by the term Emotionally Unstable
Personality Disorder). In this lecture, Marcus West will be tracing some of
the ways the concept has been understood in both psychiatric and analytic
fields, particularly focusing on Kernberg's and Fonagy's conceptualisations
and contemporary attachment and trauma theories, which have afforded
us further, and now widely accepted, ways of looking at the phenomena.
West will explore the overlap between borderline and narcissistic
organisations and ways of functioning, before focusing on the powerful and
profoundly distressing clinical phenomena as they occur in the consulting
room, understood primarily as sometimes near-unbearable (for both
patient and analyst) co-constructions in the analytic relationship of early
relational trauma. The clinical challenges, as well as the opportunities,
opened up by these co-constructions will be explored using, amongst
other things, a developed understanding of Jung's concept of the traumatic
complex.

Marcus WestNovember 7th 2019; 19.30 - 21.30
The October Gallery, 24 Old Gloucester Street, London WC1N 3AL
Psychopathology: Theory and Practice
Borderline Personality Disorder

Plan for the talk
• Main aim: To make the phenomena understandable, give a sense of the difficulties and challenges and how to address them
• An overview of how the different psychopathologies fit together
• The history of the borderline concept, concentrating on Stern, Kernberg and Fonagy
• How this is related to trauma and early relational trauma in particular - calling on Jung’s concept of the traumatic complex
• How the analyst is deeply involved in the process too - the co-construction of the relationship, the particular pressures, idealisation, the analyst’s role / process / development
• Working through - both the ‘borderline’ dynamics and the underlying, primitive narcissistic defences
• Current treatment modalities

Overview of theoretical constructs:
Narcissism & Borderline
How do the concepts fit together?

Narcissism - broad and narrow definitions
• Narcissistic personality organisation
• Bollas: ‘oblates the difference between self and other’ (2000 p. 8);
• “I am right, you must change” - the fight response
• Schizoid personality organisation
• Bollas: “the mind becomes the fundamental object of dependence … (they)
dread emotional experience” (p. 10);
• “I am good, don’t challenge me”; the flight response
• Borderline personality organisation
• Bollas: “seeks out turbulence, turning molehills into mountains and escalating
irritations into global states of rage” (p. 9);
• ‘frozen’ to bad experience; “you must pick up the pieces or you don’t care”
• Hysterical personality organisation
• Bollas: “(they) suspend the self’s idiom in order to fulfil the primary object’s
desire” (p. 12);
• the collapse response: “You don’t want me to be - care for my baby self”

Broad & narrow definitions of narcissism &
borderline
• Broad definition of narcissism: all these personality organisations
are forms of narcissistic defence as they are attempts to defend
the self against narcissistic wounding
• vs. Narrow definition: the narcissistic personality organisation
(the classical understanding of narcissism)
• Broad definition of borderline:‘where ego-functioning and relating
are disrupted and there is a preponderance of primary process
functioning’ ‒ or impaired reflective function and mentalization in
Fonagy's (1991) terms
• vs. Narrow definition: the borderline personality organisation

Borderline personality organisation
The clinical picture

Destructiveness, self-destructiveness and self-harm
• Why does someone behave so self-destructively and against their apparent best interests? Why are they bitter, full of rage, dissatisfied, unappreciative and so difficult to help? Why do they have angry outbursts and blame others, continually getting into trouble? Why can’t they contain themselves? Why do they attempt to harm themselves though cutting, drugs or alcohol
Hopeless, despairing and depressed
• Why do they remain convinced that there’s no hope, no pleasure or meaning in life and that it is not worth living? Why do they want to kill themselves so persistently? … and what’s going on in the dynamics around it?
Not getting better
• Why don't they get better? Why don't they just get on with their lives and 'get over it’? Why don’t they respond to reason and interpretation or behave reasonably? Why do they remain so regressed for so long?
Issues in therapy
• Why do they say that “you don’t care” when you have bent over backwards to help? Why are they furious when you can’t offer a changed session time, so that you dread having to bring it up? Why do you feel at the same time concerned, despairing, furious, and at your wits’ end?
Some elements of the clinical picture

The borderline concept

Adolf Stern (1938) - 10 main features:
1. “narcissism” due to a “deficiency of spontaneous maternal affection” which thus led to
“affective narcissistic malnutrition”
2. “psychic bleeding”- complete psychic collapse when the individual encounters pain
and trauma
3. “inordinate hypersensitivity”
4. “rigid personality” - he described both psychic and bodily rigidity
5. “negative therapeutic reactions”
6. “constitutionally rooted feelings of inferiority deeply embedded in the personality”
7. “masochism and self-pity”
8. “a deep, organic insecurity and anxiety” which leads to “extreme and clinging
dependency”
9. the use of projection, for example, a paranoid experience of a hostile environment
10. “difficulties in reality testing”, particularly in personal relationships.

