Defining the Epidemiology of a Novel GIST Multiple Tumor Syndrome: Results of a Population-Based Analysis Jason K. Sicklick, MD, Grace L. Ma, Joel M. Baumgartner, MD, Lisa Madlensky, PhD, CGC, Chih-Min Tang, PhD, Adam M. Burgoyne, MD, PhD, Jonathan C. Trent, MD, PhD, Maria E. Martinez, PhD, and James D. Murphy, MD, MS

Defining the Epidemiology of a Novel GIST Multiple Tumor Syndrome: Results of a Population-Based Analysis Jason K. Sicklick, MD, Grace L. Ma, Joel M. Baumgartner,
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Defining the Epidemiology of a Novel GIST Multiple Tumor Syndrome:Results of a Population-Based Analysis
Jason K. Sicklick, MD, Grace L. Ma, Joel M. Baumgartner, MD, Lisa Madlensky, PhD, CGC, Chih-Min Tang, PhD, Adam M. Burgoyne, MD, PhD, Jonathan C. Trent, MD, PhD, Maria E. Martinez, PhD,
and James D. Murphy, MD, MS
Relevant Disclosures
Consultant/Speaker for Novartis Pharmaceuticals (JKS, 2013).
Consultant for Novartis Pharmaceuticals (JCT, 2013)
Gastrointestinal Stromal Tumor• Approximately 95% of GISTs are considered non-hereditary
or sporadic.1-5
• Results of several descriptive, single institution case series suggest that patients with sporadic GIST develop synchronous or metachronous malignancies with frequencies far exceeding the often-cited 1-in-9 lifetime chance of developing 2 primary cancers.6
38 x 25 x 12 cm
1. Agaimy, A. and Hartmann, A. Pathologe 2010; 31(6): 430-7.2. Neuhann, T.M., Mansmann, V., Merkelbach-Bruse, S., et al. Am J Surg Pathol 2013; 37(6): 898-905.3. Kuroda, N., Tanida, N., Hirota, S., et al. Ann Diagn Pathol 2011; 15(5): 358-61.4. Ponti, G., Luppi, G., Martorana, D., et al. Oncol Rep 2010; 23(2): 437-44.5. Stratakis, C.A. and Carney, J.A. J Intern Med 2009; 266(1): 43-52.6. Kosary, C., LAG, R., and Miller, B., SEER Cancer statistics review 1973–1992: tables and graphs, National
Cancer Institute, N., Editor. 1995: Bethesda, MD.

Increased Frequency of Other Cancers
• 2006: Literature review of studies compromising 4,813 GIST patients, reported the frequency of additional malignancies was 4.5% to 33%.1
• 2010: Largest single institution study of 783 confirmed these findings, with 20.3% GIST patients developing ≥1 additional malignancies. 2
38 x 25 x 12 cm
1. Agaimy, A., Wunsch, P.H., Sobin, L.H., Lasota, J., and Miettinen, M. Semin Diagn Pathol 2006; 23(2): 120-9.
2. Pandurengan RK, Dumont AG, Araujo DM, Ludwig JA, Ravi V, Patel S, Garber J, Benjamin RS, Strom SS, and Trent JC. Ann Oncol 2010; 21(10): 2107-11.

Increased Frequency of Other Cancers
• Associations reported include:– Desmoids1
– Myeloid leukemias2
– Other GI malignancies discovered incidentally during resections for GIST
– GIST discovered incidentally during resections for other GI malignancies
• Limitations of published studies:– Based on single/multiple institutional series– Reported in a qualitative nature
38 x 25 x 12 cm
1. Dumont, A.G., Rink, L., Godwin, A.K., et al. Ann Oncol 2012; 23(5): 1335-40.2. Miettinen, M., Kraszewska, E., Sobin, L.H., and Lasota, J. Cancer 2008; 112(3): 645-9.
Purpose of Study
• To utilize a national cancer registry in the United States to investigate the rates and types of additional cancers in patients with GIST.
38 x 25 x 12 cm

