Distraction Distraction Osteogenesis of the Osteogenesis of the Craniofacial Skeleton Craniofacial Skeleton DR. STUART SUPER DR. STUART SUPER LENOX HILL HOSPITAL LENOX HILL HOSPITAL NYU/Bellevue Hospital Center NYU/Bellevue Hospital Center

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Distraction Distraction Osteogenesis of the Osteogenesis of the Craniofacial SkeletonCraniofacial Skeleton
DR. STUART SUPERDR. STUART SUPERLENOX HILL HOSPITALLENOX HILL HOSPITAL
NYU/Bellevue Hospital CenterNYU/Bellevue Hospital Center
What is Distraction What is Distraction Osteogenesis?Osteogenesis?
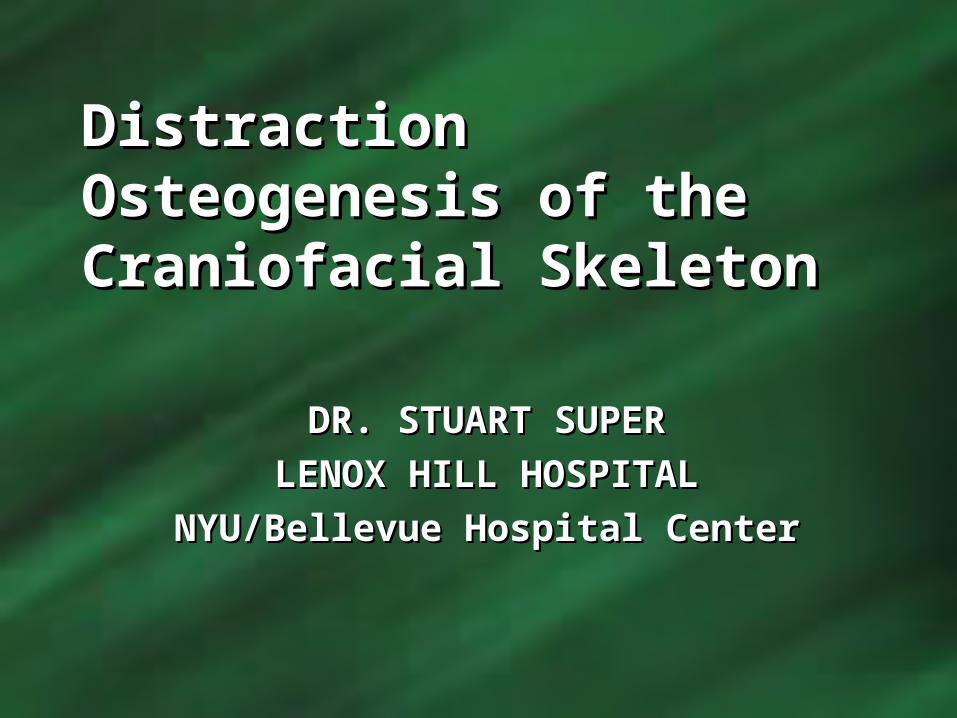
• The regeneration of bone The regeneration of bone between vascularized bone between vascularized bone surfaces that are separated surfaces that are separated by gradual distractionby gradual distraction
• A unique form of clinical A unique form of clinical tissue engineering using tissue engineering using easily controlled mechanical easily controlled mechanical conditions (i.e. slow gradual conditions (i.e. slow gradual distraction of the distraction of the corticotomized or corticotomized or osteotomized bone osteotomized bone fragmentsfragments
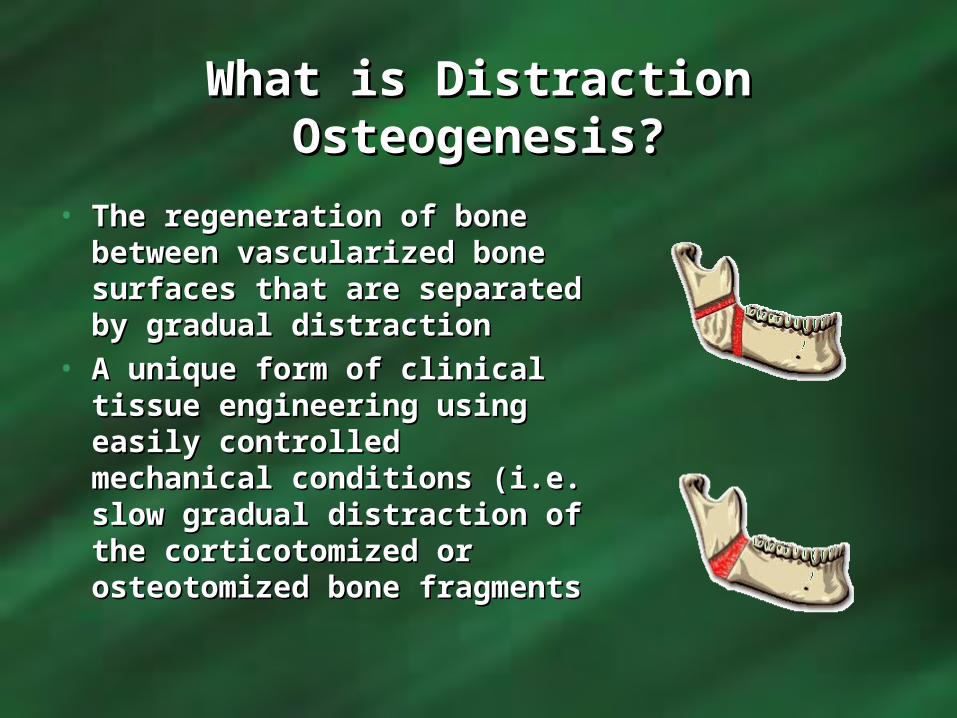
History of DistractionHistory of Distraction• Discovered by accident by Discovered by accident by
Professor Gavril Professor Gavril Abramovich Ilizarov in Abramovich Ilizarov in 19511951
• He was treating patients in He was treating patients in Siberia with fractures and Siberia with fractures and non-unions following WWIInon-unions following WWII
• Using a primative external Using a primative external ring fixator, he compressed ring fixator, he compressed the injured bone ends the injured bone ends togethertogether
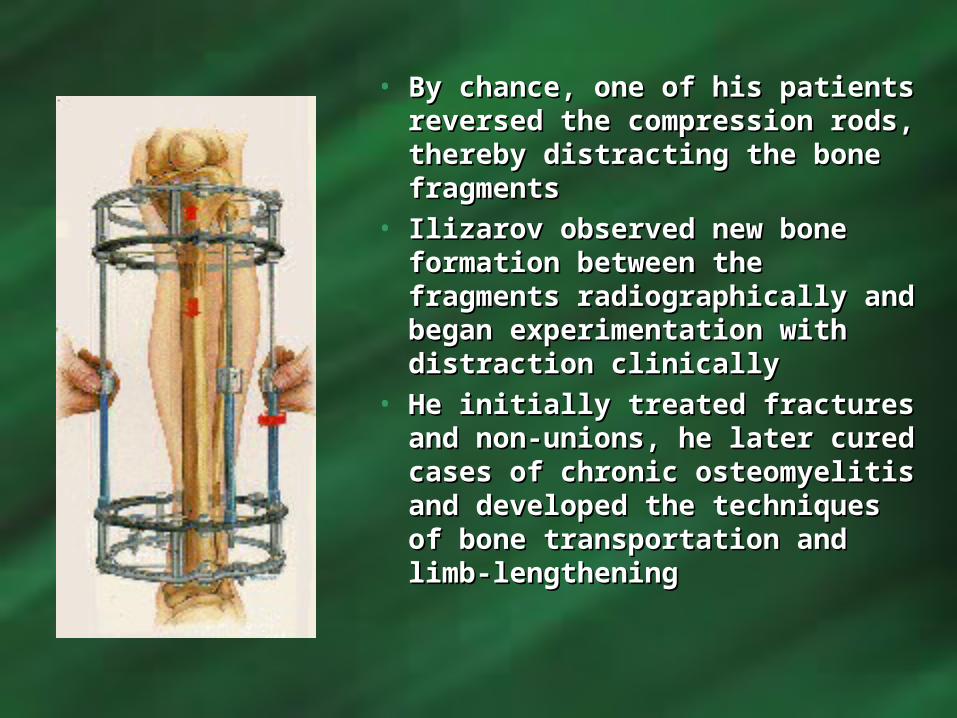
• By chance, one of his patients By chance, one of his patients reversed the compression reversed the compression rods, thereby distracting the rods, thereby distracting the bone fragmentsbone fragments
• Ilizarov observed new bone Ilizarov observed new bone formation between the formation between the fragments radiographically fragments radiographically and began experimentation and began experimentation with distraction clinicallywith distraction clinically
• He initially treated fractures He initially treated fractures and non-unions, he later and non-unions, he later cured cases of chronic cured cases of chronic osteomyelitis and developed osteomyelitis and developed the techniques of bone the techniques of bone transportation and limb-transportation and limb-lengtheninglengthening
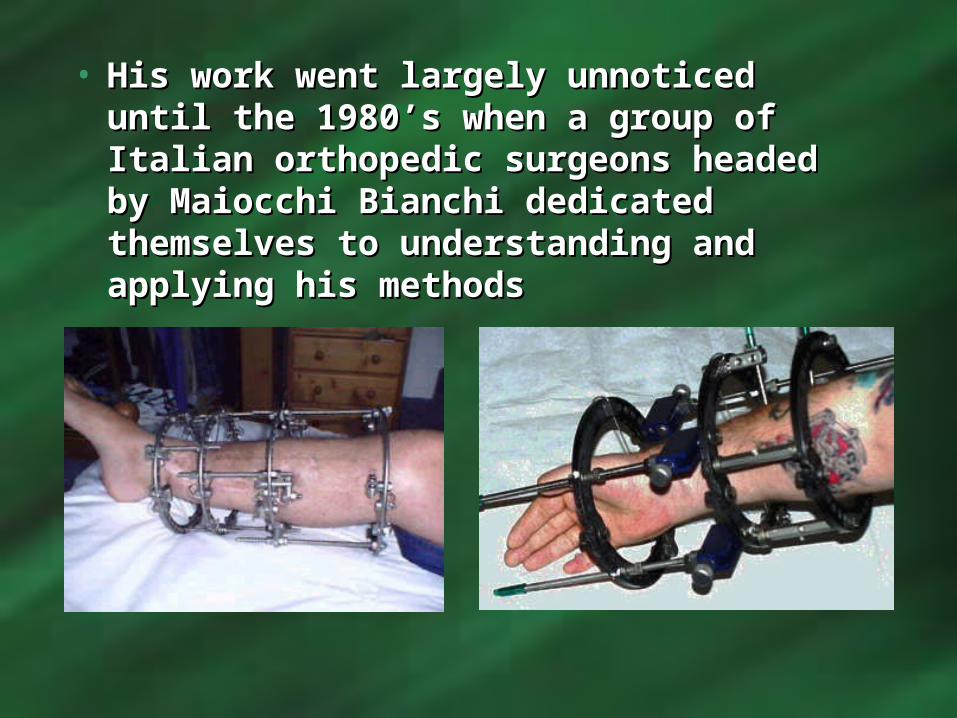
• His work went largely unnoticed until His work went largely unnoticed until the 1980’s when a group of Italian the 1980’s when a group of Italian orthopedic surgeons headed by orthopedic surgeons headed by Maiocchi Bianchi dedicated Maiocchi Bianchi dedicated themselves to understanding and themselves to understanding and applying his methodsapplying his methods
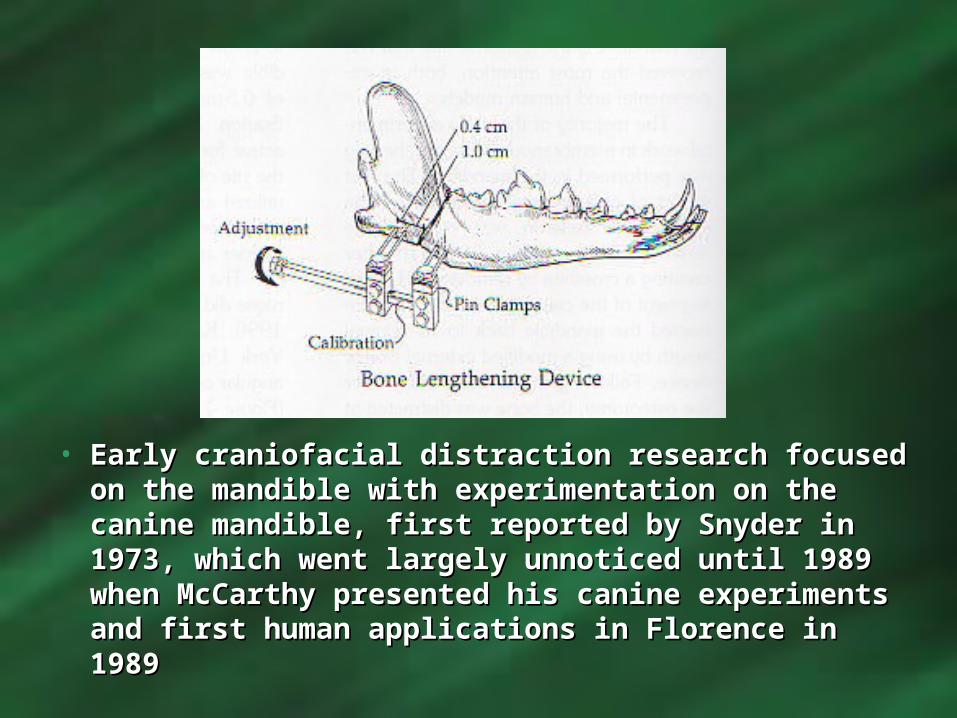
• Early craniofacial distraction research focused on Early craniofacial distraction research focused on the mandible with experimentation on the canine the mandible with experimentation on the canine mandible, first reported by Snyder in 1973, mandible, first reported by Snyder in 1973, which went largely unnoticed until 1989 when which went largely unnoticed until 1989 when McCarthy presented his canine experiments and McCarthy presented his canine experiments and first human applications in Florence in 1989first human applications in Florence in 1989
Principles of Principles of Distraction Distraction OsteogenesisOsteogenesisAccording to Ilizarov, there are two According to Ilizarov, there are two biological principles that govern biological principles that govern distraction osteogenesis, known as the distraction osteogenesis, known as the Ilizarov EffectsIlizarov Effects::1)1) The tension stress effect on the The tension stress effect on the genesis and growth of tissuesgenesis and growth of tissues2)2) The influence of the blood supply and The influence of the blood supply and loading on the shape of bones and jointsloading on the shape of bones and joints
• Low-energy osteotomyLow-energy osteotomy• Duration of latency periodDuration of latency period• Rate & Rhythm of distractionRate & Rhythm of distraction• Consolidation periodConsolidation period
Biological Factors Biological Factors influencing influencing distractiondistraction
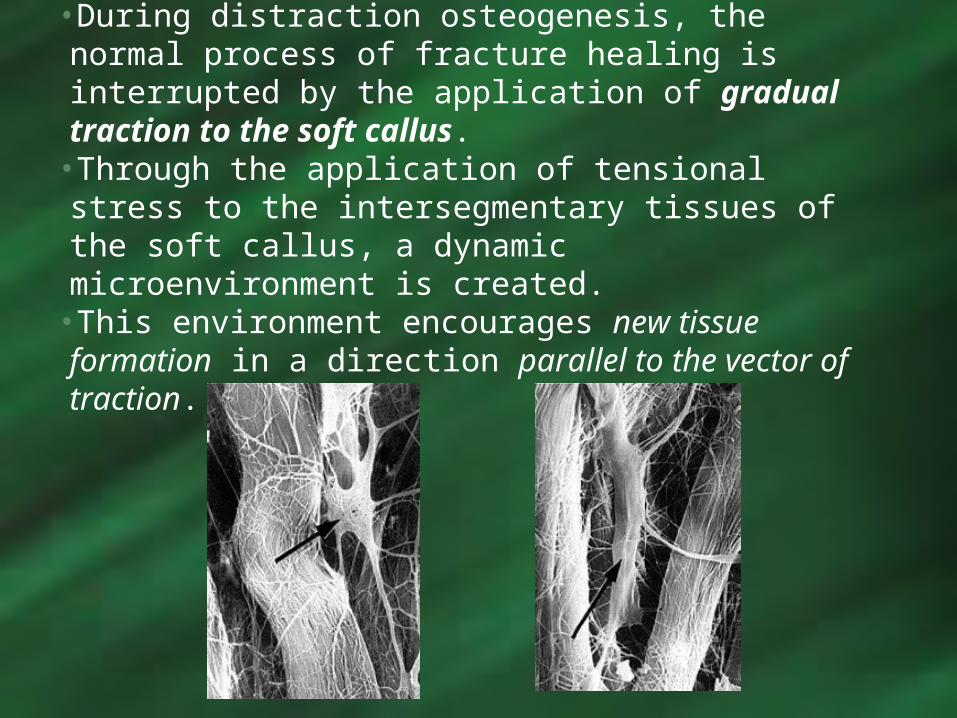
•During distraction osteogenesis, the normal process of fracture healing is interrupted by the application of gradual traction to the soft callus.
•Through the application of tensional stress to the intersegmentary tissues of the soft callus, a dynamic microenvironment is created.
•This environment encourages new tissue formation in a direction parallel to the vector of traction.
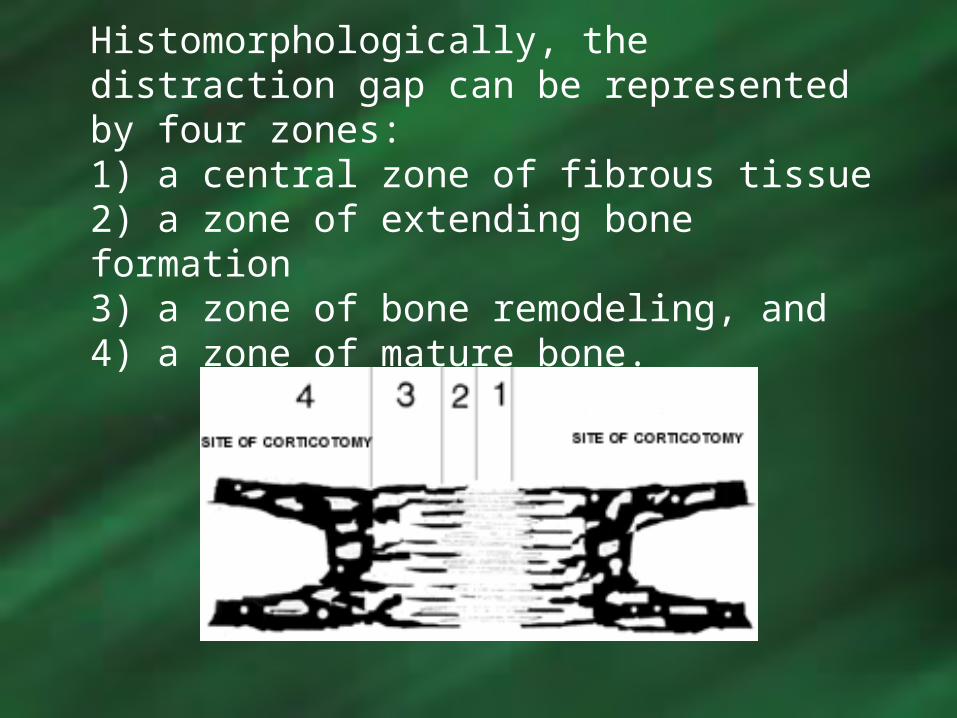
Histomorphologically, the distraction gap can be represented by four zones: 1) a central zone of fibrous tissue2) a zone of extending bone formation3) a zone of bone remodeling, and4) a zone of mature bone.