Borderline Personality Disorder - DSM V (2011)
Significant impairments in personality functioning manifest by:
• 1. Impairments in self functioning (a or b):
a. Identity: Markedly impoverished, poorly developed, or unstable self-image, often
associated with excessive self- criticism; chronic feelings of emptiness; dissociative
states under stress.
b. Self-direction: Instability in goals, aspirations, values, or career plans.
• AND
• 2. Impairments in interpersonal functioning (a or b):
a. Empathy: Compromised ability to recognize the feelings and needs of others
associated with interpersonal hypersensitivity (i.e., prone to feel slighted or insulted);
perceptions of others selectively biased toward negative attributes or vulnerabilities.
b. Intimacy: Intense, unstable, and conflicted close relationships, marked by mistrust,
neediness, and anxious preoccupation with real or imagined abandonment; close
relationships often viewed in extremes of idealization and devaluation and alternating
between over involvement and withdrawal.

Pathological personality traits in the following domains:
• 1. Negative Affectivity, characterized by:
a. Emotional lability: Unstable emotional experiences and frequent mood
changes; emotions that are easily aroused, intense, and/or out of proportion to
events and circumstances.
b. Anxiousness: Intense feelings of nervousness, tenseness, or panic, often
in reaction to interpersonal stresses; worry about the negative effects of past
unpleasant experiences and future negative possibilities; feeling fearful,
apprehensive, or threatened by uncertainty; fears of falling apart or losing
control.
c. Separation insecurity: Fears of rejection by – and/or separation from –
significant others, associated with fears of excessive dependency and
complete loss of autonomy
d. Depressivity: Frequent feelings of being down, miserable, and/or
hopeless; difficulty recovering from such moods; pessimism about the future;
pervasive shame; feeling of inferior self-worth; thoughts of suicide and suicidal
behavior.

Pathological personality traits in the following domains:
• 2. Disinhibition, characterized by:
a. Impulsivity: Acting on the spur of the moment in response to
immediate stimuli; acting on a momentary basis without a plan or
consideration of outcomes; difficulty establishing or following plans; a
sense of urgency and self-harming behavior under emotional distress
b. Risk taking: Engagement in dangerous, risky, and potentially self-
damaging activities, unnecessarily and without regard to consequences;
lack of concern for one‟s limitations and denial of the reality of personal
danger.
• 3. Antagonism, characterized by:
Hostility: Persistent or frequent angry feelings; anger or irritability in
response to minor slights and insults.

Otto Kernberg (1975)
• ‘Identity diffusion’ and a ‘characteristic ego pathology’:
• ‘ego weakness’ – lack of anxiety tolerance, impulse
control, capacity for enjoyment or creative
achievement
• ‘identity diffusion’: ‘a psychological structure
composed of multiple split-off object relations,
positive and negative, each reflecting a dyadic unit of
a self-representation, an object-representation and a
dominant affect linking them’ (2008, p. 603)
• splitting, idealization, projection, projective
identification, denial & omnipotence

Trauma related models

• 87 % of subjects with borderline personality disorder
had histories of severe childhood abuse and/or neglect
starting prior to age 7
• “borderline personality disorder significantly overlaps
with what Herman has termed complex post-traumatic
stress disorder (complex PTSD)”
• Confirmed by Battle et al. (2004) in a study of 600
adults with personality disorder showing ‘a clear link
with childhood maltreatment’
Herman, Perry and van der Kolk ‘Childhood trauma in borderline personality
disorder’ (1989)

Peter Fonagy - developing views on borderline phenomena
• Fonagy (1991): the difficulty in thinking about oneself or
others - the person cannot bear to think about what is in
the mind of the other - e.g., too painfully negative, critical,
hateful, uncaring, or murderous
• Fonagy, Gergely, Jurist, & Target (2002): early attachment
patterns & the parents' inability to think about their child as
an individual in their own right - their ability to mentalize
• relates specifically to disturbances of borderline
psychology

Liotti, disorganised attachment & borderline functioning
“The attachment and defence systems normally operate in harmony as exemplified in flight from the source of fear to find refuge in proximity to the attachment figure. However, where the caregiver is at the same time the source and the solution of the infant's fear, there is a clash” (Liotti, 2004a,b)
• To flee or to attach? - the disorganised attachment pattern - "fright without solution" (Liotti, 2007, p. 129)
• disorganised attachment - “severe dissociation, splitting among ego states, and fragmentation of the self” - borderline functioning (ibid., p. 130)

Outline understanding of ‘borderline’ states of mind
Behaviour linked to early traumatic experiences that are embodied in trauma-related complexes (experiences that were unbearable for the psyche at that time)
We all have complexes, however:
when we can mostly get round them and behave in a creative, functional way but are sometimes taken over and affected -neurotic states of mind
when the complexes dominate the ego-complex and disrupt the development of the ego - borderline states of mind
typically when the person’s fundamental expression of need and distress was aversive to the parents

Integrating trauma, relational & analytic
theory and practice

• The bad history of trauma and analytic theory
• van der Kolk - “repetition compulsion”
• Freud's seduction theory
• Ferenczi
• Klein
• Jung
Trauma theory (in brief)
and early relational trauma

