From the American Venous Forum DNA-array of gene variants in venous leg ulcers: Detection of prognostic indicators Donato Gemmati, PhD, a,b Federica Federici, PhD, a,b Linda Catozzi, PhD, a,b Sergio Gianesini, MD, b Giovanna Tacconi, MD, b Gian L. Scapoli, MD, a,b and Paolo Zamboni, MD, b Ferrara, Italy Objective: Wound healing in venous leg ulcer (VLU) is a multi-step process involving complex pathways. Scanty knowledge at molecular level hinders clinical assessment and treatment. Anomalous handling of local iron overload, as well as unbalancing in matrix metalloproteinases (MMPs) and transglutaminase, has a recognized role in VLU establishment. We selected a number of single nucleotide polymorphisms (SNPs) in candidate genes (HFE, FPN1, MMP12, and FXIII) involved in VLU to identify potentially prognostic markers by means of DNA-array technology. Methods and Results: The DNA-array-genotyping was assessed in 638 subjects for the following SNPs: HFE (C282Y, H63D), FPN1 (8CG), MMP12 (82AG) and FXIII (V34L). Of the subjects, 221 were affected by VLU (171 primary and 50 post-thrombosis), 112 by severe chronic venous disease (CVD) (CEAP, C3-C4), while 305 were matched healthy controls. The HFE and FXIII SNPs had been previously genotyped by conventional polymerase chain reaction (PCR)-methods on the same group of subjects (J Vasc Surg 2005;42:309; J Vasc Surg 2006;44:554; J Vasc Surg 2006;44:815). For the purpose of DNA-array, they were re-genotyped by means of array-techniques resulting in a 100% matching. Intergroup statistical comparisons were performed. In the risk computation, the FPN1 8GG genotype had an overall CVD risk of 4.3 (95% CI, 1.6-12) and a VLU risk of 5.2 (95% CI, 1.9-15) virtually the same among primary VLU (4.98; 95% CI, 1.82-14.9). The MMP12 82AA genotype had a VLU risk of 1.96 (95% CI, 1.18-3.2) only in primary VLU (P .01). In the genotype-ulcer size association studies, from a subgroup of 167 cases, we observed a smaller mean ulcer size in the MMP12 GG-genotype compared with the other genotypes (P .001). Combining the present results with our previous published data on the same population, we suggest them to apply as tentative prognostic indicators in primary CVD. Conclusion: By analyzing simultaneously selected SNPs, it might be possible to glean precious information in predicting VLU onset or in stratifying patients according to their potential to heal. Although significant, our findings must be considered preliminary and the proposed prognostic indicators considered with caution, before ulterior more extensive studies in different populations can eventually confirm the present findings. ( J Vasc Surg 2009;50:1444-51.) Clinical Relevance: The DNA-array evaluation could be added to clinical CVD assessment. By analyzing simultaneously selected SNPs, it is possible to have precious information in predicting VLU onset or in stratifying patients according to their potential to heal. Prevention program in primary CVD could be improved by using DNA-array evaluation in initial patient assessment. Our results must be handled with extreme caution before considering them as prognostic indicators in VLU, and further larger studies in different populations are mandatory. Among the major complications of chronic venous disease (CVD), venous leg ulcer (VLU) is one of the most severe. It accounts for a significant proportion of lower extremity wounds and is a widespread pathologic condition in developed countries. 1,2 Several conditions influence and exacerbate VLU such as diabetes mellitus, rheumatoid ar- thritis, trauma, sickle cell disease, vasculitis, and skin tumor. Both in Europe and in the United States, the prevalence of VLU is about 1%, with relative high costs for assistance and treatment. The cost is estimated at $1 billion per annum in the United States, while in the United Kingdom 14% of health costs are apportioned to wound care. 3 Gender, age, ethnicity, and environment strongly influence penetrance of disease. 2,4,5 Regardless of the clinical strategy used, evident variations in the outcome in patients with similar disease pattern and treatment are observed. 6 Therefore, apart from CVD, increasing age and female gender, irrefut- able evidence of predisposition to VLU is still limited and elusive. As regards to genetics, candidate genes could po- tentially be those involved in inflammatory processes, fibro- blast growth factors, angiogenesis, or apoptosis. However, a recent paper comparing healing vs nonhealing lesion expression profiles found that none of the assumed genes involved in wound repair (ie, platelet-derived growth fac- tors [PDGF] or keratinocyte growth factor [KGF]) were significantly downregulated in nonhealing ulcers. 7 In recent years, hypothetical molecular mechanisms have been sug- gested, by means of which local iron overload facilitates the development of VLU. This model has been compared to other iron-driven lesions in neurodegenerative disorders. 8,9 From the Haemostasis & Thrombosis Center, a and the Vascular Disease Center, b University of Ferrara. This study was supported in part by funds from MIUR (the Italian Ministry for University Instruction and Research) and thanks to a grant from Fondazione Cassa di Risparmio - Cento, Italy. Competition of interest: none. Reprint requests: Donato Gemmati, PhD, Haemostasis & Thrombosis Center, Biomedical Sciences & Advanced Therapies, Unit of Haematol- ogy, University of Ferrara, C. So Giovecca 203, I-44100 Ferrara, Italy (e-mail: [email protected]). The editors and reviewers of this article have no relevant financial relation- ships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a competition of interest. 0741-5214/$36.00 Copyright © 2009 by the Society for Vascular Surgery. doi:10.1016/j.jvs.2009.07.103 1444

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

From the American Venous Forum
DNA-array of gene variants in venous leg ulcers:Detection of prognostic indicatorsDonato Gemmati, PhD,a,b Federica Federici, PhD,a,b Linda Catozzi, PhD,a,b Sergio Gianesini, MD,b
Giovanna Tacconi, MD,b Gian L. Scapoli, MD,a,b and Paolo Zamboni, MD,b Ferrara, Italy
Objective: Wound healing in venous leg ulcer (VLU) is a multi-step process involving complex pathways. Scantyknowledge at molecular level hinders clinical assessment and treatment. Anomalous handling of local iron overload, aswell as unbalancing in matrix metalloproteinases (MMPs) and transglutaminase, has a recognized role in VLUestablishment. We selected a number of single nucleotide polymorphisms (SNPs) in candidate genes (HFE, FPN1,MMP12, and FXIII) involved in VLU to identify potentially prognostic markers by means of DNA-array technology.Methods and Results: The DNA-array-genotyping was assessed in 638 subjects for the following SNPs: HFE (C282Y,H63D), FPN1 (�8CG), MMP12 (�82AG) and FXIII (V34L). Of the subjects, 221 were affected by VLU (171 primaryand 50 post-thrombosis), 112 by severe chronic venous disease (CVD) (CEAP, C3-C4), while 305 were matched healthycontrols. The HFE and FXIII SNPs had been previously genotyped by conventional polymerase chain reaction(PCR)-methods on the same group of subjects (J Vasc Surg 2005;42:309; J Vasc Surg 2006;44:554; J Vasc Surg2006;44:815). For the purpose of DNA-array, they were re-genotyped by means of array-techniques resulting in a 100%matching. Intergroup statistical comparisons were performed. In the risk computation, the FPN1 �8GG genotype had anoverall CVD risk of 4.3 (95% CI, 1.6-12) and a VLU risk of 5.2 (95% CI, 1.9-15) virtually the same among primary VLU(4.98; 95% CI, 1.82-14.9). The MMP12 �82AA genotype had a VLU risk of 1.96 (95% CI, 1.18-3.2) only in primaryVLU (P � .01). In the genotype-ulcer size association studies, from a subgroup of 167 cases, we observed a smaller meanulcer size in the MMP12 GG-genotype compared with the other genotypes (P � .001). Combining the present results withour previous published data on the same population, we suggest them to apply as tentative prognostic indicators inprimary CVD.Conclusion: By analyzing simultaneously selected SNPs, it might be possible to glean precious information in predictingVLU onset or in stratifying patients according to their potential to heal. Although significant, our findings must beconsidered preliminary and the proposed prognostic indicators considered with caution, before ulterior more extensivestudies in different populations can eventually confirm the present findings. ( J Vasc Surg 2009;50:1444-51.)
