1992, The British Journal of Radiology, 65, 289-294 VOLUME 65 NUMBER 772 APRIL1992 The British Journal of Radiology Diagnosis of brain death: superiority of perfusion studies with 99 Tc m -HMPAO over conventional radionuclide cerebral angiography By *A. de la Riva, F. M. Gonzalez, J. M. Llamas-Elvira, J. M. Latre, A. Jimenez-Heffernan, tE. Vidal, M- Martinez, M. Torres, tR. Guerrero, tF. Alvarez and A. Mateo Departments of Nuclear Medicine, *Neurosurgery, tlnternal Medicine and ^Intensive Care, "Reina Sofia" Hospital, Avda. Menendez Pidal s/n, 14004 Cordoba, Spain (Received 20 June 1991 and in revised form 23 September 1991, accepted 8 October 1991) Keywords: "Tc m -HMPAO, Cerebral flow, Brain death Abstract. The use of technetium-99m hexamethyl-propyleneamine oxime ( 99 Tc m -HMPAO) in the diagnosis of brain death has been evaluated in 41 studies of 37 patients with severe brain injury, who were under the effect of drugs or when other diagnostic methods were equivocal. HMPAO studies were compared with conventional radionuclide angiography performed simultaneously by intravenous administration of HMPAO as a bolus. The ages of patients ranged from 4 months to 75 years. Dynamic flow images and 5-min static uptake images were acquired following bolus injection of 555 Mbq of "Tc m -HMPAO. All patients showing no brain uptake were confirmed as brain-dead by standard clinical criteria, with no contradictory cases in the static study. In addition, all patients who were not brain-dead showed HMPAO uptake at least in the brainstem. Dynamic flow images were equivocal in five patients, four of whom had no uptake on static images and clinically confirmed brain death. In addition, two other cases showed "mismatched" dynamic and static images: in one case no perfusion was observed on flow images but uptake restricted to the posterior fossa was seen on static images; the other case showed perfusion on the dynamic study and static imaging revealed hemispheric uptake with no posterior fossa uptake. Static perfusion ^"c m -HMPAO studies offer advantages over conventional brain scintigraphy, better results being due to adequate assessment of posterior fossa activity and avoiding equivocal studies. Assessment of brain death has been increasing in impor- Contrast medium angiography of the brain is con- tance since the advent of organ transplantation. sidered to be the "gold standard" for brain perfusion Advances in life-support systems and the increasing (Pjura & Kim, 1987), but is an expensive, invasive and demand for organ donors need diagnostic methods that technically complex procedure that requires transpor- identify irreversible loss of brain function accurately and tation of the patient to an angiography facility and promptly. positioning on the table with the risk of clinical deterio- The diagnosis of brain death is difficult to establish in ration (Andrews et al, 1990). patients with artificial life-support systems, and is Radionuclide cerebral angiography has been further hindered by the use of barbiturate-induced coma proposed as an alternative method for the evaluation of and hypothermia for suppression of brain metabolic brain perfusion, showing a good correlation with four- activity. In these cases, electroencephalographic (EEG) vessel angiography (Kricheff et al, 1975; Korein et al, activity may be absent or markedly reduced and the 1977). Scintigraphy has been widely accepted, although only reliable method of diagnosis is the absence of it has problems of interpretation in cases of poor bolus intracranial blood flow. This is especially important in quality, severely reduced but not absent brain perfusion patients with cranial trauma and serious facial lesions in and in some patients with haematomas and trauma. The whom neurological examination is difficult, as well as in significance of venous sinus visualization has been children in whom EEG silence and clinical signs of loss recently clarified in two papers (Lee et al, 1987; Laurin of brain functions are often equivocal. In these condi- et al, 1989). In addition, radionuclide perfusion scinti- tions the assessment of brain blood flow may constitute graphy only assesses hemispheric brain perfusion, with a decisive diagnostic criterion (Black & Zervas, 1984; poor visualization of the posterior fossa and brainstem. Pjura & Kim, 1987; Kaufman et al, 1989). Technetium-99m hexamethyl-propyleneamine oxime ( 99 Tc m -HMPAO) is a radiopharmaceutical that crosses the intact blood-brain barrier and is trapped by brain Address correspondence to: Dr J. M. Llamas-Elvira, Servicio tissue in proportion to regional perfusion. Uptake on de Medicina Nuclear, Hospital "Reina Sofia", Avda. static images reflects brain perfusion (Sharp et al, 1986; Menendez Pidal s/n, 14004 Cordoba, Spain. Neirinckx et al, 1987). Vol. 65, No. 772 289

