David Handojo Muljono, Eijkman Institute, Jakarta, Indonesia Molecular Diagnostics Symposium Himpunan Kimia Klinik Indonesia (HKKI) Jakarta, 8 April 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
David Handojo Muljono,
Eijkman Institute, Jakarta, Indonesia
Molecular Diagnostics Symposium
Himpunan Kimia Klinik Indonesia (HKKI)Jakarta, 8 April 2017
2
Common Viral Hepatitis
Hepatitis E virus
3
Lead to chronicity

• About 2000 million people have been
infected with hepatitis B virus:
– more than 240 million are chronically
infected,
– 500 000-700 000 annual deaths due
to HBV-related diseases
– 75% in Asia-Pacific region
– Indonesia: • 2007: Moderate-to-high endemicity (9.4%)
• 2013: Moderate endemicity (7.1%)
• About 130–170 million people are
chronically infected with hepatitis C
virus:– more than 350 000 people die from
HCV-related liver diseases each year.
– Indonesia: • 2013: 1.0% (provisional data)Anti-HCV (+): 1.0%
(Provisional data, 2013)
HBsAg (+): 7.1%
(Provisional data, 2013)

Leading Causes of Infectious Disease Deaths Worldwide (2010)
Disease Estimated Deaths per Year
Lower respiratory tract infections ~2.8 million
HIV/AIDS ~1.5 million
Viral Hepatitis ~1.4 million
Diarrheal diseases ~1.4 million
Tuberculosis ~1.2 million
Malaria ~1.2 million
Meningitis ~422,000
Measles ~125,000
Lozano et al. Lancet. Vol 380. 2012

Hepatitis B

Hepatitis B virus (HBV)
Small DNA virus consisting of
• Outer protein envelope containing
HBsAg
• Inner protein core (nucleocapsid)
containing HBV DNA
Gene and protein products:
• circular, double-stranded DNA with
4 ORFs:
– Gene S → Envelope (HBsAg)
– Gene C → Core (HBcAg)
– Gene P → Polymerase
– Gene X → X protein
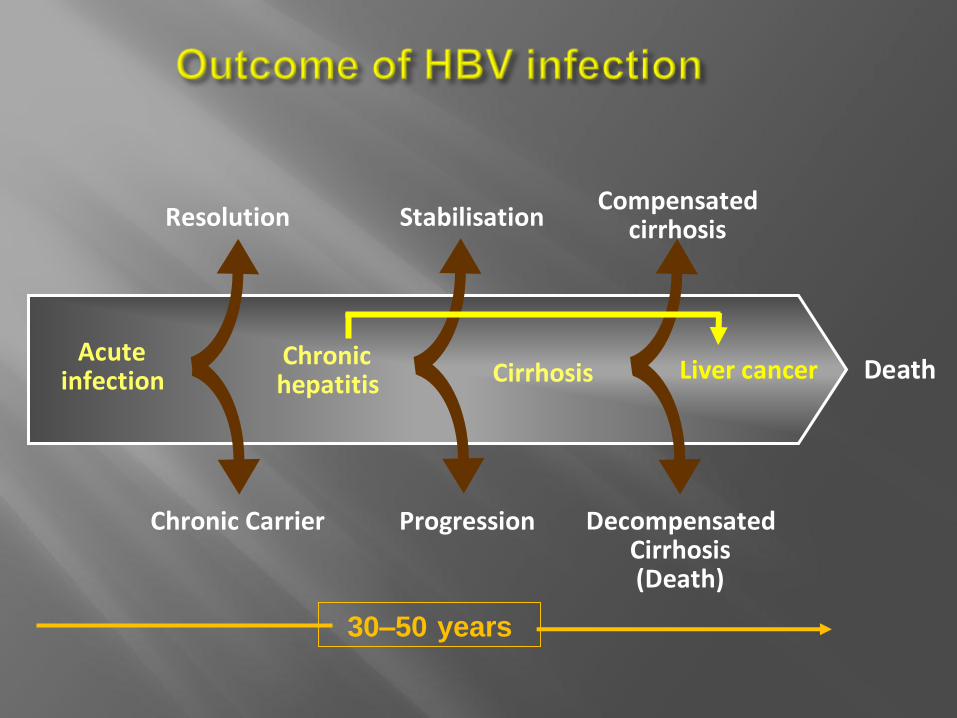
30–50 years
Acuteinfection
Chronic Carrier
Resolution
Chronichepatitis
Death
Stabilisation
Progression
Cirrhosis
Compensatedcirrhosis
Liver cancer
DecompensatedCirrhosis(Death)

•Host Virus
Manifestation of HBV Infection
is a result of Host and Virus interaction
• HBeAg status,
• HBV DNA titer
• HBV genotype,
• HBV mutants
• Gender
• Acquisition Age
• Immune system

Life cycle of hepatitis B virus
ICP = Intra cellular pathway
of cccDNA formation
No proof reading

