Duke University Health Information Systems: The Integrity of Measurements and Measures W. Ed Hammond, Ph.D. President, AMIA Chair, Data Standards WG, Connecting for Health Vice-chair, HL7 Technical Steering Committee Convenor, ISO TC 215 Working Group 2 Professor-Emeritus, Duke University

Duke University Health Information Systems: The Integrity of Measurements and Measures W. Ed Hammond, Ph.D. President, AMIA Chair, Data Standards WG, Connecting.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Duke University
Health Information Systems: The Integrity of Measurements and Measures
W. Ed Hammond, Ph.D.President, AMIA
Chair, Data Standards WG, Connecting for HealthVice-chair, HL7 Technical Steering Committee
Convenor, ISO TC 215 Working Group 2Professor-Emeritus, Duke University
Duke University
The Vision and the Need
Providers, those responsible for population health, those responsible for paying for health, those setting the policies that determine the nature of health care provided, and most importantly, consumers will have ready access to timely, relevant, reliable, and secure health care data, information and knowledge through an interconnected, electronic health information infrastructure, to drive better health and health care.
Duke University
Major Concerns in Health Care
• Reducing cost of care• Increasing the quality of care• Reducing medical errors• Accommodating an aging population• Biosurveillance and health surveillance• Better management of chronic disease• We need the aggregation, integration and
sharing of data among all stakeholders including patient care, research, policy making, management and reimbursement.
Duke University
BarriersBarriers• Lack of political will and the need for more Federal leadership• Independence of stakeholders in sharing, collaboration and
use of data• Lack of incentives to make the changes that are necessary
and to support maintenance of such systems• Lack of processes that would create unambiguous reuse of
clinical measurements. Need consensus standards.– Terminology– Definitions– Data or information model– Data types and formats– Data interchange standards
• Need for implementation guidance and migration strategies• The need for a clear value proposition for all stakeholders • The importance of privacy and security

Duke University
The value of measurement
• Theories about heat and entropy evolved after the development of measuring tools – thermometers and accurate readings
• The ability to measure the speed of light led to theories of relativity.
• We cannot model or evaluate what we cannot measure. When we can measure, we can act.
• Measurement of cholesterol led to understanding its role in cardiovascular disease, and resulted in emphasis on diets and exercise and medications.

Duke University
Measurement and Measures
• Key to the creation of knowledge• Key to judgment and evaluation• Key to understanding outcomes• Key to the creation of processes• Key to decision making and action in health care• The evidence of evidence-based ________
• Measurements are the key to health care and thus to the Electronic Health Record.
Duke University
Measurement and measures (data)
• Quantitative data– Height and weight– Laboratory data
• Soft data (judgmental)– Quality of pain– Rating scale
• Specialized data– Outcomes– Quality indices– Polls and surveys– Comparative functional imaging

Duke University
Characteristics of data
• Data must be timely.• Persistence and value of data will vary as a
function of site, time and purpose.• Data must be of high quality. Algorithms
should be used to insure quality in real time.– Block impossible entries by using gender specific and
age specific filters– Use previous data, trends, and deltas to question
implausible data– Use high/low limits to constrain data
• Data must be comprehensive• Data must be aggregated• Data must be finely grained for understanding
Duke University
Cost of data
• Obtaining data is an arduous and time-consuming task.
• Manual creation and entry of data into the EHR is expensive. People like to use data but no one wants to enter it.
• Entry of data is most preferably done by the person creating the data. <clinicians, nurses, technicians, clerks, citizens,…>
• Automated capturing of data is best.• Data should never be entered more than once.• Data should be shared for all appropriate
purposes.
Duke University
The process of health care
• The fundamental process of health care is to collect data and use that data for decision making; then collect more data to evaluate the results of those decisions.– The process starts with a query of the patient “What’s
wrong?” or the chief complaint.– Next is the process of taking a history and doing a
physical exam.– Next comes tests: laboratory, radiology, pathology,
microbiology, etc.– Then decisions are made and a treatment is
prescribed.– Finally the follow-up to determine the results and
effectiveness of the treatment.

Duke University
Data RepresentationReference terminology model + term
Knowledge representation

Duke University
Creation of Information
Data Mining
ClinicalData - EHR
KnowledgeDatabase
Information
Real time use by all interested
Decision SupportSystem

Duke University
Defining the Problem
• Health care is not taking full advantage of the information and communications technologies that have revolutionized other industries.
• Until clinical data can be reliably, efficiently and consistently shared and integrated in a manner that protects patient privacy and security, the health care system will continue to struggle with large gaps in the information that is needed at the bedside, in the office, at home, in the emergency room and at local and state public health departments.

