Circulation Cardiovascular Case Series 1110 Foreword Information about a real patient is presented in stages (bold- face type) to an expert clinician (Dr Ammash), who responds to the information, sharing his reasoning with the reader (reg- ular type). A discussion by the authors follows. A 21-year-old man with a history of Ebstein anom- aly and atrial fibrillation who had previously undergone tricuspid valve repair, pulmonary venous isolation, and the Cox maze III procedure was referred from an outside institution for the evaluation of an acute onset of left-sided upper- and lower-extremity weakness. The patient had initially presented 3 years earlier with abdominal pain and symptomatic palpitations. Physical examination at that time revealed a jugular venous pres- sure of 12 cm without a prominent V wave. Cardiac pal- pation noted a sternal heave. On auscultation, a grade II holosystolic murmur was appreciated at the left ster- nal border that increased with inspiration. Abdominal inspection noted an enlarged liver that was not pulsatile. A standard 12-lead ECG demonstrated sinus rhythm with first-degree atrioventricular block (Figure 1), and a chest x-ray noted enlargement of the right atrium (Figure 2). A 24-hour Holter monitor noted that the predominant rhythm was atrial fibrillation interrupted by brief periods of sinus rhythm. Transthoracic echocardiography demon- strated severe right atrial enlargement, dilatation of the tricuspid annulus, apical displacement of the tricuspid valve (displacement index, 10.2 mm/m 2 ), large anterior tricuspid valve leaflet, and severe tricuspid regurgitation consistent with Ebstein anomaly. Dr Ammash: Ebstein anomaly is a rare disorder account- ing for <1% of congenital cardiac abnormalities. 1 In patients with Ebstein anomaly, the most common presentation as an adult is an arrhythmia, 2 followed by heart failure secondary to tricuspid regurgitation and right ventricular dysfunction. Some patients also present with exercise intolerance or par- adoxical embolism. 3 The physical examination finding of a holosystolic murmur increasing with inspiration is consis- tent with tricuspid regurgitation. The murmur may be soft in the setting of severe tricuspid regurgitation owing to the equalization of pressures between the right ventricle and the right atrium. A V wave may be absent despite severe tri- cuspid regurgitation, because the markedly enlarged right atrium in patients with Ebstein anomaly readily absorbs the regurgitant volume. Similarly, hepatomegaly may be present owing to right ventricular failure, but a pulsatile liver may be absent given the ability of the right atrium to accommodate the regurgitant volume rather than deflecting it throughout the venous circulation. In the current case, the patient’s abdominal pain is likely secondary to underling congestive hepatopathy. The ECG is often abnormal in patients with Ebstein anomaly with typical findings including right bundle-branch block, right atrial enlargement, or decreased amplitude of the R waves in V1 and V2. 4 The presence of first-degree atrioventricular block, as noted in this case, is quite com- mon and has been documented in up to 42% of patients with Ebstein anomaly. 4 The apical displacement of the tricuspid valve compromises the continuity of the central fibrous body and septal atrioventricular ring, allowing for direct muscu- lar connections between the atrium and ventricle and result- ing in the subsequent development of accessory pathways. 5,6 Given that ≤36% of patients with Ebstein anomaly develop accessory pathways, the clinician should carefully review the ECG for associated clues such as a short PR interval, slurred upstroke of the QRS complex or delta wave, and a widened QRS. 7 The patient’s chest x-ray imaging indicates right atrial enlargement prompting the need for further structural evalua- tion of the heart. In Ebstein anomaly, the pulmonary vascularity may be decreased on chest x-ray imaging given the decreased forward flow from the right ventricle. Furthermore, marked cardiac enlargement, particularly a cardiothoracic ratio >0.65, in this patient population portends worse outcomes. 7 (Circulation. 2015;131:1110-1118. DOI: 10.1161/CIRCULATIONAHA.115.015340.) © 2015 American Heart Association, Inc. Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.115.015340 From Division of Cardiovascular Diseases, Department of Internal Medicine, Mayo Clinic, Rochester, MN. Correspondence to Naser M. Ammash, MD, Division of Cardiovascular Diseases, Department of Medicine, Mayo Clinic College of Medicine, 200 First St SW, Rochester, MN 55905. E-mail [email protected] Development of Left Atrial Thrombus and Subsequent Cardioembolic Stroke in a 21-Year-Old Man With Ebstein Anomaly Who Previously Underwent Pulmonary Vein Isolation Ablation and Cox Maze III Procedure Significance of Left Atrial Mechanical Function John P. Bois, MD; Grace Lin, MD; Peter A. Brady, MB, ChB, MD; Naser M. Ammash, MD by guest on May 2, 2016 http://circ.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Circulation Cardiovascular Case Series
1110
ForewordInformation about a real patient is presented in stages (bold-face type) to an expert clinician (Dr Ammash), who responds to the information, sharing his reasoning with the reader (reg-ular type). A discussion by the authors follows.
A 21-year-old man with a history of Ebstein anom-aly and atrial fibrillation who had previously
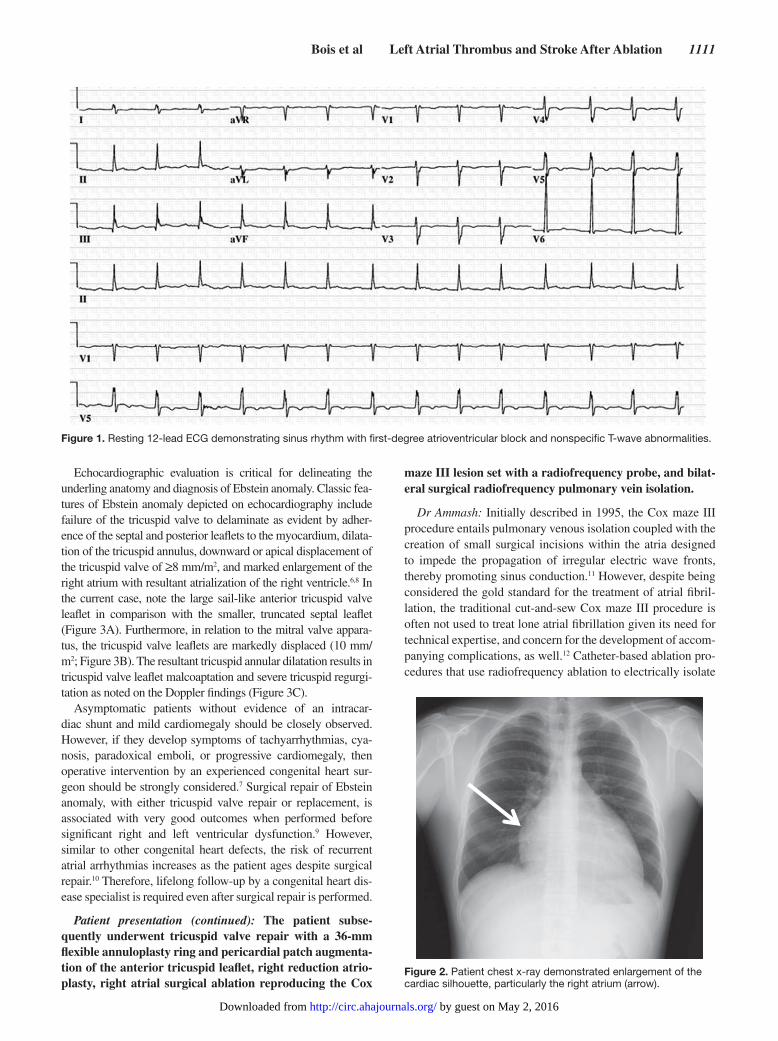
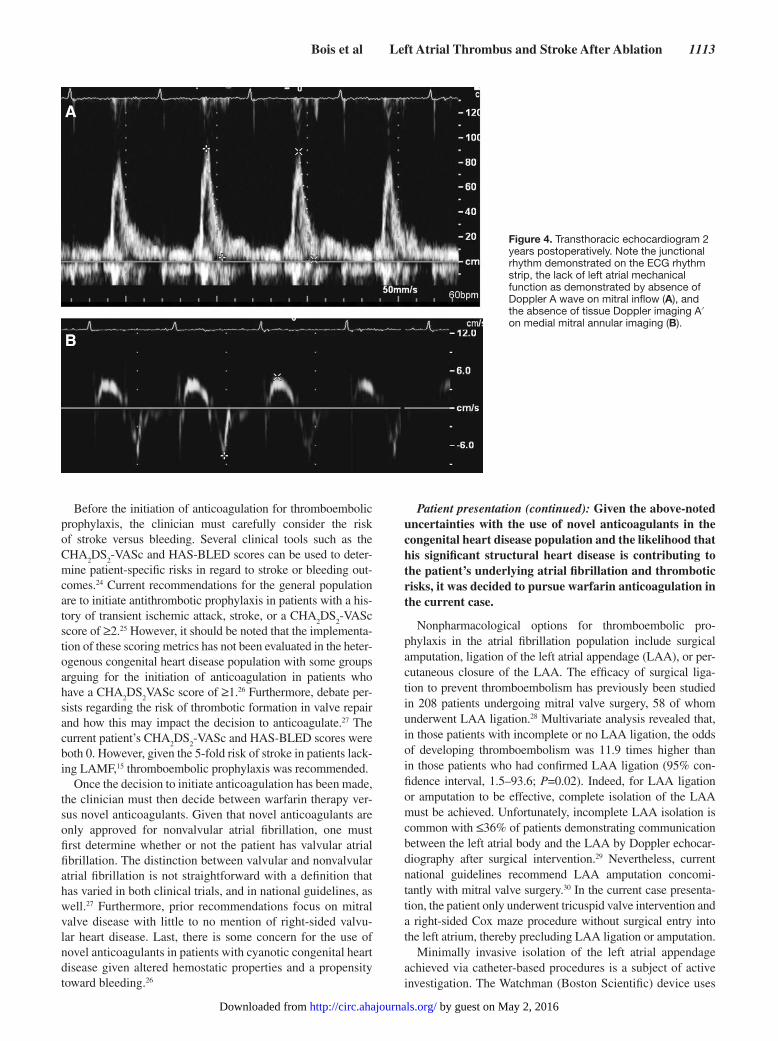