Clinical Relevance: The DNA-array evaluation could be added to clinical CVD assessment. By analyzing simultaneouslyselected SNPs, it is possible to have precious information in predicting VLU onset or in stratifying patients according totheir potential to heal. Prevention program in primary CVD could be improved by using DNA-array evaluation in initialpatient assessment. Our results must be handled with extreme caution before considering them as prognostic indicators
in VLU, and further larger studies in different populations are mandatory.Among the major complications of chronic venousdisease (CVD), venous leg ulcer (VLU) is one of the mostsevere. It accounts for a significant proportion of lowerextremity wounds and is a widespread pathologic conditionin developed countries.1,2 Several conditions influence andexacerbate VLU such as diabetes mellitus, rheumatoid ar-thritis, trauma, sickle cell disease, vasculitis, and skin tumor.Both in Europe and in the United States, the prevalence of
From the Haemostasis & Thrombosis Center,a and the Vascular DiseaseCenter,b University of Ferrara.
This study was supported in part by funds from MIUR (the Italian Ministryfor University Instruction and Research) and thanks to a grant fromFondazione Cassa di Risparmio - Cento, Italy.
Competition of interest: none.Reprint requests: Donato Gemmati, PhD, Haemostasis & Thrombosis
Center, Biomedical Sciences & Advanced Therapies, Unit of Haematol-ogy, University of Ferrara, C. So Giovecca 203, I-44100 Ferrara, Italy(e-mail: [email protected]).
The editors and reviewers of this article have no relevant financial relation-ships to disclose per the JVS policy that requires reviewers to declinereview of any manuscript for which they may have a competition ofinterest.
0741-5214/$36.00Copyright © 2009 by the Society for Vascular Surgery.
doi:10.1016/j.jvs.2009.07.1031444
VLU is about 1%, with relative high costs for assistance andtreatment. The cost is estimated at $1 billion per annum inthe United States, while in the United Kingdom 14% ofhealth costs are apportioned to wound care.3 Gender, age,ethnicity, and environment strongly influence penetranceof disease.2,4,5 Regardless of the clinical strategy used,evident variations in the outcome in patients with similardisease pattern and treatment are observed.6 Therefore,apart from CVD, increasing age and female gender, irrefut-able evidence of predisposition to VLU is still limited andelusive. As regards to genetics, candidate genes could po-tentially be those involved in inflammatory processes, fibro-blast growth factors, angiogenesis, or apoptosis. However,a recent paper comparing healing vs nonhealing lesionexpression profiles found that none of the assumed genesinvolved in wound repair (ie, platelet-derived growth fac-tors [PDGF] or keratinocyte growth factor [KGF]) weresignificantly downregulated in nonhealing ulcers.7 In recentyears, hypothetical molecular mechanisms have been sug-gested, by means of which local iron overload facilitates thedevelopment of VLU. This model has been compared to
other iron-driven lesions in neurodegenerative disorders.8,9
JOURNAL OF VASCULAR SURGERYVolume 50, Number 6 Gemmati et al 1445
Few data on single nucleotide polymorphisms (SNPs)and VLU are available in literature.10-13 Our group re-cently acknowledged the patho-physiological role of irondeposition, iron trafficking genes, and transglutaminases inVLU establishment,14-20 recognizing a strong geneticcomponent in ulcer pathogenesis.21,22 In particular, thecommon HFE-C282Y and H63D SNPs play a role, respec-tively, in the risk of venous ulceration in primary CVD andin the modulation of the lesion onset.14,15 The same genevariants also show significant effects in healing time aftersuperficial venous surgery.17,21 On the other hand, wefound that additional SNPs could act as protective factors.Such is the case of the coagulation factor XIII gene (ie,FXIII V34L and P564L) acting on extracellular matrix(ECM) components and fibroblasts. Those variants show invivo and in vitro positive effects on wound healing, tissuerepairing, and remodelling.17-21
In the present paper, we investigated two additional SNPsin CVD patients, one in the promoter of the ferroportin gene(FPN1; �8CG), and another in the promoter of the matrixmetalloproteinase 12 gene (MMP12; �82AG).
To date, no data are available concerning the role ofFPN1 gene variants in CVD. The FPN1 �8CG polymor-phism is extremely close to the iron responsive element(IRE) of the gene, thus potentially interfering with FPN1expression.23-26 The �82AG polymorphism in the MMP12gene influencing promoter activity could plausibly play arole in leg ulcer progression as well as in other complexdiseases by ECM degradation.27-32
The new data obtained from the present investigationhave been merged and computed together with previous datarecently published by us on HFE and FXIII SNPs14,17,18,20 topropose prognostic markers by means of a DNA-array ap-proach in CVD.
SUBJECTS AND METHODS
We investigated a total of 638 subjects, classified as per
Fig 1. Whole cohort of subjects investigated. C3-C6 accordingto CEAP international classification of CVD. CVD, Chronic ve-nous disease; VLU, venous leg ulcer.
the scheme in Fig 1.
Case group. Patients (n � 333), of whom 65% werefemales affected by CVD, had a mean age of 60.5 � 14.5years. Among these, 221 had C5-C6 VLU (171 primaryand 50 post-thrombosis) and 112 had C3-C4 phenotype.All patients underwent clinical and duplex scanning exam-ination. This investigation was conducted in conformitywith consensus statement criteria and the methodologypreviously described.33-35 This approach enabled us toseparate primary superficial from post-thrombotic casesand/or with deep venous reflux, as well as to identifypatients with peripheral arterial disease.
Patient selection was put in place by means of strictlyapplied exclusion criteria17 (detailed below) in order toexclude any other comorbidity factor potentially involvedin ulcer wound healing:
● diabetes;● peripheral arterial disease and/or ankle brachial index
�0.9;● hemolytic anemia and/or iron-deficiency anemia
and/or malnutrition;● inability to walk;● severe cardiac and/or hepatic and/or renal and/or
pulmonary insufficiency;● or chronic administration of cortisones for chronic
inflammatory disease and/or autoimmune disease.
