Stephanie A. Weyrauch, SPT DPT/MSCI Candidate Washington University in St. Louis 9/3/2014 Deep Vein Thrombosis: Clinical Prediction Rules and their Application

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Stephanie A. Weyrauch, SPTDPT/MSCI Candidate
Washington University in St. Louis9/3/2014
Deep Vein Thrombosis: Clinical Prediction Rules and their
Application
Overview
• Introduction• Diagnosis of Deep Vein Thrombosis (DVT)• Clinical Prediction Rules• Literature Review• Clinical Application• Conclusions
INTRODUCTION
Introduction
• Deep Vein Thrombosis– Annual incidence: 2/1000 (van der Velde et al, 2011)
– Lead to pulmonary embolism, post-phlebitic syndrome, chronic thromboembolic pulmonary hypertension (Tan et al, 2009; Wells et al, 2006; Oudega et al, 2005; Tamariz et al, 2004; Wells et al, 2003)
– Unnecessary anti-coagulation therapy (Tan et al, 2009; Wells et al, 2006; Oudega et al, 2005; Wells et al, 2003)
Natural History of DVT General History
Most start in calf Rarely cause leg symptoms
25% untreated symptomatic calf DVTs extend to proximal veins within 1 week of presentation
80% symptomatic DVTs involve proximal veins Risk highest within 2 weeks of surgery
Remains elevated ~2-3 monthsKearon C, 2003
Natural History of DVT General History
DVTs associated with surgery start intraoperatively
50% resolve spontaneously within 72 hours Risk for progression is greater in those with
continuing risk factors for DVT i.e. immobilization, large initial DVT
Kearon C, 2003
Natural History of DVT
Specific to Orthopedic Surgery 2x greater risk for DVT compared to general
surgery 75% of DVT occur in operated leg Timing of post-op DVT depends on surgery
i.e. risk higher s/p TKA initially but drops more rapidly compared to s/p THA
Kearon C, 2003
DIAGNOSIS OF DVT
Diagnosis of DVT• Medical history• Physical examination
– Homan's sign (Urbano, 2001)
• Risk assessment– Use of clinical prediction rules
• Potential referral for further testing– D-dimer testing– Ultrasonography
» False negative: about 2% (Kearon, Ginsberg & Hirsch, 1998)
– Venography
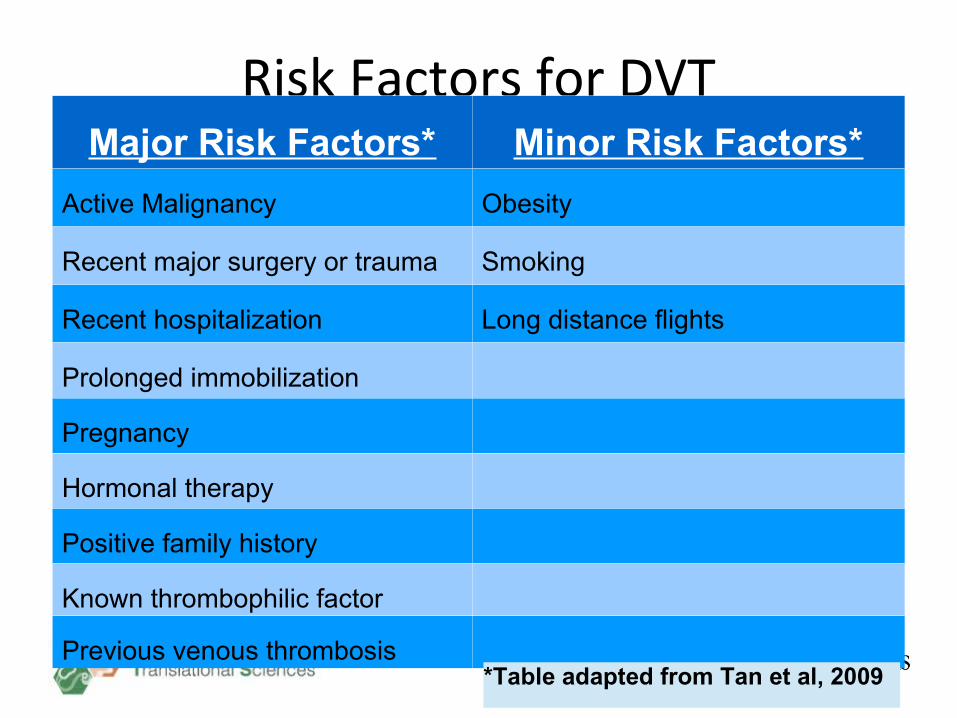
Risk Factors for DVTMajor Risk Factors* Minor Risk Factors*