undergone tricuspid valve repair, pulmonary venous isolation, and the Cox maze III procedure was referred from an outside institution for the evaluation of an acute onset of left-sided upper- and lower-extremity weakness. The patient had initially presented 3 years earlier with abdominal pain and symptomatic palpitations. Physical examination at that time revealed a jugular venous pres-sure of 12 cm without a prominent V wave. Cardiac pal-pation noted a sternal heave. On auscultation, a grade II holosystolic murmur was appreciated at the left ster-nal border that increased with inspiration. Abdominal inspection noted an enlarged liver that was not pulsatile. A standard 12-lead ECG demonstrated sinus rhythm with first-degree atrioventricular block (Figure 1), and a chest x-ray noted enlargement of the right atrium (Figure 2). A 24-hour Holter monitor noted that the predominant rhythm was atrial fibrillation interrupted by brief periods of sinus rhythm. Transthoracic echocardiography demon-strated severe right atrial enlargement, dilatation of the tricuspid annulus, apical displacement of the tricuspid valve (displacement index, 10.2 mm/m2), large anterior tricuspid valve leaflet, and severe tricuspid regurgitation consistent with Ebstein anomaly.
Dr Ammash: Ebstein anomaly is a rare disorder account-ing for <1% of congenital cardiac abnormalities.1 In patients with Ebstein anomaly, the most common presentation as an adult is an arrhythmia,2 followed by heart failure secondary to tricuspid regurgitation and right ventricular dysfunction. Some patients also present with exercise intolerance or par-adoxical embolism.3 The physical examination finding of a
holosystolic murmur increasing with inspiration is consis-tent with tricuspid regurgitation. The murmur may be soft in the setting of severe tricuspid regurgitation owing to the equalization of pressures between the right ventricle and the right atrium. A V wave may be absent despite severe tri-cuspid regurgitation, because the markedly enlarged right atrium in patients with Ebstein anomaly readily absorbs the regurgitant volume. Similarly, hepatomegaly may be present owing to right ventricular failure, but a pulsatile liver may be absent given the ability of the right atrium to accommodate the regurgitant volume rather than deflecting it throughout the venous circulation. In the current case, the patient’s abdominal pain is likely secondary to underling congestive hepatopathy.
The ECG is often abnormal in patients with Ebstein anomaly with typical findings including right bundle-branch block, right atrial enlargement, or decreased amplitude of the R waves in V1 and V2.4 The presence of first-degree atrioventricular block, as noted in this case, is quite com-mon and has been documented in up to 42% of patients with Ebstein anomaly.4 The apical displacement of the tricuspid valve compromises the continuity of the central fibrous body and septal atrioventricular ring, allowing for direct muscu-lar connections between the atrium and ventricle and result-ing in the subsequent development of accessory pathways.5,6 Given that ≤36% of patients with Ebstein anomaly develop accessory pathways, the clinician should carefully review the ECG for associated clues such as a short PR interval, slurred upstroke of the QRS complex or delta wave, and a widened QRS.7
The patient’s chest x-ray imaging indicates right atrial enlargement prompting the need for further structural evalua-tion of the heart. In Ebstein anomaly, the pulmonary vascularity may be decreased on chest x-ray imaging given the decreased forward flow from the right ventricle. Furthermore, marked cardiac enlargement, particularly a cardiothoracic ratio >0.65, in this patient population portends worse outcomes.7
(Circulation. 2015;131:1110-1118. DOI: 10.1161/CIRCULATIONAHA.115.015340.)© 2015 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.115.015340
From Division of Cardiovascular Diseases, Department of Internal Medicine, Mayo Clinic, Rochester, MN.Correspondence to Naser M. Ammash, MD, Division of Cardiovascular Diseases, Department of Medicine, Mayo Clinic College of Medicine, 200 First
St SW, Rochester, MN 55905. E-mail [email protected]
Development of Left Atrial Thrombus and Subsequent Cardioembolic Stroke in a 21-Year-Old Man With
Ebstein Anomaly Who Previously Underwent Pulmonary Vein Isolation Ablation and Cox Maze III Procedure
Significance of Left Atrial Mechanical Function
John P. Bois, MD; Grace Lin, MD; Peter A. Brady, MB, ChB, MD; Naser M. Ammash, MD
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from
Bois et al Left Atrial Thrombus and Stroke After Ablation 1111
Echocardiographic evaluation is critical for delineating the underling anatomy and diagnosis of Ebstein anomaly. Classic fea-tures of Ebstein anomaly depicted on echocardiography include failure of the tricuspid valve to delaminate as evident by adher-ence of the septal and posterior leaflets to the myocardium, dilata-tion of the tricuspid annulus, downward or apical displacement of the tricuspid valve of ≥8 mm/m2, and marked enlargement of the right atrium with resultant atrialization of the right ventricle.6,8 In the current case, note the large sail-like anterior tricuspid valve leaflet in comparison with the smaller, truncated septal leaflet (Figure 3A). Furthermore, in relation to the mitral valve appara-tus, the tricuspid valve leaflets are markedly displaced (10 mm/m2; Figure 3B). The resultant tricuspid annular dilatation results in tricuspid valve leaflet malcoaptation and severe tricuspid regurgi-tation as noted on the Doppler findings (Figure 3C).
