Dr.Sarma@works 1 Welcome to You All

Dr.Sarma@works 1 Welcome to You All. Dr.Sarma@works 2 Dr.Sarma RVSN, M.D., M.Sc (Canada) Consultant in Medicine and Chest, President IMA – Tiruvallur.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr.Sarma@works
1
Welcome to You
All

Dr.Sarma@works
2
Dr.Sarma RVSN, M.D., M.Sc (Canada)
Consultant in Medicine and Chest,
President IMA – Tiruvallur Branch
# 3, Jayanagar, Tiruvallur – 602 001
+91 98940 60593, (4116) 260593
Dyslipidemias Dx. and Rx.
Dyslipidemias Dx. and Rx.

Dr.Sarma@works
3
CD ROM Available
The contents of today’s presentation
are available in a CD-ROM format
for computer and VCD player use.
This CD, in addition, contains our talks on
ECG, Asthma, COPD, Hypertension Rx. also

Dr.Sarma@works
4
National Cholesterol Education Program - NCEP
Adult Treatment Panel III (ATP III) Guidelines -2002
Updated October 2004

Dr.Sarma@works
5
Guidelines that aren’t implemented never work
Guidelines that aren’t implemented never work

CHD Risk Factors ranking - PROCAM StudyCHD Risk Factors ranking - PROCAM Study
Risk factor Relative risk P ValueRisk factor Relative risk P Value
Smoking 2.30.001
LDL cholesterol (mg%)> 100 but < 160 1.90.01> 160 4.30.001
Hypertension (SBP > 140; DBP > 90) 1.80.001
HDL cholesterol (mg%)40 to 55 1.70.01< 40 2.70.001
Triglycerides (mg%)105- 167 1.60.01>167 2.60.001
Fasting blood glucose (mg%)110 - 126 1.40.05> 126 1.90.01
Family history of MI 1.40.05
Smoking 2.30.001
LDL cholesterol (mg%)> 100 but < 160 1.90.01> 160 4.30.001
Hypertension (SBP > 140; DBP > 90) 1.80.001
HDL cholesterol (mg%)40 to 55 1.70.01< 40 2.70.001
Triglycerides (mg%)105- 167 1.60.01>167 2.60.001
Fasting blood glucose (mg%)110 - 126 1.40.05> 126 1.90.01
Family history of MI 1.40.05

Dr.Sarma@works
7
Emerging Risk Factors
1. Lipoprotein (a)
2. Homocysteine
3. Prothrombotic factors
4. Pro-inflammatory factors
5. Metabolic syndrome
6. Sub-clinical atherosclerosis

Dr.Sarma@works
8
CHD Risk Equivalents
1. Diabetes Mellitus
2. Peripheral Vascular Disease
3. > 20% in Framingham risk score
4. Carotid atheroma
5. Reno-vascular Disease
All forms of AVD

Dr.Sarma@works
9
AVD – Clinical Manifestations
Organ Condition Impairment Clinical Presentation
Heart Coronary Heart
Disease (CHD)
Ischemia
Infarction
Angina Pectoris
Myocardial Infarction
Brain Cerebro vascular
Disease (CVD)
Ischemia
Infarction
Transient Ischemia attack
Stroke
Kidney Reno vascular
Disease (RVD)
Ischemia
Infarction
Renal HT, Renal impairment
Renal Failure
Leg Muscles
Peripheral Vascular Disease (PVD)
Ischemia
Infarction
Intermittent Claudication
Gangrene
For every thing the common denominator is ED

Dr.Sarma@works
10
Progression of Atherosclerosis

Dr.Sarma@works
11
Lipid Peroxidation
LDL, IDL Not normally taken up by the vessel wall
ROS – Free radicals and Pro-oxidants
Oxidized LDL, IDL
Freely enters the vessel wall
Scavenger pathway
Endothelium Macrophages
Foam Cells Cytokines, GF
Atherosclerosis

LDL
LDLEndothelium
Vessel LumenMonocyte
Macrophage
AdhesionMolecules
The Havoc by LDL at the endothelium
Foam Cell
IntimaModified
LDLCytokines
Cell ProliferationMatrix Degradation
Growth FactorsMetalloproteinases
Ross R. N Engl J Med 1999;340:115-126.
MCP-1

Pathogenesis of ACS
Non-Vulnerable Atherosclerotic
Plaque
Non-Vulnerable Atherosclerotic
Plaque
Vulnerable Atherosclerotic
Plaque
Vulnerable Atherosclerotic
Plaque
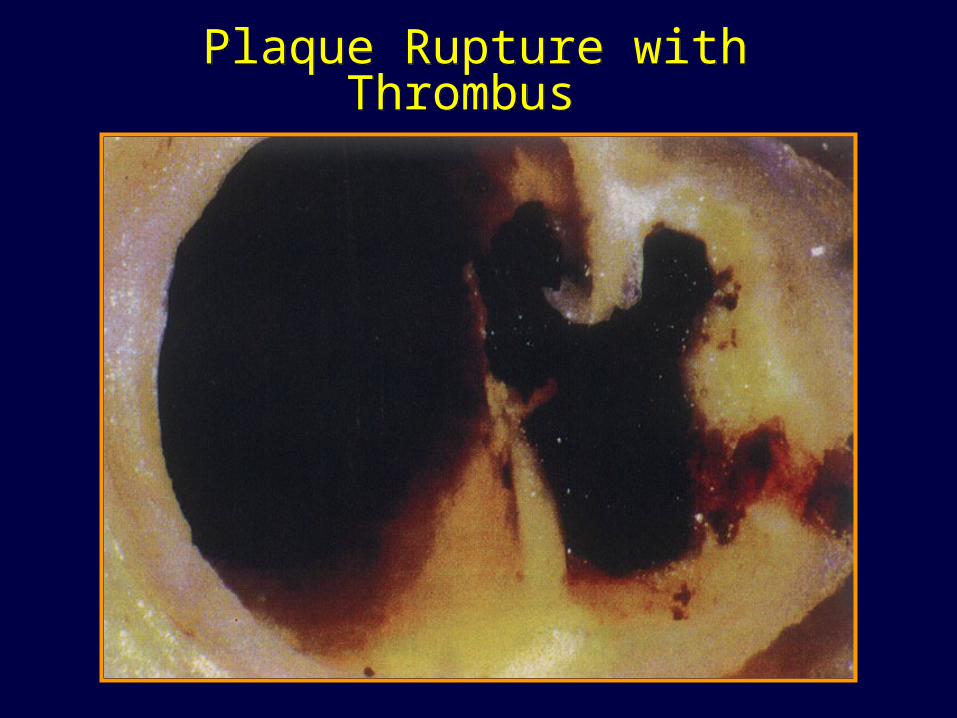
Plaque Rupture with Thrombus Plaque Rupture with Thrombus

Dr.Sarma@works
15
ECTG
Lipid Transport
Apoprotein boat
Apo A I and A II for HDL Apo B100 for LDL, Lp(a) Apo B100+C+E – VLDL, IDL Apo B48+C+A+E – Chy. microns

Dr.Sarma@works
16
Lipoproteins
CTG
B 100 + E +C
CTG
B 100
CTG
A I, A II
HDL LDL
VLDL
TG
B 48+E+C
CM

Dr.Sarma@works
17
Cholesterols and Apoproteins
• Total Cholesterol < 200 Apoprotein • ‘Bad’ Cholesterols Apo B type
– LDLc, IDLc < 100 B100 or B100 +E– VLDLc, VLDLr < 30 B100 + E + C– Lp(a), small LDL < 20 B100 + (a)
• ‘Good’ Cholesterols Apo A type– HDL 1, HDL 2, HDL 3 > 50 A I and A II
HDL 1 and HDL 2 are protective

