Defending Diagnoses • Carcinoid Tumor (11): Jack Mbabuike • Colon Adenocarcinoma (3): Joshua Gordon • Basal Cell Carcinoma (1): Owen Dubowy • Hepatocellular Carcinoma (1): Amer Assal • Other Diagnoses: Pheochromocytoma VIPoma Gastric Cancer Gastrinoma

Defending Diagnoses Carcinoid Tumor (11): Jack Mbabuike Colon Adenocarcinoma (3): Joshua Gordon Basal Cell Carcinoma (1): Owen Dubowy Hepatocellular Carcinoma.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Defending Diagnoses• Carcinoid Tumor (11): Jack Mbabuike• Colon Adenocarcinoma (3): Joshua Gordon• Basal Cell Carcinoma (1): Owen Dubowy• Hepatocellular Carcinoma (1): Amer Assal
• Other Diagnoses: Pheochromocytoma VIPoma Gastric Cancer Gastrinoma
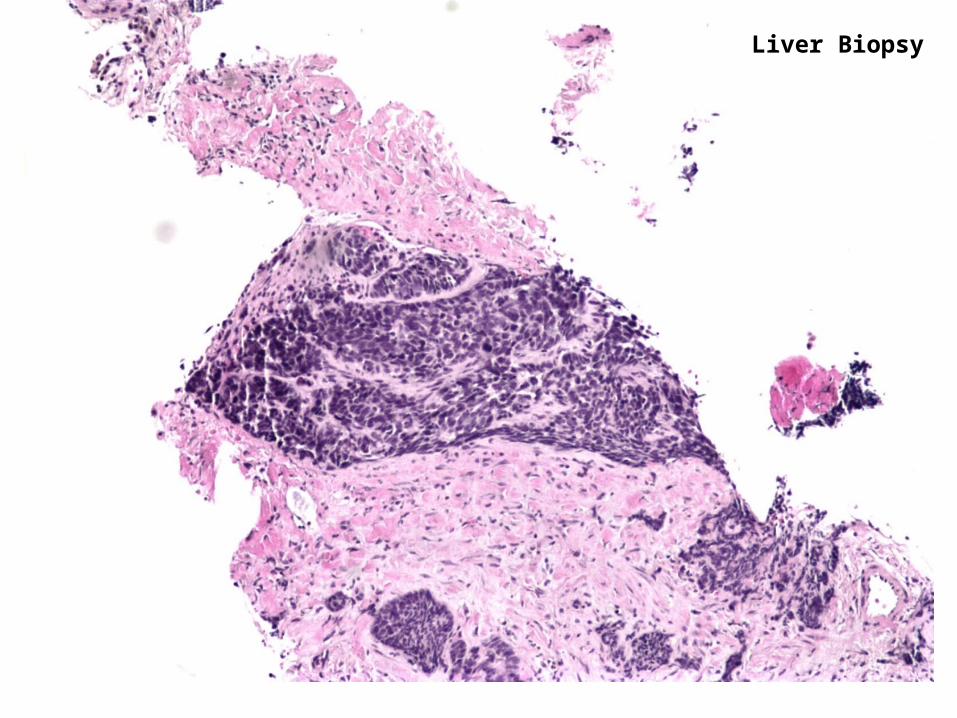
Liver Biopsy
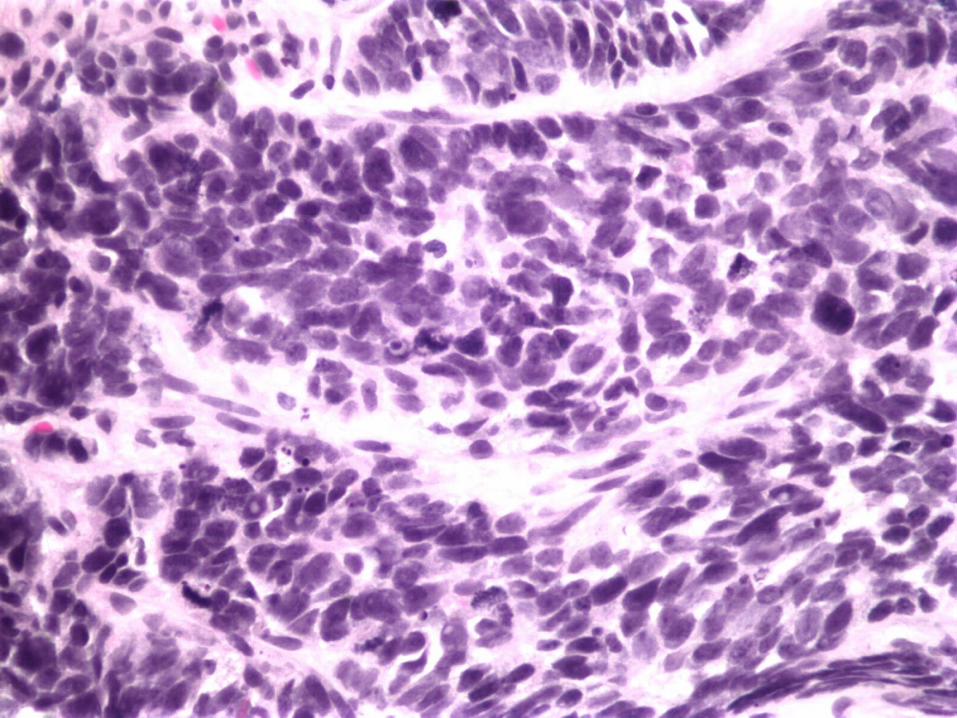