Prone to mutation(2 x 10-5 / nucleotide / year)
Surviving variants/mutants will face
the host immune response/antivirus
Most mutants are lethal
Compact genomic structure(Overlapping ORF)
After selection by host immune system/
antivirus:
Variants / mutants
Life cycle of hepatitis B virus
Mutants in Gene S, P, X
and C
• Genotype: A to J
• Subtype: adw, adr, ayw, ayr
and many genotype/subtype
members
No proof reading
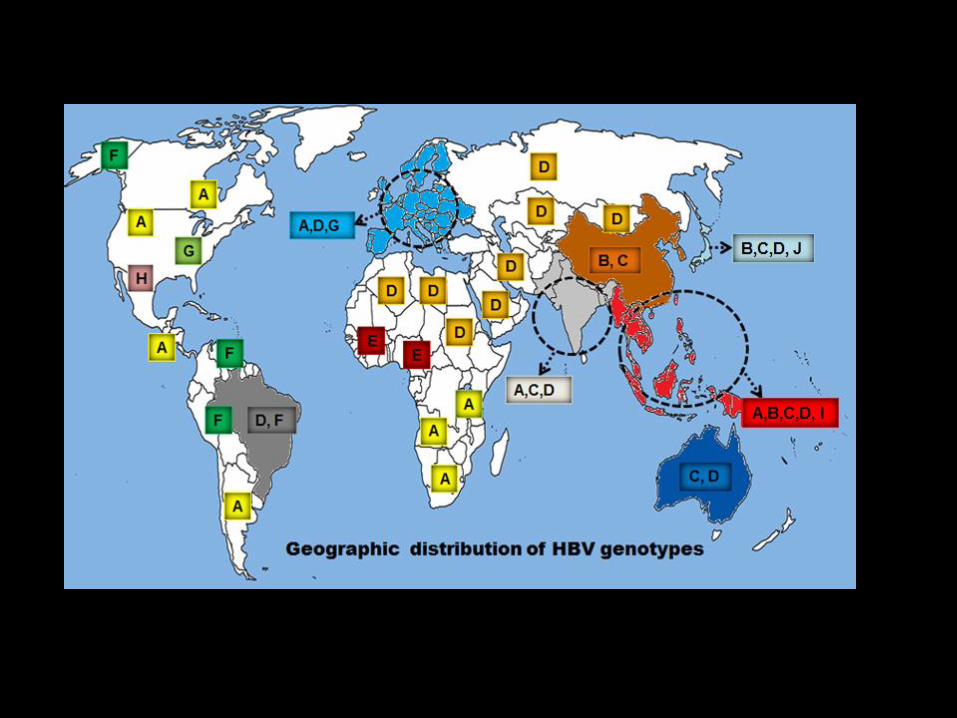


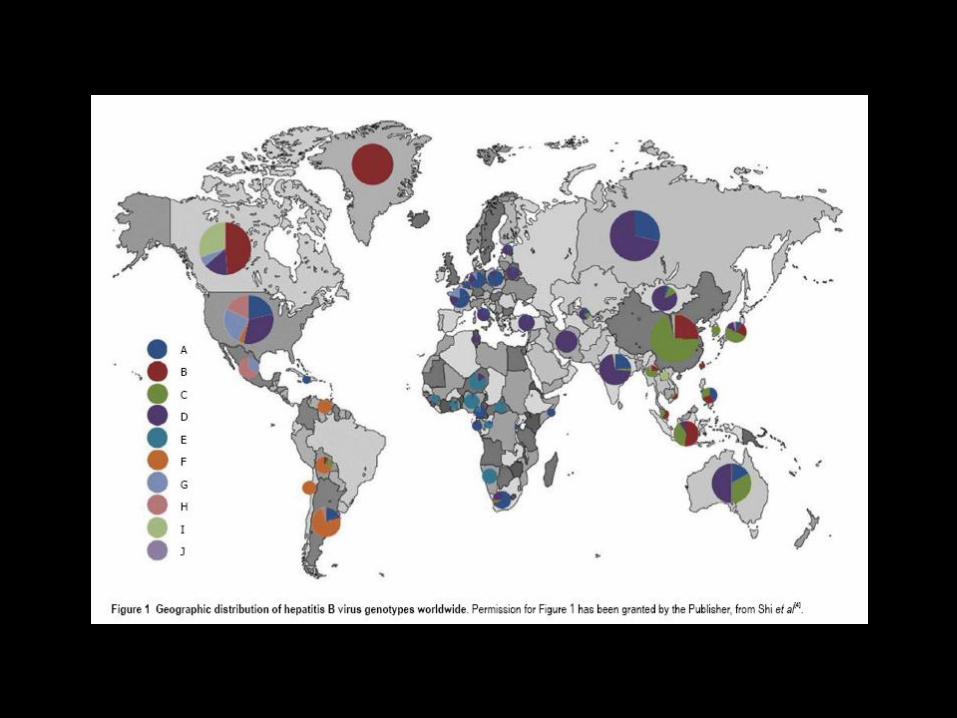
Distribution of HBV
genotype/subgenotype in ethnic populations of the Indonesian archipelago:
- B: dominant in the west
- C: dominant in the east
Genotype C
Genotype B
Genotype D
Genotype A
* Indonesian of Chinese ethnic origin
*
a
Balinese and Lombok
Sumbanese Flores
Alorese
Minahasa
and Talaud Ternate and Ambonese
C1
C5
BatakB2
B3
B7B9
C2
Malay
C2B3
B9
C1B2
B3
B8B9
C1C2
B3
B7
B5
B8B9
B3B5
B7B9
C2C1 Papuan
C1C2
C6
B3B7
Indonesian of Chinese ethnic origin
B2
B3B5
C1C2
B3B5
B8
B9
Nias and Mentawai
Minang
B3
C5
B7
b
Makasarese C1C2
B2B3B5B8B9
C1
C2
Javanese
B5
B3
B7
C1
B7B5
B8
B9
C1
C2
Torajan and Mandar
B3
B7
C1C2
B5
B3
B5B7B9

