Diabetes mellitus Diabetes mellitus (pronounced /ˌdaɪ.əˈbiːtiːz/ or /ˌdaɪ.ə ˈbiːtis/; /miˈlaɪtəs/ or /ˈmɛlitəs/)—often simply referred to as diabetes—is a condition in which a person has a high blood sugar (glucose) level as a result of the body either not producing enough insulin , or because body cells do not properly respond to the insulin that is produced. Insulin is a hormone produced in the pancreas which enables body cells to absorb glucose, to turn into energy. If the body cells do not absorb the glucose, the glucose accumulates in the blood (hyperglycemia ), leading to various potential medical complications. [2] [3] There are many types of diabetes, [3] the most common of which are: Type 1 diabetes : results from the body's failure to produce insulin, and presently requires the person to inject insulin. Type 2 diabetes : results from insulin resistance , a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. Gestational diabetes : is when pregnant women, who have never had diabetes before, have a high blood glucose level during pregnancy. It may precede development of type 2 DM. Other forms of diabetes mellitus include congenital diabetes, which is due to genetic defects of insulin secretion, cystic fibrosis-related diabetes, steroid diabetes induced by high doses of glucocorticoids, and several forms of monogenic diabetes . All forms of diabetes have been treatable since insulin became medically available in 1921, and type 2 diabetes can be controlled with tablets, but it is chronic condition that usually cannot be cured. Pancreas transplants have been tried with limited success in type 1 DM; gastric bypass surgery has been successful in many with morbid obesity and type 2 DM; and gestational diabetes usually resolves after delivery. Diabetes

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Diabetes mellitusDiabetes mellitus (pronounced /ˌdaɪ.əˈbiːtiːz/ or /ˌdaɪ.əˈbiːtɨs/; /mɨˈlaɪtəs/ or /ˈmɛlɨtəs/)—often simply referred to as diabetes—is a condition in which a person has a high blood sugar (glucose) level as a result of the body either not producing enough insulin, or because body cells do not properly respond to the insulin that is produced. Insulin is a hormone produced in the pancreas which enables body cells to absorb glucose, to turn into energy. If the body cells do not absorb the glucose, the glucose accumulates in the blood (hyperglycemia), leading to various potential medical complications.[2][3]
There are many types of diabetes,[3] the most common of which are:
Type 1 diabetes : results from the body's failure to produce insulin, and presently requires the person to inject insulin.
Type 2 diabetes : results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency.
Gestational diabetes : is when pregnant women, who have never had diabetes before, have a high blood glucose level during pregnancy. It may precede development of type 2 DM.
Other forms of diabetes mellitus include congenital diabetes, which is due to genetic defects of insulin secretion, cystic fibrosis-related diabetes, steroid diabetes induced by high doses of glucocorticoids, and several forms of monogenic diabetes.
All forms of diabetes have been treatable since insulin became medically available in 1921, and type 2 diabetes can be controlled with tablets, but it is chronic condition that usually cannot be cured. Pancreas transplants have been tried with limited success in type 1 DM; gastric bypass surgery has been successful in many with morbid obesity and type 2 DM; and gestational diabetes usually resolves after delivery. Diabetes without proper treatments can cause many complications. Acute complications include hypoglycemia, diabetic ketoacidosis, or nonketotic hyperosmolar coma. Serious long-term complications include cardiovascular disease, chronic renal failure, retinal damage. Adequate treatment of diabetes is thus important, as well as blood pressure control and lifestyle factors such as smoking cesation and maintaining a healthy body weight.
As of 2000 at least 171 million people worldwide suffer from diabetes, or 2.8% of the population.[4] Type 2 diabetes is by far the most common, affecting 90 to 95% of the U.S. diabetes population.[5]
Contents
[hide]
1 Classification o 1.1 Type 1 diabetes

o 1.2 Type 2 diabetes o 1.3 Gestational diabetes o 1.4 Other types
2 Signs and symptoms 3 Causes
o 3.1 Lifestyle o 3.2 Medical conditions o 3.3 Genetics
4 Pathophysiology 5 Diagnosis 6 Screening 7 Prevention
o 7.1 Type 1 o 7.2 Type 2
8 Management o 8.1 Lifestyle modifications o 8.2 Medications o 8.3 Support
9 Prognosis 10 Epidemiology 11 History 12 Society and culture 13 References 14 External links
Classification
Most cases of diabetes mellitus fall into the three broad categories of type 1 or type 2 and gestational diabetes. A few other types are described.
The term diabetes, without qualification, usually refers to diabetes mellitus, which roughly translates to excessive sweet urine (known as "glycosuria"). Several rare conditions are also named diabetes. The most common of these is diabetes insipidus in which large amounts of urine are produced (polyuria), which is not sweet (insipidus meaning "without taste" in Latin).
The term "type 1 diabetes" has replaced several former terms, including childhood-onset diabetes, juvenile diabetes, and insulin-dependent diabetes mellitus (IDDM). Likewise, the term "type 2 diabetes" has replaced several former terms, including adult-onset diabetes, obesity-related diabetes, and non-insulin-dependent diabetes mellitus (NIDDM). Beyond these two types, there is no agreed-upon standard nomenclature. Various sources have defined "type 3 diabetes" as: gestational diabetes,[6] insulin-resistant type 1 diabetes (or "double diabetes"), type 2 diabetes which has progressed to require injected insulin, and latent autoimmune diabetes of adults (or LADA or "type 1.5 " diabetes)[7]

Type 1 diabetes
Main article: Diabetes mellitus type 1
Type 1 diabetes mellitus is characterized by loss of the insulin-producing beta cells of the islets of Langerhans in the pancreas leading to insulin deficiency. This type of diabetes can be further classified as immune-mediated or idiopathic. The majority of type 1 diabetes is of the immune-mediated nature, where beta cell loss is a T-cell mediated autoimmune attack.[2] There is no known preventive measure against type 1 diabetes, which causes approximately 10% of diabetes mellitus cases in North America and Europe. Most affected people are otherwise healthy and of a healthy weight when onset occurs. Sensitivity and responsiveness to insulin are usually normal, especially in the early stages. Type 1 diabetes can affect children or adults but was traditionally termed "juvenile diabetes" because it represents a majority of the diabetes cases in children.
Type 2 diabetes
Main article: Diabetes mellitus type 2
Type 2 diabetes mellitus is characterized by insulin resistance which may be combined with relatively reduced insulin secretion. The defective responsiveness of body tissues to insulin is believed to involve the insulin receptor. However, the specific defects are not known. Diabetes mellitus due to a known defect are classified separately. Type 2 diabetes is the most common type.
In the early stage of type 2 diabetes, the predominant abnormality is reduced insulin sensitivity. At this stage hyperglycemia can be reversed by a variety of measures and medications that improve insulin sensitivity or reduce glucose production by the liver. As the disease progresses, the impairment of insulin secretion occurs, and therapeutic replacement of insulin may sometimes become necessary in certain patients.[citation needed]
Gestational diabetes
Main article: Gestational diabetes
Gestational diabetes mellitus (GDM) resembles type 2 diabetes in several respects, involving a combination of relatively inadequate insulin secretion and responsiveness. It occurs in about 2%–5% of all pregnancies and may improve or disappear after delivery. Gestational diabetes is fully treatable but requires careful medical supervision throughout the pregnancy. About 20%–50% of affected women develop type 2 diabetes later in life.
Even though it may be transient, untreated gestational diabetes can damage the health of the fetus or mother. Risks to the baby include macrosomia (high birth weight), congenital cardiac and central nervous system anomalies, and skeletal muscle malformations. Increased fetal insulin may inhibit fetal surfactant production and cause respiratory distress syndrome. Hyperbilirubinemia may result from red blood cell destruction. In severe cases, perinatal death may occur, most commonly as a result of poor placental perfusion due to vascular impairment.

Labor induction may be indicated with decreased placental function. A cesarean section may be performed if there is marked fetal distress or an increased risk of injury associated with macrosomia, such as shoulder dystocia.
A 2008 study completed in the U.S. found that more American women are entering pregnancy with preexisting diabetes. In fact the rate of diabetes in expectant mothers has more than doubled in the past 6 years.[8] This is particularly problematic as diabetes raises the risk of complications during pregnancy, as well as increasing the potential that the children of diabetic mothers will also become diabetic in the future.
Other types
Pre-diabetes indicates a condition that occurs when a person's blood glucose levels are higher than normal but not high enough for a diagnosis of type 2 diabetes. Many people destined to develop type 2 diabetes spend many years in a state of pre-diabetes which has been termed "America's largest healthcare epidemic,"[9]:10–11.
Some cases of diabetes are caused by the body's tissue receptors not responding to insulin (even when insulin levels are normal, which is what separates it from type 2 diabetes); this form is very uncommon. Genetic mutations (autosomal or mitochondrial) can lead to defects in beta cell function. Abnormal insulin action may also have been genetically determined in some cases. Any disease that causes extensive damage to the pancreas may lead to diabetes (for example, chronic pancreatitis and cystic fibrosis). Diseases associated with excessive secretion of insulin-antagonistic hormones can cause diabetes (which is typically resolved once the hormone excess is removed). Many drugs impair insulin secretion and some toxins damage pancreatic beta cells. The ICD-10 (1992) diagnostic entity, malnutrition-related diabetes mellitus (MRDM or MMDM, ICD-10 code E12), was deprecated by the World Health Organization when the current taxonomy was introduced in 1999.[10]
Signs and symptoms
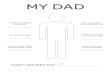
Overview of the most significant symptoms of diabetes.

The classical symptoms of DM are polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).[11] Symptoms may develop quite rapidly (weeks or months) in type 1 diabetes, particularly in children. However, in type 2 diabetes symptoms usually develop much more slowly and may be subtle or completely absent. Type 1 diabetes may also cause a rapid yet significant weight loss (despite normal or even increased eating) and irreducible mental fatigue. All of these symptoms except weight loss can also manifest in type 2 diabetes in patients whose diabetes is poorly controlled, although unexplained weight loss may be experienced at the onset of the disease. Final diagnosis is made by measuring the blood glucose concentration.
When the glucose concentration in the blood is raised beyond its renal threshold (about 10 mmol/L, although this may be altered in certain conditions, such as pregnancy), reabsorption of glucose in the proximal renal tubuli is incomplete, and part of the glucose remains in the urine (glycosuria). This increases the osmotic pressure of the urine and inhibits reabsorption of water by the kidney, resulting in increased urine production (polyuria) and increased fluid loss. Lost blood volume will be replaced osmotically from water held in body cells and other body compartments, causing dehydration and increased thirst.
Prolonged high blood glucose causes glucose absorption, which leads to changes in the shape of the lenses of the eyes, resulting in vision changes; sustained sensible glucose control usually returns the lens to its original shape. Blurred vision is a common complaint leading to a diabetes diagnosis; type 1 should always be suspected in cases of rapid vision change, whereas with type 2 change is generally more gradual, but should still be suspected.
Patients (usually with type 1 diabetes) may also initially present with diabetic ketoacidosis (DKA), an extreme state of metabolic dysregulation characterized by the smell of acetone on the patient's breath; a rapid, deep breathing known as Kussmaul breathing; polyuria; nausea; vomiting and abdominal pain; and any of many altered states of consciousness or arousal (such as hostility and mania or, equally, confusion and lethargy). In severe DKA, coma may follow, progressing to death. Diabetic ketoacidosis is a medical emergency and requires immediate hospitalization.
A rarer but equally severe possibility is hyperosmolar nonketotic state, which is more common in type 2 diabetes and is mainly the result of dehydration due to loss of body water. Often, the patient has been drinking extreme amounts of sugar-containing drinks, leading to a vicious circle in regard to the water loss.
A number of skin rashes can occur in diabetes that are collectively known as diabetic dermadromes.
Causes
Type 2 diabetes is determined primarily by lifestyle factors and genes.[12]
Lifestyle

A number of lifestyle factors are known to be important to the development of type 2 diabetes. In one study, those who had high levels of physical activity, a healthy diet, did not smoke, and consumed alcohol in moderation had an 82% lower rate of diabetes. When a normal weight was included the rate was 89% lower. In this study a healthy diet was defined as one high in fiber, with a high polyunsaturated to saturated fat ratio, and a lower mean glycemic index.[13] Obesity has been found to contribute to approximately 55% type 2 diabetes,[14] and decreasing consumption of saturated fats and trans fatty acids while replacing them with unsaturated fats may decrease the risk.[12] The increased rate of childhood obesity in between the 1960s and 2000s is believed to have lead to the increase in type 2 diabetes in children and adolescents.[15]
Environmental toxins may contribute to recent increases in the rate of type 2 diabetes. A positive correlation has been found between the concentration in the urine of bisphenol A, a constituent of some plastics, and the incidence of type 2 diabetes.[16]
Medical conditions
Subclinical Cushing's syndrome (cortisol excess) may be associated with DM type 2.[17] The percentage of subclinical Cushing's syndrome in the diabetic population is about 9%.[18] Diabetic patients with a pituitary microadenoma can improve insulin sensitivity by removal of these microadenomas.[19]
Hypogonadism is often associated with cortisol excess, and testosterone deficiency is also associated with diabetes mellitus type 2,[20][21] even if the exact mechanism by which testosterone improve insulin sensitivity is still not known.
Genetics
Both type 1 and type 2 diabetes are partly inherited. Type 1 diabetes may be triggered by certain infections, with some evidence pointing at Coxsackie B4 virus. There is a genetic element in individual susceptibility to some of these triggers which has been traced to particular HLA genotypes (i.e., the genetic "self" identifiers relied upon by the immune system). However, even in those who have inherited the susceptibility, type 1 diabetes mellitus seems to require an environmental trigger.
There is a stronger inheritance pattern for type 2 diabetes. Those with first-degree relatives with type 2 have a much higher risk of developing type 2, increasing with the number of those relatives. Concordance among monozygotic twins is close to 100%, and about 25% of those with the disease have a family history of diabetes. Genes significantly associated with developing type 2 diabetes, include TCF7L2, PPARG, FTO, KCNJ11, NOTCH2, WFS1, CDKAL1, IGF2BP2, SLC30A8, JAZF1, and HHEX.[22] KCNJ11 (potassium inwardly rectifying channel, subfamily J, member 11), encodes the islet ATP-sensitive potassium channel Kir6.2, and TCF7L2 (transcription factor 7–like 2) regulates proglucagon gene expression and thus the production of glucagon-like peptide-1.[2] Moreover, obesity (which is an independent risk factor for type 2 diabetes) is strongly inherited.[23]
Monogenic forms, e.g., MODY, constitute 1–5 % of all cases.[24]

Various hereditary conditions may feature diabetes, for example myotonic dystrophy and Friedreich's ataxia. Wolfram's syndrome is an autosomal recessive neurodegenerative disorder that first becomes evident in childhood. It consists of diabetes insipidus, diabetes mellitus, optic atrophy, and deafness, hence the acronym DIDMOAD.[25]
Gene expression promoted by a diet of fat and glucose as well as high levels of inflammation related cytokines found in the obese results in cells that "produce fewer and smaller mitochondria than is normal," and are thus prone to insulin resistance.[26]
Pathophysiology
This section does not cite any references or sources.Please help improve this article by adding citations to reliable sources. Unsourced material may be challenged and removed. (November 2009)
The fluctuation of blood sugar (red) and the sugar-lowering hormone insulin (blue) in humans during the course of a day with three meals. One of the effects of a sugar-rich vs a starch-rich meal is highlighted.
Mechanism of insulin release in normal pancreatic beta cells. Insulin production is more or less constant within the beta cells, irrespective of blood glucose levels. It is stored within vacuoles pending release, via exocytosis, which is primarily triggered by food, chiefly food containing absorbable glucose. The chief trigger is a rise in blood glucose levels after eating
Insulin is the principal hormone that regulates uptake of glucose from the blood into most cells (primarily muscle and fat cells, but not central nervous system cells). Therefore deficiency of insulin or the insensitivity of its receptors plays a central role in all forms of diabetes mellitus.

Humans are capable of digesting some carbohydrates, in particular those most common in food; starch, and some disaccharides such as sucrose, are converted within a few hours to simpler forms most notably the monosaccharide glucose, the principal carbohydrate energy source used by the body. The most significant exceptions are fructose, most disaccharides (except sucrose and in some people lactose), and all more complex polysaccharides, with the outstanding exception of starch. The rest are passed on for processing by gut flora largely in the colon. Insulin is released into the blood by beta cells (β-cells), found in the Islets of Langerhans in the pancreas, in response to rising levels of blood glucose, typically after eating. Insulin is used by about two-thirds of the body's cells to absorb glucose from the blood for use as fuel, for conversion to other needed molecules, or for storage.
Insulin is also the principal control signal for conversion of glucose to glycogen for internal storage in liver and muscle cells. Lowered glucose levels result both in the reduced release of insulin from the beta cells and in the reverse conversion of glycogen to glucose when glucose levels fall. This is mainly controlled by the hormone glucagon which acts in the opposite manner to insulin. Glucose thus forcibly produced from internal liver cell stores (as glycogen) re-enters the bloodstream; muscle cells lack the necessary export mechanism. Normally liver cells do this when the level of insulin is low (which normally correlates with low levels of blood glucose).
Higher insulin levels increase some anabolic ("building up") processes such as cell growth and duplication, protein synthesis, and fat storage. Insulin (or its lack) is the principal signal in converting many of the bidirectional processes of metabolism from a catabolic to an anabolic direction, and vice versa. In particular, a low insulin level is the trigger for entering or leaving ketosis (the fat burning metabolic phase).
If the amount of insulin available is insufficient, if cells respond poorly to the effects of insulin (insulin insensitivity or resistance), or if the insulin itself is defective, then glucose will not have its usual effect so that glucose will not be absorbed properly by those body cells that require it nor will it be stored appropriately in the liver and muscles. The net effect is persistent high levels of blood glucose, poor protein synthesis, and other metabolic derangements, such as acidosis.
Diagnosis
Main articles: Glycosylated hemoglobin and Glucose tolerance test
1999 WHO Diabetes criteria[27]
Condition 2 hour glucose Fasting glucose
mmol/l(mg/dl) mmol/l(mg/dl)
Normal <7.8 (<140) <6.1 (<110)

Impaired fasting glycaemia <7.8 (<140) ≥ 6.1(≥110) & <7.0(<126)
Impaired glucose tolerance ≥7.8 (≥140) <7.0 (<126)
Diabetes mellitus ≥11.1 (≥200) ≥7.0 (≥126)
Diabetes mellitus is characterized by recurrent or persistent hyperglycemia, and is diagnosed by demonstrating any one of the following:[10]
Fasting plasma glucose level at or above 7.0 mmol/L (126 mg/dL). Plasma glucose at or above 11.1 mmol/L (200 mg/dL) two hours after a 75 g oral glucose
load as in a glucose tolerance test. Symptoms of hyperglycemia and casual plasma glucose at or above 11.1 mmol/L
(200 mg/dL). Glycated hemoglobin (hemoglobin A1C) at or above 6.5. (This criterion was
recommended by the American Diabetes Association in 2010; it has yet to be adopted by the WHO.)[28]
About a quarter of people with new type 1 diabetes have developed some degree of diabetic ketoacidosis (a type of metabolic acidosis which is caused by high concentrations of ketone bodies, formed by the breakdown of fatty acids and the deamination of amino acids) by the time the diabetes is recognized. The diagnosis of other types of diabetes is usually made in other ways. These include ordinary health screening; detection of hyperglycemia during other medical investigations; and secondary symptoms such as vision changes or unexplainable fatigue. Diabetes is often detected when a person suffers a problem that is frequently caused by diabetes, such as a heart attack, stroke, neuropathy, poor wound healing or a foot ulcer, certain eye problems, certain fungal infections, or delivering a baby with macrosomia or hypoglycemia.
A positive result, in the absence of unequivocal hyperglycemia, should be confirmed by a repeat of any of the above-listed methods on a different day. Most physicians prefer to measure a fasting glucose level because of the ease of measurement and the considerable time commitment of formal glucose tolerance testing, which takes two hours to complete and offers no prognostic advantage over the fasting test.[29] According to the current definition, two fasting glucose measurements above 126 mg/dL (7.0 mmol/L) is considered diagnostic for diabetes mellitus.
Patients with fasting glucose levels from 100 to 125 mg/dL (5.6 to 6.9 mmol/L) are considered to have impaired fasting glucose. Patients with plasma glucose at or above 140 mg/dL (7.8 mmol/L), but not over 200 mg/dL (11.1 mmol/L), two hours after a 75 g oral glucose load are considered to have impaired glucose tolerance. Of these two pre-diabetic states, the latter in particular is a major risk factor for progression to full-blown diabetes mellitus as well as cardiovascular disease.[30]

Screening
Diabetes screening is recommended for many people at various stages of life, and for those with any of several risk factors. The screening test varies according to circumstances and local policy, and may be a random blood glucose test, a fasting blood glucose test, a blood glucose test two hours after 75 g of glucose, or an even more formal glucose tolerance test. Many healthcare providers recommend universal screening for adults at age 40 or 50, and often periodically thereafter. Earlier screening is typically recommended for those with risk factors such as obesity, family history of diabetes, high-risk ethnicity (Hispanic, Native American, Afro-Caribbean, Pacific Islander, or Māori).[31][32]
Many medical conditions are associated with diabetes and warrant screening. A partial list includes: subclinical Cushing's syndrome,[17] testosterone deficiency,[20] high blood pressure, elevated cholesterol levels[citation needed], coronary artery disease[citation needed], past gestational diabetes, polycystic ovary syndrome, chronic pancreatitis, fatty liver, hemochromatosis[citation needed], cystic fibrosis, several mitochondrial neuropathies and myopathies (such as MIDD), myotonic dystrophy, Friedreich's ataxia, some of the inherited forms of neonatal hyperinsulinism. The risk of diabetes is higher with chronic use of several medications, including long term corticosteroids, some chemotherapy agents (especially L-asparaginase), as well as some of the antipsychotics and mood stabilizers (especially phenothiazines and some atypical antipsychotics).
People with a confirmed diagnosis of diabetes are tested routinely for complications. This includes yearly urine testing for microalbuminuria and examination of the retina of the eye for retinopathy.
Prevention
Type 1
Type 1 diabetes risk is known to depend upon a genetic predisposition based on HLA types (particularly types DR3 and DR4), an unknown environmental trigger (suspected to be an infection, although none has proven definitive in all cases), and an uncontrolled autoimmune response that attacks the insulin producing beta cells.[33] Some research has suggested that breastfeeding decreased the risk in later life;[34][35] various other nutritional risk factors are being studied, but no firm evidence has been found.[36] Giving children 2000 IU of Vitamin D during their first year of life is associated with reduced risk of type 1 diabetes, though the causal relationship is obscure.[37]
Children with antibodies to beta cell proteins (i.e. at early stages of an immune reaction to them) but no overt diabetes, and treated with vitamin B-3 (niacin), had less than half the diabetes onset incidence in a 7-year time span as did the general population, and an even lower incidence relative to those with antibodies as above, but who received no vitamin B3.[38]
Type 2

Lifestyle
Type 2 diabetes risk can be reduced in many cases by making changes in diet and increasing physical activity.[39][40][41] The American Diabetes Association (ADA) recommends maintaining a healthy weight, getting at least 2½ hours of exercise per week (several brisk sustained walks appear sufficient), having a modest fat intake, and eating sufficient fiber (e.g., from whole grains). The ADA does not recommend alcohol consumption as a preventive, but it is interesting to note that moderate alcohol intake may reduce the risk (though heavy consumption absolutely and clearly increases damage to bodily systems significantly); a similarly confused connection between low dose alcohol consumption and heart disease is termed the French Paradox.[citation
needed]
There is inadequate evidence that eating foods of low glycemic index is clinically helpful despite recommendations and suggested diets emphasizing this approach.[42]
Diets that are very low in saturated fats reduce the risk of becoming insulin resistant and diabetic.[43][44] Study group participants whose "physical activity level and dietary, smoking, and alcohol habits were all in the low-risk group had an 82% lower incidence of diabetes."[13] In another study of dietary practice and incidence of diabetes, "foods rich in vegetable oils, including non-hydrogenated margarines, nuts, and seeds, should replace foods rich in saturated fats from meats and fat-rich dairy products. Consumption of partially hydrogenated fats should be minimized."[12]
There are numerous studies which suggest connections between some aspects of Type II diabetes with ingestion of certain foods or with some drugs. Breastfeeding may also be associated with the prevention of type 2 of the disease in mothers.[45]
Medications
Some studies have shown delayed progression to diabetes in predisposed patients through prophylactic use of metformin,[40] rosiglitazone,[46] or valsartan.[47] In patients on hydroxychloroquine for rheumatoid arthritis, incidence of diabetes was reduced by 77% though causal mechanisms are unclear.[48] Lifestyle interventions are however more effective than metformin at preventing diabetes regardless of weightloss.[49]
Management
Main article: Diabetes management
Diabetes mellitus is a chronic disease which is difficult to cure. Management concentrates on keeping blood sugar levels as close to normal ("euglycemia") as possible without presenting undue patient danger. This can usually be with close dietary management, exercise, and use of appropriate medications (insulin only in the case of type 1 diabetes mellitus. Oral medications may be used in the case of type 2 diabetes, as well as insulin).
Lifestyle modifications