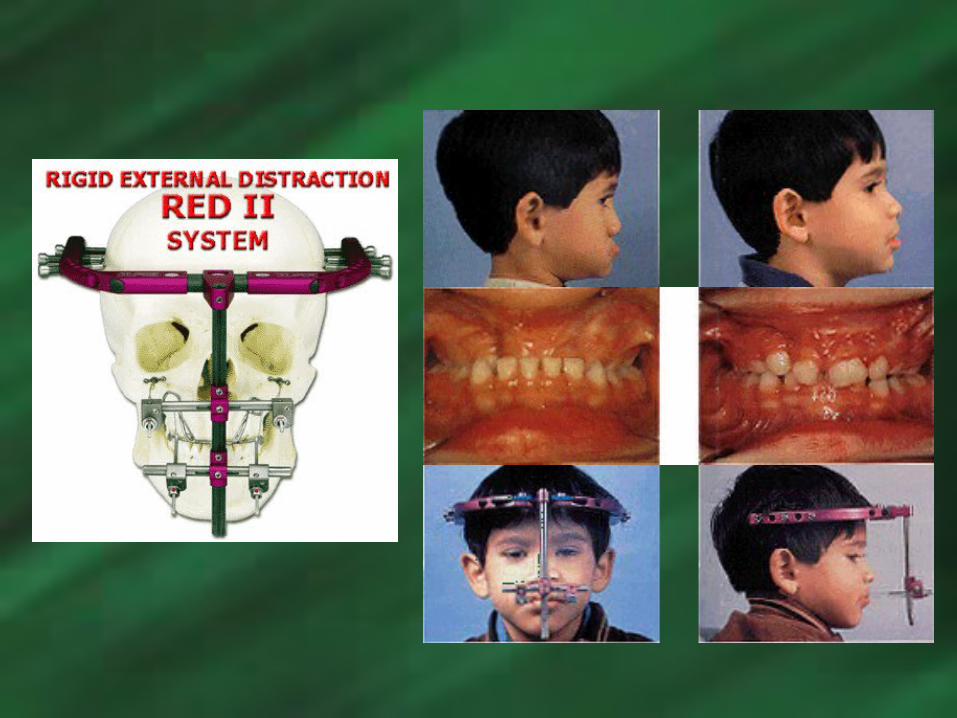
Although both of these extraoral maxillary Although both of these extraoral maxillary and mandibular distraction appliances have and mandibular distraction appliances have the ability to promote significant amounts the ability to promote significant amounts bone formation, as well as exhibit excellent bone formation, as well as exhibit excellent vector control, the primary drawbacks are:vector control, the primary drawbacks are:
Difficulty with Patient ManagementDifficulty with Patient Management Esthetically UnpleasingEsthetically Unpleasing
This led to the development of maxillary This led to the development of maxillary and mandibular intraoral distraction and mandibular intraoral distraction appliances that exhibited similar qualities appliances that exhibited similar qualities to the extraoral distraction appliances, such to the extraoral distraction appliances, such as vector control, as well as being more as vector control, as well as being more accepted and well tolerated by patients…accepted and well tolerated by patients…
Mandibular Distraction Mandibular Distraction OsteogenesisOsteogenesis
Utilizing Intraoral Utilizing Intraoral AppliancesAppliances
Primary Applications:Primary Applications: Patients with Hemifacial Patients with Hemifacial
MicrosomiaMicrosomia
Patients exhibiting moderate to Patients exhibiting moderate to severe micrognathiasevere micrognathia
Case #1Case #1• 11 y.o. male with 11 y.o. male with
Hemifacial Hemifacial microsomia microsomia
• Facial AsymmetryFacial Asymmetry• RetrognathiaRetrognathia• Multiple Ectopic Multiple Ectopic
TeethTeeth• Dental CrowdingDental Crowding