Genotype A B C D E-J
Clinical characteristics
• Modes of transmission Horizontal Perinatal/Vertical Perinatal/Vertical Horizontal Horizontal
• Tendency of chronicity Higher Lower Higher Lower ND
• Positivity of HBeAg Higher Lower Higher Lower ND
• HBeAg Seroconversion Earlier Earlier Later Later ND
• HBsAg seroclearance More More Less Less ND
• Histologic activity Lower Lower Higher Higher ND
• Clinical outcomes (LC and HCC) Better Better Worse Worse Worse in F
• Response to interferon α Higher Higher Lower Lower Lower in G
• Response to nucleos(t)ide analogues No significant differences among genotypes A to D ND
Virological characteristics
• Serum HBV DNA level ND Lower Higher ND ND
• Frequency of precore A1896 mutation Lower Higher Lower Higher ND
• Frequency of BCP T1762/A1764 mutation Higher Lower Higher Lower ND
• Frequency of preS deletion mutation ND Lower Higher ND ND
Comparison of clinical and virological features
among hepatitis B virus genotypes

‘a’ determinant (124-147)
Detection failure in regular blood donor
Thedja et al., 2010

HBV Genotyping Methods
1. Sequencing and phylogenetic analysis
– The definitive method for HBV genotyping
– defined by an inter-group divergence of >8% in the complete genome
sequence, and of >4% in the S gene
2. Restriction fragment length polymorphisms (RFLP),
– based on the amplification of an S gene amplicon followed by restriction
digestion
3. Polymerase Chain Reaction (PCR)
– PCR with specific primers for single genotypes
– Multiplex-PCR for many HBV genotypes,
4. Hybridization technologies
– HBV DNA is mplified using PCR primers complementary to a conserved
region in the PreS1 region of the HBV genome, then hybridised with
genotypic specific oligonucleotides on membrane strips.
5. Serological Method
– Enzyme-linked immunosorbent assay (ELISA) by identifying immune epitopes within the pre-S2 region using monoclonal antibodies