Methods• We identified 6,112 patients diagnosed with GIST
between 2001 and 2011 in the Surveillance, Epidemiology, and End Results (SEER) database*– GI tumor site codes (C150-C189, C199, C209-C212, C218, C220-
C221, C239-C260, C268-C269, C480-C482, C488)– GIST-specific histology code (ICD-O-3 code 8936).
• Excluded patients with high likelihood of hereditary GIST syndromes by excluding those <20 years old
* SEER covers approximately 28% of the U.S. population
38 x 25 x 12 cm

Methods• Standardized Prevalence Ratios (SPRs) Before GIST– SPR = Observed/Expected cases of additional cancers– Expected = (total at-risk person-years) x [limited-
duration cancer prevalence specific to the patients’ age (in 5-y intervals), sex, race, and SEER registry grouping]
• Standardized Incidence Ratios (SIRs) After GIST– SIR = Observed/Expected cases of additional cancers– Expected = (total at-risk person-years) x [cancer
incidence specific to the patient’s age (in 5-year intervals), sex, race, year of GIST diagnosis (in 5-year intervals), and SEER registry grouping]

17.5%
82.5%
Additional cancer (N=1071)No cancer (N=5041)
Rate of Additional Cancers• 6,112 GIST patients in SEER• 1,071 (17.5%) had additional cancers.*
38 x 25 x 12 cm
Total observation period for additional cancers:• 123,453 person-years = 101,551 (before GIST) + 21,902 (after GIST)
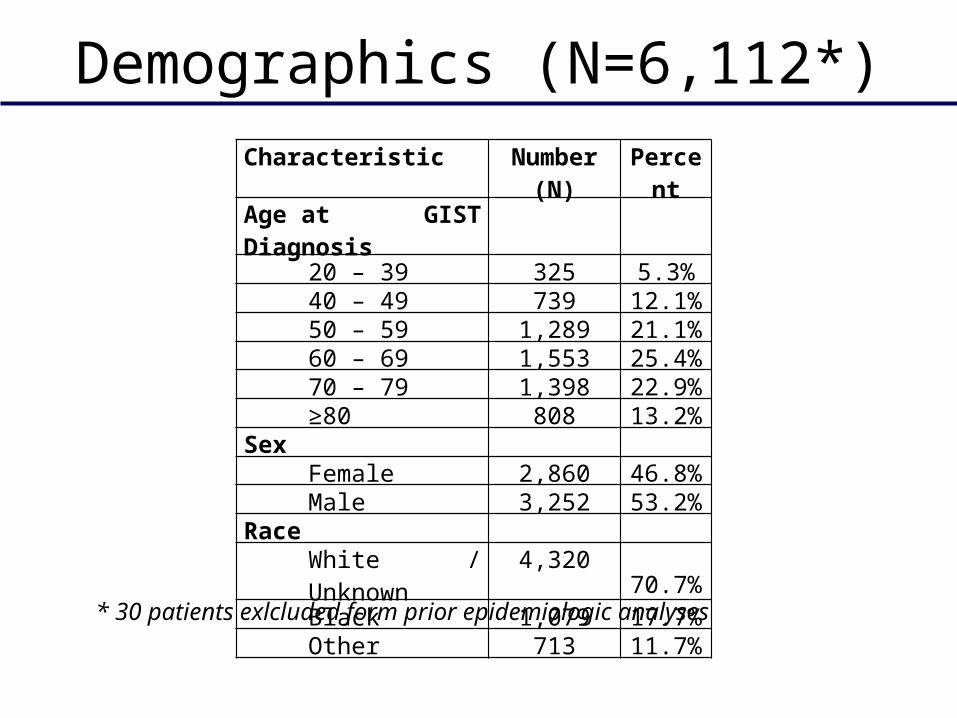
Demographics (N=6,112*)
38 x 25 x 12 cm
Characteristic Number (N) PercentAge at GIST Diagnosis
