DISTAL RADIUS FRACTURES Dr barun kumar patel Dnb orthopedic

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DISTAL RADIUS FRACTURES
Dr barun kumar patel
Dnb orthopedic
Distal Radius Fractures
Common injury
Potential for functional impairment and frequent complications
HISTORY
First surgeon to recognize these injuries was Pouteau 1783. his work was not widely publicized.
Later Abraham Colles 1814 gave the classic description of fracture
Dupuytren brought to the world attention that it is a fracture rather than a dislocation as it was previously assumed.
Goyrond 1832 differntiated between dorsal and volar displacement.
Barton 1838 described wrist subluxation consequent to intraarticular fracture of radius which could be dorsal or volar.
Smith described fracture of distal radius with ‘forward’ displacement.
Advent of X rays at the end of nineteenth century contributed much to the understanding of different patterns of injury.
Incidence
One sixth of all fractures treated in the Emergency Room
Bimodal distribution less than 30 years (70% men)
over 50 years (85% women) Males age 35 or older - 90 per 100,000 population
Introduction
Occurs through the distal metaphysis of the radius
May involve articular surface.
FOOSH
forced extension of the carpus,
impact loading of the distal radius.
Associated injuries may accompany distal radius
fractures.

Diagnosis: History and Physical Findings
History of a FOOSH
Wrist is typically swolen with ecchymosis and tender
Visible deformity of the wrist, with the hand most commonly displaced in the dorsal direction less comonly in volar direction
Movement of the hand and wrist are painful.
Adequate and accurate assessment of the neurovascular status of the hand is performed, before any treatment is carried out.

Diagnosis: Diagnostic Tests and Examination
General physical exam of the patient, including an evaluation of the injured joint, and a joint above and below
Radiographs of the injured wrist-pa and lat view , oblique view
CT scan of the distal radius to know extent of intrarticular involvement

Osseous Anatomy
Distal radius – 80% of axial load Scaphoid fossa Lunate fossa Sigmoid notch – DRUJ
Distal ulna

Anatomy scaphoid and lunate
fossa Ridge normally exists
between these two
sigmoid notch: second important articular surface
triangular fibrocartilage complex(TFCC): distal edge of radius to base of ulnar styloid
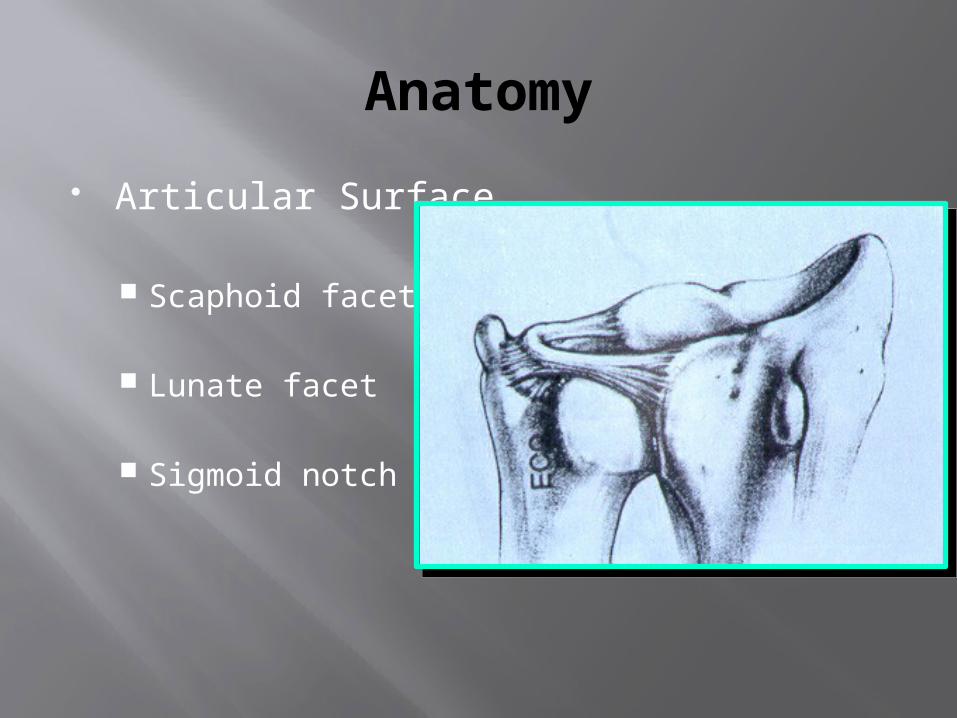
Anatomy
Articular Surface
Scaphoid facet
Lunate facet
Sigmoid notch

Normal range of movement

RADIOLOGY
Ulnar inclination (avg 23deg)
Volar inclination (avg 11 to 12deg)
Radial length (avg 11mm)
Ulnar variance (+ / - 1mm)
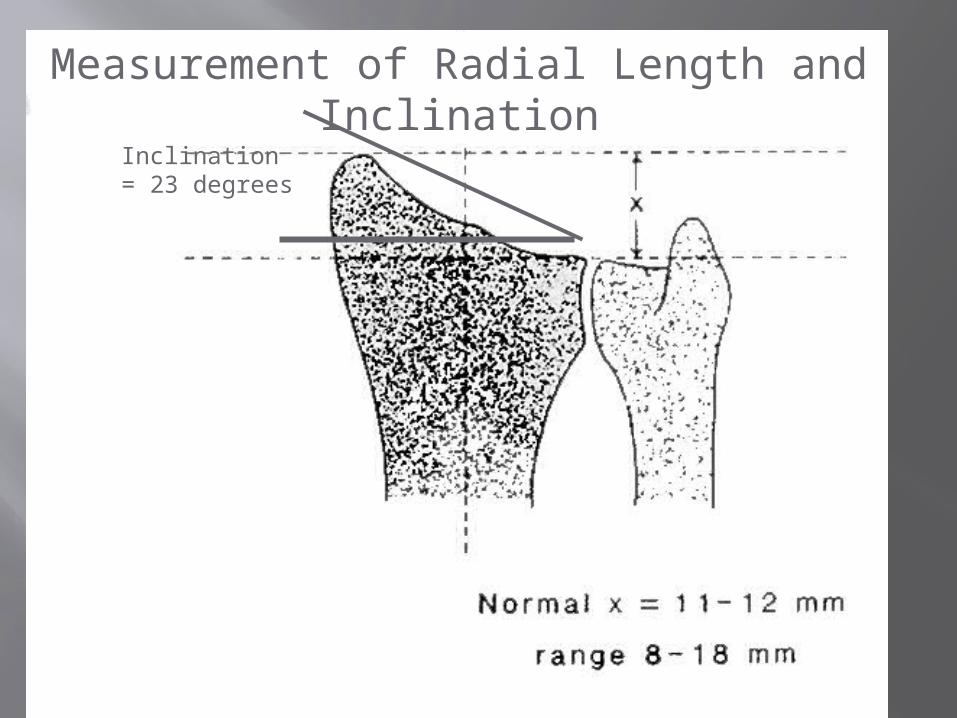
Measurement of Radial Length and Inclination
Inclination = 23 degrees

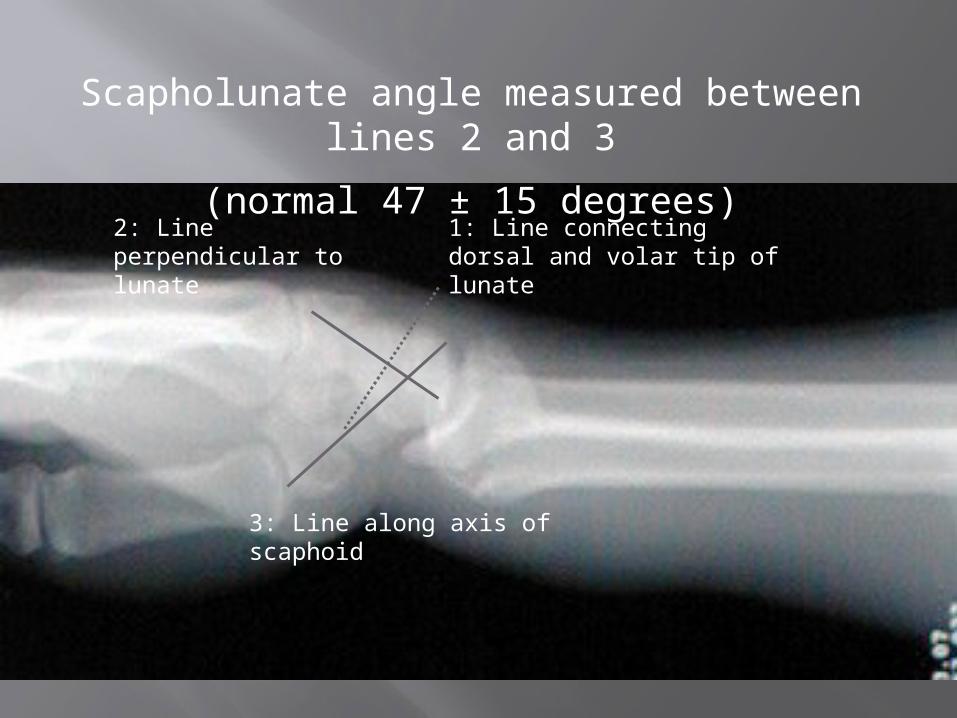
1: Line connecting dorsal and volar tip of lunate
2: Line perpendicular to lunate
3: Line along axis of scaphoid
Scapholunate angle measured between lines 2 and 3
(normal 47 ± 15 degrees)

