Differential Sensitivity to Alcohol Reinforcement in Groups of Men at Risk for Distinct Alcoholism Subtypes Patricia J. Conrod, Robert 0. Pihl, and Jasmin Vassileva The present study examinesthe relationship of familial and person- ality risk factors for alcoholism to individualdifferencesin sensitivity to the positivelyand negatively reinforcing propertiesof alcohol. Six- teen sons of male alcoholics with multigenerational family histories of alcoholism (MFH) and 11 men who self-report heightened sensi- tivity to anxiety (HAS) were compared with 13 age-matched family history negative, low anxiety sensitive men (FH-US) on sober and alcohol-intoxicated response patterns. We were interested in the effects of alcohol on specific psychophysiologicalindices of “stim- ulus reactivity,” anxiety, and incentive reward. Alcohol significantly dampened heart rate reactivity to aversive stimulation for the MFH and HAS men equally, yet did not for the FH-LAS group. HAS men evidenced idiosyncrasies with respect to alcohol-inducedchanges in electrodermal reactivity to avenive stimulation (an index of anxi- ety/fear-dampening), and MFH men demonstratedelevated alcohol- intoxicatedresting heart rates (an index of psychostimulation) rela- tive to the FH-LAS men. The results are interpreted as reflecting a sensitivity to the “stimulus reactivity-dampening” effects of alcohol in both high-risk groups, yet population-specific sensitivities to the fear-dampening and psychostimulant properties of alcohol in the HAS and MFH groups, respectively. HE MAJORITY of people drink moderately and with- T out ill effect; in fact, the objective benefits of moderate alcohol consumption on human health have been ob- served.’ However, it is estimated that 5 to 10% of adults develop serious alcohol-related problems and account for the majority of alcohol-related costs to society.’ Youth, male gender, personal and family history of alcoholism, substance abuse and other psychiatric disorders, and cer- tain occupations are all prealcoholic characteristics that have been associated with elevated risk for the eventual development of alcoh~lism.~-~ The numerous identified risk factors and correlates of alcoholism (e.g., personality or comorbid psychopathology) are generally considered to reflect the heterogeneous nature of the disorder and have stimulated research interests in alcoholism typology. Ac- From the Department of Psychology (P.J.C., R.O.P.), McCill University, Montreal, Quebec, Canada; and Finch University of Health Science, Chicago Medical School (J. K), Chicago, Illinois. Received for publication June 9, 1997; accepted December 15, 1997 This research was supported by grants from the Medical Research Council of Canada. Reprint requests: Patricia J. Conrod, Ph.D. Candidate, Department of Psychology, McGill University, 1205 Dr. Penfield Avenue, w811, Montreal, Quebec, Canada H3A 1B1. Copyright 0 1998 by The Research Society on Alcoholism. Alcohol Clin Erp Res, Vol22, No 3, 1998: pp 585-597 cordingly, researchers have found it particularly useful to study individuals classified based on the presence of onc or several of these vulnerability characteristics. The study of such factors in individuals not currently or previously af- fected by the disorder presents several advantages when attempting to delineate the etiological components of the disorder independent from the widespread and potentially chronic effects of alcohol on the central nervous system. Two general vulnerability characteristics will constitute the focus of the present investigation, they are: familial history of alcoholism and anxiety sensitivity-a personality risk factor for panic-related anxiety disorders. Such character- istics are not mutually exclusive in their contribution to risk for alcoholism, neither are they collectively exhaustive. The heritable component of alcoholism has long been recognized through controlled family, twin, and adoption studies.6 Despite their varied methodological limitations, such studies consistently find that male relatives of alcohol- ics are at elevated risk for the disorder.’ Sons of male alcoholics with multigenerational family histories of alco- holism (MFH) have been evaluated to be at a 4- to 9-fold increased risk for the development of An important distinguishing characteristic of such individuals is that they initiate use of alcohol earlier, drink more heavily, and demonstrate more drinking-related problems when they reach young adulthood.’”-” These distinctive features highlight the importance of studying this sample at a relatively young age to identify factors that directly influ- ence early involvement with alcohol and maintenance of heavier alcohol use in adolescence and early adulthood. Anxiety sensitivity (AS)“ is a personality trait that refers to the tendency to be fearful of anxiety symptoms. This trait is conceptually and empirically different from trait anxi- ety” and has been shown to be highly predictive of the eventual development of panic disorder.” Presently, the evidence implicating AS as a risk factor for alcoholism is indirect and based largely on correlational data. Neverthe- less, data suggest that AS plays an important role in ex- plaining the relationship between alcoholism and anxiety (see review by Stewart et al.’”). Although self-report studies inconsistently show a relationship between AS and drinking rates among young adult women2” and panic patients,” they invariably demonstrate a strong correlation between AS levels and self-reported frequency of drinking to cope 585

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Differential Sensitivity to Alcohol Reinforcement in Groups of Men at Risk for Distinct Alcoholism
Subtypes Patricia J. Conrod, Robert 0. Pihl, and Jasmin Vassileva
The present study examines the relationship of familial and person- ality risk factors for alcoholism to individual differences in sensitivity to the positively and negatively reinforcing properties of alcohol. Six- teen sons of male alcoholics with multigenerational family histories of alcoholism (MFH) and 11 men who self-report heightened sensi- tivity to anxiety (HAS) were compared with 13 age-matched family history negative, low anxiety sensitive men (FH-US) on sober and alcohol-intoxicated response patterns. We were interested in the effects of alcohol on specific psychophysiological indices of “stim- ulus reactivity,” anxiety, and incentive reward. Alcohol significantly dampened heart rate reactivity to aversive stimulation for the MFH and HAS men equally, yet did not for the FH-LAS group. HAS men evidenced idiosyncrasies with respect to alcohol-induced changes in electrodermal reactivity to avenive stimulation (an index of anxi- ety/fear-dampening), and MFH men demonstrated elevated alcohol- intoxicated resting heart rates (an index of psychostimulation) rela- tive to the FH-LAS men. The results are interpreted as reflecting a sensitivity to the “stimulus reactivity-dampening” effects of alcohol in both high-risk groups, yet population-specific sensitivities to the fear-dampening and psychostimulant properties of alcohol in the HAS and MFH groups, respectively.
HE MAJORITY of people drink moderately and with- T out ill effect; in fact, the objective benefits of moderate alcohol consumption on human health have been ob- served.’ However, it is estimated that 5 to 10% of adults develop serious alcohol-related problems and account for the majority of alcohol-related costs to society.’ Youth, male gender, personal and family history of alcoholism, substance abuse and other psychiatric disorders, and cer- tain occupations are all prealcoholic characteristics that have been associated with elevated risk for the eventual development of a lcoh~l i sm.~-~ The numerous identified risk factors and correlates of alcoholism (e.g., personality or comorbid psychopathology) are generally considered to reflect the heterogeneous nature of the disorder and have stimulated research interests in alcoholism typology. Ac-
From the Department of Psychology (P.J.C., R.O.P.), McCill University, Montreal, Quebec, Canada; and Finch University of Health Science, Chicago Medical School (J. K), Chicago, Illinois.
Received for publication June 9, 1997; accepted December 15, 1997 This research was supported by grants from the Medical Research Council
of Canada. Reprint requests: Patricia J. Conrod, Ph.D. Candidate, Department of
Psychology, McGill University, 1205 Dr. Penfield Avenue, w811, Montreal, Quebec, Canada H3A 1B1.
Copyright 0 1998 by The Research Society on Alcoholism.
Alcohol Clin Erp Res, Vol22, No 3, 1998: pp 585-597
cordingly, researchers have found i t particularly useful to study individuals classified based on the presence of onc or several of these vulnerability characteristics. The study of such factors in individuals not currently or previously af- fected by the disorder presents several advantages when attempting to delineate the etiological components of the disorder independent from the widespread and potentially chronic effects of alcohol on the central nervous system. Two general vulnerability characteristics will constitute the focus of the present investigation, they are: familial history of alcoholism and anxiety sensitivity-a personality risk factor for panic-related anxiety disorders. Such character- istics are not mutually exclusive in their contribution to risk for alcoholism, neither are they collectively exhaustive.
The heritable component of alcoholism has long been recognized through controlled family, twin, and adoption studies.6 Despite their varied methodological limitations, such studies consistently find that male relatives of alcohol- ics are at elevated risk for the disorder.’ Sons of male alcoholics with multigenerational family histories of alco- holism (MFH) have been evaluated to be at a 4- to 9-fold increased risk for the development of An important distinguishing characteristic of such individuals is that they initiate use of alcohol earlier, drink more heavily, and demonstrate more drinking-related problems when they reach young adulthood.’”-” These distinctive features highlight the importance of studying this sample at a relatively young age to identify factors that directly influ- ence early involvement with alcohol and maintenance of heavier alcohol use in adolescence and early adulthood.
Anxiety sensitivity (AS)“ is a personality trait that refers to the tendency to be fearful of anxiety symptoms. This trait is conceptually and empirically different from trait anxi- ety” and has been shown t o be highly predictive of the eventual development of panic disorder.” Presently, the evidence implicating AS as a risk factor for alcoholism is indirect and based largely on correlational data. Neverthe- less, data suggest that AS plays an important role in ex- plaining the relationship between alcoholism and anxiety (see review by Stewart et al.’”). Although self-report studies inconsistently show a relationship between AS and drinking rates among young adult women2” and panic patients,” they invariably demonstrate a strong correlation between AS levels and self-reported frequency of drinking to cope
585

586 CONROD ET AL.
with negative affect (A. Novak et al. Unpublished data, 1997)23-24 and frequency of drinking in negatively reinforc- ing drinking situations (S.B. Samoluk et al., Unpublished data, 1997). The latter two facets of drinking have been associated with problematic alcohol use.26 AS is also re- lated to elevated and problematic benzodiazepine use (drugs that share some depressant properties in common with alcohol) in anxiety disorders patients, alcoholics, and high AS college s t ~ d e n t s . ~ ~ - * ~ AS has also been shown to be a strong correlate of alcohol and anxiolytic drug use/misuse over and above other personality variables previously shown to be implicated in anxiety-related drinking (e.g., trait a n x i ~ t y ) . ~ ” ~ ~ More recently, Stewart et al.I9 and Mc- N a l l ~ ~ ~ have suggested that the combination of high levels of trait anxiety (increased frequency of anxiety experiences) and AS (fear of anxiety) may predispose an individual to use and misuse drugs with anxiety-reducing properties.