Main article: Diabetic diet
There are roles for patient education, dietetic support, sensible exercise, with the goal of keeping both short-term and long-term blood glucose levels within acceptable bounds. In addition, given the associated higher risks of cardiovascular disease, lifestyle modifications are recommended to control blood pressure[50] in patients with hypertension, cholesterol in those with dyslipidmia, as well as exercising more, smoking less or ideally not at all, consuming a recommended diet[citation
needed]. Patients with foot problems are also recommended to wear diabetic socks[citation needed], and possibly diabetic shoes[citation needed].
Medications
Oral medicationsMain article: Anti-diabetic drug
InsulinMain article: Insulin therapy
Type 1 treatments usually include combinations of regular or NPH insulin, and/or synthetic insulin analogs.
Support
In countries using a general practitioner system, such as the United Kingdom, care may take place mainly outside hospitals, with hospital-based specialist care used only in case of complications, difficult blood sugar control, or research projects. In other circumstances, general practitioners and specialists share care of a patient in a team approach. Optometrists, podiatrists/chiropodists, dietitians, physiotherapists, nursing specialists (e.g., DSNs (Diabetic Specialist Nurse)), nurse practitioners, or Certified Diabetes Educators, may jointly provide multidisciplinary expertise. In countries where patients must provide for their own health care (e.g. in the US, and in much of the undeveloped world).
Peer support links people living with diabetes. Within peer support, people with a common illness share knowledge and experience that others, including many health workers, do not have. Peer support is frequent, ongoing, accessible and flexible and can take many forms—phone calls, text messaging, group meetings, home visits, and even grocery shopping. It complements and enhances other health care services by creating the emotional, social and practical assistance necessary for managing disease and staying healthy.
Prognosis
Main article: Prognosis of diabetes mellitus
Patient education, understanding, and participation is vital since the complications of diabetes are far less common and less severe in people who have well-managed blood sugar levels.[51][52] Wider health problems may accelerate the deleterious effects of diabetes. These include

smoking, elevated cholesterol levels, obesity, high blood pressure, and lack of regular exercise. According to one study, women with high blood pressure (hypertension) were three times more likely to develop type 2 diabetes as compared with women with optimal BP after adjusting for various factors such as age, ethnicity, smoking, alcohol intake, body mass index (BMI), exercise, family history of diabetes, etc.[53] The study was conducted by researchers from the Brigham and Women’s Hospital, Harvard Medical School and the Harvard School of Public Health, USA, who followed over 38,000 female health professionals for ten years.
Except in the case of type 1 diabetes, which always requires insulin replacement, the way type 2 diabetes is managed may change with age. Insulin production decreases because of age-related impairment of pancreatic beta cells. Additionally, insulin resistance increases because of the loss of lean tissue and the accumulation of fat, particularly intra-abdominal fat, and the decreased tissue sensitivity to insulin. Glucose tolerance progressively declines with age, leading to a high prevalence of type 2 diabetes and postchallenge hyperglycemia in the older population.[54] Age-related glucose intolerance in humans is often accompanied by insulin resistance, but circulating insulin levels are similar to those of younger people.[55] Treatment goals for older patients with diabetes vary with the individual, and take into account health status, as well as life expectancy, level of dependence, and willingness to adhere to a treatment regimen.[56] Glycated hemoglobin is better than fasting glucose for determining risks of cardiovascular disease and death from any cause.[57]
Epidemiology
Prevalence of diabetes worldwide in 2000 (per 1000 inhabitants). World average was 2.8%. no data ≤ 7.5 7.5–15 15–22.5 22.5–30 30–37.5 37.5–45 45–52.5 52.5–60 60–67.5 67.5–75 75–82.5 ≥ 82.5
Disability-adjusted life year for diabetes mellitus per 100,000 inhabitants in 2002.[58] no data ≤ 100 100-200 200-300 300-400 400-500 500-600 600-700 700-800 800-900 900-1000 1000-1500 ≥ 1500
In 2000, according to the World Health Organization, at least 171 million people worldwide suffer from diabetes, or 2.8% of the population.[4] Its incidence is increasing rapidly, and it is estimated that by 2030, this number will almost double.[4] Diabetes mellitus occurs throughout the world, but is more common (especially type 2) in the more developed countries. The greatest

increase in prevalence is, however, expected to occur in Asia and Africa, where most patients will probably be found by 2030.[4] The increase in incidence of diabetes in developing countries follows the trend of urbanization and lifestyle changes, perhaps most importantly a "Western-style" diet. This has suggested an environmental (i.e., dietary) effect, but there is little understanding of the mechanism(s) at present, though there is much speculation, some of it most compellingly presented.[4]
For at least 20 years, diabetes rates in North America have been increasing substantially. In 2008 there were about 24 million people with diabetes in the United States alone, from those 5.7 million people remain undiagnosed. Other 57 million people are estimated to have pre-diabetes.[59]
The Centers for Disease Control has termed the change an epidemic.[60] The National Diabetes Information Clearinghouse estimates that diabetes costs $132 billion in the United States alone every year. About 5%–10% of diabetes cases in North America are type 1, with the rest being type 2. The fraction of type 1 in other parts of the world differs. Most of this difference is not currently understood. The American Diabetes Association cite the 2003 assessment of the National Center for Chronic Disease Prevention and Health Promotion (Centers for Disease Control and Prevention) that 1 in 3 Americans born after 2000 will develop diabetes in their lifetime.[61][62]
According to the American Diabetes Association, approximately 18.3% (8.6 million) of Americans age 60 and older have diabetes.[63] Diabetes mellitus prevalence increases with age, and the numbers of older persons with diabetes are expected to grow as the elderly population increases in number. The National Health and Nutrition Examination Survey (NHANES III) demonstrated that, in the population over 65 years old, 18% to 20% have diabetes, with 40% having either diabetes or its precursor form of impaired glucose tolerance.[54]
Indigenous populations in first world countries have a higher prevalence and increasing incidence of diabetes than their corresponding non-indigenous populations. In Australia the age-standardised prevalence of self-reported diabetes in Indigenous Australians is almost 4 times that of non-indigenous Australians.[64] Preventative community health programs such as Sugar Man (diabetes education) are showing some success in tackling this problem.
History
The term diabetes (Greek: διαβήτης, diabētēs) was coined by Aretaeus of Cappadocia. It was derived from the Greek verb διαβαίνειν, diabaínein, itself formed from the prefix dia-, "across, apart," and the verb bainein, "to walk, stand." The verb diabeinein meant "to stride, walk, or stand with legs asunder"; hence, its derivative diabētēs meant "one that straddles," or specifically "a compass, siphon." The sense "siphon" gave rise to the use of diabētēs as the name for a disease involving the discharge of excessive amounts of urine. Diabetes is first recorded in English, in the form diabete, in a medical text written around 1425. In 1675, Thomas Willis added the word mellitus, from the Latin meaning "honey", a reference to the sweet taste of the urine. This sweet taste had been noticed in urine by the ancient Greeks, Chinese, Egyptians,

Indians, and Persians. In 1776, Matthew Dobson confirmed that the sweet taste was because of an excess of a kind of sugar in the urine and blood of people with diabetes.[65]
Diabetes mellitus appears to have been a death sentence in the ancient era. Hippocrates makes no mention of it, which may indicate that he felt the disease was incurable. Aretaeus did attempt to treat it but could not give a good prognosis; he commented that "life (with diabetes) is short, disgusting and painful."[66]
Sushruta (6th century BCE) identified diabetes and classified it as Medhumeha.[67] He further identified it with obesity and sedentary lifestyle, advising exercises to help "cure" it.[67] The ancient Indians tested for diabetes by observing whether ants were attracted to a person's urine, and called the ailment "sweet urine disease" (Madhumeha). The Korean, Chinese, and Japanese words for diabetes are based on the same ideographs (糖尿病) which mean "sugar urine disease".
In medieval Persia, Avicenna (980–1037) provided a detailed account on diabetes mellitus in The Canon of Medicine, "describing the abnormal appetite and the collapse of sexual functions," and he documented the sweet taste of diabetic urine. Like Aretaeus before him, Avicenna recognized a primary and secondary diabetes. He also described diabetic gangrene, and treated diabetes using a mixture of lupine, trigonella (fenugreek), and zedoary seed, which produces a considerable reduction in the excretion of sugar, a treatment which is still prescribed in modern times. Avicenna also "described diabetes insipidus very precisely for the first time", though it was later Johann Peter Frank (1745–1821) who first differentiated between diabetes mellitus and diabetes insipidus.[68]
Although diabetes has been recognized since antiquity, and treatments of various efficacy have been known in various regions since the Middle Ages, and in legend for much longer, pathogenesis of diabetes has only been understood experimentally since about 1900.[69] The discovery of a role for the pancreas in diabetes is generally ascribed to Joseph von Mering and Oskar Minkowski, who in 1889 found that dogs whose pancreas was removed developed all the signs and symptoms of diabetes and died shortly afterwards.[70] In 1910, Sir Edward Albert Sharpey-Schafer suggested that people with diabetes were deficient in a single chemical that was normally produced by the pancreas—he proposed calling this substance insulin, from the Latin insula, meaning island, in reference to the insulin-producing islets of Langerhans in the pancreas.
The endocrine role of the pancreas in metabolism, and indeed the existence of insulin, was not further clarified until 1921, when Sir Frederick Grant Banting and Charles Herbert Best repeated the work of Von Mering and Minkowski, and went further to demonstrate they could reverse induced diabetes in dogs by giving them an extract from the pancreatic islets of Langerhans of healthy dogs.[71] Banting, Best, and colleagues (especially the chemist Collip) went on to purify the hormone insulin from bovine pancreases at the University of Toronto. This led to the availability of an effective treatment—insulin injections—and the first patient was treated in 1922. For this, Banting and laboratory director MacLeod received the Nobel Prize in Physiology or Medicine in 1923; both shared their Prize money with others in the team who were not recognized, in particular Best and Collip. Banting and Best made the patent available without charge and did not attempt to control commercial production. Insulin production and therapy

rapidly spread around the world, largely as a result of this decision. Banting is honored by World Diabetes Day which is held on his birthday, November 14.
The distinction between what is now known as type 1 diabetes and type 2 diabetes was first clearly made by Sir Harold Percival (Harry) Himsworth, and published in January 1936.[72]
Despite the availability of treatment, diabetes has remained a major cause of death. For instance, statistics reveal that the cause-specific mortality rate during 1927 amounted to about 47.7 per 100,000 population in Malta.[73]
Other landmark discoveries include:[69]
Identification of the first of the sulfonylureas in 1942 Reintroduction of the use of biguanides for Type 2 diabetes in the late 1950s. The initial
phenformin was withdrawn worldwide (in the U.S. in 1977) due to its potential for sometimes fatal lactic acidosis and metformin was first marketed in France in 1979, but not until 1994 in the US.
The determination of the amino acid sequence of insulin (by Sir Frederick Sanger, for which he received a Nobel Prize)
The radioimmunoassay for insulin, as discovered by Rosalyn Yalow and Solomon Berson (gaining Yalow the 1977 Nobel Prize in Physiology or Medicine)[74]
The three-dimensional structure of insulin (PDB 2INS) Dr Gerald Reaven's identification of the constellation of symptoms now called metabolic
syndrome in 1988 Demonstration that intensive glycemic control in type 1 diabetes reduces chronic side
effects more as glucose levels approach 'normal' in a large longitudinal study,[75] and also in type 2 diabetics in other large studies
Identification of the first thiazolidinedione as an effective insulin sensitizer during the 1990s
In 1980, U.S. biotech company Genentech developed human insulin. The insulin is isolated from genetically altered bacteria (the bacteria contain the human gene for synthesizing human insulin), which produce large quantities of insulin. Scientists then purify the insulin and distribute it to pharmacies for use by diabetes patients.
Society and culture
The 1990 "St Vincent Declaration"[76][77] was the result of international efforts to improve the care accorded to those with diabetes. Doing so is important both in terms of quality of life and life expectancy but also economically-expenses due to diabetes have been shown to be a major drain on health-and productivity-related resources for healthcare systems and governments.
Several countries established more and less successful national diabetes programmes to improve treatment of the disease.[78]

A study shows that diabetic patients with neuropathic symptoms such as numbness or tingling in feet or hands are twice as likely to be unemployed as those without the symptoms.[79]
References
1. ̂ (17 March 2006)"Diabetes Blue Circle Symbol". International Diabetes Federation. 17 March 2006. http://www.diabetesbluecircle.org.
2. ^ a b c Rother KI (April 2007). "Diabetes treatment—bridging the divide". The New England Journal of Medicine 356 (15): 1499–501. doi:10.1056/NEJMp078030. PMID 17429082.
3. ^ a b L M Tierney, S J McPhee, M A Papadakis (2002). Current medical Diagnosis & Treatment. International edition. New York: Lange Medical Books/McGraw-Hill. pp. 1203–15. ISBN 0-07-137688-7.
4. ^ a b c d e Wild S, Roglic G, Green A, Sicree R, King H (May 2004). "Global prevalence of diabetes: estimates for 2000 and projections for 2030". Diabetes Care 27 (5): 1047–53. doi:10.2337/diacare.27.5.1047. PMID 15111519.
5. ̂ "Type 2 Diabetes Overview". Web MD. http://diabetes.webmd.com/guide/type-2-diabetes.
Mirror [max.1gb.ru [file /eng/learn/ib005.shtml [at Fri, 06 Feb 2009 06:38:25 GMT]]]
Main : : Abstracts : : Psychiatry : : Links : Forum : : Guest book
Keywords: a case history, an endocrinology, diabetum melitous, 1 type, the serious form, subindemnification, an angioretinopathia, an angiopathia of the bottom extremities, a distal sensory polyneuropatia
the Author: Poljanskaja O.V.
THE CASE HISTORY ON THE ENDOCRINOLOGYThe clinical diagnosis:diabetum melitous, 1 type, the serious form, subindemnification.the Angioretinopathia. An angiopathia of the bottom extremities. A distal sensory polyneuropatia. Trophic infringements of calcaneal areas of both stop.

Amputating stump V of a finger left stops, III finger of the left arm. A nephropathy III. A symptomatic hypertonia. Fatty dystrophia of a liver, dyskinesia of biliferous ways. An ischemic disease, a stenocardia of a strain. Normohromnaja an anemia.
NAMEPLATE DATA1. A surname, a name, a patronymic: ***** ********** **************2. Age: 46 flying3. A sex: man's4. A nationality: Russian5. Formation: srednetehnicheskoe6. A place of work, a trade: does not work - the invalid of II group; by a trade - the carpenter7. A home address: с. Pridonskoe8. Date of entering in clinic: 15.07.20029. The diagnosis of the directed establishment: the Diabetic angiopathia of the bottom extremities
COMPLAINTS of the PATIENT AT ENTERINGOn whining, arching, sometimes - raking pains in the bottom extremities, especially expressed in the field of a calcaneus, achille tendons and on border pljusnevyh bones and phalanxes of fingers. Pains, the burning sensation, a pricking in stops of the patient connects to purulent wounds on them.Purulent wounds in area achille tendons.Cramps in ikronozhnyh muscles which arise more often when the patient in time does not accept the put medicine. Cramps are frequently accompanied by a plentiful diaphoresis, a shiver in arms and in all a body, appreciable delicacy.Strong pressing headaches, especially bright in occipital and on border frontal and temporal shares which amplify at change of weather, an emotional load. At considerably expressed headaches, accompanying with a giddiness and a nausea, sick measured arterial pressure, and it appeared considerably increased - 240 and 130.Infringements of vision: all subjects seem shrouded in a mild screen, before eyes frequently there is a hymenium which becomes more dense (" as ?«?«¬«") during an attack of strong headaches. The patient sees more precisely when has a rest and does not test any emotional discomfort.Gravity, pressure behind a breast bone which gripping pains sometimes join. Unpleasant sensations pass independently within 10-15 minutes, in dormancy calm down much faster (in 5-7 minutes).a Short wind arising at insignificant exercise stresses. Without a short wind can rise on 1-st floor on crutches.Deterioration of appetite, dryness in a mouth, a constant heartburn.

incidentally arising pains in the right the hypochondrium, sometimes bitter tastes accompanying with feeling in a mouth. An edema of a belly and the right anticnemion.Whining back pains, which occurrence of the patient to anything does not bind. Pains amplify, stoped independently, last from 30-40 minutes till 1,5 o'clock, unpleasant emotions do not cause. An emiction 2-4 times day. At the night of the patient does not rise.the Stool regular, 1 once a day.Rising of evening temperature up to 37,5°С.
the HISTORY of the PRESENT DISEASECounts itself the patient during 21 years. For the first time has addressed to the doctor 21 one year ago (in 25 flying) concerning sharp loss of weight (45-50 kg) for 2-3 years. Complained also of delicacy, a flaccidity, apathy, appreciable fatigability after a mild exercise stress, a strong diaphoresis. In a polyclinic on a residence the general analysis of a blood - a level of a glucose of 23 mmole/l has been made. The patient is hospitalized , lead a course of an insulin therapy. Felt like well, went for work, houses independently applied preparations of an insulin.In the age of 36 and 41 years got in hospitals with the diagnosis " Gipoglikemicheskaja ¬«?a", Which came that the patient in time did not accept I peep. The loss of consciousness last no more than 3 minutes (from words of the patient).Constantly disturbed tooths - were blasted and were sick, approximately in 1997 year (the patient precisely does not remember) - false teeth (all).in the Summer 1999 years of the patient has wounded to stop in the field of a heel. To the doctor has not addressed, as a pain did not test, an erythema and a tumescence in the field of a wound has not found out. The wound did not heal within 2 weeks, attributes of an inflammation have then appeared: a pain, a tumescence, an erythema, puffiness, has become inconveniently to attack a heel. The yellowish purulent discharge has appeared. At a X-ray inspection the osteoporosis of both calcaneuses (from words of the patient) has been found out. Long treatment of a purulent wound appeared not successful, periodically there come exacerbations. In 2000 year of the patient has pinned a little finger of the left leg, the wound also did not heal, then the purulent inflammation has become to be distributed, the gangrene began. Ablation of this finger is lead. In this (2000) year the long finger of the left arm concerning a diabetic gangrene is amputated.About 2001 years of the patient marks attacks of very high blood pressure (240 and 130), accompanying with strong pressing headaches. In 2001 year infringements of vision (a hymenium before eyes) have appeared.In the beginning 2002 years have appeared purulent is long not healing wounds and on other leg, with complaints to which exacerbation of the patient and have been hospitalized during the present moment.to Words of the patient, the last 3 years he is treated in a hospital not less than 2 times in year. Therapy is carried out concerning a high blood pressure and diabetic stops. Last time was hospitalized in April 2002 years. During the present moment

accepts 8.00 - humulin NPH 16 ED + aktropid 8 ED; 17.00 - humulin R 5 ED, 22.00 - humulin NPH 10 UNITS. In total for day of the patient receives 39ЕД.
the HISTORY of LIFE of the PATIENTWas born in Voronezh, in family of workers. Dews also developed in conformity with the years. At school studied well, at known diligence - it is good. Has stopped prof. Those. A school, has received a speciality of the carpenter - joiner. Worked on building objects. Periodically it was necessary to work in the street under adverse weather conditions (snow, a rain, a strong wind). From professional harmfulnesses marks an often raising of gravities, contact to diabrotic and strongly smelling substances (a drying oil, paints, dissolvents). On work tried to not enter conflicts, with colleagues and the heads without effort found common language. Now does not work, receives pension as the invalid of II group. In the days off and holiday worked on a rate, sometimes - on the building objects demanding urgent delivery in operation.Smokes from 17-18 a flying. Now smokes a pack for 3 days, 3 years smoked on 2 packs in day back. Alcohol does not use the last 5-7 flying, up to that - abused (" drank »«Onn«??«") .the Tuberculosis, oncologic, venereal diseases and AIDS denies. An allergy to foodstuffs and medicinal substances, allergic diseases denies.It is married, to the son 19 flying.At parents and close relatives of a sugar diabetes never was.
the PRESENT CONDITION of the PATIENT
The general inspection: a condition of the average patient, consciousness clear, but the patient is slightly delayed: questions answers slowly, very much razdumchivo, but it is correct. Position of the patient active. A look quiet, a little bit released. Body build normosthenic.Body height of 184 sm, mass of a body - 85 kg. An index of mass of a body: 85 / 1,842=25,1the General feed normal.Integuments acyanotic, hardly yellowish, labiums slightly cyanochroic, the person a little bit bloated; on stops, anticnemions, a back surface of brachiums and in the field of a ulnar joint plural light brown nevuses pigmentosus in diameter from 0,5 up to 1 see are observed. A skin dry, cold, on anticnemions and stops rasping, peeling, with white large (0,3-0,5 sm) flakes, the turgor of it is reduced. In the right ileal area - cicatrix after an appendectomia. On both stops in area achille tendons - purulent wounds of 1*2 and 2*3,5 sm - trophic ulcers.Nails convex, remind hour glasses under the form. A pilosis on man's type, moderate. Hair on a belly, it is especial on a white line, long, rigid. Hair on a head and a body almost completely gray-haired.the Expressed edema of the right anticnemion. Ascites (the level of a liquid is not determined).Cervical, subclavial lymph nodes are not enlarged, the submandibular lymph node

of 0,5-0,7 sm, slightly morbid, with a skin not commissured on the right is palpated.the Muscle system is well advanced, the tonus and force of muscles sufficient, morbidity of muscles of an anticnemion, are occasionally observed their cramps.Bones and joints of a regular form, are not deformed, at a palpation and a palpation painless. It is amputated V a finger left stops and III finger of the left brush.the Body temperature subfebrile - 37,5°С.System of organs of respiration: a chest of a normal form, type of respiration belly, a frequency of respiratory movements=16, a rhythm of respiration correct, respiration deep. In dormancy of a short wind is not present. A percussion sound clear above all pulmonary fields. Border mild on a mammilar line - the bottom edge of 6 ribs, on average axillary - the bottom edge of 8 ribs. Mobility of pulmonary edge on the right - 3 sm, at the left - 4 see. At an auscultation rigid respiration in the top third mild, further - vesicular is auscultated. Individual dry whistling rhonchuses.System of organs of a circulation: borders of heart are displaced to the left: the right border - 1-2 sm to the left from a right edge of a breast bone, top - the top edge of 4-th rib, left - is displaced to the left on 2-3 sm from a mammilar line.At an auscultation: cardiac sounds rhythmical, a tachycardia (up to 100 impacts in one minute), a rhythm correct. On an apex cardiac sounds are amplified, 1-st is especial. On an aorta - accent and splitting of 2-nd tone. Hums are not present.the Pulsation of vessels of a neck and a forearm is well expressed. The pulsation a. dorsalis pedis is weakened on both legs.Pulse of rhythmical, 96 impacts in minutes, good filling and a strain.a blood pressure at the moment of inspection - 150 and 90. Maximal - 240 and 130. In a dormant state - 140 and 90.System of organs of digestion: the smell from a mouth is not present. Labiums slightly cyanochroic, a mucosa of an internal surface of labiums, cheeks, firm and a soft palate, a mucosa of gingivas acyanotic, wet. Tooths are not present - plug-in. Tongue of the usual size, bright - crimson, slightly wet, with flattened papillas, with the dark yellowish raid more expressed on the right.the Belly enlarged in size, " ?nuO?a??®", participates in the act of respiration. At a superficial palpation moderate morbidity is revealed in the field of legal hypochondrium and in epigastric area. An ascites.the Liver acts on 0,5-1 sm for edge of a rib arch. The sizes on Kurlovu: 6, 8 and 12 see. The edge of a liver in connection with an expressiveness of a hypodermic fatty tissue and an ascites is good for palpating it was not possible. The lien is not palpated.System of a uropoiesis: an emiction free, painless, 3-4 once a day. Occasionally there is a mild morbidity in the field of a loin. Sign Pasternatskogo from both sides negative.Endocrine system: body height of 184 sm, weight of 85 kg, an index of mass of a body 25,1: FROM 93 sm, ABOUT 102 sm, FROM / ABOUT=93/102=0,9. The isthmus of a thyroid gland by thickness 0,5-0,7см is palpated. The smell of an acetone from a mouth at the patient is not present. Vision has worsened for last year. Legs cold, sensations of a burning sensation and a pricking - a polyneuropatia. Palpebral fissures of the usual form, sick a proportional body build,