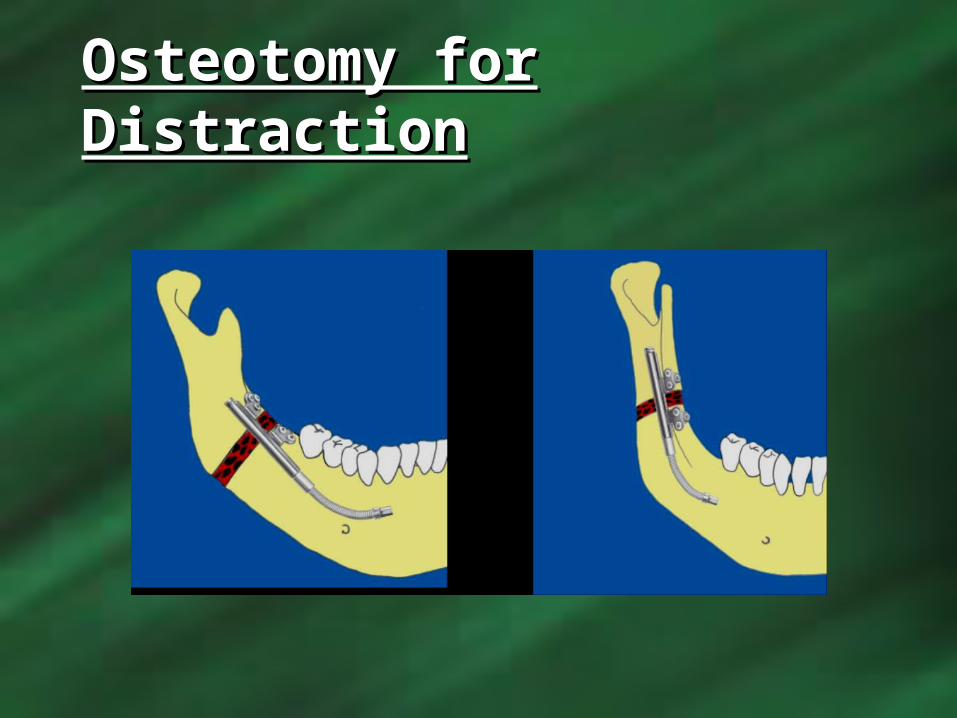
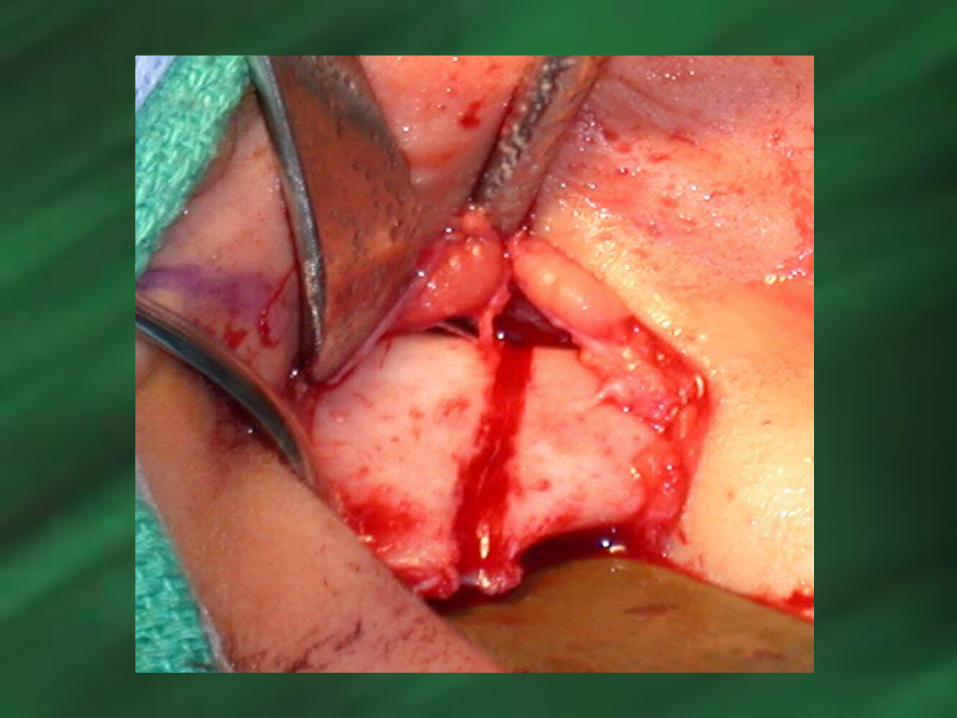
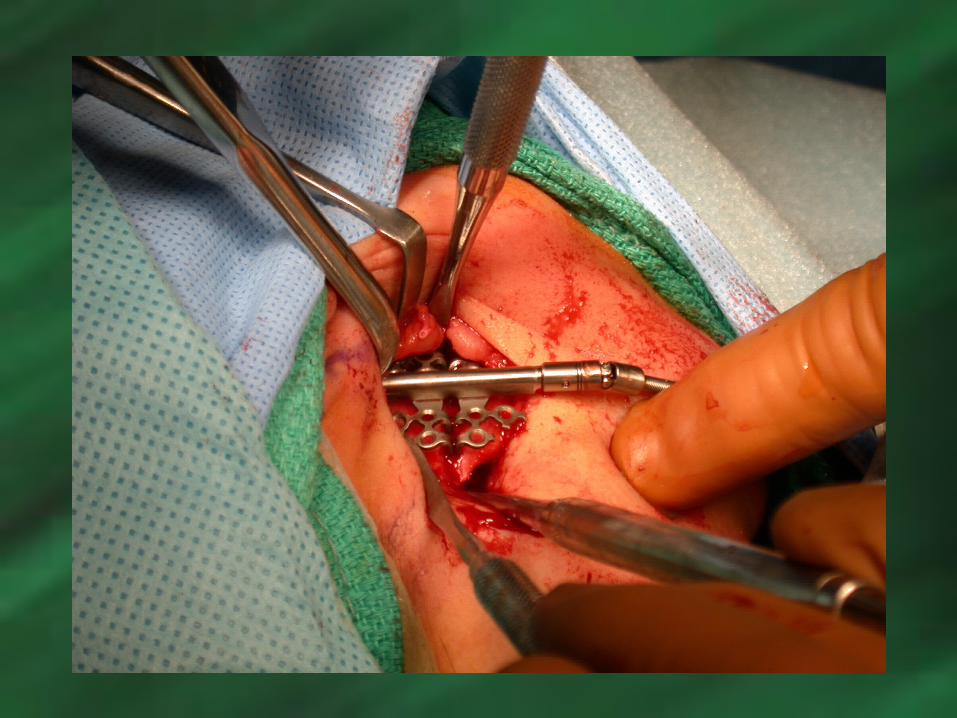
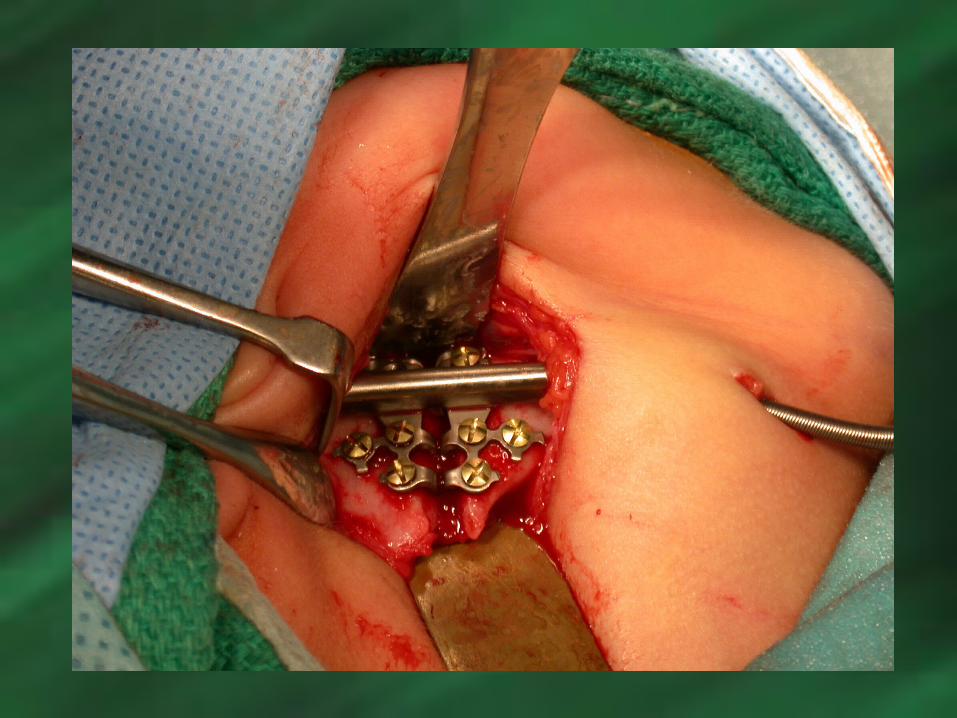
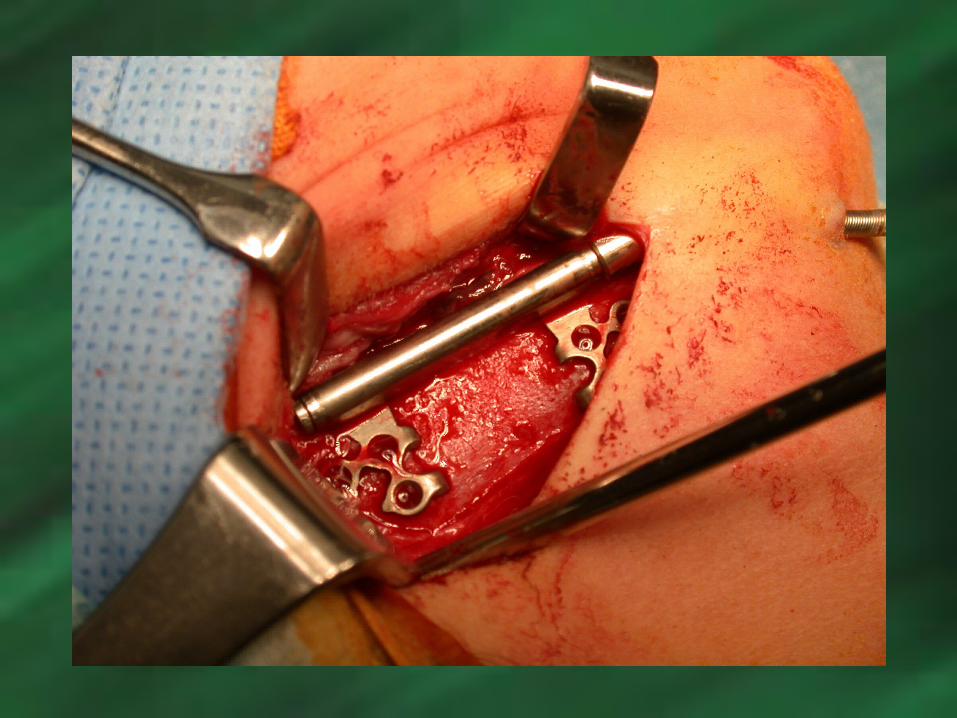
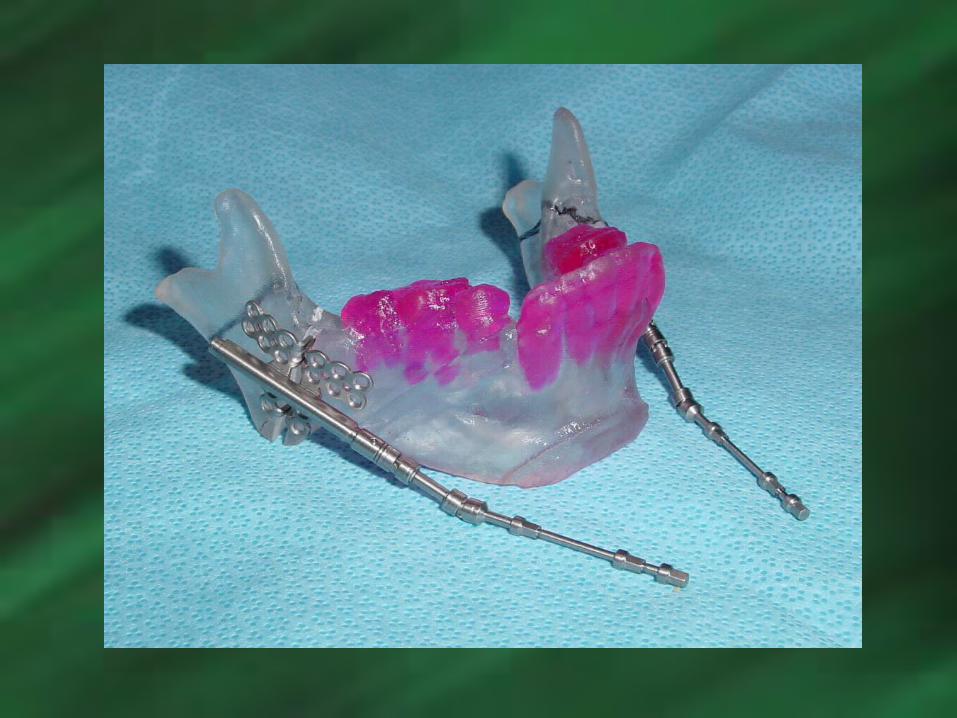
Osteotomy for Osteotomy for DistractionDistraction

