DigestiveTrac DIGESTIVE DISEASES • SPRING 2014, ISSUE 10 INSIDE THIS ISSUE: Colorectal Cancer Awareness Atypical Presentations of Colorectal Cancer Advanced Surgical and Radiation Therapy Techniques: More Options for Best Possible Outcomes Weight Loss and Exercise Reduce Risk and Improve Prognosis of CRC Chemoprevention Takes Aim at Development and Recurrence of CRC Get your FREE mobile Digestive Trac at Avera.org/TRAC-register! AWARENESS MONTH COLON CANCER

Digestive Trac • Spring 2014, Issue 10
Mar 07, 2016
INSIDE THIS ISSUE: Colorectal Cancer Awareness Atypical Presentations of Colorectal Cancer Advanced Surgical and Radiation Therapy Techniques: More Options for Best Possible Outcomes Weight Loss and Exercise Reduce Risk and Improve Prognosis of CRC Chemoprevention Takes Aim at Development and Recurrence of CRC
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DigestiveTracDIGESTIVE DISEASES • SPRING 2014, ISSUE 10
INSIDE THIS ISSUE:
Colorectal Cancer Awareness
Atypical Presentations of Colorectal Cancer
Advanced Surgical and Radiation Therapy Techniques: More Options for Best Possible Outcomes
Weight Loss and Exercise Reduce Risk and Improve Prognosis of CRC
Chemoprevention Takes Aim at Development and Recurrence of CRC
Get your FREE mobile Digestive Trac at Avera.org/TRAC-register!
AWARENESS M
ONTH
COLON CANCER
Colorectal Surgery:Scott L. Baker, MD, FACS, FASCRS
Gastroenterology andHepatology:Steven Condron, MD, MHES, FACPCristina Hill Jensen, MDChristopher Hurley, MDDany Shamoun, MD
General Surgery:Scott L. Baker, MD, FACS, FASCRSMichael Bauer, MD, FACSWade E. Dosch, MD, FACSDavid Flanagan, MDThomas E. Fullerton, MDMichael Person, MD, FACSDavid A. Strand, MD, FACSBradley C. Thaemert, MD, FACSDonald J. Wingert, MD, FACS
Genetics: Kayla York, CGC, MS
GI Navigation: Liz Harden, CNP
Hepatology:Hesham Elgouhari, MD, FACPMumtaz Niazi, MD, FACP
Medical Oncology:David Elson, MD, FACPMark R. Huber, MDMichael McHale, MD, FACPHeidi McKean, MDBenjamin Solomon, MDAddison R. Tolentino, MD
Pathology: Steven P. Olson, MD Bruce R. Prouse, MDRaed A. Sulaiman, MD
Radiation Oncology: Barbara Schlager, MDKathleen L. Schneekloth, MDJames Simon, MD
Radiology:Sabina Choudhry, MDBrad A. Paulson, MD
Research (Cancer clinical trials)
Transplant Surgery:R. Christopher Auvenshine, DOJeffery Steers, MD, FACS
Urogynecology: Matthew A. Barker, MD, FACOG
Multidisciplinary Team Includes the Following Areas of Specialty:
Scott L. Baker, MD, FACS, FASCRS Colorectal Surgery Surgical Institute of South Dakota
Surgical Director of Avera Digestive Disease Institute
Dear Colleagues,
The month of March, which is National Colorectal Cancer Awareness Month, presents an annual opportunity for the specialists of the Avera Digestive Disease Institute to address the prevention and treatment of this common malignancy. Each year, an estimated 143,000 Americans are diagnosed with the disease. With more than 50,000 deaths annually, colorectal cancer is the second-highest cause of cancer-related deaths.
In this issue, we provide the basics of colorectal cancer, including screening guidelines. Please remember that screening colonoscopy is recommended every 10 years for all people age 50 and over. People who follow screening guidelines have a 90 percent reduced risk of developing colorectal cancer.
Through regular recommended colonoscopy screenings, it is our primary goal to prevent colorectal cancer from ever happening, which is entirely possible by finding and removing precancerous adenomatous polyps before they have the opportunity to develop into cancer.