Subsequently, and prior to any treatment, the ulceratedarea was assessed by means of software for calculatingirregular areas (Visitrak Capture, Smith & Nephew UKLimited, London, UK). The age of ulcer onset in thegroups with different genotypes was recorded. We did notutilize a specific cut-off to determine patients with early orlate ulcer onset. The age was that recorded during thepatients’ initial consultation at the Vascular Disease Centreof the University-Hospital of Ferrara. In the event patientsdeveloped an ulcer before the end of data collection, theirstatus was duly modified in our database and no otherfollow-up was made. Patients were recruited during theperiod from 2002 to 2005, as previously reported. Al-though significant, we could not account for occupationalstatus or multiple pregnancies in women as confounders inthis analysis.
Healthy controls. The control group consisted of305 healthy subjects with no history of vascular disease andrecruited from the blood donor file of Ferrara Hospital.They were matched by age, gender, and geographic originwith the CVD cases. All subjects enrolled in the study gaveinformed consent, and the survey was approved by theUniversity-Hospital Ethics Committee of Ferrara.
DNA extraction and PCR conditions. The DNAwas isolated from peripheral frozen whole blood by usingthe automated DNA extraction and purification robot(BioRobot EZ1 system, QIAGEN, Hilden, Germany),which performs the fully automated extraction and purifi-cation of nucleic acids using magnetic bead technology.
The PCR-protocol for the simultaneous amplificationof the gene regions containing C282Y and H63D substitu-
tions in the HFE gene, the �8CG substitution in the FPN1
JOURNAL OF VASCULAR SURGERYDecember 20091446 Gemmati et al
gene promoter, the �82AG substitution in the MMP12promoter, and the V34L substitution in the FXIII gene wascarried out as follows: an initial 10 minutes at 94°C fol-lowed by 35 cycles of 95°C for 30 seconds, 56°C for 20seconds, and 72°C for 90 seconds. The PCR cycles wereperformed in a Peltier Thermal Cycler apparatus (PTC-200; M J Research, Inc, Watertown, Mass) and were com-pleted with a final extension step of 5 minutes at 72°C. Themultiplex PCR-reaction was performed in 100 �l finalvolume containing 100 ng of genomic DNA, 20 �MdNTPs, 1.5 mM MgCl2, 10 mM Tris-HCl (pH 8.3), 50mM KCl, 15 pmol of each primer, and 2.0 U of recombi-nant DNA polymerase (AmpliTaq Gold, Applied Biosys-tems, Branchburg, NJ).
Table I (A and B) shows the sequences of the differentpairs of primers needed for PCR and the oligos/probesutilized for genotyping according to the five polymor-phisms in the study.
Genotyping on the Nanogen system. Ampliconswere genotyped by the Nanogen microchip system (Nano-chip Molecular Biology Workstation, Nanogen Corporate,San Diego, Calif). A volume of 10-20 �l containing the
Table IA. Sequences of the different couples of PCR prim
SNP
FPN1 �8CG (Fw) Bio CCAGTTFPN1 �8CG (Rv) CATCCTHFE C282Y (Fw) CGAACCHFE C282Y (Rv) Bio CCCAATHFE H63D (Fw) GTTTGAHFE H63D (Rv) Bio CCACATMMP12 �82AG (Fw) Bio GCCTAAMMP12 �82AG (Rv) AGTCATFXIII V34L (Fw) GACCTTFXIII V34L (Rv) Bio ACCCAG
Fw, Forward primer; Rv, reverse primer; Bio, biotinylated primer.
Table IB. Oligonucleotides utilized in the reporter mix
Oligo
FPN1 �8CG Discriminator wild typeFPN1 �8CG Discriminator mutatedFPN1 �8CG StabilizerHFE C282Y Discriminator wild typeHFE C282Y Discriminator mutatedHFE C282Y StabilizerHFE H63D Discriminator wild typeHFE H63D Discriminator mutatedHFE H63D StabilizerMMP12 �82AG Discriminator wild typeMMP12 �82AG Discriminator mutatedMMP12 �82AG StabilizerFXIII-A V34L Discriminator wild typeFXIII-A V34L Discriminator mutatedFXIII-A V34L Stabilizer
In Italics are reported the universal tail recognized by the universal reporteM, indicates A or C; W, indicates A or T.
amplicon-mix was mixed with histidine buffer to 50
mmol/L final concentration in 60 �l final volume. About100-200 ng of each amplicon were addressed onto theNanochip Cartridge (H2-type) by means of the NanochipLoader using default parameters. A chemical denaturationof amplicons, by means of NaOH 0.1N for 5 minutes oftreatment, ended the addressing protocol. Each reportermix contained probes (discriminator), stabilizers, and re-porter oligonucleotides (details published on www.nanogen.com) specific for each SNP. Hybridization steps and fluo-rescence scans of the cartridge were carried out by theNanochip Reader. An optimized hybridization touchdownprotocol was determined for the analysis of each polymor-phism. The instrumentation and general protocols fol-lowed are detailed in previous reports.36,37 About 20% ofsamples were loaded and analyzed in duplicate, and het-erozygous controls were always included in each assay.Quantitative analysis and genotype designation were real-ized by using specific software supplied by Nanogen andboth were set at the diagnostic level.
Genotype confirming procedure. Haplotypes wereconfirmed by re-genotyping about 20% of random samplesselected from each different genotype group per specific
ence (5=-3=) Amplicon size
GCACTCCTG 129 bpGGCGGTTGGACGTATTGCC 183 bpTTTCTCAGCTCCT
TTTGGGCTACG 115 bpCTTGAAATTCTCTGAACTGTTCC 129 bpTTGTTTGCATGTTAGTCAAAAATGTC 195 bp
GGTGGGGAA
Sequence
TGAGTCCGAACATTGAG-AAAGGTCATGACACTAG-3=CAGTATATCGCTTGACA-AAAGGTCATGACACTAC-3=CGACCCCGCTGGCTCTTCTGCGGCTGCTA-3=TGAGTCCGAACATTGAG-AGAGATATACGTG-3=CAGTCTATCGCTTGACA-CAGAGATATACGTA-3=CMGGTGGAGCACCCAGGCCT-3=TGAGTCCGAACATTGAG-TCGTGTTCTATGATC-3=CAGTATATCGCTTGACA-TCGTGTTCTATGATG-3=TGAGWGTCGCCGTGTGGAGCCCCGAA-3=TGAGTCCGAACATTGAG-TTTGGGATGATATCAACTA-3=CAGTATATCGCTTGACA-TTTGGATGATATCAACTG-3=GAGTCACTCATAGGATTCATATTCACAGAACCCGG-3=TGAGTCCGAACATTGAG-TTTGCTTCAGGGCG-3=CAGTATATCGCTTGACA-TTTAGCTTCAGGGCT-3=GGTGCCCCGGGGCGTCAC-3=
ers
Sequ
CCTTCTCTTAAAAGATAGCCTGGGTTCGCTTGTAAAGT
5=-C5=-G5=-G5=-C5=-G5=-C5=-C5=-G5=-A5=-C5=-G5=-T5=-C5=-G5=-T
r.
polymorphism by means of enzymatic restriction or direct

JOURNAL OF VASCULAR SURGERYVolume 50, Number 6 Gemmati et al 1447
sequence of the same amplicon utilized for the Nanochipprocedure. There were no discrepancies between genotypesdetermined in duplicate and/or by different methods.