Liver BiopsyChromogranin
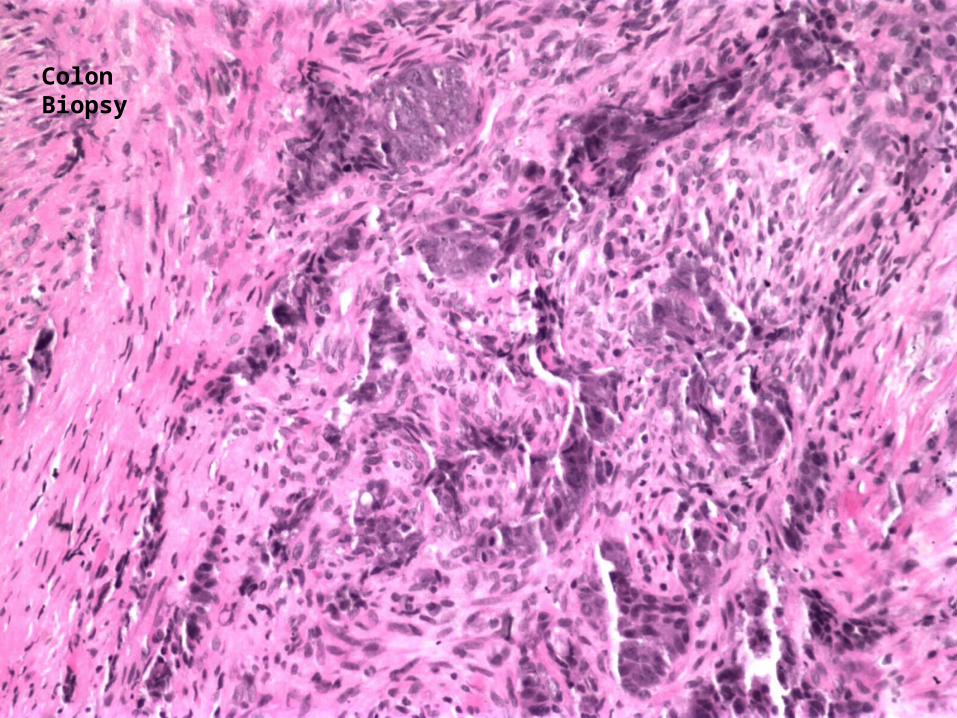
Colon Biopsy


Colon Biopsy
Chromogranin
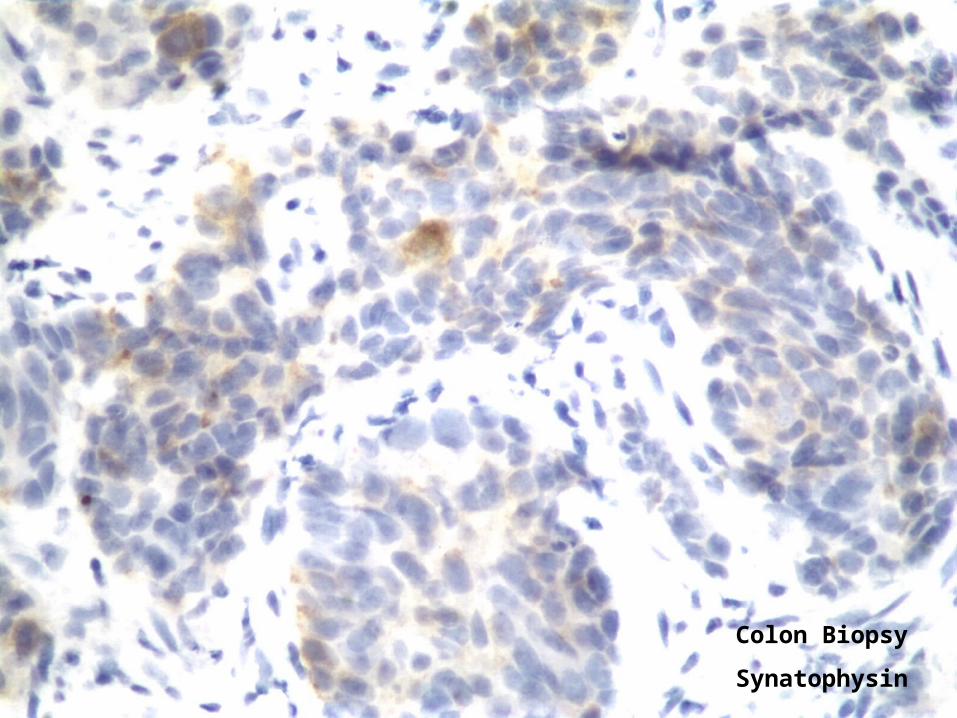
Colon Biopsy
Synatophysin
Final Diagnosis
Carcinoid syndrome secondary to poorly differentiated
neuroendocrine carcinoma of the colon with liver metastasis