Also in this issue, we address topics that shed new light on the prevention, diagnosis and treatment of colorectal cancer, including atypical presentations of the disease, leading-edge surgical and radiation therapy techniques, and the latest approaches in medical oncology.
We at Avera Digestive Disease remain dedicated to providing the highest quality care through our multidisciplinary team, which offers a full range of treatment options, patient navigation and support services.
As always, it is our privilege to work closely with primary care physicians for our patients’ best interest and continuity of care. Please feel free to contact us at 605-322-7797 with questions or for more information.
Sincerely,
1
Steven Condron, MD, MHES, FACPGastroenterology and HepatologyAvera Medical Group Gastroenterology
Medical Director of Avera Digestive Disease Institute
Learn more about successfully dealing with a colorectal cancer diagnosis. BeASurvivorAveraColon.com
Be A Survivor
Colorectal Cancer Awareness
2
Why screen?• Studies show that people who are screened have a
90 percent reduced risk of developing colorectal cancer.
• Colorectal cancer is the second leading cause of cancer-related deaths, with more than 50,000 deaths per year nationwide.
• Colorectal cancer most often develops from adenomatous polyps which develop into cancer over a period of 10 to 15 years. Finding and removing precancerous polyps virtually eliminates the potential for cancer.
Recommended screeningColonoscopy is the “gold standard” in colorectal screening, as it is the most sensitive and effective test for detecting colon polyps. This valuable screening tool:
• Examines the entire colon
• Gives the best visibility of abnormalities
• Provides the opportunity to remove precancerous polyps during the same procedure
Screening guidelines• Beginning at age 50 (45 for African Americans)
• Every 10 years (every two to five years if polyps are detected)
• Earlier screening may be recommended for people with a family history of colorectal cancer, such as a diagnosis of colon cancer in a member at age 40
Colonoscopy procedure• Patients take a preparation to cleanse the bowel the
night before and morning of the test.
• Patients abstain from solid foods the day before the test, and have nothing to eat or drink four hours before the test.
• Sedative medications make the procedure itself very comfortable. Many patients wake up after the procedure is over and don’t even realize it has already taken place.
• During the colonoscopy, a gastroenterologist gently moves a long, lighted tube with a tiny camera through the entire colon, and watches a magnified view of the inside of the colon on a monitor.
• If polyps are found, the endoscopist removes the polyps immediately with a tool attached to the colonoscope.
• Time at the clinic or outpatient hospital setting typically is three hours or less, and the actual procedure time is approximately 30 minutes.
March is National Colorectal Cancer Awareness Month, a key time for primary care physicians to remind their patients age 50 and over to schedule a screening colonoscopy.
Schedule a ColonoscopyReferring physicians and patients
who meet screening guidelines
can schedule a colonoscopy
by calling 605-322-7797
3
Atypical Presentations of Colorectal Cancer
The typical discovery of colorectal cancer happens during a routine screening colonoscopy, before
symptoms occur. Yet referring physicians should be aware of both the typical and atypical presentations that point to this disease, which is very treatable in its earliest stages, yet also remains the cause of more than 50,000 deaths each year nationwide.
In terms of symptoms of colorectal cancer, most physicians as well as patients first think of bleeding from the rectum or blood in the stool. This is only one of several symptomatic presentations.
Any bleeding – whether it is bright red blood with bowel movements, or dark/black stools – can indicate colorectal cancer. Even if a patient has a history of hemorrhoids, bleeding from the rectum should not be passed off or ignored.
A negative fecal occult blood test does not rule out colorectal cancer. Large tumors bleed, but polyps and small developing tumors often do not. Colonoscopy is considered the optimal screening test, because it can detect precancerous polyps and early tumors much earlier than the fecal occult blood test.
Another common signal is anemia, characterized by feeling run down, fatigued and short of breath with reduced exercise capacity. Iron deficiency often results from loss of blood in the digestive tract. In women, this symptom is often explained by heavy menstrual bleeding. Otherwise, the top cause of anemia is bleeding in the digestive tract due to colorectal cancer or peptic ulcer disease.
A change in bowel habits reported by a patient should be taken seriously, whether it be a change from commonly being constipated to loose stools, or from having well-formed stools and regular bowel movements to extreme constipation. Anytime the patient feels that things are different, colorectal cancer should be considered as a possible explanation.