Asymptomatic patients without evidence of an intracar-diac shunt and mild cardiomegaly should be closely observed. However, if they develop symptoms of tachyarrhythmias, cya-nosis, paradoxical emboli, or progressive cardiomegaly, then operative intervention by an experienced congenital heart sur-geon should be strongly considered.7 Surgical repair of Ebstein anomaly, with either tricuspid valve repair or replacement, is associated with very good outcomes when performed before significant right and left ventricular dysfunction.9 However, similar to other congenital heart defects, the risk of recurrent atrial arrhythmias increases as the patient ages despite surgical repair.10 Therefore, lifelong follow-up by a congenital heart dis-ease specialist is required even after surgical repair is performed.
Patient presentation (continued): The patient subse-quently underwent tricuspid valve repair with a 36-mm flexible annuloplasty ring and pericardial patch augmenta-tion of the anterior tricuspid leaflet, right reduction atrio-plasty, right atrial surgical ablation reproducing the Cox
maze III lesion set with a radiofrequency probe, and bilat-eral surgical radiofrequency pulmonary vein isolation.
Dr Ammash: Initially described in 1995, the Cox maze III procedure entails pulmonary venous isolation coupled with the creation of small surgical incisions within the atria designed to impede the propagation of irregular electric wave fronts, thereby promoting sinus conduction.11 However, despite being considered the gold standard for the treatment of atrial fibril-lation, the traditional cut-and-sew Cox maze III procedure is often not used to treat lone atrial fibrillation given its need for technical expertise, and concern for the development of accom-panying complications, as well.12 Catheter-based ablation pro-cedures that use radiofrequency ablation to electrically isolate
Figure 1. Resting 12-lead ECG demonstrating sinus rhythm with first-degree atrioventricular block and nonspecific T-wave abnormalities.
Figure 2. Patient chest x-ray demonstrated enlargement of the cardiac silhouette, particularly the right atrium (arrow).
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from

1112 Circulation March 24, 2015
the pulmonary veins, and to target foci of electric irregularity, as well, that are identified during electroanatomic mapping have arisen as a minimally invasive alternative to the traditional surgical approach.13 Comparative effectiveness between these 2 treatment modalities has been studied recently at our institu-tion.12 In this investigation, 97 patients who underwent a cut-and-sew Cox maze procedure were compared with 194 age, sex, and atrial fibrillation type–matched patients who received catheter-based ablation. Eighty-seven percent of patients receiving Cox maze treatment were free from recurrent atrial fibrillation at 5 years in comparison with 28% of patients in the catheter ablation group (P<0.001). The postoperative need for pacemaker implantation was similar between the Cox maze and the catheter ablation group (9.3% versus 7.3%, P=0.55). Ten percent of patients in the catheter ablation cohort experi-enced pulmonary vein stenosis of ≥50%. One cerebral vascular accident (0.01%) and 1 nonfatal myocardial infarction (0.01%) were reported in patients who underwent the Cox maze proce-dure, whereas no deaths occurred in either group.
Although patients with Ebstein anomaly may demonstrate decreased atrial arrhythmias following surgical repair of the tricuspid valve and right atrial reduction atrioplasty, our prac-tice is to perform a concomitant right-sided Cox maze proce-dure that further reduces the arrhythmogenic burden.14 A prior report at our institution by Porter et al15 reviewed 70 cases of patients with Ebstein anomaly and atrial fibrillation. Twenty-two of these patients were evaluated before the advent of either the Cox maze procedure or cryoablation and therefore did not have any operative intervention for treatment of atrial fibrilla-tion. Fourteen of these patients had long-term follow-up with 6 (43%) of these experiencing recurrent atrial fibrillation. Of the 48 patients who underwent either the Cox maze procedure or cryoablation at the time of surgical repair, 25.6% had recur-rent atrial fibrillation during long-term follow-up. There was no statistical difference between the 2 operative techniques in regard to the rate of atrial fibrillation recurrence. None of these patients underwent catheter-based ablation because it is not routinely implemented at our institution owing to its decreased efficacy in the Ebstein anomaly population.14
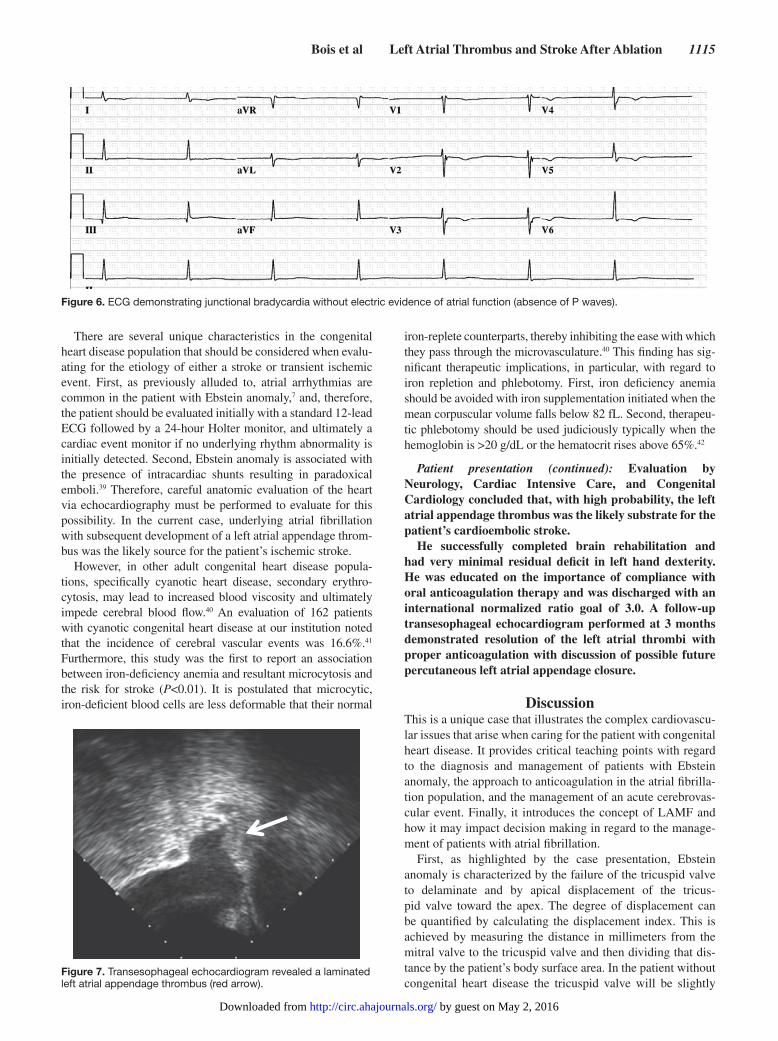
Patient presentation (continued): Two years postopera-tively, transthoracic echocardiography noted junctional rhythm with no evidence of left atrial mechanical function
(LAMF), defined as the absence of both Doppler A wave on mitral inflow and tissue Doppler imaging A′ on medial mitral annular imaging, and the lack of left atrial ejection, as well (documented as the percent of reduction in the left atrial area during diastole). These echocardiogram find-ings from the patient are demonstrated in Figure 4. The absence of LAMF indicated an increased risk of develop-ing a left atrial thrombus. Therefore, continued oral anti-coagulation with warfarin was recommended.