Active Malignancy Obesity
Recent major surgery or trauma Smoking
Recent hospitalization Long distance flights
Prolonged immobilization
Pregnancy
Hormonal therapy
Positive family history
Known thrombophilic factor
Previous venous thrombosis*Table adapted from Tan et al, 2009
Signs/Sxs of DVT
• Signs– Tenderness and swelling in affected leg– Increased warmth– Changes in skin color
• Symptoms– Pain in affected leg
• Not sensitive or specific for diagnosis
Tan et al, 2009; Urbano et al, 2001; Tamariz et al, 2004
Differential Diagnosis for DVT• DVT may have similar signs/sxs as:
– Ruptured calf muscle/tendon– Ruptured popliteal synovial membrane or
Baker's cyst– Muscle cramp– Muscle hematoma– Cellulitis– Chronic venous insufficiency– Lymphodema Tan et al, 2009
CLINICAL PREDICTION RULES
Clinical Prediction Rules
• Definition (Toll et al, 2008; Childs & Cleland, 2006; Tamariz et al, 2004)
– Designed to improve clinical decision making by assisting clinicians in making particular diagnosis, establishing prognosis, or matching patients to optimal interventions
– Based on subset of predictor variables from history and physical examination
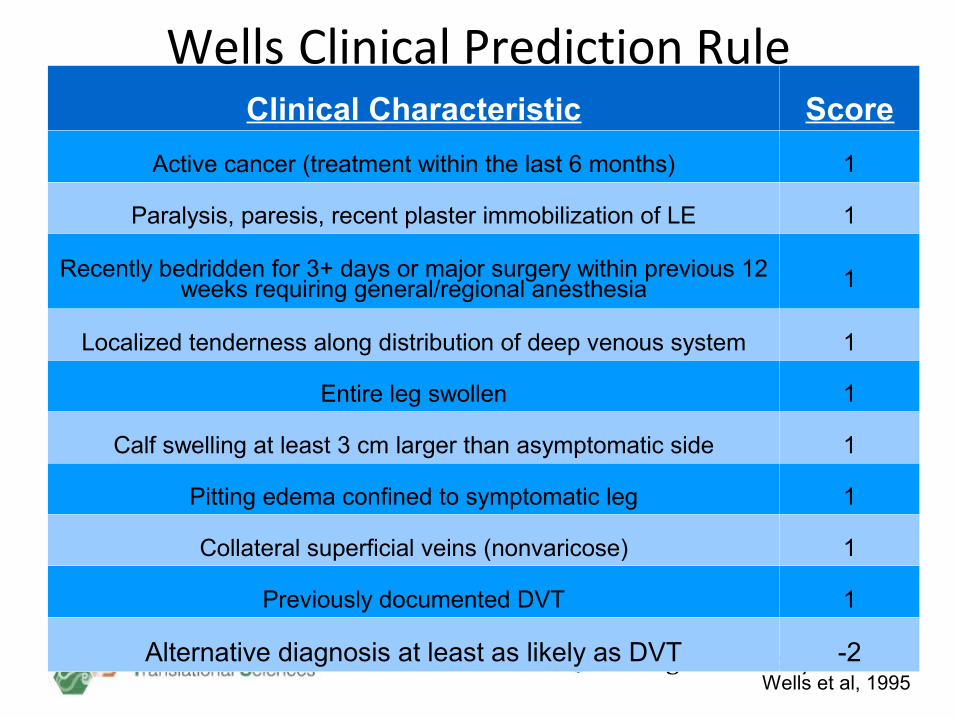
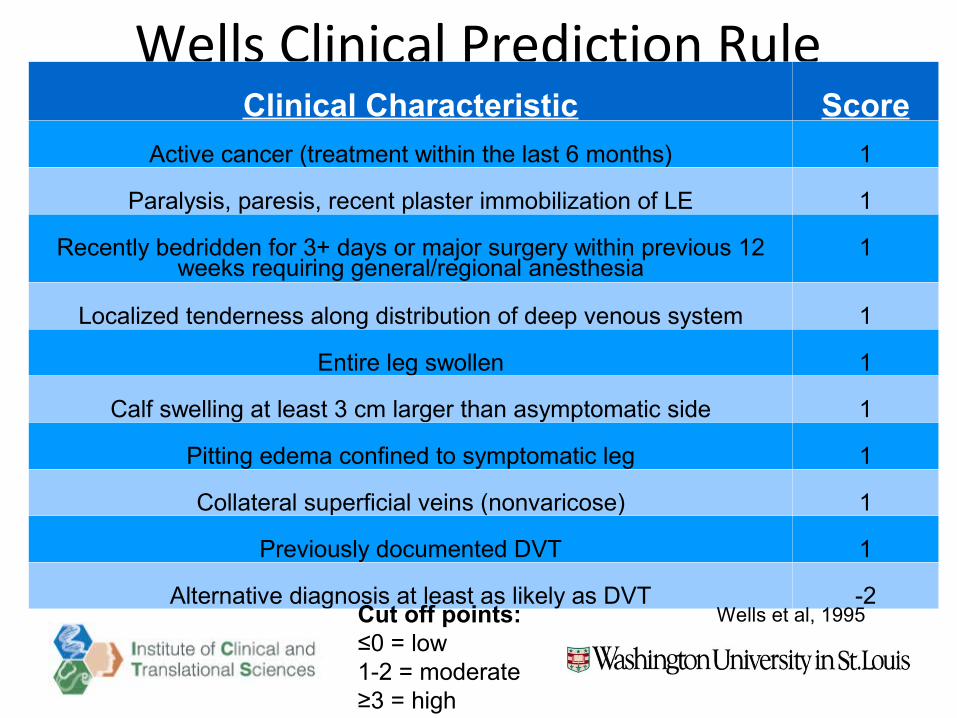
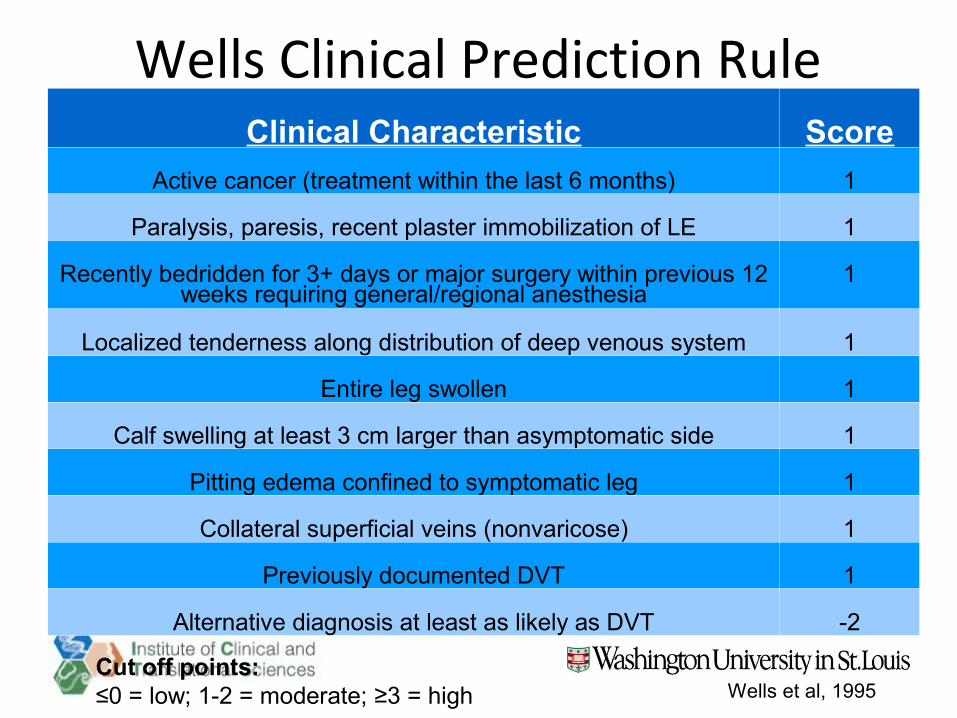
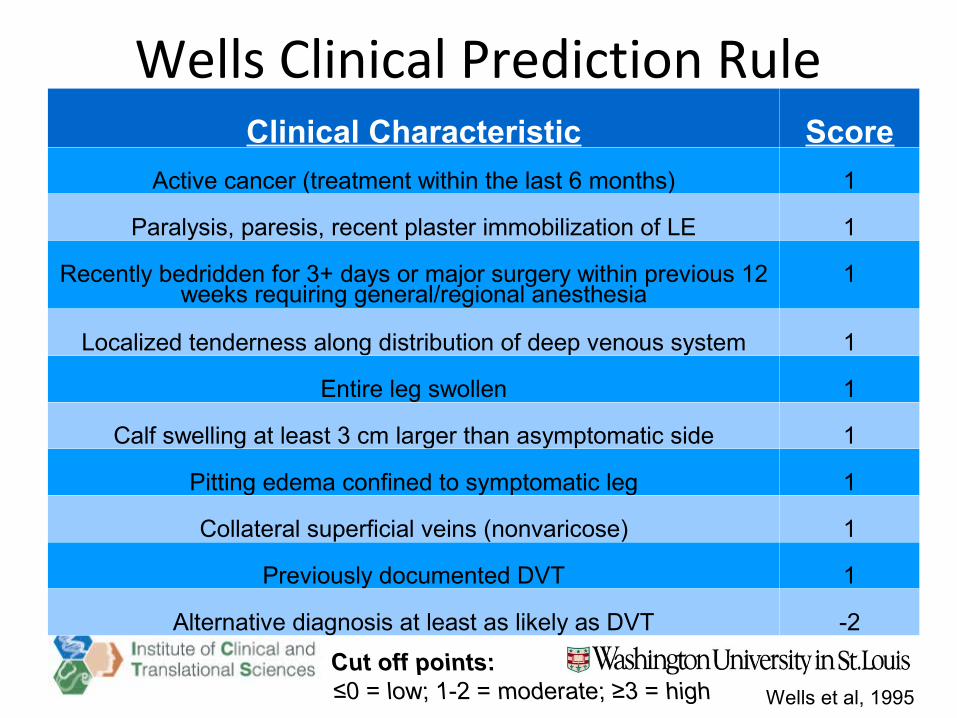
Wells Clinical Prediction RuleClinical Characteristic Score
Active cancer (treatment within the last 6 months) 1
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia 1
Localized tenderness along distribution of deep venous system 1
Entire leg swollen 1
Calf swelling at least 3 cm larger than asymptomatic side 1
Pitting edema confined to symptomatic leg 1
Collateral superficial veins (nonvaricose) 1
Previously documented DVT 1
Alternative diagnosis at least as likely as DVT -2Wells et al, 1995
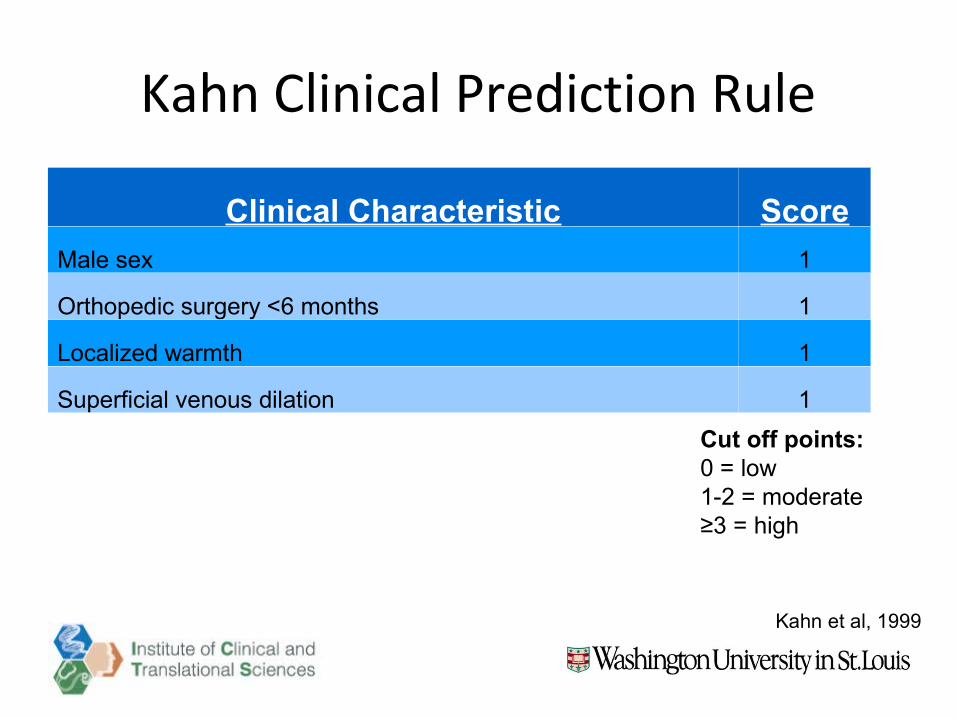
Kahn Clinical Prediction Rule
Clinical Characteristic Score
Male sex 1
Orthopedic surgery <6 months 1
Localized warmth 1
Superficial venous dilation 1
Cut off points:0 = low1-2 = moderate≥3 = high
Kahn et al, 1999
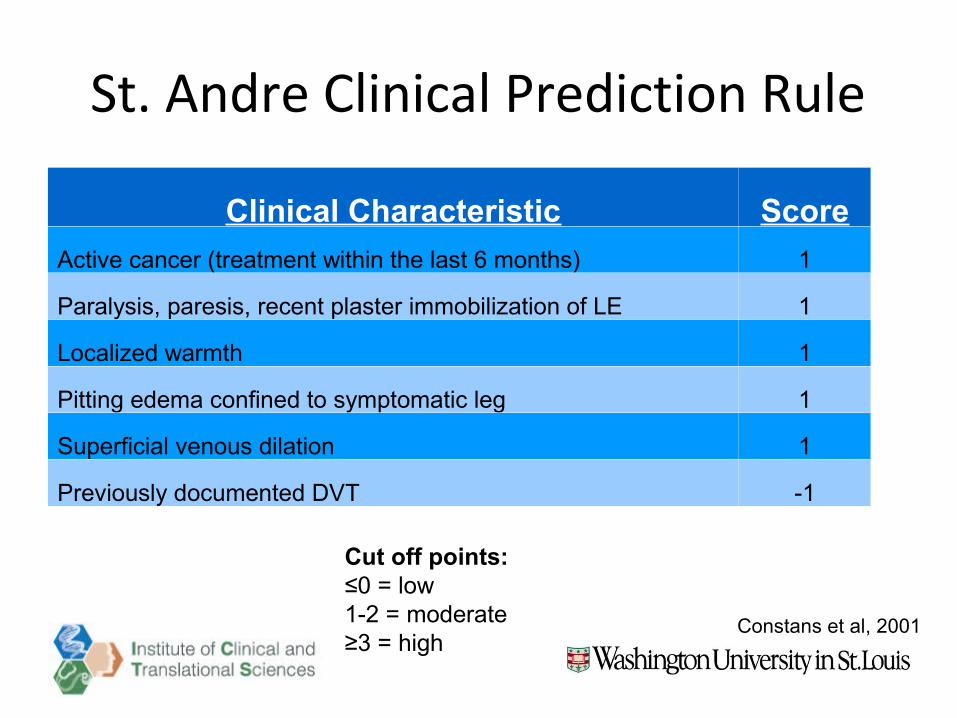
St. Andre Clinical Prediction Rule