Evidence for the hypothesis that MFH and highly anxiety sensitive (HAS) men may be at risk for distinctive alcohol- ism subtypes is derived primarily from a growing body of literature indicating that the classification of alcoholics according to age of onset of the disorder, personality fac- tors, comorbid psychopathology, and familial history of psychopathology reliably identifies at least two subtypes of a l c ~ h o l i s m . ~ ~ - ~ ~ The first subtype (type I or type A) is characterized by later age of onset of alcoholism, “neurot- ic” comorbid and familial psychopathology, and less severe clinical course, whereas the second (type I1 or type B) is characterized by earlier age of onset, more chronic and severe disorder, comorbid antisocial personality disorder, and a family history laden with alcoholism and sociopathy. HAS and MFH individuals, and their family members, appear to be at risk for lifetime comorbid psychiatric dis- orders that respectively correspond to the comorbid psy- chopathological profiles of these proposed alcoholism sub- types. 15.34,39,40 _ -
The study of subtypes of individuals at elevated risk for alcoholism is primarily inspired by the possibility that the latent class structure of prealcoholic characteristics (and correlates of drinking behavior) reflect the motivational basis (or etiology) of different alcoholic syndromes (P.J. Conrad et al. Unpublished data, 1997).38,42 Such ap- proaches have applied theory of three interacting brain motivational systems to the investigation of the eti- ology of alcoholism and its subtypes. According to Gray,43 individual differences in the regulation of emotional behav- ior can be explained by variation in the functional integrity of three theorized emotion systems, two of which are the focus of the present investigation: the behavioral activation system (BAS), which is responsible for the activation of behavior (both approach and active avoidance) in response to primary positive reinforcement and the behavioral inhi- bition system (BIS), which responds to cues for punishment with heightened sympathetic arousal and the inhibition of behavior. F ~ w l e s ~ ~ has added that human variability within these two systems is indicated by specific psychophysiolog-
ical dimensions in response to emotion-specific stimuli and that an additional “nonspecific arousal” system is concep- tually necessary to more accurately explain human motiva- tion. Several researchers have adopted this theoretical framework, or variations thereof, in order to identify mo- tivational determinants of alcohol use and m i ~ u s e . ~ ’ . ~ ’ - ~ ~ That alcohol intoxication produces at least two very distinct reinforcement effects is a basic premise of these approach- es.49 The resultant “motivational” hypothesis is that indi- vidual differences in the function of these proposed brain emotion systems translate to variations in broad dimen- sions of temperament and personality that are differentially sensitive to the reinforcing effects of substances of a b ~ ~ e . ~ ~ , ~ ~ , ~ ~ The heterogeneous nature of alcoholism can thus be understood from this theoretical Accordingly, it is proposed that individuals differentially use alcohol as a way to regulate specific motivational sen- sitivities and develop different alcoholic syndromes that can be defined primarily based on the type of alcohol reinforce- ment to which the individual is most receptive.’9336,41*42,47
This approach has been applied to the study of the relationship between anxiety and alcohol consumption (see review by Stewart et al.’9350 and Pihl and Peterson47). Ac- cording to Gra?’ and F o ~ l e s : ~ , ~ ~ sensitivity within the BIS will result in heightened autonomic reactivity and cognitive acuteness toward threat cues (i.e., heightened anxiety). The emotional and behavioral sequelea to activation in this system are dampened only when behavioral plans are exe- cuted, as determined by past experience, instinct, and higher cognitive p r o c e s ~ e s . ~ ~ ~ ~ ~ Alcohol and other antianx- iety agents are also able to deactivate this inhibitory system to reduce anxiety associated with its overactivity.” As such, alcohol intoxication is believed to be negatively reinforcing for individuals who demonstrate a sensitivity within this proposed system or who lack the cognitive and behavioral strategies required to temper emotion associated with this system. F ~ w l e s ~ ~ has further specified that variability within this system can be physiologically indexed by electrodermal reactivity.
There is a large body of evidence suggesting that high levels of AS reflect at a characterological level vulnerability to heightened BIS responding. HAS individuals are be- lieved to catastrophize or misinterpret the significance of threat cues and experience heightened anxiety as a result.s3 Such individuals have also been shown to demonstrate higher sober subjective-emotional arousal in anticipation of aversive s t i m ~ l a t i o n , ~ ~ greater sober electrodermal re- sponses to the aversive s t im~la t ion?~ and attentional biases favoring the processing of physically threatening informa- tion.55*s6 Moreover, individuals high in AS appear more sensitive to the cognitive and affective components of the stress response (e.g., fear and catastrophization), rather than to the somatic components.’9757 Alcohol at moderate- to-high doses dampens both electrodermal and cognitive hyperresponsiveness to threat in highly AS ~ o m e n . ~ ~ . ~ ~ Furthermore, HAS women demonstrate more reactivity-

DIFFERENTIAL SENSITIVITY TO ALCOHOL REINFORCEMENT ih-
dampening on cognitive and affective measures of anxiety, but not necessarily on somatic measures of a n ~ i e t y . ~ “ ~ ~ The evidence favors a negative reinforcement model to explain vulnerability to alcoholism in this at risk population (see Stewart et al.l9>j0 for review). Although recent investiga- tions with anxiety disorder patients lend support to the notion that sensitivity to the negatively reinforcing effects of alcohol may be etiologically relevant for both genders,’* HAS expressed by men has been shown to be qualitatively different than that expressed by women.5996o The validity of generalizing findings from alcohol-challenge studies on HAS female subjects to HAS males is thus presently un- founded. Therefore, one goal of the present investigation is to test the hypothesis that HAS men will demonstrate differential sensitivity to the negatively reinforcing, “fear/ anxiety-dampening’’ effects of alcohol when compared with their age-matched low anxiety-sensitive (LAS) male coun- terparts, as has already been demonstrated in HAS women.
Young adult sons of male MFH alcoholics also appear to demonstrate exaggerated autonomic reactivity-dampening when alcohol intoxicated relative to groups of men at low familial risk for alcoholism.61-63 The similarities between MFH men and HAS women with respect to sensitivity to the stress-response dampening effects of alcohol hint at the possibility that the genetic predisposition to alcoholism can be similarly explained by a negative reinforcement, “stress- response dampening” model. However, the mechanisms that may underlie the response pattern characteristic of MFH men are not well delineated, and there is indirect evidence that different and additional motivational pro- cesses may be involved in the vulnerability to alcoholism of the familial type.3747
Some researchers have suggested that cardiac responsiv- ity manifested in offspring of alcoholics is indicative of sensitivity within the BAS and that drinking behavior is motivated by the stress-dampening effects of alcohol on BAS-related arousal, rather than BIS-related arousal.4s Peterson and Pih164 have proposed a model for the inher- ited predisposition to alcoholism in which findings of heightened event-related potential, electrodermal orient- ing responses, and cardiovascular reactivity in MFH men are interpreted as reflecting a particular cognitive profile implicating specific deficits in prefrontal cortical “executive functions.” In addition to other behavioral and psychophys- iological sequelea, it was proposed that such deficits trans- late more specifically to deficits in labeling the motivational significance of novel or ambiguous information. Autonomic hyperarousal in response to nonaversive and aversive stim- ulation manifested by MFH men has been proposed to represent a pattern of responding indicative of heightened nonspecific preparedness of the individual to “act” in re- sponse to any stimulus that cannot be immediately ab- stractly classified. Therefore, this cognitive profile and its behavioral and psychophysiological consequences may re- sult in a sensitivity to the negatively reinforcing, nonspecific ‘‘stimulus reactivity”-dampening effects of alcohol, rather
than a sensitivity to the anxiety-dampening effects of alco- hol.” The hypotheses offered by Hill et and Pihl and Peterson47 to explain MFH proneness to early-onset heavy drinking involves a different negative reinforcement model than that used to describe HAS drinking.’” While the model explaining MFH drinking implicates sensitivity to the effects of alcohol on nonspecific stimulus reactivity- dampening,” the model explaining HAS drinking more distinctly implicates sensitivity fearianxiety-dampening by alcohol.”
Several researchers have attempted to specify the distinct components of the stress response. For example, Fowles‘ three-arousal theory44 suggests that response to a motiva- tionally relevant stimulus results in nonspecific autonomic arousal to prepare the organism for action. Activation of the BIS only results following the evaluation of potential danger. Accordingly, the BAS and BIS have similar inputs into a general arousal mechanism that is important for preparing an organism to respond to its environment by temporarily increasing autonomic arousal. Related work in this area indicates that this nonspecific arousal system is responsible for the “alarm reaction” of the stress response and for the increased motor and autonomic activity associ- ated with response to stress.66 Noradrenergic mechanisms have been linked to the biochemical functioning of this system.66967 Alternatively, the immobility and freezing (be- havioral inhibition) aspect of the stress response may be mediated more specifically by GABAergic mechanisms that are also more closely linked to the affective component (subjective evaluations) of aversive stimulation.66 Alcohol has been shown to directly interact with both neurotrans- mitter systems:’ and it is possible that alcohol produces two different negatively reinforcing effects by differentially interfering with the normal (or abnormal) functioning of these brain systems. Within this theoretical framework, it can be suggested that individuals who lack the higher level reasoning and problem-solving abilities (as appears to be the case in MFH individuals)”9 will appreciate the nonspe- cific stimulus reactivity-dampening effects of alcohol. By contrast, those who possess attentional biases that intensify the fear and anxiety associated with threatening stimuli (as appears be the case in HAS individuals)s’3s5~’6 will demon- strate exaggerated affective and cognitive reactivity to threatening information and will appreciate the fearianx- ety-dampening effects of alcohol. 19, j7
Recent investigation from our research group suggests that additional sensitivity to alcohol reinforcement may be implicated in the genetic predisposition to alcoholi~m.~” Specifically, we have suggested that subtle abnormalities within a brain emotion system that regulates behavioral responses to the incentive rewarding properties of stimuli (equivalent to Fowles’ BAS)44 results in the sensitivity to the positively reinforcing, psychostimulant effects of alco- ho1.70 -72 Young MFH men have repeatedly been shown to demonstrate idiosyncratic resting cardiac responses to al- coho1 Fowles et aL7‘ have argued that

CONROD ET AL. 588
heart rate increase is an index of response to incentive properties of stimuli and corresponds to activity within the BAS. Further support for the notion that this specific car- diac response observed in MFH men represents sensitivity within the BAS comes from findings indicating that the cardiac response is dependent on dose75 and rate of alcohol i nge~ t ion ,~~ is specific to the ascending limb of the blood alcohol curve,71 co-occurs with alcohol-induced increases in positive and correlates strongly with self-report and laboratory measures of alcohol consumpt i~n ,~~ character- istics logically associated with activity in the BAS. This growing body of empirical findings suggests that sensitivity to psychomotor reward from alcohol, indexed by cardiac reactivity to alcohol intoxication, is an important etiological mechanism implicated in the inherited predisposition to alcoholism.
Therefore, it appears that MFH men are particularly sensitive to at least two separate reinforcing properties of alcohol: the negatively reinforcing, “stimulus reactivity”- dampening effects and the positively reinforcing, psycho- stimulant effects. The evidence also suggests that HAS individuals are sensitive to a third form of alcohol rein- forcement: namely, feadanxiety-dampening. Whether the nature of sensitivity to alcohol reinforcement is distinct across the two at-risk populations has not been tested directly. Furthermore, in the context of Fowles’ work on psychophysiological indices of general arousal, feadanxiety (BIS activity) and incentive reward (BAS activity),44 it is possible to test the hypothesis that HAS and MFH individ- uals present distinct alcohol-reinforcement sensitivities that differentially motivate elevated alcohol consumption be- havior and may explain why such at-risk populations appear predisposed to distinct alcoholic syndromes.
Specifically, it is hypothesized that HAS and MFH men will demonstrate differential psychophysiological and sub- jective sensitivity to alcohol intoxication. To test this hy- pothesis, subjects participated in a stress-challenge para- digm while sober and moderately alcohol-intoxicated. BAS- sensitive versus BIS-sensitive physiological measures, as specified in Fowles’ three-arousal as well as sub- jective measures of anxiety, were used to index the various reinforcing effects of In contrast to the specific experimental paradigms that have been developed for the measurement of BIS- and BAS-specific sensitivity (e.g., ~ondi t ioning~~ or passive avoidance learning76 procedures), we chose to test these two at-risk populations on an un- avoidable shock paradigm, because it lends itself to the measurement of both nonspecific and BIS-specific physio- logical arousal. Furthermore, based on extensive previous testing of MFH men and HAS women on this paradigm, we have shown that population-specific sensitivities to alcohol effects are d o ~ e - d e p e n d e n t ~ ~ . ~ ~ and time along the blood alcohol curve-dependent (ascending limb versus descend- ing limb).71 Nonspecific arousal (or “stimulus” reactivity) was indexed by cardiovascular reactivity to an unavoidable aversive s t r e s ~ o r , ~ l - ~ ~ whereas BIS-specific reactivity (anx-
iety) was indexed by subjective and electrodermal response patterns.44 Sensitivity to alcohol-induced stimulus reactivi- ty-dampening versus fearianxiety-dampening was deter- mined based on the degree to which alcohol reduced each facet of the stress response (i.e., cardiovascular versus elec- trodermal reactivity-dampening, respectively). Sensitivity to positive reinforcement from alcohol was indexed by resting cardiac reactivity coupled with alcohol intoxica- tion.44,7n,7~
The present investigation is novel in two respects. First, to our knowledge, HAS men have never been compared with LAS counterparts on a stress and alcohol challenge paradigm. Second, MFH and HAS individuals, two popu- lations presupposed to be at elevated risk for the develop- ment of different alcoholism syndromes, have never been contrasted on their presumed sensitivity to the reinforcing properties of alcohol intoxication.