Neuroendocrine Cancer
• Neuroendocrine cells are widely distributed throughout the body
• GI tract and pancreas have the largest component of neuroendocrine cells than any other organ system
• Nomenclature of GI neuroendocrine tumors is confusing – WHO standardized in 2005

Classification of NE Cancers of the Colon

Classification of Neuroendocrine Cancers of the
ColonI. Well-Differentiated Tumors – Carcinoid
II. Well-Differentiated Endocrine Carcinoma – Malignant Carcinoid
III. Poorly Differentiated Endocrine Carcinoma – our patient
IV. Mixed Exocrine-Endocrine Carcinoma

Definition of Carcinoid Syndrome
• Constellation of symptoms produced by the actions of neuroendocrine tumor secretory products
Prevalence of Colon Neuroendocrine Tumors
• Likely underestimated due to need for special additional staining
• Large retrospective series of resected colorectal tumors found:
- 4% of tumors had partial neuroendocrine differentiation
- 1% complete neuroendocrine differentiation

Pathophysiology of Colon Neuroendocrine Tumors
• Poorly understood, risk factors are not known
• Some suggestion of hereditary component
• Some overlap with the genetic model of tumorigenesis of colonic adenocarcinoma
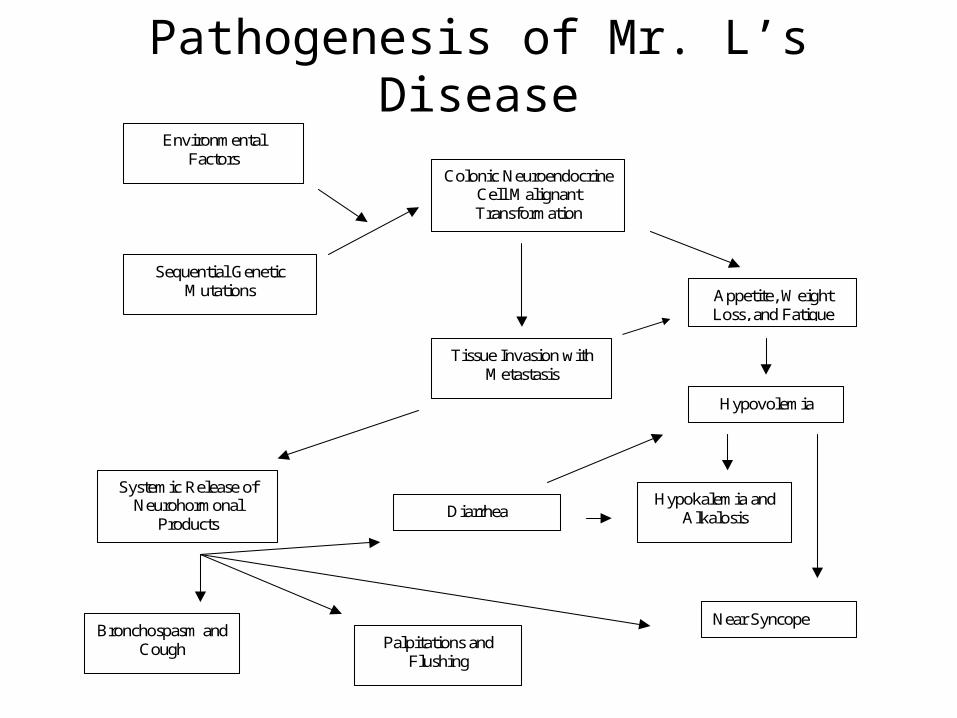
Pathogenesis of Mr. L’s Disease
Environmental Factors
Sequential Genetic Mutations
Colonic Neuroendocrine Cell Malignant Transformation
Tissue Invasion with Metastasis
Systemic Release of Neurohormonal
Products
Appetite, Weight Loss, and Fatigue
Hypovolemia
Hypokalemia and Alkalosis Diarrhea
Near Syncope Bronchospasm and
Cough Palpitations and Flushing

Clinical Presentation of Colon Neuroendocrine Cancer
• abdominal pain• change in bowel habits• melena/hematochezia• anemia, weakness, weight loss• symptoms of carcinoid syndrome rare
Diagnosis of Neuroendocrine Colon Cancer
• Colonoscopy with biopsy
• Immunohistochemical stains for chromogranin and synaptophysin

Treatment of Neuroendocrine Colon Carcinoma
• Surgery if local disease – curative
• Prognosis is poor for metastatic disease
• Chemo is similar to small cell lung cancer
- Cisplatin and Etoposide
- Irenotecan
• Treatment of symptoms - Sandostatin
Follow-up
• Patient had progression of disease after 4 cycles of cisplatin and etoposide, bone mets developed
• Irenotectan initiated with continued progression• Sandostatin initiated for worsening diarrhea and
flushing• Patient transferred to Bronx VA for palliative
radiation therapy• He passed away last week
Related Documents