Clinical Characteristic Score
Active cancer (treatment within the last 6 months) 1
Paralysis, paresis, recent plaster immobilization of LE 1
Localized warmth 1
Pitting edema confined to symptomatic leg 1
Superficial venous dilation 1
Previously documented DVT -1
Cut off points:≤0 = low1-2 = moderate≥3 = high
Constans et al, 2001
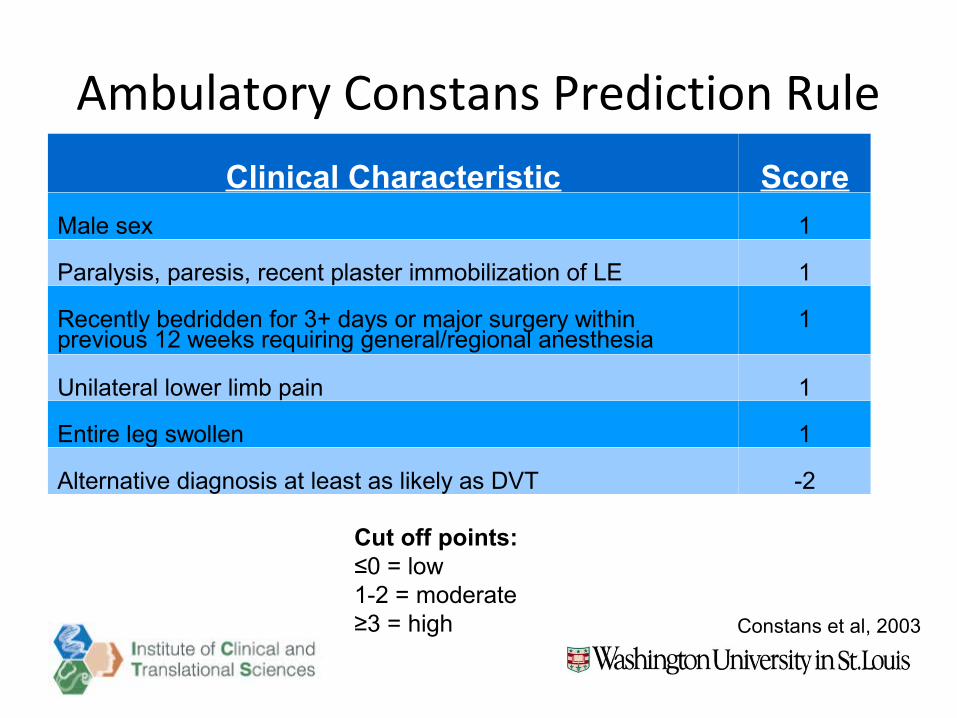
Ambulatory Constans Prediction RuleClinical Characteristic Score
Male sex 1
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia
1
Unilateral lower limb pain 1
Entire leg swollen 1
Alternative diagnosis at least as likely as DVT -2
Cut off points:≤0 = low1-2 = moderate≥3 = high Constans et al, 2003
LITERATURE REVIEW
Statistics Terminology
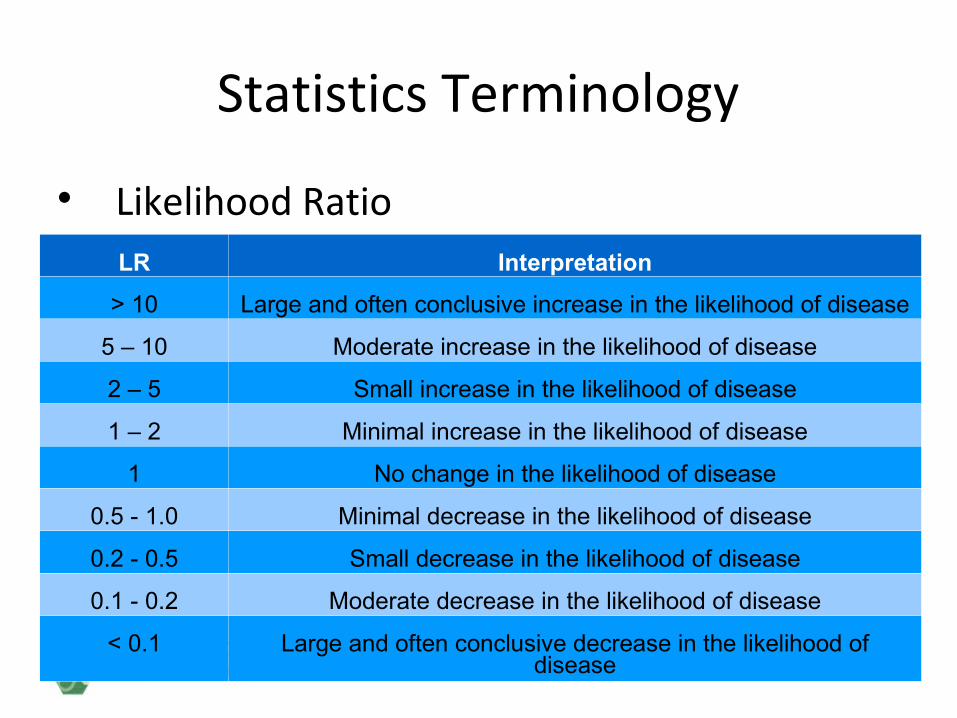
Likelihood Ratio – assesses usefulness of diagnostic test Positive (+LR) – corresponds to ruling in a
disease Negative(-LR) – corresponds to ruling out a
disease
Statistics Terminology
Likelihood RatioLR Interpretation
> 10 Large and often conclusive increase in the likelihood of disease
5 – 10 Moderate increase in the likelihood of disease
2 – 5 Small increase in the likelihood of disease
1 – 2 Minimal increase in the likelihood of disease
1 No change in the likelihood of disease
0.5 - 1.0 Minimal decrease in the likelihood of disease
0.2 - 0.5 Small decrease in the likelihood of disease
0.1 - 0.2 Moderate decrease in the likelihood of disease
< 0.1 Large and often conclusive decrease in the likelihood of disease
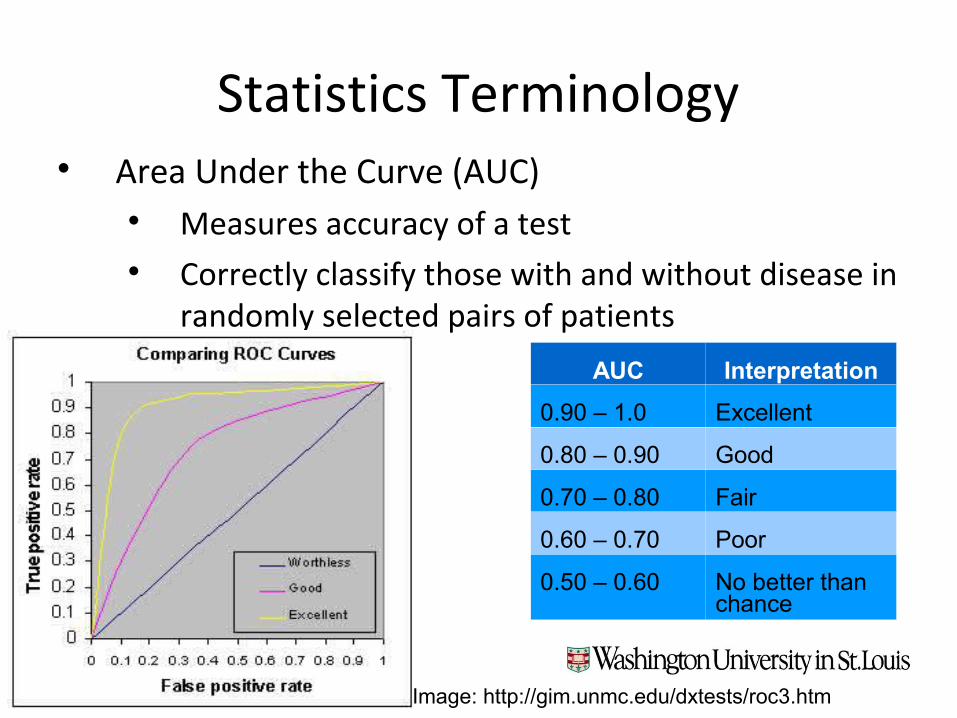
Statistics Terminology Area Under the Curve (AUC)
Measures accuracy of a test Correctly classify those with and without disease in
randomly selected pairs of patients
AUC Interpretation
0.90 – 1.0 Excellent
0.80 – 0.90 Good
0.70 – 0.80 Fair
0.60 – 0.70 Poor
0.50 – 0.60 No better than chance
Image: http://gim.unmc.edu/dxtests/roc3.htm
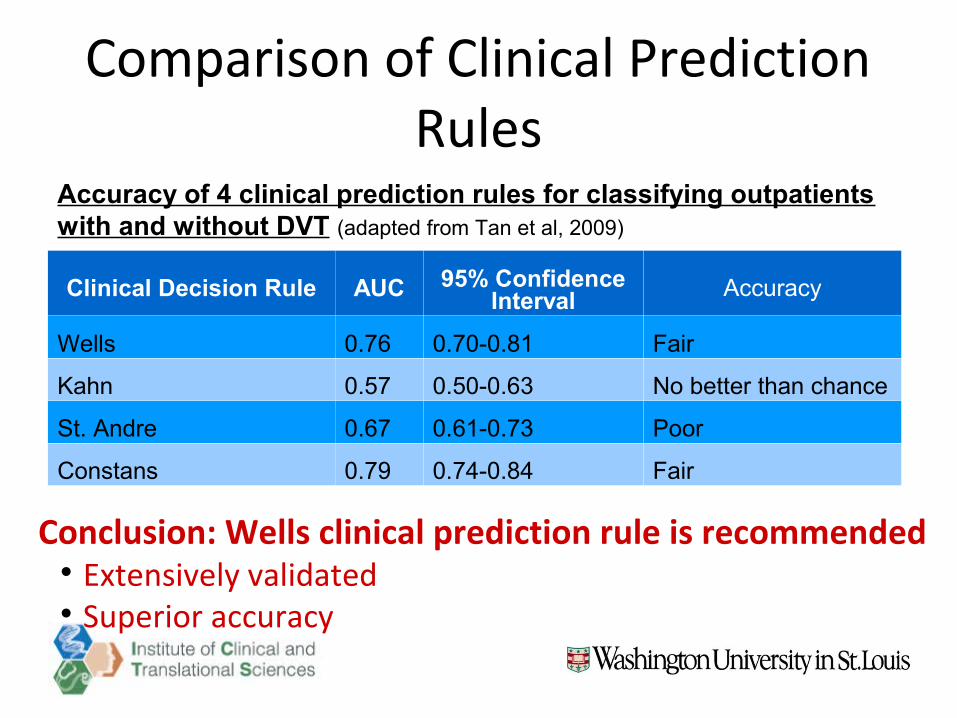
Comparison of Clinical Prediction Rules
Clinical Decision Rule AUC 95% Confidence Interval Accuracy
Wells 0.76 0.70-0.81 Fair
Kahn 0.57 0.50-0.63 No better than chance
St. Andre 0.67 0.61-0.73 Poor
Constans 0.79 0.74-0.84 Fair