normal body height. Secondary sexual attributes are well expressed.Nervous system: the consciousness is kept, speech clear, slightly time-lapse, mild block. Memory on the current events is well kept, reduced on the last events (the patient cannot remember as for a long time there was an event, forgets names of medicines). Mood equal, reduced. The patient is disturbing. Pupils in diameter of 3 mm from both sides. A straight line and sodruzhestvennaja reactions to light are expressed, symmetric. Paresises and paralysises are not present, pain sensitivity is reduced in the field of both stop.
the DATA of LABORATORY AND TOOL METHODS of INSPECTION:the General analysis of a blood:28.0818.09a haemoglobin 7866erythrocytes 2,62,46*1012a colour parameter 0,9leucocytes 10,2*109relating to stab neutrophile 3 %segmentojadernye 72 %eosinocytes of 5 %lymphocytes of 12 %monocytes of 8 %a rate of gravitation of blood 59the General analysis of urine (30.07): transparence N, relative density 1010, fiber of 2,3 mg / l, leucocytes 2-3, erythrocytes 5-6, hyaline cylinders 0-1.the Biochemical analysis of a blood (18.09): a urea 14,0, a creatinine 209, the general fiber 63.the Biochemical analysis of a blood (16.08): nuclear heating plant 17, ALT 30, a bilirubin the general 5,0, a urea 14,6, a creatinine 172, a cholesterin 5,3, lipoproteins 6,5, a prothrombin ratio 86, an amylase of a blood 5,0, the general fiber 69.Assay Reberga (15.07): a daily urine 2,0, minute - 1,38, a creatinine of a blood - 172 mmole/l, a creatinine of urine - 15,4 mmole/l, a filtration - 123,5 mmole/l (65-120), reabsorbtsija 98,9 (98 - 99) mmole/l.Glikemichesky a profile (15.07 : 8.00) - 19,1, 11.00 - 23,8, 14.00 - 11,3, 17.00 - 13,0, 21.00 - 15,2 mmole/l.Glikemichesky a profile (13.09 : 8.00) - 9,7, 11.00 - 12,4, 14.00 - 8,4 mmole/l.an electrocardiogram:the Sinus tachycardia, an electric axis of heart - a normal position, a heart rate=100 impacts in minute, attributes of a hypertrophy of the left auricle and a left ventricle. Ischemic changes on a forward wall and a septum of heart.the Tank. Crop on sensitivity of a flora to antibiotics: Oxacillinum, erythromycin, Cefazolinum, tsiprofloksatsin, Vancomycinum.
the DIAGNOSISdiabetum melitous, 1 type, the serious form, subindemnification. An angioretinopathia. An angiopathia of the bottom extremities. A distal sensory

polyneuropatia. Trophic infringements of calcaneal areas of both stop. Amputating stump V of a finger left stops, III finger of the left arm. A nephropathy III. A symptomatic hypertonia.
the SUBSTANTIATION of the DIAGNOSIS AND DIFFERENTIAL DIAGNOSISTaking into account, that disease began in pullet age (23-25 flying), proceeded zlokachestvenno (high parameters of a glucose of a blood, predilection to hypoglycemic comas, fast progressing, a forwardness of serious complications), the family anamnesis not burdened on a sugar diabetes, we assume: diabetum melitous, 1 type, the serious form. Taking into account complaints of sick vision to deterioration only in last year, absence of exercise stresses, stressful situations, traumas, we assume: an angioretinopathia, oslozhdenie diabetum melitous. For specification of a condition of the patient and the diagnosis: consultation of the oculist, viewing of an out-patient dossier. Taking into account paleness, a cold snap of a skin of anticnemions, weakening of pulse a. dorsalis pedis, characteristic complaints of the patient, the long experience of smoking, we assume: an angiopathia of the bottom extremities. We can think and of a beginning obliterating endarteritis. For specification - consultation angiohirurga. Taking into account complaints of the patient on parestezii, cramps in ikronozhnyh muscles, changes pain chuvstvitelnsti, presence of trophic ulcers, dryness and an ecdysis of a skin, we assume: a distal sensory polyneuropatia. Trophic infringements of calcaneal areas of both stop (" diabetic ?O«»a") . For specification: consultation of the neurologist, a roentgenogram of anticnemions and stop. Taking into account presence purulent separated from a wound, an appreciable edema only one leg (right), a proof subfebrile fervescence of the patient, we assume a bacterial infection of a trophic ulcer right stops. For acknowledgement of the diagnosis: a tank. Crop, definition of sensitivity of microorganisms to antibiotics, crop of a blood on a sterility. Taking into account the expressed proteinuria (2,3 g/l), the expressed arterial hypertension, normal rate of a glomerular filtration, duration of disease about 23 flying, complaints of the patient on whining, nagging pains in the field of a loin, we assume: a nephropathy III. For specification of the diagnosis: ultrasonic of kidneys, consultation of the nephrologist. Taking into account cases of rising of a blood pressure up to 240 and 130, complaints of the patient to the strong headaches, arisen year back, some odutlovatost his persons, we assume: a symptomatic hypertonia (renal). For specification: More careful interrogation of the patient: whether there were in family sick hypertonic diseases, whether there were at him attacks of rising of a blood pressure, whether they were accompanied by unpleasant sensations. Studying of an out-patient dossier. Taking into account block of the patient, a memory impairment: we assume: initial attributes of an encephalopathy? Taking into account presence of pains at a palpation in the right hypochondrium, feeling of a bitter taste in a mouth, abusing alcohol a little bit flying back, we shall assume: a dyskinesia of biliferous ways. For specification of the diagnosis: consultation of the gastroenterologist to lead duodenalnoe intubation, to investigate chemical properties of a gall. It is possible, that the fatty dystrophia of a liver (diabetum melitous in an anamnesis, abusing alcohol) is observed. Taking into

account low parameters of a haemoglobin and erythrocytes of a blood, the normal CENTRAL PROCESSING UNIT, the expressed tachycardia, paleness of integuments of the patient, we assume: normohromnaja an anemia. Considering progressing of an anemia, morbidity in a zone of an epigastrium, presence of a liquid in an abdominal cavity, and also smoking of the patient, we assume: a bleeding. Taking into account, that at patients diabetum melitous pain sensitivity can be reduced, lead: macroscopical and an analysis of a feces (to estimate colour, a consistence, presence of a blood). Consultation of the surgeon, the gastroenterologist. To recommend antianemic preparations (Durules, Totema) .Uchityvaja complaints of the patient to pains in the field of heart, ischemic changes of a myocardium, attributes of a hypertrophy of the left departments of heart (on an electrocardiogram), constantly high blood pressure, we assume: Ischemic disease, stenocardia. The differentiation is required: strains or dormancy: detailed inquiry of the patient about his position, a condition, mood at the moment of occurrence of cardiac pains. If necessary - an exercise tolerance test. Probably also: an ischemic disease and a myocardiosclerosis as result of a diabetic macroangiopathia (vessels of heart are amazed). Consultation of the cardiologist, at the decision of a question on necessity koronaroarteriografii - the cardiosurgeon. Taking into account block of the patient, some odutlovatost his persons, presence in an anamnesis of serious endocrine disease - to hand over a blood on TTG and Т4. We shall deny a hypothyroidism.Thus, the diagnosis it is possible to add to the following points: a fatty dystrophia of a liver, a dyskinesia of biliferous ways, a diabetic macroangiopathia, an ischemic disease, a stenocardia of a strain. An anemia.
THE LEAF OF PURPOSES:
1. the Table №9. 2. 8.00 - humulin NPH 16 ED + aktropid 8 ED; 17.00 - humulin R 5 ED, 22.00 - humulin NPH
10 UNITS. In total for day of the patient receives 39ЕД. 3. Tab. Erythromycini 0,25 - on 2 tablets of 5 times in day. 4. Dressings with a lavage of wounds of 3 % solution Н2О2 (Sol. Hydrogenii peroxydi diluta -
20 ml) and hlorgeksidinom ( 5. Sol. Chlorhexidini 0,05 % - 500 ml). An aseptic bandage.
the DIARY of the PATIENT18.09. The surgeon. Granulating wounds on each side achille tendons, the area about 7 sm2. On walls of a wound - the purulent - necrotic discharge, is lead a partial cut of walls and a bottom of a wound. Positive dynamics, the area ranevoj surfaces is observed decreases. To continue dressings.the Curator. Complaints to whining pains in the field of anticnemions and stop. Not strong headache, a hymenium before eyes. Subfebrile temperature (37,1°С) Morbidity at a palpation in epigastric area. The patient is acyanotic, delayed, tired. Blood pressure 150 and 90, pulse 96, a frequency of respiratory movements 16. A tachycardia, cardiac sounds rhythmical, clear, intensifying of tones on an apex of heart, accent and splitting of 2-nd tone on an aorta.19.09. The surgeon. A trophic ulcer with scanty serozno-hemorrhagic separated.

the Curator. The patient recently has woken up, therefore looks delayed. The head does not hurt, the hymenium before eyes is kept. Complaints to whining pains in ikronozhnyh muscles. Temperature 37,0°С. a blood pressure 145 and 80, pulse 92 impacts in minute, a frequency of respiratory movements 14. The nystagmus is not present. Pain sensitivity on stops is reduced.
the EPICRISIS***** ********** **************, 46 flying has acted 15.07 with complaints to pains, a burning sensation, a pricking in ikronozhnyh muscles, presence on both legs is long not healing purulent wounds. 5-th finger on left stop and 3-rd - on the left brush are amputated. Marks dryness in a mouth, headaches, a giddiness, a hymenium before eyes. Strong delicacy. It is sick of a sugar diabetes during 21-22 flying. The flying was ill at 23-25, is acute, has lost in weight *gt; 40 kg. At initial hospitalization the level of a glucose in a blood has made 23 mmole/l. Constantly accepts preparations of an insulin. For the last 3 years the condition has worsened: trophic ulcers have appeared, vision has worsened, headaches and rising of a blood pressure up to 240 and 130 have appeared. Objectively: presence on both stops in area achille tendons of trophic ulcers with yellowish purulent separated. The expressed tachycardia (pulse about 100-105 in one minute). The patient is acyanotic, the plentiful diaphoresis is observed. The smell of an acetone is not present. Level of a glucose of a blood at 11.00 (15.07) - 23,8 mmole/l.the infection of wounds by a staphylococcal flora, sensitive to erythromycin, Oxacillinum, Cefazolinum Is revealed. The expressed proteinuria (2,3). On an electrocardiogram - attributes of ischemic changes of a forward wall and a septum of heart. On the basis of an anamnesis, inquiry, the inspection, the given laboratory and tool methods of treatment, the diagnosis is put: diabetum melitous, 1 type, the serious form, subindemnification. An angioretinopathia. An angiopathia of the bottom extremities. A distal sensory polyneuropatia. Trophic infringements of calcaneal areas of both stop. Amputating stump V of a finger left stops, III finger of the left arm. A nephropathy III. A symptomatic hypertonia. A fatty dystrophia of a liver, a dyskinesia of biliferous ways. An ischemic disease, a stenocardia of a strain. Normohromnaja an anemia.Disease proceeds hardly, with a plenty of burdensome complications, the forecast unfavourable.the Patient received preparations of an insulin (39 ED in day), an antibiotic erythromycin (2,5 g in day), dressings of wounds were carried out; the table №9 is appointed. During a presence in hospital the condition of the patient by way of correction diabetum melitous has improved (a level of a glucose has considerably come nearer to normal), but the general condition of the patient has become complicated by an anemia. In general treatment can be estimated as effective.References to the local doctor: To advise the patient to carry out exercises for conservation and improvements of a trophicity of extremities, to keep to a diet, supervise a level of a glucose in a blood, to eat it is high-grade and it is various. The patient should to stop smoke. To advise it to wear convenient clothes and footwear. To supervise a blood pressure of the patient, to pick up to it

antianginalnye preparations, constantly to watch a level of a cholesterin and blood lipids.
THE LITERATURE:
1. Dedov And. И., Melnichenko N.I., Fadeev " the Endocrinology. 2. " Algorithms of diagnosis and treatment of diseases endocrine ???ON?U" under
I.I.Dedova's edition. М., 1995. 3. G.Galstjan " Diabetic ?N®O«»aO?n". 4. M.I.Balabolkin " O?n«¬O??«?«u?n", М., 1998.
To discuss a material at a forum of a site
Keywords: a case history, an endocrinology, diabetum melitous, 1 type, the serious form, subindemnification, an angioretinopathia, an angiopathia of the bottom extremities, a distal sensory polyneuropatia
Subscribe for dispatch from Subscribe.Ru
For medical students and not only for them
All updating of a site - on your e-mail
Main | Abstracts, compositions, lectures | Psychiatry | LinksForum | Guest bookMirror [max.1gb.ru [file /eng/learn/ib005.shtml [at Fri, 06 Feb 2009 06:38:25 GMT]]]
quick
job.student.max
Enter your e-mail OK
list_job.student.m
1

About Us | Privacy Policy | Site MapMarch 20, 2010
home > diabetes center > diabetes a-z list > diabetes mellitus index > diabetes mellitus article
Font Size
A
A
A
1 2 3 4 5 6 7 8
Next »
Diabetes Mellitus Index Glossary
Find a Local Doctor
Diabetes Mellitus
Type 2 Diabetes Slideshow
Quiz: Are You At Risk for Diabetic Nerve Pain?
Diabetes and Foot Problems Slideshow
Medical Author: Ruchi Mathur, MD Medical Editor: William C. Shiel, Jr., MD, FACP, FACR
What is diabetes? What is the impact of diabetes?
What causes diabetes? What are the different types of diabetes?
What are diabetes symptoms? How is diabetes diagnosed?
From WebMD
Diabetes Resources
Safe Ways to Exercise With Diabetes
Featured Centers
Foods That Can Trigger Bedwetting
Is Your Emphysema Under Control?
8 Ways to Boost Your Fertility
Health Solutions
Depression Med for You?
Fibromyalgia Center
MS Rx Options
Featured on MedicineNet
Is Sleepiness Hurting You?Check Your Fibromyalgia Symptoms Causes of Fatigue Slideshow
Are You at Risk for Diabetic Nerve Pain?
Trouble Breathing? Take the COPD Health Check
Top 10
Diabetes Mellitus Related Articles
Blood Clots Cellulitis
Creatinine Blood Test Electrolytes
Glucose Tolerance Test Heart Attack
Hemoglobin A1c Test Hypoglycemia
Stroke Triglyceride Test
Complete List »
Diabetes Topics
Diabetic Nerve Pain Quiz Diabetic Ketoacidosis Lower Cholesterol
Diabetes Diabetes Treatment
Diabetes RSS
Latest Diabetes News

Selenium Could Shield Against Diabetes
FDA OKs Insulin Pump Plus Glucose Monitor System
Online, Phone Tests Assess Diabetes Risk
Salsalate May Help Treat Type 2 Diabetes
Health Tip: Symptoms of Ketoacidosis
Want More News? Sign Up for MedicineNet
Newsletters!
Health News Feed
Why is blood sugar checked at home? What are the acute complications of diabetes? What are the chronic complications of diabetes?
What can be done to slow diabetes complications? Diabetes At A Glance
Type 2 Diabetes - Slideshow Quiz: Are You At Risk for Diabetic Nerve Pain?
Diabetes and Foot Problems - Slideshow Patient Discussions: Diabetes - Symptoms at Onset of Disease
Find a local Endocrinologist in your town
Diabetes Medication
Victoza (liraglutide) Once-Daily Injection
The U.S. Food and Drug Administration today approved Victoza (liraglutide), a once-daily injection to treat type 2
diabetes in some adults.
Victoza is intended to help lower blood sugar levels along with diet, exercise, and selected other diabetes medicines. It is not recommended as initial therapy in patients who have not achieved adequate diabetes control
on diet and exercise alone.
Insulin is a hormone that helps prevent sugar (glucose) from building up in the blood. People with type 2 diabetes have difficulty making and using
insulin. Victoza is in a class of medicines known as glucagon-like peptide-1 (GLP-1) receptor agonists that help the pancreas make more insulin after
eating a meal.
"Diabetes is a leading cause of death and disability, with more than 1.5 million new cases diagnosed annually," said Mary Parks, M.D., director, Division of Metabolism and Endocrinology Products in the FDA's Center for Drug Evaluation and Research. "Controlling blood sugar levels is very
important to preventing or reducing the long term complications of diabetes, and Victoza offers certain patients with type 2 diabetes a treatment
option for controlling their blood glucose levels."
Read more about Victoza (liraglutide) »
SOURCE: FDA Press Release
What is diabetes?
Diabetes mellitus is a group of metabolic diseases characterized by high
Diabetes
Gastroparesis »
What is gastroparesis?
Gastroparesis means paralysis of the muscles of the stomach. Gastroparesis results in delayed emptying of food from the stomach into the small intestine.
The stomach is a hollow organ composed primarily of muscle that serves as a storage container for food. Food in the stomach is ground into tiny pieces by the constant churning that is generated by the contractions of the stomach's muscles. Once the food has been adequately ground, it slowly is emptied from the stomach into the intestine in a metered fashion. Only food ground into small particles can be emptied from the stomach in a normal fashion, and smaller particles are digested better in the intestine. Moreover, the metering process allows the emptied food to be well-mixed with the digestive juices of the intestine, pancreas, and liver (bile) and to be absorbed well from the intestine.
When the stomach's muscles are paralyzed, food is not thoroughly grou...
Read the Gastroparesis article »

blood sugar (glucose) levels, that result from defects in insulin secretion, or action, or both. Diabetes mellitus, commonly referred to as diabetes (as it
will be in this article) was first identified as a disease associated with "sweet urine," and excessive muscle loss in the ancient world. Elevated
levels of blood glucose (hyperglycemia) lead to spillage of glucose into the urine, hence the term sweet urine.
Normally, blood glucose levels are tightly controlled by insulin, a hormone produced by the pancreas. Insulin lowers the blood glucose level. When the blood glucose elevates (for example, after eating food), insulin is released from the pancreas to normalize the glucose level. In patients with diabetes,
the absence or insufficient production of insulin causes hyperglycemia. Diabetes is a chronic medical condition, meaning that although it can be
controlled, it lasts a lifetime.
What is the impact of diabetes?
Over time, diabetes can lead to blindness, kidney failure, and nerve damage. These types of damage are the result of damage to small vessels,
referred to as microvascular disease. Diabetes is also an important factor in accelerating the hardening and narrowing of the arteries (atherosclerosis),
leading to strokes, coronary heart disease, and other large blood vessel diseases. This is referred to as macrovascular disease. Diabetes affects
approximately 17 million people (about 8% of the population) in the United States. In addition, an estimated additional 12 million people in the United
States have diabetes and don't even know it.
From an economic perspective, the total annual cost of diabetes in 1997 was estimated to be 98 billion dollars in the United States. The per capita
cost resulting from diabetes in 1997 amounted to $10,071.00; while healthcare costs for people without diabetes incurred a per capita cost of $2,699.00. During this same year, 13.9 million days of hospital stay were
attributed to diabetes, while 30.3 million physician office visits were diabetes related. Remember, these numbers reflect only the population in
the United States. Globally, the statistics are staggering.
Diabetes is the third leading cause of death in the United States after heart disease and cancer.
What causes diabetes?
Insufficient production of insulin (either absolutely or relative to the body's needs), production of defective insulin (which is uncommon), or the
inability of cells to use insulin properly and efficiently leads to hyperglycemia and diabetes. This latter condition affects mostly the cells of

muscle and fat tissues, and results in a condition known as "insulin resistance." This is the primary problem in type 2 diabetes. The absolute lack of insulin, usually secondary to a destructive process affecting the
insulin producing beta cells in the pancreas, is the main disorder in type 1 diabetes. In type 2 diabetes, there also is a steady decline of beta cells that
adds to the process of elevated blood sugars. Essentially, if someone is resistant to insulin, the body can, to some degree, increase production of
insulin and overcome the level of resistance. After time, if production decreases and insulin cannot be released as vigorously, hyperglycemia
develops.
Glucose is a simple sugar found in food. Glucose is an essential nutrient that provides energy for the proper functioning of the body cells.
Carbohydrates are broken down in the small intestine and the glucose in digested food is then absorbed by the intestinal cells into the bloodstream,
and is carried by the bloodstream to all the cells in the body where it is utilized. However, glucose cannot enter the cells alone and needs insulin to aid in its transport into the cells. Without insulin, the cells become starved
of glucose energy despite the presence of abundant glucose in the bloodstream. In certain types of diabetes, the cells' inability to utilize glucose gives rise to the ironic situation of "starvation in the midst of
plenty". The abundant, unutilized glucose is wastefully excreted in the urine.
Insulin is a hormone that is produced by specialized cells (beta cells) of the pancreas. (The pancreas is a deep-seated organ in the abdomen located
behind the stomach.) In addition to helping glucose enter the cells, insulin is also important in tightly regulating the level of glucose in the blood. After a
meal, the blood glucose level rises. In response to the increased glucose level, the pancreas normally releases more insulin into the bloodstream to help glucose enter the cells and lower blood glucose levels after a meal. When the blood glucose levels are lowered, the insulin release from the
pancreas is turned down. It is important to note that even in the fasting state there is a low steady release of insulin than fluctuates a bit and helps to
maintain a steady blood sugar level during fasting. In normal individuals, such a regulatory system helps to keep blood glucose levels in a tightly
controlled range. As outlined above, in patients with diabetes, the insulin is either absent, relatively insufficient for the body's needs, or not used
properly by the body. All of these factors cause elevated levels of blood glucose (hyperglycemia).

1 2 3 4 5 6 7 8
Next »
Diabetes Mellitus Index Glossary
Find a Local Doctor
Next: What are the different types of diabetes? »
Share | | | | | More
Diabetes - Symptoms at Onset of Disease
The MedicineNet physician editors ask:

The symptoms of diabetes can vary greatly from patient to patient. What were your symptoms at the onset of your disease?
Comment submissions for this question have ended. See 20 Viewer Comments
View Comments
Suggested Reading by Our Doctors
ACE Inhibitors - Read about ACE inhibitors like Altace, lisinopril, enalapril, ramparil, Zestril and more. Information includes side effects, drug interactions, and
pregnancy safety information. Creatinine Blood Test - Learn more about the creatinine blood test, a test that
measures kidney function. Abnormal creatinine levels in the blood may indicate kidney disease.