Dr.Sarma@works
18
Particle size & Density
Chylomicrons
<< 1.006
VLDL
< 1.006
IDL
< 1.019
LDL
< 1.063
Small LDL
< 1.085
HDL
< 1.210
Atherogenicity increases as density increases

Dr.Sarma@works
19
Atherogenic Particles
Apolipoprotein BApolipoprotein B
Non-HDL-CNon-HDL-CMeasurementsMeasurements
TG-rich lipoproteinsTG-rich lipoproteins
VLDLVLDL VLDLRVLDLR IDLIDL LDLLDL SDLSDL
Dr.Sarma@works
20
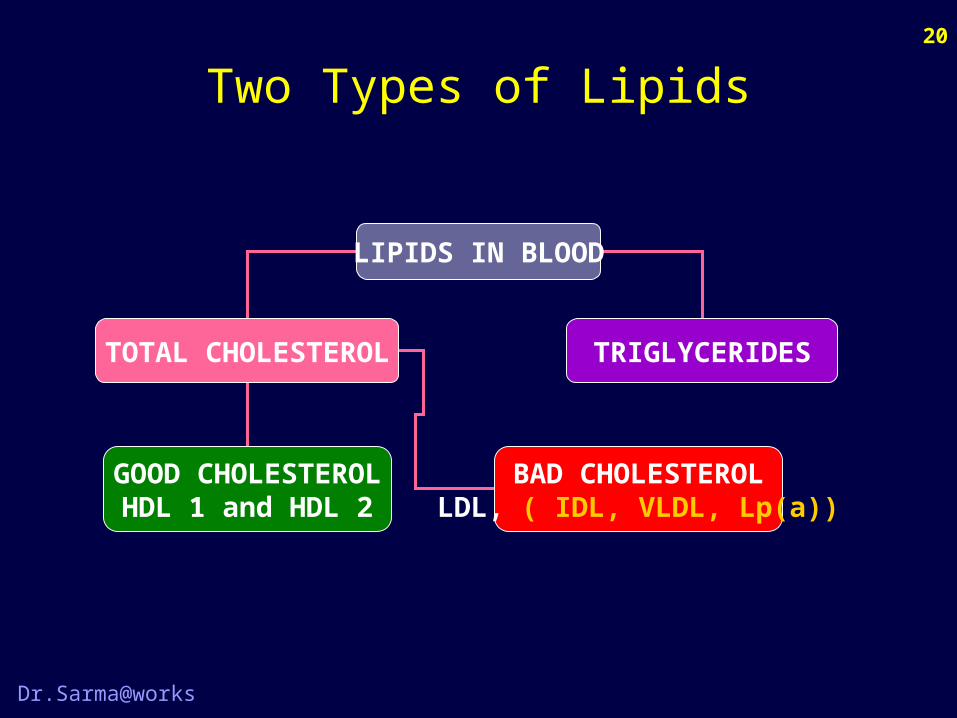
Two Types of Lipids
LIPIDS IN BLOOD
TOTAL CHOLESTEROL TRIGLYCERIDES
GOOD CHOLESTEROLHDL 1 and HDL 2
BAD CHOLESTEROLLDL, ( IDL, VLDL, Lp(a))

Dr.Sarma@works
21
LIPIDS ESTIMATED
TOTAL CHOLESTEROL (TC) TRIGLYCERIDES (TG)
HDLc LDLc VLDLc Chylomicrons VLDL
Lipid Profile Report
PP Fasting

Dr.Sarma@works
22
Lipid Calculations
A. Total Cholesterol
HDL Cholesterol
LDL Cholesterol (TC –(HDL+VLDL))
VLDL Cholesterol (1/5 of TG)
B. Triglycerides
150
30
120
50
200

Dr.Sarma@works
23
The Good and Bad
• Total Cholesterol < 200 • ‘Good’ Cholesterols
– HDL 1, HDL 2, HDL 3 > 50• ‘Bad’ Cholesterols (Non HDLc) < 150
– LDLc, IDLc < 100– VLDLc, VLDLr < 30– Lp(a), small LDL < 20
HDL 1 and HDL 2 are protective
Dr.Sarma@works
24
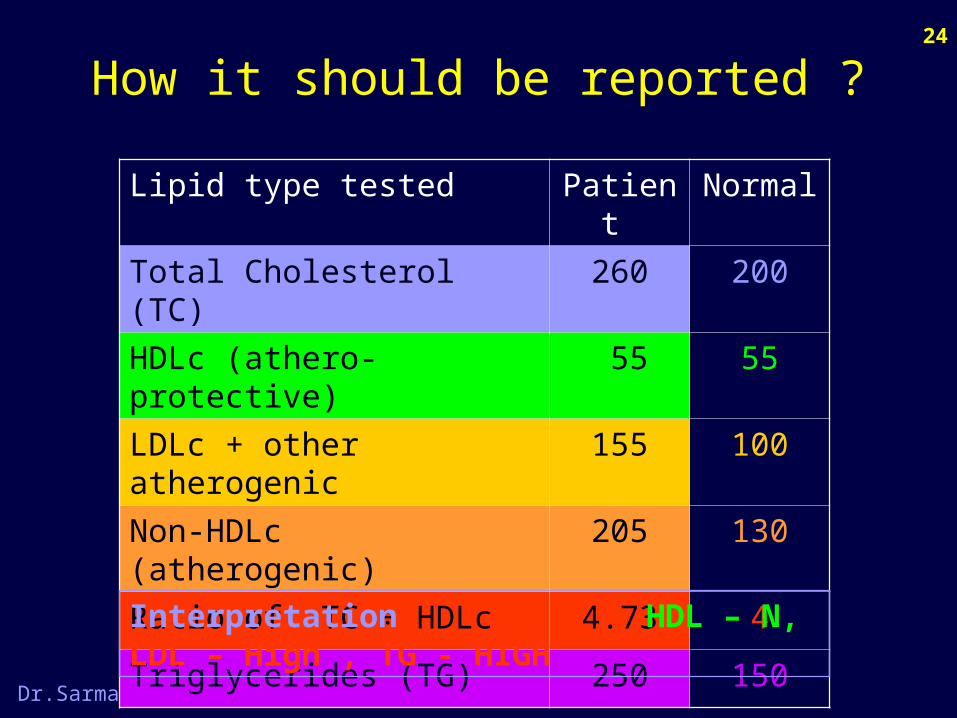
How it should be reported ?
Lipid type tested Patient Normal
Total Cholesterol (TC) 260 200
HDLc (athero-protective) 55 55
LDLc + other atherogenic 155 100
Non-HDLc (atherogenic) 205 130
Ratio of TC ÷ HDLc 4.73 4
Triglycerides (TG) 250 150
Interpretation HDL – N, LDL – High , TG - HIGH

Dr.Sarma@works
25
Today’s Safer Values
• Total Cholesterol < 200• Triglycerides < 150• LDL Cholesterol < 100• HDL Cholesterol > 50 (for women 55)• Bad Cholesterols the lower the better• Good Cholesterols the higher the better• Non HDL Cholesterol < 130• Lp(a) values < 20• Homocysteine < 14 μ mols per liter

Dr.Sarma@works
26
Indian Specialty
A. Isolated low LDL 32.90%B. Isolated low HDL 21.35%C. Isolated high TG 10.45%
IHJ, 2000, 52: 173-177Am J Med, 1998, vol 105(1A), 48S-56S
↑LDL
↓HDL
↑TG
The Triad