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1992, The British Journal of Radiology, 65, 289-294
VOLUME 65 NUMBER 772 APRIL1992
The British Journal of Radiology
Diagnosis of brain death: superiority of perfusion studieswith 99Tcm-HMPAO over conventional radionuclide cerebralangiographyBy *A. de la Riva, F. M. Gonzalez, J. M. Llamas-Elvira, J. M. Latre, A. Jimenez-Heffernan,tE. Vidal, M- Martinez, M. Torres, tR. Guerrero, tF. Alvarez and A. Mateo
Departments of Nuclear Medicine, *Neurosurgery, tlnternal Medicine and Intensive Care, "Reina Sofia"Hospital, Avda. Menendez Pidal s/n, 14004 Cordoba, Spain
(Received 20 June 1991 and in revised form 23 September 1991, accepted 8 October 1991)
Keywords: "Tcm-HMPAO, Cerebral flow, Brain death
Abstract. The use of technetium-99m hexamethyl-propyleneamine oxime (99Tcm-HMPAO) in the diagnosis of brain death hasbeen evaluated in 41 studies of 37 patients with severe brain injury, who were under the effect of drugs or when other diagnosticmethods were equivocal. HMPAO studies were compared with conventional radionuclide angiography performed simultaneouslyby intravenous administration of HMPAO as a bolus. The ages of patients ranged from 4 months to 75 years. Dynamic flowimages and 5-min static uptake images were acquired following bolus injection of 555 Mbq of "Tcm-HMPAO. All patientsshowing no brain uptake were confirmed as brain-dead by standard clinical criteria, with no contradictory cases in the static study.In addition, all patients who were not brain-dead showed HMPAO uptake at least in the brainstem. Dynamic flow images wereequivocal in five patients, four of whom had no uptake on static images and clinically confirmed brain death. In addition, twoother cases showed "mismatched" dynamic and static images: in one case no perfusion was observed on flow images but uptakerestricted to the posterior fossa was seen on static images; the other case showed perfusion on the dynamic study and staticimaging revealed hemispheric uptake with no posterior fossa uptake. Static perfusion ^"cm-HMPAO studies offer advantages overconventional brain scintigraphy, better results being due to adequate assessment of posterior fossa activity and avoiding equivocalstudies.
Assessment of brain death has been increasing in impor- Contrast medium angiography of the brain is con-tance since the advent of organ transplantation. sidered to be the "gold standard" for brain perfusionAdvances in life-support systems and the increasing (Pjura & Kim, 1987), but is an expensive, invasive anddemand for organ donors need diagnostic methods that technically complex procedure that requires transpor-identify irreversible loss of brain function accurately and tation of the patient to an angiography facility andpromptly. positioning on the table with the risk of clinical deterio-
The diagnosis of brain death is difficult to establish in ration (Andrews et al, 1990).patients with artificial life-support systems, and is Radionuclide cerebral angiography has beenfurther hindered by the use of barbiturate-induced coma proposed as an alternative method for the evaluation ofand hypothermia for suppression of brain metabolic brain perfusion, showing a good correlation with four-activity. In these cases, electroencephalographic (EEG) vessel angiography (Kricheff et al, 1975; Korein et al,activity may be absent or markedly reduced and the 1977). Scintigraphy has been widely accepted, althoughonly reliable method of diagnosis is the absence of it has problems of interpretation in cases of poor bolusintracranial blood flow. This is especially important in quality, severely reduced but not absent brain perfusionpatients with cranial trauma and serious facial lesions in and in some patients with haematomas and trauma. Thewhom neurological examination is difficult, as well as in significance of venous sinus visualization has beenchildren in whom EEG silence and clinical signs of loss recently clarified in two papers (Lee et al, 1987; Laurinof brain functions are often equivocal. In these condi- et al, 1989). In addition, radionuclide perfusion scinti-tions the assessment of brain blood flow may constitute graphy only assesses hemispheric brain perfusion, witha decisive diagnostic criterion (Black & Zervas, 1984; poor visualization of the posterior fossa and brainstem.Pjura & Kim, 1987; Kaufman et al, 1989). Technetium-99m hexamethyl-propyleneamine oxime
(99Tcm-HMPAO) is a radiopharmaceutical that crossesthe intact blood-brain barrier and is trapped by brain
Address correspondence to: Dr J. M. Llamas-Elvira, Servicio tissue in proportion to regional perfusion. Uptake onde Medicina Nuclear, Hospital "Reina Sofia", Avda. static images reflects brain perfusion (Sharp et al, 1986;Menendez Pidal s/n, 14004 Cordoba, Spain. Neirinckx et al, 1987).