20 – 39 325 5.3%40 – 49 739 12.1%50 – 59 1,289 21.1%60 – 69 1,553 25.4%70 – 79 1,398 22.9%≥80 808 13.2%
Sex Female 2,860 46.8%Male 3,252 53.2%
Race White / Unknown 4,320 70.7%Black 1,079 17.7%Other 713 11.7%
* 30 patients exlcluded form prior epidemiologic analyses
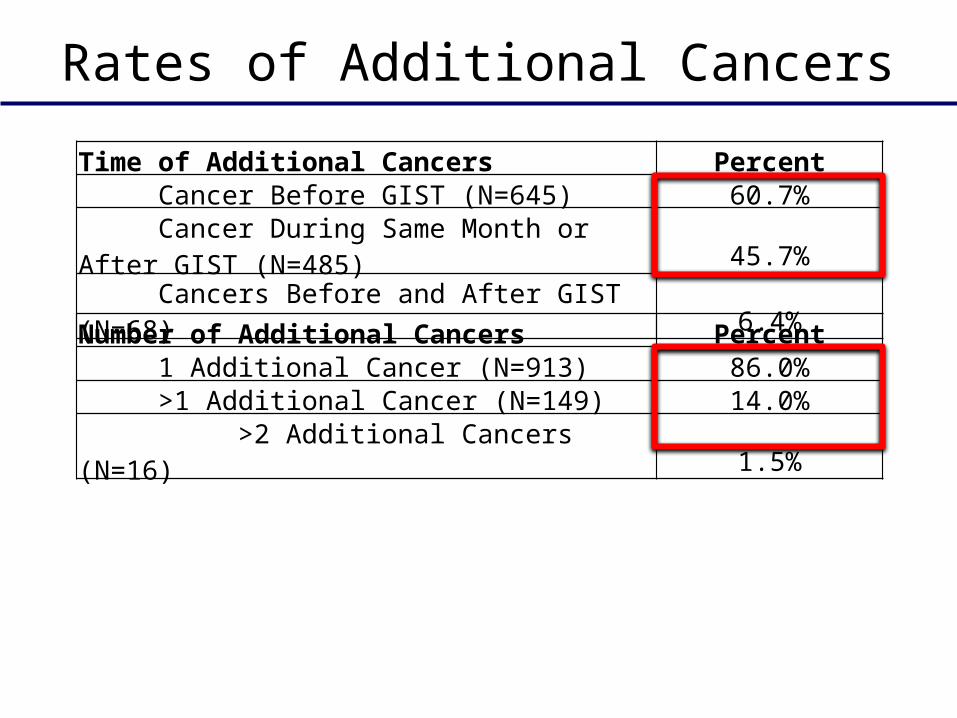
Rates of Additional Cancers
38 x 25 x 12 cmTime of Additional Cancers Percent Cancer Before GIST (N=645) 60.7% Cancer During Same Month or After GIST (N=485) 45.7% Cancers Before and After GIST (N=68) 6.4%
Number of Additional Cancers Percent 1 Additional Cancer (N=913) 86.0% >1 Additional Cancer (N=149) 14.0% >2 Additional Cancers (N=16) 1.5%

Genitourin
ary
Gastrointesti
nal
Breast
Hematologic
Cutaneous
Sarco
ma
Respira
tory
Neuroendocri
ne
Head and Neck
Thyroid
Hepatopancreatobilia
ry
Meso
thelioma
Nervous
Other0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
39.7%
15.2% 15.2%
6.5% 5.4% 4.6% 4.4%2.8% 2.1% 1.8% 0.9% 0.3% 0.1% 0.9%
Perc
ent
of a
dditi
onal
mal
igna
ncie
s by
ana
tom
ic s
ite
(%)
Additional Cancers Before GIST

Genitourin
ary
Gastrointesti
nal
Respira
tory
Breast
Hematologic
Hepatopancreatobilia
ry
Neuroendocri
ne
Thyroid
Sarco
ma
Cutaneous
Head and Neck
Nervous
Meso
thelioma
Other0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
29.4%
19.4%
13.1%
7.1% 6.5% 5.4%3.5% 3.1% 2.9% 2.7% 1.9% 0.6% 0.4% 1.2%
Perc
ent
of a
dditi
onal
mal
igna
ncie
s by
ana
tom
ic s
ite
(%)
Additional Cancers After GIST