Dr Ammash: Although surgical intervention for atrial arrhyth-mias, such as cryoablation or pulmonary venous isolation, is often successful in restoring sinus rhythm and is associated with greater freedom from recurrent atrial fibrillation, previous stud-ies have suggested that surgical ablation may adversely affect LAMF. An investigation of 150 patients who underwent either radiofrequency or cryoablation maze procedures revealed that, at a mean follow-up of 24.5 months, 47 (31%) patients lacked LAMF.16 Moreover, lack of LAMF was associated with a 5-fold increase in the risk of stroke (P=0.02).16 The absence of LAMF after the Cox maze III procedure is as high as 39%17 and has been demonstrated to persist up to 56 months.18 Moreover, the specific type of surgical intervention used may impact the degree of postoperative LAMF. For instance, a recent study of 126 patients with atrial fibrillation who underwent surgical intervention demonstrated that the cut-and-sew Cox maze III procedure and cryoablation lead to a greater decrease in postop-erative LAMF than radiofrequency ablation.19 Therefore, given the high incidence of the absence of LAMF after the Cox maze procedure, and its associated risk of stroke, as well, the authors recommend investigation of LAMF after surgical intervention as part of the clinical decision-making process regarding throm-boembolic prophylaxis administration.
Although physiological pacing (AAI or DDD pacing set-tings) has proven to reduce the development of atrial fibrilla-tion,20,21 its effect on atrial mechanical function is less certain. Belham and colleagues22 demonstrated that, regardless of the location of pacing in the right atrium, pacing itself was det-rimental to atrial electromechanical function in comparison with sinus rhythm. However, Quintana et al23 demonstrated that short-term atrial pacing improved LAMF. Whether this benefit persists after pacing or whether long-term pacing may have similar effects remains unknown.
A B C
Figure 3. Transthoracic echocardiogram at the time of presentation demonstrating apical 4-chamber view depicting the right atrium (RA), right ventricle (RV), left atrium (LA), and left ventricle (LV). A, A sail-like anterior leaflet typical of Ebstein anomaly was noted (arrows). B, Marked apical displacement of the tricuspid valve in relation to the mitral valve was evident (red line between calipers). C, Doppler interrogation noted severe tricuspid regurgitation.
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from
Bois et al Left Atrial Thrombus and Stroke After Ablation 1113
Before the initiation of anticoagulation for thromboembolic prophylaxis, the clinician must carefully consider the risk of stroke versus bleeding. Several clinical tools such as the CHA
2DS
2-VASc and HAS-BLED scores can be used to deter-
mine patient-specific risks in regard to stroke or bleeding out-comes.24 Current recommendations for the general population are to initiate antithrombotic prophylaxis in patients with a his-tory of transient ischemic attack, stroke, or a CHA
2DS
2-VASc
score of ≥2.25 However, it should be noted that the implementa-tion of these scoring metrics has not been evaluated in the heter-ogenous congenital heart disease population with some groups arguing for the initiation of anticoagulation in patients who have a CHA
2DS
2VASc score of ≥1.26 Furthermore, debate per-
sists regarding the risk of thrombotic formation in valve repair and how this may impact the decision to anticoagulate.27 The current patient’s CHA
2DS
2-VASc and HAS-BLED scores were
both 0. However, given the 5-fold risk of stroke in patients lack-ing LAMF,15 thromboembolic prophylaxis was recommended.
Once the decision to initiate anticoagulation has been made, the clinician must then decide between warfarin therapy ver-sus novel anticoagulants. Given that novel anticoagulants are only approved for nonvalvular atrial fibrillation, one must first determine whether or not the patient has valvular atrial fibrillation. The distinction between valvular and nonvalvular atrial fibrillation is not straightforward with a definition that has varied in both clinical trials, and in national guidelines, as well.27 Furthermore, prior recommendations focus on mitral valve disease with little to no mention of right-sided valvu-lar heart disease. Last, there is some concern for the use of novel anticoagulants in patients with cyanotic congenital heart disease given altered hemostatic properties and a propensity toward bleeding.26
Patient presentation (continued): Given the above-noted uncertainties with the use of novel anticoagulants in the congenital heart disease population and the likelihood that his significant structural heart disease is contributing to the patient’s underlying atrial fibrillation and thrombotic risks, it was decided to pursue warfarin anticoagulation in the current case.
Nonpharmacological options for thromboembolic pro-phylaxis in the atrial fibrillation population include surgical amputation, ligation of the left atrial appendage (LAA), or per-cutaneous closure of the LAA. The efficacy of surgical liga-tion to prevent thromboembolism has previously been studied in 208 patients undergoing mitral valve surgery, 58 of whom underwent LAA ligation.28 Multivariate analysis revealed that, in those patients with incomplete or no LAA ligation, the odds of developing thromboembolism was 11.9 times higher than in those patients who had confirmed LAA ligation (95% con-fidence interval, 1.5–93.6; P=0.02). Indeed, for LAA ligation or amputation to be effective, complete isolation of the LAA must be achieved. Unfortunately, incomplete LAA isolation is common with ≤36% of patients demonstrating communication between the left atrial body and the LAA by Doppler echocar-diography after surgical intervention.29 Nevertheless, current national guidelines recommend LAA amputation concomi-tantly with mitral valve surgery.30 In the current case presenta-tion, the patient only underwent tricuspid valve intervention and a right-sided Cox maze procedure without surgical entry into the left atrium, thereby precluding LAA ligation or amputation.
Minimally invasive isolation of the left atrial appendage achieved via catheter-based procedures is a subject of active investigation. The Watchman (Boston Scientific) device uses
Figure 4. Transthoracic echocardiogram 2 years postoperatively. Note the junctional rhythm demonstrated on the ECG rhythm strip, the lack of left atrial mechanical function as demonstrated by absence of Doppler A wave on mitral inflow (A), and the absence of tissue Doppler imaging A′ on medial mitral annular imaging (B).
