Diabetic Foot BY PROF GOUDA ELLABBAN SCU HOSPITAL/ EGYPT

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Diabetic FootBY
PROF GOUDA ELLABBANSCU HOSPITAL/ EGYPT
What is the diabetic foot?
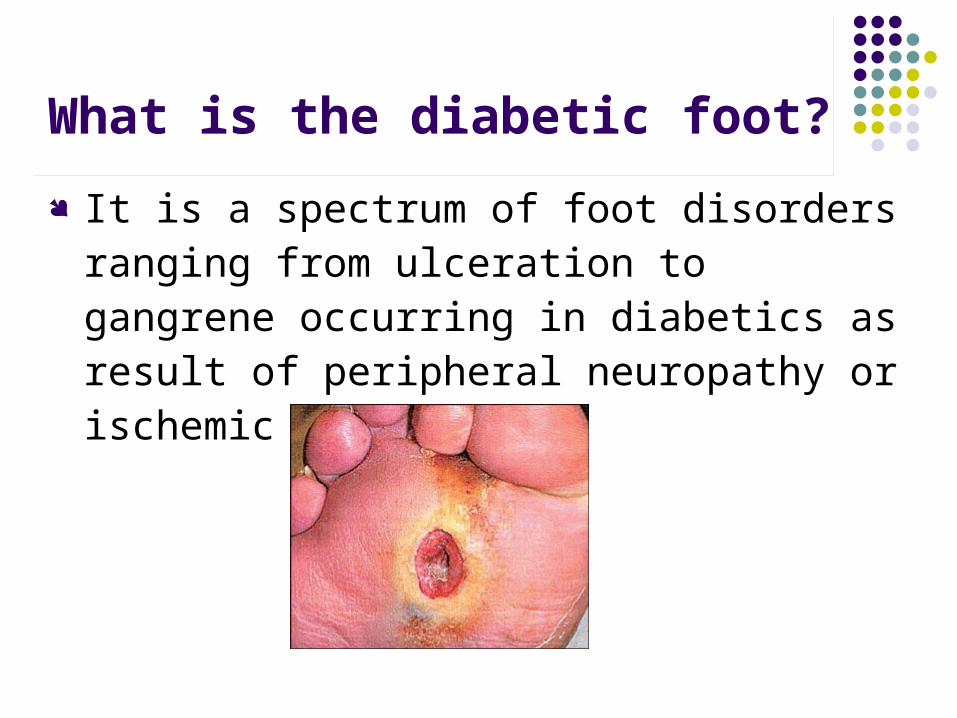
It is a spectrum of foot disorders ranging from ulceration to gangrene occurring in diabetics as result of peripheral neuropathy or ischemic or both.
Why is it important?
Because the foot is a frequent site for complications in patients with diabetes.
Tissue necrosis in the feet is a common reason for hospital admission in diabetic patients. Such admission tend to be prolonged and often end with amputation.