Duke University
Defining the Need
• Taking full advantage of IT in healthcare means going beyond “siloed” information systems and toward creating an information infrastructure that enables rapid, secure, private, and complete communication among varying information systems to meet the needs of patient care.
• The highest goal of an information infrastructure is to enable the timely and efficient access to vital health data when and where its needed to improve the quality, safety and cost-effectiveness of care and to strengthen the efforts of consumers, patients, and caregivers.

Duke University
Vision for an Information Infrastructure• Our view for realizing this high level objective of an
information infrastructure requires the creation of a dynamic network[1] within health care that allows the movement of health information that is characterized by moving only necessary information, when its needed and to where its needed in a private and secure manner.
• A cooperative, collaborative relationship between government, business, academia, providers and patients is a necessary culture for a system of “dynamic connectedness”[2].
• This infrastructure necessitates appropriate permissioning and authentication standards throughout its deployment.
[ Markle National Security Task Force Report[2]
Duke University
The Culture of Dynamic Connectedness
• All participants in the delivery system have responsibilities to the data that ultimately center on the need to provide the best possible care for patients.
• All stakeholders have responsibilities to protect the privacy and security of health information.
• All have additional responsibilities to make appropriate information available when and where it’s needed for patients and the physicians who treat them.
• This will require a change in culture, policy and practice.
Duke University
Interoperability
• Interoperability based on common data standards is a pre-requisite of this kind of a dynamic network.
• In health care, widespread interoperability opens the door to extraordinary change in areas ranging from individual patient safety during treatment, to population safety from epidemics, to the everyday chronic and acute care of millions of citizens.
Duke University
Requirements for sharing of data
• Uniquely semantically understandable• Based on common reference information model• Based on common data type• Based on common terminology
• Interchange of data requires data messaging standard
• May be contained using standard clinical document architecture

Duke University
Standards for Interoperable Health Care
• Movement towards standards will require effective processes for:– Standards development– Standards support and maintenance – Integration of standards– Creating the demand for standards at all levels of the
delivery system– Strategies for compliance and conformance– Clear and actionable consensus by both the public
and private sectors on the standards to be adopted – Implementation support (e.g. implementation guides
and other practical tools to assist with migration)

Duke University
Benefits• All stakeholders have much to gain from data
standards adoption and an interoperable health care system:– Hospitals will benefit from improvements in quality and
safety driven by a more comprehensive patient record, reductions in integration costs, and an easing of reporting burden
– Practicing Clinicians will benefit from access to patient information across multiple, fragmented components of the health care system to improve clinical decision-making
– Public Health and National Security will benefit from more rapid, accurate, cost-effective access to data to support surveillance, detection, management and response to public health threats
– Payers will benefit from a more efficient, more effective method of assessing and facilitating the improvement in quality of care across populations
– Researchers will benefit from improvements in the quality and cost-effectiveness of data collection to support analysis and evaluation
Duke University
Benefits (continued)
• Patients and consumers will derive the most value from the quality, safety, and cost-effectiveness gains that will be achieved through the use of interoperable health care systems. They will also benefit from the ability to make portable health care records more likely and easily achievable.
• Information Technology companies will benefit both from being able to provide products that easily integrate into existing infrastructure (and therefore reduce unnecessary costs), and from providing the marketplace with innovative products that maximize the potential of health information at the point of care.
• Pharmaceutical companies will benefit from the ability to do better drug research, reduce costs for data collection and conduct more real-time monitoring of drug safety and efficacy.
• Government Agencies who deliver health care will benefit by being able to improve health outcomes, increase patient safety, improve quality and help achieve optimal use of scarce resources.