Computed TomographyIndications:
Intra-articular fxs with multiple fragments
centrally impacted fragments
DRUJ incongruity
Cole et al: J Hand Surg, 1997
Classification of Distal Radius Fractures
Ideal system should describe: Type of injury Severity Evaluation Treatment Prognosis
Common Classifications
Column theory
Gartland/Werley Frykman Weber (AO/ASIF) Melone Fernandez (mechanism)
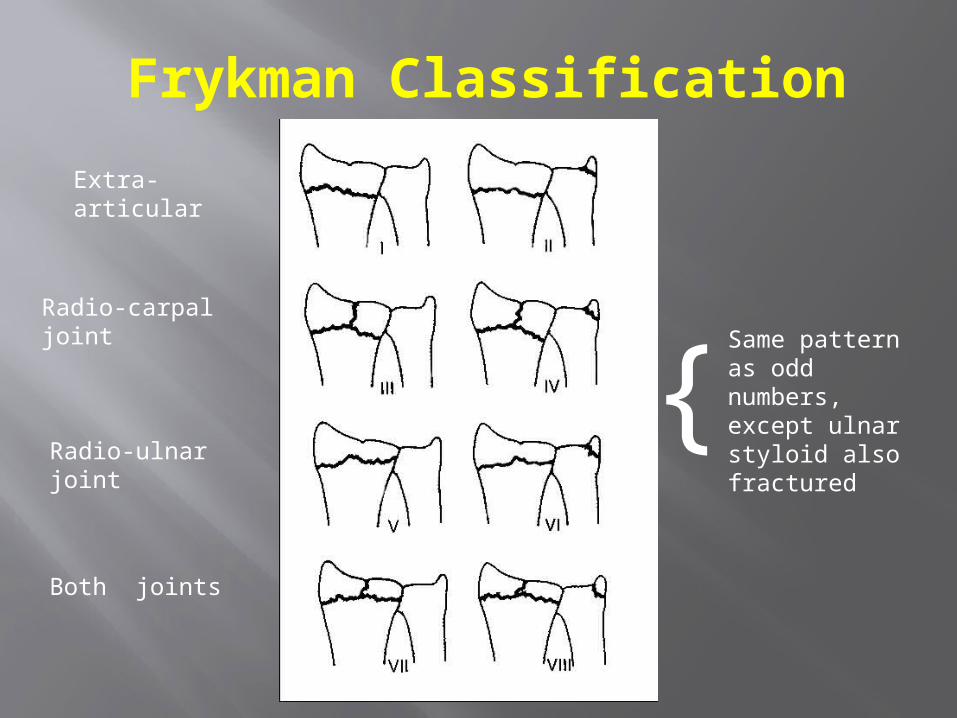
Frykman Classification
Extra-articular
Radio-carpal joint
Radio-ulnar joint
Both joints
{Same pattern as odd numbers, except ulnar styloid also fractured
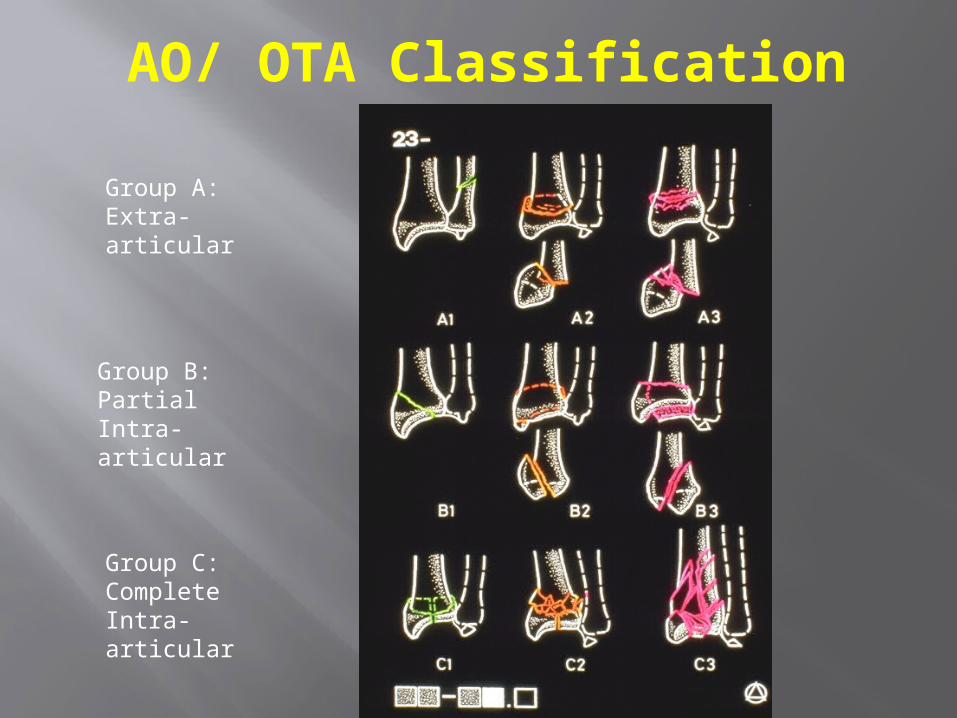
AO/ OTA Classification
Group A: Extra-articular
Group B: Partial Intra-articular
Group C: Complete Intra-articular

Gartland and Werley classification
Depends on three basic components of injury
1-metaphyseal comminution 2-intra articular extension 3-displacement of the fragment
Group i- simple colles # with no involvement
of radial articular surface Group ii- colles # with intra articula extension
without displacement Group iii- comminuted colles # with intra
articular extension with displacemet Group iv- extra articular undisplaced

COONEY (1990) UNIVERSAL CLASSIFICATION
Type I Extraarticular, undisplaced Type 2 Extraarticular, displaced Type 3 Intraarticular, undisplaced Type 4 Intraarticular, displaced
MODIFIED AO
Type A Extraarticular Type B Partial articular B1–radial styloid fracture B2–dorsal rim fracture B3–volar rim fracture B4–die-punch fracture Type C Complete articular

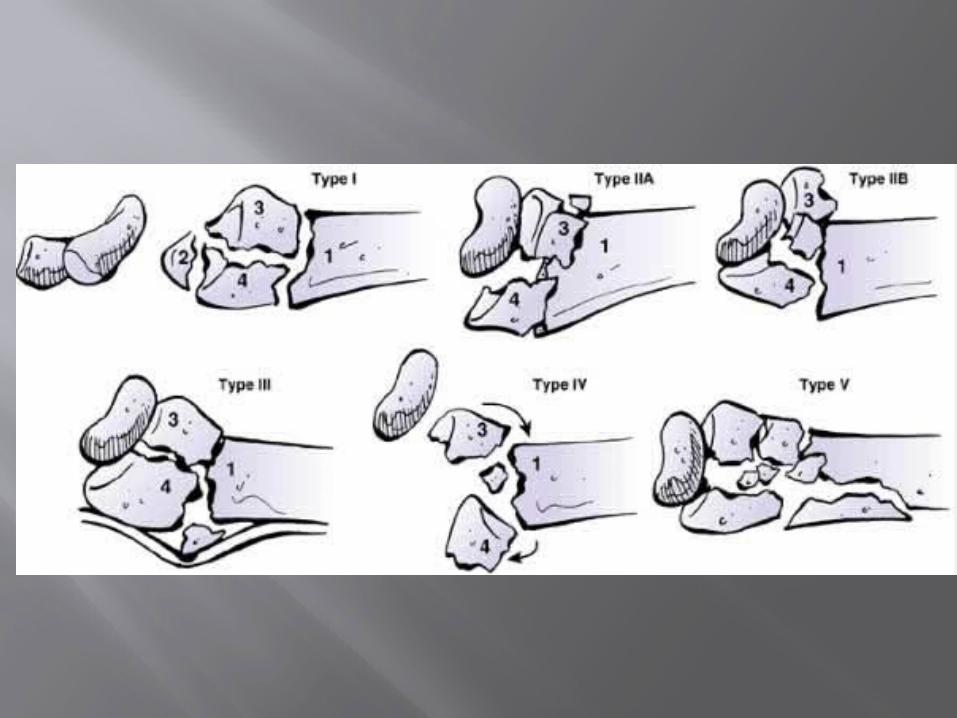
Melone classification
Depends on the impaction of the lunate on radial articular surface
Type i- stable # without displacement Type ii-unstable ‘die punch’ with
displacement of the characteristic fragment and comminution of the ant and post cotices
type ii A – reducible type iiB --irreducible
Type iii- ‘spike fracture’ ,unstable. Displacement of the articular surface and also proximal spike of radius
Type iv- ‘split’ fracture, unstable medial complex that is severly comminuted with separation and or rotation of the distal and proximal fragments
Type v- explosion injury
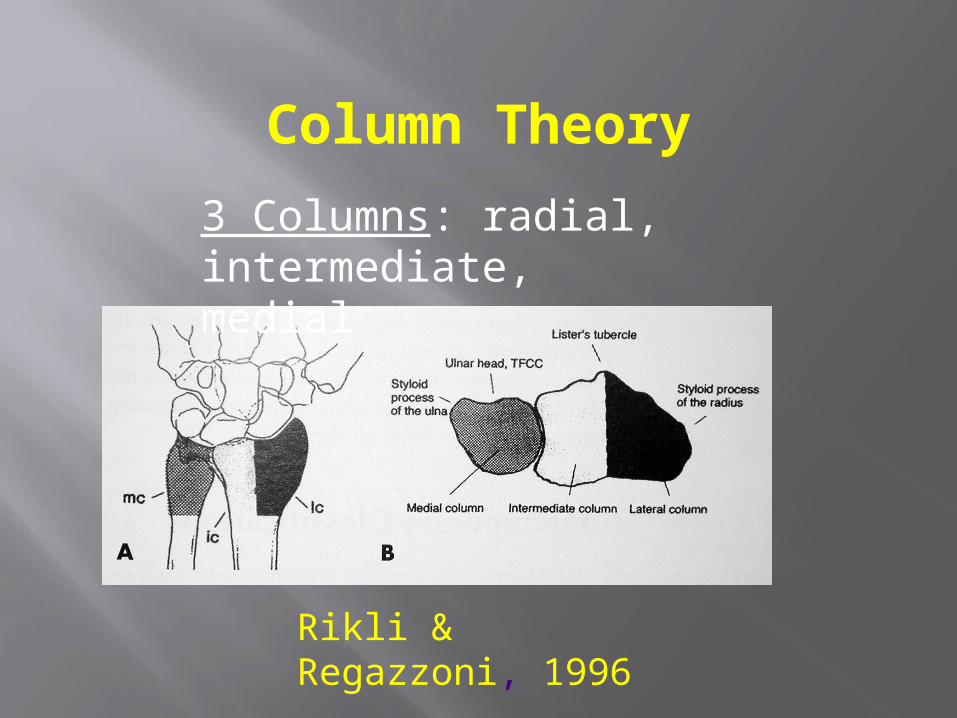
Column Theory
Rikli & Regazzoni, 1996
3 Columns: radial, intermediate, medial

Three Column Theory
Radial ColumnLateral side of radius
Intermediate ColumnUlnar side of
radius Ulnar Column
distal ulna
Radial column
Intermediate column
Ulnar column