Understanding Freud's & Klein's responses
• empathy alone does not work - confirming the position of
'victim'
• contemporary trauma theory & lack of coherent memory of
the trauma
• counter-reactions to traumatic experience embedded /
implicit relatedness vs. innate destructiveness
• analyst becomes frustrated, blames the patient, or deems
them unanalysable

The lost / murdered child metaphor
- not intentional nor ‘resistance’
• Freud: the negative therapeutic reaction - 'not
getting better' - due to the patient's attempt to prove
their superiority over their analyst (1923b), or
masochism (1924c), or the death instinct (1937c)
• the person is staying true to (and is bound to) their
core, traumatic experience
• the person is not going to ‘get better’ until the
traumatic experience (the lost / murdered child)
has been thoroughly recognised, addressed and
worked through

Trauma theory - origins
• Charcot at Salpêtrière Hospital in Paris : ‘nervous shocks’ underlie hysteria [dissociative, conversion, somatisation, bpd, ptsd]
• Janet: traumatic event - vehement emotion - dissociation - memory traces remain in the form of 'fixed ideas' {woman with curious jump}
• dissociated elements not integrated with personality, individuals 'attached' to the trauma, personalities cannot enlarge
• the mind works in two ways:
• a: ‘to preserve & reproduce the past’
• b. directed toward ‘synthesis & creation’ (integration)

Vietnam, feminist perspective & trauma theory
• PTSD & sexual abuse
• PTSD - disturbing recurrent flashbacks, avoidance or numbing of
memories of the event, and hyperarousal, which persist for more than
a month after the traumatic event, resulting in “significant distress or
impairment of major domains of life activity” (DSM)
• Complex PTSD (Herman), developmental trauma (van der Kolk)
• Herman, Perry & van der Kolk (1989)
• Fonagy (1991)
• Bowlby and relational psychoanalysis
• Adverse Childhood Experiences Study

Adverse Childhood Experience Study - 17,421 individuals

Adverse Childhood Experience Study - 17,421 individuals
1. physical abuse
2. sexual abuse
3. emotional abuse
4. physical neglect
5. emotional neglect
6. parents divorced
7. mentally ill
8. addicted
9. in prison
10. mother treated violently
• Those with a score of 4 points or more:
• 50% had learning or behavioural problems at school
• 66% of women, 35% of men - later life depression
• Alcoholism 7 times more likely than score of zero
• Those with score of 6 points or more:
• 4,600 % more likely to have IV drug use
• 15% chance of currently suffering one of the 10
leading causes of death: pulmonary disease, heart
disease, liver disease, obesity, diabetes, stroke …
• 50% more likely to have cancer
• 4 times more likely to have emphysema

The Hidden Epidemic
• Reduce depression by over 50%
• Reduce alcoholism by 66%
• Reduce suicide, IV drug use & domestic violence by 75%
• Improve workplace performance +++
• Vastly decrease the need for imprisonment

The Hidden Epidemic
The Adverse Childhood Experience Study (Felitti)
“(the researchers) realised they had stumbled upon the gravest and most costly public health issue in the United States: child abuse. (They) calculated that its overall costs exceeded those of cancer and heart disease and that eradicating child abuse in America would reduce the overall rate of depression by more than half, alcoholism by two-thirds, and suicide, IV drug use, and domestic violence by three-quarters. It would also have a dramatic effect on workplace performance and vastly decrease the need for incarceration.”
“When the Surgeon General’s report on smoking and health was published in 1964, it unleashed a decades-long legal and medical campaign that has changed daily life and long-term health prospects for millions. The number of American smokers fell from 42 percent of adults in 1965 to 19 percent in 2010, and it is estimated that nearly 800,000 deaths from lung cancer were prevented between 1975 and 2000.”
“The Adverse Childhood Experience Study, however, has had no such effect. Follow-up studies have appeared … only now (these effected children) receive high doses of psychotropic agents, which makes them more tractable but which also impairs their ability to feel pleasure and curiosity, to grow and develop emotionally and intellectually, and to become contributing members of society.”
Bessel van der Kolk, The Body Keeps the Score, p. 148

Trauma theory
• Definition of trauma = that which the psyche cannot cope with at that
moment in time - can't integrate with ego-functioning
"Janet proposed that intense arousal ("vehement emotion") seems to
interfere with proper information processing and the storage of
information in narrative (explicit) memory ... (so that) memories of trauma
may have no verbal (explicit) component whatsoever. Instead, the
memories may have been organised on an implicit or perceptual level,
without any accompanying narrative about what happened" (van der Kolk
1996b, p. 286-7)
• Disruption of ego-functioning: no coherent narrative - trauma
“disrupts individuals' capacity to perceive, represent, integrate, and
act on internal and external stimuli”(van der Kolk, McFarlane & Weisaeth 1996, p. x)
• vs. resistance & intention