Home Remedies Baby Names Food Worship Art
Home » Health » Conditions
Diabetes Home RemediesDiabetes can be treated naturally with herbal ingredients like stevia, gymnema, fenugreek, bittergourd, green tea, turmeric and neem. Diabetes is a chronic health problem which is caused by elevated blood sugar contents. Blood sugar, or glucose is needed to supply energy for every cell in the body. If glucose levels become too elevated, then they become toxic to the brain and other organs. Diabetes is characterized by elevated blood glucose levels and by the excretion of excess glucose in the urine. The absolute or relative lack of insulin can lead to abnormal metabolism of carbohydrates, fat and proteins.
Diabetes is described as a "prosperity disease" as it is caused by over-eating and consequent obesity. It is caused not just by overeating of sugar and carbohydrates, but also of proteins and fats, as they are also transformed to sugar when taken in excess. Excess food taxes the pancreas and eventually paralyses its normal functioning. Grief, worry and anxiety can also cause fluctuations in sugar metabolism. Grave diseases like cancer, tuberculosis and cerebral diseases can trigger diabetes. Heredity plays a major role in causing diabetes as well.
There are three types of diabetes. Type 1 diabetes affects children mostly and type three or gestational diabetes occurs during pregnancy. Type 2 diabetes is the most prevalent and also called adult-onset or non-insulin dependent diabetes. In this case, the body produces sufficient insulin, but the insulin and the glucose it transports cannot effectively enter into cells. Gestational diabetes affect pregnant women.
Diabetes Symptoms
Diabetes goes undetected for a long time as they do not produce serious, obvious symptoms. Do watch out for strong thirst, frequent urination, excessive appetite, weight loss, fatigue, irritability and blurred vision. In diabetics, the urine maybe pale in color, with an acidic reaction and a sweet odor. They also look pale, may suffer from secondary issues like anemia, constipation, intense itching around the genital region, palpitations and general weakness.
Diabetes Lifestyle Choices
Regular exercise is one of the best ways to help the cells use glucose efficiently and keep the blood sugar from climbing to dangerous levels. Exercise also helps the body to lose
DiabetesWMD http://w w w .medi http://w w w .medi Enter email address
01575578227320 FORID:10 UTF-8 Search
w w w .desigram.c

weight and use insulin more effectively. In the long term, it may also reduce insulin resistance.
Instead of eating three large meals, have several smaller meals throughout the day to keep insulin and blood sugar steady. Do not go longer than three hours without eating.
Don't smoke or expose yourself to second hand smoke. Diabetics are more vulnerable to heart and kidney damage, both of which are linked to smoking.
Poor circulation and nerve damage can lead to foot ulcers in diabetics. Ensure good circulation in the feet by wearing shoes that fit well.
Diabetes Diet
Eat foods that are rich in fiber. Fiber slows intestinal absorption of sugar and smoothes out blood sugar levels. Pears, beans, barley, blackberries and chick-peas are some sources of fiber.
Okra is prescribed in Ayurveda as a remedy for blood sugar. Okra is quite delicious as a steamed or roasted vegetable.
Prickly pear cactus is available in the Mexican sections of the grocery store. The pads can be diced and used in a salad or taco. It helps with diabetes, obesity and elevated blood cholesterol.
Dandelion greens are hypoglycemic and they can be juiced or chopped into salads and soups. Ingesting dandelion can improve lipid profiles, cholesterol and triglycerides in diabetic patients.
Cinnamon, nutmeg, cashew, cayenne, ginger, turmeric, bay leaf, coriander seed, turnip, lettuce, cabbage, cranberry, papaya fruit, millet, Jeruselam artichoke, barley, oats and buckwheat are a few other foods helpful for a diabetic. Incorporate some of them into your diet everyday.
Diabetes Herbal Remedies
Turmeric Therapy For Diabetes
One tsp of turmeric is added to some gooseberry(amla) juice and this mixture is consumed everyday. Alternatively, turmeric extracts or capsules can be taken. This is very effective in normalizing the blood glucose levels and reducing insulin resistance. .Read other Turmeric home remedies.
Fenugreek lowers Blood Sugar
Fenugreek is a good blood-sugar lowering herb. It is also cheap and can be easily worked into dishes. It has a high soluble fiber content and alkaloids, which help with delayed gastric emptying, slow carbohydrate absorption and glucose transport. Fenugreek may also increase the number of insulin receptors in red blood cells and improve glucose utilization in peripheral tissues, thus showing anti-diabetic properties in the pancreas and other organs. Read other Fenugreek home remedies.

Onion and Garlic help Sugar Metabolism
Onions and garlic are significant hypoglycemic. The allicin and diallyl disulphide chemicals present in these lower glucose levels by competing with insulin in the liver. Clinical studies have shown that allicin in garlic combines with Vitamin B1 and stimulate the pancrease to release more insulin. It also arrests the chemical receptors that deactivate insulin. Onion and garlic not only help with insulin normalization, but also provide significant cardiovascular benefits as well. Read other Garlic home remedies .
Cinnamon helps Type 2 Diabetes
Cinnamon is beneficial to Type 2 diabetes as it can reduce blood sugar levels and increase the body's natural production of insulin. It can also improve cholesterol metabolism, remove artery-damaging free radicals from the blood and improve the functioning of the blood vessels. Try to consume half a teaspoon of cinnamon before breakfast, for about 40 days. You can also add cinnamon in your diet by sprinkling it in your cereal, tea or entree. .Read other Cinnamon home remedies.
Aloe Vera Diabetes Home Remedy
Aloe juice is believed to lower blood sugar levels in people with type 2 diabetes. Aloe contains two chemicals - mannose and glucomannon; mannose helps open up the blood vessels and glucomannon helps in triglyceride production. Check out food grade Aloe juice in your neighbourhood. Read other Aloe home remedies.
Chicory Benefit For Diabetes
Chicory is very beneficial to diabetics as it contains Inulin, a fiber that has a low glycemic index and controls blood sugar levels. It can be used as a sweetner and added to beverages. Chicory not only helps with blood sugar, but also reduces the serum LDL cholesterol levels in the blood. .Read other Chicory home remedies. .
Neem reduces Insulin dependency
Neem can reduce insulin requirements without altering blood glucose levels. Regular consumption of neem decoction or neem tablets is an effective alternative therapy for diabetes. Read other Neem home remedies.
Amla reduces Blood Sugar
One teaspoon of Amla juice mixed with a cup of bitter gourd juice is prescribed by naturopaths as it stimulates the Pancreas and it will secrete enough insulin for reducing blood sugar. Amla seeds or dried amla is equally invaluable for the control of Diabetes. .Read other Amla home remedies.

Mango Leaves for Diabetics
Diabetics fear ripe mangoes for their high sugar content! But, mango leaves help normalize insulin levels in the blood. Boil a few mango leaves in water and allow it to saturate through the night. Consume the filtered decoction in the morning for diabetic home remedy. Alternatively, dry mango leaves, powder and store. Add about a teaspoon and boil in water and consume the filtered decoction. .Read other Mango home remedies.
Ashwagandha Treatment For Diabetic Neuropathy
Ashwagandha, renowned for its adaptogenic and anti-inflammatory properties is very effective in cases of diabetic neuropathy. It improves the weakness, fatigue and weight loss due to diabetes. Ashwagandha can be consumed as capsules or tinctures. Read other Ashwagandha home remedies.
Tinospora help for Diabetes
Tinospora is very effective in resolving the symptoms of diabetes. Boil the stem pieces in 500 ml of water for 30 minutes. Drink 50 ml of this tinospora extract twice daily for a month. There will be a marked improvement in the condition. Read other Tinospora home remedies.
Bitter Gourd Diabetes Remedy
Bitter gourd or Karela(in Hindi) or balsam pear is a vegetable grown in Asia, Africa and South America. It contains a hypoglycemic or insulin-like principle, termed as "plant insulin". It has been found to lower blood and urine sugar levels. Bitter gourd contain a lectin which links together with insulin receptors and provide a way for managing Type 2 diabetes. Excessive usage of bitter gourd can cause diarrhea and abdominal discomfort. People with hypoglycemia or low sugar levels should not take this.
Gymnema kills Sugar Cravings
Gurmar, another name for Gymnema, means "killer of sweet" in Sansktrit. It can lower blood sugar, blood fats, triglycerides, and cholesterol, and repair the liver, kidney and muscle tissues. It shows potential for fixing pancreas malfunction, raising insulin output to normal levels. Gymnema also acts on taste buds and the surface of the intestines, and reduces the appeal for sugary foods. It is promising herb for both Type I and Type II diabetes.
Stevia, the better sweetner
Stevia is thirty times sweeter than sugar and yet has 1 calorie per 10 leaves, and it is totally natural. It has a long history of use in South America and holds promise as a

sweetener for diabetics. Stevia has been found to lower blood sugar and blood pressure. It also does not cause tooth decay like regular sugars.
Green Tea's role in Diabetes
Green Tea contain catechins and epicatechins, plant compounds belonging to the flavonol category. They are powerful antioxidants and found to be beneficial for diabetes. Green tea can be consumed as a beverage, or a decaffeinated version can be ingested as capsules.
Apple Cider Vinegar usage for Diabetes
Apple cider vinegar has shown to reduce the raise of blood sugar after the consumption of a high carbohydrate meal. Fermented foods like apple cider vinegar that contain acetic acid has been shown to lower blood sugar by helping store excess glucose in the liver, thus reducing the body's rate of glucose production and absorption. Try to purchase apple cider vinegar that is least processed and dark. Two teaspoons of apple cider vinegar can be diluted in a cup of water and taken before the meal. You could also add the vinegar to your salad or main course.
Diabetes, Healing With Supplements
Vitamin C
Vitamin C helps prevent the sugar inside the cells from converting to sorbitol, a sugar alcohol that cells can neither burn for energy nor move out. Vitamin C may also be beneficial in diminishing the damage to proteins caused by free radicals. Dietary sorbitol is not a danger to diabetics though, as it is poorly absorbed and is not transported into the cells. Citrus fruits, guava and papaya are rich in Vitamin C. More on Vitamin C.
Vitamin E
Diabetics need more anti-oxidant protection than normal, Vitamin E helps alleviate some of those risks to the heart. Diabetics are two to four times more vulnerable to heart conditions. Vitamin E reduces the tendency for sugar to stick to proteins in the blood and can lower the percentage of triglycerides. More on Vitamin E
Magnesium
Magnesium is Anti-diabetic: It helps release insulin, maintenance of pancreatic insulin production cells, and maintenance of affinity and number of insulin receptors. More on Magnesium.
Chromium

Deficiency in Chromium not only affects sugar metabolism, but worsen the secondary symptoms of numbness, tingling and pain in the hands and legs. Chromium is a key player in sugar metabolism and hooks up with insulin in transporting sugar through the cell membrane and into the cell. Brewer's yeast, wheat germ, whole grains, cheese, soy products, onions and garlic are rich in chromium.
B Complex Vitamins
Vitamin B6, B12 and Biotin have important roles to play in sugar metabolism. Vitamin B6 deficiency can cause glucose intolerance, there is an abnormal increase in blood sugar after eating. People with diabetes tend to be low in B Vitamins, partly because the disease uses up most of them or they are improperly absorbed and excreted in the urine.
Conditions/Diseaseso Acne Home Remedies o Alcoholism Home Remedies o Allergy Home Remedies o Anemia Home Remedies o Arthritis Home Remedies o Hypertension Home Remedies o Cholesterol Home Remedies o Common Cold Remedies o Constipation Home Remediess o Depression Home Remedies o Diabetes Home Remedies o Endometriosis Remedies o Ear Infection Remedies o Fibromyalgia Treatment o Gingivitis Home Remedies o Indigestion Home Remedies o Insomnia Home Remedies o Kidney Stones Remedies o Obesity Home Remedies o Osteoporosis Treatment o PMS, Natural Relief o UTI Home Remedies o Weight Loss Tips
Natural Ingredientso Ajowan Health Benefits o Almond Health Benefits o Aloe Vera Health Benefits o Amla Health Benefits

o Arjuna Health Benefits o Asafoetida Health Benefits o Ashgourd Health Benefits o Ashoka Health Benefits o Ashwagandha Health Benefits o Babool Health Benefits o Bael Health Benefits o Bamboo Health Benefits o Banana Health Benefits o Banyan Health Benefits o Betel-Leaves Benefits o Betel-Nut Health Benefits o Black-Pepper Health Benefits o Brahmi Health Benefits o Camphor Health Benefits o Cardamom Health Benefits o Castor Health Benefits o Chicory Health Benefits o Cinnamon Health Benefits o Clove Health Benefits o Coriander Health Benefits o Cumin Health Benefits o Dates Health Benefits o Fennel Health Benefits o Fenugreek Health Benefits o Garlic Health Benefits o Ginger Health Benefits o Lime Health Benefits o Malabar Nut Benefits o Mango Health Benefits o Neem Oil Health Benefits o Pomegranate Health Benefits o Tamarind Health Benefits o Tea Health Benefits o Tinospora Health Benefits o Turmeric Health Benefits o More...
Start of page
Home Remedies Natural Ingredients Nutrition Vitamins Minerals
© 2010 All Rights Reserved •
About • Sitemap • Privacy Policy • Disclaimer

Skip to main page content
Home Current Issue Archive Contact Subscribe Alerts Help
Search GO Advanced Search »
User Name Password Sign In
Diagnosis and Classification of Diabetes Mellitus 1. American Diabetes Association
FPG, fasting plasma glucose
GAD, glutamic acid decarboxylase
GCT, glucose challenge test
GDM, gestational diabetes mellitus
HNF, hepatocyte nuclear factor
IFG, impaired fasting glucose
IGT, impaired glucose tolerance
MODY, maturity-onset diabetes of the young
WHO, World Health Organization
Next Section
Search yes
User Name http://care.diabete

DEFINITION AND DESCRIPTION OF DIABETES MELLITUSDiabetes mellitus is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. The chronic hyperglycemia of diabetes is associated with long-term damage, dysfunction, and failure of various organs, especially the eyes, kidneys, nerves, heart, and blood vessels.
Several pathogenic processes are involved in the development of diabetes. These range from autoimmune destruction of the β-cells of the pancreas with consequent insulin deficiency to abnormalities that result in resistance to insulin action. The basis of the abnormalities in carbohydrate, fat, and protein metabolism in diabetes is deficient action of insulin on target tissues. Deficient insulin action results from inadequate insulin secretion and/or diminished tissue responses to insulin at one or more points in the complex pathways of hormone action. Impairment of insulin secretion and defects in insulin action frequently coexist in the same patient, and it is often unclear which abnormality, if either alone, is the primary cause of the hyperglycemia.
Symptoms of marked hyperglycemia include polyuria, polydipsia, weight loss, sometimes with polyphagia, and blurred vision. Impairment of growth and susceptibility to certain infections may also accompany chronic hyperglycemia. Acute, life-threatening consequences of uncontrolled diabetes are hyperglycemia with ketoacidosis or the nonketotic hyperosmolar syndrome.
Long-term complications of diabetes include retinopathy with potential loss of vision; nephropathy leading to renal failure; peripheral neuropathy with risk of foot ulcers, amputations, and Charcot joints; and autonomic neuropathy causing gastrointestinal, genitourinary, and cardiovascular symptoms and sexual dysfunction. Patients with diabetes have an increased incidence of atherosclerotic cardiovascular, peripheral arterial, and cerebrovascular disease. Hypertension and abnormalities of lipoprotein metabolism are often found in people with diabetes.
The vast majority of cases of diabetes fall into two broad etiopathogenetic categories (discussed in greater detail below). In one category, type 1 diabetes, the cause is an absolute deficiency of insulin secretion. Individuals at increased risk of developing this type of diabetes can often be identified by serological evidence of an autoimmune pathologic process occurring in the pancreatic islets and by genetic markers. In the other, much more prevalent category, type 2 diabetes, the cause is a combination of resistance to insulin action and an inadequate compensatory insulin secretory response. In the latter category, a degree of hyperglycemia sufficient to cause pathologic and functional changes in various target tissues, but without clinical symptoms, may be present for a long period of time before diabetes is detected. During this asymptomatic period, it is possible to demonstrate an abnormality in carbohydrate metabolism by measurement of plasma glucose in the fasting state or after a challenge with an oral glucose load.
The degree of hyperglycemia (if any) may change over time, depending on the extent of the underlying disease process (Fig. 1). A disease process may be present but may not have progressed far enough to cause hyperglycemia. The same disease process can cause impaired fasting glucose (IFG) and/or impaired glucose tolerance (IGT) without fulfilling the criteria for the diagnosis of diabetes. In some individuals with diabetes, adequate glycemic control can be achieved with weight reduction, exercise, and/or oral glucose-lowering agents. These individuals therefore do not require insulin. Other individuals who have some residual insulin secretion but require exogenous insulin for adequate glycemic control can survive without it. Individuals with extensive β-cell destruction and therefore no residual insulin secretion require insulin for survival. The severity of the metabolic abnormality can progress, regress, or stay the same. Thus, the degree of hyperglycemia reflects the severity of the underlying metabolic process and its treatment more than the nature of the process itself.
Previous SectionNext Section
CLASSIFICATION OF DIABETES MELLITUS AND OTHER CATEGORIES OF GLUCOSE REGULATION

Assigning a type of diabetes to an individual often depends on the circumstances present at the time of diagnosis, and many diabetic individuals do not easily fit into a single class. For example, a person with gestational diabetes mellitus (GDM) may continue to be hyperglycemic after delivery and may be determined to have, in fact, type 2 diabetes. Alternatively, a person who acquires diabetes because of large doses of exogenous steroids may become normoglycemic once the glucocorticoids are discontinued, but then may develop diabetes many years later after recurrent episodes of pancreatitis. Another example would be a person treated with thiazides who develops diabetes years later. Because thiazides in themselves seldom cause severe hyperglycemia, such individuals probably have type 2 diabetes that is exacerbated by the drug. Thus, for the clinician and patient, it is less important to label the particular type of diabetes than it is to understand the pathogenesis of the hyperglycemia and to treat it effectively.
Type 1 diabetes (β-cell destruction, usually leading to absolute insulin deficiency)
Immune-mediated diabetes.This form of diabetes, which accounts for only 5–10% of those with diabetes, previously encompassed by the terms insulin-dependent diabetes, type I diabetes, or juvenile-onset diabetes, results from a cellular-mediated autoimmune destruction of the β-cells of the pancreas. Markers of the immune destruction of the β-cell include islet cell autoantibodies, autoantibodies to insulin, autoantibodies to glutamic acid decarboxylase (GAD65), and autoantibodies to the tyrosine phosphatases IA-2 and IA-2β. One and usually more of these autoantibodies are present in 85–90% of individuals when fasting hyperglycemia is initially detected. Also, the disease has strong HLA associations, with linkage to the DQA and DQB genes, and it is influenced by the DRB genes. These HLA-DR/DQ alleles can be either predisposing or protective.
In this form of diabetes, the rate of β-cell destruction is quite variable, being rapid in some individuals (mainly infants and children) and slow in others (mainly adults). Some patients, particularly children and adolescents, may present with ketoacidosis as the first manifestation of the disease. Others have modest fasting hyperglycemia that can rapidly change to severe hyperglycemia and/or ketoacidosis in the presence of infection or other stress. Still others, particularly adults, may retain residual β-cell function sufficient to prevent ketoacidosis for many years; such individuals eventually become dependent on insulin for survival and are at risk for ketoacidosis. At this latter stage of the disease, there is little or no insulin secretion, as manifested by low or undetectable levels of plasma C-peptide. Immune-mediated diabetes commonly occurs in childhood and adolescence, but it can occur at any age, even in the 8th and 9th decades of life.
Autoimmune destruction of β-cells has multiple genetic predispositions and is also related to environmental factors that are still poorly defined. Although patients are rarely obese when they present with this type of diabetes, the presence of obesity is not incompatible with the diagnosis. These patients are also prone to other autoimmune disorders such as Graves’ disease, Hashimoto’s thyroiditis, Addison’s disease, vitiligo, celiac sprue, autoimmune hepatitis, myasthenia gravis, and pernicious anemia.
Idiopathic diabetes.Some forms of type 1 diabetes have no known etiologies. Some of these patients have permanent insulinopenia and are prone to ketoacidosis, but have no evidence of autoimmunity. Although only a minority of patients with type 1 diabetes fall into this category, of those who do, most are of African or Asian ancestry. Individuals with this form of diabetes suffer from episodic ketoacidosis and exhibit varying degrees of insulin deficiency between episodes. This form of diabetes is strongly inherited, lacks immunological evidence for β-cell autoimmunity, and is not HLA associated. An absolute requirement for insulin replacement therapy in affected patients may come and go.
Type 2 diabetes (ranging from predominantly insulin resistance with relative insulin deficiency to predominantly an insulin secretory defect with insulin resistance)

This form of diabetes, which accounts for ∼90–95% of those with diabetes, previously referred to as non-insulin-dependent diabetes, type II diabetes, or adult-onset diabetes, encompasses individuals who have insulin resistance and usually have relative (rather than absolute) insulin deficiency At least initially, and often throughout their lifetime, these individuals do not need insulin treatment to survive. There are probably many different causes of this form of diabetes. Although the specific etiologies are not known, autoimmune destruction of β-cells does not occur, and patients do not have any of the other causes of diabetes listed above or below.
Most patients with this form of diabetes are obese, and obesity itself causes some degree of insulin resistance. Patients who are not obese by traditional weight criteria may have an increased percentage of body fat distributed predominantly in the abdominal region. Ketoacidosis seldom occurs spontaneously in this type of diabetes; when seen, it usually arises in association with the stress of another illness such as infection. This form of diabetes frequently goes undiagnosed for many years because the hyperglycemia develops gradually and at earlier stages is often not severe enough for the patient to notice any of the classic symptoms of diabetes. Nevertheless, such patients are at increased risk of developing macrovascular and microvascular complications. Whereas patients with this form of diabetes may have insulin levels that appear normal or elevated, the higher blood glucose levels in these diabetic patients would be expected to result in even higher insulin values had their β-cell function been normal. Thus, insulin secretion is defective in these patients and insufficient to compensate for insulin resistance. Insulin resistance may improve with weight reduction and/or pharmacological treatment of hyperglycemia but is seldom restored to normal The risk of developing this form of diabetes increases with age, obesity, and lack of physical activity. It occurs more frequently in women with prior GDM and in individuals with hypertension or dyslipidemia, and its frequency varies in different racial/ethnic subgroups. It is often associated with a strong genetic predisposition, more so than is the autoimmune form of type 1 diabetes. However, the genetics of this form of diabetes are complex and not clearly defined.
Other specific types of diabetes
Genetic defects of the β-cell.Several forms of diabetes are associated with monogenetic defects in β-cell function. These forms of diabetes are frequently characterized by onset of hyperglycemia at an early age (generally before age 25 years). They are referred to as maturity-onset diabetes of the young (MODY) and are characterized by impaired insulin secretion with minimal or no defects in insulin action. They are inherited in an autosomal dominant pattern. Abnormalities at six genetic loci on different chromosomes have been identified to date. The most common form is associated with mutations on chromosome 12 in a hepatic transcription factor referred to as hepatocyte nuclear factor (HNF)-1α. A second form is associated with mutations in the glucokinase gene on chromosome 7p and results in a defective glucokinase molecule. Glucokinase converts glucose to glucose-6-phosphate, the metabolism of which, in turn, stimulates insulin secretion by the β-cell. Thus, glucokinase serves as the “glucose sensor” for the β-cell. Because of defects in the glucokinase gene, increased plasma levels of glucose are necessary to elicit normal levels of insulin secretion. The less common forms result from mutations in other transcription factors, including HNF-4α, HNF-1β, insulin promoter factor (IPF)-1, and NeuroD1.
Point mutations in mitochondrial DNA have been found to be associated with diabetes mellitus and deafness The most common mutation occurs at position 3243 in the tRNA leucine gene, leading to an A-to-G transition. An identical lesion occurs in the MELAS syndrome (mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like syndrome); however, diabetes is not part of this syndrome, suggesting different phenotypic expressions of this genetic lesion.
Genetic abnormalities that result in the inability to convert proinsulin to insulin have been identified in a few families, and such traits are inherited in an autosomal dominant pattern. The resultant glucose intolerance is mild. Similarly, the production of mutant insulin molecules with resultant impaired receptor binding has also been identified in a few families and is associated with an autosomal inheritance and only mildly impaired or even normal glucose metabolism.
Genetic defects in insulin action.There are unusual causes of diabetes that result from genetically determined abnormalities of insulin action. The metabolic abnormalities associated with mutations of the insulin receptor may