Statistical analysis. A retrospective cross-sectionalstudy was performed. Statistical differences among groupswere assessed by the t test and the �2 test, respectively, formean value and genotype distribution comparisons. Whereappropriate, Yates’ correction or Fisher’s exact test wereapplied. Odds ratios (ORs) and 95% confidence intervals(95% CIs) were calculated by conditional logistic regressionmodels, accounting variables and other confounding fac-tors such as gender, age, and weight. In addition, the modelaccounts for a mutual adjustment of the different SNPsconsidered. The reported values were obtained by multiplecomparison tests. Any P values �.05 were considered sta-tistically significant. All analyses were performed using Sys-tat V.5.0 (Systat Inc, Evanston, Ill) and SPSS StatisticalPackage (SPSS Inc, Chicago, Ill).
RESULTS
Computing VLU risk.
FPN1 �8CG. Table II shows the computing of VLUrisk assessed in the group of VLU cases (n � 221) com-pared to a subset of completely matched healthy controls(OR � 5.2; 95% CI, 1.9-15; P � .005). This was obtainedby the comparison of the homozygous genotype in theFPN1 gene (GG) with the counterpart wild-type genotype(CC). Comparing the GG condition with the rest of thegenotypes, the risk value remained stable and signific-ance increased (OR � 4.4; CI 95%, 1.55-12.1; P � .002).In addition, the comparison between the subsets of C5-C6patients (ie, primary vs post-thrombotic VLU) did notshow significant associations to FPN1 genotypes, althoughan over-representation of the GG-homozygotes was presentamong primary VLU (9.35% vs 6.0%; P �.05). Consider-ing the C5-C6 vs C3-C4 comparison, (ie, CVD patientswith ulcer vs those without), it has obtained a significantover-representation of G-carriers among C5-C6 (43% vs31.25%). This yielded an associated risk in developing thelesion of 1.7; (95% CI, 1.03-2.7; P � .045).
Table III shows the computing of VLU risk assessed inthe subgroup of primary VLU cases (n � 171) compared toa subset of completely matched healthy controls (OR �4.98; 95% CI, 1.82-14.9; P � .005). This was obtainedfrom the comparison of the homozygous genotype in theFPN1 gene (GG) with the counterpart wild-type genotype
Table II. All VLU vs controls
FPN1 �8CG Cases (n � 221) Controls (n � 221)
CC 126 (57.0) 148 (67.0)CG 76 (34.0) 68 (30.8)GG 19 (8.6) 5 (2.3)P value .005OR (95% CI) 5.2 (1.9-15)
VLU, Venous leg ulcer; OR, odds ratio; CI, confidence interval.
(CC). Comparing the GG condition with the rest of the
genotypes, risk value remained stable and significance in-creased (OR � 4.7; 95% CI, 1.6-14.1; P � .002).
In addition, the comparison of all CVD patients (n �333) with the healthy controls (n � 305) yielded an in-creased risk of 4.3 (95% CI, 1.6-12; P � .002).
MMP12 �82AG. Considering the MMP12 polymor-phism, a different genotype distribution was observed (P �.010) comparing primary VLU vs matched healthy controls(ie, cases: AA n � 139 [81.3%], AG n � 26 [15.2%], GG n �6 [3.5%] vs controls: AA n � 118 [69%], AG n � 49[28.7%], GG n � 4 [2.3%]). In addition (Table IV),considering only the homozygous AA-genotype, this wasover-represented among primary VLUs with an associatedrisk of 1.96 (95% CI, 1.18-3.22; P � .010).
HFE C282Y and H63D. Risk assessment in thegroups of patients investigated fully resembled that of ourprevious reports.14,17 In the present survey, C2282Yyielded a significant overall risk for CVD (OR � 4.5; 95%CI, 1.3-14.9; P � .001) and among primary CVD the riskfurther increased (OR � 6.5; 95% CI, 1.5-26.5; P � .001)(Table V). Conversely, the H63D gene variant did notshow increased risk, but was responsible for an earlier ulceronset among primary CVD (wild type vs 63D-carriers: 64years � 15 vs 55 years � 14; P � .0001) in conformity with
Table III. Primary VLU vs controls
FPN1 �8CG Cases (n � 171) Controls (n � 171)
CC 96 (56.1) 115 (67.2)CG 59 (34.5) 52 (30.4)GG 16 (9.4) 4 (2.3)P value .005OR (95% CI) 4.98 (1.82-14.9)
VLU, Venous leg ulcer; OR, odds ratio; CI, confidence interval.
Table IV. Primary VLU vs controls
MMP �82AG Cases (n � 171) Controls (n � 171)
AA 139 (81.3) 118 (69.0)AG 26 (15.2) 49 (28.7)GG 6 (3.5) 4 (2.3)P value .01OR (95% CI) 1.96 (1.18-3.22)
VLU, Venous leg ulcer; OR, odds ratio; CI, confidence interval.
Table V. Primary VLU vs CVD (C3C4)
HFE C282Y Cases (n � 171) Controls (n � 112)
CC 153 (89.5) 110 (98.2)CY 17 (9.9) 2 (1.8)YY 1 (0.6) 0 (0.0)P value .001OR (95% CI) 6.5 (1.5-26.5)
CVD, Chronic venous disease; VLU, venous leg ulcer; OR, odds ratio; CI,confidence interval.
our previous reports.14,15
JOURNAL OF VASCULAR SURGERYDecember 20091448 Gemmati et al
VLU size and different genotypes.
FPN1 �8CG. In a subgroup of VLU patients (n �167), the lesion size was available at the recruitment step.Considering the relationships between a specific FPN1genotype and the relative mean ulcer size, it has obtained anonsignificant trend (P � .30) towards increased size andthe G-allele (CC, n � 101: 10 � 19.26 cm2; CG, n � 56:12.0 � 25.6 cm2; GG, n � 10: 13.6 � 14.2 cm2).