Accuracy of 4 clinical prediction rules for classifying outpatients with and without DVT (adapted from Tan et al, 2009)
Conclusion: Wells clinical prediction rule is recommended Extensively validated Superior accuracy
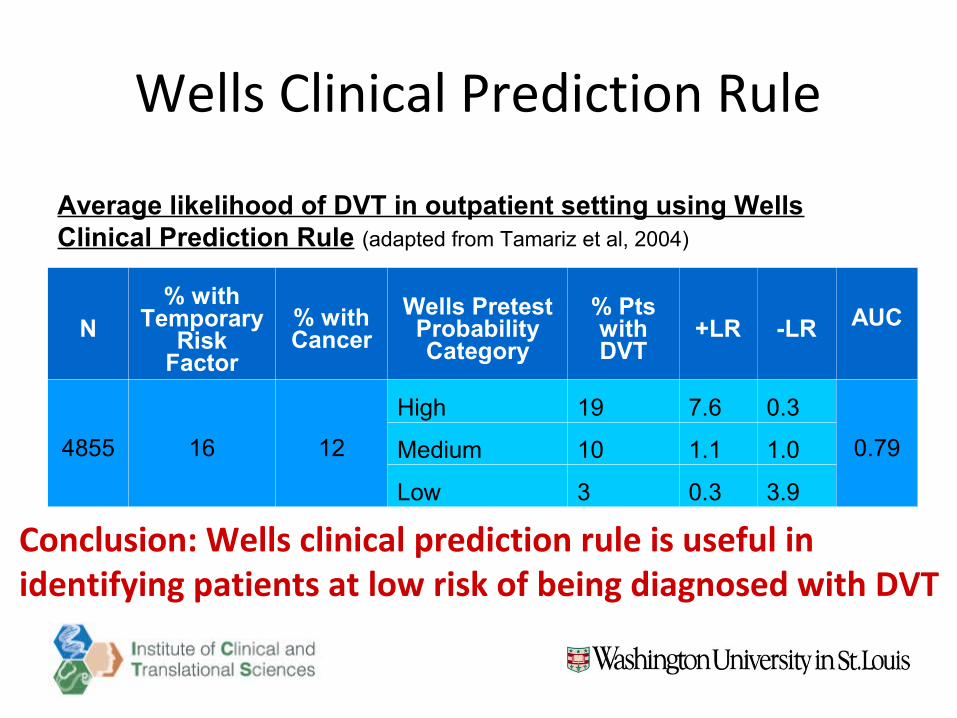
Wells Clinical Prediction Rule
N% with
Temporary Risk
Factor
% with Cancer
Wells Pretest Probability Category
% Pts with DVT
+LR -LR AUC
4855 16 12
High 19 7.6 0.3
0.79Medium 10 1.1 1.0
Low 3 0.3 3.9
Average likelihood of DVT in outpatient setting using Wells Clinical Prediction Rule (adapted from Tamariz et al, 2004)
Conclusion: Wells clinical prediction rule is useful in identifying patients at low risk of being diagnosed with DVT
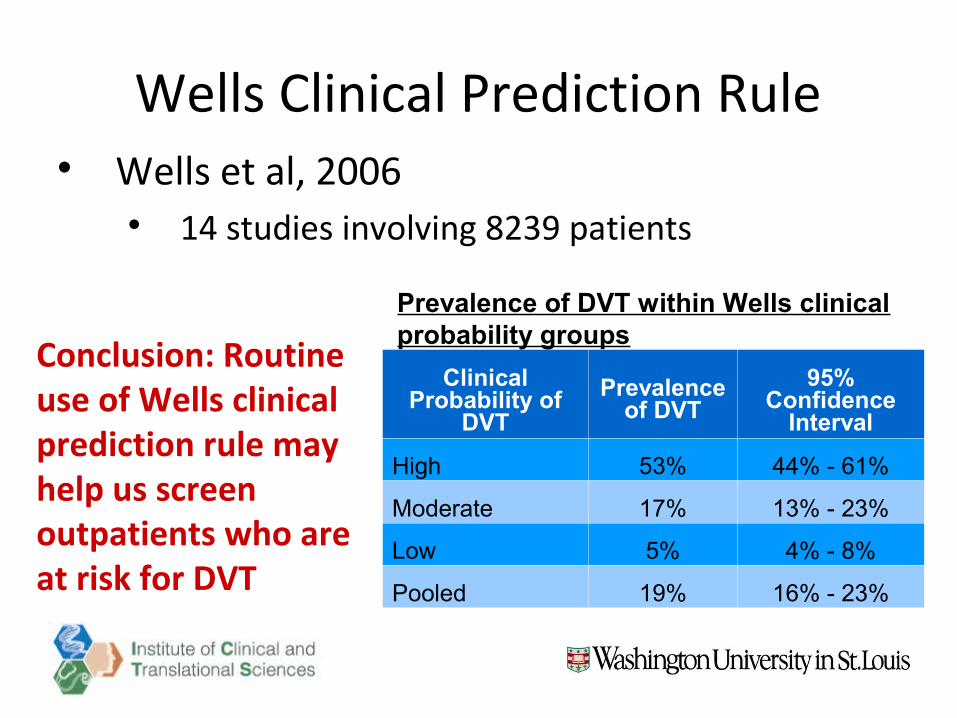
Wells Clinical Prediction Rule Wells et al, 2006
14 studies involving 8239 patients
Clinical Probability of
DVT
Prevalence of DVT
95% Confidence
Interval
High 53% 44% - 61%
Moderate 17% 13% - 23%
Low 5% 4% - 8%
Pooled 19% 16% - 23%
Prevalence of DVT within Wells clinical probability groups
Conclusion: Routine use of Wells clinical prediction rule may help us screen outpatients who are at risk for DVT
CLINICAL APPLICATION
Case Examples
CA 22 year old male PMH: obesity, L ACLR x 6 years ago Fell off mechanical bull, rupture ACLR,
medial/lateral menscus tears, patellar tendon tear
Case Examples CA
s/p L knee arthroscopy revision, ACLR bone-patellar-bone autograph, medial & lateral meniscal repair, patellar tendon repair, removal of medal hardware/screws/staples within bone (6/5/14)
Precautions• TDWB x 6 weeks (brace locked in extension)• Brace locked in extension x12 weeks• ROM 3x/week by PT only 0-90 deg x 12 weeks
Case Examples CA
– 6/6/14 (1 day s/p surgery)• 3-4/10 pain (Narco, Oxycontin, Keflex)
– 6/10 (5 days s/p surgery)• New c/o lateral calf pain (rest, TTP) 2/10• No warmth, swelling, redness, (-) Homans• Differential Diagnosis: DVT vs. muscle cramp
Use Wells Clinical Prediction Rule to determine likelihood of DVT. Would you refer him out?
Wells Clinical Prediction RuleClinical Characteristic Score
Active cancer (treatment within the last 6 months) 1
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia
1