Dr.Sarma@works
27
Look at the risks
• Low HDL + High LDL +• LP(a) excess > 30 mg% + • LP(a) excess > 30 mg% + LDL high ++• LP(a) excess > 30 mg% + low HDL +++• LP(a) excess > 30 mg% + Incr. tHCy ++++• LP(a) excess + Incr. tHCy + low HDL ++++
+• Circulating lipids are one aspects• Tissue lipid content is more important
J. Atherosclerosis : Hopkins PN, 1997 – 17, 2792

Dr.Sarma@works
28
Additive Effect
SBP >160
Dyslipidemia
Smoking
4
3
5
4.5
16
With DM all risks are doubledWith DM all risks are doubled
Relative risk of CHD
1.6
6

Dr.Sarma@works
29
Intestinal Cholesterol Absorption
Bays H et al. Expert Opin Pharmacother 2003;4:779-790.
Intestinal Intestinal epithelial cellepithelial cell
BiliaryBiliarycholesterolcholesterol
DietaryDietarycholesterolcholesterol
LuminalLuminalcholesterolcholesterol
MicellarMicellarcholesterolcholesterol
Bile Bile acidacid
Cholesteryl esters
Freecholesterol
excretion
uptakeuptake
ACATACAT
ABCG5ABCG5ABCG8ABCG8
(esterification)
MTPMTPCMCM
Through Through lymphatic lymphatic system to system to the liverthe liver

Dr.Sarma@works
30
LymphLymphLymphLymph EnterocyteEnterocyteEnterocyteEnterocyte IntestinalIntestinalLumenLumen
IntestinalIntestinalLumenLumen
Cholesterol Absorption
Cholesterol
NPC1L1
CholesterylEster ABCG5/G8
ACAT
Ezetimibe
Avasimibe

Dr.Sarma@works
31
Fat Absorption
DuodenumDuodenumDuodenumDuodenum
JejunumJejunumJejunumJejunum
IleumIleumIleumIleum
BiliaryBiliaryTransportTransportand Storageand Storage
BiliaryBiliaryTransportTransportand Storageand Storage
ColonColonColonColon
LiverLiverLiverLiver

Dr.Sarma@works
32
LymphLymphLymphLymph EnterocyteEnterocyteEnterocyteEnterocyte IntestinalIntestinalLumenLumen
IntestinalIntestinalLumenLumen
Triglyceride Absorption
2 Fatty Acid+
Monoglyceride
DGAT
Triglyceride

Dr.Sarma@works
33
LymphLymphLymphLymph EnterocyteEnterocyteEnterocyteEnterocyte IntestinalIntestinalLumenLumen
IntestinalIntestinalLumenLumen
Chylomicron Formation
CholesterylEster
CMapoB48
Triglyceride

Dr.Sarma@works
34
Structure of HDL Particle
A-I A-I
A-II
A-I, A-II = apolipoprotein A-I, A-II; CE = cholesterol ester; TG = triglycerides
CETG

Dr.Sarma@works
35
HDL Types
CE
A-I
CE
A-I
CE
A-II A-II
HDL 1 HDL 2 HDL 3
APO A I Protective Alcohol increases

Dr.Sarma@works
36
LIVER
Reverse Cholesterol Transport
MF in Vascular Endothelium
Free Chol.
L CAT Enzyme
UECEC
HDL

Dr.Sarma@works
37HDL Metabolism and
Reverse Cholesterol Transport
Liver
ABC1 = ATP-binding cassette protein 1; A-I = apolipoprotein A-I; CE = cholesteryl ester; FC = free cholesterol;
LCAT = lecithin:cholesterol acyltransferase; SR-BI = scavenger receptor class BI
Mature HDL
CE
A-I
CECE
FCFCLCAT
FC
Bile
SR-BI
A-I
ABC1Macrophage
Nascent HDL

Dr.Sarma@works
38
B
SRA
Mature HDL
Role of CETP in HDL Metabolism
A-I
Liver
CE
CEFC
FC
LCATFC
Bile
SR-BI
A-I
ABC1
Macrophage
CE
CETP = cholesteryl ester transfer proteinLDL = low-density lipoprotein
LDLR = low-density lipoprotein receptorVLDL = very-low-density lipoprotein
LDLR
VLDL/LDL
CETP
Nascent HDL
CE
Oxidation
Torcitrapib
X

Dr.Sarma@works
39
Hyperlipidemias
Secondary 95%
Primary 5%Familial & genetic

Dr.Sarma@works
40
Secondary Hyperlipidemia
↑ LDL Cholesterol ↑ TGNephrotic syndrome. ObesityHypothyroidism DiabetesObstr. liver disease UremiaAnorexia nervosa Alcoholism, SmokingAcute Int. Porphyria Oral contraceptivesProgestogens Beta blockersThiazides PregnancyAnabolic steroids Steroids, Thiazides

Dr.Sarma@works
41
Clinical Action
• Presence of secondary causes of Hyperlipidemia– Order for full lipid profile (LP) – HT also
• Presence of hyperlipidemia – increased TG or EC– Investigate for all secondary causes
• For all above 20 years once in every 5 years • For those above 45 yrs – once in 2 years• For those with already known lipid abnormality
follow-up every 3-6 months • Extended Lipid profile includes Homocysteine,
LP(a), SD-LDL, ALP, Apo A and Apo B, HS-CRP

Dr.Sarma@works
42
Clinical Photoes
Tuberous xanthoma. Flat-topped, yellow, firm tumor
Xanthelasma. Multiple, longitudinal, creamy-orange, slightly elevated papules on eyelids .

Dr.Sarma@works
43
Clinical Photoes
Tendinous xanthomas. Large sub-cutaneous tumors adherent to the Achilles tendons.
Papular eruptive xanthomas. Multiple, discrete, red-to-yellow confluent papules

Dr.Sarma@works
44
Evaluation
1. History of eruptive xanthomas, Abd. pain
2. H/o wt. gain, DM, estrogens, Alcohol, Ex.
3. Fasting Lipid profile (TC, LDL, HDL, TG)
4. OGTT, TSH, Liver & Renal Function tests
5. CHD assessment by ECG, TMT, Angio
6. Risk factor assessment, Family H/o P.CHD

Dr.Sarma@works
45
Treatment Strategy
Lipid Profile, Risk Assessment
LDL > 100 Look For Sec. CausesTreat the cause, if found
Treatment
Sec. PreventionPrimary Prevention
High Risk Low Risk
LDL < 130
LDL <160
CHD +
NO CHD
< 2 RF 2 or more RF
LDL > 100

Dr.Sarma@works
46
Treatment Plan - LDLc
Clinical Status Goal Diet Drugs
No CHD< 2 RF
<160 >160 >190
No CHD2 or more RF
<130 >130 >160
CHD Present <100 >100 >130
For Indians all the values must be 20 mg less

Dr.Sarma@works
47
Treatment Options
• Diet – Two step approach• Drug therapy
1. HMG¢ co A Reductase Inhibitors2. Fibric Acid derivatives3. Nicotinic Acid4. Ezetimibe5. Bile Acid binding Resins (BAR)6. Probucol
¢ HMG is Hydroxy Methyl Glutaryl

Dr.Sarma@works
48
New Treatments
Drug therapy
1. Colesevelam (BAR)
2. Phytosterols
3. Avasimibe – ACAT inhibitor
4. Torcetrapib – CETP inhibitor
5. Drugs decreasing Apo B synthesis