Vol. 65, No. 772 289

A. de la Riva et al
Few reports exist about the usefulness of"Tcm-HMPAO in the diagnosis of brain death (Roine etal, 1986; Galaske et al, 1988; Laurin et al, 1989; Reidet al, 1989). HMPAO brain uptake has been reported inpatients thought to be brain-dead on clinical groundsand who subsequently recovered (Reid et al, 1989). Weagree with George (1991) that further study is necessaryto determine the role these studies may play in diagnos-tic protocols for establishing brain death, especially inrelation to early diagnosis in organ donors inbarbiturate-induced coma, children and traumapatients.
The purpose of this paper is two-fold. First, we reviewour experience with "Tcm-HMPAO in the diagnosis ofbrain death, verifying its diagnostic usefulness and reli-ability in potential organ donors under the effects ofdrugs or when other diagnostic methods are equivocal.Secondly we compare these studies with conventionalradionuclide angiography performed simultaneouslythrough the intravenous administration of the radio-pharmaceutical as a bolus with registration of sequentialdynamic images of brain arterial perfusion.
Patients and methodsWe performed 41 brain flow studies with
"Tcm-HMPAO (dynamic phase and perfusion staticimaging) in 37 patients (24 men and 13 women) withacute and severe brain injury. Ages ranged from4 months to 75 years (mean 28.8 years). Patients wereadmitted to the hospital with the following conditions:multitrauma with head injury (20), head trauma (4),brain haemorrhage (7), and sepsis, encephalitis, cerebralinfarction, dehydration, myocardial infarction, andrenal failure in one case each. Table I shows age, sex,reason for admission to hospital and other clinicaldetails at the time of study.
Barbiturate coma was present at scintigraphy in 12patients. Five other patients were studied 24-48 hfollowing barbiturate withdrawal.
Scintigraphy was performed when brain death wasclinically suspected. When the study disclosed brainuptake of HMPAO or brain activity on dynamic imagesin patients with a deteriorating clinical state, the studywas repeated 24-48 h later. Standard clinical criteria forthe diagnosis of brain death were applied in casesshowing no brain uptake on scintigraphy except in thegroup of patients in barbiturate-induced coma. In thelatter, a 48-h interval after barbiturate withdrawal wasleft before the evaluation of standard clinical criteria.
Radiopharmaceutical preparation"Tcm-HMPAO was prepared by the addition of
2.5 ml of an eluate obtained from a recently eluatedMo/Tc generator (less than 6 h) with 1750 MBq activityto a Ceretec vial (code nlO9z, Amersham Internationalpic) with vortex mixing for 3 min. Quality controlensued and individual doses were prepared: 555 MBqfor adults and activity proportional to body surface inchildren with a minimum dose of 148 MBq.
Quality control was performed with column
chromatography to determine the proportion ofprimary complex following the method validated byMah et al (1989). Preparations with less than 85% ofprimary complex were rejected following the criteria ofimage quality reported by Ballinger et al (1990).
Doses were injected intravenously as a bolus using themost central venous line available. All doses wereinjected within 10 min of preparation.
Study acquisitionScintigraphy was performed with the patient supine,
including head and neck (or part of it) in the gammacamera's field of view. A stationary Siemens ZLC-37gamma camera was used, and all patients were studiedin the Nuclear Medicine facility. Rapid-sequence angio-graphic images with no scalp compression were acquiredand registered on a 64 x 64 computer data matrix at 1 simages during 60 s. Simultaneously, 20 analogic imageswere obtained on radiographic film at 2 s per image.Five minutes later static brain images were obtained.Three planar static images (anterior and both laterals)were obtained on film at a minimum of 500 Kcountsand registered on a 128 x 128 matrix. Special care wastaken to obtain good visualization of the posterior fossaon both lateral views.
Image evaluationAngiographic images were carefully screened for
activity in the principal cranial arteries. In cases of poorbolus quality, tracer extravasation or faint hemisphericactivity, the study was interpreted as equivocal. Absenceof HMPAO uptake in hemispheres and posterior fossaon static images was interpreted as consistent with braindeath. Visualization of activity in saggital or transversesinuses was not taken into account.
A nuclear medicine physician retrospectively re-evaluated all studies, and no changes in interpretationresulted.
Standard brain death criteriaCriteria for the diagnosis of brain death in this study
were as follows.
1. Previous criteria: known aetiology of loss of brainfunction, central temperature higher than 33°C, sys-temic arterial blood pressure higher than80/40 mmHg, no previous endogenous or exogenousintoxication, no previous administration of musclerelaxants.
