ÓRGÃO OFICIAL DA SOCIEDADE PORTUGUESA DE REUMATOLOGIA 86 IMAGES IN RHEUMATOLOGY Antibodies (ANA) = 1/240 centromere pattern. Chest, shoulders and hips x-rays (Figures 1A and B, 2 and 3) showed universal calcinosis. During those 19 years, in addition to treatment for systemic sclerosis (nifedipine, D - penicillamine, pre- dinisone and azathioprine), different calcinosis treat- ments were used, including diltiazem, colchicine, bis- phosphonates (pamidronate and zoledronic acid), war- farin and surgery, but all were ineffective. dIscussIon Calcinosis pathophysiology is not clear, but there are some theories that inflammation and vascular ischemia play a role in its process 1,2,4 . Diagnosis can be made by plain radiography, as it has a very good sensitivity to detect calcinosis and is in- dicated as initial imaging evaluation 1,2,4 . Management includes general measures, pharmaco- logical and non-pharmacological treatment. As gene ral measures, it is important to improve blood flow in ex- tremities 1 . Pharmacological treatment includes diltiazem, which reduces intracellular calcium influx and alters calcium nidus formation. It’s considered as a first-line approach. Warfarin acts at vitamin K levels, which is in- volved in the calcium-biding process, but studies re- sults are contradictory 1,2,4 . Biphosphonates may be used to inhibit osteitis and bone resorption and have shown positive results. Colchicine is not effective in reducing calcium deposit sizes, but works on reducing local inflammation. . Pa- tients treated with rituximab seem to have bene ficial results, but more studies are required to infer some- thing concrete 1-4 . Finally, surgery is indicated mainly in localized cal- cinosis or when there is major pain or function loss 2-4 . As observed, our patient had the main treatment options for calcinosis and they were not effective. Cur- 1. Departamento de Medicina, Universidade Nilton Lins 2. Departamento de Clínica Médica, Universidade Federal do Amazonas Dystrophic calcinosis: do we really know how to treat it? Nunes GPS 1 , Souza RB 2 , Ribeiro SLE 2 ACTA REUMATOL PORT. 2019;44:86-87 IntroductIon Calcinosis cutis is the deposition of calcium in the skin and subcutaneous tissue. It’s a rare disorder occurring more frequently in systemic sclerosis and dermato- myositis 1-5 . The classification of soft-tissue calcifications includes the metastatic, tumoral, dystrophic and idiopathic types. The most common is the dystrophic type, cha- racterized by normal calcium metabolism (normal serum level of calcium and phosphate) 1,3 . It’s a long-term manifestation and clinical features associated to it are digital ulcers, osteoporosis, anti- centromere antibody and anti-PM-Scl antibody 1,2 . We hereby present a case of a patient with treatment- refractory extensive calcinosis. case report A 63-year-old female was diagnosed with CREST syn- drome (calcinosis, Raynaud’s phenomenon, esophageal dysmotility, sclerodactyly and telangectasias) 19 years ago. She currently reports inability to walk and dys- pnea. On the clinical examination, she had masklike face, skin thickening and hardening (modified Ro dnan score 26); major muscular atrophy and extensive cal- cinosis on shoulders, elbows, thorax, abdomen, knees and feet with joint involvement, causing pain and re- current minor infections, requiring antibiotics and surgery. On the laboratory results, she had normocy t ic and normochromic anemia, Erythrocyte Sedimentation Rate (ESR) = 110mm, calcium = 8.3mg/dl, phosphorus = 4.1mg/dl, alkaline phosphatase = 131U/l and Crea- tine Phosphokinase (CPK) = 47U/l, negative anti-Scl- -70 antibody, anticentromere antibody +, Antinuclear