METHODS
Participants
Forty nonalcoholic, Caucasian males between the ages of 18 and 25 were recruited from advertisements featured in English arts and enter- tainment newspapers. Respondents were initially contacted by telephone and screened for family and personal history of alcoholism and other relevant psychiatric and medical disorders. Subjects were included in the study if they met the following inclusion criteria: (1) nonalcoholic status within the previous 12 months [score below 10 on the Brief Michigan Alcoholism Screening Test (brief MAST)]77; (2) did not report a medical condition for which alcohol consumption was contraindicated; (3) re- ported absence of a family history of bipolar or psychotic disorder; (4) did not report a history of maternal alcoholism (to rule out the potential effects of fetal alcohol syndrome); ( 5 ) did not report parental history of hypertension (to rule out the potential effects on sober cardiovascular response patterns);63 and (6) met criteria for inclusion into one of three experimental groups [i.e., MFH, HAS, or family history negative-LAS (FH-LAS)]. MFH status was assigned if a subject reported, at minimum, an alcoholic father, an alcoholic paternal grandfather, and one other male alcoholic member from the previous two generations of the paternal lineage. Alcoholic status for family members was also determined using the brief MAST, as well as DSM-111-R criteria for alcohol abuse.78 AS was assessed using the Anxiety Sensitivity Index (ASI)I6 and cut-off scores for HAS and LAS were determined based on normative data on male subjects matched for age.16 Eleven subjects who scored above 27 on the AS1 and who did not report a MFH of alcoholism were assigned HAS status, and 13 subjects who scored below 10 on the AS1 and who reported no history of alcoholism or substance abuse within the previous two generations of the maternal and paternal lineage were assigned FH-LAS status. Seven- teen subjects were assigned MFH status (one of which also scored in the HAS range on the AS1 and was thus excluded). All subjects were asked to abstain from consuming alcohol 72 hours prior to their participation in the study. Upon completion of the experiment, each participant was payed as compensation for time spent in the laboratory.
Tests and Materials
Drinking Behavior. Two alcohol consumption measures were used to reflect drinking behavior patterns: self-report number of alcoholic bever- ages consumcd per week and self-report number of lifetime problem drinking symptoms. For the former measure, subjects participated in a semistructured interview detailing an average number of drinking occa- sions per week and the quantity of alcohol consumed on such occasions. For the latter measure, the brief MAST” was used as a method of

DIFFERENTIAL SENSITIVITY TO ALCOHOL REINFORCEMENT 5 30
assessing symptoms related to substance abuse and the number of prob- lems manifested in a person’s life due to their involvement with alcohol. Three questions were also asked to reflect onset of drinking behavior: “At what age do you remember having your first alcoholic beverage?,” “At what age do you remember first becoming intoxicated from alcohol?,” and “At what age did you first begin to drink on a regular basis?” Subjects were also administered the Drinking Motives Questionnaire (DMQ),’9 a 15- item scale that assesses the degree to which individuals report consuming alcohol for coping, enhancement, and social reasons.
Personality Questionnaires. Sensation seeking was assessed using Zuck- erman’s Sensations Seeking Scale (SSS),” AS using the ASI,I6 and trait anxiety using the State-Trait Anxiety Inventory-Trait form (STAI-T).*’
Subjective Responses to Shock. The Shock Anticipation Scale, devcl- oped by Finn et al.,73 consists of five items rated on a 10-point Likert scale concerning the degree of tension, anxiety, worry, fear, and anger experi- enced in anticipation of shock administration, with higher scores reflecting higher levels of subjective anticipatory emotional arousal. The Shock Rating Scale73 consists of two items that concern the degree of discomfort and degree of pain experienced associated with receipt of shock. Degree of subjective sensitivity to the shock was reflected by total scores on the scale (higher scores reflecting more discomfort and pain).
Physiological Measurements. Heart rate (HR) and skin conductance (SC) levels (SCLs) were recorded using a Contact Precision Instruments polygraph. Two Medi-Trace pellet electrodes placed bilaterally on the lower chest were used to detect HR. Two Beckman large biopotential SC electrodes were attached to the medial phalanges of the second and third fingers of the nondominant hand. Saline mixed with Gaxal-base cream was used as an intermediary for the recording of SC (as recommended by F ~ w l e s ~ ~ ) .
Experimental Manipulation [Countdown to Shock + Shock (CTSS)]. Electric shocks were administered using a Farral Instrument Mark I at an intensity of 1.85 mA for 0.5 sec using a concentric electrode attached to the inside of the elbow of the subject’s nondominant arm. A tone played on the computer channeled through Realistic Nova 10 stereo headphones that were connected to the internal speaker of the computer. It was presented to the subjects 12 sec prior to the delivery of the shock. Countdown stimuli were presented visually by computer. The CTSS pro- cedure has been previously reported by other researchers affiliated with the McGill University Alcohol Research Lab0ratory,6’,~~,~~ in the investi- gation of MFH subjects’ responses to aversive stimulation. The only modification to the original procedure was that countdown stimuli were presented visually on a computer screen, rather than as auditory stimuli. This stress challenge procedure is also similar to that used by Stewart and Pih1:4 with female HAS subjects with the exception that the latter study presented loud noise bursts as the aversive stimulus.
Alcohol Administration. Each participant was administered a dose of 1.0 mlkg of body weight of 95% USP alcohol mixed 5:l parts orange juice. The beverage was presented to the subject in three separate glasses, and subjects were instructed to consume each beverage within 5 min. Rate of alcohol consumption has been shown to influence the magnitude of cardiac responses to alcohol intoxication.” Therefore, an experimenter remained in the room to ensure that subjects consumed the beverages at a stable rate of one drink every 5 min. Blood alcohol concentrations (BACs) were determined using an Alco-Sensor 111 (Thomas Instruments, Montreal, Canada). Subjects were asked to provided a strong breath that remained at a consistent intensity for 6 sec. The Alco-Sensor 111 estimates BACs with an error of measurement of 20.003.
subjccts were weighed and then given the S S S , STAI-T, and AS1 to complete. Subjccts were then asked to remain seated and relaxed for I 0 min, during which time 5-min baseline mcaburcs for HR and SC were recorded.
A concentric shock elcctrodc was then attached to the inside of the subject’s forearm and headphones werc placed over his ears. The shock delivery procedure consisted of three successive electric shock trials. Trial onset, signaled to thc subject by a low-frequency tone, was heard through the earphones and was followed by a countdown from 10 to 1 (actual time lapse was 12 sec) presented visually on a computer screen. A second. higher frcquency tone signaled shock onset and trial termination. The intertrial interval for each shock trial was 20 sec.
The subject was then provided with thc 1.0 mlikg dose of 95% USP alcohol mixed with fivc parts orange juice and consumcd the dose in threc divided drinks over a 15-min period. To allow time for the alcohol to be digested, subjects relaxed for 10 min. Following this absorption period, a BAC mcasurement was taken (25 min post-onset of alcohol consumption) and a second 5-min baseline measure (-30 to 35 min post-onset of alcohol consumption) was recorded, and the CTSS procedure was repeated (35 t u 50 min post-onset of alcohol consumption). The subject was then discon- nected from the cardiovascular recording devices, fed, debricfcd regarding the experimental procedures, and allowcd to leave the laboratory only once BAC reduced to below 0.04%.
RESULTS
Risk Group Characteristics at Baseline Table 1 presents group means and standard deviations
for demographic, personality, and drinking-related vari- ables. Analyses of variance (ANOVAs) revealed that the groups were matched for age and years of education. Con- sistent with our original subject selection procedure, the HAS group scored significantly higher in anxiety sensitivity [ASI: F(2,38) = 72.5, p < 0.001], as well as trait anxiety [STAI-T: F(2,38) = 6.88, p < 0.011, compared with the FH-LAS and MFH groups. However, post-hoc analyses also indicated that the MFH group self-reported signifi- cantly higher AS levels, compared with the FH-LAS group ( p < 0.05). Nevertheless, the mean AS score for the MFH group was within the low-to-moderate range according to normative data on AS in young men.16 A significant effect for age of first alcoholic beverage was yielded [F(2,38) = 5.43, p < 0.011 and post-hoc analyses indicated that the MFH group reported first consuming alcohol at a signifi- cantly younger age, compared with the HAS and FH-LAS groups ( p < 0.05). A trend was revealed for the MFH group to self-report significantly higher quantityifrequency estimates for weekly alcohol consumption, compared with the HAS group only [F(2,38) = 2 . 1 4 , ~ < 0.11, Due to the fact that there was a low rate of endorsement on the brief MAST for the sample, brief MAST scores were converted to a categorical variable representing the presence or ab- sence of problem drinking symptoms (lifetime brief MAST scores > or = 0) . x2 analysis indicated a trend for the FH-LAS grOUD to Self-reDort a lower rate of Dresence of
Procedure
Upon their arrival, subjects were briefed as to the procedure of the study and were then presented with a consent form to sign. All subjects
“ I
were aware that they could withdraw from participation at any time in the experiment, but once intoxicated could not leave the laboratory until their BAC had reduced to below a 0.04% level. A short semistructured inter- view was conducted to collect demoarauhic and uersonal drinking infor-
drinking-related with the MFH and
ANOVA% the groups were compared On the DMQ. The HAS groups [,y2(2) = 5 . 8 8 , ~ < 0.11. Finally, using one-way
I * - mation. Before being attached to the physiological recording devices, HAS group was shown to score significantly higher on all
590 CONROD ET AL.
Table 1. Means 5 SD for Baseline Demographic, Personality, and Drinking-Related Characteristics of Three Groups of Men Presumed Differentially at Risk for Alcoholism
Baseline variables
Risk group
HAS (n = 11) FH-LAS (n = 13) MFH (n = 16)
Mean 2 SD Mean 2 SD Mean t SD Post-hoc (p < 0.05)
Demographics and personality Age Years of education AS1 scores STAI-T scores SSS scores
Alcohol-related behavior Age of first drink Age first intoxicated Age began drinking regularly No. of alcoholic beveragedweek % (no.) reporting problem drinking symptoms Social drinking motives Coping drinking motives (covaried for social motives) Enhancement drinking motives (covaried for social motives)
21 .O 2 2.6 15.2 2 2.1 6.1 2 2.6
35.8 2 4.7 25.8 f 5.2
12.8 2 1.9 15.1 2 1.3 16.0 t 1.5 10.1 2 8.4 15.4 (2)
10.8 2 2.3 7.6 t 2.0
11.7 2 3.1
21.6 t 2.5 14.9 2 1.4 32.3 2 7.1 46.3 2 6.0 28.2 t 5.4
13.6 2 3.0 14.1 2 2.9 16.2 2 2.1 7.5 f 6.0 54.5 (6)
14.3 2 2.3 10.1 2 3.0 13.6 t 3.4
22.5 t 2.7 14.2 t 2.5 11.8 t 6.2 40.3 f 8.9 28.0 2 4.1
HAS > MFH > U S HAS > MFH > LAS
HAS, U S > MFH 10.4 2 3.1 13.6 t 3.1 15.7 2 1.3 14.5 5 11.0 56.3 (9)
11.75 2 3.6
MFH > HAS MFH, HAS > U S HAS > MFH, U S
8.2 2 3.5 12.7 t 3.7
HAS > MFH
three subscales of the DMQ. To test the relative level of endorsement on the two subscales that are hypothesized to reflect “risky” drinking motives,42 two separate analyses of covariance were performed on coping and enhancement motives with social motives as a covariate. As indicated in Table 1, a trend was revealed for the HAS group to self- report more coping motives for drinking when social mo- tives are accounted for [F(2,38) = 2.26, p < 0.11. The groups did not differ with respect to enhancement motives once adjusted for covariation with social motives.