The colon runs throughout the entire abdominal cavity, so unexplained pain anywhere in the abdomen could be related to a tumor and should be investigated.
When symptoms occur, regardless of age, colorectal cancer should be considered as a possibility. While the typical presentation is after age 50, patients as young as their mid-20s have developed colorectal cancer.
Raed A. Sulaiman, MD, board-certified Pathologist
Investigate colorectal cancer as a possible cause of:
• Unexplained anemia
• Bleeding from the rectum or blood in the stools
• A change in bowel habits
• S. bovis bacteremia in the blood
• Elevated alkaline phosphatase
Do not rule out colorectal cancer based upon:
• Age under 50
• Lack of family history
• Negative fecal occult blood test
• Negative distant screening colonoscopy
4
Patients often mistakenly believe that if they have no family history of colorectal cancer, they are not at risk. Yet 80 to 85 percent of colorectal cancer cases are sporadic, meaning that they have no link to heredity. Approximately 15 percent of colorectal cancers can be attributed to instability in microsatellites, which are sequences of DNA.
Avera pathologists screen all colorectal tumors for microsatellite instability (MSI) to check for genetic mutation. Genetic testing can help physicians know how to better treat certain types of cancer, and gives further insight on prognosis. For patients and their families, genetic testing can indicate the need for more frequent or earlier cancer screening.
The most common hereditary syndromes include Lynch syndrome, which increases the risk of colon and other cancers, and familial adenomatous polyposis (FAP), which results in the formation of precancerous polyps at an early age.
“Identifying patients and families with
conditions like Lynch syndrome allows appropriate
medical management and preventative services
to be in place to reduce hereditary cancer risk
and improve outcomes.” – Dr. Raed Sulaiman,
board-certified Pathologist
Screening colonoscopy is recommended every 10 years because that is the average length of time it takes for tissue to change from normal mucosa to malignancy. In the vast majority of cases, non-malignant polyps appear first, and can be removed during screening colonoscopy.
Yet in cases like Lynch syndrome and FAP, colorectal cancer can develop faster. In such cases, it is an unwelcome surprise to patients when they develop symptoms of cancer five years after an “all clear” screening colonoscopy. While it doesn’t happen often, it’s possible, and cancer should not be “crossed off the list” just because a recent screening colonoscopy was negative.
Abnormal lab results can be cause to investigate the possibility of colorectal cancer. For example, presence of S. bovis bacteremia in the blood has an approximate 40 percent association with CRC.
Elevated alkaline phosphatase in the blood in routine screenings for patients on cholesterol-lowering medications can be indicative of metastatic colon cancer in the liver.
Another unusual presentation of colorectal cancer is that of a malignant fistula, in which cancer erodes into another structure or organ. An abnormal communication between organs, a malignant fistula may connect the bowel and the vagina or the bowel and bladder. In these cases, patients might notice that they pass air when urinating or through the vagina.
“Colorectal cancer is the second leading cause of cancer-related deaths. When there’s any kind of vague symptom or indication that could be caused by colorectal cancer, colon cancer testing and specifically colonoscopy should be considered in the diagnostic workup,” Dr. Condron said.
Screening colonoscopy is our preferred way of finding colorectal cancer, because it means that symptoms have not developed yet, and we likely have discovered it in its earliest, most treatable stages.
– Dr. Steven Condron, board-certified Gastroenterologist
“ “
Finding the Atypical Colorectal Cancer Case
5
Advanced Surgical and Radiation Therapy Techniques:
More Options for Best Possible Outcomes
Across the spectrum of medical specialties, surgical techniques are becoming more minimally invasive, and colorectal surgery is no exception. Robotic technology allows surgeons to consider minimally invasive techniques in a wider range of cases, with patient benefits including less pain, less blood loss, fewer complications and a shorter recovery.
Dr. Scott Baker, board-certified Surgeon and fellowship-trained Colorectal Surgeon says that while 80 percent of colorectal procedures nationwide are performed using a traditional open technique, the vast majority of his cases involve minimally invasive techniques, including laparoscopy, single-incisionlaparoscopy and robotics.