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from

1114 Circulation March 24, 2015
a nitinol cage coated with polyethylene terephthalate that expands once deployed in the LAA. In the Watchman Left Atrial Appendage System for Embolic Protection in Patients With Atrial Fibrillation (PROTECT AF) noninferiority study, the efficacy of the Watchman device to prevent thromboem-bolic events was compared with traditional warfarin therapy in patients with nonvalvular atrial fibrillation.31 Noninferiority was proven during this trial, but several complications with Watchman implantation were also noted, including pericardial effusions requiring pericardiocentesis. Other percutaneous LAA closure or isolation devices currently under investigation include the Amplatzer Cardiac plug (St. Jude Medical)32 and the LARIAT system (SentreHeart, Inc).33 Until further trials are performed, the use of these devices is currently relegated to those patients with an elevated thromboembolic risk and contraindications to traditional oral anticoagulation therapy. The patient in the current case presentation had no appar-ent contraindications to warfarin therapy, and, therefore, this option was chosen for thromboembolic prophylaxis.
Patient presentation (continued): Six months after his last follow-up the patient presented to an outside institution with acute onset of left-sided upper- and lower-extremity weak-ness and recurrent falls toward his left side. He indicated that a week before his presentation, he had been noncompli-ant with his warfarin therapy and had a documented sub-therapeutic international normalized ratio of 1.09.
An emergent head MRI demonstrated an acute isch-emic stroke in the right middle cerebral artery (Figure 5). Thrombolysis was administered, but repeat cerebral angiogram demonstrated persistent occlusion of the right middle cerebral artery. Consequently, a mechani-cal thrombectomy was successfully performed. Follow-up imaging noted a residual stroke in the deep right middle cerebral artery territory.
Dr Ammash: A pooled meta-analysis has demonstrated a marked improvement in morbidity with early administration of alteplase defined as within 4.5 hours from the onset of stroke symptoms.34 Indeed, the beneficial effect of thrombolytics correlates with the promptness of administration with a 2.55 reduction in morbidity if given within the first 90 minutes of presentation and falling to a 1.22 decline in morbidity if used after 4 hours.34 Before the administration of thrombolytic ther-apy, the clinician must ensure that there are no absolute con-traindications to its use including intracranial neoplasm, prior hemorrhagic stroke, or prior ischemic stroke within the past 3 months.35 Recanalization of the occluded artery occurs sponta-neously in 24% of cases.36 However, intra-arterial thrombolysis can raise the rate of recanalization to 64% with an associated improvement of morbidity and mortality.36 Clot size,37 and age and composition, as well, are associated with the rates of recan-alization. Thrombolysis accompanied by mechanical throm-bectomy has demonstrated equipoise ion comparison with thrombolysis alone with a trend toward improved outcomes.38
Patient presentation (continued): The patient was trans-ferred to our institution the following day for further management. Vital signs at the time of admission noted bra-dycardia at 41 bpm, blood pressure of 124/75 mm Hg, oxy-gen saturations of 95% on room air, and a temperature of 37.1°C. Physical examination revealed a regular bradycar-dia, with auscultation of the first heart sound and physiolog-ical splitting of the second heart sound with no appreciable murmurs, gallops, or rubs. The point of maximal impulse was palpated and was neither accentuated nor displaced, and a sternal heave was no longer appreciated. The neuro-logical examination noted mild decreased dexterity in the left hand without appreciable weakness or sensory deficit. The abdomen was soft and nontender with mild hepato-megaly, and the lungs were clear to auscultation bilaterally.
Serum studies noted a normocytic anemia of 11.7 g/dL (mean corpuscular value, 77.6 fL), leukocytosis of 11.9×109 cells/L with a neutrophilia of 9.21×109 cells/L, and a nor-mal platelet count of 231×109 cells/L. Creatine (0.9 g/dL), sodium (137 mmol/L), and potassium (4.0 mmol/L) were within normal limits. The international normalized ratio was therapeutic at 2.3.
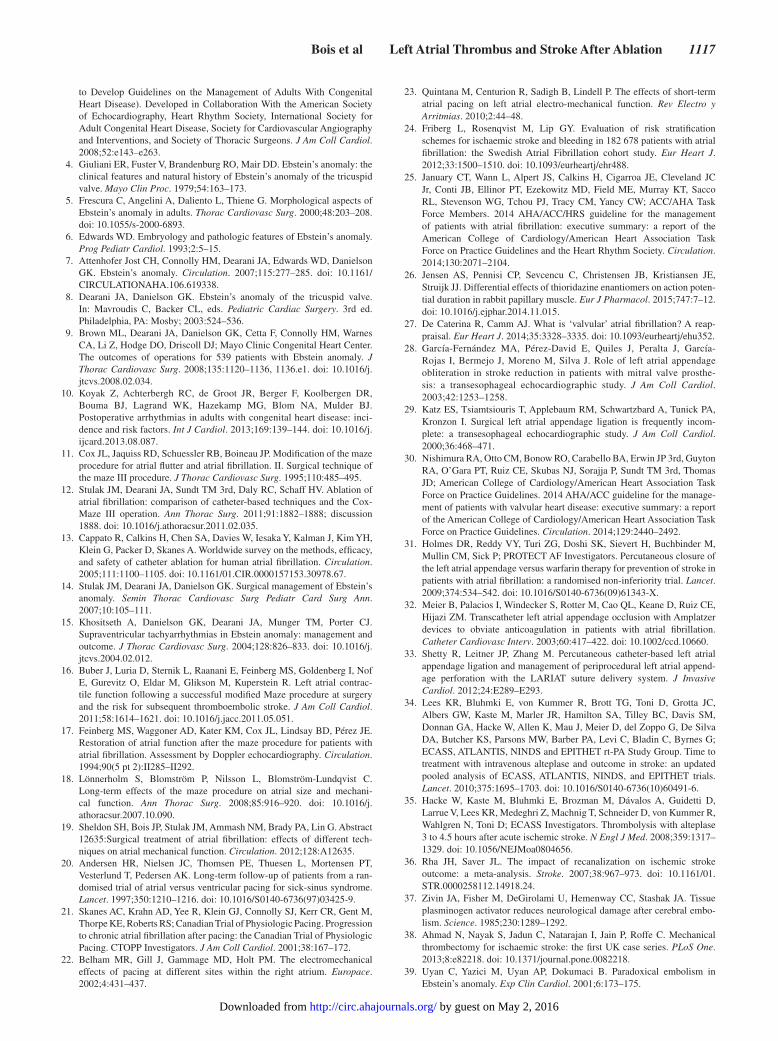
ECG revealed a junctional bradycardia without electric evidence of atrial function (absence of P waves) as shown in Figure 6.
A transesophageal echocardiogram revealed a lami-nated left atrial appendage thrombus and severe left atrial enlargement (Figure 7).
Dr Ammash: Transesophageal echocardiogram is indicated to look for the source of embolism especially in patients with structural heart disease and prior history of atrial arrhythmias. The most common source of embolism noted on echocardiog-raphy in an undifferentiated patient following an ischemic neurological event include left atrial thrombi or spontaneous echo contrast, left ventricular thrombi, infective or thrombotic vegetations, intracardiac tumors such as myxoma, fibroelas-tomas, atrial shunt such as atrial septal defect or patent fora-men ovale, and atherosclerotic plaques of the aorta, not in any particular order.
Figure 5. Diffusion head MRI demonstrating acute ischemic stroke in the territory of the right middle cerebral artery (arrow).