Hepatitis C

Hepatitis C Virus
• Single-shelled RNA Virus of
Flaviviridae family
10 protein products
- Structure: C, E, (p7)
- Function: NS2, NS3, NS4,
NS5
Genetic structure
• 9600 bp RNA,
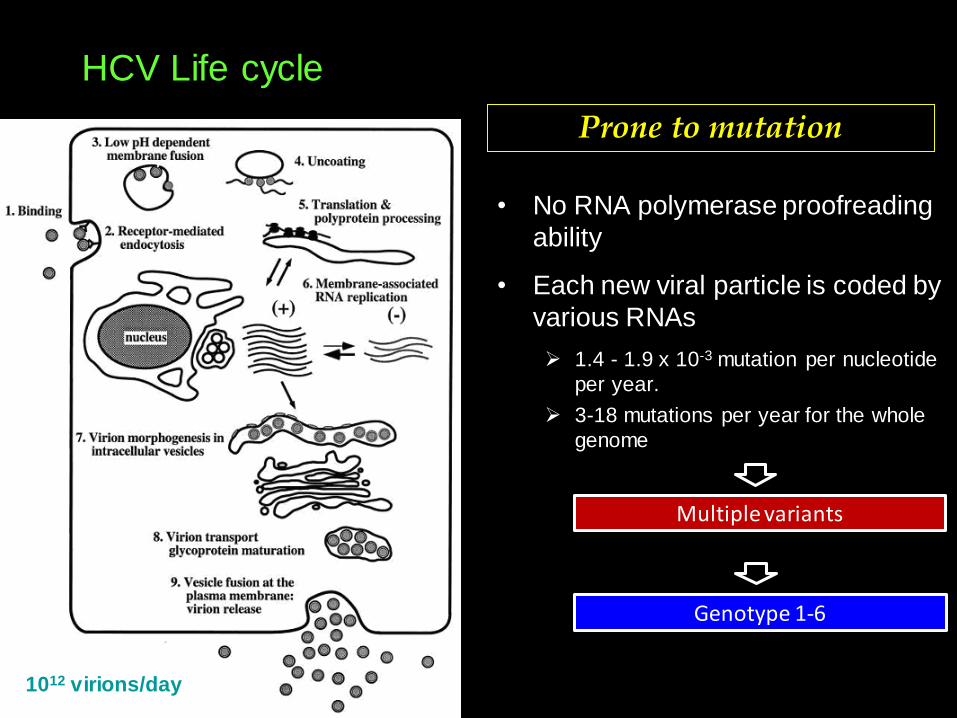
• No RNA polymerase proofreading
ability
• Each new viral particle is coded by
various RNAs
1.4 - 1.9 x 10-3 mutation per nucleotide
per year.
3-18 mutations per year for the whole
genome
Prone to mutation
1012 virions/day
HCV Life cycle
Multiple variants
Genotype 1-6
1 3
2
4 5
6
c
a da
lb
10a
ac
cb
bc
ad
ef
a
ceg
b a6a
6b c
ba
11a
6a6b
9c9b9a
d7
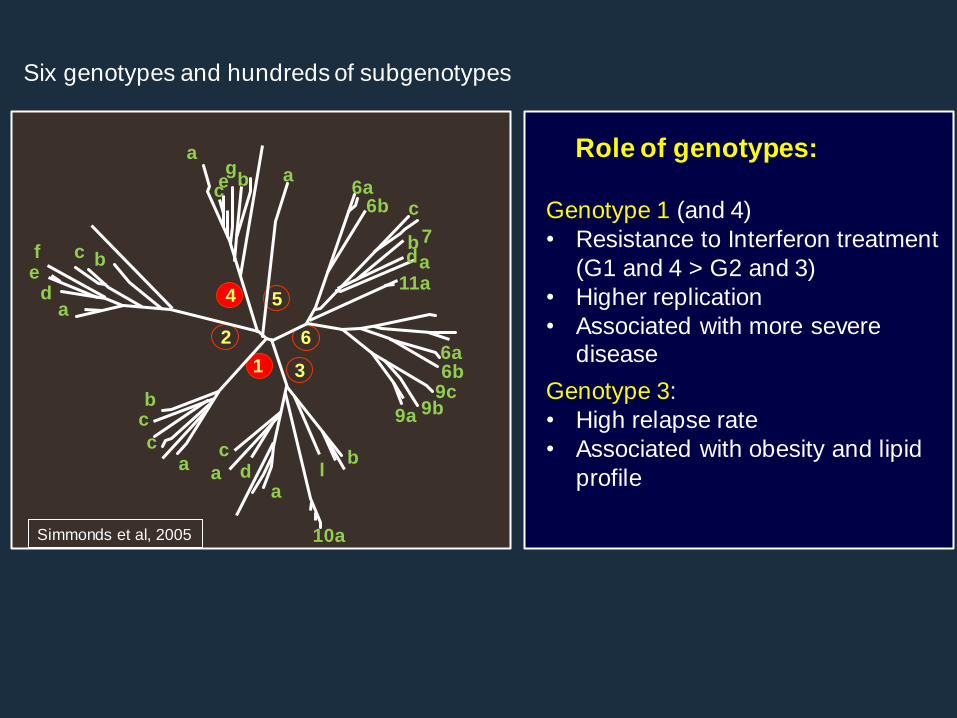
Six genotypes and hundreds of subgenotypes
Simmonds et al, 2005
Genotype 1 (and 4)
• Resistance to Interferon treatment
(G1 and 4 > G2 and 3)
• Higher replication