range from hyperinsulinemia and modest hyperglycemia to severe diabetes. Some individuals with these mutations may have acanthosis nigricans. Women may be virilized and have enlarged, cystic ovaries. In the past, this syndrome was termed type A insulin resistance. Leprechaunism and the Rabson-Mendenhall syndrome are two pediatric syndromes that have mutations in the insulin receptor gene with subsequent alterations in insulin receptor function and extreme insulin resistance. The former has characteristic facial features and is usually fatal in infancy, while the latter is associated with abnormalities of teeth and nails and pineal gland hyperplasia.
Alterations in the structure and function of the insulin receptor cannot be demonstrated in patients with insulin-resistant lipoatrophic diabetes. Therefore, it is assumed that the lesion(s) must reside in the postreceptor signal transduction pathways.
Diseases of the exocrine pancreas.Any process that diffusely injures the pancreas can cause diabetes. Acquired processes include pancreatitis, trauma, infection, pancreatectomy, and pancreatic carcinoma. With the exception of that caused by cancer, damage to the pancreas must be extensive for diabetes to occur; adrenocarcinomas that involve only a small portion of the pancreas have been associated with diabetes. This implies a mechanism other than simple reduction in β-cell mass. If extensive enough, cystic fibrosis and hemochromatosis will also damage β-cells and impair insulin secretion. Fibrocalculous pancreatopathy may be accompanied by abdominal pain radiating to the back and pancreatic calcifications identified on X-ray examination. Pancreatic fibrosis and calcium stones in the exocrine ducts have been found at autopsy.
Endocrinopathies.Several hormones (e.g., growth hormone, cortisol, glucagon, epinephrine) antagonize insulin action. Excess amounts of these hormones (e.g., acromegaly, Cushing’s syndrome, glucagonoma, pheochromocytoma, respectively) can cause diabetes. This generally occurs in individuals with preexisting defects in insulin secretion, and hyperglycemia typically resolves when the hormone excess is resolved.
Somatostatinoma- and aldosteronoma-induced hypokalemia can cause diabetes, at least in part, by inhibiting insulin secretion. Hyperglycemia generally resolves after successful removal of the tumor.
Drug- or chemical-induced diabetes.Many drugs can impair insulin secretion. These drugs may not cause diabetes by themselves, but they may precipitate diabetes in individuals with insulin resistance. In such cases, the classification is unclear because the sequence or relative importance of β-cell dysfunction and insulin resistance is unknown. Certain toxins such as Vacor (a rat poison) and intravenous pentamidine can permanently destroy pancreatic β-cells. Such drug reactions fortunately are rare. There are also many drugs and hormones that can impair insulin action. Examples include nicotinic acid and glucocorticoids. Patients receiving α-interferon have been reported to develop diabetes associated with islet cell antibodies and, in certain instances, severe insulin deficiency. The list shown in Table 1 is not all-inclusive, but reflects the more commonly recognized drug-, hormone-, or toxin-induced forms of diabetes.
Infections.Certain viruses have been associated with β-cell destruction. Diabetes occurs in patients with congenital rubella, although most of these patients have HLA and immune markers characteristic of type 1 diabetes. In addition, coxsackievirus B, cytomegalovirus, adenovirus, and mumps have been implicated in inducing certain cases of the disease.
Uncommon forms of immune-mediated diabetes.In this category, there are two known conditions, and others are likely to occur. The stiff-man syndrome is an autoimmune disorder of the central nervous system characterized by stiffness of the axial muscles with painful spasms. Patients usually have high titers of the GAD autoantibodies, and approximately one-third will develop diabetes.
Anti-insulin receptor antibodies can cause diabetes by binding to the insulin receptor, thereby blocking the binding of insulin to its receptor in target tissues. However, in some cases, these

antibodies can act as an insulin agonist after binding to the receptor and can thereby cause hypoglycemia. Anti-insulin receptor antibodies are occasionally found in patients with systemic lupus erythematosus and other autoimmune diseases. As in other states of extreme insulin resistance, patients with anti-insulin receptor antibodies often have acanthosis nigricans. In the past, this syndrome was termed type B insulin resistance.
Other genetic syndromes sometimes associated with diabetes.Many genetic syndromes are accompanied by an increased incidence of diabetes mellitus. These include the chromosomal abnormalities of Down’s syndrome, Klinefelter’s syndrome, and Turner’s syndrome. Wolfram’s syndrome is an autosomal recessive disorder characterized by insulin-deficient diabetes and the absence of β-cells at autopsy. Additional manifestations include diabetes insipidus, hypogonadism, optic atrophy, and neural deafness. Other syndromes are listed in Table 1.
Gestational diabetes mellitus (GDM)GDM is defined as any degree of glucose intolerance with onset or first recognition during pregnancy. The definition applies regardless of whether insulin or only diet modification is used for treatment or whether the condition persists after pregnancy. It does not exclude the possibility that unrecognized glucose intolerance may have antedated or begun concomitantly with the pregnancy. GDM complicates ∼4% of all pregnancies in the U.S., resulting in ∼135,000 cases annually. The prevalence may range from 1 to 14% of pregnancies, depending on the population studied. GDM represents nearly 90% of all pregnancies complicated by diabetes.
Deterioration of glucose tolerance occurs normally during pregnancy, particularly in the 3rd trimester.
Impaired glucose tolerance (IGT) and impaired fasting glucose (IFG)The Expert Committee (1,2) recognized an intermediate group of subjects whose glucose levels, although not meeting criteria for diabetes, are nevertheless too high to be considered normal. This group is defined as having fasting plasma glucose (FPG) levels ≥100 mg/dl (5.6 mmol/l) but <126 mg/dl (7.0 mmol/l) or 2-h values in the oral glucose tolerance test (OGTT) of ≥140 mg/dl (7.8 mmol/l) but <200 mg/dl (11.1 mmol/l). Thus, the categories of FPG values are as follows:
FPG <100 mg/dl (5.6 mmol/l) = normal fasting glucose;
FPG 100–125 mg/dl (5.6–6.9 mmol/l) = IFG (impaired fasting glucose);
FPG ≥126 mg/dl (7.0 mmol/l) = provisional diagnosis of diabetes (the diagnosis must be confirmed, as described below).
The corresponding categories when the OGTT is used are the following:
2-h postload glucose <140 mg/dl (7.8 mmol/l) = normal glucose tolerance;
2-h postload glucose 140–199 mg/dl (7.8–11.1 mmol/l) = IGT (impaired glucose tolerance);
2-h postload glucose ≥200 mg/dl (11.1 mmol/l) = provisional diagnosis of diabetes (the diagnosis must be confirmed, as described below).
Patients with IFG and/or IGT are now referred to as having “pre-diabetes” indicating the relatively high risk for development of diabetes in these patients. In the absence of pregnancy, IFG and IGT are not clinical entities in their own right but rather risk factors for future diabetes as well as cardiovascular disease. They can be observed as intermediate stages in any of the disease processes listed in Table 1. IFG and IGT are associated with the metabolic syndrome, which includes obesity (especially abdominal or visceral obesity), dyslipidemia of the high-triglyceride and/or low-HDL type, and hypertension. It is worth mentioning that medical nutrition therapy aimed at producing 5–10% loss of body weight, exercise, and certain pharmacological agents have been variably demonstrated to prevent or delay the development of diabetes in people with IGT; the potential impact of such interventions to reduce cardiovascular risk has not been examined to date.
Note that many individuals with IGT are euglycemic in their daily lives. Individuals with IFG or IGT may have normal or near normal glycated hemoglobin levels. Individuals with IGT often manifest hyperglycemia only when challenged with the oral glucose load used in the standardized OGTT.

Previous SectionNext Section
DIAGNOSTIC CRITERIA FOR DIABETES MELLITUSThe criteria for the diagnosis of diabetes are shown in Table 2. Three ways to diagnose diabetes are possible, and each, in the absence of unequivocal hyperglycemia, must be confirmed, on a subsequent day, by any one of the three methods given in Table 2. The use of the hemoglobin A1c (A1C) for the diagnosis of diabetes is not recommended at this time.
Diagnosis of GDMThe criteria for abnormal glucose tolerance in pregnancy are those of Carpenter and Coustan (3). Recommendations from the American Diabetes Association’s Fourth International Workshop-Conference on Gestational Diabetes Mellitus held in March 1997 support the use of the Carpenter/Coustan diagnostic criteria as well as the alternative use of a diagnostic 75-g 2-h OGTT. These criteria are summarized below.
Testing for gestational diabetes.Previous recommendations included screening for GDM performed in all pregnancies. However, there are certain factors that place women at lower risk for the development of glucose intolerance during pregnancy, and it is likely not cost-effective to screen such patients. Pregnant women who fulfill all of these criteria need not be screened for GDM.
This low-risk group comprises women who
are <25 years of age
are a normal body weight
have no family history (i.e., first-degree relative) of diabetes
have no history of abnormal glucose metabolism
have no history of poor obstetric outcome
are not members of an ethnic/racial group with a high prevalence of diabetes (e.g., Hispanic American, Native American, Asian American, African American, Pacific Islander)
Risk assessment for GDM should be undertaken at the first prenatal visit. Women with clinical characteristics consistent with a high risk of GDM (marked obesity, personal history of GDM, glycosuria, or a strong family history of diabetes) should undergo glucose testing (see below) as soon as feasible. If they are found not to have GDM at that initial screening, they should be retested between 24 and 28 weeks of gestation. Women of average risk should have testing undertaken at 24–28 weeks of gestation.
A fasting plasma glucose level >126 mg/dl (7.0 mmol/l) or a casual plasma glucose >200 mg/dl (11.1 mmol/l) meets the threshold for the diagnosis of diabetes. In the absence of unequivocal hyperglycemia, the diagnosis must be confirmed on a subsequent day. Confirmation of the diagnosis precludes the need for any glucose challenge. In the absence of this degree of hyperglycemia, evaluation for GDM in women with average or high-risk characteristics should follow one of two approaches.
One-step approach.Perform a diagnostic OGTT without prior plasma or serum glucose screening. The one-step approach may be cost-effective in high-risk patients or populations (e.g., some Native-American groups).
Two-step approach.Perform an initial screening by measuring the plasma or serum glucose concentration 1 h after a 50-g oral glucose load (glucose challenge test [GCT]) and perform a diagnostic OGTT on that subset of women exceeding the glucose threshold value on the GCT. When the two-step approach is used, a glucose threshold value >140 mg/dl (7.8 mmol/l) identifies ∼80% of women with GDM, and the yield is further increased to 90% by using a cutoff of >130 mg/dl (7.2 mmol/l).
With either approach, the diagnosis of GDM is based on an OGTT. Diagnostic criteria for the 100-g OGTT are derived from the original work of O’Sullivan and Mahan (4) modified by Carpenter and Coustan (3) and are shown in the top of Table 3. Alternatively, the diagnosis can be made using a

75-g glucose load and the glucose threshold values listed for fasting, 1 h, and 2 h (Table 2, bottom); however, this test is not as well validated as the 100-g OGTT.
Previous SectionNext Section
View larger version:
In this page In a new window
Figure 1—
Disorders of glycemia: etiologic types and stages. ∗Even after presenting in ketoacidosis, these patients can briefly return to normoglycemia without requiring continuous therapy (i.e., “honeymoon” remission); ∗∗in rare instances, patients in these categories (e.g., Vacor toxicity, type 1 diabetes presenting in pregnancy) may require insulin for survival.
View this table:
In this window In a new window
Table 1—
Etiologic classification of diabetes mellitusView this table:
In this window In a new window
Table 2—
Criteria for the diagnosis of diabetes mellitusView this table:
In this window In a new window
Table 3—
Diagnosis of GDM with a 100-g or 75-g glucose load
Previous SectionNext Section
Footnotes The information that follows is based largely on the reports of the Expert
Committee on the Diagnosis and Classification of Diabetes (Diabetes Care 20:1183–1197, 1997, and Diabetes Care 26:3160–3167, 2003).
DIABETES CARE
Previous Section
References1. ↵

The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus: Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 20: 1183–1197, 1997Medline Web of Science
2. ↵ The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus: Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 26: 3160–3167, 2003FREE Full Text
3. ↵ Carpenter MW, Coustan DR: Criteria for screening tests for gestational diabetes. Am J Obstet Gynecol 144: 768–773, 1982Medline Web of Science
4. ↵ O’Sullivan JB, Mahan CM: Criteria for the oral glucose tolerance test in pregnancy. Diabetes 13: 278, 1964
erican Study of Kidney Disease aDiffering effects of antihypertensive drugs on the incidence of diabetes mellitus among patients with hypertensive kidney disease. Archives of Internal Medicine April 10, 2006 166:797-805
What are the different types of diabetes?
There are three main types of diabetes that have been categorized by medical scientists.
The first type is called Type I Diabetes. Formerly known as juvenile diabetes, this type begins to make its appearance in pre-adolescence or adolescent growth. It is an insulin dependent autoimmune disease in which the body destroys its own beta cells. It accounts for 10% of all diabetes types.
The second type is called Type II Diabetes. This disease generally appears after 40 years of age. It is most likely triggered by poor diet and lack of exercise. Because of poor diets and the availability of fast food, Type II diabetes is now showing up in teenagers. It is non-insulin dependent, meaning insulin is used to control blood sugar levels but is not crucial to maintaining life.
Gestational Diabetes is the third type of diabetes. Occurring during a woman’s pregnancy, the mother has difficulty digesting carbohydrates. Gynecologists usually perform this test on all pregnant women early in the first trimester.
There is also a condition called Pre-Diabetes. This condition is defined as someone who has elevated blood sugar levels, but does not fall into a clearly defined category.
Syndrome X, Polycystic Ovary Disease, Hemocromatosis and Cystic Fibrosis are additional types of insulin resistant diabetes.
As a Type I diabetic ages, the symptomatic lines begin to blur into Type II. A person can also be typed as Type 1.5, Type 2-s or Type 2-d.
It is very important that factors such as ketones, antibodies, high triglyceride and low HDL, uric acid, and C-peptide be taken into account for your diagnosis.
Incorrectly categorizing diabetes is very common. Conditions that worsen or don’t show improvement should be brought to the attention of a diabetic specialist.

As aging blurs the lines of the types of diabetes, it is very important to review your symptoms often.
Learn More About Controlling Diabetes!
Like this information? Help us by sharing it with others using the social media buttons below.
Managing Diabetes – Understanding the IssueIs managing diabetes possible? The attitudes towards diabetes may range from indifference to extreme fear and agitation. Therefore, a clear understanding of the disease will help promote a proactive attitude towards its management. Simply put, diabetes is a condition in which the amount of glucose in the blood is too high because the body cannot handle it properly. This condition results from the inability of the pancreas to produce sufficient amounts of insulin. Insulin is the hormone that enables the body to properly use glucose and directing it to the cells where it is used for fuel. Glucose comes from carbohydrate digestion. In order to successfully manage diabetes, a means must be found to assist the body in properly digesting and metabolizing glucose.
Managing Diabetes – Practical StepsThere are several ways to manage diabetes. However, every program of diabetes management will require a change of mindset and lifestyle.
The first step in managing diabetes is to commit yourself to the care of a health professional. The healthcare professional will determine the severity of the patient’s diabetes and decide if insulin injections are required. In some less severe cases, pills may be given to aid in the body’s use of glucose. One of the aims of the health professional is to instruct the patient about controlling blood glucose levels. Insulin injections or pills taken at prescribed times achieve this goal.
Beyond medical intervention, the most important method of managing diabetes is a change in lifestyle. This change will include careful attention to diet and increased physical activity. Since diabetes is a condition where the blood glucose levels are too high, dietary plans to manage diabetes will include maintaining consistent levels of blood glucose throughout the day. A certified dietician can help determine what levels are optimal for each individual. These levels will be determined by many physical factors, including sex, age, occupation, and other health conditions. It is important to note (and take heart) that modifying diet to manage diabetes does not mean that any one food must be eliminated from your diet.
The key to proper diet is balance and the healthy diabetic diet is simply a healthy diet, one that all individuals should adopt. Proper dietary management of diabetes includes eating regular meals based on wholegrain varieties of breads, cereals and pasta. At least five portions of fruits and vegetables should be eaten on a daily basis. Fruit intake should be spread out during the day to maintain optimal blood glucose levels. A good diet will also have lower salt and fat intake. Sugary foods should be cut to a minimum. If rich desserts are eaten, intake of other fats and carbohydrates need to be drastically reduced.
Another factor in diabetic management is maintaining a safe weight. Most individuals with type 2 diabetes, the type of diabetes that occurs when the body doesn’t produce enough insulin or the insulin produced does not work properly, are overweight. Losing weight will not only help control diabetes but lower the risk of other health problems such as cardiovascular diseases.
Successful diabetic management will require increased physical activity. Walking is a natural exercise that most people can do. Whenever possible, walk instead of ride, and take stairs instead of elevators and escalators. Increased physical activity goes beyond regulating blood sugar levels, it also benefits the heart, lungs, and joints and gives a sense of well being.

No one needs to succumb to the long-term negative side effects of diabetes. One needs to submit to the regular care of a health professional and take prescribed medication. Adopting a new lifestyle and mindset is a vital key to success. Eating wisely, watching your weight and increasing physical activity bring diabetes management into the realm of the possibility. These lifestyle changes make for all around good health.
Managing Diabetes – Understanding the IssueIs managing diabetes possible? The attitudes towards diabetes may range from indifference to extreme fear and agitation. Therefore, a clear understanding of the disease will help promote a proactive attitude towards its management. Simply put, diabetes is a condition in which the amount of glucose in the blood is too high because the body cannot handle it properly. This condition results from the inability of the pancreas to produce sufficient amounts of insulin. Insulin is the hormone that enables the body to properly use glucose and directing it to the cells where it is used for fuel. Glucose comes from carbohydrate digestion. In order to successfully manage diabetes, a means must be found to assist the body in properly digesting and metabolizing glucose.
Managing Diabetes – Practical StepsThere are several ways to manage diabetes. However, every program of diabetes management will require a change of mindset and lifestyle.
The first step in managing diabetes is to commit yourself to the care of a health professional. The healthcare professional will determine the severity of the patient’s diabetes and decide if insulin injections are required. In some less severe cases, pills may be given to aid in the body’s use of glucose. One of the aims of the health professional is to instruct the patient about controlling blood glucose levels. Insulin injections or pills taken at prescribed times achieve this goal.
Beyond medical intervention, the most important method of managing diabetes is a change in lifestyle. This change will include careful attention to diet and increased physical activity. Since diabetes is a condition where the blood glucose levels are too high, dietary plans to manage diabetes will include maintaining consistent levels of blood glucose throughout the day. A certified dietician can help determine what levels are optimal for each individual. These levels will be determined by many physical factors, including sex, age, occupation, and other health conditions. It is important to note (and take heart) that modifying diet to manage diabetes does not mean that any one food must be eliminated from your diet.
The key to proper diet is balance and the healthy diabetic diet is simply a healthy diet, one that all individuals should adopt. Proper dietary management of diabetes includes eating regular meals based on wholegrain varieties of breads, cereals and pasta. At least five portions of fruits and vegetables should be eaten on a daily basis. Fruit intake should be spread out during the day to maintain optimal blood glucose levels. A good diet will also have lower salt and fat intake. Sugary foods should be cut to a minimum. If rich desserts are eaten, intake of other fats and carbohydrates need to be drastically reduced.
Another factor in diabetic management is maintaining a safe weight. Most individuals with type 2 diabetes, the type of diabetes that occurs when the body doesn’t produce enough insulin or the insulin produced does not work properly, are overweight. Losing weight will not only help control diabetes but lower the risk of other health problems such as cardiovascular diseases.
Successful diabetic management will require increased physical activity. Walking is a natural exercise that most people can do. Whenever possible, walk instead of ride, and take stairs

instead of elevators and escalators. Increased physical activity goes beyond regulating blood sugar levels, it also benefits the heart, lungs, and joints and gives a sense of well being.
No one needs to succumb to the long-term negative side effects of diabetes. One needs to submit to the regular care of a health professional and take prescribed medication. Adopting a new lifestyle and mindset is a vital key to success. Eating wisely, watching your weight and increasing physical activity bring diabetes management into the realm of the possibility. These lifestyle changes make for all around good health.
Managing Diabetes – The Mental AspectsThe mental aspect of managing diabetes is often overlooked in published information. Diabetes can be emotionally difficult and may lead to depression. It is important to remember that you are not alone.
“I found help through a support groups. They provided me with instruction, comfort, and peace of mind. I also relied heavily on God to give me comfort. He did not choose to cure my physical illness but He helped me with the daily mental struggles. I found comfort in Matthew 11:28-30, ‘Come to me, all of you who are weary and carry heavy burdens, and I will give you rest. Take my yoke upon you. Let me teach you, because I am humble and gentle, and you will find rest for your souls.’ As diabetics, we can experience rest from the fears of what diabetes can do.
“If you have not experienced the peace of knowing God and would like to seek His comfort and security of eternal life, investigate what a life of knowing Jesus as your Savior and comforter can do for you. I know that in Him and I have found my rest.”
Cause of diabetes - What are the major causes?
Scientists are still working on the cause of diabetes. Since there are different types of diabetes, each type has a unique possible cause.
The main cause of diabetes is the body’s failure to produce enough of the insulin hormone. Another cause could be that the body develops a resistance to insulin.
Type I diabetes is caused by decreased insulin production. Type II is insulin resistant in peripheral tissues. In juvenile diabetes, the cause could be a lack of vitamin D.
There is also gestational diabetes that only occurs in pregnant women. These are only a few of the different types of diabetes.
It is suspected that there may be many contributors to diabetes. Genetics, environmental factors, obesity, lack of exercise, and high fat diets are just a few causes linked to diabetes. You cannot become a diabetic just because you eat a lot of sugars and candies, but if you are predisposed to the disease these factors may raise your risk of becoming a diabetic.
A sedentary lifestyle can also lead to diabetes, since the body cannot perform as well as someone in good physical condition.
Most scientists believe that you must be born predisposed to this disease. In other words, your body is

more susceptible because of the genetic make-up of your ancestors. If your parents, grandparents, or siblings have diabetes you are at greater risk. However, this is dependant upon the type of diabetes.
The cause of diabetes may seem to be elusive, but with the direction of science and how far we’ve come in the last 100 years, the answer could be right around the corner.
Is controlling diabetes possible?
Many people find controlling diabetes difficult because it is hard to change eating habits, find the time to exercise, or even to get the courage to use painful glucose meters. However, all of those things are necessary when it comes to successfully controlling diabetes.
Education: Controlling diabetes begins with knowing as much as you can about the disease. The more you know about diabetes, the more it will help you understand the need to take care of yourself. You need to learn about the medications you take and what they do and don’t do. You also need to learn about other complications that result from not keeping your diabetes in check. You need to learn as much as possible about how your life has changed and what to do about it.
Food: Controlling diabetes is all about good eating habits. The amount of carbohydrates a diabetic takes in can mean the difference between high and low blood sugar levels. So the first step to controlling diabetes is to keep a diary of your carbohydrate intake. A diary will allow you to see what foods you are eating and will allow you to make necessary adjustments.
Exercise: Controlling diabetes means making time for regular exercise. Exercise, added to a program of good eating habits, will help control diabetes and keep sugar levels under control. The more you exercise, the more sugar you will burn and the lower your blood sugar levels will be. The level and degree of your exercise should depend upon what your doctor recommends for you. However, most recommendations average out to about one-half hour to a full hour per day. Remember, exercise will also help to minimize the other complications of diabetes such as heart disease.
Sugar Levels: Controlling diabetes means you must regularly monitor your sugar levels. A useful tool to monitoring your blood sugar levels is the glucose meter. The glucose meter allows you to determine if your regiment of diet and exercise, in combination with your medication, is effectively lowering your blood sugar. It can also help you determine whether your doctor needs to be consulted.
A glucose meter should be used at the least once per day, and possibly more often, depending upon the severity of your diabetes. This enables you to detect any drastic or sudden changes in your blood sugar levels
You are here: Life Challenges >> Learn More About Controlling Diabetes! >> Signs Of Diabetes
What are the signs of diabetes?
Diabetes is a chronic disease in which the body does not produce enough insulin. Diabetes, when left

untreated, has been linked to other health problems such as heart disease and kidney failure. At the present time, diabetes is not a curable disease but it is a controllable disease provided you recognize the early warning signs of diabetes and then seek treatment immediately.
There is a long list of the warning signs of diabetes. The following are some of the ones I experienced when I was diagnosed with Type 2 diabetes. Once these symptoms were recognized, I went to see my family doctor who verified for me what I already suspected.
Rapid weight loss – Even though I ate the same types of food I began losing weight. Increased Hunger – After each meal I was still very hungry and would eat more. Thirsty – I could not drink enough water to satisfy my thirst. Frequent urination – It seemed like I was making frequent trips to the restroom. Tiredness – No matter how much sleep I received, I remained tired. Tingling in the Hands and feet – My hands and feet often felt like they were numb.
Additional signs of diabetes include blurry vision, sores that do not heal, and in extreme cases spells of unconsciousness. The warning signs of diabetes vary from person to person as well as from Type 1 to Type 2 diabetes.
Seeking helpThe best thing that you can do for yourself if you are experiencing any the signs of diabetes is to seek out the advice of your family physician. Your family physician can administer a blood test which can indicate what you sugar levels have been like over the last three months as well as how well your pancreas is working. From the blood test, your physician can find out if you truly have diabetes or not.
What are the different types of diabetes?
There are three main types of diabetes that have been categorized by medical scientists.
The first type is called Type I Diabetes. Formerly known as juvenile diabetes, this type begins to make its appearance in pre-adolescence or adolescent growth. It is an insulin dependent autoimmune disease in which the body destroys its own beta cells. It accounts for 10% of all diabetes types.
The second type is called Type II Diabetes. This disease generally appears after 40 years of age. It is most likely triggered by poor diet and lack of exercise. Because of poor diets and the availability of fast food, Type II diabetes is now showing up in teenagers. It is non-insulin dependent, meaning insulin is used to control blood sugar levels but is not crucial to maintaining life.
Gestational Diabetes is the third type of diabetes. Occurring during a woman’s pregnancy, the mother has difficulty digesting carbohydrates. Gynecologists usually perform this test on all pregnant women early in the first trimester.
There is also a condition called Pre-Diabetes. This condition is defined as someone who has elevated blood sugar levels, but does not fall into a clearly defined category.
Syndrome X, Polycystic Ovary Disease, Hemocromatosis and Cystic Fibrosis are additional types of insulin resistant diabetes.