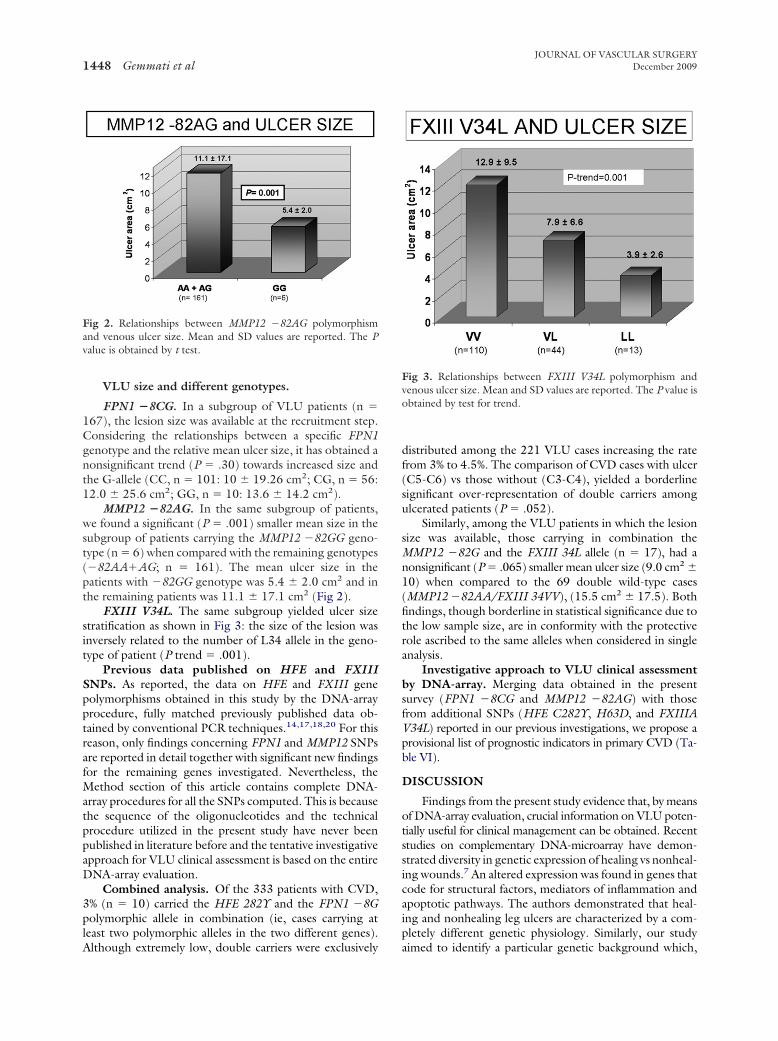
MMP12 �82AG. In the same subgroup of patients,we found a significant (P � .001) smaller mean size in thesubgroup of patients carrying the MMP12 �82GG geno-type (n � 6) when compared with the remaining genotypes(�82AA�AG; n � 161). The mean ulcer size in thepatients with �82GG genotype was 5.4 � 2.0 cm2 and inthe remaining patients was 11.1 � 17.1 cm2 (Fig 2).
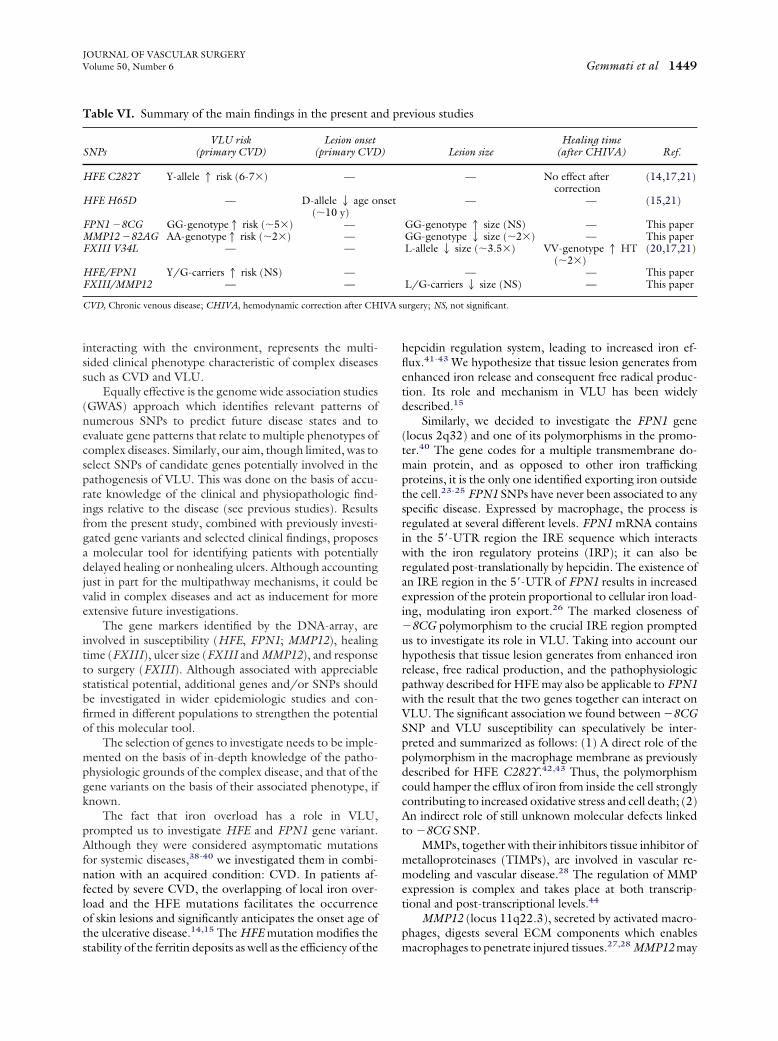
FXIII V34L. The same subgroup yielded ulcer sizestratification as shown in Fig 3: the size of the lesion wasinversely related to the number of L34 allele in the geno-type of patient (P trend � .001).
Previous data published on HFE and FXIIISNPs. As reported, the data on HFE and FXIII genepolymorphisms obtained in this study by the DNA-arrayprocedure, fully matched previously published data ob-tained by conventional PCR techniques.14,17,18,20 For thisreason, only findings concerning FPN1 and MMP12 SNPsare reported in detail together with significant new findingsfor the remaining genes investigated. Nevertheless, theMethod section of this article contains complete DNA-array procedures for all the SNPs computed. This is becausethe sequence of the oligonucleotides and the technicalprocedure utilized in the present study have never beenpublished in literature before and the tentative investigativeapproach for VLU clinical assessment is based on the entireDNA-array evaluation.
Combined analysis. Of the 333 patients with CVD,3% (n � 10) carried the HFE 282Y and the FPN1 �8Gpolymorphic allele in combination (ie, cases carrying atleast two polymorphic alleles in the two different genes).
Fig 2. Relationships between MMP12 �82AG polymorphismand venous ulcer size. Mean and SD values are reported. The Pvalue is obtained by t test.
Although extremely low, double carriers were exclusively
distributed among the 221 VLU cases increasing the ratefrom 3% to 4.5%. The comparison of CVD cases with ulcer(C5-C6) vs those without (C3-C4), yielded a borderlinesignificant over-representation of double carriers amongulcerated patients (P � .052).
Similarly, among the VLU patients in which the lesionsize was available, those carrying in combination theMMP12 �82G and the FXIII 34L allele (n � 17), had anonsignificant (P � .065) smaller mean ulcer size (9.0 cm2 �10) when compared to the 69 double wild-type cases(MMP12 �82AA/FXIII 34VV), (15.5 cm2 � 17.5). Bothfindings, though borderline in statistical significance due tothe low sample size, are in conformity with the protectiverole ascribed to the same alleles when considered in singleanalysis.