• Associated with more severe disease
Genotype 3:
• High relapse rate
• Associated with obesity and lipid
profile
Role of genotypes:
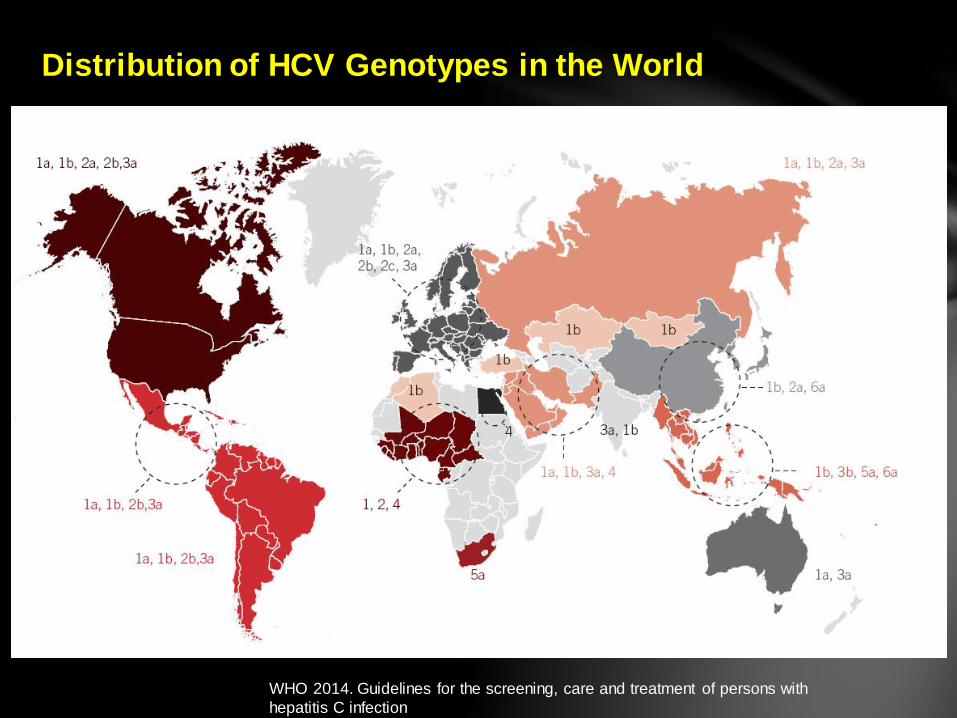
Distribution of HCV Genotypes in the World
WHO 2014. Guidelines for the screening, care and treatment of persons with
hepatitis C infection
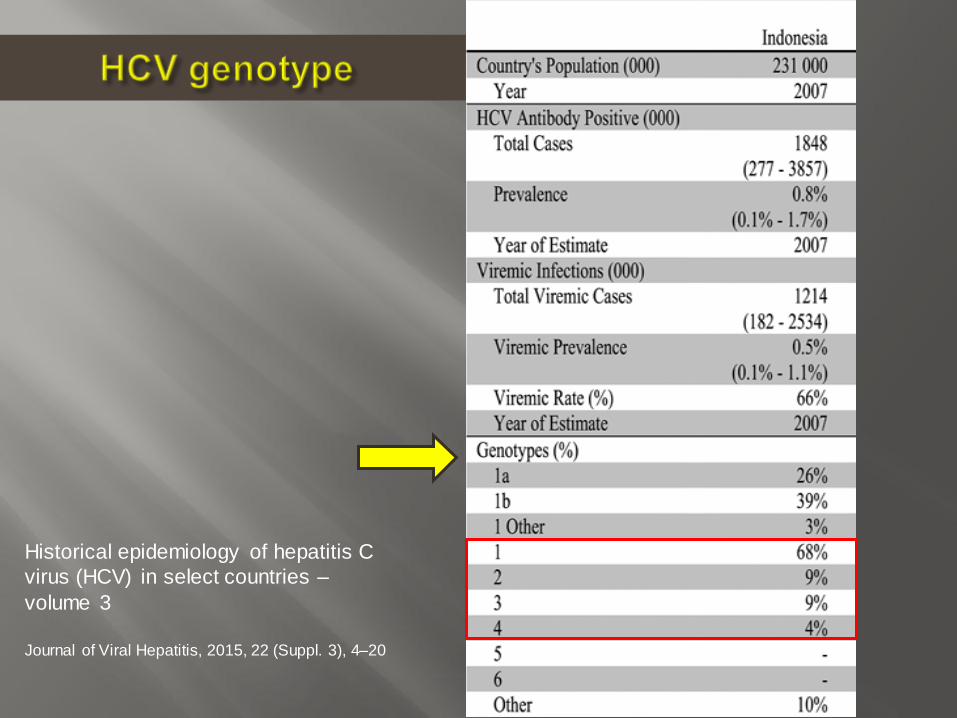
Historical epidemiology of hepatitis C
virus (HCV) in select countries –
volume 3
Journal of Viral Hepatitis, 2015, 22 (Suppl. 3), 4–20
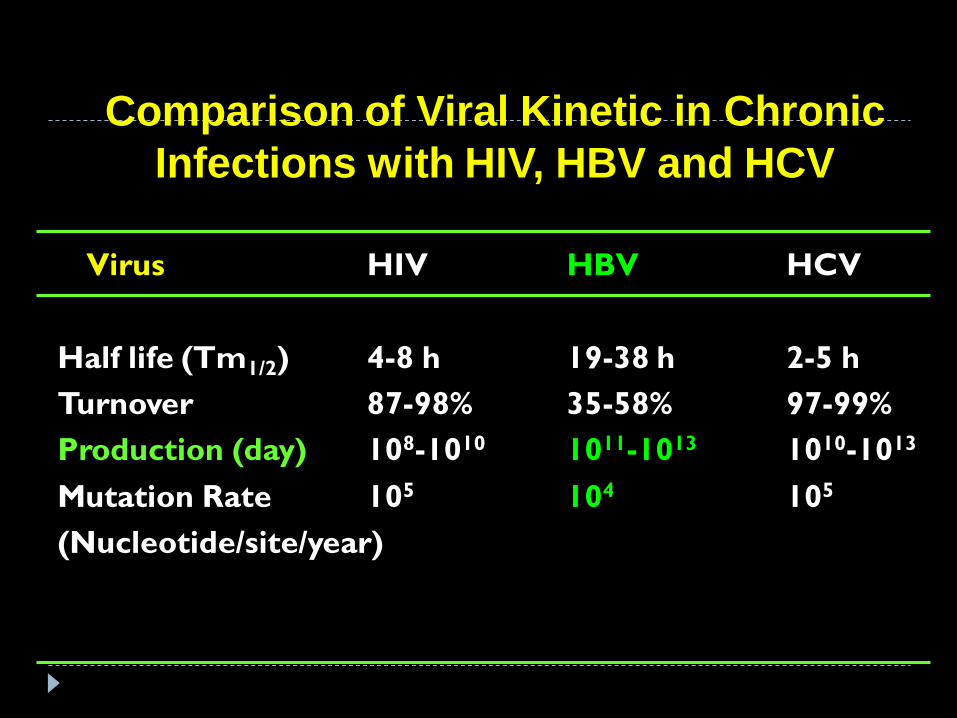
Comparison of Viral Kinetic in Chronic
Infections with HIV, HBV and HCV
Virus HIV HBV HCV
Half life (Tm1/2) 4-8 h 19-38 h 2-5 h
Turnover 87-98% 35-58% 97-99%
Production (day) 108-1010 1011-1013 1010-1013
Mutation Rate 105 104 105
(Nucleotide/site/year)