2. Neurological criteria: profound coma and absence ofresponse to painful stimuli, muscular hypotonia,non-reactive and dilated pupils, abolition of brain-stem reflexes, unresponsiveness to the apnoea testdespite hypoxaemia and hypercarbia, absentresponse of the heart rate to atropine.
3. EEG criteria: isoelectric EEG tracing for a period of30 min despite stimulation.
4. Persistence criteria: persistence of all above criteria6 h after the first examination in adults and 12 h inchildren.
290 The British Journal of Radiology, April 1992
Superiority of "T^-HMPAO over conventional radionuclide angiography
Table I. Details of patients and findings
Case
1
2
3456789
10111213
14
15161718
19
2021
2223242526272829
29303132
33
333435
3536
36
37
Age
4 mon
20
453
21402228
1
3819468 mon
16
16372714
28
1917
5520441231235642
191149
61
7520
30
59
Sex
M
F
FFMFMMM
MMMF
M
MFFF
F
MF
FFMMMMMM
MMM
M
MM
M
F
Previous condition
Head trauma
Head trauma
Head traumaFever convulsionHead traumaPolytraumaPolytraumaEncephalitisPolytrauma
Brainstem haemorrhagePolytraumaPolytraumaDehydration
Polytrauma
Ventricular haemorrhagePolytraumaPolytraumaSubarachnoidhaemorrhagePolytrauma
PolytraumaPolytrauma
PolytraumaPolytraumaThalamic haemorrhageVentricular haemorrhagePolytraumaCardiac arrestPolytraumaPolytrauma
PolytraumaRenal failureIntracerebralhaemorrhageCerebeliar haemorrhage
PolytraumaPolytrauma
Polytrauma
Cerebeliar infarct
Additional dataat time of study
Pentobarbitalwithdrawn 48 h before
PentobarbitalPentobarbital
Pentobarbital
PentobarbitalPentobarbitalwithdrawn 24 h beforePentobarbitalwithdrawn 48 h before
Pentobarbitalwithdrawn 34 h beforePentobarbitalPentobarbitalwithdrawn 3 h before
Pentobarbital
Pentobarbital
Pentobarbital