Compared with open colon resection, laparoscopy is associated with less need for postoperative pain medication, faster return of bowel function, earlier resumption of eating and drinking, earlier return of intestinal motility,
shorter hospital stay, and smaller scars – and virtually no visible scar in the case of single-incision procedures.
While easier on the patient, laparoscopic colectomy is a complex procedure for the surgeon to perform. It requires working in multiple quadrants of the abdomen at the same time. Unless there are multiple adhesions or a very large tumor, most colon resection cases can be performed laparoscopically by an experienced surgeon. Single-incision laparoscopic surgery (SILS) involves one small incision in the navel, with all instruments being placed through this central port.
Robotic technology available at Avera McKennan Hospital & University Health Center is comprised of two da Vinci® surgical systems: the da Vinci Si™ and the da Vinci S HD.
Not every colorectal case is a candidate for robotics. Yet for some procedures, including low pelvic cases such as sigmoid resection or total
mesorectal excision (TME), robotics has key advantages. In the lower pelvis, space is confined. Three-D, high-definition vision of the operative field with up to 10 times magnification helps surgeons identify nerves and other structures, leading to fewer complications such as urinary retention or sexual dysfunction. Miniaturized surgical instruments can be controlled in human wrist-like motions with 360-degree range of motion leading to precise removal of cancerous tissue.
Controlling the robot via a computerized console, surgeons have ambidextrous capability and can manipulate instruments with multiple degrees of freedom.
M ultidisciplinary specialists with Avera Digestive Disease Institute consider all options in the treatment of colorectal cancer, including the latest surgical and radiation therapy techniques.
6
The patient has four small incisions, leading to minimal scarring, less blood loss and faster recovery than the traditional open incision, which is several inches in length. Surgical principles are similar to those of laparoscopy, including removal of margins on either side of tumor-affected area, removal of the lymph nodes that drain from the tumor area, and anastomosis, or connection of the remaining ends of the structure.
Magnification of vision and precision of instruments are helpful in ensuring removal of all involved lymph nodes and the fascia that envelops them, which along with circumferential margin is key to preventing recurrence.
Robotic technology is constantly improving. Newly available are staplers that aid surgeons in dividing the bowel, and technology that allows surgeons to benefit from fluorescence imaging in identifying structures, such as the supplying blood vessels.
Improving technology may one day resolve some of the limitations of robotics, for example, lack of sensory feedback by the surgeon in determining how tissues feel, and a limitation to one field as opposed to the entire abdomen.
“Robotics allow us to approach certain cases