Dr.Sarma@works
49
Therapeutic Lifestyle Changes - TLC
Nutrient Recommended Intake• Saturated fat < 7% of calories• PUFA fat Up to 10% of calories• MUFA fat Up to 20% of calories• Total fat 25–35% of calories• Carbohydrate 50–60% of calories• Fiber 20–30 grams per day• Protein Approx. 15% of
calories• Cholesterol Less than 200 mg/day
DIETARY THERAPY
Dr.Sarma@works
50
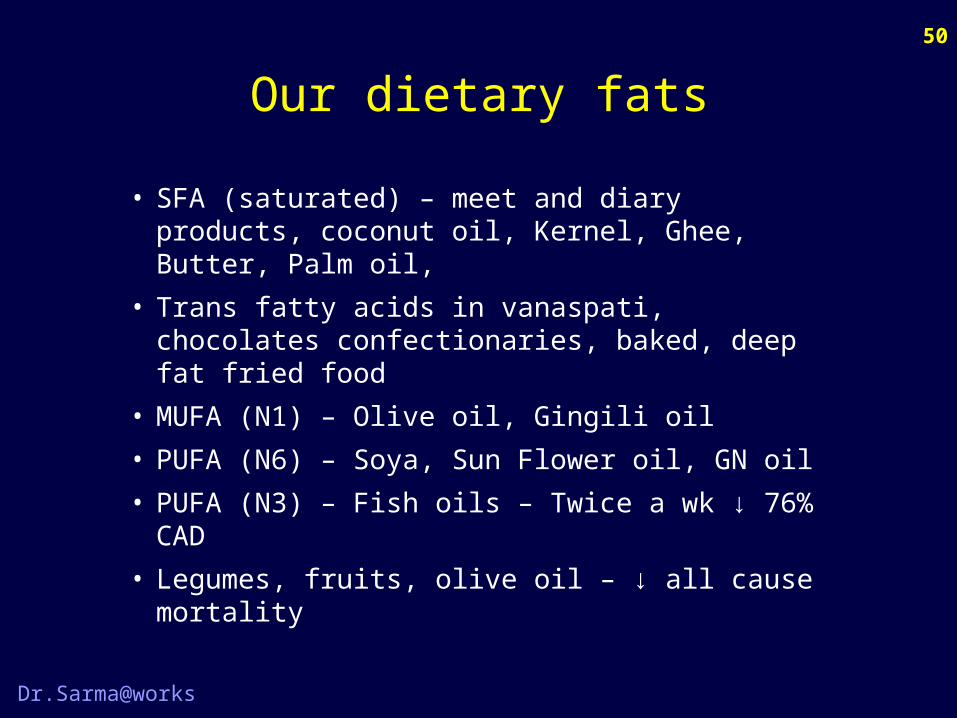
Our dietary fats
• SFA (saturated) – meet and diary products, coconut oil, Kernel, Ghee, Butter, Palm oil,
• Trans fatty acids in vanaspati, chocolates confectionaries, baked, deep fat fried food
• MUFA (N1) – Olive oil, Gingili oil• PUFA (N6) – Soya, Sun Flower oil, GN oil• PUFA (N3) – Fish oils – Twice a wk ↓ 76% CAD• Legumes, fruits, olive oil – ↓ all cause mortality

Dr.Sarma@works
51
Treatment of ↑ LDLc
High LDLcHigh LDLcHigh LDLcHigh LDLc
Therapeutic Lifestyle ChangeTherapeutic Lifestyle ChangeTherapeutic Lifestyle ChangeTherapeutic Lifestyle Change
Add on drug - EZ , Niacin, BARAdd on drug - EZ , Niacin, BARAdd on drug - EZ , Niacin, BARAdd on drug - EZ , Niacin, BAR
Therapy of Choice: StatinTherapy of Choice: StatinTherapy of Choice: StatinTherapy of Choice: Statin
Drug TherapyDrug TherapyDrug TherapyDrug Therapy

Dr.Sarma@works
52
Statins – Mechanism of Action
1.1. Reduce hepatic cholesterol synthesis (HMG CoA), Reduce hepatic cholesterol synthesis (HMG CoA),
2.2. lowering intracellular cholesterol,lowering intracellular cholesterol,
3.3. Upregulation of LDL receptor and Upregulation of LDL receptor and
4.4. ↑ ↑ the uptake of non-HDL from circulation.the uptake of non-HDL from circulation.
LDL receptorLDL receptor––mediated mediated hepatic uptake of LDL hepatic uptake of LDL and VLDL remnantsand VLDL remnants
Serum VLDL remnantsSerum VLDL remnants
Serum LDL-CSerum LDL-C
Cholesterol Cholesterol synthesissynthesis
LDL receptor LDL receptor
(B(B––E receptor) E receptor)
synthesissynthesisIntracellular Intracellular CholesterolCholesterol
Apo BApo B
Apo EApo E
Apo BApo B
Systemic CirculationSystemic CirculationHepatocyteHepatocyte
LDLLDL
Serum IDLSerum IDL
VLDLVLDLRRVLDLVLDLRR
VLDLVLDL
HMGCoA

Dr.Sarma@works
53
–45
CHD Risk Reduction – Statin Therapy
La Rosa JC et al. JAMA 1999;282:2340-2346.
EndpointsEndpoints +20 –35–30–250 –5 –10–15–20Relative Risk Reduction (%)
–40 –50
Major coronary events
Coronary deaths
Cardiovascular deaths
Noncardiovascular events
Total mortality
Strokes
Intermittent claudication
Angina

Dr.Sarma@works
54
Time course of Statin effects
* Time course establishedDaysDays YearsYears
LDL-C LDL-C lowered*lowered*
InflammationInflammationreducedreduced
VulnerableVulnerableplaquesplaques
stabilizedstabilized
EndothelialEndothelialfunctionfunctionrestoredrestored
IschemicIschemicepisodesepisodesreducedreduced
Cardiac eventsCardiac eventsreduced*reduced*
Dr.Sarma@works
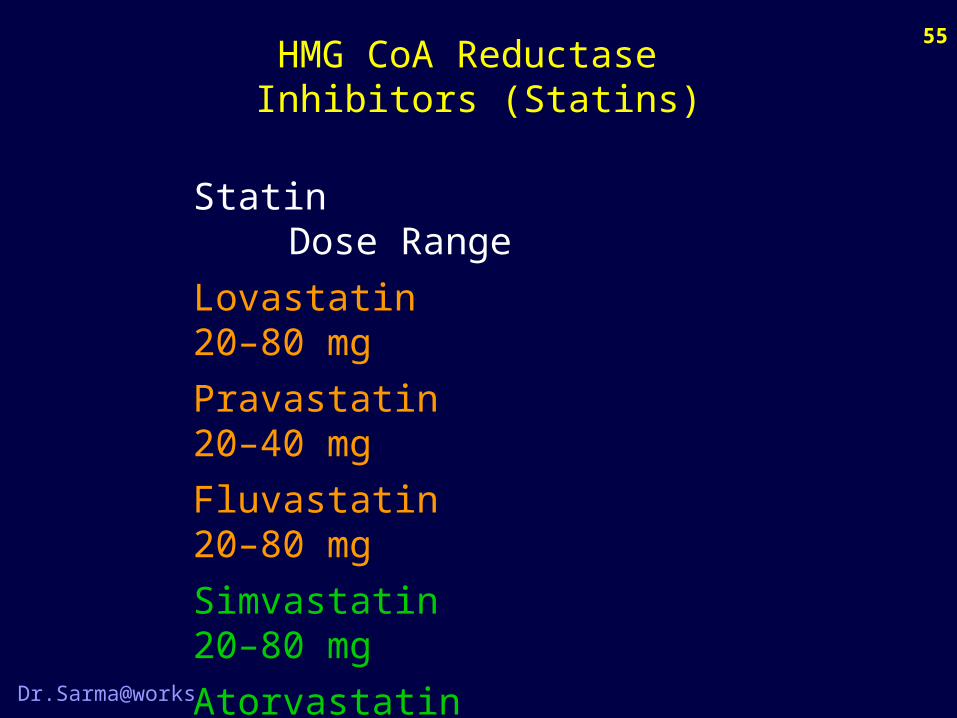
55HMG CoA Reductase
Inhibitors (Statins)
Statin Dose RangeLovastatin 20–80 mgPravastatin 20–40 mgFluvastatin 20–80 mgSimvastatin 20–80 mgAtorvastatin 10–80 mgRosuvastatin 5–20 mgCerivastatin 0.4–0.8 mg