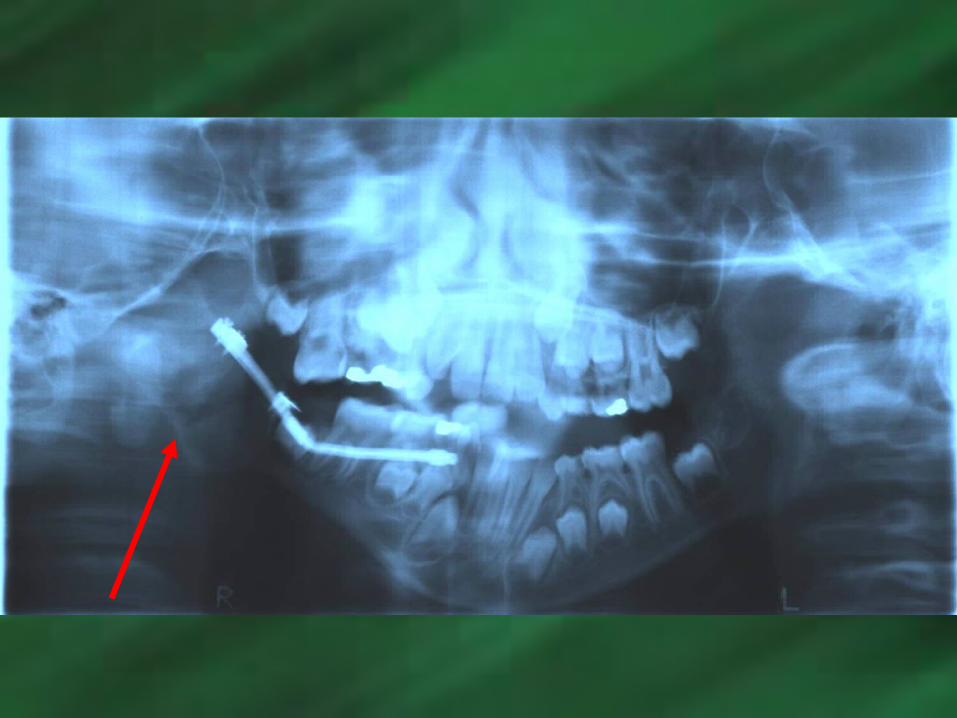
Mandibular Zurich Mandibular Zurich Distraction ApplianceDistraction Appliance

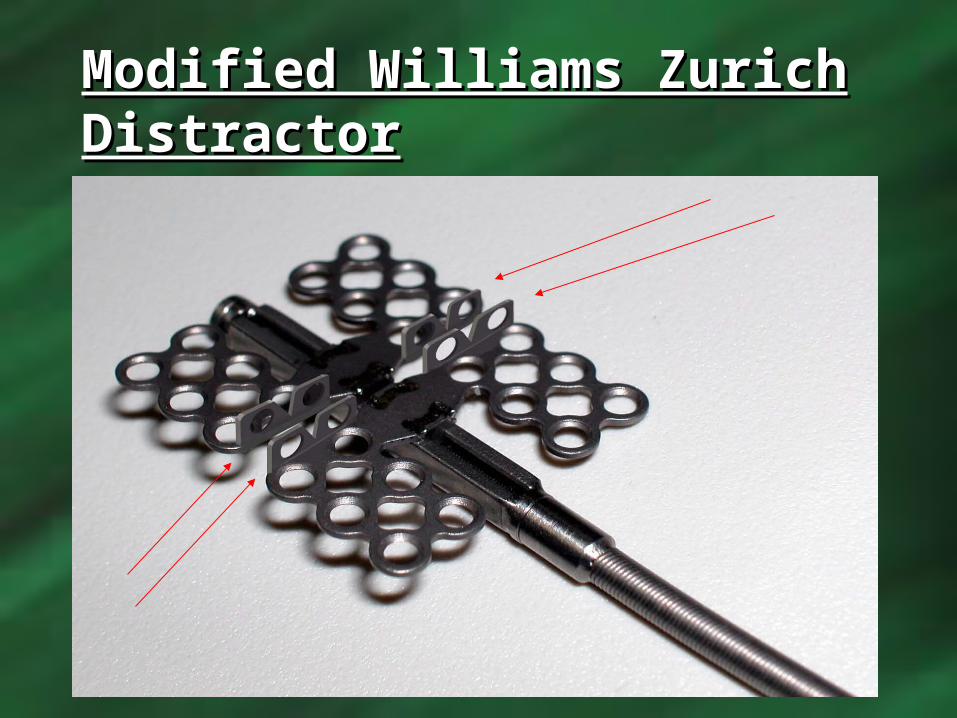
Modified Williams Zurich Modified Williams Zurich DistractorDistractor


Case #2Case #2• 7 y.o. female with 7 y.o. female with
Goldenhar Syndrome Goldenhar Syndrome (Hemifacial (Hemifacial microsomia with microsomia with rib/vertebral rib/vertebral anomalies and anomalies and systemic anomalies systemic anomalies such as such as CNS/cardiac/renal/GI/CNS/cardiac/renal/GI/pulmonary)pulmonary)


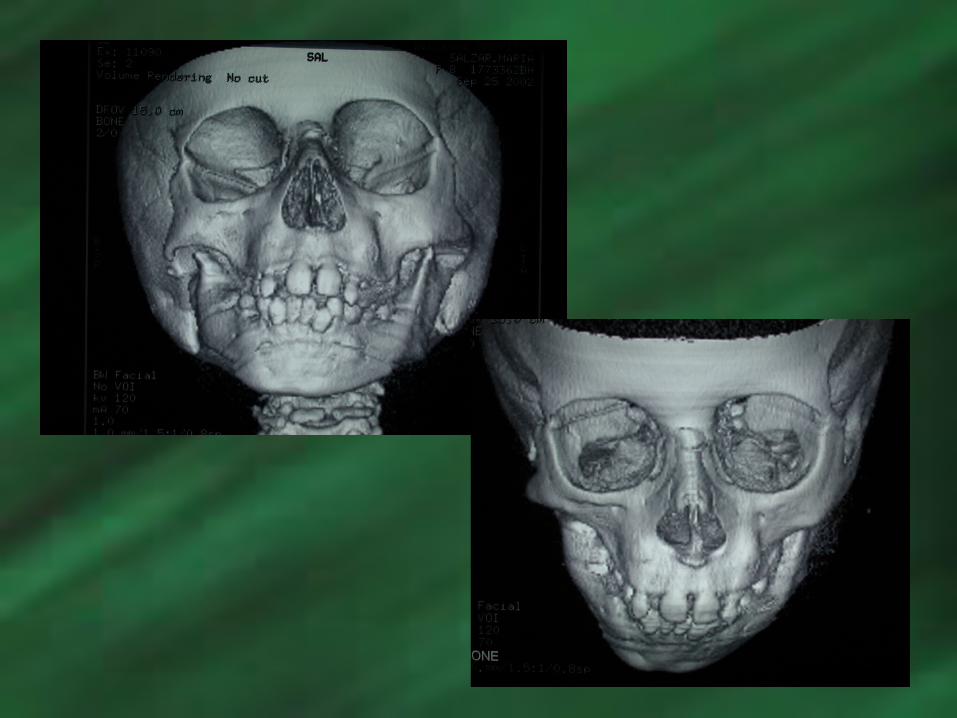
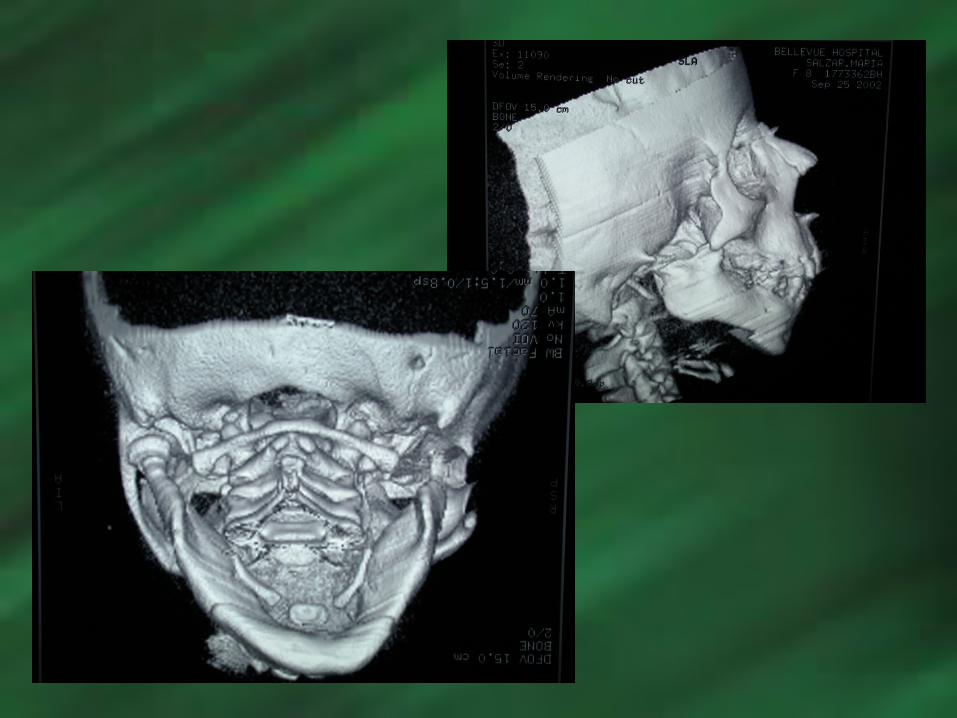