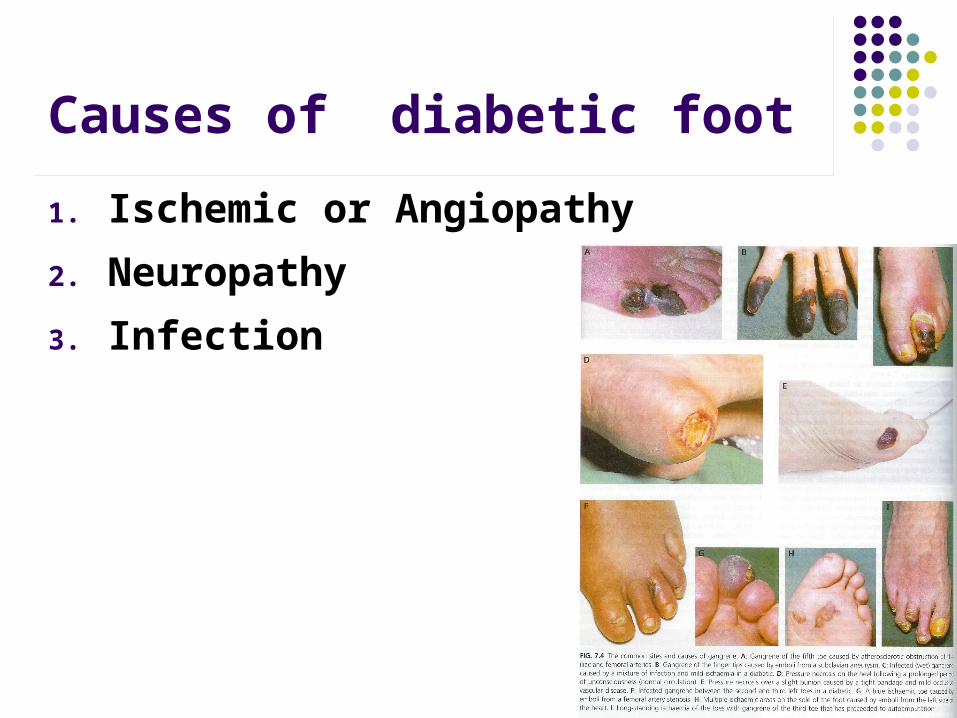
Causes of diabetic foot
1. Ischemic or Angiopathy
2. Neuropathy
3. Infection
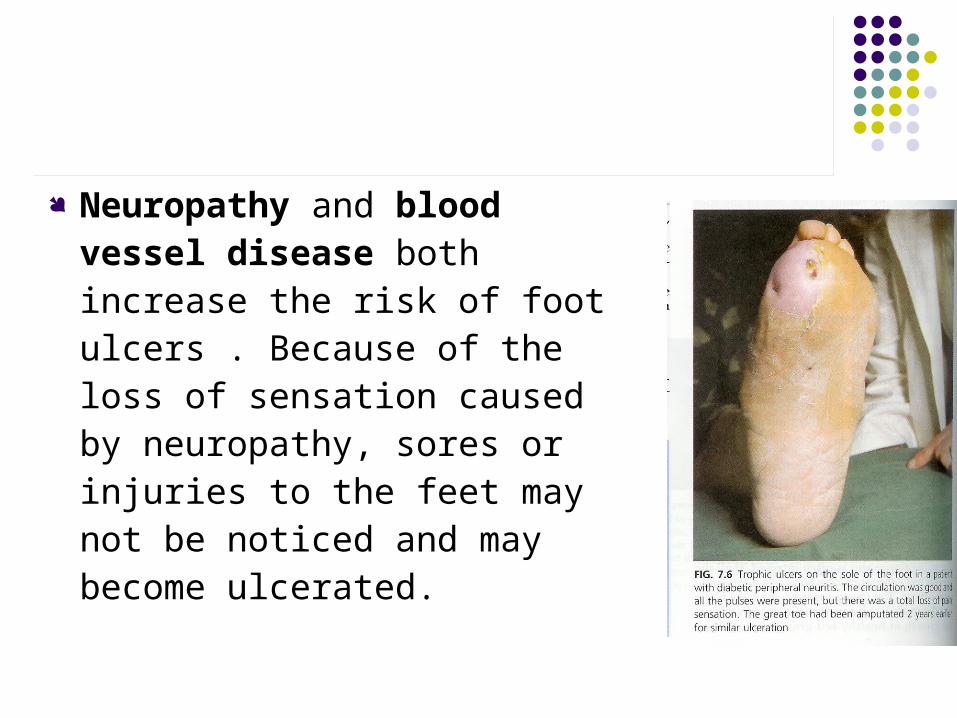
Neuropathy and blood vessel disease both increase the risk of foot ulcers . Because of the loss of sensation caused by neuropathy, sores or injuries to the feet may not be noticed and may become ulcerated.

Infection
such as cellulitis are caused by the same organisms as those in healthy hosts, namely group A streptococci and Staph aureus.
If the patient is hyperglycemic, this will be good media for polymicrobial infection.