AnisocoriaPentobarbital, fixedmidriasisPentobarbital,Pentobarbital,brainstem reflexesPentobarbitalwithdrawn 48 h beforeComa, spontaneousbreathing
Radionuclideangiography
Equivocal(poor bolus)Equivocal
Absent flowAbsent flowAbsent flowAbsent flowAbsent flowAbsent flowEquivocal(poor bolus)Absent flowEquivocalAbsent flowAbsent flow
Absent flow
Absent flowAbsent flowAbsent flow
Absent flowAbsent flow
Absent flowAbsent flow
Absent flowAbsent flowAbsent flowAbsent flowAbsent flowAbsent flowAbsent flowAbsent flow
Absent flowAbsent flowAbsent flow
Absent flowPresent flow
Absent flowPresent flowPresent flow
EquivocalPresent flow
Absent flow
Present flow
Static imaging
Absent uptake
Absent uptake
Absent uptakeAbsent uptakeAbsent uptakeAbsent uptakeAbsent uptakeAbsent uptakeAbsent uptake
Absent uptakeAbsent uptakeAbsent uptakeAbsent uptake
Absent uptake
Absent uptakeAbsent uptakeAbsent uptake
Absent uptakeAbsent uptake
Absent uptakeAbsent uptake
Absent uptakeAbsent uptakeAbsent uptakeAbsent uptakeAbsent uptakeAbsent uptakeAbsent uptake
Time interval betweenscan and clinicalbrain death diagnosis
48 h
24 h
48 h48 h48 h
48 h
48 h24 h
48 h
24 h
24 h
48 h48 h
48 h24 h
Absent hemispheric uptake, brainstemuptakeAbsent uptakeAbsent uptakeAbsent uptake
Absent uptake
48 h
Hemispheric uptake, absent brainstemuptakeAbsent uptakeUptakeUptake
Faint uptakeUptake
Absent uptake
Hemispheric uptake, absent uptake inipsilateral cerebeliar hemisphere
Vol. 65, No. 772 291
A. de la Riva et al
*
*•**>*"
(d)
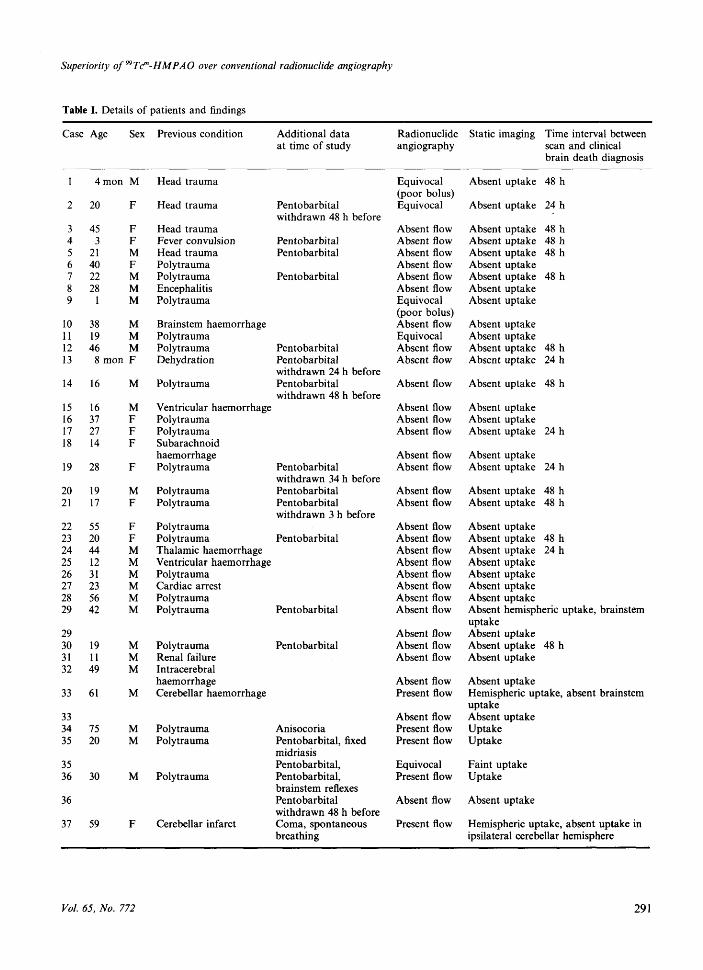
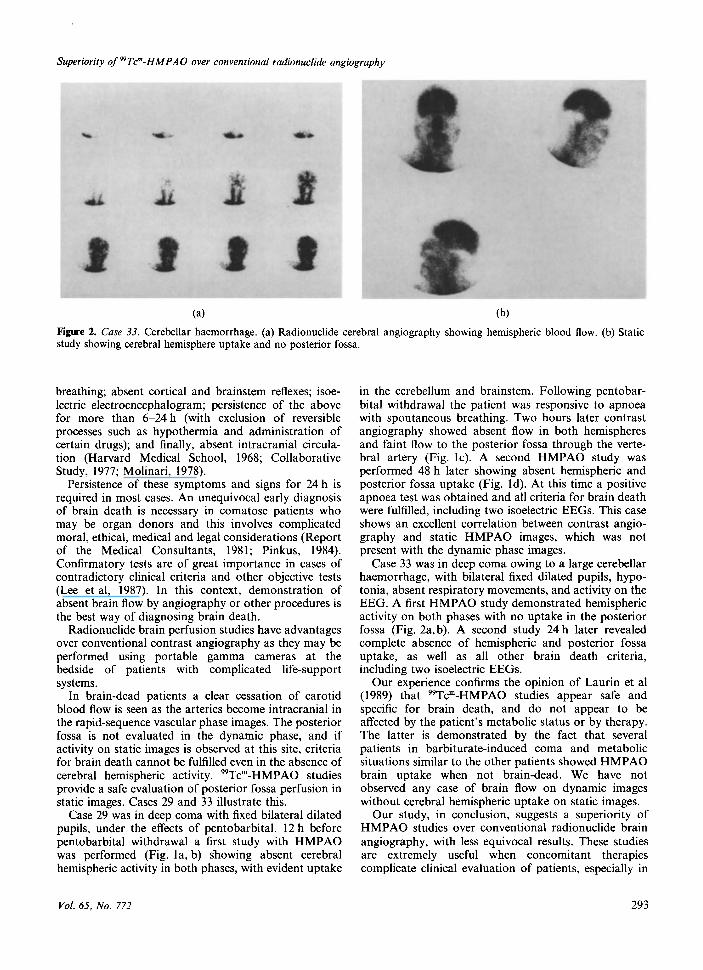
Figure 1. Case 29. (a, b) Absent hemispheric activity in both phases; uptake in cerebellum and brainstem (arrows), (c) Faint flow(arrow) through vessel dependent of vertebral artery, (d) 48 h later: no uptake in cerebral hemispheres and posterior fossa.