Initial
June 16, 2003

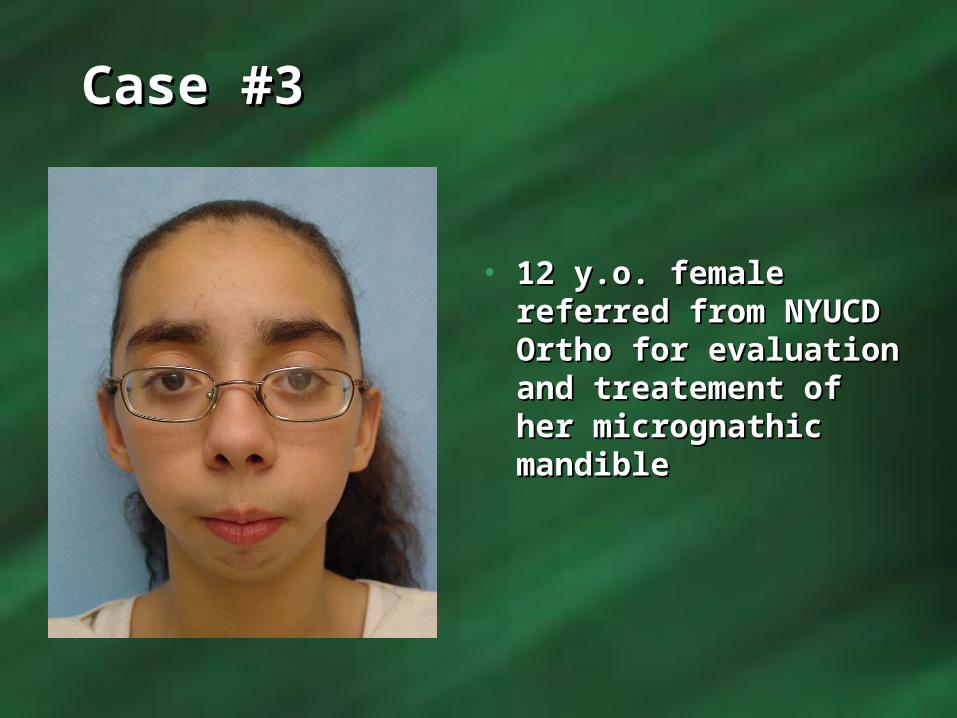
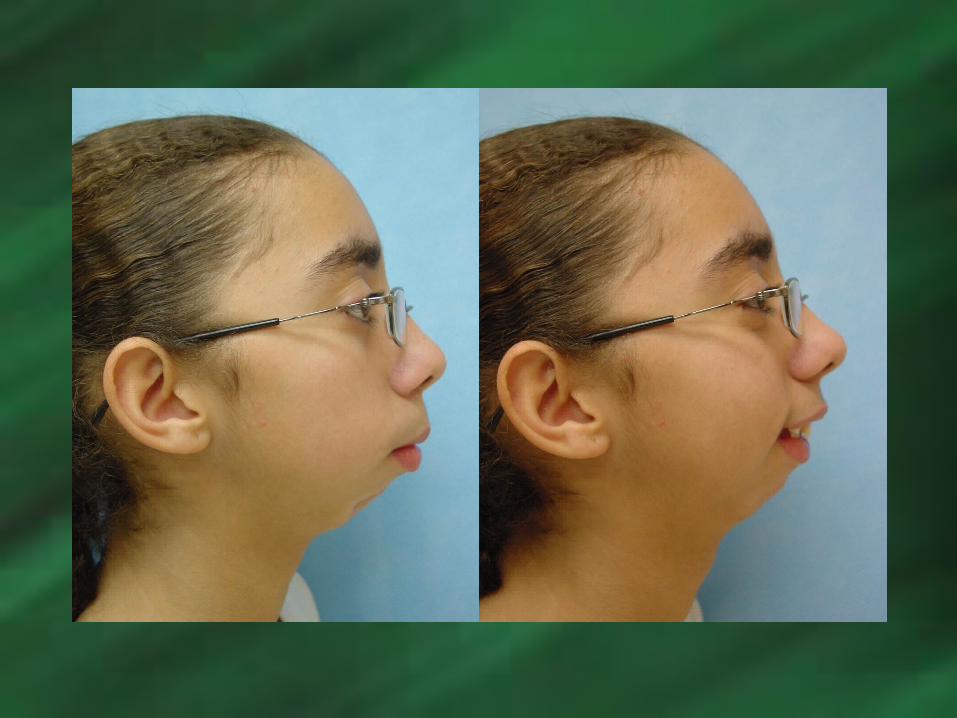
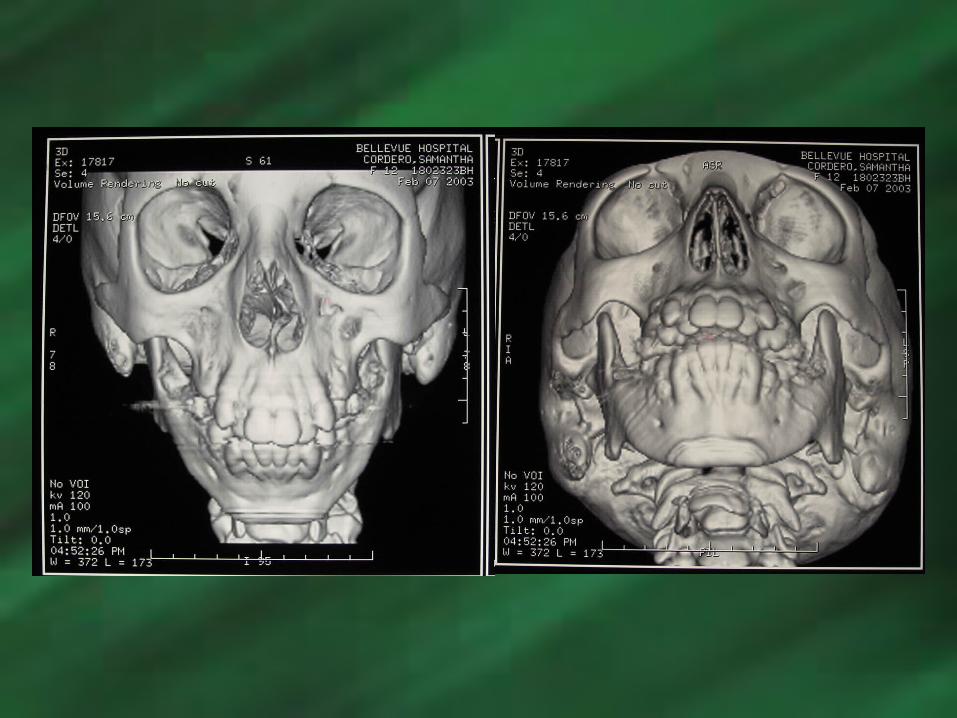
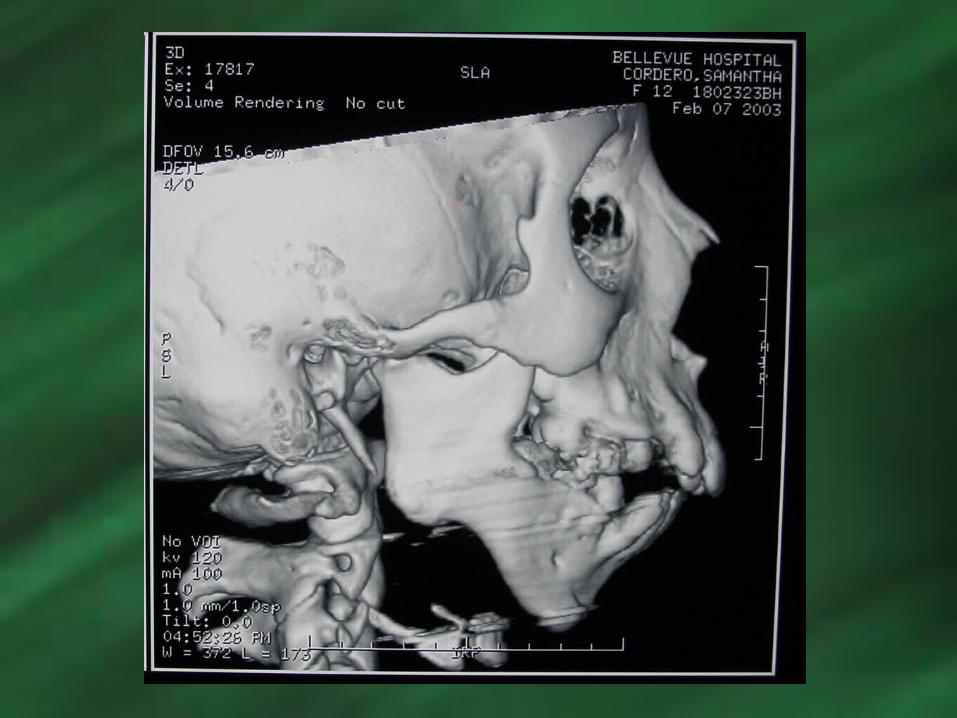
Case #3Case #3
• 12 y.o. female 12 y.o. female referred from NYUCD referred from NYUCD Ortho for evaluation Ortho for evaluation and treatement of and treatement of her micrognathic her micrognathic mandiblemandible


Maxillary Distraction Maxillary Distraction Osteogenesis Osteogenesis
Utilizing Intraoral Utilizing Intraoral AppliancesAppliances
Primary Applications:Primary Applications:
Patients with Moderate to Severe Patients with Moderate to Severe Maxillary Hypoplasia Requiring 8-15mm Maxillary Hypoplasia Requiring 8-15mm of Advancementof Advancement
Patients who require a maxillary Patients who require a maxillary advancement procedure and had advancement procedure and had previously undergone Cleft Lip and previously undergone Cleft Lip and Palate Repair and have developed large Palate Repair and have developed large quantities of fibrous scar tissue quantities of fibrous scar tissue This fibrous scar tissue promotes a high This fibrous scar tissue promotes a high
incidence of relapse when using incidence of relapse when using conventional orthognathic surgical conventional orthognathic surgical techniques (eg. Maxillary Advancement)techniques (eg. Maxillary Advancement)
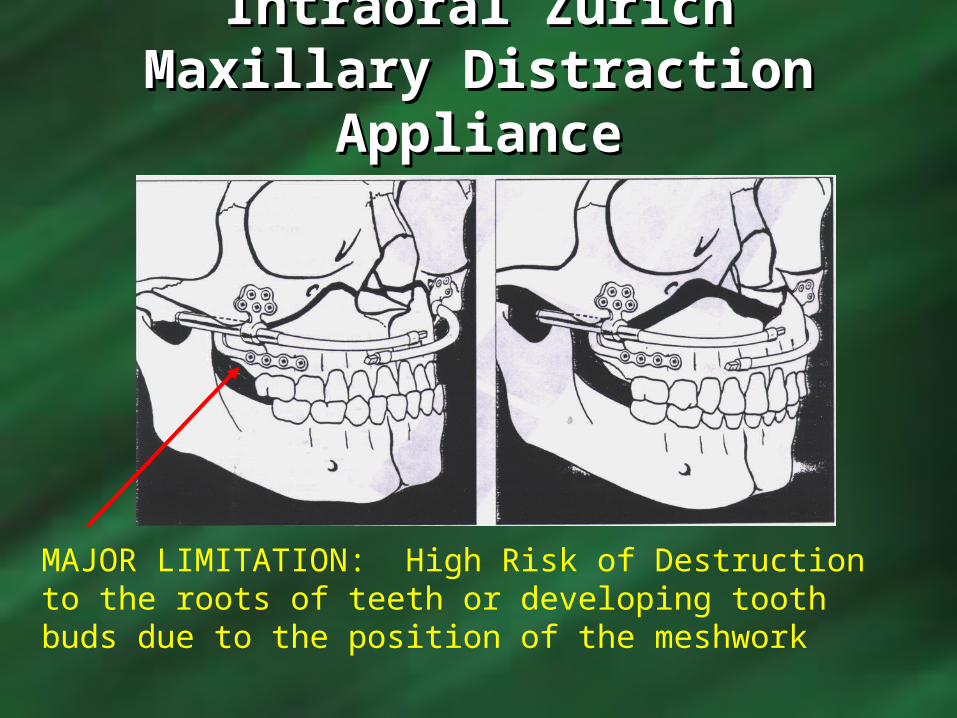
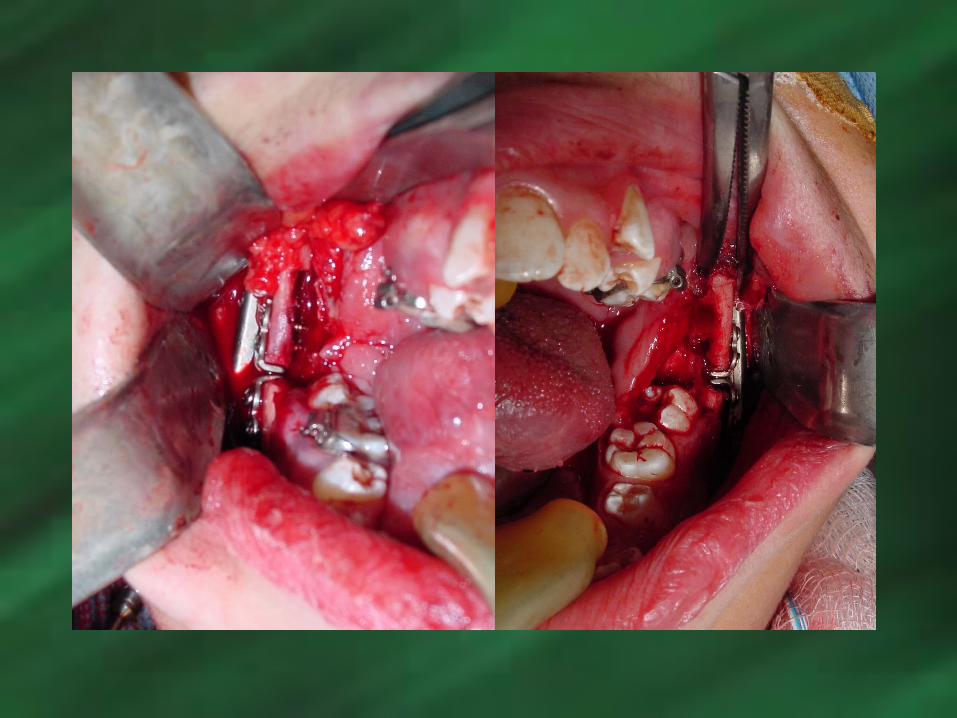
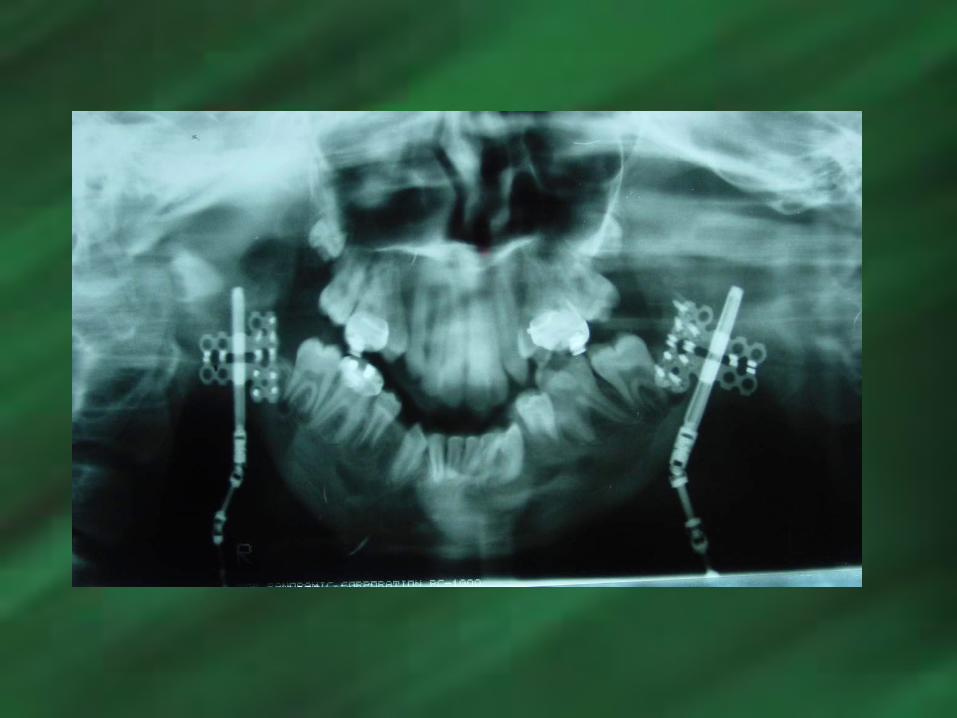
Intraoral Zurich Maxillary Intraoral Zurich Maxillary Distraction ApplianceDistraction Appliance
MAJOR LIMITATION: High Risk of Destruction to the roots of teeth or developing tooth buds due to the position of the meshwork
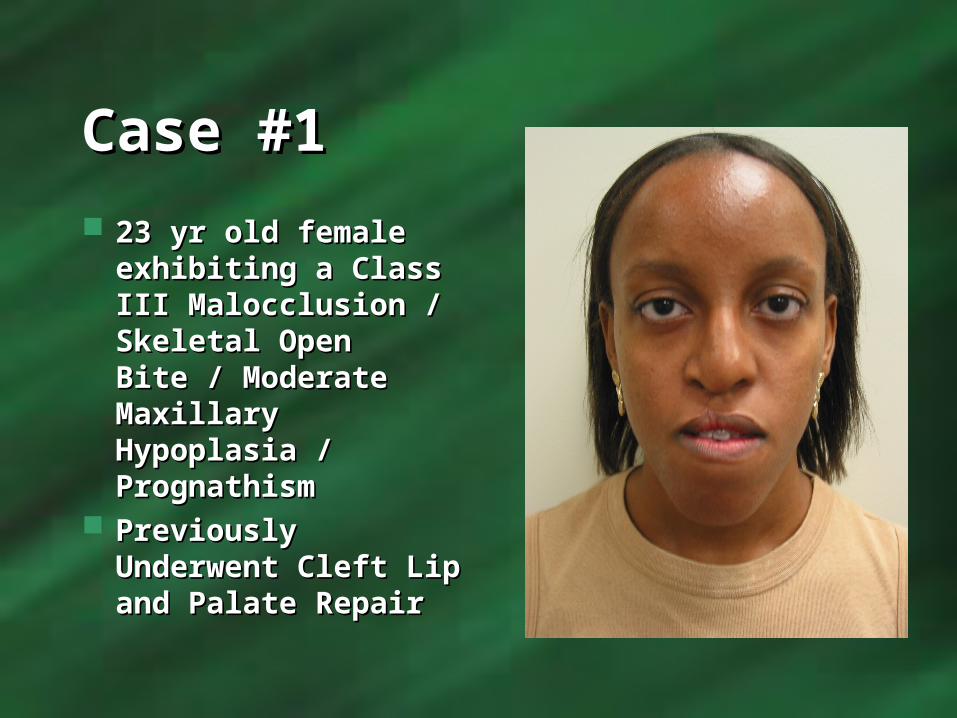
Case #1Case #1 23 yr old female 23 yr old female
exhibiting a Class III exhibiting a Class III Malocclusion / Malocclusion / Skeletal Open Bite / Skeletal Open Bite / Moderate Maxillary Moderate Maxillary Hypoplasia / Hypoplasia / PrognathismPrognathism
Previously Previously Underwent Cleft Lip Underwent Cleft Lip and Palate Repair and Palate Repair