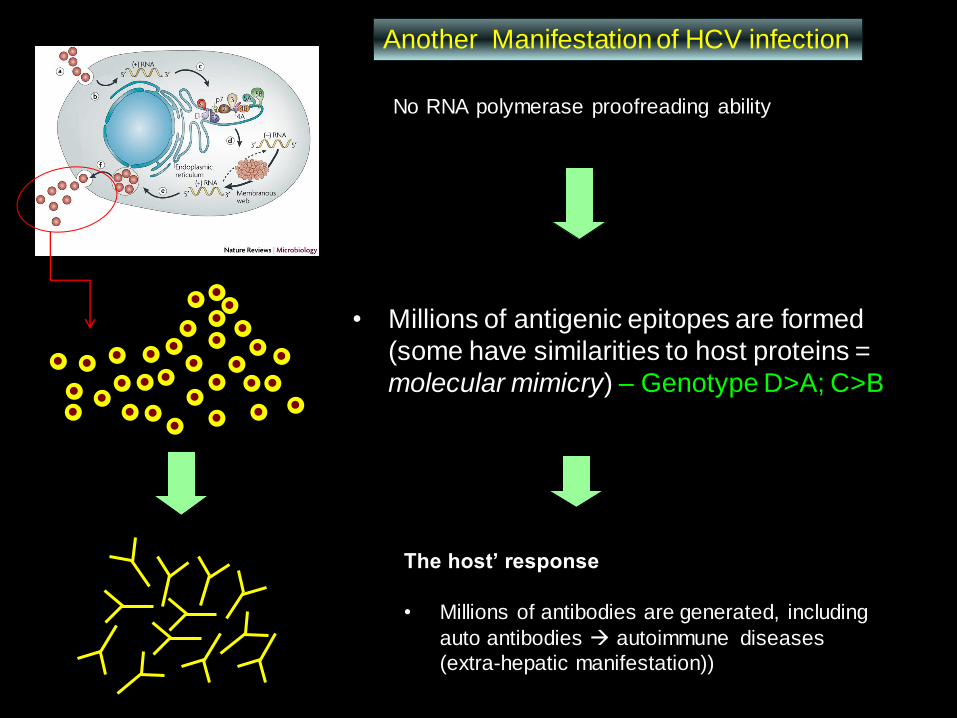
• Millions of antigenic epitopes are formed
(some have similarities to host proteins =
molecular mimicry) – Genotype D>A; C>B
The host’ response
• Millions of antibodies are generated, including
auto antibodies autoimmune diseases
(extra-hepatic manifestation))
No RNA polymerase proofreading ability
Another Manifestation of HCV infection
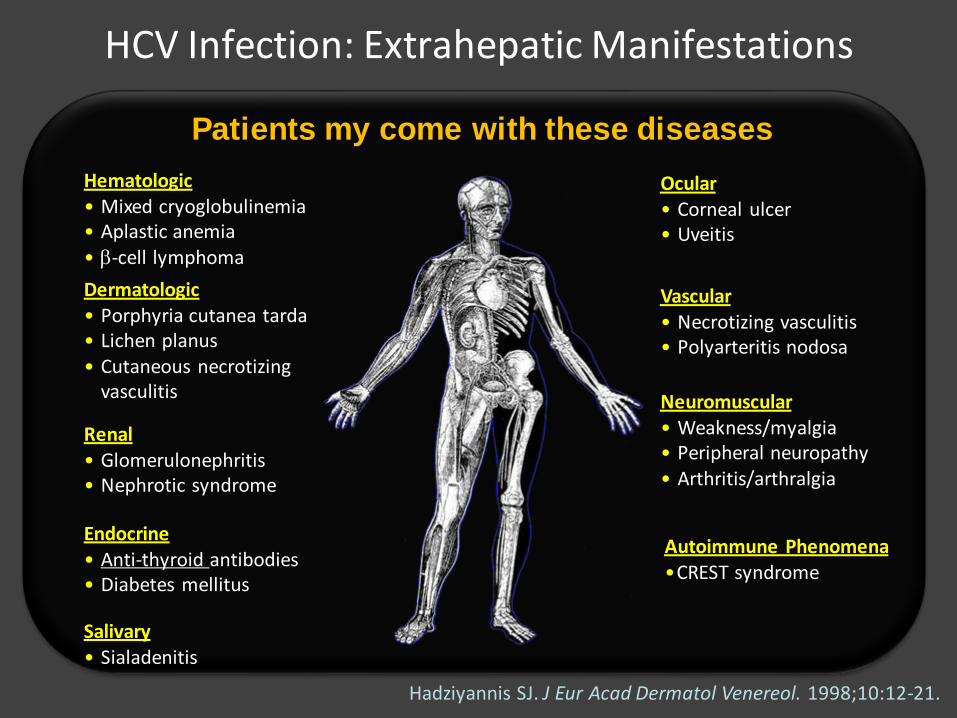
Hadziyannis SJ. J Eur Acad Dermatol Venereol. 1998;10:12-21.
HCV Infection: Extrahepatic Manifestations
Hematologic• Mixed cryoglobulinemia• Aplastic anemia• -cell lymphoma
Dermatologic• Porphyria cutanea tarda• Lichen planus• Cutaneous necrotizing
vasculitis
Renal• Glomerulonephritis• Nephrotic syndrome
Endocrine• Anti-thyroid antibodies• Diabetes mellitus
Salivary• Sialadenitis
Ocular• Corneal ulcer• Uveitis
Vascular• Necrotizing vasculitis• Polyarteritis nodosa
Neuromuscular• Weakness/myalgia• Peripheral neuropathy• Arthritis/arthralgia
Autoimmune Phenomena•CREST syndrome
Patients my come with these diseases