ResultsAll cases showing no brain HMPAO uptake were
confirmed by standard brain death criteria. In addition,in all patients who were not brain-dead, static imageswith HMPAO showed activity at least in the brainstem.
Equivocal dynamic flow images were seen in fivecases, two of which were due to poor bolus quality(Cases 1 and 9). The other three were inconclusivestudies (Cases 2, 11 and 35). On static images, four ofthese five patients (Cases 1, 2, 9 and 11) had absentbrain uptake and were clinically confirmed as brain-dead; the fifth patient (Case 35) showed faint hemi-spheric uptake on static images, precluding an inter-pretation of a positive study for brain death, and died24 h later.
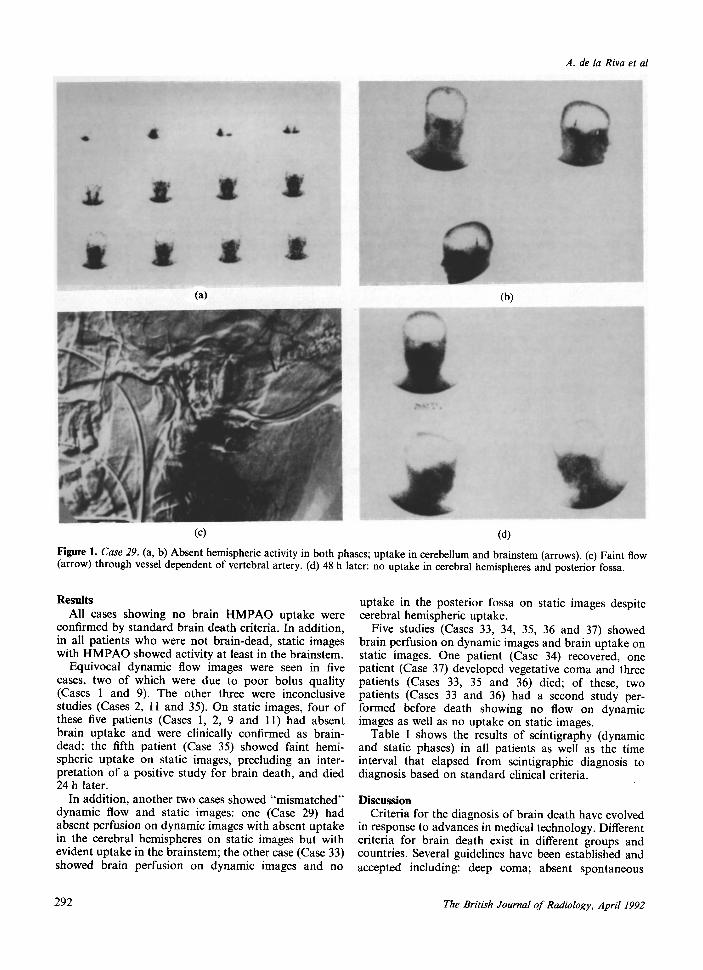
In addition, another two cases showed "mismatched"dynamic flow and static images: one (Case 29) hadabsent perfusion on dynamic images with absent uptakein the cerebral hemispheres on static images but withevident uptake in the brainstem; the other case (Case 33)showed brain perfusion on dynamic images and no
uptake in the posterior fossa on static images despitecerebral hemispheric uptake.
Five studies (Cases 33, 34, 35, 36 and 37) showedbrain perfusion on dynamic images and brain uptake onstatic images. One patient (Case 34) recovered, onepatient (Case 37) developed vegetative coma and threepatients (Cases 33, 35 and 36) died; of these, twopatients (Cases 33 and 36) had a second study per-formed before death showing no flow on dynamicimages as well as no uptake on static images.
Table I shows the results of scintigraphy (dynamicand static phases) in all patients as well as the timeinterval that elapsed from scintigraphic diagnosis todiagnosis based on standard clinical criteria.
DiscussionCriteria for the diagnosis of brain death have evolved
in response to advances in medical technology. Differentcriteria for brain death exist in different groups andcountries. Several guidelines have been established andaccepted including: deep coma; absent spontaneous
292 The British Journal of Radiology, April 1992
Superiority of"Tcm-HMPAO over conventional radionuclide angiography
•wm *w
(a) (b)
Figure 2. Case 33. Cerebellar haemorrhage, (a) Radionuclide cerebral angiography showing hemispheric blood flow, (b) Staticstudy showing cerebral hemisphere uptake and no posterior fossa.
breathing; absent cortical and brainstem reflexes; isoe-lectric electroencephalogram; persistence of the abovefor more than 6-24 h (with exclusion of reversibleprocesses such as hypothermia and administration ofcertain drugs); and finally, absent intracranial circula-tion (Harvard Medical School, 1968; CollaborativeStudy, 1977; Molinari, 1978).