Classification – Fernandez (1997)
I. Bending-metaphysis bending with loss of palmar tilt and radial shortening ,DRUJ injury(Colles, Smith)
II. Shearing-fractures of joint surface (Barton, radial styloid)
Classification – Fernandez (1997)
III. Compression-intraarticular fracture with impaction of subchondral and metaphyseal bone (die-punch)
IV. Avulsion-fractures of ligament attachments (ulna, radial styloid)
V. Combined/complex - high velocity injuries
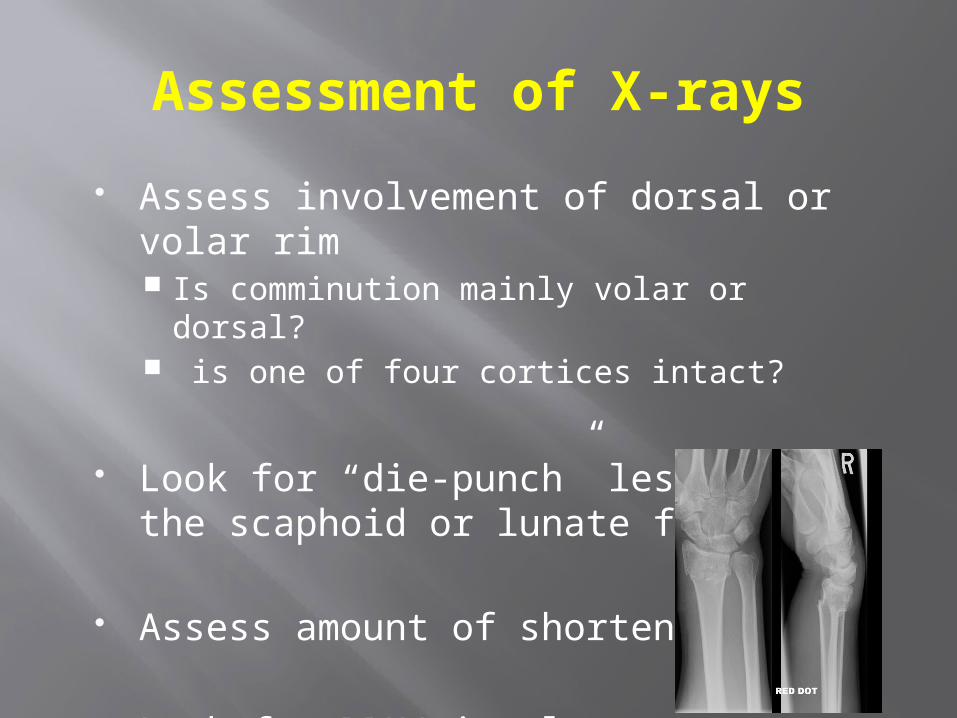
Assessment of X-rays
Assess involvement of dorsal or volar rim Is comminution mainly volar or dorsal? is one of four cortices intact?
Look for “die-punch” lesions of the scaphoid or lunate fossa.
Assess amount of shortening
Look for DRUJ involvement
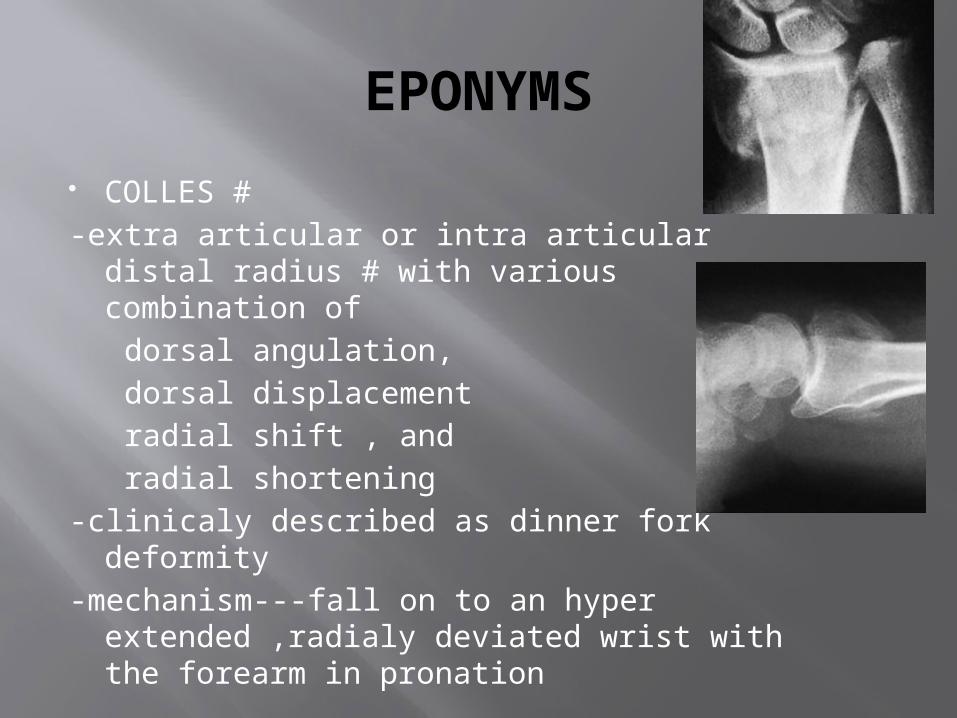
EPONYMS
COLLES #-extra articular or intra articular distal
radius # with various combination of dorsal angulation, dorsal displacement radial shift , and radial shortening-clinicaly described as dinner fork deformity-mechanism---fall on to an hyper
extended ,radialy deviated wrist with the forearm in pronation

SMITH #(REVERSE COLLES #)
# distal radius with volar angulation or volar displacement of the hand and distal radius
mechanism—fall on to a flexed wrist with the forearm fixed in supination
unstable pattern often requires ORIF because of difficulty in maintaining closed reduction
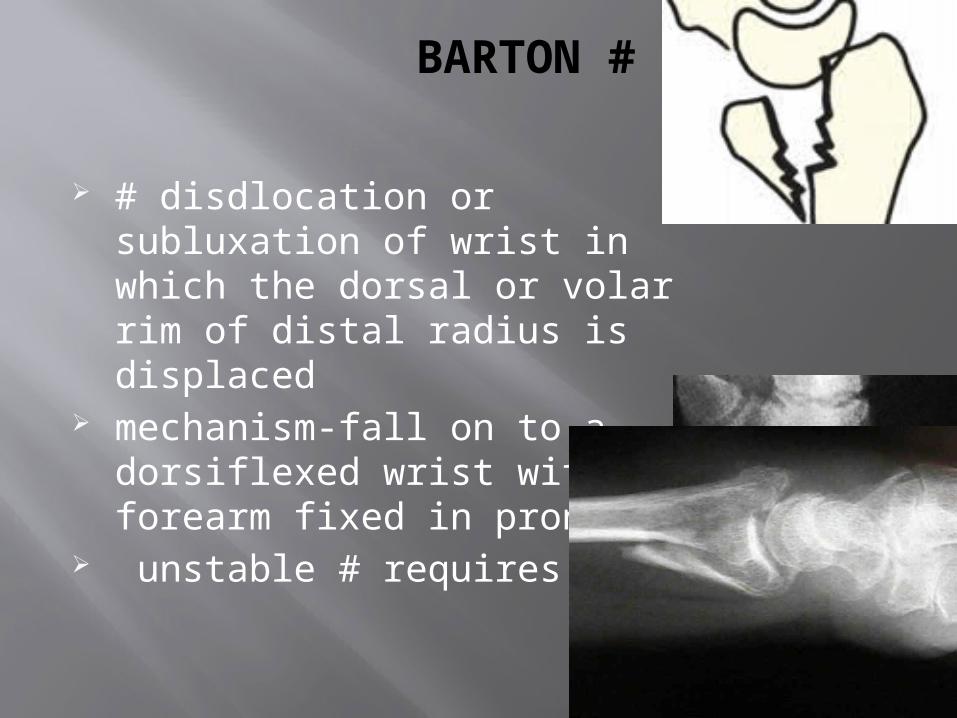
BARTON #
# disdlocation or subluxation of wrist in which the dorsal or volar rim of distal radius is displaced
mechanism-fall on to a dorsiflexed wrist with the forearm fixed in pronation
unstable # requires ORIF
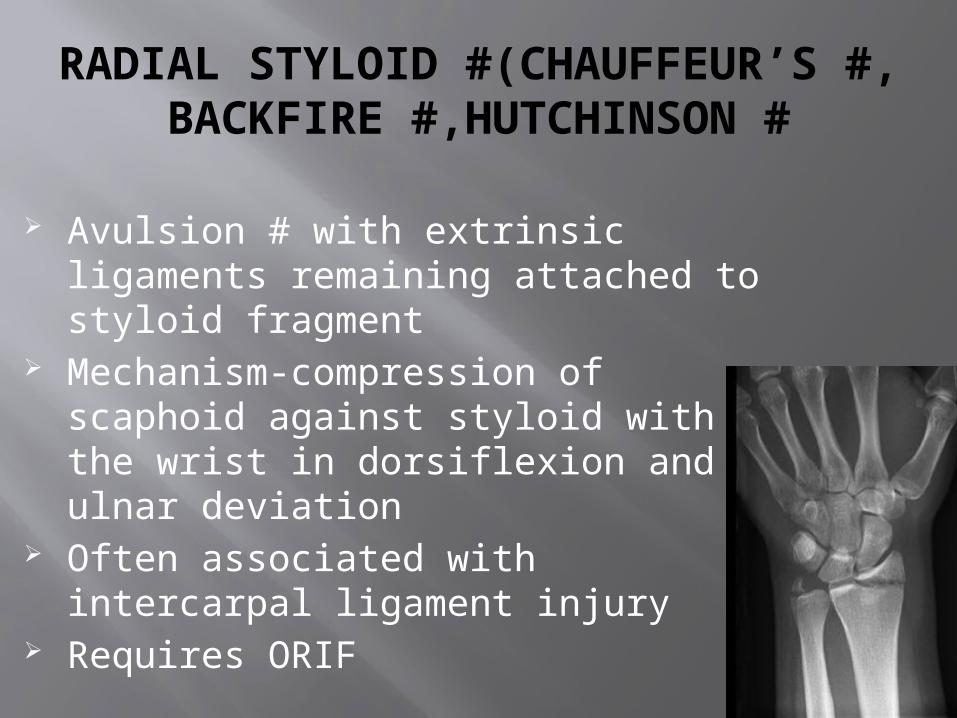
RADIAL STYLOID #(CHAUFFEUR’S #, BACKFIRE #,HUTCHINSON #
Avulsion # with extrinsic ligaments remaining attached to styloid fragment
Mechanism-compression of scaphoid against styloid with the wrist in dorsiflexion and ulnar deviation
Often associated with intercarpal ligament injury
Requires ORIF
ASSESSMENT OF STABILITY
five factors indicative of instability (1)initial dorsal angulation of more than 20
degrees (volar tilt),(2) dorsal metaphyseal comminution,(3) intraarticular involvement, (4) an associated ulnar fracture, and(5) patient age older than 60 years
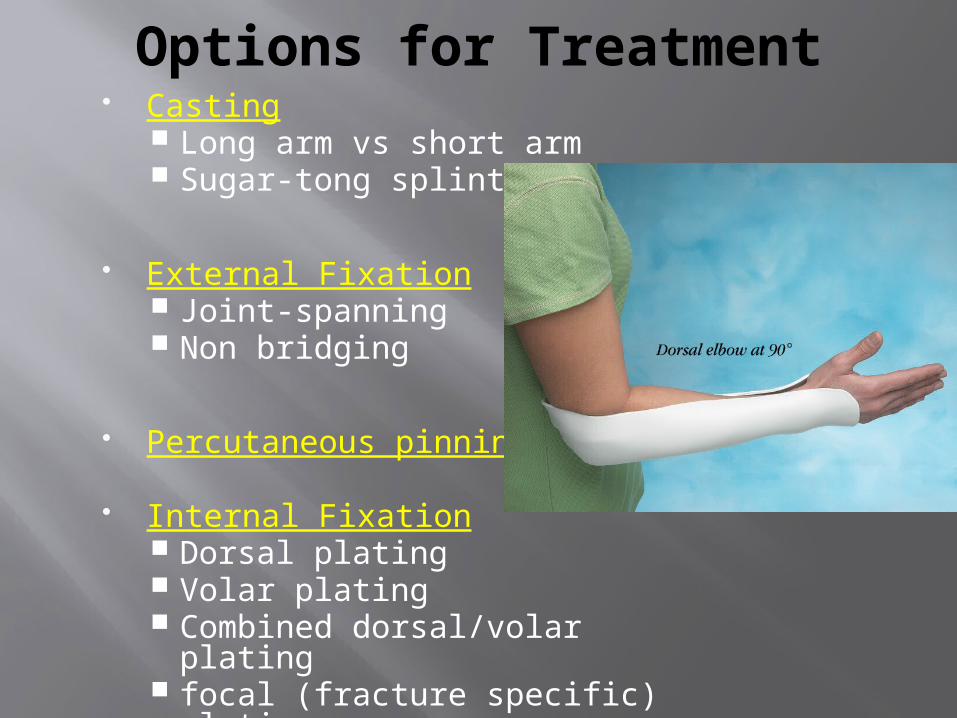
Options for Treatment Casting
Long arm vs short arm Sugar-tong splint
External Fixation Joint-spanning Non bridging
Percutaneous pinning
Internal Fixation Dorsal plating Volar plating Combined dorsal/volar plating focal (fracture specific) plating