Investigative approach to VLU clinical assessmentby DNA-array. Merging data obtained in the presentsurvey (FPN1 �8CG and MMP12 �82AG) with thosefrom additional SNPs (HFE C282Y, H63D, and FXIIIAV34L) reported in our previous investigations, we propose aprovisional list of prognostic indicators in primary CVD (Ta-ble VI).
DISCUSSION
Findings from the present study evidence that, by meansof DNA-array evaluation, crucial information on VLU poten-tially useful for clinical management can be obtained. Recentstudies on complementary DNA-microarray have demon-strated diversity in genetic expression of healing vs nonheal-ing wounds.7 An altered expression was found in genes thatcode for structural factors, mediators of inflammation andapoptotic pathways. The authors demonstrated that heal-ing and nonhealing leg ulcers are characterized by a com-pletely different genetic physiology. Similarly, our study
Fig 3. Relationships between FXIII V34L polymorphism andvenous ulcer size. Mean and SD values are reported. The P value isobtained by test for trend.
aimed to identify a particular genetic background which,
IVA s
JOURNAL OF VASCULAR SURGERYVolume 50, Number 6 Gemmati et al 1449
interacting with the environment, represents the multi-sided clinical phenotype characteristic of complex diseasessuch as CVD and VLU.
Equally effective is the genome wide association studies(GWAS) approach which identifies relevant patterns ofnumerous SNPs to predict future disease states and toevaluate gene patterns that relate to multiple phenotypes ofcomplex diseases. Similarly, our aim, though limited, was toselect SNPs of candidate genes potentially involved in thepathogenesis of VLU. This was done on the basis of accu-rate knowledge of the clinical and physiopathologic find-ings relative to the disease (see previous studies). Resultsfrom the present study, combined with previously investi-gated gene variants and selected clinical findings, proposesa molecular tool for identifying patients with potentiallydelayed healing or nonhealing ulcers. Although accountingjust in part for the multipathway mechanisms, it could bevalid in complex diseases and act as inducement for moreextensive future investigations.
The gene markers identified by the DNA-array, areinvolved in susceptibility (HFE, FPN1; MMP12), healingtime (FXIII), ulcer size (FXIII and MMP12), and responseto surgery (FXIII). Although associated with appreciablestatistical potential, additional genes and/or SNPs shouldbe investigated in wider epidemiologic studies and con-firmed in different populations to strengthen the potentialof this molecular tool.
The selection of genes to investigate needs to be imple-mented on the basis of in-depth knowledge of the patho-physiologic grounds of the complex disease, and that of thegene variants on the basis of their associated phenotype, ifknown.
The fact that iron overload has a role in VLU,prompted us to investigate HFE and FPN1 gene variant.Although they were considered asymptomatic mutationsfor systemic diseases,38-40 we investigated them in combi-nation with an acquired condition: CVD. In patients af-fected by severe CVD, the overlapping of local iron over-load and the HFE mutations facilitates the occurrenceof skin lesions and significantly anticipates the onset age ofthe ulcerative disease.14,15 The HFE mutation modifies the
Table VI. Summary of the main findings in the present an
SNPsVLU risk
(primary CVD)Lesion onset
(primary CVD
HFE C282Y Y-allele1 risk (6-7) —
HFE H65D — D-allele2 age o(10 y)
FPN1 �8CG GG-genotype1 risk (5) —MMP12 �82AG AA-genotype1 risk (2) —FXIII V34L — —
HFE/FPN1 Y/G-carriers1 risk (NS) —FXIII/MMP12 — —
CVD, Chronic venous disease; CHIVA, hemodynamic correction after CH
stability of the ferritin deposits as well as the efficiency of the
hepcidin regulation system, leading to increased iron ef-flux.41-43 We hypothesize that tissue lesion generates fromenhanced iron release and consequent free radical produc-tion. Its role and mechanism in VLU has been widelydescribed.15
Similarly, we decided to investigate the FPN1 gene(locus 2q32) and one of its polymorphisms in the promo-ter.40 The gene codes for a multiple transmembrane do-main protein, and as opposed to other iron traffickingproteins, it is the only one identified exporting iron outsidethe cell.23-25 FPN1 SNPs have never been associated to anyspecific disease. Expressed by macrophage, the process isregulated at several different levels. FPN1 mRNA containsin the 5=-UTR region the IRE sequence which interactswith the iron regulatory proteins (IRP); it can also beregulated post-translationally by hepcidin. The existence ofan IRE region in the 5=-UTR of FPN1 results in increasedexpression of the protein proportional to cellular iron load-ing, modulating iron export.26 The marked closeness of�8CG polymorphism to the crucial IRE region promptedus to investigate its role in VLU. Taking into account ourhypothesis that tissue lesion generates from enhanced ironrelease, free radical production, and the pathophysiologicpathway described for HFE may also be applicable to FPN1with the result that the two genes together can interact onVLU. The significant association we found between �8CGSNP and VLU susceptibility can speculatively be inter-preted and summarized as follows: (1) A direct role of thepolymorphism in the macrophage membrane as previouslydescribed for HFE C282Y.42,43 Thus, the polymorphismcould hamper the efflux of iron from inside the cell stronglycontributing to increased oxidative stress and cell death; (2)An indirect role of still unknown molecular defects linkedto �8CG SNP.
MMPs, together with their inhibitors tissue inhibitor ofmetalloproteinases (TIMPs), are involved in vascular re-modeling and vascular disease.28 The regulation of MMPexpression is complex and takes place at both transcrip-tional and post-transcriptional levels.44
MMP12 (locus 11q22.3), secreted by activated macro-phages, digests several ECM components which enables
evious studies
Lesion sizeHealing time
(after CHIVA) Ref.
— No effect aftercorrection
(14,17,21)
— — (15,21)
GG-genotype1 size (NS) — This paperGG-genotype2 size (2) — This paperL-allele2 size (3.5) VV-genotype1 HT
(2)(20,17,21)
— — This paperL/G-carriers2 size (NS) — This paper
urgery; NS, not significant.