Autonomic Data Analysis Polygraph data were computer-scored. HR, SC levels
(SCLs), and SC responses [(SCRs) and average amplitude] were recorded for 5 min of the pre- and postalcohol con- sumption baseline periods. Two baseline measures were thus obtained for each of the psychophysiological mea- sures. Psychophysiological responses to the countdown to shock period were similarly recorded for both pre- and postalcohol consumption periods, and average levels were calculated based on mean calculation across the three countdown-to-shock trials. Mean HR (in beats per minute), SCL (in micromhos = reciprocal of resistance), and SCR measures were obtained for the 7-sec windows that fol- lowed the three shock trials. Average HR and SCLs were calculated for the entire sober CTSS procedure for each pre- and postalcohol consumption conditions. Pre- and postalcohol consumption HR and SCL reactivity scores were calculated by subtracting resting baseline levels from these derived means (i.e., predrink HR and SCLs during CTSS minus predrink baseline HR and SCLs and postdrink HR and SCLs during CTSS minus postdrink baseline HR and SCLs). F ~ w l e s ~ ~ has argued that, because SCL is a measure of physiological arousal that is both sensitive to discrete emotional stimuli and susceptible to peripheral physiological factors, it may not be the most sensitive indi- cator of BIS response to a stimulus. Accordingly, electro-
dermal responses (SCRs) are more proportionally related to the emotional valence of a stimulus than electrodermal levels, per se. Therefore, additional electrodermal mea- sures (number of electrodermal responses and average am- plitude of responses) were recorded and analyzed to ad- dress this potential restriction with respect to the measurement of BIS reactivity. Due to the fact that the time intervals for the CTSS periods differed (i.e., 12 sec vs. 7 sec), the nature of the SCRs (i.e., time available for discrete responses) differed considerably across the two time periods. Therefore, SCR data for these two periods were analyzed separately and will be reported accordingly.
Sober Subjective and Physiological Responses Multiple one-way ANOVAs were performed on sober
resting baseline physiological levels, and subjective and physiological reactivity to the CTSS procedure indicated that the groups did not differ with respect to resting base- line physiological measures or physiological response to the CTSS procedure. Analysis of subjective-emotional re- sponse to the anticipation period and receipt of shock indicated trends for significant risk group main effects [F(2,37) = 2 . 2 6 , ~ = 0.12 and F(2,37) = 2 . 7 6 , ~ < 0.08, respectively]. Fisher’s least significant difference post-hoc comparisons indicated that HAS subjects reported greater subjective emotional responses, compared with MFH sub- jects for both anticipation and receipt of shock periods (p < 0.05). Table 2 presents group means for sober sub- jective ratings of arousal and pain associated with anticipa- tion and receipt of shock.
Response to Alcohol Intoxication Resting Baseline Measures. BACs were first subjected to a
one-way ANOVA, which indicated that the groups achieved similar BACs immediately prior to the recording of alcohol resting and stress-induced physiological mea- sures [F(2,37) = 1.45, NS; X = 0.064 -+ 0.0251. Resting
DIFFERENTIAL SENSITIVITY TO ALCOHOL REINFORCEMENT
Table 2. Means 2 SD for Subjective Ratings of Anxiety and Pain in Association with the Anticipation and Receipt of Aversive Stimulation for Three
Groups of Men Presumed Differentially at Risk for Alcoholism
Risk group
FH-LAS HAS MFH
Mean ? SD Mean 2 SD Mean 2 SD
Sober ratings Subjective anticipatory arousal 25.8 2 9.3 29.7 +- 11 .O 21.9 2 8.3 Subjective pain and discomfort 9.8 2 3.8 12.3 t- 3.6 8.9 2 3.8
Subjective anticipatory arousal 21.5 2 9.7 20.7 2 8.5 17.1 2 7.0 Subjective pain and discomfort 9.5 2 4.8 10.4 2 4.0 7.5 2 3.2
Alcohol-intoxicated ratings
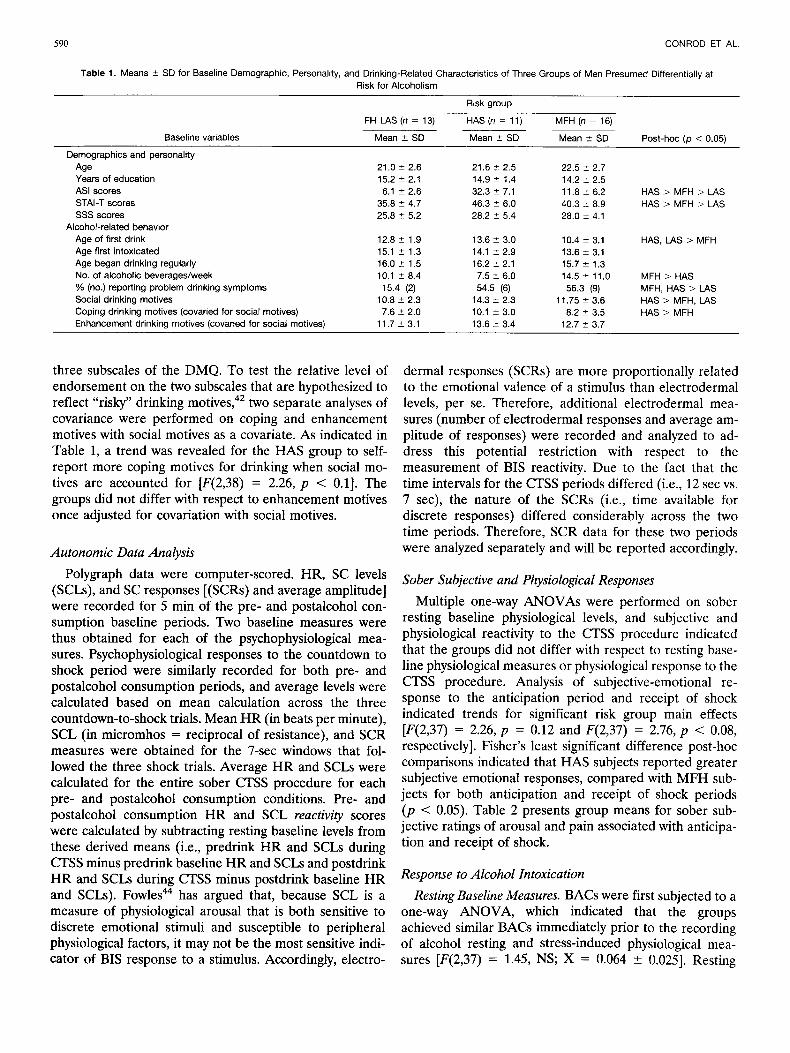
baseline levels were then subjected to two-way (risk group X alcohol condition) repeated-measures ANOVAs. A trend for a significant risk group X alcohol interaction was indicated only for resting HR [F(2,37) = 2.85, p = 0.071. Analyses of simple interactions indicated a significant risk X alcohol interaction for the comparison between MFH and FH-LAS individuals only [F(1,27) = 5 . 7 0 , ~ < 0.051. Additional simple main effects analyses indicated that this MFH versus FH-LAS simple interaction could be accounted for by the fact that only the MFH group dem- onstrated a robust increase in resting HR postalcohol con- sumption [F(1,15) = 2 2 . 6 2 , ~ < 0.00011, whereas the FH- LAS group did not evidence a significant increase resting HR levels following alcohol consumption. The group X alcohol interaction for resting baseline HR and results from subsequent simple interactions and simple main effects analyses are illustrated in Fig. l.* Risk group main effects and interactions were not significant for SCL or SCR. However, significant main effects for alcohol indicated that SCL and SCR increased from pre- to postalcohol condi- tions [F(2,38) = 6 . 6 0 , ~ < 0.05; F(2,38) = 13 .15 ,~ < 0.001, respectively].
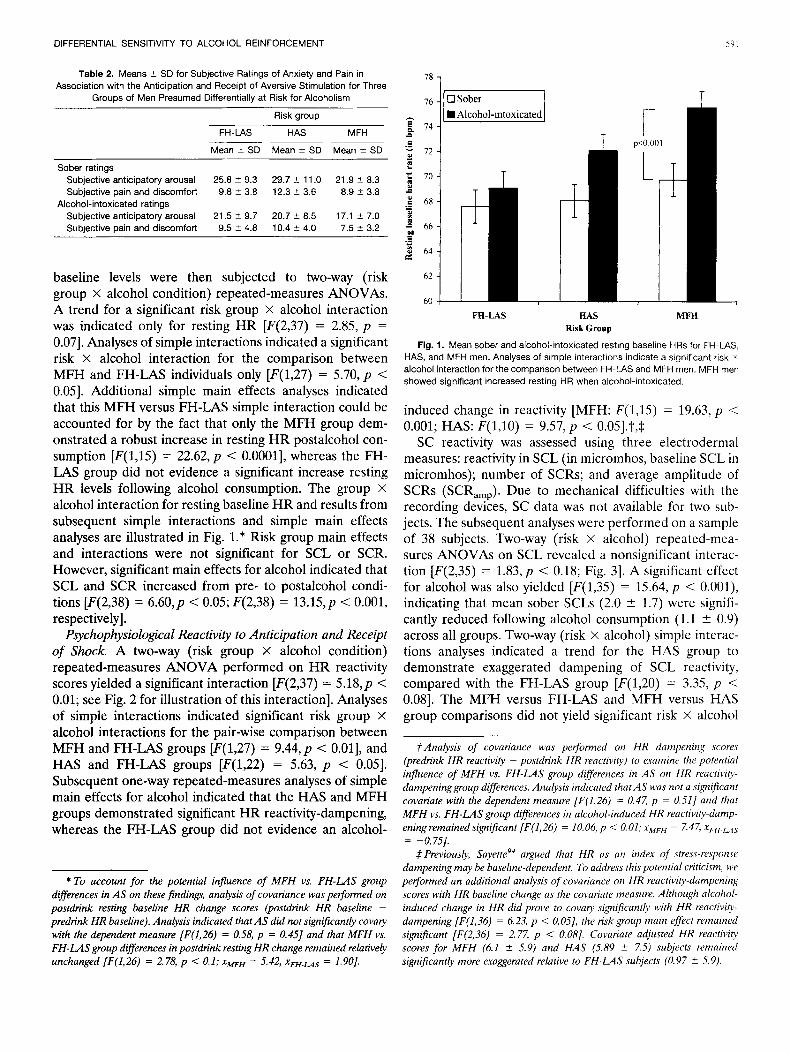
Psychophysiological Reactivity to Anticipation and Receipt of Shock. A two-way (risk group X alcohol condition) repeated-measures ANOVA performed on HR reactivity scores yielded a significant interaction [F(2,37) = 5 . 1 8 , ~ < 0.01; see Fig. 2 for illustration of this interaction]. Analyses of simple interactions indicated significant risk group X alcohol interactions for the pair-wise comparison between MFH and FH-LAS groups [F(1,27) = 9 . 4 4 , ~ < 0.011, and HAS and FH-LAS groups [F(1,22) = 5.63, p < 0.051. Subsequent one-way repeated-measures analyses of simple main effects for alcohol indicated that the HAS and MFH groups demonstrated significant HR reactivity-dampening, whereas the FH-LAS group did not evidence an alcohol-
* To account for the potential influence of MFH vs. F H - U S group differences in AS on these findings, analysis of covariance was performed on postdrink resting baseline H R change scores (postdrink H R baseline - predrink H R baseline). Analysis indicated that AS did not significantly covary with the dependent measure [F(1,26) = 0.58, p = 0.451 and that MFH vs. F H - U S group differences in postdrink resting H R change remained relatively unchanged [F(1,26) = 2.78, p < 0.1; xMFH = 5.42, xFH.us = 1.901.