Treatment Goals
Preserve hand and wrist function
Realign normal osseous anatomy
promote bony healing
Avoid complications
Allow early finger and elbow ROM
Indications for Closed Treatment
Low-energy fracture
Medical co-morbidities
Minimal displacement- acceptable alignment
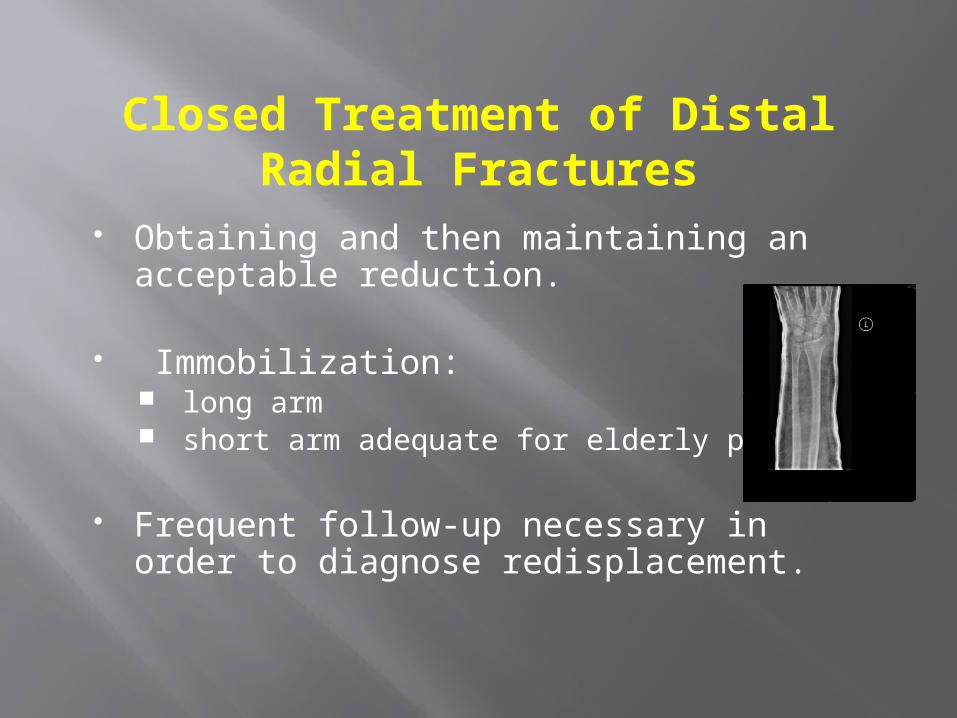
Closed Treatment of Distal Radial Fractures
Obtaining and then maintaining an acceptable reduction.
Immobilization: long arm short arm adequate for elderly patients
Frequent follow-up necessary in order to diagnose redisplacement.
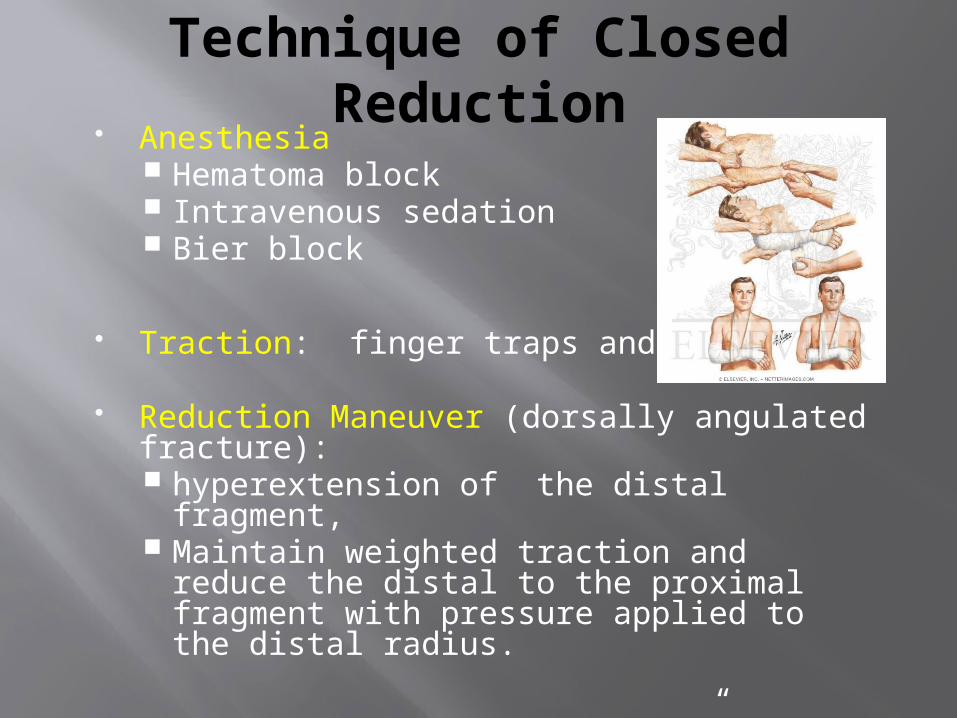
Technique of Closed Reduction
Anesthesia Hematoma block Intravenous sedation Bier block
Traction: finger traps and weights
Reduction Maneuver (dorsally angulated fracture): hyperextension of the distal fragment, Maintain weighted traction and reduce the
distal to the proximal fragment with pressure applied to the distal radius.
Apply well-molded “sugar-tong” splint or cast, with wrist in neutral to slight flexion.
Avoid Extreme Positions!
Acceptable Reduction Criteria
Radial length- within 2-3 mm of the controlateral wrist
Palmar tilt- neutral tilt(o degree ) intrarticular step-off or gap< 2mm Radial inclination <5 degree loss Carpal malalignment – absent Ulnar variance- no more than 2 mm of
shortening compare to ulnar head

After-treatment
Watch for median nerve symptoms parasthesias common but should diminish
over few hours If persist release pressure on cast, take
wrist out of flexion Acute carpal tunnel: symptoms progress;
CTR required
Follow-up x-rays needed in 1-2 weeks to evaluate reduction.
Change to short-arm cast after 2-3 weeks, continue until fracture healing.
Management of Redisplacement
Repeat reduction and casting – high rate of failure
Repeat reduction and percutaneous pinning External Fixation ORIF

Indications for Immediate Surgical Treatment
High-energy injury Open injury Secondary loss of reduction Articular comminution, step-off, or gap Metaphyseal comminution or bone loss Loss of volar buttress with
displacement DRUJ incongruity
Operative Management of Distal Radius Fractures

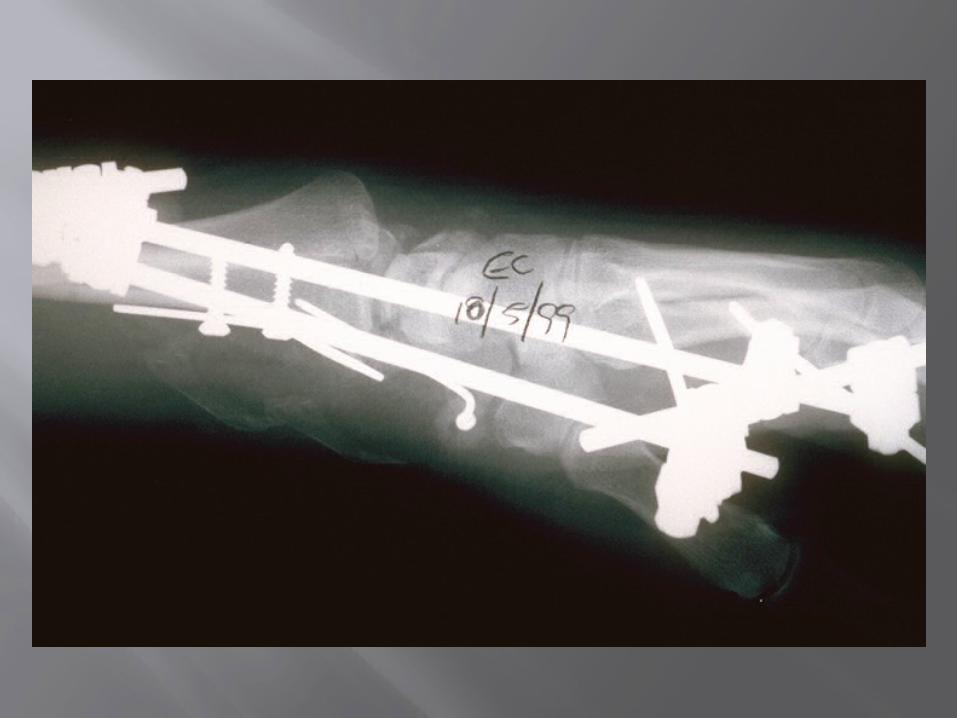
External fixation:
The treatment of choice for distal radius fractures
in the 1980’s