d pr
)
nset
macrophages to penetrate injured tissues.27,28 MMP12 may

JOURNAL OF VASCULAR SURGERYDecember 20091450 Gemmati et al
block angiogenesis by converting plasminogen to angiosta-tin, a potent angiogenesis inhibitor. The �82AG polymor-phism in the MMP12 promoter is very close to the tran-scriptional factor-binding site for AP1. For this reason, itmay influence their specific interactions. The higher pro-moter activity of the A-allele described above compared tothe G-allele gives expected higher expression levels. Al-though no basal difference was described between expres-sions of the two alleles, in transfecting experiments theresponse of A-allele is higher when cells are stimulated withinsulin or phorbol myristate acetate.29 Small change inpromoter activity was recorded between the two alleles andthis could be sufficient and have significant effects onlong-staying wounds. Accordingly, chronic higher expres-sion of MMP12 in wounds of patients with �82A-allelemay be responsible for the significant smaller ulcer sizefound in �82GG patients. The controversial fact that wedid not find any risk association with the MMP12 A-allele(ie, cases with �82AG � �82AA genotypes), but onlywhen the �82A-allele was in the homozygous condition,might indicate that the A-allele in single copy is not strongenough to be causative for ulcer onset. However, once thelesion appears it may modulate the size: AA and AG caseshad a significant larger wound area. Finally, findings on theassociation of the polymorphism with coronary artery dis-ease, cancer, and endometriosis have also been recentlypublished.29-32
FXIII strengthens the ECM components against unre-strained MMP proteolysis, favoring in turn fibroblast mi-gration and proliferation and promoting neoangiogenesisand healing. The extent of these and additional actionsstrictly depends on the associated gene variants.19-21,45 Itcould be hypothesized that a significant higher FXIII ac-tivity (ie, that of the L34-variant) at the wound site, couldbetter promote wound healing by ameliorating the above-mentioned pathway resulting in reduced wound size andshortened wound healing time.17,20
Apart from specific genotypes, the VLU area may alsobe influenced by past treatment practiced prior to our firstclinical assessment. With regard to our data, the lesion sizewas recorded at the recruitment step before the start of anysurgical or medical treatment. In addition, the cases inwhich the lesion area was recorded belonged to a groupwith restrictive inclusion criteria, as previously reported,17
this was in order to minimize several confounding factorsmasking the genotype effects.
In short, on the basis of the described results, preven-tion programs in primary CVD could be improved by usingDNA-array evaluation in the initial patient assessmentphase. Clinical practice could be potentially influenced bythese results.22 One example is given by using HFE andFPN1 SNPs. A positive test for one or both gene variantswould suggest indication and priority for surgical correc-tion of superficial venous insufficiency while primary vari-cose veins could be treated more appropriately before anylesion appears in those patients with a critical gene haplo-
type.21,22,46We conclude that by simultaneous analysis of selectedSNPs, it might be possible to glean important informationfor predicting VLU onset stratifying patients according totheir potential to heal.
It should be emphasized, however, that although sig-nificant, these findings have to be considered as prelimi-nary. The proposed prognostic indicators should be usedwith caution and subjected to further trials on differentpopulations prior to definitive confirmation.
We thank Dr Kathleen Galvin for the complete revisionof the manuscript.
AUTHOR CONTRIBUTIONS
Conception and design: GD, FF, CL, GS, TG, SL, ZPAnalysis and interpretation: GD, ZPData collection: GD, FF, CL, GS, TG, SL, ZPWriting the article: GD, FF, CL, GS, TG, SL, ZPCritical revision of the article: GD, FF, CL, GS, TG, SL, ZPFinal approval of the article: GD, FF, CL, GS, TG, SL, ZPStatistical analysis: GD, FF, CL, ZPObtained funding: GD, ZPOverall responsibility: GD, ZP
REFERENCES
1. Bergqvist D, Lindholm C, Nelzén O. Chronic leg ulcers: the impact ofvenous disease. J Vasc Surg 1999;29:752-5.
2. Abbade LP, Lastória S. Venous ulcer: epidemiology, physiopathology,diagnosis and treatment. Int J Dermatol 2005;44:449-56.
3. McGuckin M, Waterman R, Brooks J, Cherry G, Porten L, Hurley S,Kerstein MD. Validation of venous leg ulcer guidelines in the UnitedStates and United Kingdom. Am J Surg 2002;183:132-7.
4. Abbade LP, Lastória S, de Almeida Rollo H, Stolf HO. A sociodemo-graphic, clinical study of patients with venous ulcer. Int J Dermatol2005;44:989-92.
5. Cesarone MR, Belcaro G, Nicolaides AN, Geroulakos G, Griffin M,Incandela L, et al. ‘Real’ epidemiology of varicose veins and chronicvenous diseases: the San Valentino Vascular Screening Project. Angiol-ogy 2002;53:119-30.
6. Gohel MS, Taylor M, Earnshaw JJ, Heather BP, Poskitt KR, WhymanMR. Risk factors for delayed healing and recurrence of chronic venousleg ulcers—an analysis of 1324 legs. Eur J Vasc Endovasc Surg 2005;29:74-7.
7. Charles CA, Tomic-Canic M, Vincek V, Nassiri M, Stojadinovic O,Eaglstein WH, Kirsner RS. A gene signature of nonhealing venousulcers: potential diagnostic markers. J Am Acad Dermatol 2008;59:758-71.
8. Zamboni P. The big idea: iron-dependent inflammation in venousdisease and proposed parallels in multiple sclerosis. J R Soc Med2006;99:589-93.
9. Simka M, Rybak Z. Hypothetical molecular mechanisms by which localiron overload facilitates the development of venous leg ulcers andmultiple sclerosis lesions. Med Hypotheses 2008;71:293-7.
10. Ashworth JJ, Smyth JV, Pendleton N, Horan M, Payton A, Worthing-ton J, et al. The dinucleotide (CA) repeat polymorphism of estrogenreceptor beta but not the dinucleotide (TA) repeat polymorphism ofestrogen receptor alpha is associated with venous ulceration. J SteroidBiochem Mol Biol 2005;97:266-70.
11. Nagy N, Szolnoky G, Szabad G, Bata-Csörgo Z, Dobozy A, Kemeny L,Szell M. Single nucleotide polymorphisms of the fibroblast growthfactor receptor 2 gene in patients with chronic venous insufficiency withleg ulcer. J Invest Dermatol 2005;124:1085-8.
12. Wallace HJ, Vandongen YK, Stacey MC. Tumor necrosis factor-alphagene polymorphism associated with increased susceptibility to venous
leg ulceration. J Invest Dermatol 2006;126:921-5.
JOURNAL OF VASCULAR SURGERYVolume 50, Number 6 Gemmati et al 1451
13. Ashworth JJ, Smyth JV, Pendleton N, Horan M, Payton A, Worthing-ton J, et al. Polymorphisms spanning the 0N exon and promoter of theestrogen receptor-beta (ERbeta) gene ESR2 are associated with venousulceration. Clin Genet 2008;73:55-61.
14. Zamboni P, Tognazzo S, Izzo M, Pancaldi F, Scapoli GL, Liboni A,Gemmati D. Hemochromatosis C282Y gene mutation increases therisk of venous leg ulceration. J Vasc Surg 2005;42:309-14.
15. Zamboni P, Izzo M, Tognazzo S, Carandina S, De Palma M, Catozzi L,et al. The overlapping of local iron overload and HFE mutation invenous leg ulcer pathogenesis. Free Radic Biol Med 2006;40:1869-73.
16. Zamboni P, Scapoli G, Lanzara V, Izzo M, Fortini P, Legnaro R, et al.Serum iron and matrix metalloproteinase-9 variations in limbs affectedby chronic venous disease and venous leg ulcers. Dermatol Surg 2005;31:644-9; discussion 649.