0 Sober
T
FU-LAS
I r
p<o 001
.iY I
T
HAS MFH RiskGroup
Fig. I. Mean sober and alcohol-intoxicated resting baseline HRs for FH-LAS, HAS, and MFH men. Analyses of simple interactions indicate a significant risk x alcohol interaction for the comparison between FH-US and MFH men. MFH men showed significant increased resting HR when alcohol-intoxicated.
induced change in reactivity [MFH: F(1,15) = 19.63, p < 0.001; HAS: F(1,lO) = 9 . 5 7 , ~ < 0.05].?,$
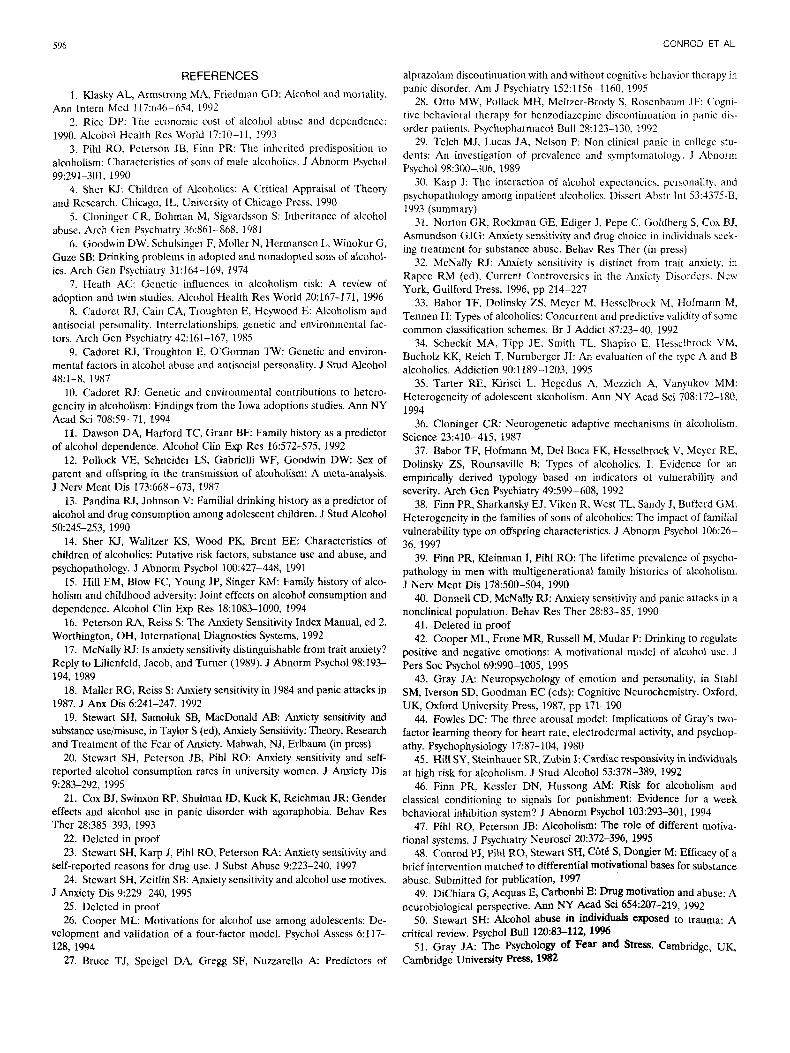
SC reactivity was assessed using three electrodermal measures: reactivity in SCL (in micromhos, baseline SCL in micromhos); number of SCRs; and average amplitude of SCRs (SCR,,,). Due to mechanical difficulties with the recording devices, SC data was not available for two sub- jects. The subsequent analyses were performed on a sample of 38 subjects. Two-way (risk X alcohol) repeated-mea- sures ANOVAs on SCL revealed a nonsignificant interac- tion [F(2,35) = 1 . 8 3 , ~ < 0.18; Fig. 31. A significant effect for alcohol was also yielded [F(1,35) = 15.64, p < O.OOl), indicating that mean sober SCLs (2.0 2 1.7) were signifi- cantly reduced following alcohol consumption (1.1 & 0.9) across all groups. Two-way (risk X alcohol) simple interac- tions analyses indicated a trend for the HAS group to demonstrate exaggerated dampening of SCL reactivity, compared with the FH-LAS group [F(1,20) = 3.35, p < 0.081. The MFH versus FH-LAS and MFH versus HAS group comparisons did not yield significant risk X alcohol
fAnalysis of covariance was performed on HR dampening scores (predrink H R reactivity - postdrink HR reactivity) to examine the potential influence of MFH vs. FH-LAS group differences in AS on HR reactivity- dampeninggroup differences. Analysis indicated that AS was not a significant covariate with the dependent measure [F(1,26) = 0.47, p = 0.51] and that MFH vs. F H - U S group differences in alcohol-induced HR reactivity-damp- eningremained significant [F(1,26) = 10.06, p < 0 . 0 1 ; ~ ~ ~ ~ = 7.47, xfi-H.us
.#Previously, S a ~ e t t e ~ ~ argued that HR as an index of stress-response dampening may be baseline-dependent. To address this potential criticism, we performed an additional analysis of covariance on HR reactivity-dampening scores with HR baseline change as the covariate measure. Although alcohol- induced change in H R did prove to covaiy significantly with HR reactiviw- dampening [F(1,36) = 6.23, p < O.OS], the risk group main effect remained significant [F(2,36) = 2.77, p < 0.08]. Covariate adjusted HR reactivity scores for MFH (6.1 2 5.9) and HAS (5.89 2 7.5) subjects remained significantly more exaggerated relative to F H - U S subjects (0.97 * 5.9).
= -0.7S].

CONROD ET AL.
0 Sober
FR-LAS BAS MFA
Risk Group
Fig. 2. Mean sober and alcohol-intoxicated HR reactivity to anticipation and receipt of shock for FH-US, HAS, and MFH men. Analyses of simple interactions indicated a significant risk x alcohol interaction for the comparisons between FH-LAS and MFH men and FH-LAS and HAS men. Both HAS and MFH men demonstrated significant HR reactivity-dampening when alcohol intoxicated.
T
FH-LAS HAS
0 Sober H Alcohol-intoxicated
Risk Group
Fig. 3. Mean sober and alcohol-intoxicated reactivity in SCL for anticipation and receipt of shock periods combined. Risk groups are: FH-LAS, HAS, and MFH men. Analyses of simple interactions indicated a significant risk x alcohol inter- action for the FH-LAS vs. HAS comparison. Only HAS men evidenced significant SCL reactivity-dampening.
interactions, indicating that the groups did not differ with respect to SCL reactivity-dampening. Analysis of simple main effects for alcohol indicated that the significant HAS versus FH-LAS simple interaction could be explained by the fact that only the HAS group demonstrated significant dampening of SCL reactivity [F(1,8) = 9.38, p < 0.051, whereas the FH-LAS group did not demonstrate such dampening. Figure 3 illustrates these group by alcohol condition interactions and simple interactions for SCL re- activity.
For the reasons discussed, SCR reactivity to the count- down to shock and receipt of shock periods were analyzed
FH-LAS vs HAS x Alcohol, p<O 1
HAS vs MFH x Alcohol, p<O 06
FH-US BAS Risk Group
il MFH
Fig. 4. Mean sober and alcohol-intoxicated number of SCRs to receipt of shock period only. Risk groups are: FH-L4S. HAS, and MFH men. Analyses of simple interactions indicated a significant risk x alcohol interaction for FH-LAS vs. HAS and MFH vs. HAS comparisons.
separately. Repeated-measures ANOVAs on electroder- ma1 responses (number of SCRs and SCR,,,) during the shock anticipation period revealed no significant main ef- fects or interactions. Analyses on total number of SCRs during the shock period yielded a trend for a significant risk X alcohol interaction [F(2,35) = 2 . 1 4 , ~ = 0.1; Fig. 41. Analyses of simple interactions indicated that the trend was best accounted for by a risk X alcohol interaction for the comparison between MFH and HAS groups [F(1,23) = 4.18, p < 0.061. Figure 4 illustrates this interaction and shows how the MFH group evidenced an increase in the number of SCRs postalcohol consumption, in contrast to an alcohol-induced decrease in SCRs to the receipt of shock demonstrated by the HAS group. Similar findings were yielded for the simple main effect comparing HAS and FH-LAS groups [F(1,20) = 2 . 1 8 , ~ = 0.1; Fig. 4). The MFH versus FH-LAS comparison yielded a nonsignificant interaction, but a significant alcohol main effect indicated that alcohol intoxication resulted in a significant increase in SCRs for these two groups only [F(1,27) = 5 . 0 6 , ~ < 0.051.
Similar analyses on SCRamp indicated a trend for a significant interaction for the shock period [F(2,35) = 2.82, p < 0.081. Tests of simple two-way interactions indicated significant effects for FH-LAS versus HAS and MFH ver- sus HAS comparisons [F(1,20) = 3 . 1 8 , ~ < 0.08; F(1,23) = 5.67, p < 0.05, respectively]. Analyses of simple main ef- fects indicated trends toward opposite alcohol effects on mean amplitude of the SCRs for HAS versus MFH and FH-LAS groups (Fig. 5). A significant simple main effect of alcohol was yielded for the MFH group only [F(1,15) = 4.50, p < 0.051, indicating that alcohol significantly in- creased in SCRs to the shock period postalcohol consump- tion for this group, in contrast to a nonsignificant decrease in such responses for the HAS group.

DIFFERENTIAL SENSITIVITY TO ALCOHOL REINFORCEMENT
T
Alcohol-intoxicated FH-LAS vs HAS x
Alcohol. p<O 08 HAS vs MFH x Alcohol, p<O 05
T
FB-LAS :I MFE
Risk Group
Fig. 5. Mean sober and alcohol-intoxicated amplitude of SCR,,, to receipt of shock period only. Risk groups are: FH-LAS, HAS, and MFH men. Analyses of simple interactions indicated a significant risk X alcohol interaction for FH-LAS vs. HAS and MFH vs. HAS men comparisons.