Types of External Fixation
Spanning Dynamic
Clyburne Agee Pennig
Static AO Ace
Non-spanning Hoffman 2 Cobra Zimmer AO
Neutralize the axial load imparted by physiologic forearm musculature
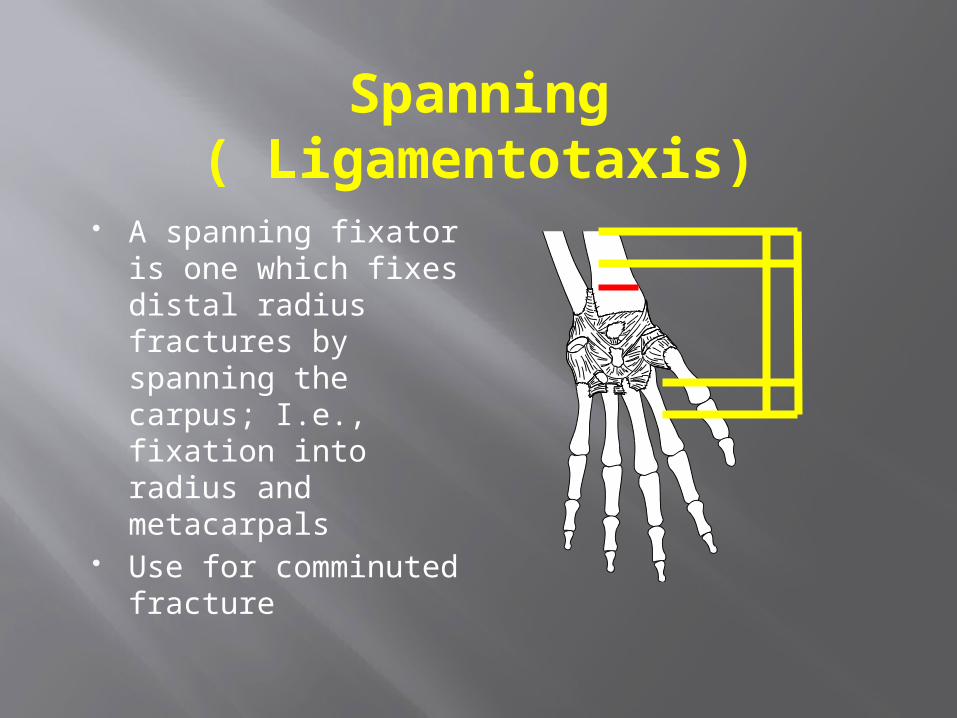
Spanning ( Ligamentotaxis)
A spanning fixator is one which fixes distal radius fractures by spanning the carpus; I.e., fixation into radius and metacarpals
Use for comminuted fracture
Used to restore radial length and radial inclination but palmer tilt is rarely restored
Supplemental k wire fixation is needed to prevent loss of palmer tilt and some degree of colapse
Pins are retained for 6 to 8 weeks Overdistraction results in finger stiffness

Complications
Mal-union Pin track infection Finger stiffness Loss of reduction; early vs late Tendon rupture

Non-spanning
A non-spanning fixator is one which fixes distal radius fracture by securing pins in the radius alone, proximal to and distal to the fracture site.
Indicated for extra articular or minimal intra articular dorsaly displaced fracture
Minimum 1 cm of intact volar cortex is required to give purchase for the pins
Better to preserve volar tilt and carpal malalignment

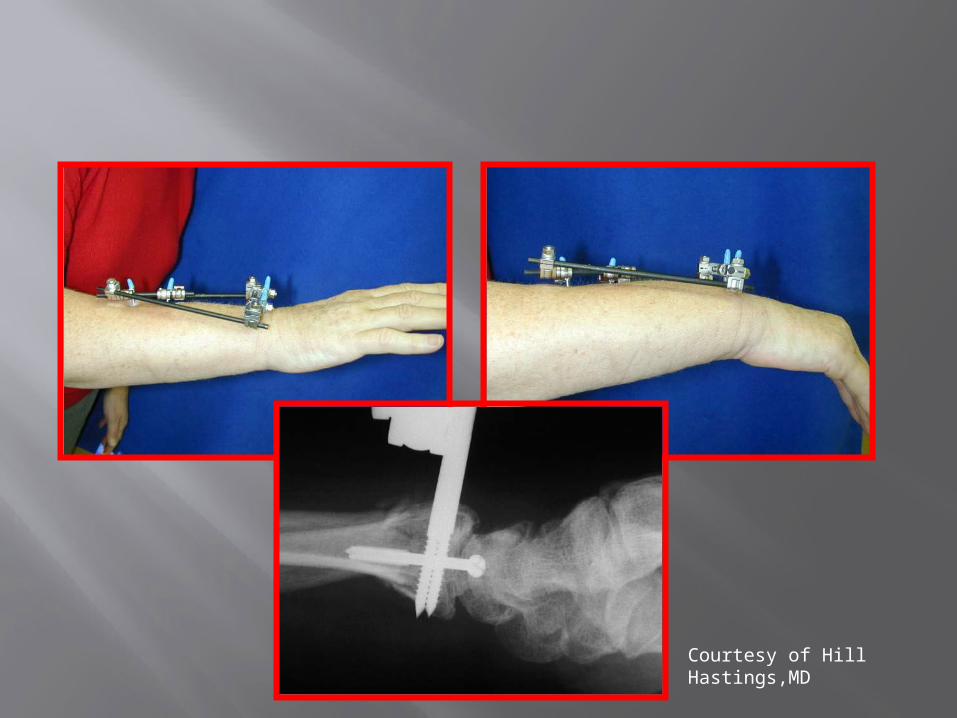
Courtesy of Hill Hastings,MD

External Fixation- Disadvantages -
Bulky
Poor screw hold in porosis and comminution
Screws do not buttress
Cutaneous radial nerve injury
Pin tract infection
Reflex sympathetic dystrophy

Postoperative care
Wrist is immobilized in a supinated position with sugar tongue splint for 10 days
External fixator frame is removed at 6 weeks
Any supplemental pins are kept in place for 8 weeks
Active and passive finger motion is begun as soon as the anesthesia wears off
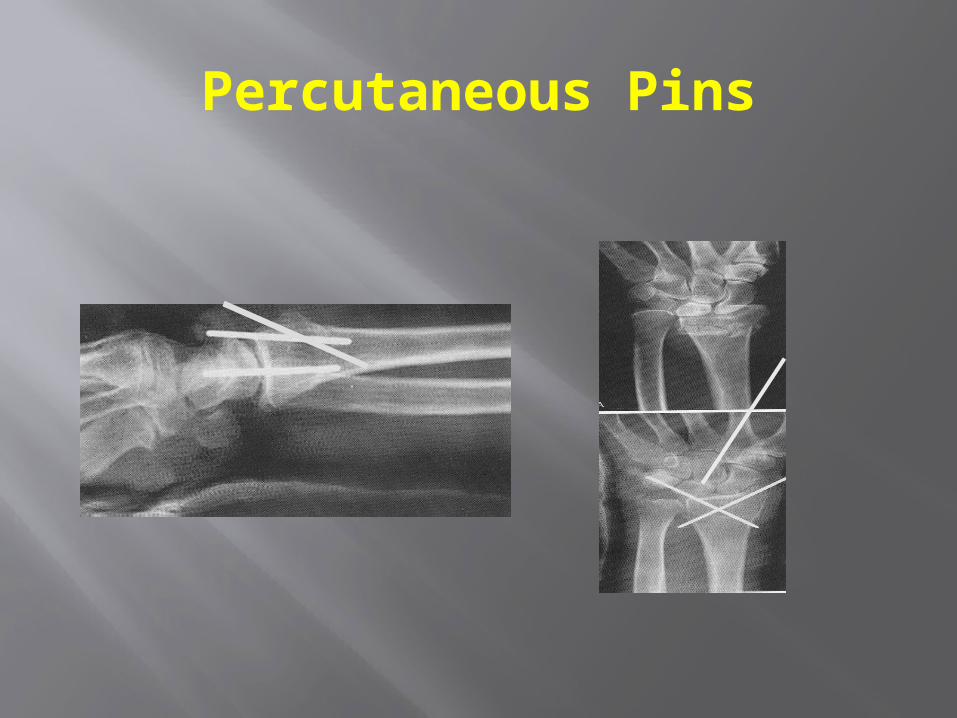
Percutaneous Pins