Localized tenderness along distribution of deep venous system 1
Entire leg swollen 1
Calf swelling at least 3 cm larger than asymptomatic side 1
Pitting edema confined to symptomatic leg 1
Collateral superficial veins (nonvaricose) 1
Previously documented DVT 1
Alternative diagnosis at least as likely as DVT -2Cut off points:≤0 = low1-2 = moderate≥3 = high
Wells et al, 1995
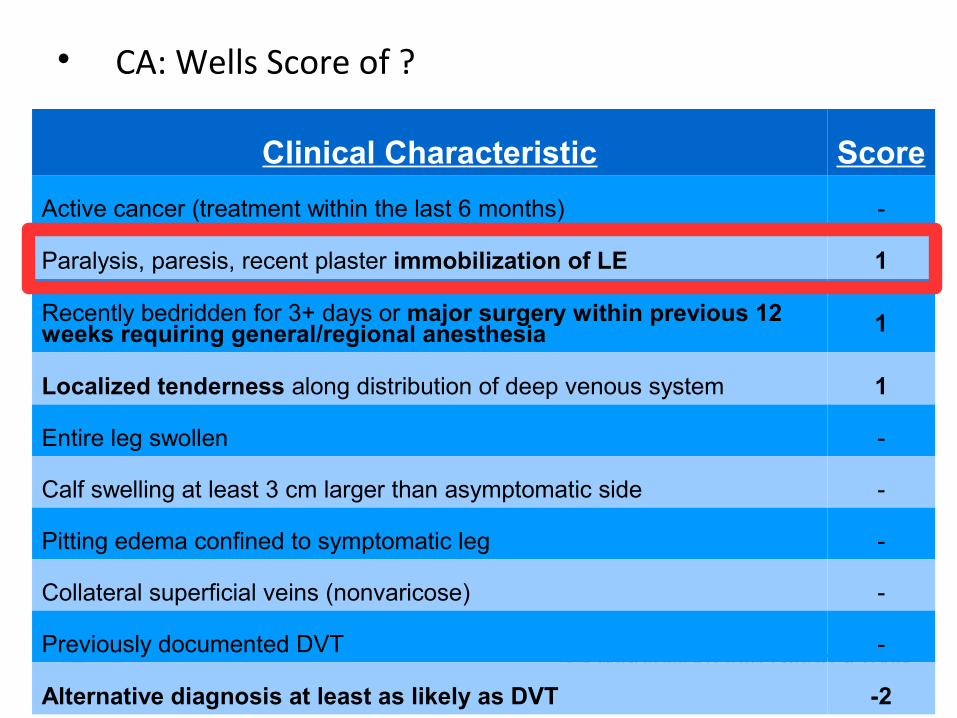
CA: Wells Score of ?
Clinical Characteristic Score
Active cancer (treatment within the last 6 months) -
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia 1
Localized tenderness along distribution of deep venous system 1
Entire leg swollen -
Calf swelling at least 3 cm larger than asymptomatic side -
Pitting edema confined to symptomatic leg -
Collateral superficial veins (nonvaricose) -
Previously documented DVT -
Alternative diagnosis at least as likely as DVT -2
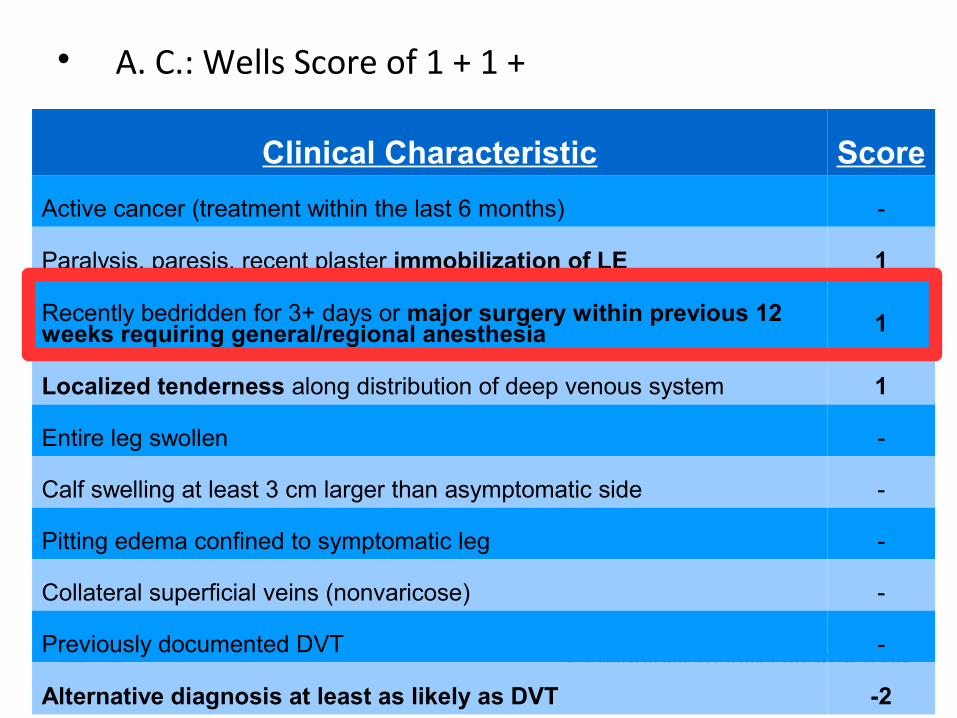
A. C.: Wells Score of 1 + 1 +
Clinical Characteristic Score
Active cancer (treatment within the last 6 months) -
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia 1
Localized tenderness along distribution of deep venous system 1
Entire leg swollen -
Calf swelling at least 3 cm larger than asymptomatic side -
Pitting edema confined to symptomatic leg -
Collateral superficial veins (nonvaricose) -
Previously documented DVT -
Alternative diagnosis at least as likely as DVT -2
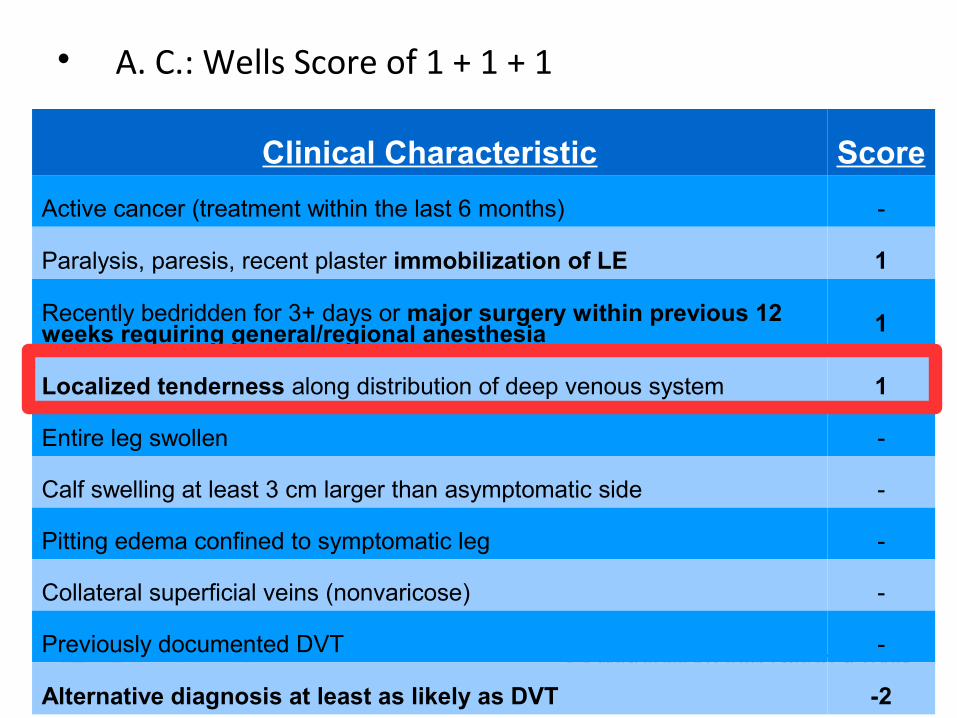
A. C.: Wells Score of 1 + 1 + 1
Clinical Characteristic Score
Active cancer (treatment within the last 6 months) -
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia 1
Localized tenderness along distribution of deep venous system 1
Entire leg swollen -
Calf swelling at least 3 cm larger than asymptomatic side -
Pitting edema confined to symptomatic leg -
Collateral superficial veins (nonvaricose) -
Previously documented DVT -
Alternative diagnosis at least as likely as DVT -2
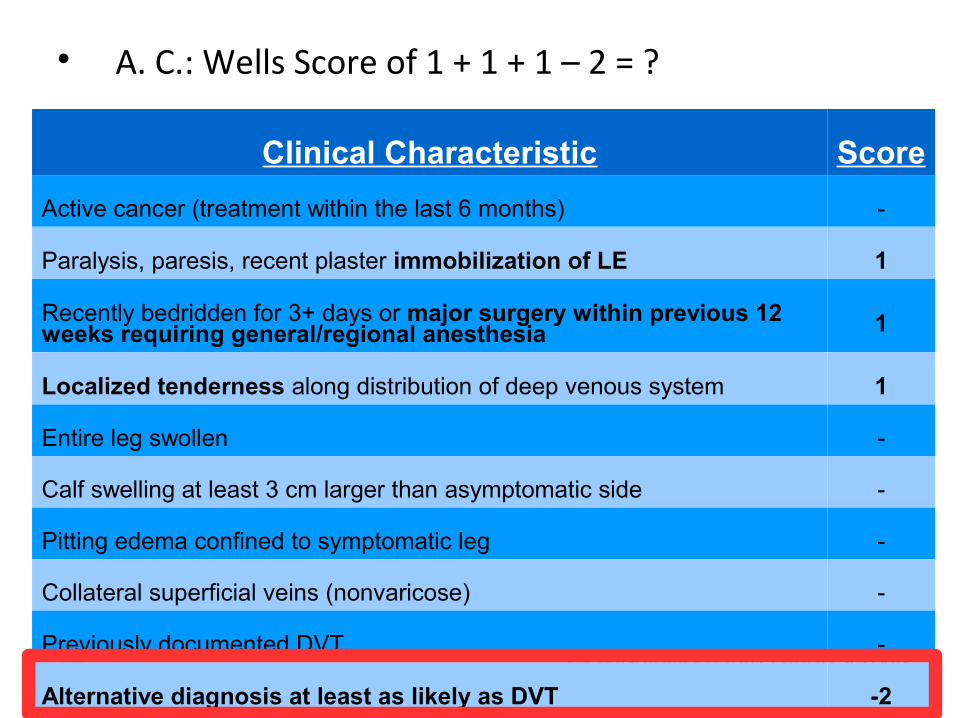
A. C.: Wells Score of 1 + 1 + 1 – 2 = ?
Clinical Characteristic Score
Active cancer (treatment within the last 6 months) -
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia 1