Duke University
The Role of the Clinical Community
• The clinical community plays an active role in efforts to migrate toward an interoperable health care system if we are to be successful.
• This will require:– Leadership and commitment– Commitment to organizational change– Investment of resources– Keeping the focus on delivering higher quality, safer
health care– Engaging in activities related to clinical content and
terminology
Duke University
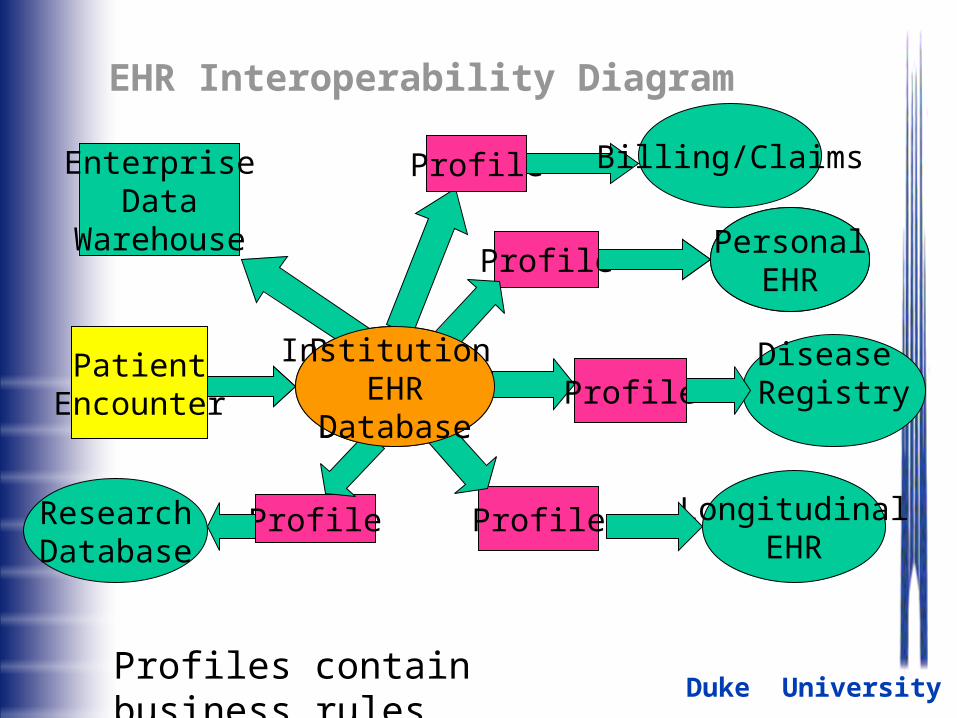
EHR Interoperability Diagram
PatientEncounter
Provider EHR
Database
PersonalEHR
LongitudinalEHR
Profile
Profile
ProfileResearchDatabase
EnterpriseData
Warehouse PersonalEHR
ProfileDisease Registry
Profile Billing/Claims
Profiles contain business rules
Institution EHR
Database
Duke University
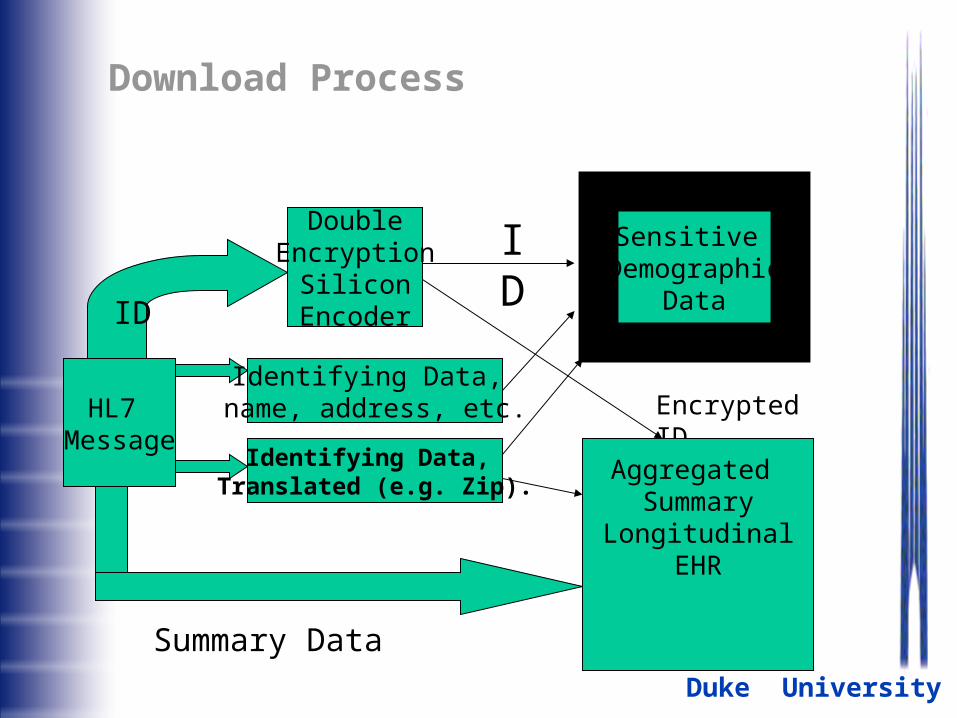
Download Process
HL7 Message
ID
DoubleEncryption
SiliconEncoder
Sensitive Demographic
Data
Encrypted IDIdentifying Data, name, address, etc.
Identifying Data, Translated (e.g. Zip).
Aggregated Summary
LongitudinalEHR
Summary Data
ID
Duke University
Policy Requirements at National Level
• Share in the grand vision of informed health care
• Support <mandate> creation and use of data standards at the national level including one integrated terminology.
• Create infrastructure for sharing of data among all stakeholders.
• Become the enabler sharing decisions, evaluations, and process with all constituencies including citizens
• Policy set at national levels; execution at local levels; coordinate at appropriate points.
Related Documents