Summary
Angiopathy ischemia ulcer or gangrene, if infected wet gangrene
Neuropathy Injury + loss of sensation ulcers and gangrene without noticing
Factors that interferes with Wound Healing Vascular [Atherosclerosis,Poor blood supply,
Microthrombi] Neurologic [loss of sensation] Infection [Inadequate
debridement,Hyperglycemia, Decreased neutrophil function, Polymicrobial infection, Immunosuppression ]
Mechanical [Edema, Weight bearing ] Poor nutrition
Clinical presentations of diabetic foot
Cellulitis
1. Erythema
2. Tenderness
3. Hot (warm)
4. Swelling of the foot (edema)
5. Fungal infection Hairless
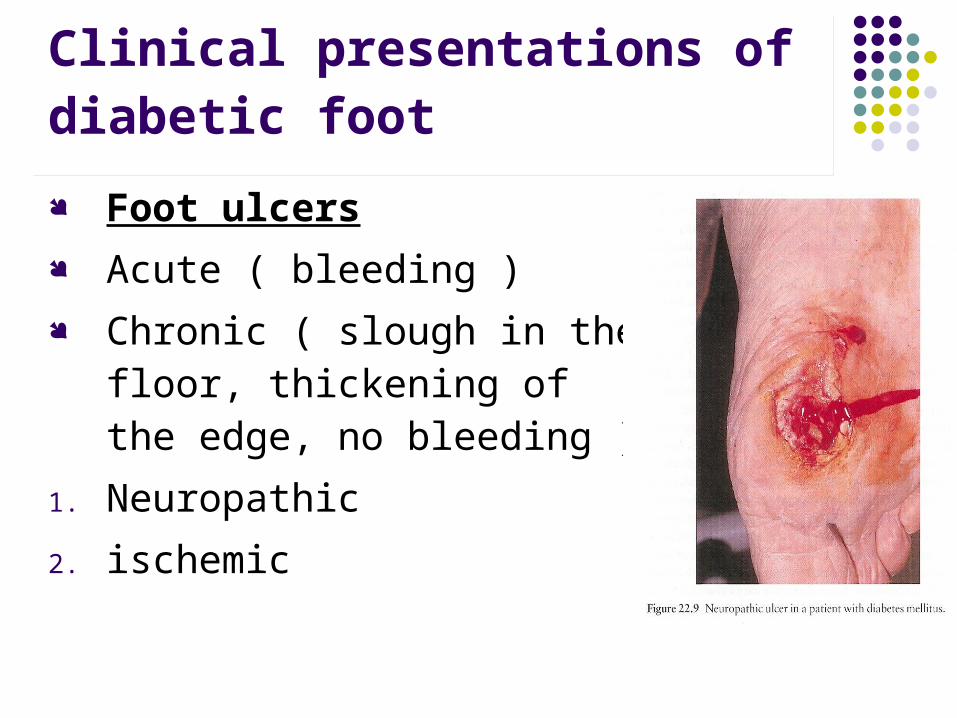
Clinical presentations of diabetic foot
Foot ulcers Acute ( bleeding ) Chronic ( slough in the floor,
thickening of the edge, no bleeding )
1. Neuropathic