Localized tenderness along distribution of deep venous system 1
Entire leg swollen -
Calf swelling at least 3 cm larger than asymptomatic side -
Pitting edema confined to symptomatic leg -
Collateral superficial veins (nonvaricose) -
Previously documented DVT -
Alternative diagnosis at least as likely as DVT -2
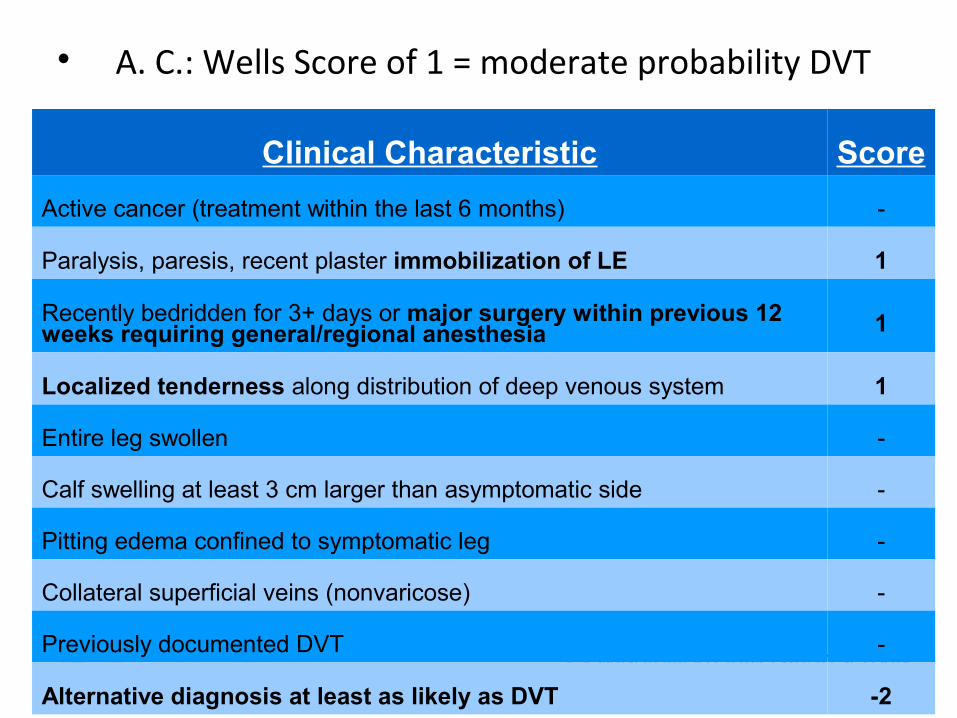
A. C.: Wells Score of 1 = moderate probability DVT
Clinical Characteristic Score
Active cancer (treatment within the last 6 months) -
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia 1
Localized tenderness along distribution of deep venous system 1
Entire leg swollen -
Calf swelling at least 3 cm larger than asymptomatic side -
Pitting edema confined to symptomatic leg -
Collateral superficial veins (nonvaricose) -
Previously documented DVT -
Alternative diagnosis at least as likely as DVT -2
Case Example
We referred CA to MD to rule out DVTGiven Narco, (-) Doppler US
Case Examples CA
– 6/16 (1.5 weeks s/p surgery)• Less calf pain but still TTP lateral gastroc• Insurance restrictions: PT 1x/week; ROM by
family daily
– 6/20 (2 weeks s/p surgery)• No calf pain
– 6/26 (3 weeks s/p surgery)• Only performed ROM once
Case Examples CA
– 7/10 (5 weeks s/p surgery)• L ankle pain (standing, walking, 2/10) for one
week, resolved prior to PT session• Mild edema posterior knee
– 7/18 (6 weeks s/p surgery)• New c/o inner thigh pain (walking, laying on R
side, 3/10), TTP adductors• Took Narco, no pain in knee/patellar tendon• Mild edema throughout LE• Able to reduce LE pain (1/10) with gait
training, adding padding to brace
Case Examples CA
– 7/24 (7 weeks s/p surgery)• No pain in LE after replacing padding in brace• Mild edema and redness throughout LE, no
warmth (reduced with elevation, STM)
Case Examples CA
– 7/28 (8 weeks s/p surgery)• 7/10 pain, pressure inner thigh, groin (rest,
movement, with/without brace), took Narco• Moderate-severe edema, redness throughout
LE, pitting edema near lateral patella• Hardness in calf, inner thigh, groin• Stopped activity, rested in bed during
weekend
Use Wells Clinical Prediction Rule to determine likelihood of DVT. Would you refer him out?