Persistence of these symptoms and signs for 24 h isrequired in most cases. An unequivocal early diagnosisof brain death is necessary in comatose patients whomay be organ donors and this involves complicatedmoral, ethical, medical and legal considerations (Reportof the Medical Consultants, 1981; Pinkus, 1984).Confirmatory tests are of great importance in cases ofcontradictory clinical criteria and other objective tests(Lee et al, 1987). In this context, demonstration ofabsent brain flow by angiography or other procedures isthe best way of diagnosing brain death.
Radionuclide brain perfusion studies have advantagesover conventional contrast angiography as they may beperformed using portable gamma cameras at thebedside of patients with complicated life-supportsystems.
In brain-dead patients a clear cessation of carotidblood flow is seen as the arteries become intracranial inthe rapid-sequence vascular phase images. The posteriorfossa is not evaluated in the dynamic phase, and ifactivity on static images is observed at this site, criteriafor brain death cannot be fulfilled even in the absence ofcerebral hemispheric activity. "Tcm-HMPAO studiesprovide a safe evaluation of posterior fossa perfusion instatic images. Cases 29 and 33 illustrate this.
Case 29 was in deep coma with fixed bilateral dilatedpupils, under the effects of pentobarbital. 12 h beforepentobarbital withdrawal a first study with HMPAOwas performed (Fig. la, b) sliowing absent cerebralhemispheric activity in both phases, with evident uptake
in the cerebellum and brainstem. Following pentobar-bital withdrawal the patient was responsive to apnoeawith spontaneous breathing. Two hours later contrastangiography showed absent flow in both hemispheresand faint flow to the posterior fossa through the verte-bral artery (Fig. lc). A second HMPAO study wasperformed 48 h later showing absent hemispheric andposterior fossa uptake (Fig. Id). At this time a positiveapnoea test was obtained and all criteria for brain deathwere fulfilled, including two isoelectric EEGs. This caseshows an excellent correlation between contrast angio-graphy and static HMPAO images, which was notpresent with the dynamic phase images.
Case 33 was in deep coma owing to a large cerebellarhaemorrhage, with bilateral fixed dilated pupils, hypo-tonia, absent respiratory movements, and activity on theEEG. A first HMPAO study demonstrated hemisphericactivity on both phases with no uptake in the posteriorfossa (Fig. 2a, b). A second study 24 h later revealedcomplete absence of hemispheric and posterior fossauptake, as well as all other brain death criteria,including two isoelectric EEGs.
Our experience confirms the opinion of Laurin et al(1989) that "Tcm-HMPAO studies appear safe andspecific for brain death, and do not appear to beaffected by the patient's metabolic status or by therapy.The latter is demonstrated by the fact that severalpatients in barbiturate-induced coma and metabolicsituations similar to the other patients showed HMPAObrain uptake when not brain-dead. We have notobserved any case of brain flow on dynamic imageswithout cerebral hemispheric uptake on static images.
Our study, in conclusion, suggests a superiority ofHMPAO studies over conventional radionuclide brainangiography, with less equivocal results. These studiesare extremely useful when concomitant therapiescomplicate clinical evaluation of patients, especially in
Vol. 65, No. 772 293
A. de la Riva et al
potential organ donors in whom an early diagnosis maybe of vital importance.
ReferencesANDREWS, P. J. D., PIPER, I. R., DEARDEN, N. M. & MILLER,
J. D., 1990. Secondary insults during intrahospital transportof head-injured patients. Lancet, 335, 327-330.
BALLINGER, J. R., GULENCHYN, K. Y. & REID, R. H., 1990.Radiopharmaceutical factors in the variable quality of"Tcm-HMPAO images of the brain. Journal of NuclearMedicine, 31, 118-122.
BLACK, P . M C . L. & ZERVAS, N. T., 1984. Declaration of braindeath in neurosurgical and neurological practice.Neurosurgey, 15, 170-174.
COLLABORATIVE STUDY, 1977. An appraisal of the criteria ofcerebral death—a summary statement: a collaborative study.Journal of the American Medical Association, 237, 982-986.
GALASKE, R. G., SCHOBER, O. & HEYER, R., 1988."Tcm-HMPAO and 123I-amphetamine cerebral scintigraphy:a new, non-invasive method in determination of brain deathin children. European Journal of Nuclear Medicine, 14,446-452.