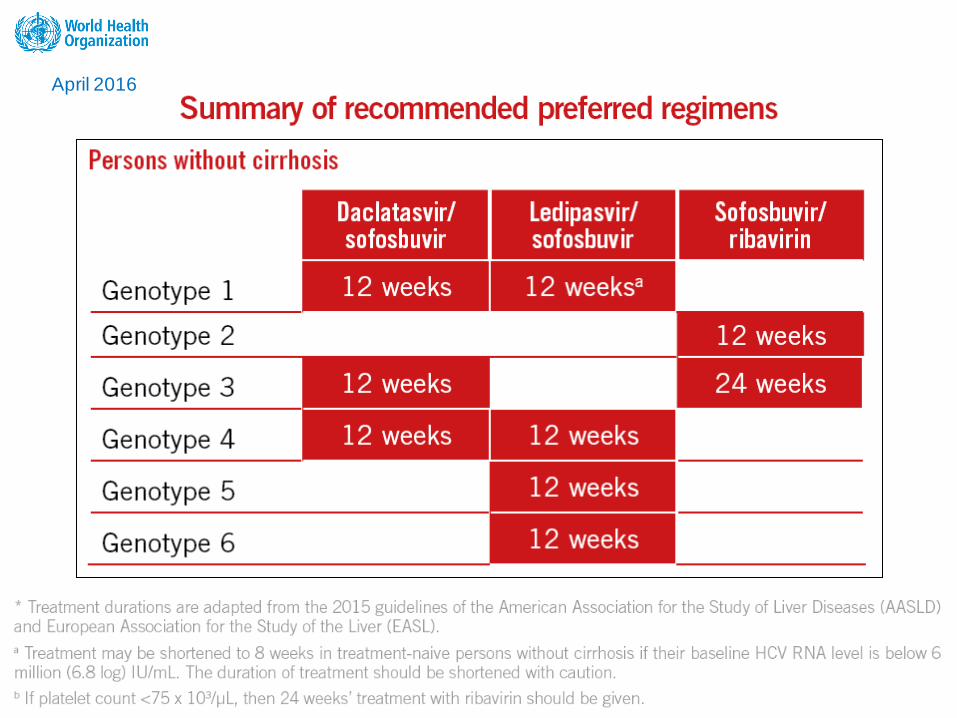
Source: WHO 2014. Guidelines for the screening, care and
treatment of persons with hepatitis C infection
Manifestation of HCV infection