Dr.Sarma@works
56
AtorvastatinAtorvastatin211 mg/dl*211 mg/dl*
SimvastatinSimvastatin219 mg/dl*219 mg/dl*
-60%
-50%
-40%
-30%
-20%
-10%
0%
Mea
n %
Cha
nge
from
Bas
e li n
eLDL-C Lowering - Statin Dose
Adapted from Jones P et al. Am J Cardiol 1998;81:582-587.
Daily DoseDaily Dose
10 mg
20 mg
40 mg
80 mg16% with16% with3 Titrations3 Titrations
13%13%
38%
46%
51%54%
28%
35%
41%

Dr.Sarma@works
57
HMG CoA Reductase Inhibitors (Statins)
Common side effects Headache, Myalgia, Fatigue, GI intol. Flu-like symptoms
Increase in liver enzymes – serious problems are very rare Occurs in 0.5 to 2.5% of cases in dose-dependent manner
Myopathy occurs in 0.2 to 0.4% of patients Rare cases of Rhabdomyolysis We can reduce this risk by Cautiously using statins in impaired renal function Using the lowest effective dose Cautiously combining statins with fibrates Muscle toxicity requires the discontinuation of statin

Dr.Sarma@works
58
Short falls of Statins
Effectiveness and community impact are to be improved
Rebound increase in lipids and ↑ of events after withdrawal of statin Rx.
High rate of discontinuation by patients
Differences in the efficacy of different statins
They reduce only endogenous lipids – Individual variation
Modest effect on TG and HDL, No effect on Lp(a)
No effect on chylomicrons; escape phenomenon

Dr.Sarma@works
59
LymphLymphLymphLymph EnterocyteEnterocyteEnterocyteEnterocyte IntestinalIntestinalLumenLumen
IntestinalIntestinalLumenLumen
Ezetimibe
Cholesterol
NPC1L1
CholesterylEster ABCG5/G8
ACAT
Ezetimibe
XX

Dr.Sarma@works
60
Dual Inhibition
DuodenumDuodenumDuodenumDuodenum
JejunumJejunumJejunumJejunum
IleumIleumIleumIleum
CMapoB48
LiverLiverLiverLiver
CM RemnantapoB48
VLDLapoB100
Ezetimibe
XX
LDLapoB100
XXStatinStatin
ColonColonColonColon

Dr.Sarma@works
61
Ezetimibe Efficacy (“10 + 10 = 80”)
Ballantyne CM et al. Circulation 2003;107:2409-2415.
Atorvastatin40 mg(n=66)
20 mg(n=60)
10 mg(n=60)
Me a
n %
Cha
n ge
in L
DL-C
f ro m
Bas
e li n
e
–53%
–37%–42%
–45%
–54%
P < 0.01P < 0.01
80 mg(n=62)
-60%
-50%
-40%
-30%
-20%
-10%
0%
Ezt + Ator10+10 mg
(n=65)

Dr.Sarma@works
62
Bile Acid Resins: Mechanism of Action
Net Effect - Net Effect - LDL-CLDL-CNet Effect - Net Effect - LDL-CLDL-C
Gall BladderGall Bladder
LDL ReceptorsLDL Receptors
VLDL and LDL removalVLDL and LDL removal
Cholesterol 7-Cholesterol 7- hydroxylase hydroxylase
Conversion of cholesterol to BAConversion of cholesterol to BA
BA SecretionBA Secretion
LiverLiver
BA ExcretionBA Excretion
Terminal IleumTerminal Ileum
Bile AcidBile Acid
Enterohepatic RecirculationEnterohepatic Recirculation
Reabsorption of Reabsorption of bile acidsbile acids

Dr.Sarma@works
63
Bile Acid Resins (BAR)
Major actions• Reduce LDLc by 15–30%• Raise HDLc by 3–5%• May increase TG
Side effects• GI distress / constipation / nausea• Decreased absorption of other drugs
Contra indications• Dysbetalipoproteinemia,• Biliary Obstruction• Raised TG (especially >400 mg/dL)

Dr.Sarma@works
64
Bile Acid Resins
Drug Dose Range
Cholestyramine 4–16 g
Colestipol 5–20 g
Colesevelam 2.6–3.8 g

Dr.Sarma@works
65
Treatment of ↓ HDLc
Low HDLcLow HDLcLow HDLcLow HDLc
Therapeutic Lifestyle ChangeTherapeutic Lifestyle ChangeTherapeutic Lifestyle ChangeTherapeutic Lifestyle Change
Add on drug - FinofibrateAdd on drug - FinofibrateAdd on drug - FinofibrateAdd on drug - Finofibrate
Therapy of Choice : NiacinTherapy of Choice : NiacinTherapy of Choice : NiacinTherapy of Choice : Niacin
Drug TherapyDrug TherapyDrug TherapyDrug Therapy

The CADI study [Coronary Artery Disease in Asian Indians]
14% of Asian Indian males & 5% of females have Optimal HDL
Prevalence of coronary heart disease and its risk factors in Asian Indians
Atherosclerosis , Rosemount , IL Oct 6-11 , 1991
120
86
100
80604020
0 14
95
5
Asian Indian males
Asian Indian females
% with < optimal level of HDL-C
% with an optimal HDL-C levels
In Indian patients with CAD, High TG levels are
found more often than high cholesterol levels.
Journal, Ind. Acad. clin. med vol 2 Jul-Sept 2001

Dr.Sarma@works
67
Causes of Low HDL
Smoking
Obesity (visceral fat), Physical inactivity
Very high Carbohydrate diet
Type II Diabetes
Hyper-triglyceridemia
Drugs like beta-blockers, androgenic steroids
and androgenic progestins

Dr.Sarma@works
68
Nicotinic Acid – Mechanism of Action
LiverLiver CirculationCirculationHDLHDL
Serum VLDL Serum VLDL results in reduced results in reduced lipolysis to LDL lipolysis to LDL
Serum LDLSerum LDL
VLDL
Decreases hepatic production of VLDL and of apo BDecreases hepatic production of VLDL and of apo B
VLDL VLDL secretionsecretion
Apo BApo B
HepatocyteHepatocyte Systemic CirculationSystemic Circulation
Mobilization of FFAMobilization of FFA
TG TG synthesissynthesis
VLDL
LDL

Dr.Sarma@works
69
Effect of Niacin on Lipoproteins
Adapted from Knopp RH. N Engl J Med 1999;341:498-511..
0 1 g / d 2 g / d 3 g / d
Baseline
-15%
12.5%
25%
-30%
HDL-C with NiaspanHDL-C with Niaspan®®
TG with NiaspanTG with Niaspan®®
TG with crystalline niacinTG with crystalline niacin
LDL-C with NiaspanLDL-C with Niaspan®®
LDL-C with crystalline niacinLDL-C with crystalline niacin
35%HDL-C with crystalline niacinHDL-C with crystalline niacin