Wells Clinical Prediction RuleClinical Characteristic Score
Active cancer (treatment within the last 6 months) 1
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia
1
Localized tenderness along distribution of deep venous system 1
Entire leg swollen 1
Calf swelling at least 3 cm larger than asymptomatic side 1
Pitting edema confined to symptomatic leg 1
Collateral superficial veins (nonvaricose) 1
Previously documented DVT 1
Alternative diagnosis at least as likely as DVT -2
Cut off points:≤0 = low; 1-2 = moderate; ≥3 = high Wells et al, 1995
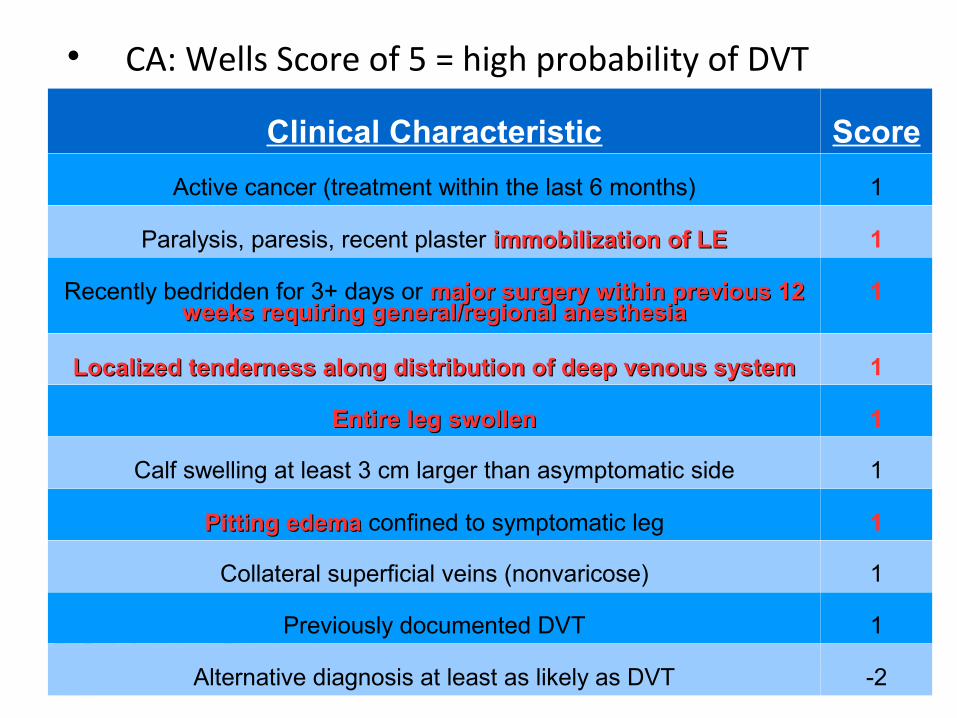
CA: Wells Score of 5 = high probability of DVT
Clinical Characteristic Score
Active cancer (treatment within the last 6 months) 1
Paralysis, paresis, recent plaster immobilization of LEimmobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 major surgery within previous 12 weeks requiring general/regional anesthesiaweeks requiring general/regional anesthesia
1
Localized tenderness along distribution of deep venous systemLocalized tenderness along distribution of deep venous system 1
Entire leg swollenEntire leg swollen 1
Calf swelling at least 3 cm larger than asymptomatic side 1
Pitting edemaPitting edema confined to symptomatic leg 1
Collateral superficial veins (nonvaricose) 1
Previously documented DVT 1
Alternative diagnosis at least as likely as DVT -2
Case Example
We referred CA to MD to rule out DVT
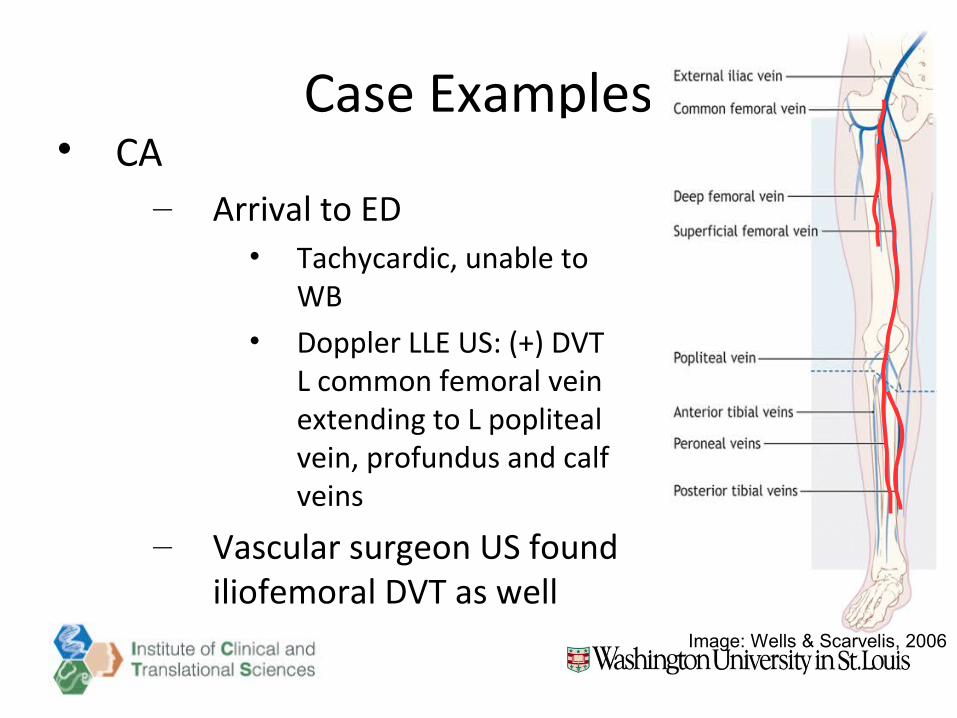
Case Examples CA
– Arrival to ED• Tachycardic, unable to
WB• Doppler LLE US: (+) DVT
L common femoral vein extending to L popliteal vein, profundus and calf veins
– Vascular surgeon US found iliofemoral DVT as well
Image: Wells & Scarvelis, 2006
Case Examples CA
– 7/31/14 (8.5 weeks s/p surgery)• Thrombolysis vascular surgery via venogram
(catherization of IVC)
– 8/25 (12 weeks s/p surgery)• US – non-occlusive obstruction of femoral and
popliteal vein, gastro vein; occlusive obstruction of soleal vein at mid calf. Resolved obstruction of common, external iliac, common, distal femoral veins
Case Examples
R. J. (Wells et al, 2006)
60 year old male Seeing you for knee pain Cut plantar aspect of L foot on glass 10 days
ago Resting in bed since
History of diabetes No history of previous DVT
Case Examples
R. J. (Wells et al, 2006)
Presentation L leg pain, mild calf swelling, redness, heat Febrile Pitting edema of L calf Erythema is hot, tender, well demarcated
Differential diagnosis: cellulitus vs. DVT Use Wells Clinical Prediction Rule to determine
likelihood of DVT. Would you refer him out?