As a Type I diabetic ages, the symptomatic lines begin to blur into Type II. A person can also be typed as Type 1.5, Type 2-s or Type 2-d.
It is very important that factors such as ketones, antibodies, high triglyceride and low HDL, uric acid, and C-peptide be taken into account for your diagnosis.
Incorrectly categorizing diabetes is very common. Conditions that worsen or don’t show improvement should be brought to the attention of a diabetic specialist.
As aging blurs the lines of the types of diabetes, it is very important to review your symptoms often.
Sulfonylureas (as Glipizide/Glucotrol, Glyburide/Micronase) Thiazolidinediones (Pioglitazone/Actos, Rosiglitazone/Avandia) a-Glucosidase inhibitors (Acarbose/Precose, Miglitol/Glyset) DPP IV Inhibitors (Vildagliptin/Galvus, Sitagliptin/Januvia PO) Biguanides (Metformin/Glucophage) Meglitinide (Prandin/Repaglinide, Starlix/Nataglinide)
Injectable medications: GLP Analogues (Exenatide/Byetta, Pramlintide/Symlin Subc) Insulin, etc Rx , New Inhaled Insulin (Exubera)
Sulfonylureas: first choice for normal weight; hypoglycemia with monotherapy - stimulate insulin secretion in response to glucose. Watch for weight gain.
Glipizide (Glucotrol) Dose: lowest effective single dose, 5mg, Usually dose 5-10 mg 1-2 tab BID (Max 40 mg/day)
Glipizide (GI therapeutic system) Glucotrol XL 5-10mg tab once/day (Max 20 mg/day)Dose: lowest effective single dose, 5 mg; daily max, 20 mg
Glyburide (Micronase, Diabeta) - (2nd generation) Dose: lowest effective single dose, 1.25 mg; Usually dose 1.25-2.5-5 mg 1-2 tab BID (Max 20 mg/day)
Micronized glyburide (Glynase)Dose: lowest effective single dose, 1.5 mg; daily max, 6 mg
Glimepiride (Amaryl) (3rd generation) Dose: lowest effective single dose, 0.5 mg; 1,2,4 mg tab/day. Start 1-2 mg/d, usual maintenance dose is 1-4mg once/d (Max: 8mg/d)
Gliclazide/ Diamicron 80-160 mg daily, max 320 mg PO daily.Modified release Diamicron MR 30 mg PO daily, mas 120 mg daily
Combination meds:Glucovance (Glyburide and Metformin)

Avandaryl (Glimepiride and Avandia/Rosiglitazone)
Diabenese/Chlorpropamide (1st generation) 100-250 mg 1-3 tab/d; 100-250 mg tab
Orinase /Tolbutamide (1st generation) 250-500 mg tab 1-3x/d
Tolinase/Tolazamide (1st generation) 100-500 mg tab -2x/d; 100-250-500 mg tab.
Dymelor/Acetohexamide 500-750 mg once or divided.
Sulfonylureas (as Glipizide/Glucotrol, Glyburide/Micronase) | Biguanides (Metformin/Glucophage) Thiazolidinediones (Pioglitazone/Actos, Rosiglitazone/Avandia) | Meglitinide (Prandin/Repaglinide, Starlix/Nataglinide) a-Glucosidase inhibitors (Acarbose/Precose, Miglitol/Glyset) | GLP Analogues (Exenatide/Byetta, Pramlintide/Symlin Subc) DPP IV Inhibitors (Vildagliptin/Galvus, Sitagliptin/Januvia PO) | Insulin, etc Rx , New Inhaled Insulin (Exubera)
Biguanides - Primary action is reduction of excessive hepatic glucose output; it also has some activity on insulin resistance in skeleton muscle, though less than troglitazone. - Metformin may cause life-threatening lactic acidosis. - Takes about 2 wks to work well. Do not use in renal or hepatic dysfunction, dehydrated, or hospital patients. - Hold this med prior to IV contrast agents and for for 48 hours after. - Avoid if ethanol abuse, heart failure, hepatic or renal insufficiency (Cr >1.4-1.5), or hypoxic states.
Metformin: first choice for obese Dose: 500 - 850 mg tab 2-3x/day or 1000 mg bid with meals. (MAX 2550 mg/day)
Glumetza/ Extended Metformin 500-1,000 mg dosage strength Glucovance (Glyburide and Metformin) Avandamet (Avandia/Rosiglitazone and Metformin) Janumet (Januvia/Sitagliptin and Metformin)
Sulfonylureas (as Glipizide/Glucotrol, Glyburide/Micronase) Thiazolidinediones (Pioglitazone/Actos, Rosiglitazone/Avandia)

a-Glucosidase inhibitors (Acarbose/Precose, Miglitol/Glyset) DPP IV Inhibitors (Vildagliptin/Galvus, Sitagliptin/Januvia PO) Biguanides (Metformin/Glucophage) Meglitinide (Prandin/Repaglinide, Starlix/Nataglinide)
Injectable medications: GLP Analogues (Exenatide/Byetta, Pramlintide/Symlin Subc) Insulin, etc Rx , New Inhaled Insulin (Exubera)
Sulfonylureas: first choice for normal weight; hypoglycemia with monotherapy - stimulate insulin secretion in response to glucose. Watch for weight gain.
Glipizide (Glucotrol) Dose: lowest effective single dose, 5mg, Usually dose 5-10 mg 1-2 tab BID (Max 40 mg/day)
Glipizide (GI therapeutic system) Glucotrol XL 5-10mg tab once/day (Max 20 mg/day)Dose: lowest effective single dose, 5 mg; daily max, 20 mg
Glyburide (Micronase, Diabeta) - (2nd generation) Dose: lowest effective single dose, 1.25 mg; Usually dose 1.25-2.5-5 mg 1-2 tab BID (Max 20 mg/day)
Micronized glyburide (Glynase)Dose: lowest effective single dose, 1.5 mg; daily max, 6 mg
Glimepiride (Amaryl) (3rd generation) Dose: lowest effective single dose, 0.5 mg; 1,2,4 mg tab/day. Start 1-2 mg/d, usual maintenance dose is 1-4mg once/d (Max: 8mg/d)
Gliclazide/ Diamicron 80-160 mg daily, max 320 mg PO daily.Modified release Diamicron MR 30 mg PO daily, mas 120 mg daily
Combination meds:Glucovance (Glyburide and Metformin) Avandaryl (Glimepiride and Avandia/Rosiglitazone)
Diabenese/Chlorpropamide (1st generation) 100-250 mg 1-3 tab/d; 100-250 mg tab
Orinase /Tolbutamide (1st generation) 250-500 mg tab 1-3x/d
Tolinase/Tolazamide (1st generation) 100-500 mg tab -2x/d; 100-250-500 mg tab.
Dymelor/Acetohexamide 500-750 mg once or divided.
Sulfonylureas (as Glipizide/Glucotrol, Glyburide/Micronase) | Biguanides (Metformin/Glucophage) Thiazolidinediones (Pioglitazone/Actos, Rosiglitazone/Avandia) | Meglitinide (Prandin/Repaglinide, Starlix/Nataglinide) a-Glucosidase inhibitors (Acarbose/Precose, Miglitol/Glyset) | GLP Analogues (Exenatide/Byetta, Pramlintide/Symlin Subc)

DPP IV Inhibitors (Vildagliptin/Galvus, Sitagliptin/Januvia PO) | Insulin, etc Rx , New Inhaled Insulin (Exubera)
Biguanides - Primary action is reduction of excessive hepatic glucose output; it also has some activity on insulin resistance in skeleton muscle, though less than troglitazone. - Metformin may cause life-threatening lactic acidosis. - Takes about 2 wks to work well. Do not use in renal or hepatic dysfunction, dehydrated, or hospital patients. - Hold this med prior to IV contrast agents and for for 48 hours after. - Avoid if ethanol abuse, heart failure, hepatic or renal insufficiency (Cr >1.4-1.5), or hypoxic states.
Metformin: first choice for obese Dose: 500 - 850 mg tab 2-3x/day or 1000 mg bid with meals. (MAX 2550 mg/day)
Glumetza/ Extended Metformin 500-1,000 mg dosage strength Glucovance (Glyburide and Metformin) Avandamet (Avandia/Rosiglitazone and Metformin) Janumet (Januvia/Sitagliptin and Metformin)
Definition of Diabetes mellitus
Type 2 Diabetes Slideshow
Quiz: Are You At Risk for Diabetic Nerve Pain?
Diabetes and Foot Problems Slideshow
Diabetes mellitus: Better known just as "diabetes" -- a chronic disease associated with abnormally high levels of the sugar glucose in the blood. Diabetes is due to one of two
mechanisms:(1) Inadequate production of insulin (which is made by the pancreas and lowers blood glucose)
or(2) Inadequate sensitivity of cells to the action of insulin.
The two main types of diabetes correspond to these two mechanisms and are called insulin dependent (type 1) and non-insulin dependent (type 2) diabetes. In type 1 diabetes there is no

insulin or not enough of it. In type 2 diabetes, there is generally enough insulin but the cells upon it should act are not normally sensitive to its action.
The signs and symptoms of both types of diabetes include increased urine output and decreased appetite as well as fatigue. Diabetes is diagnosed by blood glucose testing, the glucose tolerance test, and testing of the level of glycosylated hemoglobin (glycohemoglobin or hemoglobin A1C).
The mode of treatment depends on the type of the diabetes.
The major complications of diabetes include dangerously elevated blood sugar, abnormally low blood sugar due to diabetes medications, and disease of the blood vessels which can damage the
eye, kidneys, nerves, and heart.Last Editorial Review: 1/6/2001
Common Misspellings: diabetes mallitus, diabeties mellitus, diabeties mallitus, diabettes mellitus, diabettes mallitus, diabetis mellitus, diabetis mallitus
Diabetes mellitus is a common metabolic disorder resulting from defects
in insulin action, insulin production, or both. Insulin, a hormone secreted
by the pancreas, helps the body use and store glucose produced during the
digestion of food. Characterized by hyperglycemia , symptoms of diabetes
include frequent urination, increased thirst, dehydration , weight loss,
blurred vision, fatigue , and, occasionally, coma. Uncontrolled
hyperglycemia over time damages the eyes, nerves, blood vessels, kidneys,
and heart, causing organ dysfunction and failure. A number of risk factors
are attributed to the incidence of diabetes, including family history, age,
ethnicity, and social group characteristics, as well as behavioral ,
lifestyle, psychological , and clinical factors.
The World Health Organization estimates that 150 million people had
diabetes worldwide in 2002. This number is projected to double by the year
2025. Much of this increase will occur in developing countries and will be
due to population growth, aging, unhealthful diets, obesity , and sedentary
lifestyles. In the United States, diabetes is the sixth leading cause of death.
While 6.2 percent of the population has diabetes, an estimated 5.9 million
people are unaware they have the disease. In addition, about 19 percent of

all deaths in the United States for those age twenty-five and older are due
to diabetes-related complications.
The prevalence of diabetes varies by age, gender, race, and ethnicity. In
the United States, about 0.19 percent of the population less than twenty
years of age (151,000 people) have diabetes, versus 8.6 percent of the
population twenty years of age and older. In addition, adults sixty-five and
older account for 40 percent of those with diabetes, despite composing only
12 percent of the population. Considerable variations also exist in the
prevalence of diabetes among various racial and ethnic groups. For
example, 7.8 percent of non-Hispanic whites, 13 percent of non-Hispanic
blacks, 10.2 percent of Hispanic/Latino Americans, and 15.1 percent of
American Indians and Alaskan Natives have diabetes. Among Asian
Americans and Pacific
The standard method of measuring blood glucose level is called a fingerstick,
which is a small blood sample taken from the fingertip. Diabetics must monitor
their blood glucose levels daily in order to avoid dire complications such as kidney
disease, blindness, stroke, and poor blood circulation.
[Photograph by Tom Stewart. Corbis. Reproduced by permission.]
Islanders, the rate of diabetes varies substantially and is estimated at 15 to 20
percent. The prevalence of diabetes is comparable for males and females—8.3 and

8.9 percent respectively. Nevertheless, the disease is more devastating and more
difficult to control among women, especially African-American and non-Hispanic
white women. In fact, the risk for death is greater among young people (3.6 times
greater for people from 25 to 44 years of age) and women (2.7 times greater for
women ages 45 to 64 than men of the same age).
Types of Diabetes
Diabetes mellitus is classified into four categories: type 1, type 2,
gestational diabetes, and other. In type 1 diabetes, specialized cells in the
pancreas are destroyed, leading to a deficiency in insulin production. Type 1
diabetes frequently develops over the course of a few days or weeks. Over
95 percent of people with type 1 diabetes are diagnosed before the age of
twenty-five. Estimates show 5.3 million people worldwide live with type 1
diabetes. Although the diagnosis of type 1 diabetes occurs equally among
men and women, an increased prevalence exists in the white population.
Type 1 diabetes in Asian children is relatively rare.
Family history, diet , and environmental factors are risk factors for type 1
diabetes. Studies have found an increased risk in children whose parents
have type 1 diabetes, and this risk increases with maternal age.
Environmental factors such as viral infections, toxins , and exposure to
cow's milk are being contested as causing or modifying the development of
type 1 diabetes.
Type 2 diabetes is characterized by insulin resistance and/or decreased
insulin secretion. It is the most common form of diabetes mellitus,
accounting for 90 to 95 percent of all diabetes cases worldwide. Risk factors
for type 2 diabetes include family history, increasing age, obesity, physical
inactivity, ethnicity, and a history of gestational diabetes. Although type 2

Type 1 diabetics are more likely than other diabetics to require insulin injections to
regulate blood glucose levels. Insulin pumps like the one shown here can provide
an extra measure of control by administering a very accurate dose of insulin on a
set schedule.
[Photograph by Paul Sakuma. AP/Wide World Photos. Reproduced by permission.]
diabetes is frequently diagnosed in adult populations, an increasing number of
children and adolescents are currently being diagnosed. Type 2 diabetes is also
more common in blacks, Hispanics, Native Americans, and women, especially
women with a history of gestational diabetes.
Genetics and environmental factors are the main contributors to type 2
diabetes. Physical inactivity and adoption of a Western lifestyle (particularly
choosing foods with more animal protein , animal fats, and processed
carbohydrates ), especially in indigenous people in North American and
within ethnic groups and migrants, have contributed to weight gain and
obesity. In fact, obesity levels increased by 74 percent between 1991 and
2003. Increased body fat and abdominal obesity are associated with insulin
resistance, a precursor to diabetes. Impaired glucose tolerance (IGT) and
impaired fasting glucose (IFG) are two prediabetic conditions associated
with insulin resistance. In these conditions, the blood glucose concentration
is above the normal range, but below levels required to diagnose diabetes.
Subjects with IGT and/or IFG are at substantially higher risk of developing
diabetes and cardiovascular disease than those with normal glucose
tolerance. The conversion of individuals with IGT to type 2 diabetes varies
with ethnicity, anthropometric measures related to obesity, fasting blood
glucose (a measurement of blood glucose values after not eating for 12 to
14 hours), and the two-hour post-glucose load level (a measurement of

blood glucose taken exactly two hours after eating). In addition to IGT and
IFG, higher than normal levels of fasting insulin, called hyperinsulinemia,
are associated with an increased risk of developing type 2 diabetes. Insulin
levels are higher in African Americans than in whites, particularly African-
American women, indicating their greater predisposition for developing
type 2 diabetes.
The complexity of inheritance and interaction with the environment makes
identification of genes involved with type 2 diabetes difficult. Only a small
percentage (2–5%) of diabetes cases can be explained by single gene
defects and are usually atypical cases. However, a "thrifty gene," although
not yet identified, is considered predictive of weight gain and the
development of type 2 diabetes. Thrifty-gene theory suggests that
indigenous people who experienced alternating periods of feast and famine
gradually developed a way to store fat more efficiently during periods of
plenty to better survive famines. Regardless of the thrifty gene, the
contribution of genetic mutations in the development of type 2 diabetes has
not been established, due to the number of genes that may be involved.
Gestational diabetes mellitus (GDM) is defined as any degree of glucose
intolerance with onset or first recognition during pregnancy. This definition
applies regardless of whether insulin or diet modification is used for
treatment, and whether or not the condition persists after pregnancy. GDM
affects up to 14 percent of the pregnant population—approximately 135,000
women per year in United States. GDM complicates about 4 percent of all
pregnancies in the U.S. Women at greatest risk for developing GDM are
obese , older than twenty-five years of age, have a previous history of
abnormal glucose control, have first-degree relatives with diabetes, or are
members of ethnic groups with a high prevalence of diabetes. Infants of a
woman with GDM are at a higher risk of developing obesity, impaired
glucose tolerance, or diabetes at an early age. After a pregnancy with GDM,
the mother has an increased risk of developing type 2 diabetes.

Other forms of diabetes are associated with genetic defects in the
specialized cells of the pancreas, drug or chemical use, infections, or other
diseases. The most notable of the genetically linked diabetes is maturity
onset diabetes of the young (MODY). Characterized by the onset of
hyperglycemia before the age of twenty-five, insulin secretion is impaired
while minimal or no defects exist in insulin action. Drugs , infections, and
diseases cause diabetes by damaging the pancreas and/or impairing insulin
action or secretion.
Diabetes Complications
People with diabetes are at increased risk for serious long-term
complications. Hyperglycemia, as measured by fasting plasma glucose
concentration or glycosylated hemoglobin (HbA1c), causes structural and
functional changes in the retina, nerves, kidneys, and blood vessels. This
damage can lead to blindness, numbness, reduced circulation, amputations,
kidney disease, and cardiovascular disease. Type 1 diabetes is more likely to
lead to kidney failure. About 40 percent of people with type 1 diabetes
develop severe kidney disease and kidney failure by the age of fifty.
Nevertheless, between 1993 and 1997, more than 100,000 people in the
United States were treated for kidney failure caused by type 2 diabetes.
African Americans experience higher rates of diabetes-related
complications such as eye disease, kidney failure, and amputations. They
also experience greater disability from these complications. The frequency
of diabetic retinopathy (disease of the small blood vessels in the retina
causing deterioration of eyesight) is 40 to 50 percent higher in African
Americans than in white Americans. In addition, the rate of diabetic
retinopathy among Mexican Americans is more than twice that of non-
Hispanic white Americans. Furthermore, African Americans with diabetes
are much more likely to undergo a lower-extremity amputation than white
or Hispanic Americans with diabetes. Little is known about these
complications in Asian and Pacific Islander-Americans.

Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemia state (HHS)
are serious diabetic emergencies and the most frequent cause of mortality.
Both DKA and HHS result from an insulin deficiency and an increase in
counter-regulatory hormones (a.k.a. hyperglycemia). Hyperglycemia leads
to glycosuria (glucose in the urine), increased urine output, and
dehydration. Because the glucose is excreted in the urine, the body
becomes starved for energy . At this point, the body either continues to
excrete glucose in the urine making the hyperglycemia worse (HHS), or the
body begins to break down triglycerides causing the release of ketones
(by-products of fat breakdown) into the urine and bloodstream (DKA). The
mortality rate of patients with DKA is less than 5 percent while the
mortality rate of HHS patients is about 15 percent. Infection (urinary tract
infections and pneumonia account for 30 to 50 percent of cases), omission
of insulin, and increased amounts of counter-regulatory hormones
contribute to DKA and HHS. Type 1 and type 2 diabetic patients may
experience DKA and HHS. However, DKA is more common in type 1
diabetic patients, while HHS is more common in type 2 diabetic patients.
Treatment of DKA and HHS involves correction of dehydration,
hyperglycemia, ketoacidosis, and electrolyte deficits and imbalances.
Treatment for Diabetes
Treatment for diabetes involves following a regimen of diet, exercise, self-
monitoring of blood glucose, and taking medication or insulin injections.
Although type 1 diabetes is primarily managed with daily insulin injections,
type 2 diabetes can be controlled with diet and exercise. However, when
diet and exercise fail, medication is added to stimulate the production of
insulin, reduce insulin resistance, decrease the liver

Diabetes mellitus is a common metabolic disorder resulting from defects
in insulin action, insulin production, or both. Insulin, a hormone secreted
by the pancreas, helps the body use and store glucose produced during the
digestion of food. Characterized by hyperglycemia , symptoms of diabetes
include frequent urination, increased thirst, dehydration , weight loss,
blurred vision, fatigue , and, occasionally, coma. Uncontrolled
hyperglycemia over time damages the eyes, nerves, blood vessels, kidneys,
and heart, causing organ dysfunction and failure. A number of risk factors
are attributed to the incidence of diabetes, including family history, age,
ethnicity, and social group characteristics, as well as behavioral ,
lifestyle, psychological , and clinical factors.
The World Health Organization estimates that 150 million people had
diabetes worldwide in 2002. This number is projected to double by the year
2025. Much of this increase will occur in developing countries and will be
due to population growth, aging, unhealthful diets, obesity , and sedentary
lifestyles. In the United States, diabetes is the sixth leading cause of death.
While 6.2 percent of the population has diabetes, an estimated 5.9 million
people are unaware they have the disease. In addition, about 19 percent of
all deaths in the United States for those age twenty-five and older are due
to diabetes-related complications.
The prevalence of diabetes varies by age, gender, race, and ethnicity. In
the United States, about 0.19 percent of the population less than twenty
years of age (151,000 people) have diabetes, versus 8.6 percent of the
population twenty years of age and older. In addition, adults sixty-five and
older account for 40 percent of those with diabetes, despite composing only
12 percent of the population. Considerable variations also exist in the
prevalence of diabetes among various racial and ethnic groups. For
example, 7.8 percent of non-Hispanic whites, 13 percent of non-Hispanic
blacks, 10.2 percent of Hispanic/Latino Americans, and 15.1 percent of
American Indians and Alaskan Natives have diabetes. Among Asian
Americans and Pacific