Treatment PlanTreatment Plan PHASE I:PHASE I:
Maxillary Intraoral Distraction Maxillary Intraoral Distraction Advancing the Maxilla Forward and DownwardAdvancing the Maxilla Forward and Downward
PHASE II:PHASE II: Removal of Distraction Appliances Removal of Distraction Appliances Bilateral Intraoral Vertical Ramus Bilateral Intraoral Vertical Ramus
OsteotomiesOsteotomies Vertical Genioplasty ReductionVertical Genioplasty Reduction

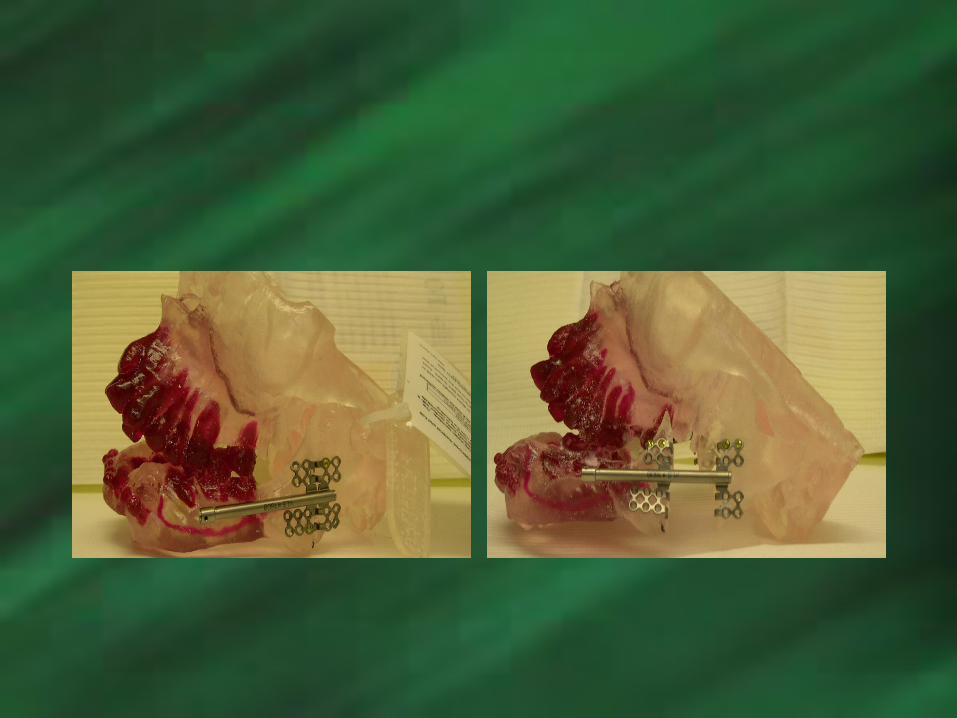
Maxillary Trans-SinusoidalMaxillary Trans-SinusoidalDistraction ApplianceDistraction Appliance
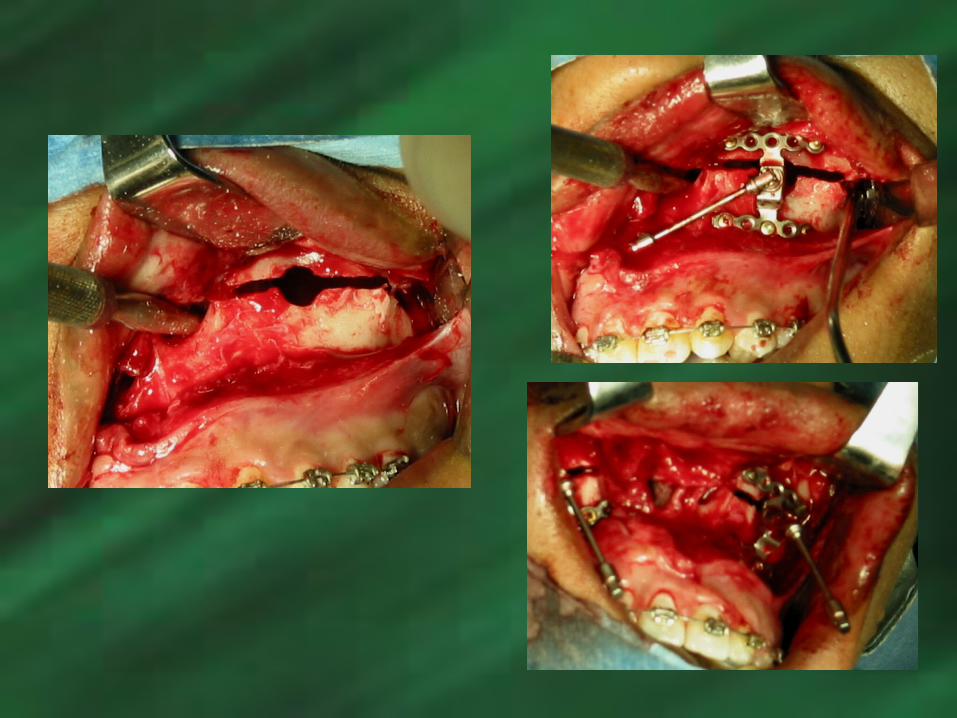
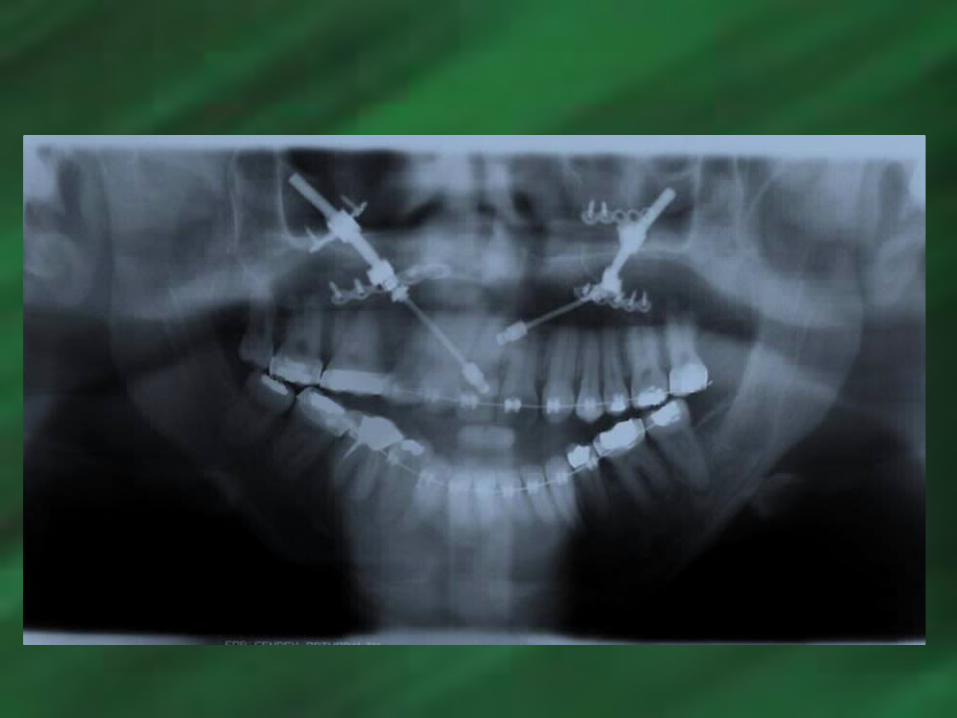