Subjective Emotional Responses to Shock Anticipation and Receipt of Shock
Total scores for subjective ratings of anticipatory arousal were similarly subjected to a two-way (risk X alcohol) repeated-measures ANOVA. A trend for a significant main effect for risk was indicated [F(2,36) = 2 . 8 2 , ~ < 0.081, with the HAS group self-reporting heightened subjective antic- ipatory arousal (mean: 25.2 ? 10.5), compared with the MFH (19.5 5 7.9) group only (p < 0.05). A robust effect for alcohol [F(1,36) = 9 . 8 9 , ~ < 0.011 indicated that alcohol significantly tempered subjective ratings of anxiety in an- ticipation of the shock across all three groups (prealcohol mean: 25.3 ? 9.7; postalcohol mean: 19.5 5 8.4). Similar results were yielded for the analysis of subjective ratings of pain and discomfort in association with receipt of the elec- tric shock. A trend for a significant main effect for risk was indicated [F(2,36) = 2.81, p < 0.081, with post-hoc com- parisons revealing a significant difference between the HAS (11.4 5 3.8) and MFH (8.2 ? 3.5) groups (p < 0.05) averaged across both sober and alcohol-intoxicated condi- tions. Alcohol was shown to significantly reduce of subjec- tive pain ratings to the aversive stimulation [F(1,36) = 4.51, p < 0.051 across all groups (prealcohol mean: 10.2 ? 3.9; postalcohol mean: 8.9 5 4.1). Table 2 presents group means and standard deviations for sober and alcohol-intox- icated ratings of anxiety and pain associated with the shock procedure.
DISCUSSION
The present investigation addressed two important the- oretical questions that, to our knowledge, have not been examined previously. The first question involved the com- parison of HAS males to LAS males on sensitivity to alco- hol reinforcement. The findings replicate, in many respects,
those reported by Stewart and Pihl,'4 investigating the effects of alcohol intoxication on physiological and subjec- tive responses to aversive stimulation in HAS women. Ac- cording to the present findings, HAS men responded much like HAS women, in that they manifested heightened sub- jective-emotional responses to threat, but did not neccssar- ily demonstrate physiological hyperresponsiveness. The findings are in line with recent reports indicating that HAS hyperresponsiveness to stress may be limited to the cmo- tional domain rather than the somatic domain."),x7 Fur- thermore, alcohol was shown to dampen subjective-emo- tional responses to threat in all subjects, but selectively dampened physiological indices of fear-responding in HAS men (e.g., electrodermal levels and responses). HAS men also reported elevated subjective ratings of anticipatory anxiety and pain to receipt of shock relative to MFH men. Asmundson and Taylorx3 recently reported that AS (and associated fear of pain) was positively related to the ten- dency to use pain-related escape/avoidance behaviors (in- cluding using pharmacological agents) as a means of coping with chronic musculoskeletal pain. Furthermore Coxx4 sug- gested that high AS might encompass a broader range of fears, such as fear of pain, harmfulness, and strong internal sensations, rather than being specific to anxiety symptoms. According to the present findings, alcohol has the potential to be negatively reinforcing for individuals who fear anxi- ety-related symptoms and for those who are prone to in- tense affective responses to pain. The apparent role of AS in the affective response to pain might explain why HAS individuals of the present study evidenced reactivity and dampening to the physically aversive stimulus across a greater diversity of reactivity and dampening measures (e.g., subjective, cardiovascular, and electrodermal) relative to the findings from a previous study, with HAS subjects involving different aversive stimulus (i.e., loud noise bursts) that likely did not result in physical arousal of equal inten- sity.
These idiosyncratic alcohol-intoxicated response pat- terns manifested by HAS men are suggestive of a sensitivity to the negatively reinforcing, potentially fear-dampening, properties of alcohol. Whether this sensitivity is qualita- tively different from that demonstrated by men with MFH, who are presumably at elevated risk for an alternative subtype of alcoholism, was the second empirical question of the present investigation. The findings partially shed light on this query. The nature of the alcohol-intoxicated re- sponse patterns manifested by these two at-risk groups are both similar and distinct, depending on the physiological measures used to reflect sensitivity to alcohol reinforce- ment. When the measures used were nonspecific indices of stimulus reactivity, such as HR (not coupled with incentive reward), the two at-risk groups appeared to demonstrate similar sensitivity to the stress-response dampening effects of alcohol. However, analysis of the physiological measures (i.e., electrodermal responses) that are presumed to reflect more distinctly reactivity within the brain emotion system

594 CONROD ET AL.
responsible for behavioral inhibition in response to poten- tial danger revealed that the HAS group manifested idio- syncratic alcohol-intoxicated response patterns. These find- ings, specifically, may be indicative of a sensitivity to “fear- dampening” from alcohol in HAS individuals in contrast to general “stimulus reactivity-dampening” evidenced by MFH individuals.
MFH individuals appear to be highly sensitive to the effects of alcohol on resting HR levels, at least relative to the FH- control group. Further evidence is no doubt required before we can conclusively state that resting car- diac responses to alcohol intoxication reflect response to the psychostimulant, incentive rewarding properties of al- cohol intoxication as suggested by Pihl and Peterson.47 However, there is an accumulating body of empirical work with animals and human subjects (particularly those at elevated risk for heavy consumption of the drug) suggesting that sensitivity to the positively reinforcing psychostimulant properties of alcohol is indexed by resting cardiac reactivity to alcohol intoxication (reviewed by Peterson et al.70) and is an important biological marker of the genetic predisposi- tion to familial a l c ~ h o l i s m . ~ ~ - ~ ~ We have demonstrated in a number of studies that this cardiac response corresponds to self-report and laboratory measures of drinking behavior,72 alcohol-induced changes in positive mood states,72 and other proposed biological markers for the inherited predis- position to a l c o h ~ l i s m . ~ ~ Furthermore, we have demon- strated that faster rate of alcohol consumption results in an even further exaggeration of this idiosyncratic response pattern,’l a characteristic of drugs with psychostimulant properties (e.g., cocaine, heroin, and r ~ i c o t i n e ) . ~ ~ ’ ~ ~
It has previously been reported that HAS women do not demonstrate such a response to alcohol i n to~ ica t ion .~~ In the present study, HAS men were similarly shown not to differ significantly from the FH-LAS control group with respect to this particular cardiac response to alcohol intox- ication. However, neither were they shown to differ signif- icantly from the MFH group. It was, nevertheless, indicated that the increase in resting HR manifested by MFH men was greater than that demonstrated by HAS men and that only MFH men differed significantly from the control group on this response. Further investigation with larger sample sizes may clarify the nature of the similarities and differences between these high-risk groups.
The three groups were equally physiologically reactive to aversive stimulation in the present study. This is somewhat in contrast to previous findings that have shown MFH versus FH - group differences in cardiovascular reactivi- ty61-63 and HAS versus LAS group differences in electro- dermal reactivity to aversive ~ t imula t ion .~~’~’ However, physiological reactivity to aversive stimulation has been inconsistently associated with genetic risk for alcoholism and ~ ~ , 5 4 , 8 7 - 8 9 possibly because the stress paradigms used to test these relationships vary widely across studies. It is suggested that future studies investigating the potential role of specific motivational systems in the predisposition
to alcoholism use stress paradigms that more distinctly measure BIS- versus BAS-specific reactivity.”976 Stewart and PihlS4 previously suggested that a loud noise burst stressor may only indirectly increase arousal symptoms so feared by HAS individuals that may also be the case for the electric shock stressor (although possibly less so). More relevant stressors for eliciting HAS versus LAS group dif- ferences in stress-responding might be hyperventilation and CO, inhalation challenges that more directly result in phys- iological changes that are then only misinterpreted by HAS individuals to result in heightened fear responses.57958 Fur- thermore, as AS appears to manifest itself as a bias toward socially threatening information in men rather than physi- cally threatening information as it does in women,6o stres- sors that incorporate a social component (e.g., performance involving social evaluation) might maximally reveal height- ened fear-responding in HAS male subjects.
Of concern was the finding that MFH and FH-LAS men did not differ on the stress paradigm that previously differ- entiated these groups of men. In comparison to these pre- vious reports, the FH-LAS men of the present sample appear to demonstrate uncharacteristically high sober au- tonomic reactivity patterns. Furthermore, the correlation between sober reactivity and alcohol-induced dampening in the present sample was unusually low (R = 0.36 versus R =
0.88 reported for previous and can be entirely accounted for by the fact that reactivity and dampening were uncorrelated in the F H - U S group, yet highly corre- lated in the HAS and MFH groups (r = 0.78 and r = 0.85, respectively) and at levels equivalent to those reported for previous studies.72290 We are unable to offer an explanation as to why the present experimental design resulted in ele- vated sober autonomic reactivity for the low-risk group. However, we have previously shown that certain individual variables (e.g., family history of hypertension) are associ- ated with elevated sober cardiovascular reactivity patterns that do not appear to be susceptible to dampening from alcohol i n to~ ica t ion .~~ What is highlighted in the present study is that individuals presumed at risk for alcoholism demonstrate autonomic reactivity patterns that are partic- ularly susceptible to the effects of alcohol. This important and consistent finding should be considered in future in- vestigations of the psychobiological constituents of popula- tion-specific vulnerability to alcoholism.
A novel finding from the present investigation was that stress-response dampening appears to be made up of dis- similar elements that are indexed by specific subjective and psychophysiological measures. This distinction is particu- larly relevant for the prevention and treatment of subtypes of alcoholism syndromes. Alcohol consumption in HAS individuals could be motivated by a sensitivity to the fear/ anxiety-dampening effects of alcohol. As such, anxiety- provoking situations may represent circumstances in which the HAS individual is at elevated risk for increased alcohol use. Alternatively, MFH individuals appear to be sensitive to the “stimulus reactivity”-dampening effects of alcohol

DIFFERENTIAL SENSITIVITY TO ALCOHOL REINFORCEMENT iOi
and additionally sensitive to the stimulating effects of alco- hol on general arousal. MFH young men have also been shown to demonstrate deficits in classical conditioning to signals of punishment (presumed to reflect weak BIS pro- c e ~ s e s ) . ~ ~ Each of these psychophysiological response pat- terns have been shown to correspond to alcohol related- behavior.46972291 The findings collectively suggest that situations that involve intense sensory stimulation will rep- resent circumstances in which MFH individuals are at ele- vated risk for drinking and may lack behavioral inhibitory mechanisms that would otherwise moderate alcohol intake in circumstances when alcohol intoxication is not appropri- ate. Additional sensitivity to the incentive rewarding prop- erties of alcohol may reinforce the MFH individual to consume larger amounts of alcohol within that particular situation and in subsequent situations with similar stimu- lating features. This pattern of physiological and behavioral characteristics might explain the link between externalizing disorders, elevated alcohol consumption behavior, and the early onset and severe course of the alcoholic syndrome to which MFH men appear most s ~ s c e p t i b l e . ' ~ , ~ ~ ~ ~ ~ , ~ ~ ~ ~ ~ It is suggested that intervention strategies for such high-risk populations and treatment or relapse prevention programs for affected individuals manifesting such motivational pro- files target reducing sensitivity to alcohol reinforcement and associated susceptibility to various high-risk drinking situations.
An interesting finding was that the MFH group self- reported elevated weekly alcohol consumption at this early stage of life (age 21 approximately) and reported having been exposed to alcohol at a significantly earlier age, com- pared with the other two groups. These findings are in line with the hypothesis that MFH individuals are at elevated risk for the type I1 alcoholic syndrome that is characterized primarily by earlier onset problem drinking.3-5,92 Interest- ingly, both the MFH and HAS groups reported problem drinking at this early age, compared with the FH-LAS controls. Why HAS individuals reported elevated problem drinking symptoms without actually self-reporting elevated alcohol consumption patterns might be explained by the fact that they self-reported relatively more coping-related drinking motives. Problem drinking symptoms have previ- ously been shown to correlate with coping-related drinking motives, even after accounting for typical levels of alcohol use.26 We tested this possible explanation by investigating whether group differences in brief MAST scores could be accounted for by group differences in reasons for drinking. An analysis of covariance, with DMQ coping motives as a covariate, indicated that the HAS and FH-LAS groups no longer differed in prevalence of problem drinking symp- toms, whereas the MFH and FH-LAS groups remained different (p < 0.1). Thus, it appears that coping-related drinking mediates the relationship between AS and prob- lem drinking symptoms, but not the relationship between MFH status and problem drinking symptoms. In light of these findings, it is suggested that future research investi-
gate the differential relationships of alcohol-reinforcement sensitivities to specific aspects of drinking behavior or drinking-related problems.