2. ischemic
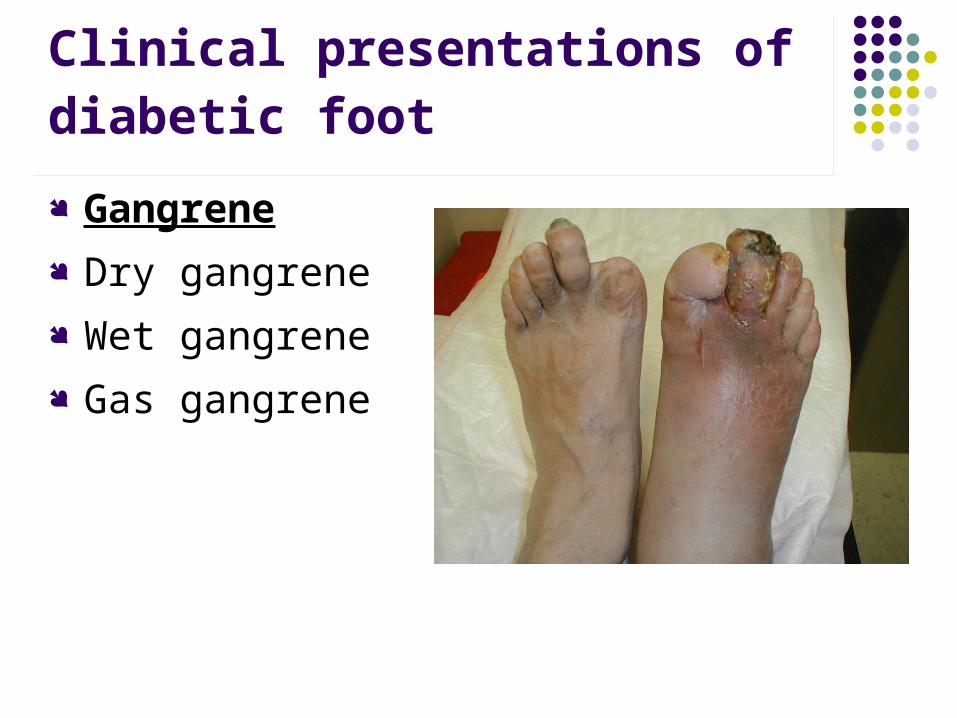
Clinical presentations of diabetic foot
Gangrene Dry gangrene Wet gangrene Gas gangrene
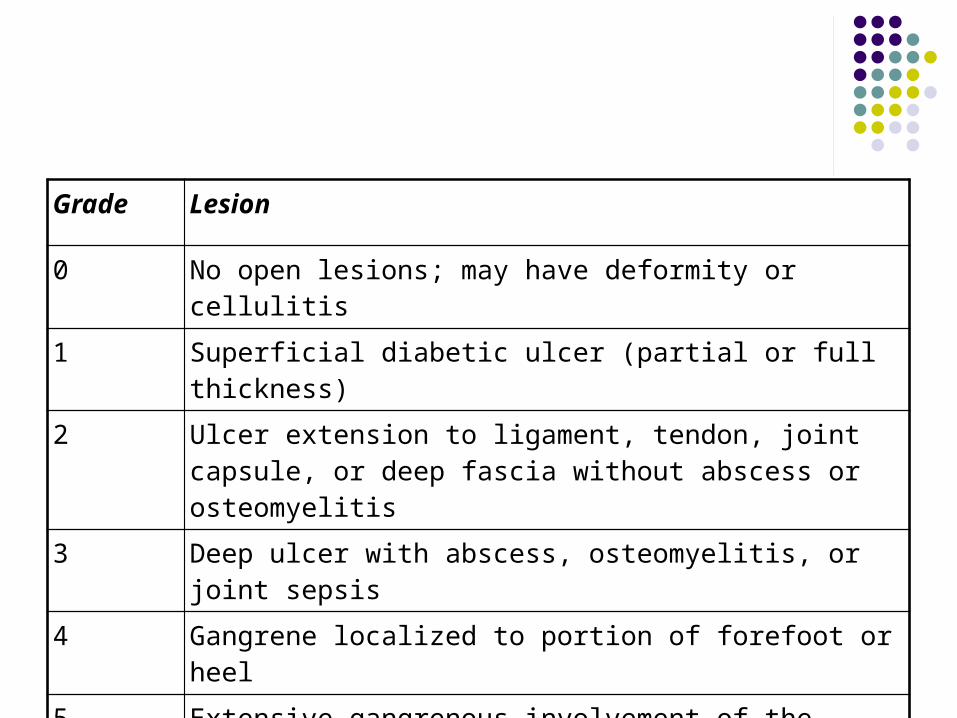
Grade Lesion
0 No open lesions; may have deformity or cellulitis
1 Superficial diabetic ulcer (partial or full thickness)
2 Ulcer extension to ligament, tendon, joint capsule, or deep fascia without abscess or osteomyelitis
3 Deep ulcer with abscess, osteomyelitis, or joint sepsis
4 Gangrene localized to portion of forefoot or heel
5 Extensive gangrenous involvement of the entire foot
Differential diagnosis:
1. Wet gangrene
2. Atherosclerosis
3. Arteritis
4. DVT with venous gangrene
5. Varicose veins
6. Venous ulcer
7. Malignant ulcer
8. Traumatic ulcer
Diagnosis
Evaluation on three levels: the patient, wound, and infection.