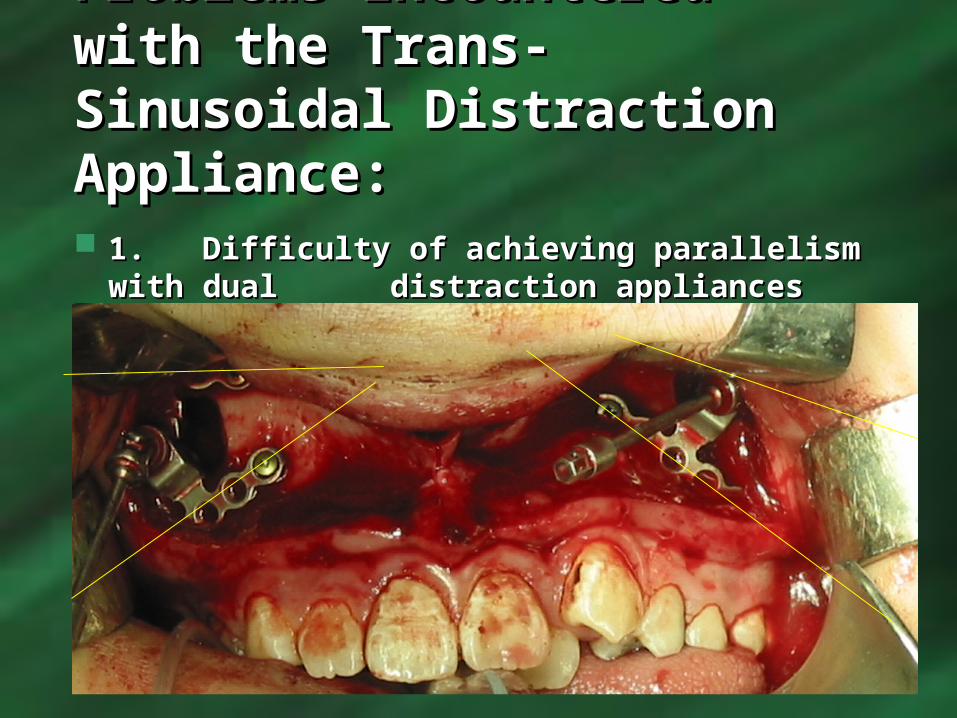
Problems Encountered Problems Encountered with the Trans-Sinusoidal with the Trans-Sinusoidal Distraction Appliance:Distraction Appliance: 1.1. Difficulty of achieving parallelism Difficulty of achieving parallelism
with dual with dual distraction appliancesdistraction appliances

2. Quality and Depth of Sinus2. Quality and Depth of Sinus
15 mm Distraction Arm
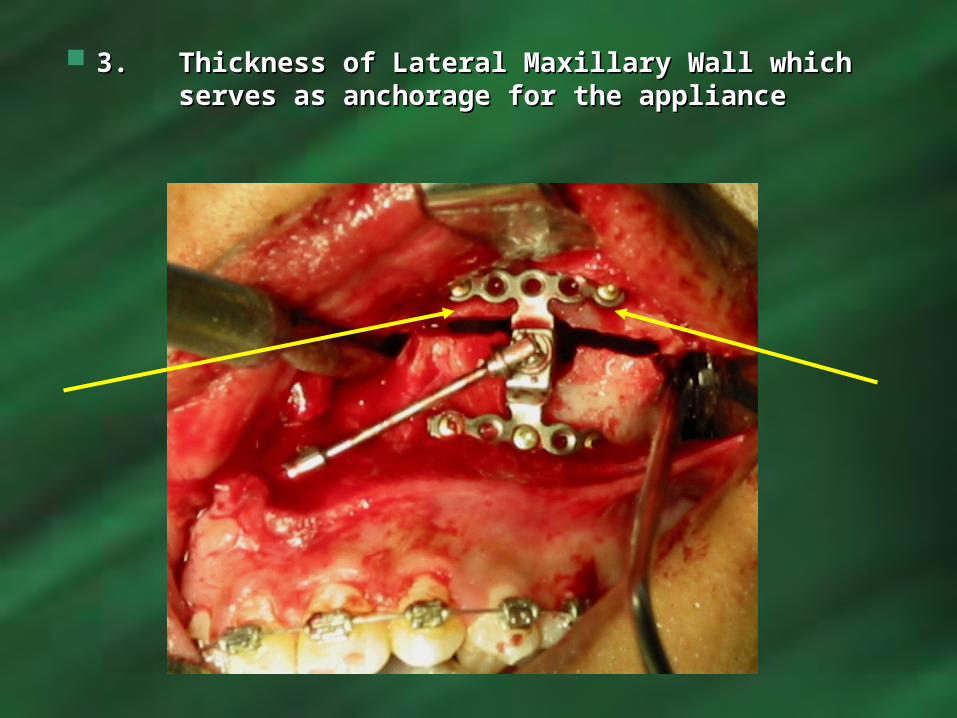
3. 3. Thickness of Lateral Maxillary Wall which Thickness of Lateral Maxillary Wall which serves as anchorage for the applianceserves as anchorage for the appliance
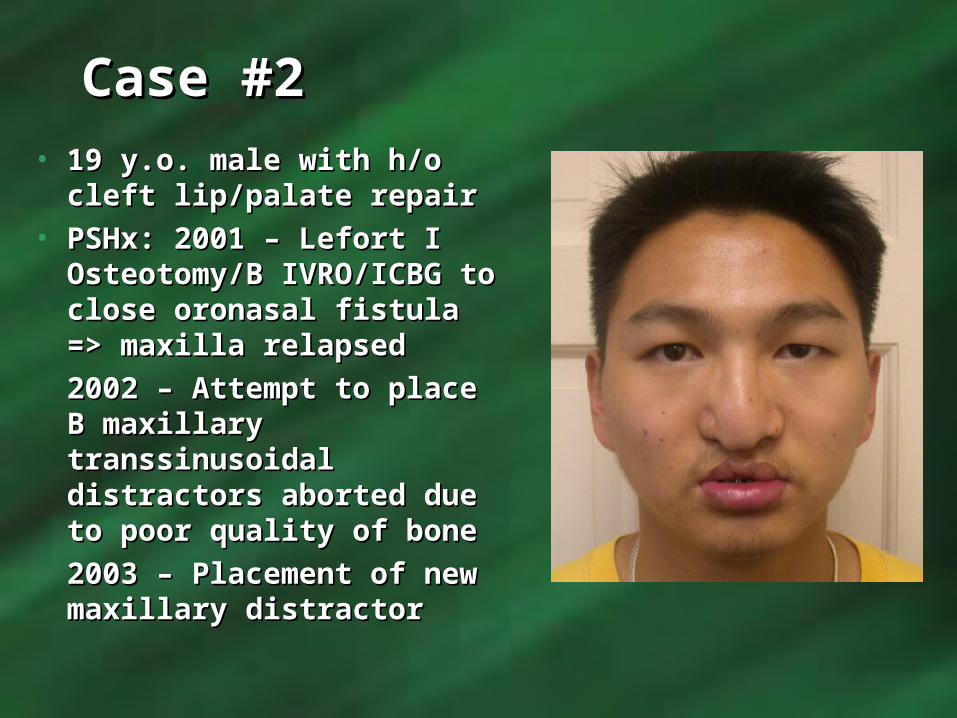
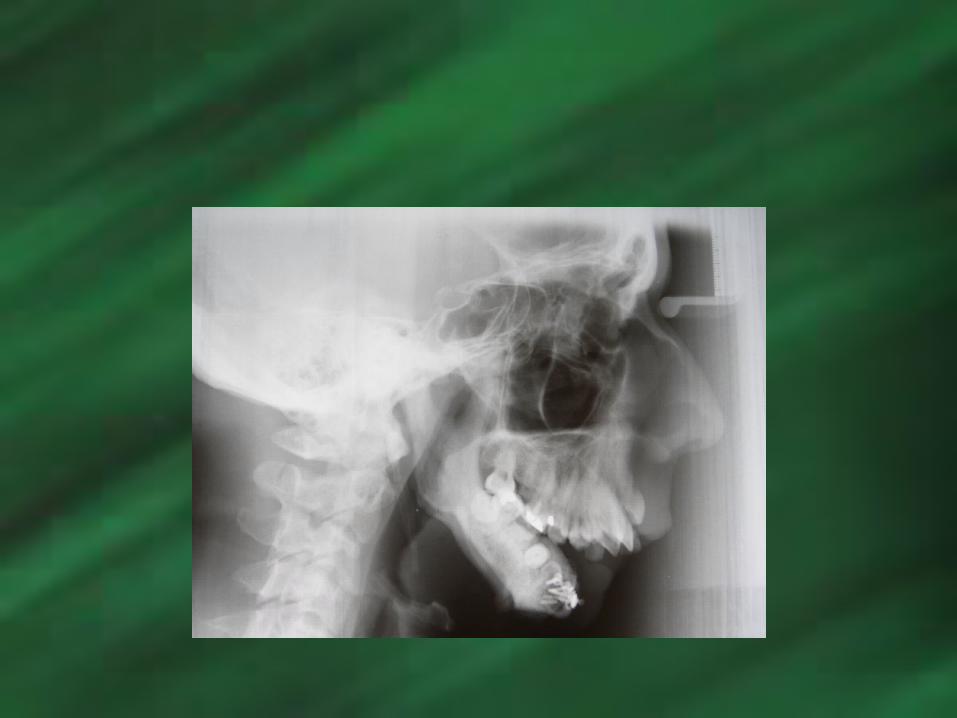
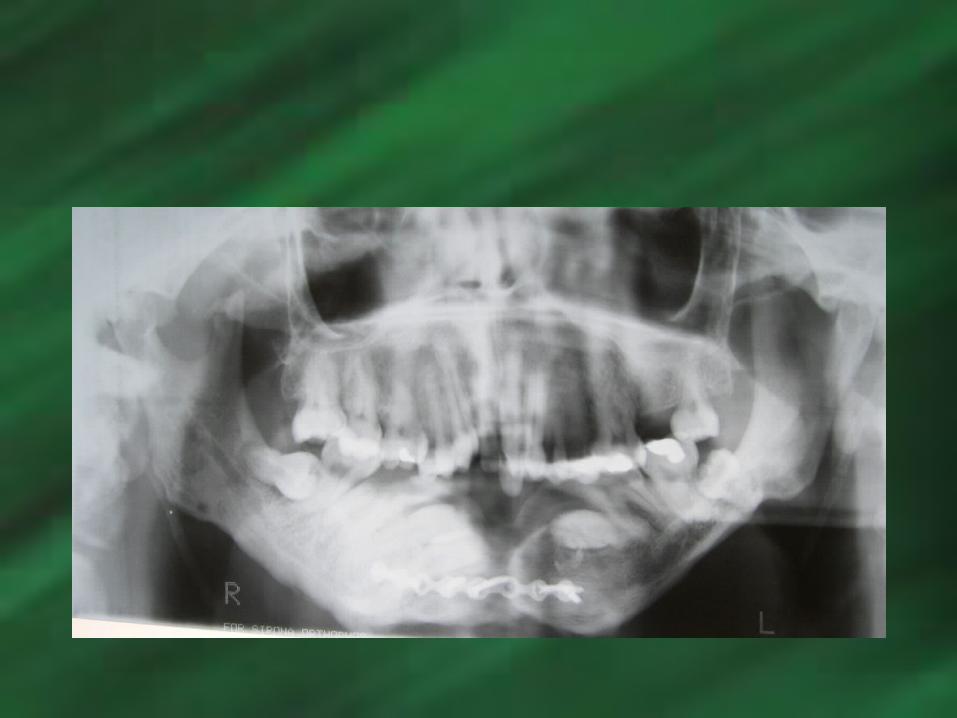
Case #2Case #2• 19 y.o. male with h/o cleft 19 y.o. male with h/o cleft
lip/palate repairlip/palate repair• PSHx: 2001 – Lefort I PSHx: 2001 – Lefort I
Osteotomy/B IVRO/ICBG Osteotomy/B IVRO/ICBG to close oronasal fistula to close oronasal fistula => maxilla relapsed=> maxilla relapsed2002 – Attempt to place B 2002 – Attempt to place B maxillary transsinusoidal maxillary transsinusoidal distractors aborted due distractors aborted due to poor quality of boneto poor quality of bone2003 – Placement of new 2003 – Placement of new maxillary distractormaxillary distractor