Dr.Sarma@works
70
Nicotinic Acid Products availableProducts available
Immediate-release, 2–4 g/d, Sustained Release 3 g /dImmediate-release, 2–4 g/d, Sustained Release 3 g /d Extended-release (NiaspanExtended-release (Niaspan®®) 1–2 g/d) 1–2 g/d
Best agent to raise HDL-CBest agent to raise HDL-C Reduces coronary events Reduces coronary events Adverse effectsAdverse effects
Flushing, itching, headache (immediate-release, NiaspanFlushing, itching, headache (immediate-release, Niaspan®®)) Hepatotoxicity, GI (sustained-release)Hepatotoxicity, GI (sustained-release) Activation of peptic ulcerActivation of peptic ulcer Hyperglycemia and reduced insulin sensitivityHyperglycemia and reduced insulin sensitivity
ContraindicationsContraindications Active liver disease or unexplained LFT elevationsActive liver disease or unexplained LFT elevations Peptic ulcer diseasePeptic ulcer disease

Coronary heart disease and HDL-CFramingham Heart Study
Coronary heart disease and HDL-CFramingham Heart Study
Gordon, Castelli et al. Am J Med 1977; 62: 707–714Gordon, Castelli et al. Am J Med 1977; 62: 707–714
0
50
100
150
200
Rat
e/10
00
<25 25–34 35–44 45–54 55–64 65–74 75+
HDL-C (mg/dl)
Women
Men
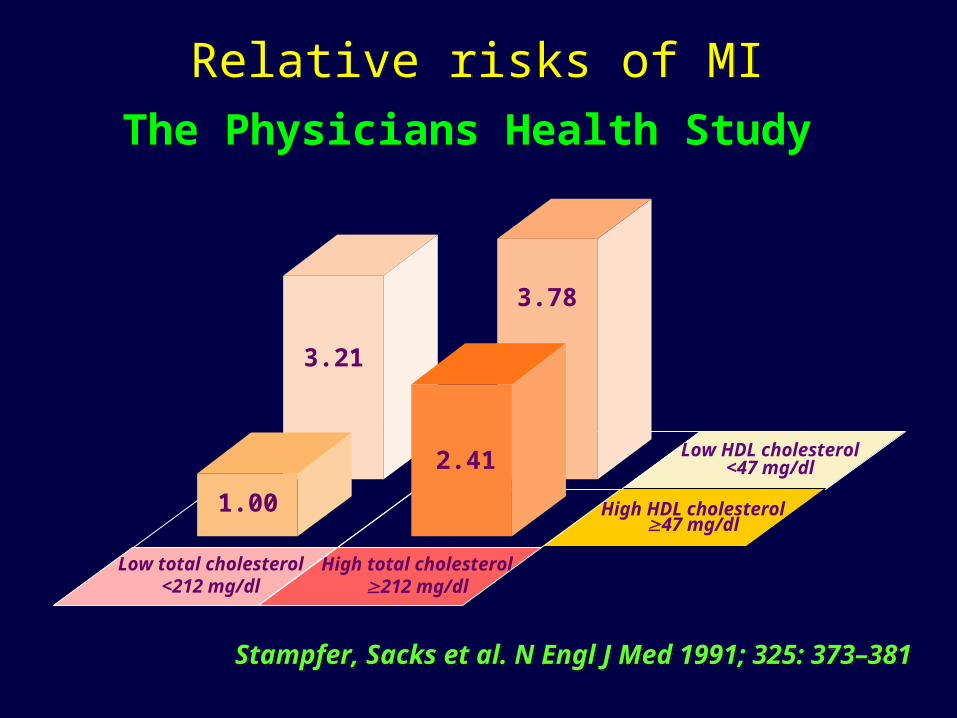
Relative risks of MIRelative risks of MI
3.21
3.78
1.00
2.41 Low HDL cholesterol<47 mg/dl
High HDL cholesterol47 mg/dl
Low total cholesterol<212 mg/dl
High total cholesterol212 mg/dl
Stampfer, Sacks et al. N Engl J Med 1991; 325: 373–381Stampfer, Sacks et al. N Engl J Med 1991; 325: 373–381
The Physicians Health Study

HDL-C vs LDL-C as a predictor of CHD risk
HDL-C vs LDL-C as a predictor of CHD risk
*Men aged 50–70 Gordon, Castelli et al. Am J Med 1977; 62: 707–714Gordon, Castelli et al. Am J Med 1977; 62: 707–714
100 mg/dl 160 mg/dl 220 mg/dl0
0.5
1
1.5
2
2.5
3
Risk of CAD over 4years of follow-up*
LDL-C
85 mg/dl
65 mg/dl
45 mg/dl
25 mg/dl
CHD RR
HDL-C

Dr.Sarma@works
74
LDL cholesterol is primary target of therapy
Weight reduction and increased physical activity (if the metabolic syndrome is present)
Non-HDL cholesterol is secondary target of therapy (if triglycerides 200 mg/dL)
Consider nicotinic acid or fibrates (for patients with CHD or CHD risk equivalents)
Management of Low HDLc
Dr.Sarma@works
75
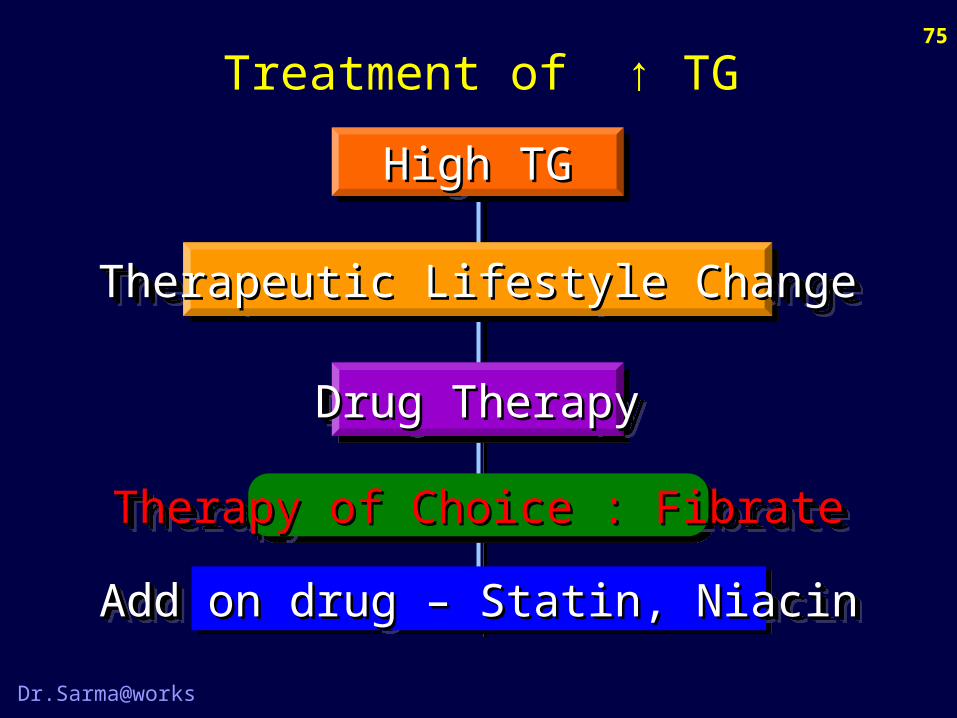
Treatment of ↑ TG
High TGHigh TGHigh TGHigh TG
Therapeutic Lifestyle ChangeTherapeutic Lifestyle ChangeTherapeutic Lifestyle ChangeTherapeutic Lifestyle Change
Add on drug – Statin, NiacinAdd on drug – Statin, NiacinAdd on drug – Statin, NiacinAdd on drug – Statin, Niacin
Therapy of Choice : FibrateTherapy of Choice : FibrateTherapy of Choice : FibrateTherapy of Choice : Fibrate
Drug TherapyDrug TherapyDrug TherapyDrug Therapy