April 2016
April 2016

April 2016

April 2016

2014 2017Perhimpunan Peneliti Hati Indonesia (PPHI)

Available DAAs (in Indonesia)

Terapi Hepatitis C (DAA):
Tanpa Sirosis
GTPegIFN,
RBVPegIFN,RBV,SOF
PegIFN,RBV,SIM
SOF,RBV
SOF/LED
SOF,DAC
SOF,SIM
ELB/GRA
SOF/VEL
1
Response guided
12 24-48* - 12 12 1212**
16 (+RBV)***12
2 12 - 12 12 12 - - 12
3 12 - 24 - 12 - - 12
4 12 24-48* - 12 12 1212
16 (+RBV)***12
5 12 - - 12 12 - - 12
6 12 - - 12 12 - - 12
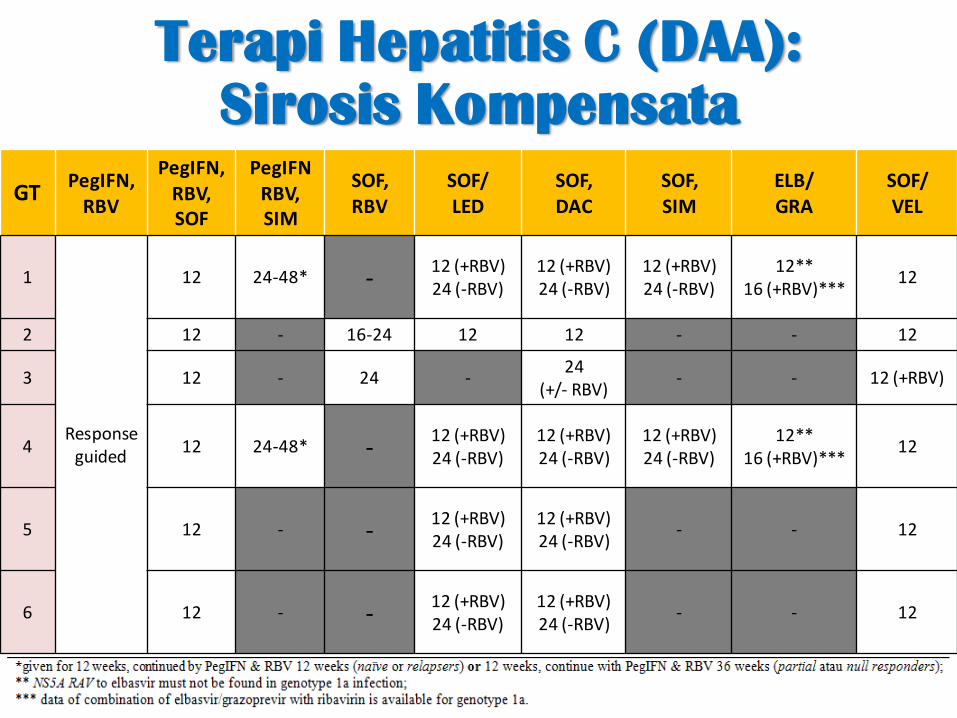
Terapi Hepatitis C (DAA):
Sirosis Kompensata
GTPegIFN,
RBV
PegIFN,RBV,SOF
PegIFNRBV,SIM
SOF,RBV
SOF/LED
SOF,DAC
SOF,SIM
ELB/GRA
SOF/VEL
1
Response guided
12 24-48* -12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
12**16 (+RBV)***
12
2 12 - 16-24 12 12 - - 12
3 12 - 24 -24
(+/- RBV)- - 12 (+RBV)
4 12 24-48* -12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
12**16 (+RBV)***
12
5 12 - -12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
- - 12
6 12 - -12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
- - 12

Terapi Hepatitis C (DAA):
Sirosis Dekompensata
GTPegIFN,
RBVPegIFN,RBV,SOF
PegIFN,RBV,SIM
SOF,RBV
SOF,LED
SOF,DAC
SOF,SIM
ELB/GRA
SOF,VEL
1
KontraIndikasi
KontraIndikasi
KontraIndikasi
-12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
KontraIndikasi
KontraIndikasi
12 (+RBV)24 (-RBV)
2 16-20 -12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
3 - - 24 (+/-RBV) 24 (+/-RBV)
4 -12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
5 -12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
6 -12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)
12 (+RBV)24 (-RBV)

1. Sequencing and phylogenetic analysis
• The best genotyping method, by sequencing the most conserved regions
– The 5’ untranslated region (5’ UTR),
– The 3’untranslated region.
2. Several commercial assays:
• TruGene 5’ NC HCV Genotyping kit (Siemens, Tarrytown, NY, USA):
– based on direct sequence analysis of the 5’UTR (untranslated region);
• VERSANT HCV Genotype Assay (LiPA) 2.0 (Siemens, Tarrytown, NY, USA),
reverse hybridization line-probe assay targeting the 5’ UTR and core regions
• Abbott m2000 Real-Time HCV Genotype II assay (Abbott Molecular Inc., Des
Plaines, IL, USA):
– PCR-based assay targeting specific regions of the 5’NCR and the NS5B genes
3. Newly developed methods:
• Liquid Microarray
– based on liquid microarray technology (xMAP Technology, Luminex Corp, Texas).
• Next generation sequencing (NGS)
– Perform rapid and mass sequencing, and distinguish viral population from a single host
HCV Genotyping Methods

Thank you
Related Documents