Percutaneous Pinning-Methods most common radial styloid pinning
+ dorsal-ulnar corner of radius pinning
supplemental immobilization with cast, splint
in conjunction with external fixation (Augmented external fixation)
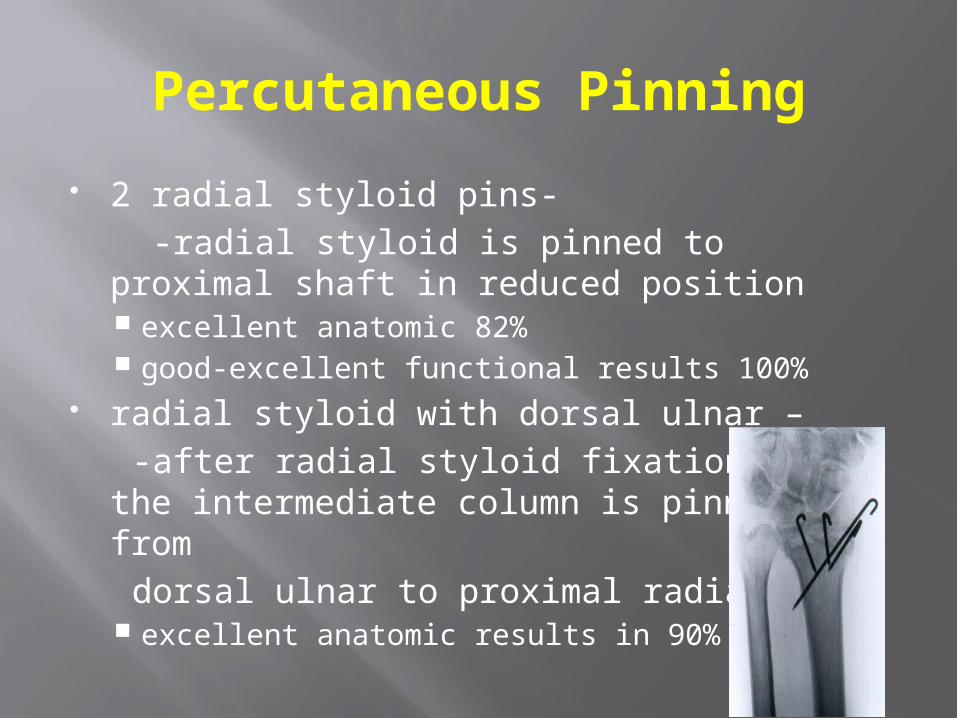
Percutaneous Pinning
2 radial styloid pins- -radial styloid is pinned to proximal
shaft in reduced position excellent anatomic 82% good-excellent functional results 100%
radial styloid with dorsal ulnar – -after radial styloid fixation the
intermediate column is pinned from dorsal ulnar to proximal radial
excellent anatomic results in 90%
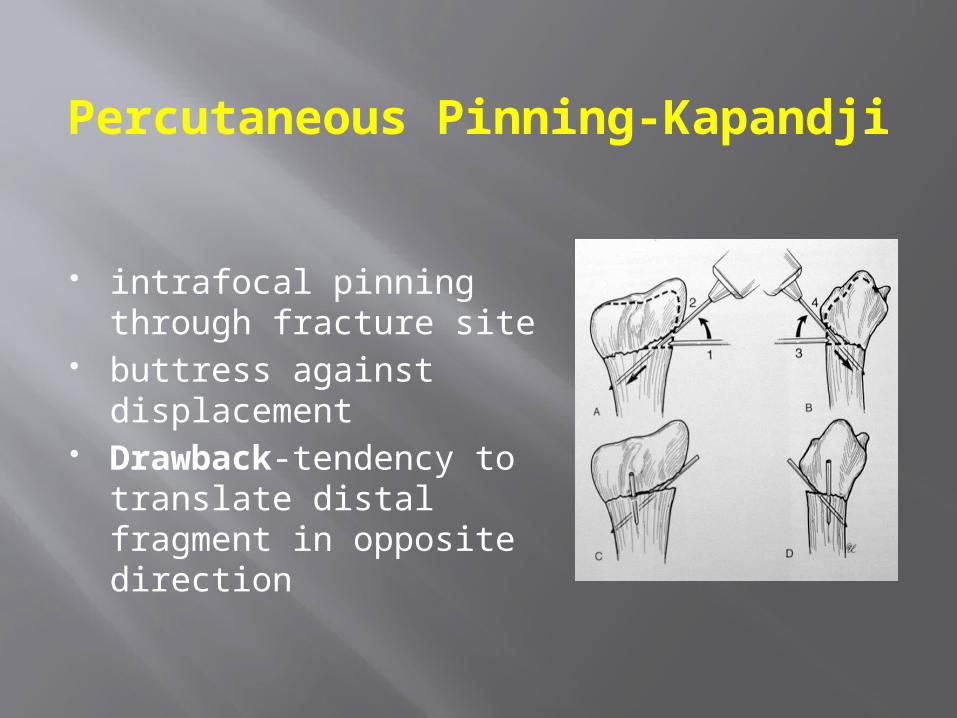
Percutaneous Pinning-Kapandji
intrafocal pinning through fracture site
buttress against displacement
Drawback-tendency to translate distal fragment in opposite direction
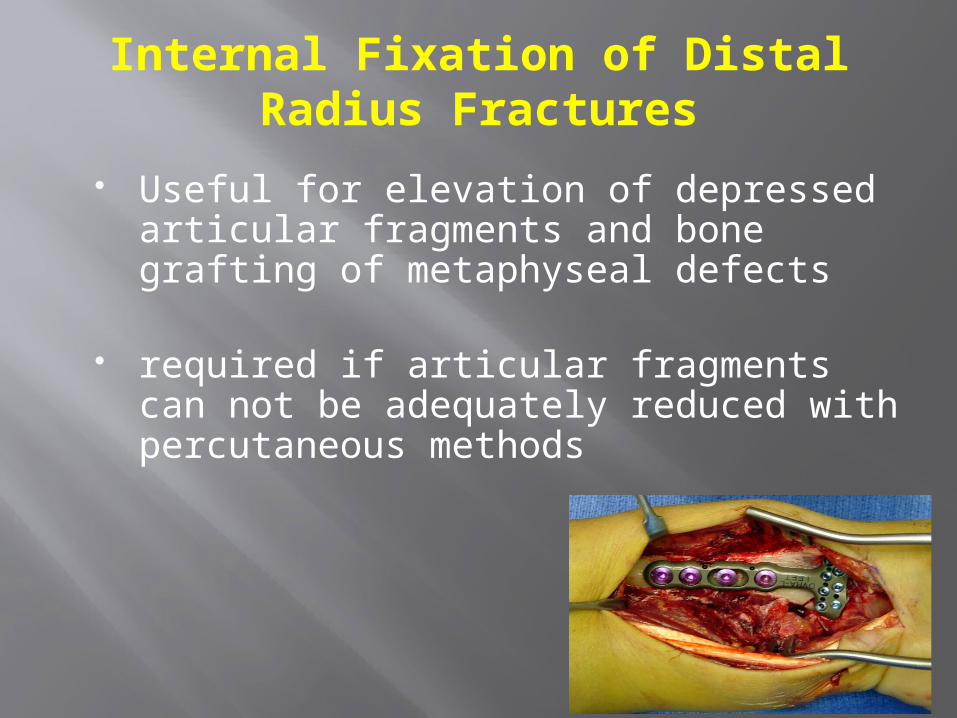
Internal Fixation of Distal Radius Fractures
Useful for elevation of depressed
articular fragments and bone grafting of metaphyseal defects
required if articular fragments can not be adequately reduced with percutaneous methods
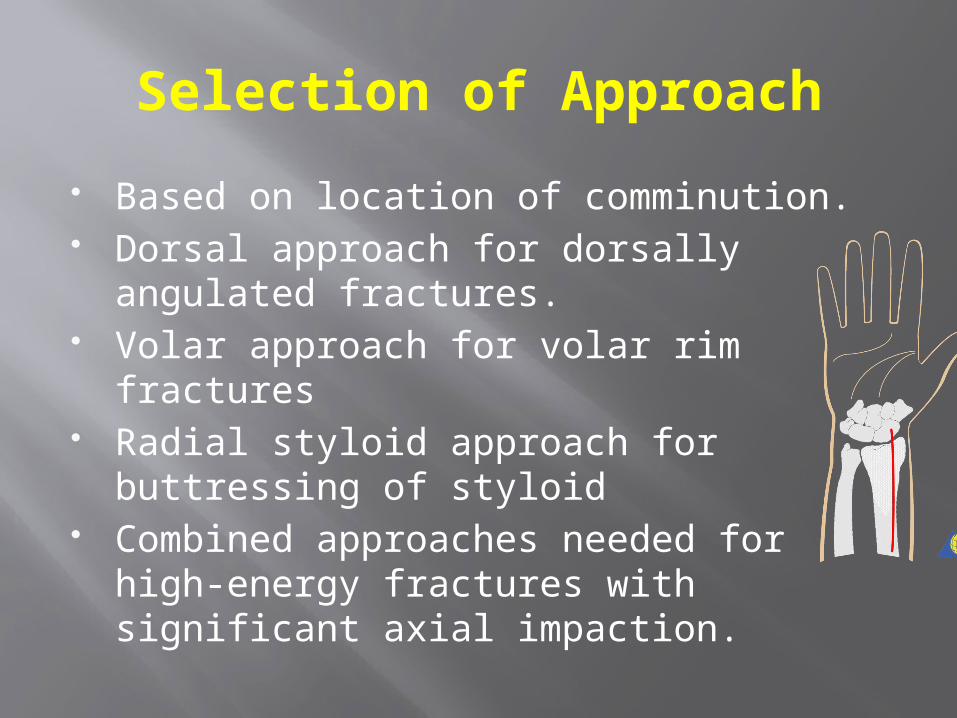
Selection of Approach
Based on location of comminution. Dorsal approach for dorsally angulated
fractures. Volar approach for volar rim fractures Radial styloid approach for buttressing of
styloid Combined approaches needed for high-
energy fractures with significant axial impaction.

Classical Henry approach(chung)
Extended carpal tunnel approach
VOLAR
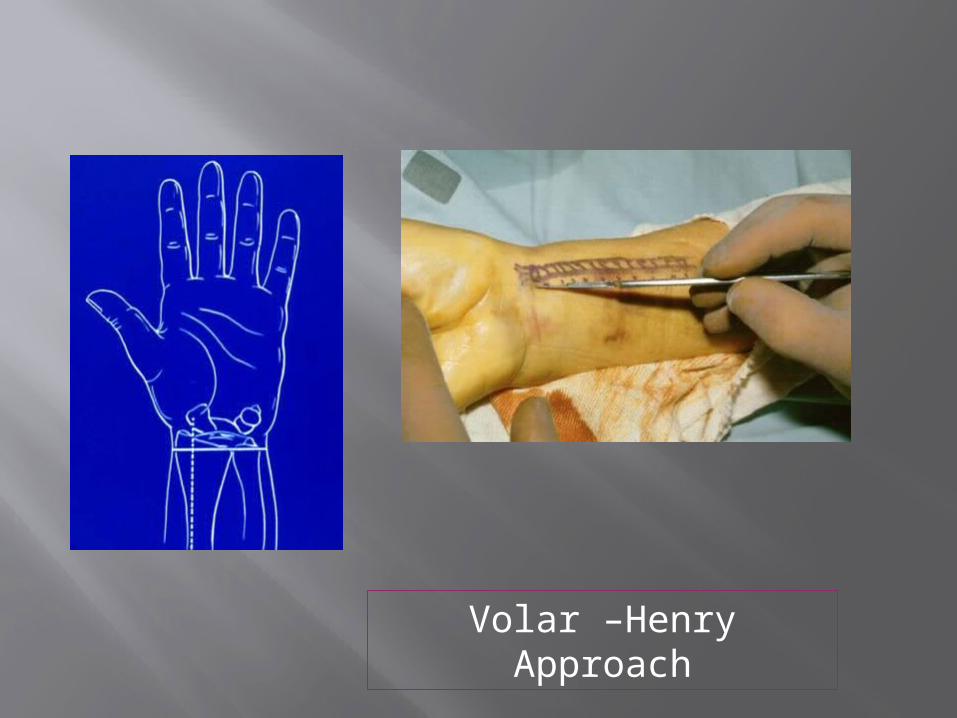
Volar –Henry Approach
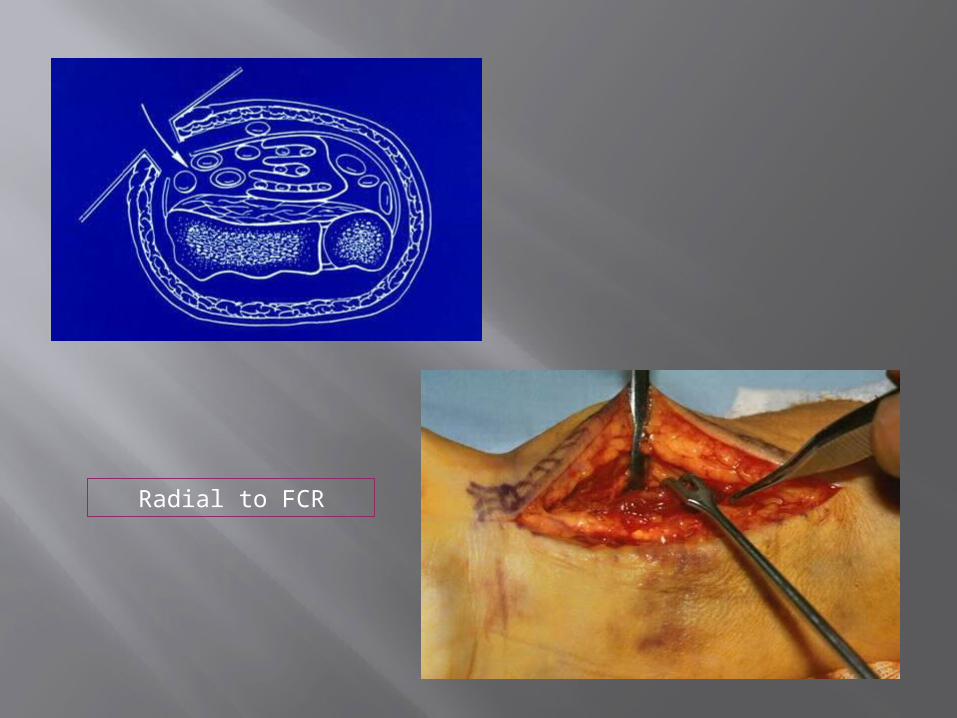
Radial to FCR