Dr.Sarma@works
76
Treatment Strategy
Fasting TG Level TG < 150
↑Fasting TG LevelNormal
< 2 RF
TG >150, No CHD
TG > 150, CHD +
TG > 500, CHD +/-
Diet Modify
Diet + Fibrate
2 or > RF
Diet + Fibrate + Niacin
Diet + Fibrate + Statin

Dr.Sarma@works
77
Triglycerides
TG Level Classification Treatment
< 150 mg% Normal TG No Rx.
150 to 200 mg% Borderline high Diet alone
201 to 500 mg% High Diet + drugs
> 500 mg% Very high Diet + Intensive Rx
NCEP 2002 Guidelines by expert panel on TG

Fenofibrate Fenofibrate
Mode of Action
Enhances the activity of lipoprotein lipase
Reduces hepatic fatty acid synthesis
Inhibits HMG co-enzyme A reductase activity
Reduces the CETP activity
Increases the LCAT activity
Increases the production of Apo AI and Apo A II
Mode of Action
Enhances the activity of lipoprotein lipase
Reduces hepatic fatty acid synthesis
Inhibits HMG co-enzyme A reductase activity
Reduces the CETP activity
Increases the LCAT activity
Increases the production of Apo AI and Apo A II

Dr.Sarma@works
79
Fibric Acid Derivatives
• Major actions– Lower TG 20–50%,↓VLDL synthesis– Raise HDL-C 10–20%– ↓ LDL (TG is N), ↑ LDL (TG is ↑)– Increase the SDL particle size (less athero)
• Side effects Dyspepsia, gallstones, myopathy, Abn. LFT• Contraindications Severe renal or hepatic / biliary disease

Dr.Sarma@works
80
Fibric Acid Derivatives
Drug DoseClofibrate 1000 mg BIDBezafibrate 200 mg BIDGemfibrozil 600 mg BIDFenofibrate 200 mg ODFenofibrate micronized 160 mg OD

Dr.Sarma@works
81
Treatment of ↑ LDL + ↑ TG
CombinedCombinedCombinedCombined
Therapeutic Lifestyle ChangeTherapeutic Lifestyle ChangeTherapeutic Lifestyle ChangeTherapeutic Lifestyle Change
Add on drug – Niacin, BARAdd on drug – Niacin, BARAdd on drug – Niacin, BARAdd on drug – Niacin, BAR
Therapy of Choice : Statin + FibrateTherapy of Choice : Statin + FibrateTherapy of Choice : Statin + FibrateTherapy of Choice : Statin + Fibrate
Drug TherapyDrug TherapyDrug TherapyDrug Therapy

Dr.Sarma@works
82
Da Col PG et al. Curr Ther Res Clin Exp 1973;53:473-482.
Statin + Fibrate
-60
-50
-40
-30
-20
-10
0
10
20
30
Simva +Simva +GemfibrozilGemfibrozil
––50%50%––39%39%
16%16%22%22%
––41%41%
––28%28%
Ator or Simva +Ator or Simva +FenofibrateFenofibrate
230230 332332
3838
191191166166
LDLLDLTGTG
HDLHDL
LDLLDL
TGTG
HDLHDL
Perc
ent C
hang
ePe
rcen
t Cha
nge
3434

Dr.Sarma@works
83
Statin + Fibrate – Precautions
Use statin alone for non-HDL-C goalsUse statin alone for non-HDL-C goals
Use fish oils or niacin rather than fibratesUse fish oils or niacin rather than fibrates
Keep the doses of the statin and fibrate lowKeep the doses of the statin and fibrate low
Dose the fibrate in the AM and the statin in the PMDose the fibrate in the AM and the statin in the PM
Avoid (or cautiously use) combo in renal impairmentAvoid (or cautiously use) combo in renal impairment
Teach the patient to recognize muscle symptomsTeach the patient to recognize muscle symptoms
Discontinue therapy if muscle symptoms are present Discontinue therapy if muscle symptoms are present and CK is >10 times the upper limit of normaland CK is >10 times the upper limit of normal

Dr.Sarma@works
84
Probucol
1. Probucol (Lorelco) 500mg b.i.d with food
2. Third line drug – erratic effect on LDL & HDL
3. Lowers Cholesterol and the only drug which regresses xanthomas
4. It is an antioxidant of LDL
5. Diarrohea, flatulence, nausea, increases QTc
6. Can be combined with BAR
Dr.Sarma@works
85
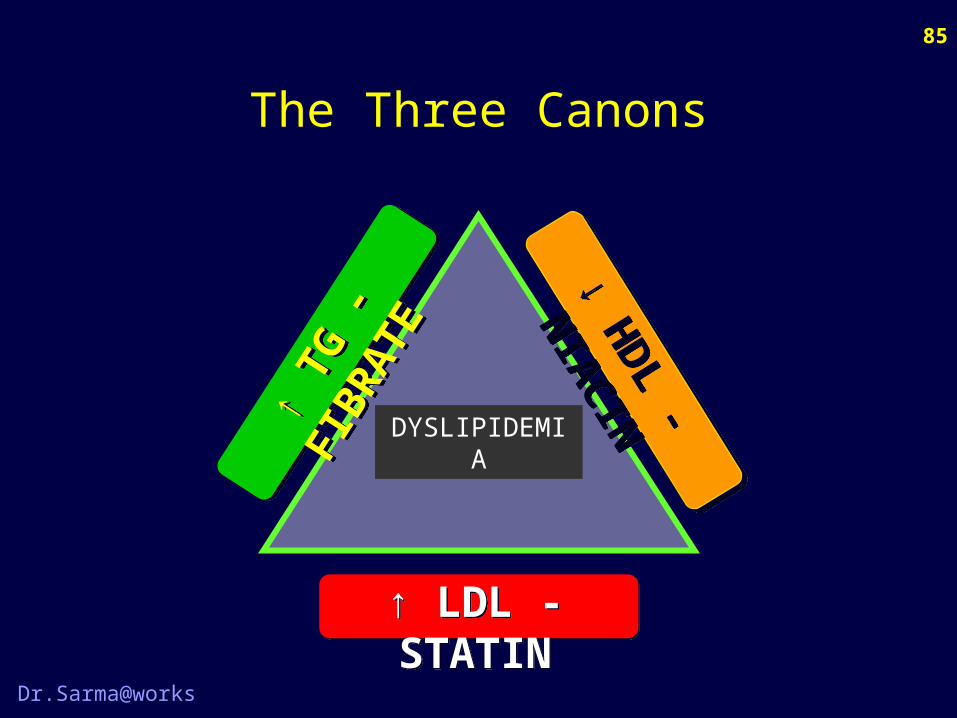
The Three Canons
↑ LDL - STATIN↑ LDL - STATIN
↑ TG
- FI
BRAT
E
↑ TG
- FI
BRAT
E ↓ HDL - NIACIN
↓ HDL - NIACINDYSLIPIDEMIA

Dr.Sarma@works
86
Summary of Drug choice
Lipid abnormality type First choice Additional Remarks
↑ LDL Statin Ezetimibe Myopathy ↑
↑ TG Fibrate Niacin ↓ CHO intake
↓ HDL Niacin Fibrate Exercise
↑ LDL + ↑ TG Statin + Fibrate Niacin Myo risk ↑ ↑
↑ LDL + ↓ HDL Statin + Niacin Fibrate Exercise
↑ TG + ↓ HDL Fibrate + Niacin Statin Exercise
↑ LDL + ↑ TG + ↓ HDL Statin + Fibrate E, N, BA, FO Myo risk ↑ ↑ ↑