The standard method of measuring blood glucose level is called a fingerstick,
which is a small blood sample taken from the fingertip. Diabetics must monitor
their blood glucose levels daily in order to avoid dire complications such as kidney
disease, blindness, stroke, and poor blood circulation.
[Photograph by Tom Stewart. Corbis. Reproduced by permission.]
Islanders, the rate of diabetes varies substantially and is estimated at 15 to 20
percent. The prevalence of diabetes is comparable for males and females—8.3 and
8.9 percent respectively. Nevertheless, the disease is more devastating and more
difficult to control among women, especially African-American and non-Hispanic
white women. In fact, the risk for death is greater among young people (3.6 times
greater for people from 25 to 44 years of age) and women (2.7 times greater for
women ages 45 to 64 than men of the same age).
Types of Diabetes
Diabetes mellitus is classified into four categories: type 1, type 2,
gestational diabetes, and other. In type 1 diabetes, specialized cells in the
pancreas are destroyed, leading to a deficiency in insulin production. Type 1
diabetes frequently develops over the course of a few days or weeks. Over
95 percent of people with type 1 diabetes are diagnosed before the age of
twenty-five. Estimates show 5.3 million people worldwide live with type 1
diabetes. Although the diagnosis of type 1 diabetes occurs equally among

men and women, an increased prevalence exists in the white population.
Type 1 diabetes in Asian children is relatively rare.
Family history, diet , and environmental factors are risk factors for type 1
diabetes. Studies have found an increased risk in children whose parents
have type 1 diabetes, and this risk increases with maternal age.
Environmental factors such as viral infections, toxins , and exposure to
cow's milk are being contested as causing or modifying the development of
type 1 diabetes.
Type 2 diabetes is characterized by insulin resistance and/or decreased
insulin secretion. It is the most common form of diabetes mellitus,
accounting for 90 to 95 percent of all diabetes cases worldwide. Risk factors
for type 2 diabetes include family history, increasing age, obesity, physical
inactivity, ethnicity, and a history of gestational diabetes. Although type 2
Type 1 diabetics are more likely than other diabetics to require insulin injections to
regulate blood glucose levels. Insulin pumps like the one shown here can provide
an extra measure of control by administering a very accurate dose of insulin on a
set schedule.
[Photograph by Paul Sakuma. AP/Wide World Photos. Reproduced by permission.]
diabetes is frequently diagnosed in adult populations, an increasing number of
children and adolescents are currently being diagnosed. Type 2 diabetes is also
more common in blacks, Hispanics, Native Americans, and women, especially
women with a history of gestational diabetes.
Genetics and environmental factors are the main contributors to type 2
diabetes. Physical inactivity and adoption of a Western lifestyle (particularly

choosing foods with more animal protein , animal fats, and processed
carbohydrates ), especially in indigenous people in North American and
within ethnic groups and migrants, have contributed to weight gain and
obesity. In fact, obesity levels increased by 74 percent between 1991 and
2003. Increased body fat and abdominal obesity are associated with insulin
resistance, a precursor to diabetes. Impaired glucose tolerance (IGT) and
impaired fasting glucose (IFG) are two prediabetic conditions associated
with insulin resistance. In these conditions, the blood glucose concentration
is above the normal range, but below levels required to diagnose diabetes.
Subjects with IGT and/or IFG are at substantially higher risk of developing
diabetes and cardiovascular disease than those with normal glucose
tolerance. The conversion of individuals with IGT to type 2 diabetes varies
with ethnicity, anthropometric measures related to obesity, fasting blood
glucose (a measurement of blood glucose values after not eating for 12 to
14 hours), and the two-hour post-glucose load level (a measurement of
blood glucose taken exactly two hours after eating). In addition to IGT and
IFG, higher than normal levels of fasting insulin, called hyperinsulinemia,
are associated with an increased risk of developing type 2 diabetes. Insulin
levels are higher in African Americans than in whites, particularly African-
American women, indicating their greater predisposition for developing
type 2 diabetes.
The complexity of inheritance and interaction with the environment makes
identification of genes involved with type 2 diabetes difficult. Only a small
percentage (2–5%) of diabetes cases can be explained by single gene
defects and are usually atypical cases. However, a "thrifty gene," although
not yet identified, is considered predictive of weight gain and the
development of type 2 diabetes. Thrifty-gene theory suggests that
indigenous people who experienced alternating periods of feast and famine
gradually developed a way to store fat more efficiently during periods of
plenty to better survive famines. Regardless of the thrifty gene, the
contribution of genetic mutations in the development of type 2 diabetes has
not been established, due to the number of genes that may be involved.

Gestational diabetes mellitus (GDM) is defined as any degree of glucose
intolerance with onset or first recognition during pregnancy. This definition
applies regardless of whether insulin or diet modification is used for
treatment, and whether or not the condition persists after pregnancy. GDM
affects up to 14 percent of the pregnant population—approximately 135,000
women per year in United States. GDM complicates about 4 percent of all
pregnancies in the U.S. Women at greatest risk for developing GDM are
obese , older than twenty-five years of age, have a previous history of
abnormal glucose control, have first-degree relatives with diabetes, or are
members of ethnic groups with a high prevalence of diabetes. Infants of a
woman with GDM are at a higher risk of developing obesity, impaired
glucose tolerance, or diabetes at an early age. After a pregnancy with GDM,
the mother has an increased risk of developing type 2 diabetes.
Other forms of diabetes are associated with genetic defects in the
specialized cells of the pancreas, drug or chemical use, infections, or other
diseases. The most notable of the genetically linked diabetes is maturity
onset diabetes of the young (MODY). Characterized by the onset of
hyperglycemia before the age of twenty-five, insulin secretion is impaired
while minimal or no defects exist in insulin action. Drugs , infections, and
diseases cause diabetes by damaging the pancreas and/or impairing insulin
action or secretion.
Diabetes Complications
People with diabetes are at increased risk for serious long-term
complications. Hyperglycemia, as measured by fasting plasma glucose
concentration or glycosylated hemoglobin (HbA1c), causes structural and
functional changes in the retina, nerves, kidneys, and blood vessels. This
damage can lead to blindness, numbness, reduced circulation, amputations,
kidney disease, and cardiovascular disease. Type 1 diabetes is more likely to
lead to kidney failure. About 40 percent of people with type 1 diabetes
develop severe kidney disease and kidney failure by the age of fifty.

Nevertheless, between 1993 and 1997, more than 100,000 people in the
United States were treated for kidney failure caused by type 2 diabetes.
African Americans experience higher rates of diabetes-related
complications such as eye disease, kidney failure, and amputations. They
also experience greater disability from these complications. The frequency
of diabetic retinopathy (disease of the small blood vessels in the retina
causing deterioration of eyesight) is 40 to 50 percent higher in African
Americans than in white Americans. In addition, the rate of diabetic
retinopathy among Mexican Americans is more than twice that of non-
Hispanic white Americans. Furthermore, African Americans with diabetes
are much more likely to undergo a lower-extremity amputation than white
or Hispanic Americans with diabetes. Little is known about these
complications in Asian and Pacific Islander-Americans.
Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemia state (HHS)
are serious diabetic emergencies and the most frequent cause of mortality.
Both DKA and HHS result from an insulin deficiency and an increase in
counter-regulatory hormones (a.k.a. hyperglycemia). Hyperglycemia leads
to glycosuria (glucose in the urine), increased urine output, and
dehydration. Because the glucose is excreted in the urine, the body
becomes starved for energy . At this point, the body either continues to
excrete glucose in the urine making the hyperglycemia worse (HHS), or the
body begins to break down triglycerides causing the release of ketones
(by-products of fat breakdown) into the urine and bloodstream (DKA). The
mortality rate of patients with DKA is less than 5 percent while the
mortality rate of HHS patients is about 15 percent. Infection (urinary tract
infections and pneumonia account for 30 to 50 percent of cases), omission
of insulin, and increased amounts of counter-regulatory hormones
contribute to DKA and HHS. Type 1 and type 2 diabetic patients may
experience DKA and HHS. However, DKA is more common in type 1
diabetic patients, while HHS is more common in type 2 diabetic patients.

Treatment of DKA and HHS involves correction of dehydration,
hyperglycemia, ketoacidosis, and electrolyte deficits and imbalances.
Treatment for Diabetes
Treatment for diabetes involves following a regimen of diet, exercise, self-
monitoring of blood glucose, and taking medication or insulin injections.
Although type 1 diabetes is primarily managed with daily insulin injections,
type 2 diabetes can be controlled with diet and exercise. However, when
diet and exercise fail, medication is added to stimulate the production of
insulin, reduce insulin resistance, decrease the liver
Medscape
eMedicine Medscape CME Physician Connect Find a Physician...
CLOSE [X]
SPECIALTY SITES Allergy & Clinical
Immunology Anesthesiology Cardiology Critical Care Dermatology
Diabetes & Endocrinology Emergency Medicine Family Medicine Gastroenterology General Surgery
Hematology-Oncology HIV/AIDS
Infectious Diseases
Internal Medicine Lab Medicine Nephrology Neurology
Ob/Gyn & Women's Health Oncology
Ophthalmology Orthopaedics
Pathology & Lab Medicine Pediatrics
Plastic Surgery & Aesthetic Medicine
Psychiatry & Mental Health Public Health & Prevention
Pulmonary Medicine
Radiology Rheumatology
Surgery Transplantation
Urology Women's Health
OTHER SITES Business of
Medicine Medscape Today Med Students
Nurses Pharmacists
Medscape Medscape CME eMedicine Drug Reference MEDLINE All

Log In | Register
MEDICINE
SURGERY
PEDIATRICS
Allergy and Immunology
Cardiology Clinical Procedures
Critical Care Dermatology
Emergency Medicine Endocrinology
Gastroenterology Genomic Medicine
Hematology Infectious Diseases
Nephrology
Neurology Obstetrics/Gynecology
Oncology Pathology
Perioperative Care Physical Medicine and
Rehabilitation Psychiatry
Pulmonology Radiology
Rheumatology Sports Medicine
eMedicine Specialties > Endocrinology > Diabetes Mellitus
Diabetes Mellitus, Type 2
Author: Kenneth Patrick L Ligaray, MD, Fellow, Department of Endocrinology, Diabetes and Metabolism, St Louis UniversityCoauthor(s): William L Isley, MD, Senior Associate Consultant, Associate Professor of Medicine, Division of Endocrinology, Diabetes, Metabolism, and Nutrition, Mayo Clinic of RochesterContributor Information and Disclosures
Updated: Feb 4, 2010
Print This
Email This
Overview Differential Diagnoses & Workup Treatment & Medication Follow-up Multimedia
References Keywords Further Reading
INFORMATION FROM INDUSTRY

Effective non-narcotic, non-benzodiazepine treatment of insomnia
Explore a hypothetical case in insomnia
Introduction
Background
Type 2 diabetes mellitus is a group of disorders characterized by hyperglycemia and associated with
microvascular (ie, retinal, renal, possibly neuropathic), macrovascular (ie, coronary, peripheral vascular), and
neuropathic (ie, autonomic, peripheral) complications. Unlike patients with type 1 diabetes mellitus, patients
with type 2 are not absolutely dependent upon insulin for life, even though many of them are ultimately treated
with insulin. See below for images on diagnosis and treatment.
Diagnostic criteria (American Diabetes Association) for diabetes mellitus type 2.


Treatment of type 2 diabetes mellitus.

Pathophysiology
Hyperglycemia results from lack of endogenous insulin, which is either absolute, as in type 1 diabetes mellitus,
or relative, as in type 2 diabetes mellitus. Relative insulin deficiency usually occurs because of resistance to the
actions of insulin in muscle, fat, and the liver and an inadequate response by the pancreatic beta cell. Insulin
resistance, which has been attributed to elevated levels of free fatty acids in plasma,1 leads to decreased
glucose transport in muscle, elevated hepatic glucose production, and increased breakdown of fat.

The genetics of type 2 diabetes are complex and not completely understood, but presumably this disease is
related to multiple genes (with the exception of maturity-onset diabetes of the young [MODY]). Evidence
supports inherited components for pancreatic beta-cell failure and insulin resistance. Considerable debate
exists regarding the primary defect in type 2 diabetes mellitus. Most patients have insulin resistance and some
degree of insulin deficiency. However, insulin resistance per se is not the sine qua non for type 2 diabetes
mellitus because many people with insulin resistance (particularly those who are obese) do not develop
glucose intolerance. Therefore, insulin deficiency is necessary for the development of hyperglycemia. Insulin
concentrations may be high, yet inappropriately low for the level of glycemia.
MODY is associated with autosomal dominant inheritance and is characterized by onset in at least 1 family
member younger than 25 years, absence of autoantibodies, correction of fasting hyperglycemia without insulin
for at least 2 years, and absence of ketosis. At least 6 genetically different types of MODY have been
described.2 Some patients ultimately require insulin to control glycemia. Variants in 2 of the genes associated
with MODY (HNF-1alpha and, to a lesser extent, HNF-4alpha) have been shown to predict future type 2
diabetes.3
Presumably, the defects of type 2 diabetes mellitus occur when a diabetogenic lifestyle (ie, excessive caloric
intake, inadequate caloric expenditure, obesity) is superimposed upon a susceptible genotype. The body mass
index at which excess weight increases risk for diabetes varies with different racial groups. For example,
compared with persons of European ancestry, persons of Asian ancestry are at increased risk for diabetes at
lower levels of overweight.4 In addition, an in utero environment resulting in low birth weight may predispose
some individuals to develop type 2 diabetes mellitus.5,6 A simplified scheme for the pathophysiology of abnormal
glucose metabolism in type 2 diabetes mellitus is depicted in the image below.
Simplified scheme for the pathophysiology of type 2 diabetes mellitus.

Hyperglycemia appears to be the determinant of microvascular and metabolic complications. However,
glycemia is much less related to macrovascular disease. Insulin resistance with concomitant lipid (ie, small
dense low-density lipoprotein [LDL] particles, low high-density lipoprotein-cholesterol [HDL-C] levels, elevated
triglyceride-rich remnant lipoproteins) and thrombotic (ie, elevated type-1 plasminogen activator inhibitor [PAI-
1], elevated fibrinogen) abnormalities, as well as conventional atherosclerotic risk factors (eg, family history,
smoking, hypertension, elevated low-density lipoprotein-cholesterol [LDL-C], low HDL-C), determine
cardiovascular risk.
Increased cardiovascular risk appears to begin prior to the development of frank hyperglycemia, presumably
because of the effects of insulin resistance. Stern in 19967 and Haffner and D'Agostino in 19998 developed the
"ticking clock" hypothesis of complications, asserting that the clock starts ticking for microvascular risk at the
onset of hyperglycemia, while the clock starts ticking for macrovascular risk at some antecedent point,
presumably with the onset of insulin resistance.
Frequency
United States

In 2007, the estimated prevalence of diabetes in the United States was 7.8% (23.6 million people); almost one
third of cases were undiagnosed.9 More than 90% of cases of diabetes are type 2 diabetes mellitus. With
increasing obesity in the population, an older population, and an increase in the population of higher-risk
minority groups (see Race), prevalence is increasing.
International
Type 2 diabetes mellitus is less common in non-Western countries where the diet contains fewer calories and
caloric expenditure on a daily basis is higher. However, as people in these countries adopt Western lifestyles,
weight gain and type 2 diabetes mellitus are becoming virtually epidemic.
Mortality/Morbidity
Diabetes mellitus is one of the leading causes of morbidity and mortality in the United States because of its role
in the development of optic, renal, neuropathic, and cardiovascular disease. These complications, particularly
cardiovascular disease (~50-75% of medical expenditures), are the major sources of expenses for patients with
diabetes mellitus. Approximately two thirds of people with diabetes die from heart disease or stroke. Men with
diabetes face a 2-fold increased risk for coronary heart disease, and women have a 3- to 4-fold increased risk.
In 1994, 1 of every 7 health care dollars in the United States was spent on patients with diabetes mellitus. The
2002 estimate for direct medical costs due to diabetes in the United States was $92 billion, with another $40
billion in indirect costs. Approximately 20% of Medicare funds are spent on these patients.
Diabetes mellitus is the leading cause of blindness in working-age adults in the United States; diabetic
retinopathy accounts for 12,000-24,000 newly blind persons every year.9 The National Eye Institute
estimates that laser surgery and appropriate follow-up care can reduce the risk of blindness from
diabetic retinopathy by 90%.10
Diabetes mellitus is the leading cause of end-stage renal disease (ESRD), accounting for 44% of new
cases, according to the Centers for Disease Control and Prevention (CDC).11 In 2005, 46,739 people in
the United States and Puerto Rico began renal replacement therapy, and 178,689 people with
diabetes were on dialysis or had received a kidney transplant.9
Diabetes mellitus is the leading cause of nontraumatic lower limb amputations in the United States,
with a 15- to 40-fold increase in risk over that of the nondiabetic population. In 2004, about 71,000
nontraumatic lower limb amputations were performed related to neuropathy and vasculopathy.9
Race
The prevalence of type 2 diabetes mellitus varies widely among various racial and ethnic groups. The image
below shows data for various groups. Type 2 diabetes mellitus is becoming virtually pandemic in some groups
of Native Americans and Hispanic people. The risk of retinopathy and nephropathy appears to be greater in
blacks, Native Americans, and Hispanics.
Prevalence of diabetes mellitus type 2 in various racial and ethnic groups in the United
States (2007 estimates).

Sex
Type 2 diabetes mellitus is slightly more common in older women than men.
Age
While type 2 diabetes mellitus traditionally has been thought to affect individuals older than 40 years, it is being
recognized increasingly in younger persons, particularly in highly susceptible racial and ethnic groups and the
obese. In some areas, more type 2 than type 1 diabetes mellitus is being diagnosed in prepubertal children,
teenagers, and young adults. The prevalence of diabetes mellitus by age is shown in the image below. Virtually
all cases of diabetes mellitus in older individuals are type 2.
Prevalence of diabetes mellitus type 2 by age in the United States (2007 estimates).

Clinical
History
While a diagnosis of diabetes mellitus is readily entertained when a patient presents with classic
symptoms (ie, polyuria, polydipsia, polyphagia, weight loss), most patients with type 2 diabetes
mellitus are asymptomatic for years. Other symptoms that might suggest hyperglycemia include
blurred vision, lower extremity paresthesias, or yeast infections, particularly balanitis in men. However,
the asymptomatic state does not mean that hyperglycemia is not affecting the individual.
The possible presence of diabetes mellitus should be considered in obese patients, patients with a
first-degree relative with type 2 diabetes mellitus, members of high-risk ethnic groups (ie, black,
Hispanic, Native American, Asian American, Pacific Islander), women with a previous delivery of a
large infant (>9 lb) or with a history of gestational diabetes mellitus, patients with hypertension, or
patients with high triglycerides (>250 mg/dL) or low HDL-C (<35 mg/dL). While the United States
Public Health Service and the American College of Physicians do not recommend routine screening for
diabetes, targeted screening may be useful. For example, in one study of patients admitted to the
hospital with acute coronary syndrome, none of whom were known to have diabetes, admission and
fasting plasma glucose testing identified diabetes in 27%.12
Because polycystic ovary disease is an insulin-resistant state, screening these women may be
warranted.
Whether at-risk persons should be screened for prediabetes is unclear at present. The therapy would
generally be lifestyle changes to facilitate weight loss and improve cardiovascular fitness, and in
virtually all cases, this would be the recommendation for such patients without a measured glucose
value.

Physical
Early in the course of diabetes mellitus, the physical examination findings are likely to be unrevealing.
However, ultimately, end-organ damage may be observed. Potential findings are listed in the image below.
Possible physical examination findings in patients with type 2 diabetes mellitus.

Causes
Superimposition of caloric excess (typically, high intake and low expenditure) on a susceptible
genotype appears to cause type 2 diabetes mellitus. A large, population-based, prospective study has
shown that an energy-dense diet may be a risk factor for the development of diabetes that
is independent of baseline obesity.13
Diabetes mellitus may be caused by other conditions. Secondary diabetes may occur in patients taking
glucocorticoids or when patients have conditions that antagonize the actions of insulin (eg, Cushing
syndrome, acromegaly, pheochromocytoma).
More on Diabetes Mellitus, Type 2
Overview: Diabetes Mellitus, Type 2
Differential Diagnoses & Workup: Diabetes Mellitus, Type 2
Treatment & Medication: Diabetes Mellitus, Type 2
Follow-up: Diabetes Mellitus, Type 2
Multimedia: Diabetes Mellitus, Type 2
References
Further Reading
Next Page »
Print This
Email This
Search for CME/CE on This Topic »
medscapecme

RELATED EMEDICINE ARTICLES
Diabetes Mellitus, Type 2 (Pediatrics: General Medicine) Diabetes Mellitus and Pregnancy (Endocrinology) Diabetes Mellitus, Type 2 - A Review (Emergency Medicine) Diabetes Mellitus, Type 1 (Endocrinology)
Patient Education
Diabetes Causes Diabetes Treatment Diabetes Overview Diabetes Center Diabetes Symptoms
RELATED MEDSCAPE ARTICLES
News
Optimal Insulin Dosing Regimen for Type 2 Diabetes Identified Weight Loss Should Improve OSA in Obese Patients With Type 2 Diabetes Smoking Cessation Linked to Higher Short-Term Risk for Type 2 Diabetes
Articles
Timing Is Everything: Age of Onset Influences Long-term Retinopathy Risk in Type 2 Diabetes, Independent of Traditional Risk Factors
Determining Effective Insulin Analog Therapy Based on the Individualized Needs of Patients With Type 2 Diabetes Mellitus
Impact of Untreated Obstructive Sleep Apnea on Glucose Control in Type 2 Diabetes. F1000: "Changes Clinical Practice"Resource Centers
Incretin Hormones in Diabetes and Metabolism Resource Center Hypogonadism Resource Center Diabetic Microvascular Complications Resource Center
Medscape Medscape CME eMedicine Drug Reference MEDLINE All

\Patient information: Diabetes mellitus type 2:
Overview AuthorDavid K McCulloch, MD
Section EditorRury R Holman, FRCP
Deputy EditorsLeah K Moynihan, RNC, MSNJean E Mulder, MD
Find Print Email ShareThis
Contents of this article
INTRODUCTION THE IMPACT OF DIABETES CAUSES DIAGNOSIS TREATMENT COMPLICATIONS PREGNANCY AND DIABETES WHERE TO GET MORE INFORMATION REFERENCES
GRAPHICS
FIGURES Pancreas anatomy TABLES A1C and blood glucose
INTRODUCTION
Type 2 diabetes mellitus occurs when the pancreas (an organ in the abdomen) produces insufficient amounts of the hormone insulin and/or the body's tissues become resistant to normal or even high levels of insulin (figure 1). This causes high blood glucose (sugar) levels, which can lead to a number of complications if untreated.
Type 2 diabetes is a chronic medical condition that requires regular monitoring and treatment. Treatment, which includes lifestyle adjustments, self-care measures, and sometimes medications, can control blood sugar levels in the near-normal range and minimize the risk of diabetes-related complications.
In the United States, Canada, and Europe, type 2 diabetes accounts for about 90 percent of all cases of diabetes. More than 6 percent of all people between the ages of 20 and 74 years and more than 12 percent of people over age 40 have type 2 diabetes; these numbers continue to increase.
Topics that discuss other aspects of type 2 diabetes are also available. (See "Patient information: Diabetes mellitus type 2: Treatment" and "Patient information: Diabetes mellitus type 2: Insulin treatment" and "Patient information: Type 2 diabetes mellitus and diet" and "Patient information: Self-blood glucose monitoring in diabetes mellitus" and "Patient information: Hypoglycemia (low blood sugar) in diabetes mellitus" and "Patient information: Diabetes mellitus type 2: Alcohol, exercise, and medical care" and "Patient information: Preventing complications in diabetes mellitus".)