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from
Bois et al Left Atrial Thrombus and Stroke After Ablation 1115
There are several unique characteristics in the congenital heart disease population that should be considered when evalu-ating for the etiology of either a stroke or transient ischemic event. First, as previously alluded to, atrial arrhythmias are common in the patient with Ebstein anomaly,7 and, therefore, the patient should be evaluated initially with a standard 12-lead ECG followed by a 24-hour Holter monitor, and ultimately a cardiac event monitor if no underlying rhythm abnormality is initially detected. Second, Ebstein anomaly is associated with the presence of intracardiac shunts resulting in paradoxical emboli.39 Therefore, careful anatomic evaluation of the heart via echocardiography must be performed to evaluate for this possibility. In the current case, underlying atrial fibrillation with subsequent development of a left atrial appendage throm-bus was the likely source for the patient’s ischemic stroke.
However, in other adult congenital heart disease popula-tions, specifically cyanotic heart disease, secondary erythro-cytosis, may lead to increased blood viscosity and ultimately impede cerebral blood flow.40 An evaluation of 162 patients with cyanotic congenital heart disease at our institution noted that the incidence of cerebral vascular events was 16.6%.41 Furthermore, this study was the first to report an association between iron-deficiency anemia and resultant microcytosis and the risk for stroke (P<0.01). It is postulated that microcytic, iron-deficient blood cells are less deformable that their normal
iron-replete counterparts, thereby inhibiting the ease with which they pass through the microvasculature.40 This finding has sig-nificant therapeutic implications, in particular, with regard to iron repletion and phlebotomy. First, iron deficiency anemia should be avoided with iron supplementation initiated when the mean corpuscular volume falls below 82 fL. Second, therapeu-tic phlebotomy should be used judiciously typically when the hemoglobin is >20 g/dL or the hematocrit rises above 65%.42
Patient presentation (continued): Evaluation by Neurology, Cardiac Intensive Care, and Congenital Cardiology concluded that, with high probability, the left atrial appendage thrombus was the likely substrate for the patient’s cardioembolic stroke.
He successfully completed brain rehabilitation and had very minimal residual deficit in left hand dexterity. He was educated on the importance of compliance with oral anticoagulation therapy and was discharged with an international normalized ratio goal of 3.0. A follow-up transesophageal echocardiogram performed at 3 months demonstrated resolution of the left atrial thrombi with proper anticoagulation with discussion of possible future percutaneous left atrial appendage closure.
DiscussionThis is a unique case that illustrates the complex cardiovascu-lar issues that arise when caring for the patient with congenital heart disease. It provides critical teaching points with regard to the diagnosis and management of patients with Ebstein anomaly, the approach to anticoagulation in the atrial fibrilla-tion population, and the management of an acute cerebrovas-cular event. Finally, it introduces the concept of LAMF and how it may impact decision making in regard to the manage-ment of patients with atrial fibrillation.
First, as highlighted by the case presentation, Ebstein anomaly is characterized by the failure of the tricuspid valve to delaminate and by apical displacement of the tricus-pid valve toward the apex. The degree of displacement can be quantified by calculating the displacement index. This is achieved by measuring the distance in millimeters from the mitral valve to the tricuspid valve and then dividing that dis-tance by the patient’s body surface area. In the patient without congenital heart disease the tricuspid valve will be slightly
Figure 7. Transesophageal echocardiogram revealed a laminated left atrial appendage thrombus (red arrow).
Figure 6. ECG demonstrating junctional bradycardia without electric evidence of atrial function (absence of P waves).
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from

1116 Circulation March 24, 2015
more displaced toward the apex than the mitral valve, but the overall displacement index should be <8 mm/m2. If >8 mm/m2, Ebstein anomaly should be suspected.6,8 As noted in Figure 3A through 3C, the underlying structural abnormali-ties of the tricuspid valve coupled with its unusual anatomic positioning lead to the development of severe tricuspid regur-gitation and marked right atrial enlargement. This patient pop-ulation is predisposed to several cardiac sequelae, including arrhythmias2 and heart failure,3 and therefore should be fol-lowed closely by a congenital heart disease specialist who can help determine when and if surgical intervention is indicated.
A second key discussion point prompted by the current case is how to approach thromboembolic prophylaxis in the atrial fibrillation population. Use of validated risk stratifica-tion tools such as the CHA
2DS
2-VASc or HAS-BLED scores
provides an initial starting point for determining if anticoagu-lation should be initiated.24 However, as will be elaborated on further in the discussion, other factors including the presence or absence of LAMF should impact decision making regard-ing thromboembolic prophylaxis. Once it has been decided to pursue anticoagulation, the clinician must determine whether or not their patient is a candidate for novel anticoagulant therapies in lieu of the traditional warfarin protocol. Before considering the use of novel anticoagulants, one must con-sider the patient’s age and renal function, and note the limited reversibility of these agents., as well Furthermore, the clini-cian must determine whether or not the patient is classified as having valvular or nonvalvular atrial fibrillation, because the novel anticoagulants have yet to be approved for nonval-vular atrial fibrillation. The definition of valvular versus non-valvular atrial fibrillation varies in the literature,27 which can make the distinction between the 2 challenging. In the current scenario, the severity of tricuspid regurgitation coupled with surgical valve repair compelled us to choose warfarin therapy.
A third critical issue proposed by the present case discus-sion is the management of cerebral vascular events in patients with congenital heart disease. This patient population is prone to atrial arrhythmias, particularly atrial fibrillation, and there-fore is inclined to the development of atrial clots (Figure 7). However, the clinician must also entertain several other etiolo-gies for stroke or transient ischemic events unique to the con-genital heart disease population such as paradoxical emboli from atrial or ventricular shunts or sludging of poorly deform-able microcytic red blood cells in the cerebral vasculature.40
A particularly unique component to this case presentation is the role of LAMF in clot formation and how this may impact follow-up and clinical decision making. Left atrial function as defined by pressure-volume relationship analysis consists of 3 phases.43 First, pulmonary venous blood flow enters the left atrium during systole. Second, in early diastole, the left atrium serves as a conduit to allow passive blood flow into the left ventricle from the pulmonary veins. The third component is defined by left atrial contraction that contributes a further 20% to left ventricular stroke volume.44
Several methods have been used to define left atrial mechani-cal function, including left atrial appendage emptying velocity, left atrial spontaneous echocardiographic contrast, and pulmo-nary vein blood flow velocity.45 Left atrial mechanical function was determined in the current case by examining Doppler A
wave on mitral inflow, tissue Doppler imaging A′ on medial mitral annular imaging, and left atrial ejection fraction, which have been defined and implemented in prior reports.46–48
The role of LAMF and the risk of developing an ini-tial or recurrent arrhythmia following cardiac interven-tions has become a topic of several investigations. For instance, American College of Cardiology/American Heart Association/European Society of Cardiology standard-of-care guidelines recommend 4 weeks of anticoagulation fol-lowing cardioversion in patients who present >48 hours after the onset of atrial arrhythmia to prevent thromboembolism.49 Grimm and colleagues45 have demonstrated decreased LAMF following cardioversion and have postulated that the lack of atrial mechanical function may be the underlying mechanism of atrial clot formation and subsequent thromboembolism. Thomas et al50 demonstrated that LAMF is compromised to a further extent in patients after they undergo linear radiofre-quency ablation than patients who had undergone cardiover-sion only and markedly less than a control population.