One possible limitation of the present investigation is that alcohol response patterns were not contrasted against responses to a placebo-control drinking condition. How- ever, a substantial number of previous studies using these stress and alcohol challenge paradigms with MFH and HAS subjects have demonstrated that susceptibility to al- cohol-induced reactivity-dampening and alcohol-induced psychostimulation are relatively independent of placebo, expectancy, or habituation effects. For example, a series of studies by Finn & Pih1"',62 and Finn et al.73 have shown that order of beverage condition (alcohol/placebo) had no effect on psychophysiological measures of reactivity-dampening to aversive stimulation. Furthermore, Stewart et al.7s dem- onstrated that repeated administration of the tone-shock paradigm results in dampening of reactivity following con- sumption of moderate to high doses of alcohol only. More- over, Stewart and Pihls4 showed that alcohol-induced dampening of electrodermal reactivity could not be ac- counted for by potential habituation to repeated adminis- tration of aversive stimulation prior to the consumption of alcohol. Rather, HAS women in this study evidenced mild sensitivity to repeated administration of the aversive stim- ulus when sober. Finally, two placebo-controlled studies exploring cognitive, affective, and somatic responses of HAS individuals to hyperventilation and attentional inter- ference tasks demonstrate dose-dependent alcohol effects that appear independent of expectancy effects.s5357
Although the relatively restricted sample size in the present investigation appeared to limit some of the findings to trends only, certain robust risk group by alcohol inter- actions indicated that groups of men presumed to be at elevated risk for specific alcoholism syndromes were signif- icantly and differentially sensitive to the effects of alcohol intoxication. Whether these alcohol effects constitute rein- forcement for alcohol-related behavior warrants further study. Research paradigms that incorporate the use of laboratory measures of alcohol consumption (e.g., taste- rating paradigm) have identified individual and situational variables that result in exaggerated alcohol consumption by HAS and MFH individuals relative to their respective con- troI g r o ~ p s ~ ~ . ~ ~ * ~ ~ and may prove further informative with future study. Furthermore, it is recommended that future investigations of population-specific alcohol sensitivities be conducted with larger sample sizes, and utilize more finely developed experimental paradigms that are gender-sensitive and that more distinctly reflect BIS- and BAS-specific activity.
ACKNOWLEDGMENTS
The authors acknowledge the contribution of Mr. Marc Gross for the development of the data acquisition and scoring programs for psychophysiological recordings, and Dr. Sherry Stewart for her comments on earlier drafts of the manuscript.
596 CONROD ET AL.
REFERENCES alprazolam discontinuation with and without cognitive behavior therapy in
1. Klasky AL, Armstrong MA, Friedman GD: Alcohol and mortality. Ann Intern Med 117:646-654, 1992
2. Rice DP: The cconomic cost o f alcohol abuse and dcpcndcncc: 1990. Alcohol Health Res World 17:lO-11, 1993
3. Pihl RO, Pcterson JB, Finn PR: The inherited predisposition to alcoholism: characteristics of sons of male alcoholics. J Abnorm Psychol 99:291-301, 1990
4. Shcr KJ: Children of Alcoholics: A Critical Appraisal of Theory and Research. Chicago, IL, University of Chicago Press, 1990
5. Cloningcr CR, Bohman M, Sigvardsson S: Inheritance of alcohol abuse. Arch Gcn Psychiatry 36:861-868, 1981
6. Goodwin DW, Schulsinger F, Moller N, Hcrmansen L, Winokur G, Guze SB: Drinking problems in adopted and nonadopted sons of alcohol- ics. Arch Gen Psychiatry 31:164-169, 1974
7. Heath AC: Genetic influences in alcoholism risk A review of adoption and twin studies. Alcohol Health Res World 20:167-171, 1996
8. Cadoret RJ, Cain CA, Troughton E, Heywood E. Alcoholism and antisocial personality. Interrclationships, genetic and environmental fac- tors. Arch Fen Psychiatry 42:161-167, 1985
9. Cadoret RJ, Troughton E, OGorman TW: Genetic and environ- mental factors in alcohol abuse and antisocial personality. J Stud Alcohol
10. Cadoret RJ: Genetic and environmental contributions to hetero- geneity in alcoholism: Findings from the Iowa adoptions studies. Ann NY Acad Sci 70859-71, 1994
11. Dawson DA, Harford TC, Grant BF: Family history as a predictor of alcohol dependence. Alcohol Clin Exp Res 16:572-575, 1992
12. Pollock VE, Schneider LS, Gabrielli WF, Goodwin DW: Sex of parent and offspring in the transmission of alcoholism: A meta-analysis. J New Ment Dis 173:668-673, 1987
13. Pandina RJ, Johnson V Familial drinking history as a predictor of alcohol and drug consumption among adolescent children. J Stud Alcohol 50:245-253, 1990
14. Sher KJ, Walitzer KS, Wood PK, Brent EE: Characteristics of children of alcoholics: Putative risk factors, substance use and abuse, and psychopathology. J Abnorm Psychol 100:427-448, 1991
15. Hill EM, Blow FC, Young JP, Singer KM: Family history of alco- holism and childhood adversity: Joint effects on alcohol consumption and dependence. Alcohol Clin Exp Res 18:1083-1090, 1994
16. Peterson RA, Reiss S: The Anxiety Sensitivity Index Manual, ed 2. Worthington, OH, International Diagnostics Systems, 1992
17. McNally RJ: Is anxiety sensitivity distinguishable from trait anxiety? Reply to Lilienfeld, Jacob, and Turner (1989). J Abnorm Psychol 98:193- 194, 1989
18. Maller RG, Reiss S: Anxiety sensitivity in 1984 and panic attacks in 1987. J Anx Dis 6:241-247, 1992
19. Stewart SH, Samoluk SB, MacDonald AB: Anxiety sensitivity and substance useimisuse, in Taylor S (ed), Anxiety Sensitivity: Theory, Research and Treatment of the Fear of Anxiety. Mahwah, NJ, Erlbaum (in press)
20. Stewart SH, Peterson JB, Pihl RO: Anxiety sensitivity and self- reported alcohol consumption rates in university women. J Anxiety Dis
21. Cox BJ, Swinxon RP, Shulman ID, Kuck K, Reichman JR: Gender effects and alcohol use in panic disorder with agoraphobia. Behav Res Ther 28:385-393, 1993
48:1-8, 1987
9~283-292, 1995
22. Deleted in proof 23. Stewart SH, Karp J, Pihl RO, Peterson RA: Anxiety sensitivity and
24. Stewart SH, Zeitlin SB: Anxiety sensitivity and alcohol use motives.
25. Deleted in proof 26. Cooper M L Motivations for alcohol use among adolescents: De-
velopment and validation of a four-factor model. Psychol Assess 6:117- 128, 1994
27. Bruce TJ, Speigel DA, Gregg SF, Nuzzarello A: Predictors of
self-reported reasons for drug use. J Subst Abuse 9:223-240, 1997
J Anxiety Dis 9229-240, 1995
panic disorder. Am J Psychiatry 152:1156-1160, 1995 28. Otto MW, Pollack MH, Meltzer-Brody S, Rosenbaum JF: Cogni-
tivc hchavioral therapy for bcnzodiazcpinc discontinuation in panic dis- order patients. Psychopharmaco! Bull 28:123-130. 1992
29. Telch MJ, Lucas JA, Nelson P: Non-clinical panic in college stu- dents: An investigation of prevalence and symptomatology. J Ahnorm Psychol 98:300-306, 1989
30. Karp J: The interaction of alcohol cxpcctancics, pcrsonaiity, and psychopathology among inpatient alcoholics. Disscrt Ahstr Int 53:4375-B, 1993 (summary)
31. Norton GR, Rockman GE, Ediger J, Pepe C, Goldberg S , Cox BJ, Asmundson GJG: Anxiety sensitivity and drug choice in individuals xek- ing treatment for substance abuse. Behav Res Thcr (in press)
32. McNally RJ: Anxiety scnsitivity is distinct from trait anxiety, in Rapec RM (ed), Current Controvcrsics in the Anxiety Disorders. New York, Guilford Press, 1996, pp 214-227
33. Babor TF, Dolinsky ZS, Mcyer M, Hessclbrock M, Hofmann M, Tennen H: Types of alcoholics: Concurrcnt and predictive validity of some common classification schemes. Br J Addict 87:23-40, 1992
34. Schuckit MA, Tipp JE, Smith TL. Shapiro E, Hessclbrock VM, Bucholz KK, Reich T, Nurnbcrgcr JI: An evaluation of the type A and B alcoholics. Addiction 90:1189-1203, 1995
35. Tarter RE, Kirisci L, Hcgedus A, Mczzich A, Vanyukov MM: Heterogeneity of adolescent alcoholism. Ann NY Acad Sci 708:172-180, 1994
36. Cloninger CR: Neurogenetic adaptive mechanisms in alcoholism. Science 23:410-415, 1987
37. Babor TF, Hofmann M, Dcl Boca FK, Hesselbrock V, Meyer RE, Dolinsky ZS, Rounsaville B: Types of alcoholics. I. Evidence for an empirically derived typology based on indicators of vulnerability and severity. Arch Gen Psychiatry 49:599-608, 1992
38. Finn PR, Sharkansky EJ, Viken R, West TL, Sandy J, Buffcrd GM: Heterogeneity in the families of sons of alcoholics: The impact of familial vulnerability type on offspring characteristics. J Abnorm Psychol 106:26- 36, 1997
39. Finn PR, Kleinman I, Pihl RO: The lifetime prevalence of psycho- pathology in men with multigenerational family histories of alcoholism. J Nerv Ment Dis 178:500-504, 1990
40. Donnell CD, McNally RJ: Anxiety sensitivity and panic attacks in a nonclinical population. Behav Res Ther 28:83-85, 1990
41. Deleted in proof 42. Cooper ML, Frone MR, Russell M, Mudar P: Drinking to rcgulate
positive and negative emotions: A motivational model of alcohol use. J Pers Soc Psychol 69:990-1005, 1995
43. Gray JA: Neuropsychology of emotion and personality, in Stahl SM, Iverson SD, Goodman EC (eds): Cognitive Neurochemistry. Oxford, UK, Oxford University Press, 1987, pp 171-190
44. Fowles DC: The three arousal model: Implications of Gray’s two- factor learning theory for heart rate, electrodermal activity, and psychop- athy. Psychophysiology 17:87-104, 1980
45. Hill SY, Steinhauer SR, Zubin J: Cardiac tespansivity in individuals at high risk for alcoholism. J Stud Alcohol 53:378-389, 1992
46. Finn PR? Kcssler DN, Hussong AM: Risk for alcoholism and classical conditioning to signals for punishment: Evidence for a week behavioral inhibition system? J Abnorm Psycho1 103:293-301, 1994
47. Pihl RO, Peterson JB: Alcoholism: The role O f different motiva- tional systems. J Psychiatry Neurosci 20:372-396, 1995 48. Conrod PJ, Pihl RO, Stewart SH, C6tk s, Dongier M. Efficacy of a
brief intervention matched to differential motivational bases for substance abuse. Submitted for publication, 1997
49. DiChiara G, Acquas E, Carbonbi E: Drug motivation and abuse: A neurobiological perspective. Ann NY A a d Sci 654207-219, 1992
50. Stewart SH: Alcohol abuse in individuals exposed to trauma: A critical review. Psychol Bull 120:83-1!2 1996
d?heS. Cambridge, UK, 51. Gray J A The P~chologY Of I .