Dissociated traumatic elements & the
disruption of ego-functioning
Traditional psychoanalytic view:
• "the borderline feels that his or her core object is to be found only through
turbulent states of mind. Unconsciously, therefore, the borderline
character seeks out turbulence, turning molehills into mountains,
and escalating irritations into global states of rage" (Bollas, 2000, p. 9)
• Vs. powerful affective-somatic reactions - flashbacks - form core
elements of the transference e.gs. being kept waiting, non-
responsiveness, asking questions, irritating the other
• regression and dissociation - the disruption of ego-functioning = dissociated
from everyday, well-adapted functioning
• subjectively, experiences feel more powerful, more intense, more terrible,
more certain, more spontaneous / impulsive, more true, more real …

The triune brain & the polyvagal theory

Narcissism - broad and narrow definitions
• Narcissistic personality organisation
• Bollas: ‘oblates the difference between self and other’ (2000 p. 8);
• “I am right, you must change” - the fight response
• Schizoid personality organisation
• Bollas: “the mind becomes the fundamental object of dependence … (they)
dread emotional experience” (p. 10);
• “I am good, don’t challenge me”; the flight response
• Borderline personality organisation
• Bollas: “seeks out turbulence, turning molehills into mountains and escalating
irritations into global states of rage” (p. 9);
• ‘frozen’ to bad experience; “you must pick up the pieces or you don’t care”
• Hysterical personality organisation
• Bollas: “(they) suspend the self’s idiom in order to fulfil the primary object’s
desire” (p. 12);
• the collapse response: “You don’t want me to be - care for my baby self”

The window of tolerance
• Daniel Siegal (1999) due to hyper- and hypo-arousal - therapy needs to be conducted within the 'window of tolerance' to allow the individual to process the traumatic experience
• Ogden, Minton & Pain: 'therapists must consistently employ techniques facilitating interactive repair to keep clients' arousal within a window of tolerance' (2006, p. 61)
• recognising the somatic cues for when the trauma is being triggered e.g., critical parent (tension in shoulders, shortness of breath, increased heart rate) - response (measured deep breaths, maintaining eye contact, grounding in chair)
• other examples - grounding, not addressing the traumatic memories until the individual is ready - a steady sympathetic presence

Peter Levine & the polar bear‘incompleted action tendencies’ of fight, flight, freeze or collapse
'Long after the original traumatic events are over, many
individuals find themselves compelled to anticipate, orient to, and
react to stimuli that directly or indirectly resemble the original
traumatic experience or its context'. (2006, p. 65)

• Due to repeated triggering the
amygdala - the brain’s smoke
detector - in a state of high alert
• Orbitofrontal systems - deal with
self-control and rational thought -
less activated due to repeated
trauma
• Alexander McFarlane' study of
Australian combat veterans
• Difficulty with self-soothing and
inhibition of fear activation by
amygdala
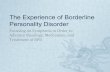
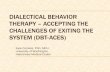
The Impact of Trauma on the BrainCozolino (2002)

The Impact of Trauma on the BrainBessel van der Kolk - The Body Keeps the Score (2014)
Trauma triggered in brain scanner
van der Kolk et al. (1994)
Emotional / limbic system, centred on
the amygdala
Visual cortex -
associated with
visual flashbacks
Marked decrease in
Broca's area - speech
- speechless terror

Dorsolateral prefrontal cortex - links past, present & future & gives a sense of continuity -
goes OFFLINE - feel something will last forever
Thalamus - integrates bits of experience into a coherent story - goes OFFLINE
The midline structures of the brain - your deeper sense of yourself - CAN be accessed
(LeDoux)
+ve & -ve experiences never integrated in orbitofrontal systems
The Impact of Trauma on the BrainBessel van der Kolk - The Body Keeps the Score (2014)
DissociatedDorsolateral prefrontal cortex Thalamus

EMDR & Adaptive Information Processing
theory - Shapiro (2001)
• the cause of the current problem is unprocessed memories of
traumatic experiences - dysfunctionally stored memories
• this manifests in the present when associated situations and
experiences trigger responses similar to earlier experiences that
have been dysfunctionally stored
• it is maintained in the present because other memory networks where
information is stored which would enable more adaptive resolution of
the past experience are not being accessed
• the personal meaning of these memories, or ‘touchstone events’,
become the lens through which we view ourselves in the present
• EMDR & memory channels - free association - the trauma complex

Early relational trauma

The failure to repair mismatches & the
negative affective core - Ed Tronick
• Tronick and Gianino (1986): a “mismatch” causes distress
• infant or mother try to repair the mismatch
• infant successful in repairing the mismatches - they “experience
positive emotions and establish a positive affective core”
• sense of agency is enhanced, and they "internalize a pattern of
interaction that they bring to interactions with others"
• unsuccessful in repairing mismatches - feel helpless, focus
behaviour on self-regulation, limit their engagement with others,
and “establish a negative affective core” (p. 156).