Genitourin
ary
Gastrointesti
nal
Breast
Respira
tory
Hematologic
Cutaneous
Sarco
ma
Neuroendocri
ne
Hepatopancreatobilia
ry
Thyroid
Head and Neck
Nervous
Meso
thelioma
Other0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
35.3%
17.0%
11.8%
8.1%6.5%
4.2% 3.8% 3.1% 2.8% 2.4% 2.0%0.3% 0.3% 1.0%
Perc
ent
of a
dditi
onal
mal
igna
ncie
s by
ana
tom
ic s
ite
(%)
Additional Cancers Before +After GIST

Standard Prevalence/Incidence Rates
* Other female genitourinary (GU) includes vulvar cancer (N=4), vaginal cancer (N=1), fallopian tube (N=2), and NOS (N=1).** Hepatobiliary adenocarcinoma includes liver adenocarcinoma (N=2), intrahepatic cholangiocarcinoma (N=1), extrahepatic cholangiocarcinoma (N=1), and ampullary adenocarcinoma (N=4).
NOTE: While multiple GISTs were characteristic of hereditary GIST syndromes, only 16 additional GIST cases were noted in the SEER cohort, accounting for only 1.3% of second cancers.

Timeline for Occurrence95% CI* P<0.05.
>
> 5 yr 1 yr before to 1 after

Limitations• Cancers were identified using histology and site-specific codes;
as such, misdiagnosis or miscoding remain potential sources of error.
• We likely underestimated the actual number of patients with GIST in the database, and the diagnoses of second GISTs might be indicative of the miscoding of metastatic disease.
• While we attempted to eliminate patients with hereditary syndromes from our analysis by excluding those diagnosed <20 yo, we had no way of directly identifying these patients.
• As with all studies on 2nd cancers, the elevated incidence and prevalence rates might be partially attributed to detection bias during work-up and treatment, rather than a truly meaningful link.
38 x 25 x 12 cm

Summary-1• 17.5% of GIST patients (or 1-in-5.7) developed an
additional cancer– 60.7% Before GIST– 45.7% After GIST– 1-in-16 patients develop cancers Before and After GIST
• Additional cancers were most often diagnosed within 1 year of GIST diagnosis
38 x 25 x 12 cm

Summary-2• Before and After– Sarcomas, NET-carcinoid tumors, colorectal
adenocarcinoma, and NHL
• Before Only– Melanomas – Adenocarcinomas of the esophagus, bladder, and
prostate
• After Only– Papillary thyroid cancer, NSCLC, bladder TCC– Adenocarcinomas of the stomach, small intestine,
kidneys, hepatopancreatobiliary system, and female GU tract
38 x 25 x 12 cm

Conclusion-1• These data point to the possibility of a new GIST multiple
tumor syndrome, which we believe to be distinct from known disorders such as:– Familial GIST syndromes
• Only 16 additional GIST cases were noted in the SEER cohort, accounting for only 1.3% of second cancers
– Neurofibromatosis type 1 (e.g., GIST, sarcomas, periampullary/PNETs, and pheochromocytoma)• Sarcomas and PNETS comprised only 7.1% (6.9% and 0.2%, respectively) of
the 1,224 additional cancers
– Carney's triad (gastric GIST, pulmonary chondroma, extra-adrenal paraganglioma, adrenal adenomas)• Benign tumors are not coded in SEER
– Carney-Stratakis syndrome (e.g., GIST and paragangliomas)
38 x 25 x 12 cm
Conclusion-2• To our knowledge, this is the first population-based study
to quantify the occurrence of specific malignancies before and after GIST.
• We confirmed many previous institutional studies and identified several novel cancer associations, providing a comprehensive description and statistical examination to support the existence of a new GIST multiple tumor syndrome.
• Further investigations are necessary to link these epidemiological findings with relevant clinical decision-making, including screening and prevention.
38 x 25 x 12 cm
Related Documents