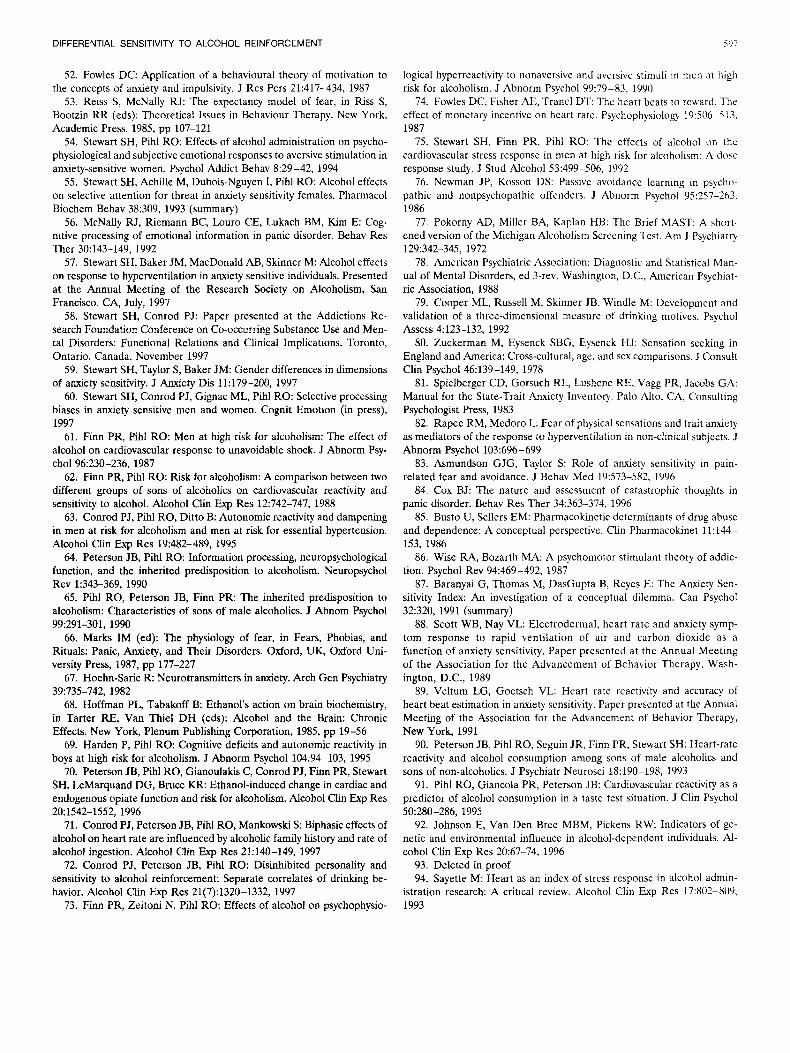
DIFFERENTIAL SENSITIVITY TO ALCOHOL REINFORCEMENT 3117
52. Fowles D C Application of a behavioural theory of motivation to the concepts of anxiety and impulsivity. J Res Pers 21:417-434, 1987
53. Reiss S, McNally RJ: The expectancy model of fear, in Riss S, Bootzin RR (eds): Theoretical Issues in Behaviour Therapy. New York, Academic Press, 1985, pp 107-121
54. Stewart SH, Pihl RO: Effects of alcohol administration on psycho- physiological and subjective emotional responses to aversive stimulation in anxiety-sensitive women. Psychol Addict Behav 8:29-42, 1994
55. Stewart SH, Achille M, Dubois-Nguyen I, Pihl RO: Alcohol effects on selective attention for threat in anxiety sensitivity females. Pharmacol Biochem Behav 38:309, 1993 (summary)
56. McNally RJ, Riemann BC, Louro CE, Lukach BM, Kim E: Cog- nitive processing of emotional information in panic disorder. Behav Res Ther 30:143-149, 1992
57. Stewart SH, Baker JM, MacDonald AB, Skinner M: Alcohol effects on response to hyperventilation in anxiety sensitive individuals. Presented at the Annual Meeting of the Research Society on Alcoholism, San Francisco, CA, July, 1997
58. Stewart SH, Conrod PJ: Paper presented at the Addictions Re- search Foundation Conference on Co-occurring Substance Use and Men- tal Disorders: Functional Relations and Clinical Implications. Toronto, Ontario, Canada, November 1997
59. Stewart SH, Taylor S, Baker JM: Gender differences in dimensions of anxiety sensitivity. J Anxiety Dis 11:179-200, 1997
60. Stewart SH, Conrod PJ, Gignac ML, Pihl RO: Selective processing biases in anxiety sensitive men and women. Cognit Emotion (in press), 1997
61. Finn PR, Pihl RO: Men at high risk for alcoholism: The effect of alcohol on cardiovascular response to unavoidable shock. J Abnorm Psy-
62. Finn PR, Pihl RO: Risk for alcoholism: A comparison between two different groups of sons of alcoholics on cardiovascular reactivity and sensitivity to alcohol. Alcohol Clin Exp Res 12:742-747, 1988
63. Conrod PJ, Pihl RO, Ditto B: Autonomic reactivity and dampening in men at risk for alcoholism and men at risk for essential hypertension. Alcohol Clin Exp Res 19:482-489, 1995 64. Peterson JB, Pihl RO: Information processing, neuropsychological
function, and the inherited predisposition to alcoholism. Neuropsychol Rev 1:343-369, 1990
65. Pihl RO, Peterson JB, Finn P R The inherited predisposition to alcoholism: Characteristics of sons of male alcoholics. J Abnom Psychol
66. Marks IM (ed): The physiology of fear, in Fears, Phobias, and Rituals: Panic, Anxiety, and Their Disorders. Oxford, UK, Oxford Uni- versity Press, 1987, pp 177-227
67. Hoehn-Saric R: Neurotransmitters in anxiety. Arch Gen Psychiatry
68. Hoffman PL, Tabakoff B: Ethanol's action on brain biochemistry, in Tarter RE, Van Thiel DH (eds): Alcohol and the Brain: Chronic Effects. New York, Plenum Publishing Corporation, 1985, pp 19-56
69. Harden P, Pihl RO: Cognitive deficits and autonomic reactivity in boys at high risk for alcoholism. J Abnorm Psychol 104:94-103, 1995
70. Peterson JB, Pihl RO, Gianoulakis C, Conrod PJ, Finn PR, Stewart SH, LeMarquand DG, Bruce KR: Ethanol-induced change in cardiac and endogenous opiate function and risk for alcoholism. Alcohol Clin Exp Res
71. Conrod PJ, Peterson JB, Pihl RO, Mankowski S: Biphasic effects of alcohol on heart rate are influenced by alcoholic family history and rate of alcohol ingestion. Alcohol Clin Exp Res 21:140-149, 1997
72. Conrod PJ, Peterson JB, Pihl RO: Disinhibited personality and sensitivity to alcohol reinforcement: Separate correlates of drinking be- havior. Alcohol Clin Exp Res 21(7):1320-1332, 1997
73. Finn PR, Zeitoni N, Pihl RO: Effects of alcohol on psychophysio-
chol 96~230-236, 1987
99~291-301, 1990
39~735-742, 1982
20:1542-1552, 1996
logical hypcrreactivity to nonaversive and avcrsivc stimuli in mcn a t high risk for alcoholism. J Abnorm Psychol 99:79-83, 1990
74. Fowles DC, Fisher AE, Trancl DT: The heart beats to reward. The effect of monetary incentivc on heart ratc. Psychophysiology 19:506-5 13. 1987
75. Stewart SH, Finn PR, Pihl RO: The effects of alcohol on thc cardiovascular stress response in men at high risk for alcoholism: A dosc response study. J Stud Alcohol 53:499-506, 1992
76. Newman JP, Kosson DS: Passive avoidancc learning in psycho- pathic and nonpsychopathic offenders. J Abnorm Psychol 95:257-263. 1986
77. Pokorny AD, Miller BA, Kaplan HB: Thc Brief MAST: A short- ened version of the Michigan Alcoholism Screening Test. Am J Psychiatry
78. American Psychiatric Association: Diagnostic and Statistical Man- ual of Mental Disorders, ed 3-rev. Washington, D.C., American Psychiat- ric Association, 1988
79. Cooper ML, Russell M, Skinner JB, Windle M: Dcvelopmcnt and validation of a three-dimensional measurc of drinking motives. Psychol Assess 4:123-132, 1992
80. Zuckerman M, Eysenck SBG, Eyscnck HJ: Sensation seeking in England and America: Cross-cultural, age, and sex comparisons. J Consult Clin Psychol 46:139-149, 1978
81. Spielberger CD, Gorsuch RL, Lushene RE, Vagg PR, Jacobs GA: Manual for the State-Trait Anxiety Inventory. Palo Alto, CA, Consulting Psychologist Press, 1983
82. Rapee RM, Medoro L: Fear of physical sensations and trait anxiety as mediators of the response to hyperventilation in non-clinical subjects. J Abnorm Psychol 103:696-699
83. Asmundson GJG, Taylor S: Role of anxiety sensitivity in pain- related fear and avoidance. J Bchav Med 19573-582, 1996
84. Cox BJ: The nature and assessment of catastrophic thoughts in panic disorder. Behav Res Ther 34:363-374, 1996
85. Busto U, Sellers EM: Pharmacokinetic determinants of drug abuse and dependence: A conceptual perspective. Clin Pharmacokinet 11:144- 153, 1986
86. Wise RA, Bozarth MA: A psychomotor stimulant theory of addic- tion. Psychol Rev 94:469-492, 1987
87. Baranyai G, Thomas M, DasGupta B, Rcycs E: The Anxiety Sen- sitivity index: An investigation of a conceptual dilemma. Can Psychol 32:320, 1991 (summary)
88. Scott WB, Nay VL: Electrodermal, heart rate and anxiety symp- tom response to rapid ventilation of air and carbon dioxide as a function of anxiety sensitivity. Paper presented at the Annual Meeting of the Association for the Advancement of Behavior Therapy, Wash- ington, D.C., 1989
89. Veltum LG, Goetsch VL: Heart ratc reactivity and accuracy of heart beat estimation in anxiety scnsitivity. Paper presented at the Annual Meeting of the Association for the Advancement of Behavior Therapy, New York, 1991
90. Peterson JB, Pihl RO, Seguin JR, Finn PR, Stewart SH: Heart-rate reactivity and alcohol consumption among sons of male alcoholics and sons of non-alcoholics. J Psychiatr Neurosci 18:190-198, 1993
91. Pihl RO, Giancola PR, Peterson JB: Cardiovascular reactivity as a predictor of alcohol consumption in a taste test situation. J Clin Psychol
92. Johnson E, Van Den Bree MBM, Pickens RW: Indicators of ge- netic and environmental influence in alcohol-dependent individuals. Al- cohol Clin Exp Res 20:67-74, 1996
129~342-345, 1972
50~280-286, 1995
93. Deleted in proof 94. Sayette M: Heart as an index of strcss response in alcohol admin-
istration research: A critical review. Alcohol Clin Exp Res 17:802-809, 1993
Related Documents