Surgical interventions to address atrial fibrillation also appear to affect LAMF. Buber and colleagues conducted a prospective study of 150 patients who underwent radiofre-quency and cryoablation maze (without atrial incisions) and noted that up to 31% of patients had no evidence of LAMF postoperatively. Multivariate analysis demonstrated that the lack of LAMF was associated with a 5-fold increase in the risk for stroke (P=0.02).16
The current case study involves a patient whom underwent pulmonary vein isolation, and the Cox maze III procedure, as well, and had a marked absence of LAMF postoperatively. This case illustrates the importance of evaluating LAMF after the Cox maze procedure or pulmonary vein isolation to determine the length of anticoagulation needed to prevent thromboembolic sequelae. Further investigation is needed to determine the prevalence, duration, and clinical importance of impaired atrial mechanical function in the postsurgical atrial fibrillation patient population.
DisclosuresNone.
References 1. Perloff JK. The Clinical Recognition of Congenital Heart Disease. 5th ed.
Philadelphia, PA: WB Saunders; 2003. 2. Celermajer DS, Bull C, Till JA, Cullen S, Vassillikos VP, Sullivan ID,
Allan L, Nihoyannopoulos P, Somerville J, Deanfield JE. Ebstein’s anom-aly: presentation and outcome from fetus to adult. J Am Coll Cardiol. 1994;23:170–176.
3. Warnes CA, Williams RG, Bashore TM, Child, JS, Connolly HM, Dearani JA, del Nido, P, Fasules, JW, Graham TP Jr, Hijazi ZM, Hunt, SA, King, ME, Landzberg, MJ, Miner, PD, Radford MJ, Walsh, EP, Webb, GD, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Buller CE, Creager MA, Ettinger SM, Halperin JL. Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura RA, Page RL, Riegel B, Tarkington LG, Yancy CW; American College of Cardiology; American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease); American Society of Echocardiography; Heart Rhythm Society; International Society for Adult Congenital Heart Disease; Society for Cardiovascular Angiography and Inverventions; Society of Thoracic Surgeons. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from
Bois et al Left Atrial Thrombus and Stroke After Ablation 1117
to Develop Guidelines on the Management of Adults With Congenital Heart Disease). Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e143–e263.
4. Giuliani ER, Fuster V, Brandenburg RO, Mair DD. Ebstein’s anomaly: the clinical features and natural history of Ebstein’s anomaly of the tricuspid valve. Mayo Clin Proc. 1979;54:163–173.
5. Frescura C, Angelini A, Daliento L, Thiene G. Morphological aspects of Ebstein’s anomaly in adults. Thorac Cardiovasc Surg. 2000;48:203–208. doi: 10.1055/s-2000-6893.
6. Edwards WD. Embryology and pathologic features of Ebstein’s anomaly. Prog Pediatr Cardiol. 1993;2:5–15.
7. Attenhofer Jost CH, Connolly HM, Dearani JA, Edwards WD, Danielson GK. Ebstein’s anomaly. Circulation. 2007;115:277–285. doi: 10.1161/CIRCULATIONAHA.106.619338.
8. Dearani JA, Danielson GK. Ebstein’s anomaly of the tricuspid valve. In: Mavroudis C, Backer CL, eds. Pediatric Cardiac Surgery. 3rd ed. Philadelphia, PA: Mosby; 2003:524–536.
9. Brown ML, Dearani JA, Danielson GK, Cetta F, Connolly HM, Warnes CA, Li Z, Hodge DO, Driscoll DJ; Mayo Clinic Congenital Heart Center. The outcomes of operations for 539 patients with Ebstein anomaly. J Thorac Cardiovasc Surg. 2008;135:1120–1136, 1136.e1. doi: 10.1016/j.jtcvs.2008.02.034.
10. Koyak Z, Achterbergh RC, de Groot JR, Berger F, Koolbergen DR, Bouma BJ, Lagrand WK, Hazekamp MG, Blom NA, Mulder BJ. Postoperative arrhythmias in adults with congenital heart disease: inci-dence and risk factors. Int J Cardiol. 2013;169:139–144. doi: 10.1016/j.ijcard.2013.08.087.
11. Cox JL, Jaquiss RD, Schuessler RB, Boineau JP. Modification of the maze procedure for atrial flutter and atrial fibrillation. II. Surgical technique of the maze III procedure. J Thorac Cardiovasc Surg. 1995;110:485–495.
12. Stulak JM, Dearani JA, Sundt TM 3rd, Daly RC, Schaff HV. Ablation of atrial fibrillation: comparison of catheter-based techniques and the Cox-Maze III operation. Ann Thorac Surg. 2011;91:1882–1888; discussion 1888. doi: 10.1016/j.athoracsur.2011.02.035.
13. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Packer D, Skanes A. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation. 2005;111:1100–1105. doi: 10.1161/01.CIR.0000157153.30978.67.
14. Stulak JM, Dearani JA, Danielson GK. Surgical management of Ebstein’s anomaly. Semin Thorac Cardiovasc Surg Pediatr Card Surg Ann. 2007;10:105–111.
15. Khositseth A, Danielson GK, Dearani JA, Munger TM, Porter CJ. Supraventricular tachyarrhythmias in Ebstein anomaly: management and outcome. J Thorac Cardiovasc Surg. 2004;128:826–833. doi: 10.1016/j.jtcvs.2004.02.012.
16. Buber J, Luria D, Sternik L, Raanani E, Feinberg MS, Goldenberg I, Nof E, Gurevitz O, Eldar M, Glikson M, Kuperstein R. Left atrial contrac-tile function following a successful modified Maze procedure at surgery and the risk for subsequent thromboembolic stroke. J Am Coll Cardiol. 2011;58:1614–1621. doi: 10.1016/j.jacc.2011.05.051.
17. Feinberg MS, Waggoner AD, Kater KM, Cox JL, Lindsay BD, Pérez JE. Restoration of atrial function after the maze procedure for patients with atrial fibrillation. Assessment by Doppler echocardiography. Circulation. 1994;90(5 pt 2):II285–II292.
18. Lönnerholm S, Blomström P, Nilsson L, Blomström-Lundqvist C. Long-term effects of the maze procedure on atrial size and mechani-cal function. Ann Thorac Surg. 2008;85:916–920. doi: 10.1016/j.athoracsur.2007.10.090.
19. Sheldon SH, Bois JP, Stulak JM, Ammash NM, Brady PA, Lin G. Abstract 12635:Surgical treatment of atrial fibrillation: effects of different tech-niques on atrial mechanical function. Circulation. 2012;128:A12635.
20. Andersen HR, Nielsen JC, Thomsen PE, Thuesen L, Mortensen PT, Vesterlund T, Pedersen AK. Long-term follow-up of patients from a ran-domised trial of atrial versus ventricular pacing for sick-sinus syndrome. Lancet. 1997;350:1210–1216. doi: 10.1016/S0140-6736(97)03425-9.
21. Skanes AC, Krahn AD, Yee R, Klein GJ, Connolly SJ, Kerr CR, Gent M, Thorpe KE, Roberts RS; Canadian Trial of Physiologic Pacing. Progression to chronic atrial fibrillation after pacing: the Canadian Trial of Physiologic Pacing. CTOPP Investigators. J Am Coll Cardiol. 2001;38:167–172.