Skin incision
Incision carried to flexor carpi radialis sheath
Flexor pollicis longus muscle belly is partially detached from radius to expose pronator quadratus
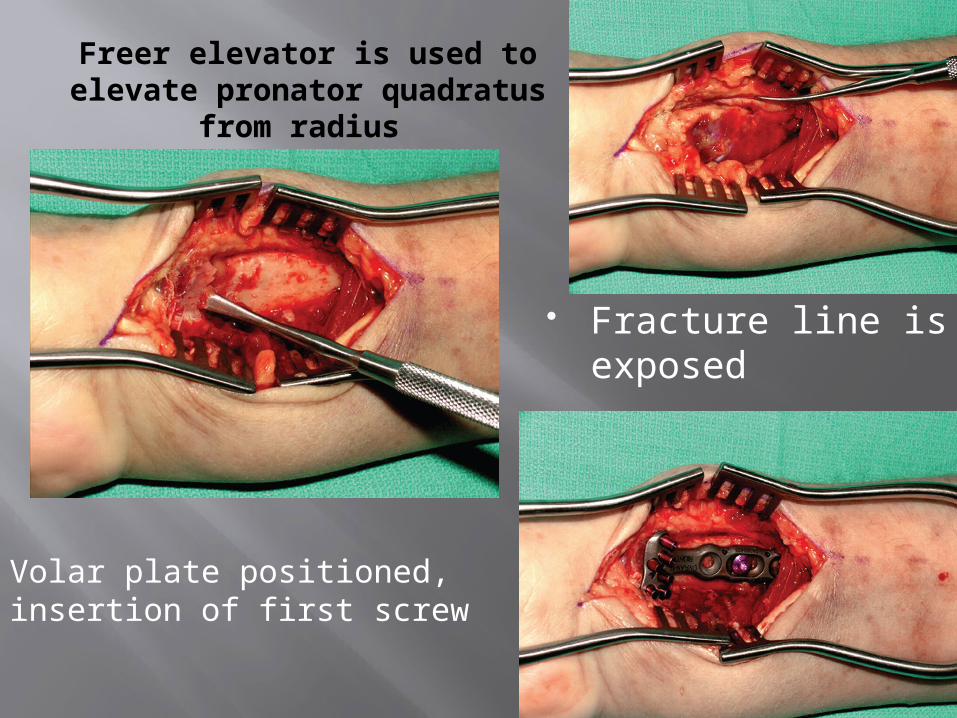
Freer elevator is used to elevate pronator quadratus
from radius
Fracture line is exposed
Volar plate positioned, insertion of first screw
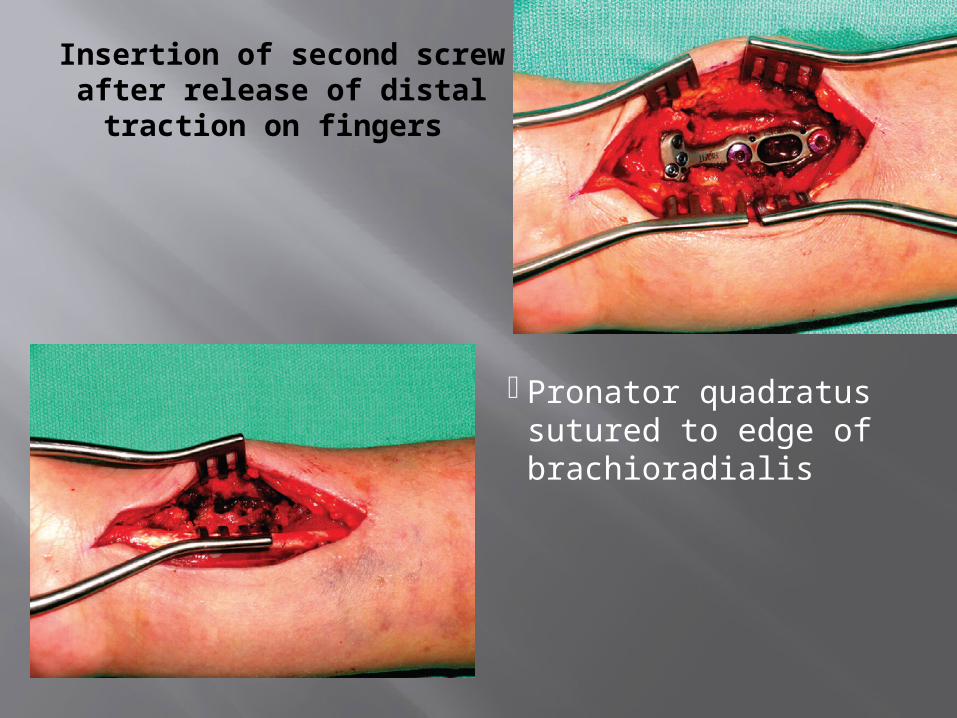
Insertion of second screw after release of distal traction on fingers
Pronator quadratus sutured to edge of brachioradialis
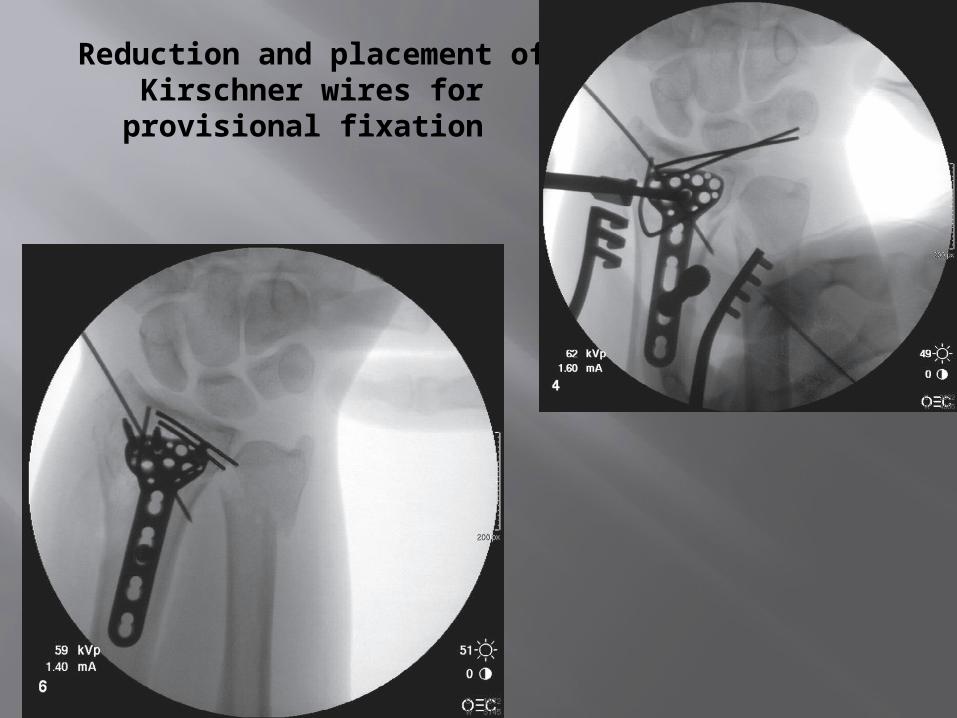
Reduction and placement of Kirschner wires for provisional fixation

Courtesy J. Orbay, MD
POSTOPERATIVE CARE
At 1 week, the sutures are removed and active wrist motion is begun when there is confidence in fracture stability
A removable Orthoplast splint is worn for 6 weeks.

-
DORSAL APPROACH
3rd DC –EPL(extensile)1-2nd DC
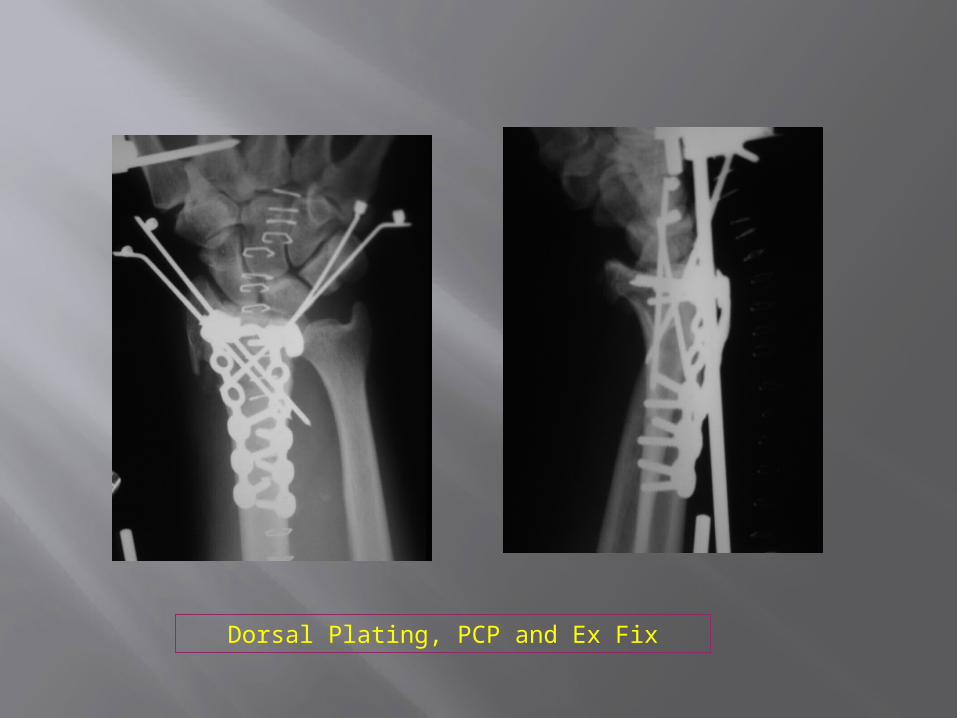
Dorsal Plating, PCP and Ex Fix
Generally not prefere because of high rate of complication like
- tendon dysfunction and rupture - tenosynovitis of extensor tendons indicated for- dorsal die-punch fractures or
fractures with displaced dorsal lunate facet fragments