minimally invasively, so that patients can benefit
from a lesser risk of complications, less post-surgical
pain and a faster recovery. Key advantages of
robotics are visualization and range of motion
in a limited space, as well as the precision of
instruments. Robotic technology is the future of
minimally invasive surgery, and
patients will continue to benefit as
this technology advances.” – Dr. Scott Baker, board-certified
Colorectal Surgeon
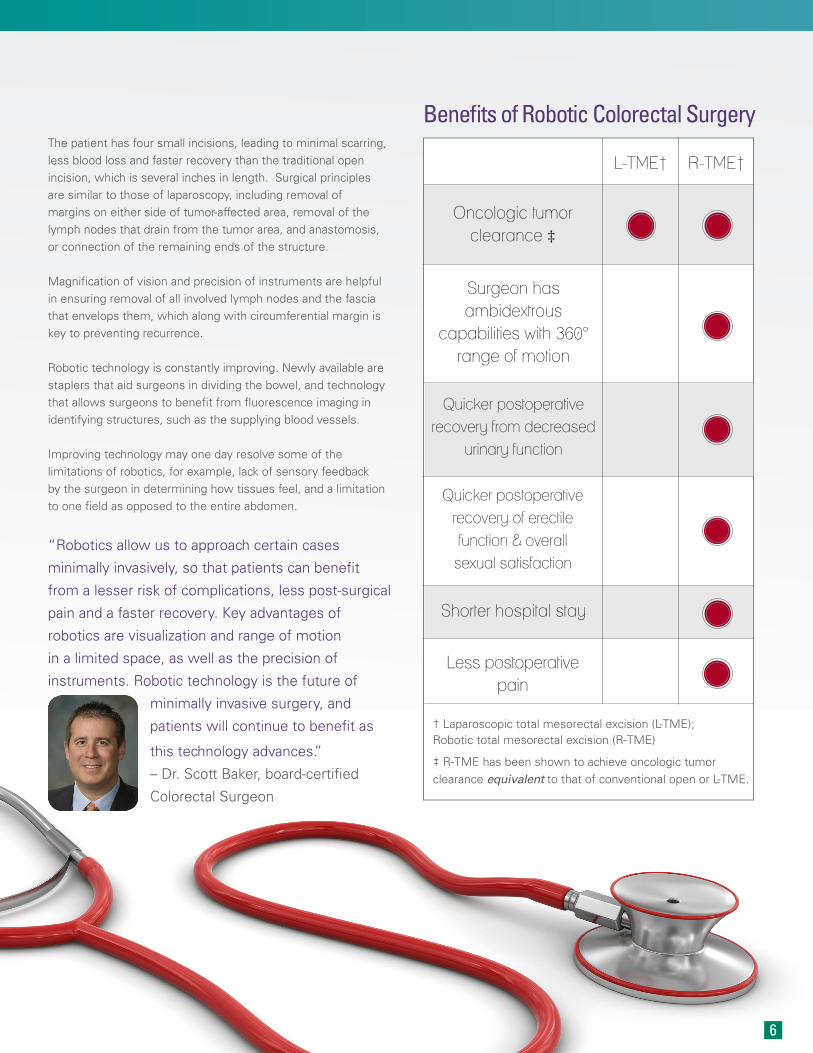
Oncologic tumor clearance ‡
Surgeon has ambidextrous
capabilities with 360° range of motion
Quicker postoperative recovery from decreased
urinary function
Quicker postoperative recovery of erectile function & overall
sexual satisfaction
Shorter hospital stay
Less postoperative pain
† Laparoscopic total mesorectal excision (L-TME); Robotic total mesorectal excision (R-TME)
‡ R-TME has been shown to achieve oncologic tumor clearance equivalent to that of conventional open or L-TME.
L-TME† R-TME†
Benefits of Robotic Colorectal Surgery

7
Advanced Surgical and Radiation Therapy Techniques
• Robotics
• Single-incision laparoscopy
• Intraoperative electron radiation therapy (IOeRT)
• Intraoperative HDR brachytherapy
• Stereotactic radiosurgery/stereotactic body radiation therapy (SRS/SBRT)
At Avera McKennan, IOeRT is used primarily in the treatment of breast cancer through participation in an international research trial, and it has also been used incidentally for gynecologic cancers, soft tissue sarcoma and pancreatic cancer in addition to colorectal cancer.
Avera McKennan also has the technology to offer intraoperative high-dose rate brachytherapy for similar indications.
At the time of surgery, straw-like hollow catheters are inserted close to the tumor bed. After surgery, in the Avera Cancer Institute’s dedicated brachytherapy suite, a radioactive source is delivered through the channels directly to the tumor site, delivering a very precise dose to high-risk areas while sparing other structures. Brachytherapy may be helpful when working around a curve in the body, as opposed to IOeRT which is delivered in a straight path.
For patients who are not candidates for surgery, the Avera Cancer Institute offers stereotactic radiosurgery/stereotactic body radiation therapy (SRS/SBRT) using the Elekta Versa HD. This linear accelerator delivers a high dose of radiation with extremely high precision.
Advanced technology at Avera McKennan also allows select patients to benefit from a radiation boost at the time of surgery, directly to the surgical site, without impact to skin, tissues or organs.
Intraoperative electron radiation therapy (IOeRT) has a proven track record in the treatment of colorectal cancer, and this technology has been available at Avera McKennan since 2011.
Dr. Kathleen Schneekloth, board-certified Radiation Oncologist, said that when physicians believe that a selected patient could be a candidate for IOeRT, his or her case is scheduled in the surgical suite that is equipped with the Mobetron unit. Yet the surgeon and radiation oncologist do not make a final decision to use IOeRT until surgery is underway, and the tumor bed is visible.