GEORGE, M. S., 1991. Establishing brain death: the potentialrole of nuclear medicine in the search for a reliableconfirmatory test. European Journal of Nuclear Medicine, 18,75-77.
HARVARD MEDICAL SCHOOL, 1968. Report of the ad hoccommittee for the Harvard Medical School to examine thedefinition for brain death. Journal of the American MedicalAssociation, 205, 337-340.
KAUFMAN, H. H., GEISLER, F. H., KOPITNIK, T., HIGGINS, W. &STEWART, D., 1989. Detection of brain death in barbituratecoma: the dilemma of an intracranial pulse. Neurosurgery,25, 275-278.
KOREIN, J., BRAUNSTEIN, P., GEORGE, A., WICHTER, M.,KRICHEFF, I., LIEBERMAN, A. & PEARSON, J., 1977. Braindeath: I. Angiographic correlation with the radioisotopicbolus technique for the evaluation of critical deficit ofcerebral blood flow. Annals of Neurology, 2, 195-205.
KRICHEFF, I. I., BRAUNSTEIN, P., KOREIN, J., GEORGE, A. E. &KUMAR, A. J., 1975. Isotopic and angiographicdetermination of cerebral blood flow. A correlation inpatients with cerebral death. Ada Radiologica (Suppl), 347,119-129.
LAURIN, N. R., DRIEDGER, A. A., HURWITZ, G. A., MATTAR,A. G., POWE, J. E., CHAMBERLAIN, M. J., ZABEL, P. L. &
PAVLOSKY, W. F., 1989. Cerebral perfusion imaging withtechnetium-99m HMPAO in brain death and severe centralnervous system injury. Journal of Nuclear Medicine, 30,1627-1635.
LEE, V. W., HAUCK, R. M., MORRISON, M. C , DENG, T. T.,FISHER, E. & CARTER, A., 1987. Scintigraphic evaluation ofbrain death; significance of sagittal sinus visualization.Journal of Nuclear Medicine, 28, 1279-1283.
MAH, G., REILLY, R. M., WONG, G. L. M. & HOULE, S., 1989.A comparison of three methods to determine theradiochemical purity of "Tcm-hexamethylpropylene amineoxime (99Tcm-HMPAO). Nuclear Medicine Communications,10, 733-740.
MOLINARI, G. F., 1978. Review of clinical criteria of braindeath. Annals of the New York Academy of Sciences, 315,62-69.
NEIRINCKX, R. D., CANNING, L. R., PIPER, I. M., NOWOTNIK,D. P., PICKETT, R. D., HOLMES, R. A., VOLKERT, W. A.,FORSTER, A. M., WEISNER, P. S., MARRIOTT, J. A. &CHAPLIN, S. B., 1987. Technetium-99m,c?,/-HMPAO: a newradiopharmaceutical for SPECT imaging of regional cerebralblood perfusion. Journal of Nuclear Medicine, 28, 191-202.
PINKUS, R. L., 1984. Families, brain death, and traditionalmedical excellence. Journal of Neurosurgery, 60, 1192-1194.
PJURA, G. A. & KIM, E. E., 1987. Radionuclide evaluation ofBrain death. In Nuclear Medicine Annual 1987, ed. by L. M.Freeman & H. S. Weissmann (Raven Press, New York),pp. 269-293.
REID, R. H., GULENCHYN, K. Y. & BALLINGER, J. R., 1989.Clinical use of technetium-99m HMPAO for determinationof brain death. Journal of Nuclear Medicine, 30, 1621-1626.
REPORT OF THE MEDICAL CONSULTANTS, 1981. Report on thediagnosis of death to the President's Commission for thestudy of ethical problems in medicine and biomedical andbehavioral research: guidelines for the determination ofdeath. Journal of the American Medical Association, 246,2184-2186.
ROINE, R. O., LAUNES, J., LINDROTH, L. & NIKKINEN, P., 1986."Tcm-Hexamethylpropyleneamine oxime scans to confirmbrain death. Lancet, ii, 1223-1224.
SHARP, P. F., SMITH, F. W., GEMMELL, H. G., LYALL, D.,EVANS, N. T. S., GVOZDANOVIC, D., DAVIDSON, J., TYRRELL,D. A., PICKETT, R. D. & NEIRINCKX, R. D., 1986.Technetium-99m HMPAO stereoisomers as potential agentsfor imaging regional blood flow: human volunteer studies.Journal of Nuclear Medicine, 27, 171-177.
294 The British Journal of Radiology, April 1992
Related Documents