Beebe & Lachmann - The Origins of Attachment(2013)
Studied infants at 4 months who would go on to be classified as having a disorganised attachement pattern at 1 year; they observed (2013, p. 63):
• mother greeting distressed infant with smile
• infant jerked their body while turning away in the chair -"could be considered a precursor of 'fight-flight' "
• mother poked and pushed her infant's face
• infant did not move at all, other than blink - "moments of freezing"
• after multiple maternal intrusions, looming, pulling infant's arm to orient him after he'd turned away
• infant collapsed like a ragdoll

Trauma & relational psychoanalysis‘In the Shadow of the Tsunami’ Bromberg (2011)
• Philip Bromberg: trauma is when self-invalidation or self-annihilation by another is inescapable, and the mind is flooded by powerful affects that disrupt the individual’s capacity to think
• these “precipitous psychological events ... disrupt the patterns of meaning that constitute the person's overarching experience of self”
(the normal multiplicity of self-states are unlinked so that the person's normal sense of self is disrupted)
• “the process of psychoanalysis is about helping patients reclaim their dissociated self-states”

Understanding & working with the traumatic
complex

Jung's word association experiments &
the complex
• 100 words: bread, table, war, ink, love, dog, head, faithful, water, stroke, lamp ...
• delayed, emotion-laded or peculiar responses
"A 'feeling-toned complex' ... is the image of a certain psychic situation which is strongly accentuated emotionally and is, moreover, incompatible with the habitual attitude of consciousness. ... [I]t has ... a relatively high degree of autonomy, so that it is subject to the control of the conscious mind to only a limited extent, and therefor behaves like an animated foreign body in the sphere of consciousness" (Jung 1934, para. 201)

The trauma was and remains unbearable
• Right from the start of therapy the patient is telling you, explicitly &/or
implicitly, what they find unbearable in the world and themselves … their
complexes … often it is they themselves that feel unbearable
• what is going to be your attitude to this?
• The patient is watching to see what you will do. Will you say:
• “you are not really like that?” or
• “the world is not really like that” or
• “I am not like that, and it won’t be like that here?”
• or will you help the person face the traumatic complexes and work them
through recognising that they will likely recur in some form in the analytic
relationship?
• Retraumatisation - violation - fury, hatred & murderousness

Idealisation
• idealisation - the wish for an ideal, conflict-free world where there
will be no possibility of re-traumatisation
• a universal(?), very powerful phenomenon inevitably and
understandably associated with trauma
“Acknowledging the impossibility of bringing this fantasy [of a
new and idealized, compensatory childhood] to realization
represents a betrayal of [the patient’s] most sacred inner self”
(Davies & Frawley, 1992a, p. 25)
• will the therapist try to be the ideal, good, rescuer?
• will describe later the immense difficulties this can cause …

Reconstruction, re-enactment &
the subtle effects of co-construction
• Reconstruction - contentious … ?
• Why are we so affected by our patients and drawn into these
dynamics?
• still unbearable - threat of re-traumatisation
• internal working models held in implicit memory deeply
embedded in the person’s personality
• intense negative transference, where the therapist is
experienced as cold, cruel, inhuman or sadistic
• We need to be drawn in in so far as we can then recognise the
dynamic

The complex - the site of the traumatic reaction -
‘contains’
1. Overpowering affective-somatic response - the
disruption of ego-functioning
“intense arousal interferes with proper information
processing and the storage of information in narrative
(explicit) memory”
“bad”, “useless”,
“unwanted”, “unlovable”,
shame

Dissociated from core self
2. Unbearable core traumatic experience - can't bear to be
who you are, but which you have to recognise you 'are' - self-
attack & envy
• the person is at odds with themselves, feels they are
wrong, can’t bear their feelings or responses, become
alienated from their core self and readily falls into envying
others, through either idealising others or denigrating
themselves or both
“bad”, “useless”,
“unwanted”, “unloved”,
shame

Primitive defensive reactions
3. primitive defensive reactions - fight, flight, freeze, collapse -not well-adapted
• combative, fight response
• avoidant, flight response
• despairing, frozen-to-the-bad response
• submissive, collapse, helpless response
• hypervigilant, anxious response
“bad”, “useless”,
“unwanted”, “unloved”,
shame

Conflict compromises identity & functioning
4. an (unconscious) talion response to the traumatiser/aggressor/abuser
• represents an identification with the aggressor, usually anathema, usually projected, binding the individual to the bad object
• (unconsciously) being themselves critical, shaming, bullying
• requires extreme sensitivity in interpreting this (eventually)
• the problem when people avoid identification with the aggressor -e.g., they 'need' to be more critical, selfish, blaming etc.
“bad”, “useless”,
“unwanted”, “unloved”,
shame

Trauma-related internal working models
5. Trauma-related internal working models are
embodied in the complex (Knox 1999)
• held in implicit / procedural memory
• “I am bad, unwanted, useless, and unloveable - the
world is critical and will reject me”, that is how
things work
“bad”, “useless”,
“unwanted”, “unloved”,
shame