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ÓRGÃO OFICIAL DA SOCIEDADE PORTUGUESA DE REUMATOLOGIA
86
IMAGES IN RHEUMATOLOGY
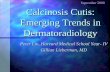
Antibodies (ANA) = 1/240 centromere pattern. Chest,shoulders and hips x-rays (Figures 1A and B, 2 and 3)showed universal calcinosis.
During those 19 years, in addition to treatment forsystemic sclerosis (nifedipine, D - penicillamine, pre-dinisone and azathioprine), different calcinosis treat-ments were used, including diltiazem, colchicine, bis-phosphonates (pamidronate and zoledronic acid), war-farin and surgery, but all were ineffective.
dIscussIon
Calcinosis pathophysiology is not clear, but there aresome theories that inflammation and vascular ischemiaplay a role in its process1,2,4.
Diagnosis can be made by plain radiography, as ithas a very good sensitivity to detect calcinosis and is in-dicated as initial imaging evaluation1,2,4.
Management includes general measures, pharmaco-logical and non-pharmacological treatment. As gene ralmeasures, it is important to improve blood flow in ex-tremities1.
Pharmacological treatment includes diltiazem,which reduces intracellular calcium influx and alterscalcium nidus formation. It’s considered as a first-lineapproach. Warfarin acts at vitamin K levels, which is in-volved in the calcium-biding process, but studies re-sults are contradictory1,2,4.
Biphosphonates may be used to inhibit osteitis andbone resorption and have shown positive results.Colchicine is not effective in reducing calcium depositsizes, but works on reducing local inflammation.. Pa-tients treated with rituximab seem to have bene ficialresults, but more studies are required to infer some-thing concrete1-4.
Finally, surgery is indicated mainly in localized cal-cinosis or when there is major pain or function loss2-4.
As observed, our patient had the main treatment options for calcinosis and they were not effective. Cur-
1. Departamento de Medicina, Universidade Nilton Lins2. Departamento de Clínica Médica, Universidade Federal do Amazonas
Dystrophic calcinosis: do we really know how to treat it?
Nunes GPS1, Souza RB2, Ribeiro SLE2
ACTA REUMATOL PORT. 2019;44:86-87
IntroductIon
Calcinosis cutis is the deposition of calcium in the skinand subcutaneous tissue. It’s a rare disorder occurringmore frequently in systemic sclerosis and dermato-myositis1-5.
The classification of soft-tissue calcifications includesthe metastatic, tumoral, dystrophic and idiopathictypes. The most common is the dystrophic type, cha -racterized by normal calcium metabolism (normalserum level of calcium and phosphate)1,3.
It’s a long-term manifestation and clinical featuresassociated to it are digital ulcers, osteoporosis, anti-centromere antibody and anti-PM-Scl antibody1,2.
We hereby present a case of a patient with treatment-refractory extensive calcinosis.
case report
A 63-year-old female was diagnosed with CREST syn-drome (calcinosis, Raynaud’s phenomenon, esophagealdysmotility, sclerodactyly and telangectasias) 19 yearsago. She currently reports inability to walk and dys -pnea. On the clinical examination, she had masklikeface, skin thickening and hardening (modified Ro dnanscore 26); major muscular atrophy and extensive cal-cinosis on shoulders, elbows, thorax, abdomen, kneesand feet with joint involvement, causing pain and re-current minor infections, requiring antibiotics andsurgery. On the laboratory results, she had normocy ticand normochromic anemia, Erythrocyte SedimentationRate (ESR) = 110mm, calcium = 8.3mg/dl, phosphorus= 4.1mg/dl, alkaline phosphatase = 131U/l and Crea-tine Phosphokinase (CPK) = 47U/l, negative anti-Scl--70 antibody, anticentromere antibody +, Antinuclear

ÓRGÃO OFICIAL DA SOCIEDADE PORTUGUESA DE REUMATOLOGIA
87
NuNes GPs et al
rently, she still lives with a lot of pain and extensivecalcinosis all over her body. In light of the above, wewonder, do we really know how to treat calcinosis?More studies are required for more robusts conclu-sions and to improve our patients’ quality of life.
correspondence to
Gabriel NunesAv Maneca Marques, 55 Residencial Rubi APTO 501Phone Number / Telefone: +5592991220870Email: [email protected]
reFerences
1. Valenzuela A, Chung L. Calcinosis: pathophysiology and ma-nagement. CO Rheumatology, 2015: 27 (6): 542-548.
2. Henrrick AL, Gallas A. Systemic sclerosis-related calcinosis.JSRD, 2016; 1(2): 194-203.
3. Dima A, Balanescu P, Baicus C. Pharmacological treatment incalcinosis cutis associated with connective-tissue diseases. RomJ Intern Med, 2014; 52(2): 55-67.
4. Valenzuela A, Song P, Chung L. Calcinosis in Scleroderma. CORheumatology, 2018: 30(6): 554 – 561.
5. Du� zgu� n N. Cutaneous calcinosis in a patient with limited scle-roderma: CREST Syndrome. Eur J Rheumatol, 2017; 4: 305-6.
FIGure 1a and B, 2 and 3. Extensive calcinosis lesions – shoulders, thorax and hips
Related Documents


![Case Report Metastatic Calcinosis Cutis: A Case in a Child ...downloads.hindawi.com/journals/crihem/2015/384821.pdf · phoblastic and myeloid acute leukemia []. Metastatic cal-cinosis](https://static.cupdf.com/doc/110x72/5f903fad69bb713af81a8e96/case-report-metastatic-calcinosis-cutis-a-case-in-a-child-phoblastic-and-myeloid.jpg)