Atherogenecity of small, dense LDLAtherogenecity of small, dense LDL
SDL is highly atherogenic. It
Generates free radicals
Increases trans endothelial filtration
Increases susceptibility to oxidation
Reduces affinity for the LDL receptor
Increased binding to intimal proteoglycan
↑ Formation of pro-aggregators / vasoconstrictors
Impaired in vivo ED independent of HDL, LDL, TGCirculation, 2000, 102: 716-721
SDL is highly atherogenic. It
Generates free radicals
Increases trans endothelial filtration
Increases susceptibility to oxidation
Reduces affinity for the LDL receptor
Increased binding to intimal proteoglycan
↑ Formation of pro-aggregators / vasoconstrictors
Impaired in vivo ED independent of HDL, LDL, TGCirculation, 2000, 102: 716-721
Dr.Sarma@works
88
Lp(a) or Little‘a’
• Similar to LDL molecule• Apo B + additional Apo ‘a’ attached by S=S bond• Primary determinant is genetic• Normal value 20 mg %, > 30 high risk• It competes with plasminogen because of its
structural similarity and so interferes with plasmin synthesis and thrombolytic pathway
• Nicotinic acid, ? Bezafibrate, Estrogens ↓it

This ALP or phenotype B is present and seen in most often• Insulin resistant individuals
• Diabetics
• Obese persons
• Sedentary life style
More prevalent in India
Apo A I ÷ Apo B will be < 1
Phenotype B or ALP

0
10
20
30
40
50
60
70
80
90
100
20 40 60 80 100 120 140 160 180 200 220 240 260 280 300 500
Phenotype A
Phenotype B
% Cumulativefrequency
TG (mg/dL)
Cumulative Distribution of TG Levels Phenotypes A and B
Cumulative Distribution of TG Levels Phenotypes A and B
Austin M et al. Circulation. 1990;82:495-506.

20 25 30 35 40 45 50 55 60 65 70 75 80
Phenotype A
Phenotype B
% Cumulativefrequency
HDL-C (mg/dL)
100
90
80
70
60
50
40
30
20
Cumulative Distribution of HDL levels Phenotypes A and B
Cumulative Distribution of HDL levels Phenotypes A and B
Austin M et al. Circulation. 1990;82:495-506.

Metabolic Syndrome - Characteristics
HypertriglyceridemiaLow HDL-cholesterolElevated apolipoprote in BSmall, dense LDL particlesInflammatory profile
Insulin resistanceHyperinsulinem iaGlucose intoleranceImpaired fibrino lysisEndothelial dysfunction
These features can lead to type 2 diabetes,
hypertension and cardiovascular disease

The interaction between our current genotype and
our present day life style and eating habits places us
at very high risk of having this phenotype B that
makes us highly susceptible to Atherosclerosis.
Journal of Internal Medicine 2003:254(2):114-25

ATP-III Criteria for Metabolic Syndrome
Abdominal obesity (waist circumference): men >100 cm (40 in); women >88 cm (35 in)
Triglycerides > 150 mg/dl
HDL cholesterol: men < 40 mg/dl; women < 50 mg/dl
Blood pressure > 130/ 85 mmHg.
Fasting glucose > 110 mg/dl
Diagnosis of metabolic syndrome is made when 3 or more of the risk determinants shown above are present.

Dr.Sarma@works
95
Homocysteine
• Normal value is up to 15 μ mols./L• Folic acid, Vitamin B6 and B12 are essential for
the normal transulfuration and remethylation cycles
• Excess of homocystine generates oxidative stress on the cell membranes. DNA and protein denaturation through ROS formation
• Folic acid 5 mg/ day + Vit. B6 and B12 are to be given on regular basis

Dr.Sarma@works
96
Summary of Drug choice
Lipid abnormality type Advised Rx. Remarks
↑ Homocysteine Folic acid B6 + B12 helps
↑ Small dense LDL Statin + Fibrate Aggressive Rx.
↑ Little ‘a’ or LP(a) Niacin Statin no effect
↑ Phenotype B Under research DM, Obesity ↓
↓ in Phenotype A Under research Aerobic exercise

Dr.Sarma@works
97
Some Brand Names
Drug class Brand name
Atorvastatin TG-TOR, Storvas, Avastin, Atcor
Simvastatin Sim, Simvotin, Simcard, Simvas
Atorvastatin + Ezetimibe TG tor Z, Storvas Z,
Ezetimibe Ezedoc, Ezee, Ezet
Fenofibrate Lipicard, Fibrate, Finolip, Stanlip
Gemfibrozyl Lopid, Lipizyl, Normolip, Losterol
Niacin Niasyn, Nialip, Nicocin

Dr.Sarma@works
98
Atherosclerosis and IR and DM
HypertensionHypertension
ObesityObesity
HyperinsulinemiaHyperinsulinemia
DiabetesDiabetes
HypertriglyceridemiaHypertriglyceridemia
Small, dense LDLSmall, dense LDL
Low HDLLow HDL
HypercoagulabilityHypercoagulability
InsulinInsulinResistanceResistance
InsulinInsulinResistanceResistance AtherosclerosisAtherosclerosisAtherosclerosisAtherosclerosis

Dr.Sarma@works
99
Elevated TG Elevated VLDL Reduced HDL-C Increase in SD-LDL Decrease in Apo A I Increase in Apo B Ratio of Apo A I / Apo B < 1
Dyslipidemia in IR and DM
All Diabetics must be given STATIN

Dr.Sarma@works
100
Diabetes Treatment and Lipids
Type Rx used Effect on lipids
1. Insulin Favourable
2. Metformin Mildly favourable
3. Sulfonylureas Not favourable
4. Glitazones Favourable
5. Acarbose No effect

Dr.Sarma@works
101
Hypertension Treatment and Lipids
Type Rx used Effect on lipids
1. Diuretics Unfavourable
2. Indapamide Mildly favourable
3. ACEi and ARB Very favourable
4. Betablockers Unfavourable
5. Ca channel blockers No effect

Dr.Sarma@works
102
Who is to be blamed ??
We do not care at all to We soon end up having
Restrict diet, over eat CHO, sweet toothed Over weight and obesity
Eat more fruits, fiber, vegetables Atherosclerosis and AVD
Avoid fatty, crunchy, munchy tasty food Dyslipidemia and CHD
Avoid salty, savory, preserved food, NV Hypertension, CVA
Do the minimum required exercise Diabetes, IR, ↓ HDL, OA
Take enough milk and milk products, Ca Osteoporosis & fractures
Quit smoking and abstain from alcohol What not !
Control worry, anger, vengeance, jealousy Mental & physical illness

Where are we heading ? ?
Journal of internal medicine 2003:254(2):114-25
20000 B.C. 2004
Hunting-gatheringsubsistence
High level ofphysical activity
Processedfoods
Animal fatsand glucidesDietary fibre¯
Sedentary life
Paleolithic sup. age Neolithic age 19th century 21st century
Thrifty genotype Susceptibility genotype
Technology has changed a lot in the way we live
But, we have not altered our life style

We have to pay the very heavy price !!
What could be prevented, we treat or leave

Dr.Sarma@works
105
Web Resources on Lipids
www.lipidsonline.org
www.hypertensiononline.org
www.ncbi.nlm.nih.gov
www.univ baylor.org

Dr.Sarma@works
106
CD ROM Available
The contents of today’s presentation
are available in a CD-ROM format
for computer and VCD player use.
This CD, in addition, contains our talks on
ECG, Asthma, COPD, Hypertension Rx. also

Dr.Sarma@works
107
Wishing YOU all
A HAPPAY NEW YEAR
Related Documents