History and physical examination [ inspection, palpation]
Foot pulse, blood pressure Neurological examination

Investigation
Lab Studies:
1. CBC count
2. erythrocyte sedimentation rate (ESR
3. Blood culture
4. platelet count
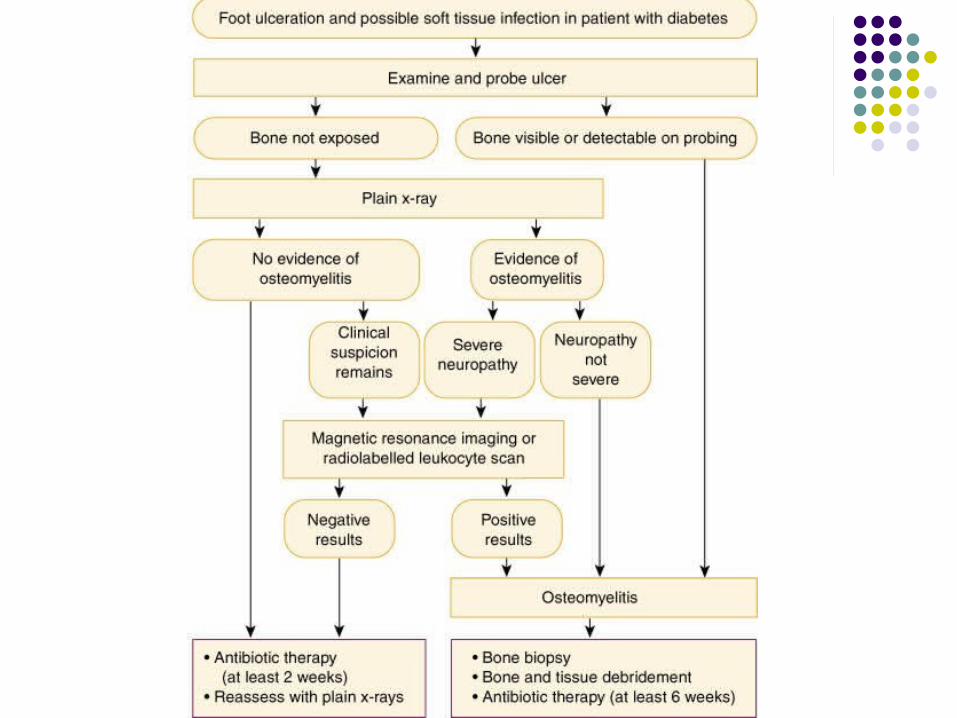
Imaging Studies:
1. plain radiography
2. CT scan for deep abscess, gas gangrene
3. MRI detection of osteomyelitis
4. Check blood vessels by Doppler ultrasound, angiography.
Investigation

Management of diabetic foot
Debridement [ to remove necrotic tissue ]
Treat infection [ampicillin, gentamycin, fungal]
Avoid weight-bearing Ensure good diabetic control Control edema Angiogram to assess feasibility of vascular
reconstruction where indicated
MAJOR OUTCOMES CONSIDERED
Severe morbidities Amputation Hospital length of stay Financial burden

Prevention begins with: Daily foot inspections (Look for redness,
cracks in skin, or sores.) Daily foot care (Dry completely between your
toes and use lotion to keep skin moist.) Regular visits to your physician Foot-care education Wearing proper shoes at all times (Do not go
barefoot.) Early treatment of any trouble areas.

People with diabetes should have a foot exam every year. Exams include:
1. Checking for sensation (feeling) in the feet
2. Looking at the foot for changes in shape and size
3. Checking blood flow and circulation
4. Looking for discoloration.
Prevention begins with:
Related Documents