Direct & reversed forms on different levels
- a pattern which can be applied in different ways
“I am bad - the world is critical and will reject me”
• objective level (current & historical)
• subjective level (interior)
• transference level (relational)
• archetypal level (this is the way things are / the way the world
works)
• direct & reversed forms - beyond the ‘victim’ position
• needs to be worked through on all levels

The analytic relationship

Bromberg (2011) The Shadow of the Tsunami
- the value of reliving
“the analytic relationship become[s] a place that supports
risk and safety simultaneously ‒ a relationship that allows
the painful reliving of early trauma, without the reliving
being just a blind repetition of the past.”
“It is optimally a relationship that I have described as ‘safe
but not too safe’… by which I mean that the analyst is
communicating both his ongoing concern for his patient's
affective safety and his commitment to the value of the
inevitably painful process of reliving.” (p. 16-17)

"The therapeutic effect comes from the doctor's efforts
to enter into the psyche of his patient, thus establishing
a psychologically adapted relationship. For the patient is
suffering precisely from the absence of such a
relationship"
Jung 1928 para 276
Accompanying the patient through ‘the
darkest places’

The defeat of the analyst's ego
• the analyst’s intellect and reason rendered powerless - addressing
primarily affective-somatic elements and implicit ‘ways of being with
others’ which cannot be worked through simply by being named
• not ejecting what seems destructive or ill-adapted
• finding the kernel of truth in what is being said - probably a
reconstruction
• e.g. "You are a block of wood and are not interested in related to me"
('depressed mother dynamic')
• desperate attempts to relate vs. recognising the wound?
• patient's/child's failure to repair the mother the core traumatic
experience being reconstructed

The underlying narcissistic defences
• Working through:
• both the trauma related ‘borderline’ dynamics
• and the underlying, primitive narcissistic defences against
overwhelming suffering:
1. Avoid and evacuate suffering 2. Control 3. Distance
oneself from relationship or from one’s own reactions
• Anne Alvarez, working with autistic patients: a point when
early ways of relating, once necessary defences, no longer
necessary in the same way - become simply ways of
relating, sometimes in the absence of knowing other ways
of being (1999, ch. 5 esp. pgs. 73-4).

Michael
/ Bryony
grateful for their
permission

Some particular pressures

The reconstruction of the inhuman
• The patient needs to constellate the bad, inhuman object in
order to work through the early relational trauma
• dyadically expanded states of consciousness (Tronick)
• however good you are it doesn’t work through the trauma
… (my failed analyses …)
• Casement: “an analytic good object … is that which can
tolerate being used to represent the worst in the patient’s
experience” (2001, p. 384)
• but when those are inhuman?

The masochisto-sadistic dynamic
• out of the moral defence - drawn to / resonates to situations
of suffering
• the punishment of the other is justified by the individual's
woundedness and re-wounding - the victim becomes the
aggressor
• underlies splitting - not just good and bad
• Shabila - murderous feelings toward me
• political / cultural consequences

The moral defence
• the wound to the core self feels so bad that it feels
morally wrong - "this must not be allowed to happen
under any circumstances!" - "you are bad”
• when the analyst re-wounds, they cause moral
outrage
• Shabila - arriving early
• addressing the wound compassionately
• vs. Fairbairn's moral defence: "I am bad" - keeps the
object, upon whom the child depends, good

The analyst’s personal journey
The earlier and more profound the early relational trauma, the more the
trauma will need to be fully constellated and lived through in the analytic
relationship by both patient and analyst
• the analyst thus has to accompany the patient into and through
‘the darkest places’
The process of the analysis goes at the pace at which analyst and
patient can bear to experience and embody the experiences of being in
identification with the aggressor, or victim, or bystander, or rescuer; and
will be delayed until they can do so
• the process is held up by the analyst failing to bear / allow
themselves to be bad, to fail, to be defeated, or to be good, loved
etc.
“Don’t look back!” Faith in the process

Treatment models

Otto Kernberg & the Menninger Foundation
Transference Focused Psychotherapy (TFP)
• ‘Patients with Severe Personality Disorders … (‘significant ego-weakness’) …
improved more with a psychotherapeutic approach that focused on transference
interpretations in the sessions’ (with support outside the sessions ‘to maintain the
treatment frame’) (Kernberg et al. 2008, p. 601-2)
• Pts suffer from ‘identity diffusion’ - a chronic, stable lack of integration of the
concept of self and of the significant others… ultimate cause: … failure of
psychological integration resulting from the predominance of aggressive
internalised object relations over idealised ones…. to protect the idealised
segment of self and object representations … there are primitive splitting and
dissociative mechanisms’ (p. 602)
• ‘Main strategy’ of TFP: ‘the reactivation in the treatment of the patient’s split-off
internalised object relations that are then observed and interpreted in the
transference’ (p. 603)
• Interpretation links the dissociated positive and negative dyads/transferences,
which underpin the split and identity diffusion e.g., indifferent mother / bad child
vs. totally caring mother / happy child.
• Transference interpretations are linked to the patient’s problems in external
reality, in contrast to Kleinian technique (p. 609)