IOeRT is indicated for locally advanced disease that is varied in resectability. Indicators include gross residual disease at the resection bed, gross positive margins or positive microscopic margins, based on pathology review.
IOeRT is intended to give a supplemental dose, in addition to any pre- or post-surgical radiation and chemotherapy prescribed for the patient, in order to prevent recurrence in a high-risk area. In addition to sparing nearby organs, it spares nerves, and the ureters. “The data shows the treatment is well tolerated, and in appropriately selected patients, provides a higher tumor control rate with normal morbidity to other organs,” Dr. Schneekloth said.
A typical dose, through collimators ranging in size from 4 mm to 9 mm, is 10 to 20 gray. Actual treatment is a minute to a minute and a half, when all care staff step out of the room and the patient is monitored remotely by the anesthesiologist. After the treatment, the patient is not radioactive, and there is no residual radioactivity in the room.
Known as “radiosurgery,” the treatment is non-invasive, through the skin. Radiation beams converge on a small spot, making this technology applicable for small fields, including metastases to the liver, brain or spine.
“Surgical and radiation techniques are considered
on a case-by-case basis through a multidisciplinary
approach as part of an appropriate treatment plan,
designed for the best possible outcome.”
– Dr. Kathleen Schneekloth, board-certified Radiation
Oncologist
8
Weight Loss and Exercise Reduce Risk and Improve
Prognosis of CRC
Research has shown that excess weight is associated with both an increased risk for colorectal cancer, and a poorer prognosis, according to a presentation at the 2013 Gastrointestinal Cancers Symposium by Peter T. Campbell, PhD, cancer epidemiologist and Director of the Tumor Repository at the American Cancer Society.
Research has found that every five-unit increase in body mass index (BMI) is associated with an 18 percent rise in risk for CRC. An individual with an obese BMI of greater or equal to 30 has about a 40 percent higher risk for CRC compared with a person in the lower range of normal (18.5-25). The association is stronger in men than in women, and stronger for cancers that occur in the colon than the rectum.
In addition, follow-up research on more than 2,200 CRC survivors found that patients who reported having an obese BMI several years before their cancer diagnosis had a 35 percent increased risk for death from CRC and a 68 percent increased risk for death from cardiovascular disease.
Studies have also shown that adults with higher levels of physical activity – in intensity, duration or frequency – can reduce their risk for developing colon cancer by 30 to 40 percent relative to those who are sedentary.
The Avera Digestive Disease Institute encourages obese patients to pursue weight loss based on the many comorbidities of obesity, including a higher cancer risk, metabolic syndrome, cardiac disease, joint and back pain, depression, sleep apnea and more. In the specialty of gastroenterology, conditions including nonalcoholic steatohepatitis (NASH), gastroesophageal reflux disease, and general GI complaints such as bloating often result from obesity, or are worsened by obesity.
In addition to medical expertise, Avera offers the counsel of dietary, fitness and behavioral health experts for patients desiring to lose weight. Avera’s Integrative Medicine program offers the Ideal Living program, as well as complementary therapies such as acupuncture and mind-body movement. Through a recent Avera study, a cohort of 24 breast cancer survivors with an average body weight of 220 pounds lost an average 44 pounds during a five-month period on the Ideal Living program.
If lasting weight loss cannot be achieved through diet and lifestyle changes, Avera offers an experienced bariatric surgery program, which is accredited as a Level 1 bariatric center by the American College of Surgeons. This well-rounded program ensures that patients are first committed to the eating and lifestyle changes required by bariatric surgery. After surgery, the needed support is provided to help patients experience success.
In the realm of medical oncology, today’s approach is to treat higher-stage cancers and/or those at high risk for recurrence with chemotherapy. Tomorrow’s approach may be to use drug therapy to prevent cancer from occurring in the first place, as well as recurrences of cancer.
It’s called “chemoprevention,” and the Avera Cancer Institute has taken part in a number of clinical studies to determine the efficacy of possible preventive agents, including statins and NSAIDs. “The pathways for preventing cancer are many and varied, because each cancer has its own pathway of development,” said Dr. Addison Tolentino, board-certified Medical Oncologist.