17. Gemmati D, Tognazzo S, Catozzi L, Federici F, De Palma M, GianesiniS, et al. Influence of gene polymorphisms in ulcer healing process aftersuperficial venous surgery. J Vasc Surg 2006;44:554-62.
18. Tognazzo S, Gemmati D, Palazzo A, Catozzi L, Carandina S, LegnaroA, et al. Prognostic role of factor XIII gene variants in nonhealingvenous leg ulcers. J Vasc Surg 2006;44:815-9.
19. Zamboni P, De Mattei M, Ongaro A, Fogato L, Carandina S, De PalmaM, et al. Factor XIII contrasts the effects of metalloproteinases inhuman dermal fibroblast cultured cells. Vasc Endovascular Surg 2004;38:431-8.
20. Gemmati D, Tognazzo S, Serino ML, Fogato L, Carandina S, De PalmaM, et al. Factor XIII V34L polymorphism modulates the risk of chronicvenous leg ulcer progression and extension. Wound Repair Regen2004;12:512-7.
21. Zamboni P, Gemmati D. Clinical implications of gene polymorphismsin venous leg ulcer: a model in tissue injury and reparative process.Thromb Haemost 2007;98:131-7.
22. Zamboni P. Genetics of venous leg ulcer: an indication to priority ofvaricose veins treatment? Int Angiol 2008;27:91-2.
23. Donovan A, Brownlie A, Zhou Y, Shepard J, Pratt SJ, Moynihan J, et al.Positional cloning of zebrafish ferroportin1 identifies a conserved ver-tebrate iron exporter. Nature 2000;403:776-81.
24. McKie AT, Marciani P, Rolfs A, Brennan K, Wehr K, Barrow D, et al. Anovel duodenal iron-regulated transporter, IREG1, implicated in thebasolateral transfer of iron to the circulation. Mol Cell 2000;5:299-309.
25. Abboud S, Haile DJ. A novel mammalian iron-regulated protein involvedin intracellular iron metabolism. J Biol Chem 2000;275:19906-12.
26. De Domenico I, Ward DM, Musci G, Kaplan J. Iron overload due tomutations in ferroportin. Haematologica 2006;91:92-5.
27. Shapiro SD, Kobayashi DK, Ley TJ. Cloning and characterization of aunique elastolytic metalloproteinase produced by human alveolar mac-rophages. J Biol Chem 1993;268:23824-9.
28. Raffetto JD, Khalil RA. Matrix metalloproteinases and their inhibitorsin vascular remodeling and vascular disease. Biochem Pharmacol 2008;75:346-59.
29. Jormsjö S, Ye S, Moritz J, Walter DH, Dimmeler S, Zeiher AM, et al.Allele-specific regulation of matrix metalloproteinase-12 gene activity isassociated with coronary artery luminal dimensions in diabetic patientswith manifest coronary artery disease. Circ Res 2000;86:998-1003.
30. Lamblin N, Bauters C, Hermant X, Lablanche JM, Helbecque N,Amouyel P. Polymorphisms in the promoter regions of MMP-2,MMP-3, MMP-9 and MMP-12 genes as determinants of aneurysmal
coronary artery disease. J Am Coll Cardiol 2002;40:43-8.31. Borghese B, Chiche JD, Vernerey D, Chenot C, Mir O, Bijaoui G, et al.Genetic polymorphisms of matrix metalloproteinase 12 and 13 genesare implicated in endometriosis progression. Hum Reprod 2008;23:1207-13.
32. Su L, Zhou W, Asomaning K, Lin X, Wain JC, Lynch TJ, et al.Genotypes and haplotypes of matrix metalloproteinase 1, 3 and 12genes and the risk of lung cancer. Carcinogenesis 2006;27:1024-9.
33. Zamboni P, Cisno C, Marchetti F, Mazza P, Fogato L, Carandina S, etal. Minimally invasive surgical management of primary venous ulcers vs.compression treatment: a randomized clinical trial. Eur J Vasc EndovascSurg 2003;25:313-8.
34. Nicolaides AN. Investigation of chronic venous insufficiency: a consensusstatement (France, March 5-9, 1997). Circulation 2000;102:E126-63.
35. Eklöf B, Rutherford RB, Bergan JJ, Carpentier PH, Gloviczki P, KistnerRL, et al. Revision of the CEAP classification for chronic venousdisorders: consensus statement. J Vasc Surg 2004;40:1248-52.
36. Ferrari M, Cremonesi L, Bonini P, Foglieni B, Stenirri S. Single-nucleotide polymorphism and mutation identification by the nanogenmicroelectronic chip technology. Methods Mol Med 2005;114:93-106.
37. Sosnowski R, Heller MJ, Tu E, Forster AH, Radtkey R. Active micro-electronic array system for DNA hybridization, genotyping and phar-macogenomic applications. Psychiatr Genet 2002;12:181-92.
38. McCune CA, Ravine D, Worwood M, Jackson HA, Evans HM, HuttonD. Screening for hereditary haemochromatosis within families andbeyond. Lancet 2003;362:1897-8.
39. Beutler E, Felitti VJ, Koziol JA, Ho NJ, Gelbart T. Penetrance of845G—� A (C282Y) HFE hereditary haemochromatosis mutation inUSA. Lancet 2002;359:211-8.
40. Lee P, Gelbart T, West C, Halloran C, Beutler E. Seeking candidatemutations that affect iron homeostasis. Blood Cells Mol Dis 2002;29:471-87.
41. Drakesmith H, Schimanski LM, Ormerod E, Merryweather-Clarke AT,Viprakasit V, Edwards JP, et al. Resistance hepcidin is conferred byhemochromatosis-associated mutations ferroportin. Blood 2005;106:1092-7.
42. Drakesmith H, Sweetland E, Schimanski L, Edwards J, Cowley AshrafM, et al. The hemochromatosis protein HFE inhibits iron export frommacrophages. Proc Natl Acad Sci U S A 2002;99:15602-7.
43. Moura E, Noordermeer MA, Verhoeven N, Verheul AF, Marx JJ. Ironrelease from human monocytes after erythrophagocytosis vitro: aninvestigation in normal subjects and hereditary hemochromatosis pa-tients. Blood 1998;92:2511-9.
44. Tavaré JM, Rutter GA, Griffiths MR, Dobson SP, Gray H. Regulationof gene expression by insulin: analysis in single living cells. Biochem SocTrans 1996;24:378-84.
45. Gemmati D, Federici F, Campo G, Tognazzo S, Serino ML, De MatteiM, et al. Factor XIIIA-V34L and factor XIIIB-H95R gene variants:effects on survival in myocardial infarction patients. Mol Med 2007;13:112-20.
46. Lanzara S, Catozzi L, De Palma M, Federici F, Palazzo A, Tacconi G, etal. The inflammatory chain in chronic venous leg ulcer. Acta Phlebol2006;7:39-44.
Submitted Feb 6, 2009; accepted Jul 25, 2009.
Related Documents