Dialectical Behaviour TherapyLineham (1993, et al. 2006)
• Sees Borderline Personality Disorder as due to the
individual’s emotional dysregulation
• Validates affective states and teaches skills to avoid
or distract in order to reduce or eliminate painful
emotions and stop problem behaviours
• Clear and articulated treatment structure, priority of
the issues to be addressed, stress on and protection
of the frame of treatment

STEPPSSystems Training for Emotional Predictability and Problem Solving
Nancee Blum
• A group based learning programme based on CBT principles,
focused on learning:
• to challenge maladaptive schemas
• self-care skills: sleep, exercise, diet
• problem solving, communication and relationship skills
• skills for dealing with intense emotions, anxiety,
depression, anger, and self-destructive impulses
• encouraged to share appropriate topics from their skills
training with close friends and family members, and also with
their therapists

Supportive Psychotherapy(Clarkin et. al. 2007)
• Seen as due to a deficit
• Supportive psychotherapy aims to strengthen
patients’ adaptive functioning by means of:
• cognitive support (advice or information giving)
• affective support (reassurance, praise, verbal
conveyance of empathy)
• direct intervention in patient’s life
• minimal transference interpretation due to fostering
positive transference

Schema Focused Therapy(Young et al. 2003; Giesen-Bloo et al. 2006)
• Problem due to ‘maladaptive schemas’ - cognitions
• Deficit model: patient has unfulfilled ‘core childhood’ needs,
such as safety, a stable base, predictability, love, nurturing,
attention, acceptance, praise, empathy, realistic limits, and
the validation of feelings and needs
• SFT addresses these needs with: cognitive restructuring,
emotion-focused techniques, behavioural life pattern change,
‘limited reparenting’ and ‘schema mode work’
• Explicitly supportive, recommending the therapist nurture,
praise, provide extra time and transitional objects and, ‘when
appropriate’, physically hold the patient
• Aggressive affects seen as stemming from justifiable anger

Mentalisation Based TherapyBateman & Fonagy (1999, 2004)
• Based on consistent efforts to increase the patient’s
mentalization. i.e., the patient’s capacity to recognise
mental states in themself and others & to allow self-
reflection and assessment of others to improve
mental functioning and symptomatology
• Disagrees with early interpretation as it may impute
mental states to patients that are incorrect
• vs. TFP which aims to interpret and help the patient
link dissociated, conflicting mental states as they are
reflected in the transference


References
Alvarez, A. (1999). ‘Disorder, deviance and personality: factors in the persistence and modifiability of autism’. In: Autism and
Personality: Findings from the Tavistock Autism Workshop. A. Alvarez & S. Reid (Eds.). London& New York: Routledge.
Battle, CL; Shea, MT; Johnson, DM; et al. (2004). ‘Childhood maltreatment associated with adult personality disorders: findings
from the Collaborative Longitudinal Personality Disorders Study’. Journal of Personality Disorder, 18(2): 193-211.
Beebe, B., & Lachmann, F. (2013). The Origins of Attachment: Infant Research and Adult Treatment. Abingdon: Taylor &
Francis.
Benjamin, J. (2004). Beyond doer and done to: An intersubjective view of thirdness. Psychoanalytic Quarterly, 73: 5-46.
Bollas, C. (2000). Hysteria. Abingdon: Taylor & Francis.
Bromberg, P. (2011). The Shadow of the Tsunami: and the Growth of the Relational Mind. New York: Routledge
Casement, P. J. (2001). Commentaries. Journal of the American Psychoanalytic Association, 49: 381-386.
Cozolino L. (2002) The impact of trauma on the brain. In The neuroscience of psychotherapy. Building and rebuilding the human
brain (pp.257-288). New York: W.W. Norton.
Davies, J.M. (1994). Love in the afternoon: A relational reconsideration of desire and dread. Psychoanalytic Dialogues, 4: 153-
170.
Davies, J. M. (2004). Whose bad objects are we anyway? Psychoanalytic Dialogues, 14: 711-732
Davies, J. M., & Frawley, M. G. (1992). ‘Dissociative processes and transference-countertransference paradigms in the
psychoanalytically oriented treatment of adult survivors of childhood sexual abuse’. Psychoanalytic Dialogues, 2: 5-36
Fonagy, P. (1991). ‘Thinking about thinking: some clinical and theoretical considerations in the treatment of a borderline patient’.
International Journal of Psychoanalysis, 72: 639-656.
Fonagy, P., Gergely, G., Jurist, E., & Target, M. (2002). Affect Regulation, Mentalization and the Development of the Self.
London: Karnac.