DISTRACTION PLATE FIXATION
POSTOPERATIVE CARE
Finger and other joint upper extremity exercises are begun immediately
If a splint was applied, it is removed at 3 weeks
When union is achieved, the distraction plate is removed and range-of-motion exercises are begun
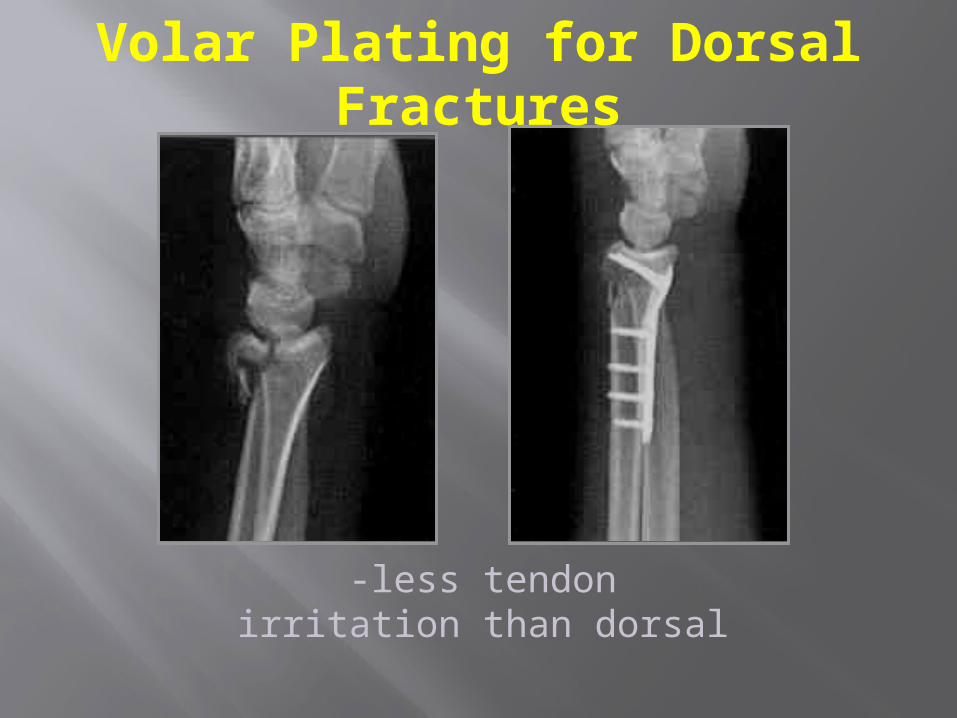
-less tendon irritation than dorsal
Volar Plating for Dorsal Fractures

Fixed angle locked screws ,,variable angle

Fragment Specific System

Five potential fracture fragments
radial column, dorsal cortical
wall, dorsal ulnar split, volar rim, and the central
intraarticular fragment
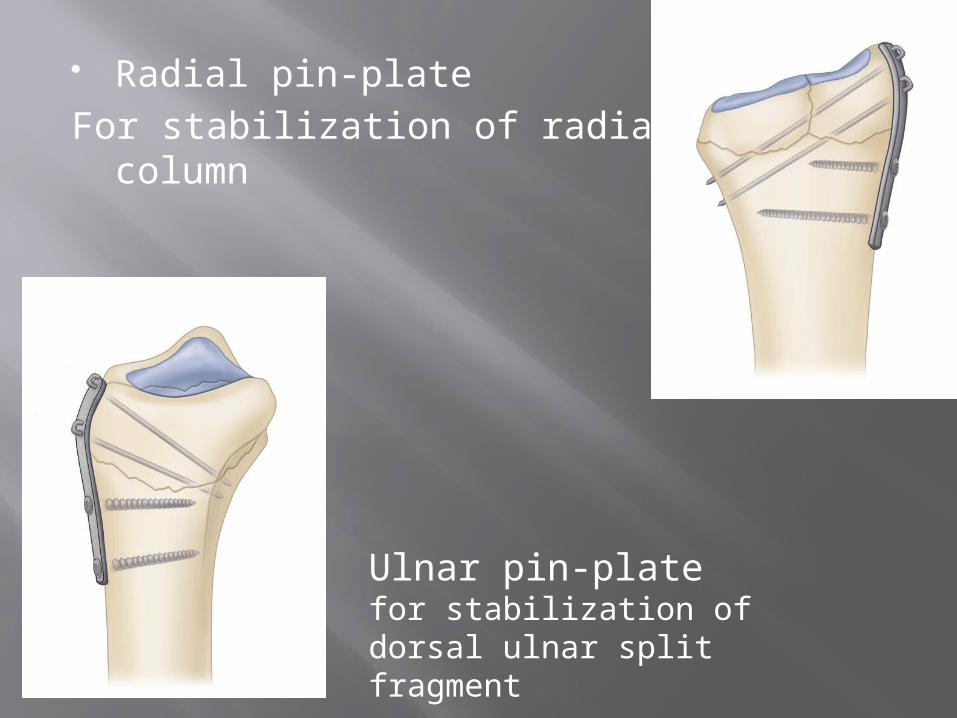
Radial pin-plate For stabilization of radial column
Ulnar pin-plate for stabilization of dorsal ulnar split fragment

Dorsal cortical wall fragment stabilized by small fragment clamp
simultaneously stabilization of dorsal wall fragment and intraarticular component
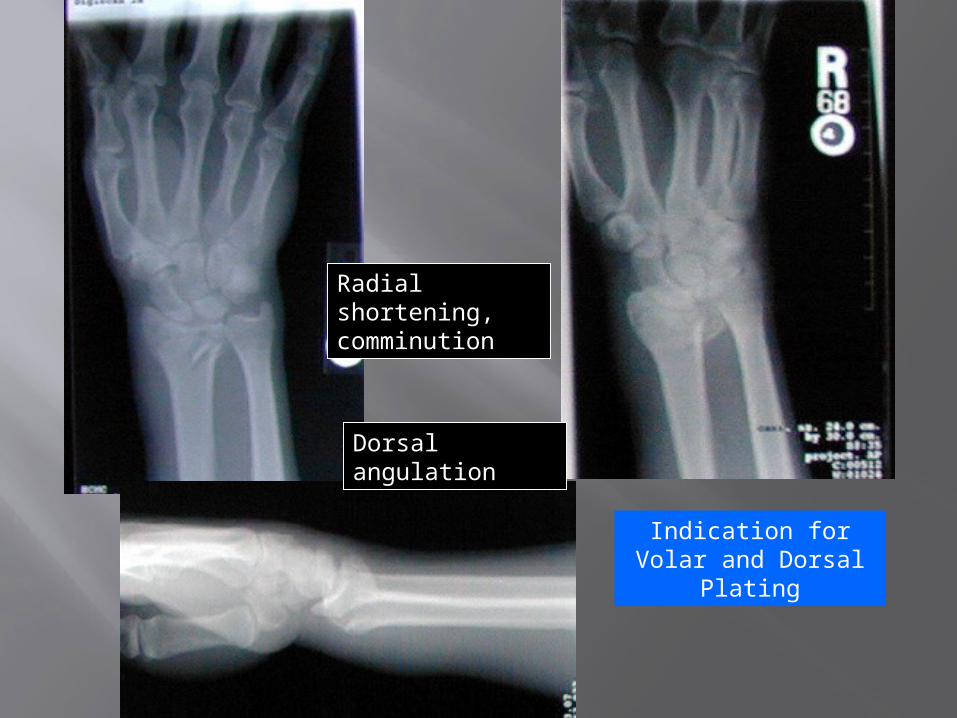
Radial shortening, comminution
Dorsal angulation
Indication for Volar and Dorsal Plating

Volar approach, application buttress plate

Dorsal approach, application of 2 “L” buttress plates
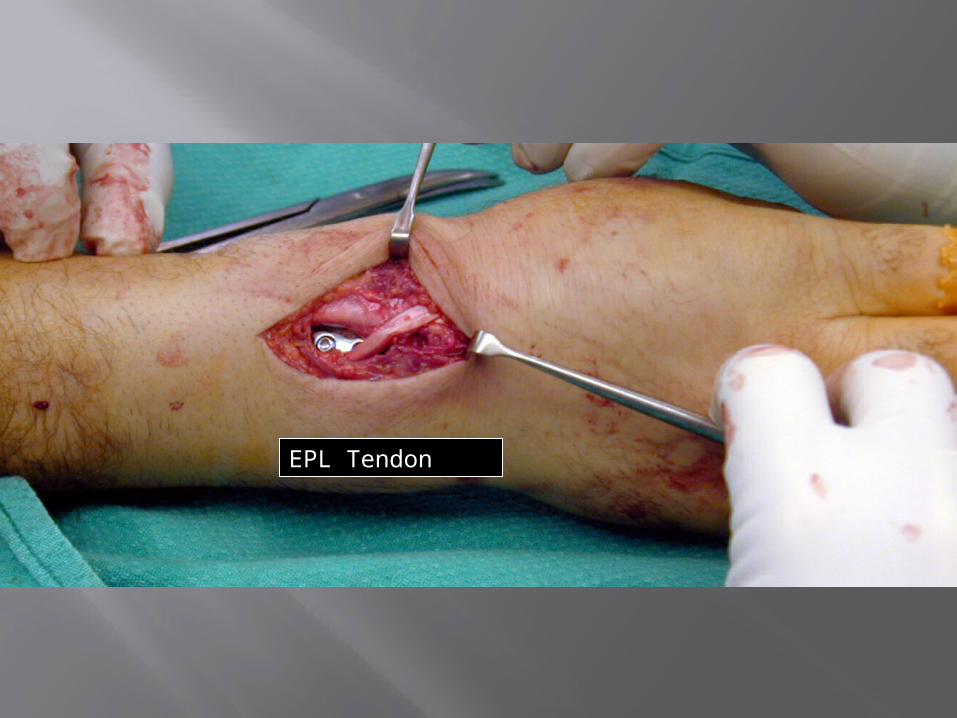
EPL Tendon

Extensor retinaculum repaired beneath EPL to prevent erosion against plate- EPL left transposed

Advanced TechniquesArthroscopic-Assisted
reduce articular incongruities also diagnose associated soft tissue
lesions minimally invasive
Indicated for 1-complex articular fracture without
metaphyseal comminution 2-# with evidence of substantial
interosseous ligament or TFCC injury without a large ulnar styloid fragment.
Timing-between 5 to 15 days post injury to prevent extravasation of irrigation fluid into the surrounding soft tissue
Complications After Fracture of Distal Radius
Arthritis/arthrosis Loss of motion Hardware complications Nerve compression/neuritis Osteomyelitis Dupuytren contracture Persistent pain/pain syndromes (CRPS) Tendon (rupture, lag, trigger, tenosynovitis) Delayed union/nonunion/malunion Radioulnar (synostosis, disturbance)
Conclusions
ORIF better in high-energy fractures associated with depression of articular surface
ORIF gives better anatomic restoration, although not necessarily higher patient satisfaction.
Conclusions
External fixators still have a role in the treatment of distal radius fractures
Spanning ex fix does not completely correct fracture deformity by itself
Should usually combined with percutaneous pins (augmented fixation)
Conclusions new plating techniques allow for
accurate and rigid fixation of fragments
Plating allows early wrist ROM
Volar, smaller and more anatomic plates are better tolerated
combination treatment is often needed

THANK YOU
Relationship of Anatomy to Function
Colles; “The wrist will regain perfect freedom in all of its motions and be completely exempt from pain” (1814)
Generally true for low demand individuals Direct relation between residual deformity and
disability Quality of reduction more important than
method of immobilisation
Related Documents
![Mir Distal Radius 2018 · for Select Slides/Images Evolution of Distal Radius Fracture Treatment [Chung Hand Clinics 2012] Casting -Cotton-LoderPosition Pins & Plaster External Fixation.](https://static.cupdf.com/doc/110x72/5f38d7993ae00a6eee18c252/mir-distal-radius-2018-for-select-slidesimages-evolution-of-distal-radius-fracture.jpg)