Wells Clinical Prediction RuleClinical Characteristic Score
Active cancer (treatment within the last 6 months) 1
Paralysis, paresis, recent plaster immobilization of LE 1
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia
1
Localized tenderness along distribution of deep venous system 1
Entire leg swollen 1
Calf swelling at least 3 cm larger than asymptomatic side 1
Pitting edema confined to symptomatic leg 1
Collateral superficial veins (nonvaricose) 1
Previously documented DVT 1
Alternative diagnosis at least as likely as DVT -2
Wells et al, 1995
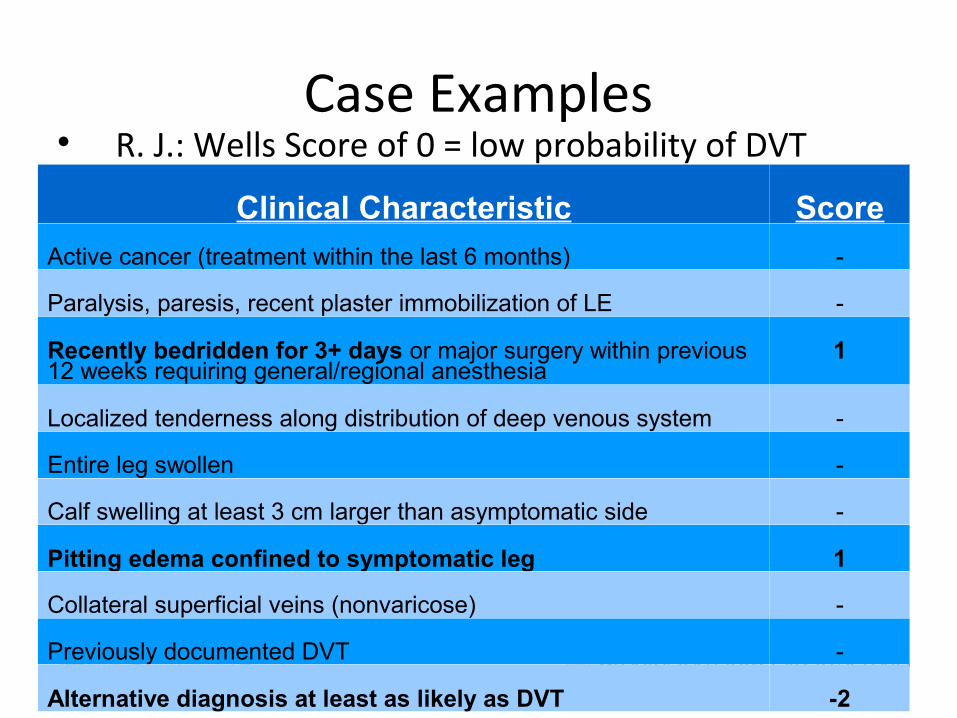
Case Examples R. J.: Wells Score of 0 = low probability of DVT
Clinical Characteristic Score
Active cancer (treatment within the last 6 months) -
Paralysis, paresis, recent plaster immobilization of LE -
Recently bedridden for 3+ days or major surgery within previous 12 weeks requiring general/regional anesthesia
1
Localized tenderness along distribution of deep venous system -
Entire leg swollen -
Calf swelling at least 3 cm larger than asymptomatic side -
Pitting edema confined to symptomatic leg 1
Collateral superficial veins (nonvaricose) -
Previously documented DVT -
Alternative diagnosis at least as likely as DVT -2
CONCLUSIONS
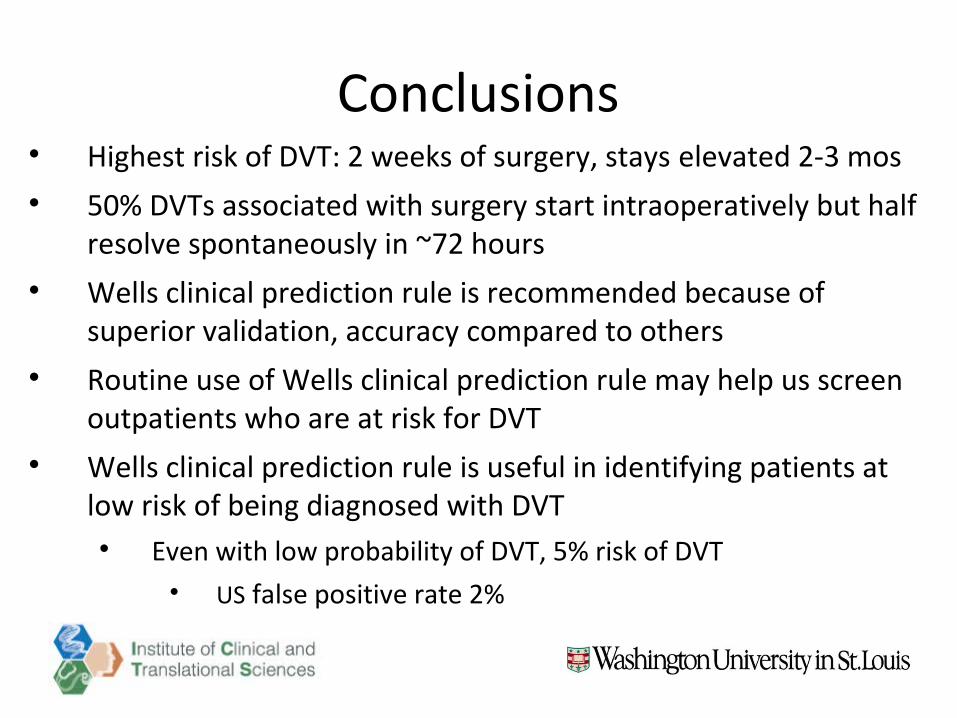
Conclusions Highest risk of DVT: 2 weeks of surgery, stays elevated 2-3 mos 50% DVTs associated with surgery start intraoperatively but half
resolve spontaneously in ~72 hours Wells clinical prediction rule is recommended because of
superior validation, accuracy compared to others Routine use of Wells clinical prediction rule may help us screen
outpatients who are at risk for DVT Wells clinical prediction rule is useful in identifying patients at
low risk of being diagnosed with DVT Even with low probability of DVT, 5% risk of DVT
US false positive rate 2%
ReferencesChilds JD, Cleland JA. Development and application of clinical prediction rules to improve decision
making in physical therapist practice. Phys Ther. 2006;86:122-131.
Constans J, Boutinet C, Salmi LR, Salby JC, Nelzy ML, Baudouin P et al. Comparison of four clinical prediction scores for the diagnosis of lower limb deep venous thrombosis in outpatients. Am J Med. 2003;115:436-440.
Constans J, Nelzy ML, Salmi LR, Skopinski S, Salby JC, Le Metayer P et al. Clinical prediction of lower limb deep vein thrombosis in symptomatic hospitalized patients. Thromb Haemostasis. 2001;86:985-990.
Kahn SR, Abenhaim JL, Leclerc JR. Clnical prediction of deep vein thrombosis in patients with leg: symptoms. Thromb Haemostasis. 1999;81:353-357.
Kearon C, Ginsberg JS, Hirsch J, The role of venous ultrasonography in the diagnosis of suspected deep venous thrombosis and pulmonary embolism. Ann Intern Med. 1998;129:1044-1049.
Kearon C. Natural history of venous thromboembolism. Circulation. 2003;107:I22-I33.
Oudega R, Hoes AW, Moons KGM. The Wells Rule does not adequately rule out deep vein thrombosis in primary care patients. Ann Intern Med. 2005;143:100-107.
ReferencesTamariz LJ, Eng J, Segal JB, Krishnan JA, Bolger DT, Streiff MB, et al. Usefulness of clinical prediction
rules for the diagnosis of venous thromboembolism: a systematic review. Am J Med. 2004;117:676-684.
Tan M, van Rooden CJ, Westerbeek RE, Huisman MV. Diagnostic management of clinically suspected acute deep vein thrombosis. Brit J Hematol. 2009;46:347-360.
Toll DB, Janssen KJM, Yergouwe Y, Moons KGM. Validation, updating and impact of clinical prediction rules: a review. J Clin Epidemiol. 2008;61:1085-1094.
Urbano FL. Homans' sign in the diagnosis of deep venous thrombosis. Hosp Physician. 2001:22-24.
van der Velede EF, Toll DB, ten Cate-Hock, Oudega R, Stoffers HEJH, Bossuyt PM et al. Comparing the diagnostic performance of 2 clinical decision rules to rule out deep vein thrombosis in primary care patients. Ann Fam Med. 2011;9:31-36.
Wells PS, Anderson DR, Rodger M, Forgie M, Dreyer J, Kovacs G. Evaluation of D-dimer in diagnosis of suspected deep-vein thrombosis. New Eng J Med. 2003;349(13):1227-1235.
Wells PS, Hirsh J, Anderson DR, Lensing AWA, Foster G, Kearon C, et al. Accuracy of clinical assessment of deep-vein thrombosis. Lancet. 1998;345:1330-1332.
Wells PS, Owen C, Doucette S, Fergusson D, Tran H. Does this patient have deep vein thrombosis? JAMA. 2006;295(2):199-207.

Questions??
Related Documents