Fordham, M. (1974). Defences of the self. Journal of Analytical Psychology, 19: 192-199.
Harris, A. (2009). ‘You must remember this’. Psychoanalytic Dialogues, 19: 2-21.
Herman, J. L., Perry, J. C., & van der Kolk, B. A. (1989). Childhood trauma in borderline personality disorder. American
Journal of Psychiatry, 146: 490-495
Kernberg, O. (1975). Borderline Conditions and Pathological Narcissism. New York: Aronson.
Jung, C. G. (1928). The relations between the ego and the unconscious. CW 7. London: Routledge & Kegan Paul.
Jung, C. G. (1934). A review of the complex theory. In: The Structure and Dynamics of the Psyche, C.W. 8. London:
Routledge & Kegan Paul.
Jung, C. G. (1938/1954). Psychological aspects of the mother archetype. In: The Archetypes and the Collective
Unconscious, C.W. 9i. London: Routledge & Kegan Paul
Kernberg, O.F., Yeomans, F.E., Clarkin, J.F., & Levy, K.N. (2008). 'Transference focused therapy: overview and update’.
International Journal of Psychoanalysis, 89, 3, 601-620.
Knox, J. (1999). The relevance of attachment theory to a contemporary Jungian view of the internal world. Journal of
Analytical Psychology, 44: 511-530.
Krystal, H. (1988). Integration and Self-healing: Affect, Trauma, and Alexithymia. Hillsdale, NJ: Analytic Press.
Liotti, G. (2004a). ‘Trauma, dissociation, and disorganized attachment: three strands of a single braid’. Psychotherapy:
Theory, research, practice, training; 41: 472-486.
Liotti, G. (2004b). ‘The inner schema of borderline states and its correction during psychotherapy: a cognitive-evolutionary
approach'. In: P. Gilbert (Ed.), Evolutionary Theory and Cognitive Psychotherapy (pp. 137-160). New York: Springer.

Liotti, G. (2007). ‘Disorganized attachment and the therapeutic relationship with people in shattered states’. In: J. Yellin & K.
White (Eds.), Shattered States: Disorganised Attachment and Its Repair (pp. 127-156). London: Karnac, 2012
Meares, R. (2012). A Dissociation Model of Borderline Personality Disorder. New York: Norton.
Mills, J. (2012). Conundrums - A critique of contemporary psychoanalysis. New York & Hove: Routledge.
Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the Body: A Sensorimotor Approach to Psychotherapy. New York:
Norton.
Panksepp, J. & Biven, L. (2012). The Archaeology of Mind. New York: Norton.
Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication,
and Self-regulation. New York: Norton.
Racker, H. (1958). Psychoanalytic technique and the analyst's unconscious masochism. Psychoanalytic Quarterly, 27: 555-
562.
Shapiro, F. (2001). Eye Movement Desensitization and Reprocessing: Basic principles, protocols and Procedures (2nd
ed.). New York, NY: Guildford Press.
Siegal, D. (1999). The Developing Mind. New York: Guildford Press.
Stern, A. (1938). Psychoanalytic investigation of and therapy in the borderline group of neuroses. Psychoanalytic Quarterly,
7: 467-489.
Stern, D. N. (1985/1998). The Interpersonal World of the Infant: a View from Psychoanalysis and Developmental
Psychology. London: Karnac

Tronick, E. Z., & Gianino, A. (1986). Interactive mismatch and repair: challenges to the coping infant. Zero to Three,
Bulletin of the National Center for Clinical Infant Programs, 5: 1-6.
Tronick, E.Z., Bruschweiler-Stern N., Harrison A.M., Lyons-Ruth, K., Morgan A.C., Nahum J.P., Sander, L., & Stern, N.
D. (1998). Dyadically expanded states of consciousness and the process of therapeutic change. Infant Mental Health
Journal, 19: 290-299
van der Kolk, B. (1996b). Trauma and memory. In: A. C. McFarlane, L. Weisaeth & B. Van der Kolk (Eds.), Traumatic Stress:
The Effects of Overwhelming Experience on Mind, Body, and Society (pp. 279-302). New York: Guilford Press, 1996.
van der Kolk, B (2011). The Body Keeps the Score: Mind, Brain & Body in the Transformation of Trauma. Penguin.
van der Kolk, B., & d’Andrea, W. (2010). Towards a developmental trauma disorder diagnosis for childhood interpersonal
trauma. In: R. Lanius, E. Vermetten & C. Pain (Eds.), The Impact of Early Life Trauma on Health and Disease:- The Hidden
Epidemic (pp. 57-68). Cambridge: Cambridge University Press.
van der Kolk, B., McFarlane, A. & Weisaeth, L. (1996). Traumatic Stress: The Effects of Overwhelming Experience on
Mind, Body, and Society. B. van der Kolk, A. C. McFarlane & L. Weisaeth, (Eds.). New York: Guilford Press.
West, M. A. S. (2007). Feeling, Being and the Sense of Self: A New Perspective on Identity, Affect and Narcissistic
Disorders. London: Karnac
West, M. (2016). Into the Darkest Places: Early Relational Trauma and Borderline States of Mind. London: Karnac.
Winnicott, D.W. (1974). Fear of Breakdown. International Review of Psycho-Analysis, 1:103-107
Related Documents