One open study is looking at the prevention of polyp formation and colon cancer through a combination of eflornithine and Sulindac. Sulindac is an NSAID, known toinhibit the COX-2 pathway. Eflornithine in cream form is actually used to retard the growth of facial hair. It inhibits an enzyme that is involved in polyamine synthesis. Excess polyamines have a role in the development of colorectal cancer. Eflornithine slows the body’s production of polyamines, while Sulindac helps cells eliminate excess polyamines.
CHEMOPREVENTION
TAKES AIM AT D E V E L O P M E N T A N D R E C U R R E N C E O F C R C
Similar to NSAIDs, statins may stop the growth of tumor cells by blocking some of the enzymes
needed for cell growth. A study that is now closed at Avera tested the drug rosuvastatin versus a placebo,
in patients who had polyps and/or stage 0-3 colon cancer.
An open trial is testing the use of celecoxib (Celebrex), an NSAID, in conjunction with FOLFOX, a standard chemotherapy regimen that is given 12 times over a period of six months. It is also testing the difference between giving FOLFOX six times over a period of three months, versus the regular 12-dose regimen. One of the drugs in FOLFOX, oxaliplatin, is known to cause neuropathy as a side effect. “Damage to nerve endings can be mild, or debilitating in some patients. The idea of this study is to see if we can decrease the amount of FOLFOX to half, and at the same time, see if Celebrex will in some way compensate for the three months not given,” Dr. Tolentino said.
9

10
GENOMICS IN CRC: TODAY AND THE FUTUREThrough applied genomics, Avera is unlocking the science behind why some medications are more effective for some patients than others.
Specialists of the Avera Digestive Disease Institute and Avera Cancer Institute offer two key genetic tests to patients with colorectal cancer. One is the oncotype DX colon cancer assay, which studies the activity of 12 genes for patients who have newly diagnosed colon cancer at stage 2 and 3. This test predicts a higher risk for the recurrence or metastasis of cancer, and is especially helpful for patients diagnosed at stage 2. While most
stage 2 patients will not have a recurrence, genotyping is used to identify which cancers are more aggressive, and in turn, whether or not chemotherapy would be beneficial.
For patients with stage 4 advanced cancer, patients can be tested for the KRAS gene mutation, helping medical oncologists in their selection of chemotherapy agents.
A genomics medicine team, led by Dr. Brian Leyland-Jones, recently joined the Avera Cancer Institute and works closely with the Avera Institute for Human Genetics. This team works to bring personalized cancer therapies to patients, based on their individual genetic profile, specifically in cases in which cancer is resistant to common treatment protocols, or cancer has recurred. While this team specializes in breast cancer, they will accept patients with other types of cancer
who can benefit from personalized therapy.
“These developments are not on the horizon – they’re happening now. Yet this is just the beginning in terms of genetics and cancer care. We anticipate that more possibilities will continue to appear in the future for application in the clinical setting,” said Dr. Addison Tolentino, board-certified Medical Oncologist.
“The field of medical research is testing old drugs in new ways, and coming up with new drugs with the ultimate goal of greater effectiveness and fewer side effects. With chemoprevention, the hope is that certain agents will prevent the formation of precancerous polyps, tumors, or the recurrence of colorectal cancer.”
Brian Leyland-Jones, PhD, BS, MB
Addison R. Tolentino, MD, board-certified Hematologist, Oncologist
Hours: 8 a.m. - 5 p.m. • 605-322-7797
To learn more, visit our website atAveraDigestiveDisease.org
1325 S. Cliff Ave.Sioux Falls, SD 57105
ADDI-41849-REVFE0614
Digestive Trac is now available online!
• Works on all mobile devices
• Access to additional content
• Social-media friendly
• Delivered instantly to your mobile device via email
We’ve Gone Digital
Take 30 seconds and register NOW at Avera.org/TRAC-register.
DigestiveTracDIGESTIVE DISEASES • WINTER 2013
Issue 9
INSIDE THIS ISSUE:NEUROENDOCRINE TUMORS
Medical Management of Neuroendocrine Tumors
Surgical Removal of NETs is Ideal for Curative Treatment
Medical Oncology Offers Approaches for Advanced or Aggressive NETs
Related Documents