22. Belham MR, Gill J, Gammage MD, Holt PM. The electromechanical effects of pacing at different sites within the right atrium. Europace. 2002;4:431–437.
23. Quintana M, Centurion R, Sadigh B, Lindell P. The effects of short-term atrial pacing on left atrial electro-mechanical function. Rev Electro y Arritmias. 2010;2:44–48.
24. Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33:1500–1510. doi: 10.1093/eurheartj/ehr488.
25. January CT, Wann L, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–2104.
26. Jensen AS, Pennisi CP, Sevcencu C, Christensen JB, Kristiansen JE, Struijk JJ. Differential effects of thioridazine enantiomers on action poten-tial duration in rabbit papillary muscle. Eur J Pharmacol. 2015;747:7–12. doi: 10.1016/j.ejphar.2014.11.015.
27. De Caterina R, Camm AJ. What is ‘valvular’ atrial fibrillation? A reap-praisal. Eur Heart J. 2014;35:3328–3335. doi: 10.1093/eurheartj/ehu352.
28. García-Fernández MA, Pérez-David E, Quiles J, Peralta J, García-Rojas I, Bermejo J, Moreno M, Silva J. Role of left atrial appendage obliteration in stroke reduction in patients with mitral valve prosthe-sis: a transesophageal echocardiographic study. J Am Coll Cardiol. 2003;42:1253–1258.
29. Katz ES, Tsiamtsiouris T, Applebaum RM, Schwartzbard A, Tunick PA, Kronzon I. Surgical left atrial appendage ligation is frequently incom-plete: a transesophageal echocardiographic study. J Am Coll Cardiol. 2000;36:468–471.
30. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM 3rd, Thomas JD; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC guideline for the manage-ment of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:2440–2492.
31. Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, Mullin CM, Sick P; PROTECT AF Investigators. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009;374:534–542. doi: 10.1016/S0140-6736(09)61343-X.
32. Meier B, Palacios I, Windecker S, Rotter M, Cao QL, Keane D, Ruiz CE, Hijazi ZM. Transcatheter left atrial appendage occlusion with Amplatzer devices to obviate anticoagulation in patients with atrial fibrillation. Catheter Cardiovasc Interv. 2003;60:417–422. doi: 10.1002/ccd.10660.
33. Shetty R, Leitner JP, Zhang M. Percutaneous catheter-based left atrial appendage ligation and management of periprocedural left atrial append-age perforation with the LARIAT suture delivery system. J Invasive Cardiol. 2012;24:E289–E293.
34. Lees KR, Bluhmki E, von Kummer R, Brott TG, Toni D, Grotta JC, Albers GW, Kaste M, Marler JR, Hamilton SA, Tilley BC, Davis SM, Donnan GA, Hacke W, Allen K, Mau J, Meier D, del Zoppo G, De Silva DA, Butcher KS, Parsons MW, Barber PA, Levi C, Bladin C, Byrnes G; ECASS, ATLANTIS, NINDS and EPITHET rt-PA Study Group. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375:1695–1703. doi: 10.1016/S0140-6736(10)60491-6.
35. Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, Larrue V, Lees KR, Medeghri Z, Machnig T, Schneider D, von Kummer R, Wahlgren N, Toni D; ECASS Investigators. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. doi: 10.1056/NEJMoa0804656.
36. Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke. 2007;38:967–973. doi: 10.1161/01.STR.0000258112.14918.24.
37. Zivin JA, Fisher M, DeGirolami U, Hemenway CC, Stashak JA. Tissue plasminogen activator reduces neurological damage after cerebral embo-lism. Science. 1985;230:1289–1292.
38. Ahmad N, Nayak S, Jadun C, Natarajan I, Jain P, Roffe C. Mechanical thrombectomy for ischaemic stroke: the first UK case series. PLoS One. 2013;8:e82218. doi: 10.1371/journal.pone.0082218.
39. Uyan C, Yazici M, Uyan AP, Dokumaci B. Paradoxical embolism in Ebstein’s anomaly. Exp Clin Cardiol. 2001;6:173–175.
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from

1118 Circulation March 24, 2015
40. Territo MC, Rosove M, Perloff J. Cyanotic congenital heart disease: hematologic management. In: Perloff JK, Child JS, eds. Congenital Heart Disease in Adults. Philadelphia, PA: W.B. Saunders; 1991:93–103.
41. Ammash N, Warnes CA. Cerebrovascular events in adult patients with cyanotic congenital heart disease. J Am Coll Cardiol. 1996;28:768–772.
42. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87:1954–1959.
43. Pagel PS, Kehl F, Gare M, Hettrick DA, Kersten JR, Warltier DC. Mechanical function of the left atrium: new insights based on analysis of pressure-volume relations and Doppler echocardiography. Anesthesiology. 2003;98:975–994.
44. Mitchell JH, Shapiro W. Atrial function and the hemodynamic conse-quences of atrial fibrillation in man. Am J Cardiol. 1969;23:556–567.
45. Dimitri H, Sanders P. Atrial mechanical function-implications for catheter ablation of atrial fibrillation. Asia-Pacific Cardiol. 2007;1:54–56.
46. Jones CJ, Song GJ, Gibson DG. An echocardiographic assessment of atrial mechanical behaviour. Br Heart J. 1991;65:31–36.
47. Nakatani S, Garcia MJ, Firstenberg MS, Rodriguez L, Grimm RA, Greenberg NL, McCarthy PM, Vandervoort PM, Thomas JD. Noninvasive assessment of left atrial maximum dP/dt by a combina-tion of transmitral and pulmonary venous flow. J Am Coll Cardiol. 1999;34:795–801.
48. Thomas L, Thomas SP, Hoy M, Boyd A, Schiller NB, Ross DL. Comparison of left atrial volume and function after linear ablation and after cardiover-sion for chronic atrial fibrillation. Am J Cardiol. 2004;93:165–170.
49. Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Junt SA, Nishimura R, Omato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo JL, Zamorano JL; American College of Cardiology/American Heart Association Task Force on Practice Guidelines; European Society of Cardiology Committee for Practice Guidelines; European Heart Rhythm Association; Heart Rhythm Society. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114:e257–e354.
50. Grimm RA, Stewart WJ, Maloney JD, Cohen GI, Pearce GL, Salcedo EE, Klein AL. Impact of electrical cardioversion for atrial fibrillation on left atrial appendage function and spontaneous echo contrast: characterization by simultaneous transesophageal echocardiography. J Am Coll Cardiol. 1993;22:1359–1366.
KEY WORDS: atrial fibrillation ◼ atrial function, left ◼ cerebral infarction ◼ heart defects, congenital
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from
John P. Bois, Grace Lin, Peter A. Brady and Naser M. AmmashFunction
Isolation Ablation and Cox Maze III Procedure: Significance of Left Atrial Mechanical21-Year-Old Man With Ebstein Anomaly Who Previously Underwent Pulmonary Vein
Development of Left Atrial Thrombus and Subsequent Cardioembolic Stroke in a
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2015 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.115.015340
2015;131:1110-1118Circulation.
http://circ.ahajournals.org/content/131/12/1110World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 2, 2016http://circ.ahajournals.org/Downloaded from
Related Documents