Before and 12 mos Before and 12 mos postoppostop
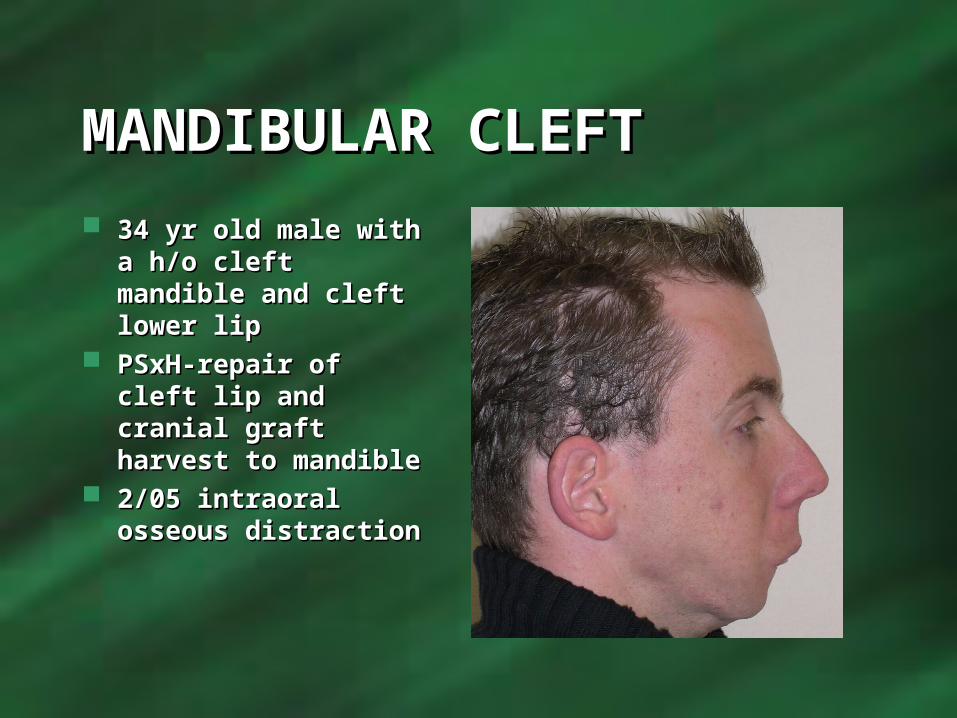
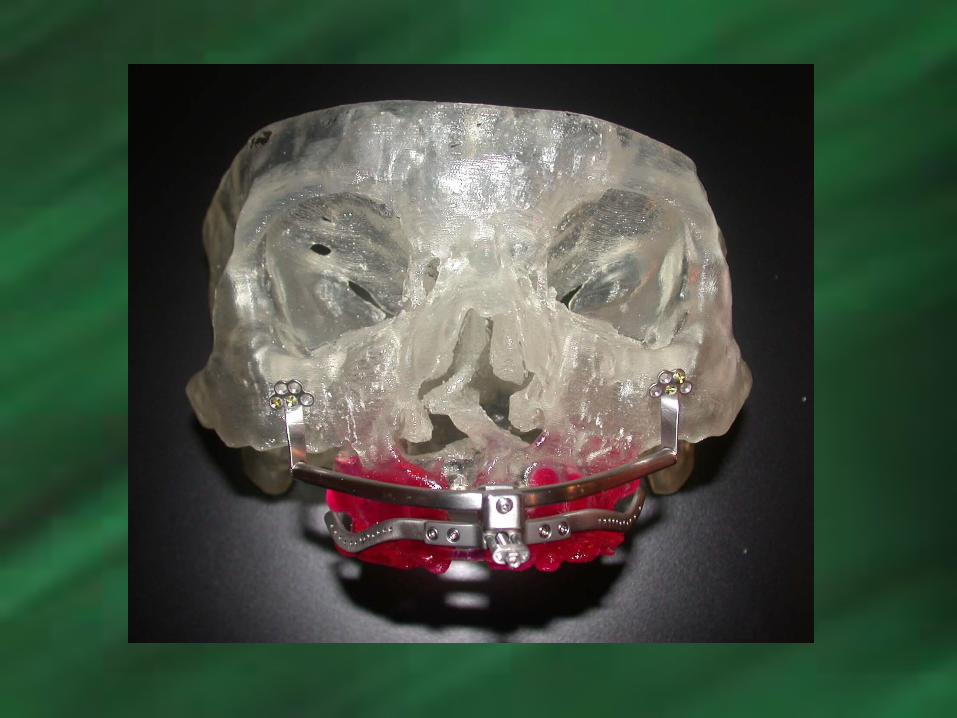
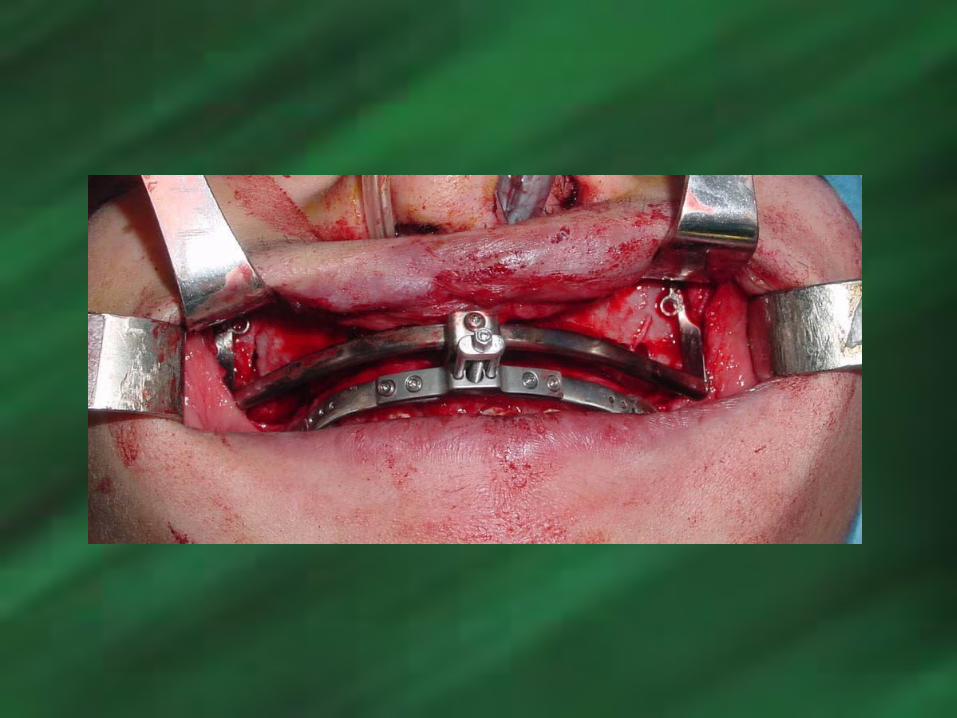
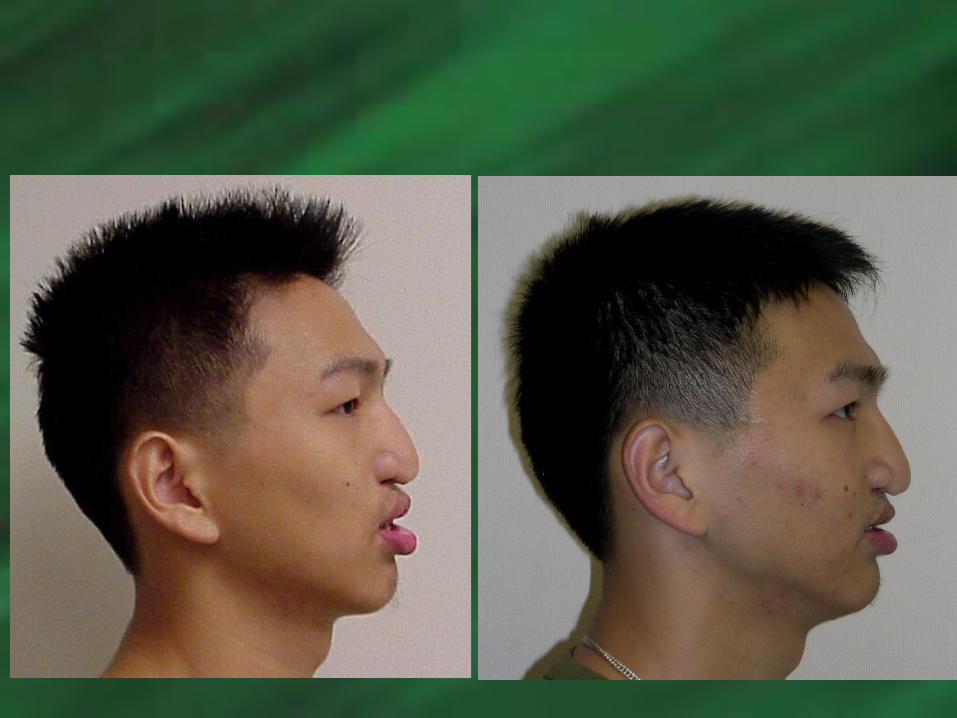
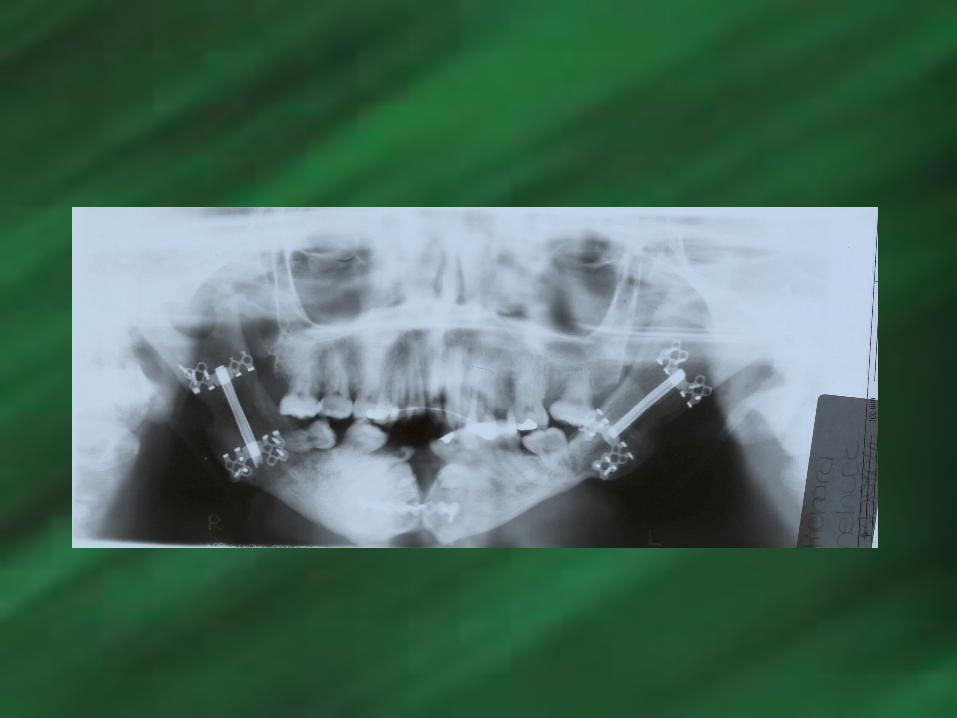
MANDIBULAR CLEFTMANDIBULAR CLEFT 34 yr old male with 34 yr old male with
a h/o cleft mandible a h/o cleft mandible and cleft lower lipand cleft lower lip
PSxH-repair of cleft PSxH-repair of cleft lip and cranial graft lip and cranial graft harvest to mandibleharvest to mandible
2/05 intraoral 2/05 intraoral osseous distractionosseous distraction




THE ENDTHE END
Thank YouThank You
Related Documents