THE IMPACT OF DIABETES
Being diagnosed with type 2 diabetes can be a frightening and overwhelming experience for some people, and it is common to have questions about why it developed, what it means for long-term health, and how it will affect everyday life. For most people, the first few months after being diagnosed are filled with emotional highs and lows. People with newly-diagnosed diabetes, as well as their families, can use this time to learn as much as possible so that diabetes-related care (eg, blood sugar testing, medical appointments, daily medications) becomes a "normal" part of the daily routine.
In addition, people who are newly diagnosed should talk to their healthcare provider about resources that are available for medical as well as psychological support. This may include group classes, meetings with a nutritionist, social worker, or nurse educator, and other educational resources such as books, web sites, or magazines. Several of these resources are listed below (see 'Where to get more information' below.
Despite the risks associated with type 2 diabetes, most people can lead active lives and continue to enjoy the foods and activities that they previously enjoyed. Diabetes does not mean an end to special occasion foods like birthday cake, and with a little advanced planning, most people with diabetes can enjoy exercise in almost any form.
CAUSES
Type 2 diabetes is probably caused by a complex interaction of environmental factors and predisposing genetic factors.
Genetic causes — Many people with type 2 diabetes have a family member with type 2 diabetes or conditions commonly associated with diabetes, such as high cholesterol levels, high blood pressure, or obesity.
The lifetime risk that a first-degree relative (sister, brother, son, daughter) will develop diabetes is five to ten times higher than that of a person with no family history of diabetes.
The likelihood of developing type 2 diabetes is greater in certain ethnic groups; for example, people of Hispanic, African, and Asian descent are at greater risk of developing type 2 diabetes compared to people who are white.
Environmental conditions — Environmental factors such as diet and activity levels interact with genetic causes to influence the development of type 2 diabetes. The incidence of type 2 diabetes has increased dramatically in the United States over the last 20 years as the percentage of people who are obese increases.
Pregnancy — About 3 to 5 percent of pregnant women develop gestational diabetes, usually after 24 to 28 weeks of pregnancy. Gestational diabetes is similar to type 2 diabetes, but generally resolves after a woman delivers her baby. Hormones cause an increase in insulin resistance during pregnancy, which can lead to gestational diabetes. Women who develop gestational diabetes during pregnancy are at high risk for developing type 2 diabetes later in life. (See "Patient information: Gestational diabetes mellitus".)
Other causes — Other, less common causes of diabetes include endocrine conditions that indirectly change the production and action of insulin and lead to diabetes. These include

Cushing's syndrome, acromegaly, pheochromocytoma, hyperthyroidism and polycystic ovarian syndrome (PCOS). (See "Patient information: Cushing's syndrome" and "Patient information: Acromegaly" and "Patient information: Hyperthyroidism" and "Patient information: Polycystic ovary syndrome (PCOS)".)
DIAGNOSIS
The diagnosis of diabetes is based upon a person's symptoms and the results of laboratory tests.
Symptoms — Before being diagnosed with diabetes, some people have symptoms of high blood sugar, including frequent urination, excessive thirst, and blurred vision. Sometimes, diabetes is discovered when a person seeks medical help for another problem (such as erectile dysfunction or pain and numbness in the feet). However, most people with type 2 diabetes have no symptoms at all, and the diagnosis is often delayed for five or more years.
Because family history is a factor in the development of type 2 diabetes, people with family members with diabetes or conditions commonly associated with diabetes, such as hypertension, high blood lipid levels, and obesity, should mention this to their healthcare provider. There are usually few signs of diabetes on a physical examination early in the course of the disease.
Laboratory tests — Several blood tests are used to measure blood glucose levels, the primary test for diagnosing diabetes. Additional tests can determine the type of diabetes and its severity.
Random blood sugar test — For a random blood sugar test, blood can be drawn at
any time throughout the day, regardless of when the person last ate. A random blood sugar
level of 200 mg/dL (11.1 mmol/L) or higher in persons who have symptoms of high blood
sugar (see 'Symptoms' above) suggests a diagnosis of diabetes.
Fasting blood sugar test — Fasting blood sugar testing involves measuring blood
sugar after not eating or drinking for 8 to 12 hours (usually overnight). A normal fasting
blood sugar level is less than 100 mg/dL (5.55 mmol/L). A fasting blood sugar of 126 mg/dL
(7.0 mmol/L) or higher indicates diabetes. The test is done by taking a small sample of blood
from a vein or fingertip. It must be repeated on another day to confirm that it remains
abnormally high (see 'Criteria for diagnosis' below.
Hemoglobin A1C test (A1C) — The A1C blood test measures the average blood sugar
level during the past two to three months. It is used to monitor blood sugar control in people
with known diabetes. Normal values for A1C are 4 to 6 percent (table 1). The test is done by
taking a small sample of blood from a vein or fingertip.
One expert group has recommended using a hemoglobin A1C test to diagnose diabetes. Unlike other tests, the A1C test can be done at any time of day (before or after eating).

Oral glucose tolerance test — Oral glucose tolerance testing (OGTT) can be used to
diagnose diabetes and pre-diabetes. However, the OGTT is not routinely recommended
because it is inconvenient compared to a fasting blood sugar test.
The standard OGTT includes a fasting blood sugar test. The person then drinks a 75 gram liquid glucose solution (which tastes very sweet, and is usually cola or orange-flavored). Two hours later, a second blood sugar level is measured. In some cases, a blood sugar level is measured at 30 minutes and one hour after drinking the glucose solution.
Criteria for diagnosis — The following criteria are used to define a person's blood sugar levels as normal, suggestive of pre-diabetes (defined as an abnormal blood sugar level which is not high enough to be considered diabetic, but with an increased risk of diabetes in the future), or as diagnostic for diabetes.
Normal — Fasting sugar <100 mg/dL (5.55 mmol/L).
Pre-diabetes — Pre-diabetes can be diagnosed based upon a fasting blood sugar test or an OGTT.
Impaired fasting glucose is defined as a fasting blood sugar level between 100 and
125 mg/dL (5.6 to 6.9 mmol/L).
Impaired glucose tolerance is defined as a blood sugar level of 140 to 199 mg/dL,
measured two hours after a 75 gram oral glucose tolerance test.
At least 50 percent of people with impaired glucose tolerance eventually develop type 2 diabetes, and they have an increased risk of heart disease even if diabetes does not develop. Impaired glucose tolerance is very common; about 11 percent of all people between the ages of 20 and 74 years have impaired glucose tolerance.
Diabetes mellitus — A person is considered to be diabetic if he or she has one or more of the following criteria:
- Symptoms of diabetes (see 'Symptoms' above) and a random blood sugar of 200
mg/dL (11.1 mmol/L) or higher
- A fasting blood sugar level of 126 mg/dL (7.0 mmol/L) or higher
- A blood sugar of 200 mg/dL (11.1 mmol/L) or higher two hours after a 75 gram oral
glucose tolerance test.
The blood tests must be repeated on another day to confirm that they remain abnormally high.
Type 1 versus type 2 diabetes — A healthcare provider is usually able to determine whether a person has type 1 or type 2 diabetes, based upon the person's need for insulin (needed from the beginning in type 1, and less commonly early in type 2), and the presence of ketones in the urine when blood sugar levels are elevated (common in type 1, uncommon in type 2). Other characteristics such as older age and higher weight suggest, but do not prove, type 2 diabetes.

However, there are situations where it is less clear if a person has type 1 or 2 diabetes. In this situation, additional blood testing may be needed. When the type of diabetes is in doubt, the clinician will usually treat the patient with insulin, as if they have type 1, since it is critical to avoid a potentially dangerous condition known as diabetic ketoacidosis (DKA). People with type 2 diabetes do not usually develop DKA. (See "Patient information: Diabetes mellitus type 1: Overview".)
TREATMENT
A full discussion of the treatment for type 2 diabetes is available separately. (See "Patient information: Diabetes mellitus type 2: Treatment" and "Patient information: Diabetes mellitus type 2: Insulin treatment".)
COMPLICATIONS
Complications of type 2 diabetes may be related to the disease itself or to the treatments necessary to manage diabetes. (See "Patient information: Preventing complications in diabetes mellitus".)
PREGNANCY AND DIABETES
Women with type 2 diabetes are usually able to become pregnant and have a healthy baby. However, it is important to tightly control blood sugar levels before and during pregnancy to minimize the risk of complications. A full discussion of this topic is available separately. (See "Patient information: Care during pregnancy for women with type 1 or 2 diabetes mellitus".)
WHERE TO GET MORE INFORMATION
Your healthcare provider is the best source of information for questions and concerns related to your medical problem. Because no two people are exactly alike and recommendations can vary from one person to another, it is important to seek guidance from a provider who is familiar with your individual situation.
This discussion will be updated as needed every four months on our web site (www.uptodate.com/patients). Additional topics as well as selected discussions written for healthcare professionals are also available for those who would like more detailed information.
Some of the most pertinent include:
Patient Level Information:Patient information: Diabetes mellitus type 2: Alcohol, exercise, and medical carePatient information: Foot care in diabetes mellitusPatient information: Hypoglycemia (low blood sugar) in diabetes mellitusPatient information: Preventing complications in diabetes mellitusPatient information: Self-blood glucose monitoring in diabetes mellitusPatient information: Diabetes mellitus type 2: TreatmentPatient information: Diabetes mellitus type 2: Insulin treatmentPatient information: Type 2 diabetes mellitus and dietPatient information: Gestational diabetes mellitus

Patient information: Cushing's syndromePatient information: AcromegalyPatient information: HyperthyroidismPatient information: Polycystic ovary syndrome (PCOS)Patient information: Diabetes mellitus type 1: OverviewPatient information: Care during pregnancy for women with type 1 or 2 diabetes mellitus
Professional Level Information:Blood glucose self-monitoring in management of diabetes mellitusClassification of diabetes mellitus and genetic diabetic syndromesDiagnosis of diabetes mellitusEffects of exercise in diabetes mellitus in adultsEstimation of blood glucose control in diabetes mellitusGlycemic control and vascular complications in type 2 diabetes mellitusInsulin therapy in type 2 diabetes mellitusManagement of hypoglycemia during treatment of diabetes mellitusManagement of persistent hyperglycemia in type 2 diabetes mellitusNutritional considerations in type 1 diabetes mellitusNutritional considerations in type 2 diabetes mellitusPrediction and prevention of type 2 diabetes mellitusScreening for diabetes mellitusSmoking and cardiovascular risk in diabetes mellitusThe metabolic syndrome (insulin resistance syndrome or syndrome X)Treatment of diabetes mellitus in elderly adultsPatient information: Foot care in diabetes mellitus
A number of web sites have information about medical problems and treatments, although it can be difficult to know which sites are reputable. Information provided by the National Institutes of Health, national medical societies and some other well-established organizations are often reliable sources of information, although the frequency with which they are updated is variable.
National Library of Medicine
(www.nlm.nih.gov/medlineplus/healthtopics.html)
National Institute of Diabetes and Digestive and Kidney Diseases
(www.niddk.nih.gov)
American Diabetes Association (ADA)
(800)-DIABETES (800-342-2383) (www.diabetes.org)
The Endocrine Society
(www.endo-society.org)
The Hormone Foundation

(www.hormone.org/public/diabetes.cfm, available in English and Spanish)
[1-7]
Last literature review version 17.3: September 2009 This topic last updated: June 15, 2009 (More)
Find Print Email
The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek the advice of your own physician or other qualified health care professional regarding any medical questions or conditions. The use of this website is governed by the UpToDate Terms of Use (click here) ©2010 UpToDate, Inc.
References Top
1. Knowler, WC, Barrett-Connor, E, Fowler, SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346:393.
2. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352:854.
3. Kjos, SL, Peters, RK, Xiang, A, et al. Predicting future diabetes in Latino women with gestational diabetes: Utility of early postpartum glucose tolerance testing. Diabetes 1995; 44:586.
4. Selvin, E, Coresh, J, Golden, SH, et al. Glycemic control, atherosclerosis, and risk factors for cardiovascular disease in individuals with diabetes: the atherosclerosis risk in communities study. Diabetes Care 2005; 28:1965.
Patient information: Diabetes mellitus type 2:
Overview AuthorDavid K McCulloch, MD
Section EditorRury R Holman, FRCP
Deputy EditorsLeah K Moynihan, RNC, MSNJean E Mulder, MD
Find Print Email ShareThis
Contents of this article
INTRODUCTION THE IMPACT OF DIABETES CAUSES DIAGNOSIS TREATMENT COMPLICATIONS PREGNANCY AND DIABETES WHERE TO GET MORE INFORMATION REFERENCES
GRAPHICS

FIGURES Pancreas anatomy TABLES A1C and blood glucose
INTRODUCTION
Type 2 diabetes mellitus occurs when the pancreas (an organ in the abdomen) produces insufficient amounts of the hormone insulin and/or the body's tissues become resistant to normal or even high levels of insulin (figure 1). This causes high blood glucose (sugar) levels, which can lead to a number of complications if untreated.
Type 2 diabetes is a chronic medical condition that requires regular monitoring and treatment. Treatment, which includes lifestyle adjustments, self-care measures, and sometimes medications, can control blood sugar levels in the near-normal range and minimize the risk of diabetes-related complications.
In the United States, Canada, and Europe, type 2 diabetes accounts for about 90 percent of all cases of diabetes. More than 6 percent of all people between the ages of 20 and 74 years and more than 12 percent of people over age 40 have type 2 diabetes; these numbers continue to increase.
Topics that discuss other aspects of type 2 diabetes are also available. (See "Patient information: Diabetes mellitus type 2: Treatment" and "Patient information: Diabetes mellitus type 2: Insulin treatment" and "Patient information: Type 2 diabetes mellitus and diet" and "Patient information: Self-blood glucose monitoring in diabetes mellitus" and "Patient information: Hypoglycemia (low blood sugar) in diabetes mellitus" and "Patient information: Diabetes mellitus type 2: Alcohol, exercise, and medical care" and "Patient information: Preventing complications in diabetes mellitus".)
THE IMPACT OF DIABETES
Being diagnosed with type 2 diabetes can be a frightening and overwhelming experience for some people, and it is common to have questions about why it developed, what it means for long-term health, and how it will affect everyday life. For most people, the first few months after being diagnosed are filled with emotional highs and lows. People with newly-diagnosed diabetes, as well as their families, can use this time to learn as much as possible so that diabetes-related care (eg, blood sugar testing, medical appointments, daily medications) becomes a "normal" part of the daily routine.
In addition, people who are newly diagnosed should talk to their healthcare provider about resources that are available for medical as well as psychological support. This may include group classes, meetings with a nutritionist, social worker, or nurse educator, and other educational resources such as books, web sites, or magazines. Several of these resources are listed below (see 'Where to get more information' below.
Despite the risks associated with type 2 diabetes, most people can lead active lives and continue to enjoy the foods and activities that they previously enjoyed. Diabetes does not mean an end to special occasion foods like birthday cake, and with a little advanced planning, most people with diabetes can enjoy exercise in almost any form.

CAUSES
Type 2 diabetes is probably caused by a complex interaction of environmental factors and predisposing genetic factors.
Genetic causes — Many people with type 2 diabetes have a family member with type 2 diabetes or conditions commonly associated with diabetes, such as high cholesterol levels, high blood pressure, or obesity.
The lifetime risk that a first-degree relative (sister, brother, son, daughter) will develop diabetes is five to ten times higher than that of a person with no family history of diabetes.
The likelihood of developing type 2 diabetes is greater in certain ethnic groups; for example, people of Hispanic, African, and Asian descent are at greater risk of developing type 2 diabetes compared to people who are white.
Environmental conditions — Environmental factors such as diet and activity levels interact with genetic causes to influence the development of type 2 diabetes. The incidence of type 2 diabetes has increased dramatically in the United States over the last 20 years as the percentage of people who are obese increases.
Pregnancy — About 3 to 5 percent of pregnant women develop gestational diabetes, usually after 24 to 28 weeks of pregnancy. Gestational diabetes is similar to type 2 diabetes, but generally resolves after a woman delivers her baby. Hormones cause an increase in insulin resistance during pregnancy, which can lead to gestational diabetes. Women who develop gestational diabetes during pregnancy are at high risk for developing type 2 diabetes later in life. (See "Patient information: Gestational diabetes mellitus".)
Other causes — Other, less common causes of diabetes include endocrine conditions that indirectly change the production and action of insulin and lead to diabetes. These include Cushing's syndrome, acromegaly, pheochromocytoma, hyperthyroidism and polycystic ovarian syndrome (PCOS). (See "Patient information: Cushing's syndrome" and "Patient information: Acromegaly" and "Patient information: Hyperthyroidism" and "Patient information: Polycystic ovary syndrome (PCOS)".)
DIAGNOSIS
The diagnosis of diabetes is based upon a person's symptoms and the results of laboratory tests.
Symptoms — Before being diagnosed with diabetes, some people have symptoms of high blood sugar, including frequent urination, excessive thirst, and blurred vision. Sometimes, diabetes is discovered when a person seeks medical help for another problem (such as erectile dysfunction or pain and numbness in the feet). However, most people with type 2 diabetes have no symptoms at all, and the diagnosis is often delayed for five or more years.
Because family history is a factor in the development of type 2 diabetes, people with family members with diabetes or conditions commonly associated with diabetes, such as hypertension, high blood lipid levels, and obesity, should mention this to their healthcare provider. There are usually few signs of diabetes on a physical examination early in the course of the disease.

Laboratory tests — Several blood tests are used to measure blood glucose levels, the primary test for diagnosing diabetes. Additional tests can determine the type of diabetes and its severity.
Random blood sugar test — For a random blood sugar test, blood can be drawn at
any time throughout the day, regardless of when the person last ate. A random blood sugar
level of 200 mg/dL (11.1 mmol/L) or higher in persons who have symptoms of high blood
sugar (see 'Symptoms' above) suggests a diagnosis of diabetes.
Fasting blood sugar test — Fasting blood sugar testing involves measuring blood
sugar after not eating or drinking for 8 to 12 hours (usually overnight). A normal fasting
blood sugar level is less than 100 mg/dL (5.55 mmol/L). A fasting blood sugar of 126 mg/dL
(7.0 mmol/L) or higher indicates diabetes. The test is done by taking a small sample of blood
from a vein or fingertip. It must be repeated on another day to confirm that it remains
abnormally high (see 'Criteria for diagnosis' below.
Hemoglobin A1C test (A1C) — The A1C blood test measures the average blood sugar
level during the past two to three months. It is used to monitor blood sugar control in people
with known diabetes. Normal values for A1C are 4 to 6 percent (table 1). The test is done by
taking a small sample of blood from a vein or fingertip.
One expert group has recommended using a hemoglobin A1C test to diagnose diabetes. Unlike other tests, the A1C test can be done at any time of day (before or after eating).
Oral glucose tolerance test — Oral glucose tolerance testing (OGTT) can be used to
diagnose diabetes and pre-diabetes. However, the OGTT is not routinely recommended
because it is inconvenient compared to a fasting blood sugar test.
The standard OGTT includes a fasting blood sugar test. The person then drinks a 75 gram liquid glucose solution (which tastes very sweet, and is usually cola or orange-flavored). Two hours later, a second blood sugar level is measured. In some cases, a blood sugar level is measured at 30 minutes and one hour after drinking the glucose solution.
Criteria for diagnosis — The following criteria are used to define a person's blood sugar levels as normal, suggestive of pre-diabetes (defined as an abnormal blood sugar level which is not high enough to be considered diabetic, but with an increased risk of diabetes in the future), or as diagnostic for diabetes.
Normal — Fasting sugar <100 mg/dL (5.55 mmol/L).
Pre-diabetes — Pre-diabetes can be diagnosed based upon a fasting blood sugar test or an OGTT.
Impaired fasting glucose is defined as a fasting blood sugar level between 100 and
125 mg/dL (5.6 to 6.9 mmol/L).
Impaired glucose tolerance is defined as a blood sugar level of 140 to 199 mg/dL,
measured two hours after a 75 gram oral glucose tolerance test.

At least 50 percent of people with impaired glucose tolerance eventually develop type 2 diabetes, and they have an increased risk of heart disease even if diabetes does not develop. Impaired glucose tolerance is very common; about 11 percent of all people between the ages of 20 and 74 years have impaired glucose tolerance.
Diabetes mellitus — A person is considered to be diabetic if he or she has one or more of the following criteria:
- Symptoms of diabetes (see 'Symptoms' above) and a random blood sugar of 200
mg/dL (11.1 mmol/L) or higher
- A fasting blood sugar level of 126 mg/dL (7.0 mmol/L) or higher
- A blood sugar of 200 mg/dL (11.1 mmol/L) or higher two hours after a 75 gram oral
glucose tolerance test.
The blood tests must be repeated on another day to confirm that they remain abnormally high.
Type 1 versus type 2 diabetes — A healthcare provider is usually able to determine whether a person has type 1 or type 2 diabetes, based upon the person's need for insulin (needed from the beginning in type 1, and less commonly early in type 2), and the presence of ketones in the urine when blood sugar levels are elevated (common in type 1, uncommon in type 2). Other characteristics such as older age and higher weight suggest, but do not prove, type 2 diabetes.
However, there are situations where it is less clear if a person has type 1 or 2 diabetes. In this situation, additional blood testing may be needed. When the type of diabetes is in doubt, the clinician will usually treat the patient with insulin, as if they have type 1, since it is critical to avoid a potentially dangerous condition known as diabetic ketoacidosis (DKA). People with type 2 diabetes do not usually develop DKA. (See "Patient information: Diabetes mellitus type 1: Overview".)
TREATMENT
A full discussion of the treatment for type 2 diabetes is available separately. (See "Patient information: Diabetes mellitus type 2: Treatment" and "Patient information: Diabetes mellitus type 2: Insulin treatment".)
COMPLICATIONS
Complications of type 2 diabetes may be related to the disease itself or to the treatments necessary to manage diabetes. (See "Patient information: Preventing complications in diabetes mellitus".)
PREGNANCY AND DIABETES
Women with type 2 diabetes are usually able to become pregnant and have a healthy baby. However, it is important to tightly control blood sugar levels before and during pregnancy to

minimize the risk of complications. A full discussion of this topic is available separately. (See "Patient information: Care during pregnancy for women with type 1 or 2 diabetes mellitus".)
WHERE TO GET MORE INFORMATION
Your healthcare provider is the best source of information for questions and concerns related to your medical problem. Because no two people are exactly alike and recommendations can vary from one person to another, it is important to seek guidance from a provider who is familiar with your individual situation.
This discussion will be updated as needed every four months on our web site (www.uptodate.com/patients). Additional topics as well as selected discussions written for healthcare professionals are also available for those who would like more detailed information.
Some of the most pertinent include:
Patient Level Information:Patient information: Diabetes mellitus type 2: Alcohol, exercise, and medical carePatient information: Foot care in diabetes mellitusPatient information: Hypoglycemia (low blood sugar) in diabetes mellitusPatient information: Preventing complications in diabetes mellitusPatient information: Self-blood glucose monitoring in diabetes mellitusPatient information: Diabetes mellitus type 2: TreatmentPatient information: Diabetes mellitus type 2: Insulin treatmentPatient information: Type 2 diabetes mellitus and dietPatient information: Gestational diabetes mellitusPatient information: Cushing's syndromePatient information: AcromegalyPatient information: HyperthyroidismPatient information: Polycystic ovary syndrome (PCOS)Patient information: Diabetes mellitus type 1: OverviewPatient information: Care during pregnancy for women with type 1 or 2 diabetes mellitus
Professional Level Information:Blood glucose self-monitoring in management of diabetes mellitusClassification of diabetes mellitus and genetic diabetic syndromesDiagnosis of diabetes mellitusEffects of exercise in diabetes mellitus in adultsEstimation of blood glucose control in diabetes mellitusGlycemic control and vascular complications in type 2 diabetes mellitusInsulin therapy in type 2 diabetes mellitusManagement of hypoglycemia during treatment of diabetes mellitusManagement of persistent hyperglycemia in type 2 diabetes mellitusNutritional considerations in type 1 diabetes mellitusNutritional considerations in type 2 diabetes mellitusPrediction and prevention of type 2 diabetes mellitusScreening for diabetes mellitusSmoking and cardiovascular risk in diabetes mellitusThe metabolic syndrome (insulin resistance syndrome or syndrome X)Treatment of diabetes mellitus in elderly adultsPatient information: Foot care in diabetes mellitus

A number of web sites have information about medical problems and treatments, although it can be difficult to know which sites are reputable. Information provided by the National Institutes of Health, national medical societies and some other well-established organizations are often reliable sources of information, although the frequency with which they are updated is variable.
National Library of Medicine
(www.nlm.nih.gov/medlineplus/healthtopics.html)
National Institute of Diabetes and Digestive and Kidney Diseases
(www.niddk.nih.gov)
American Diabetes Association (ADA)
(800)-DIABETES (800-342-2383) (www.diabetes.org)
The Endocrine Society
(www.endo-society.org)
The Hormone Foundation
(www.hormone.org/public/diabetes.cfm, available in English and Spanish)
[1-7]
Last literature review version 17.3: September 2009 This topic last updated: June 15, 2009 (More)
Find Print Email
The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek the advice of your own physician or other qualified health care professional regarding any medical questions or conditions. The use of this website is governed by the UpToDate Terms of Use (click here) ©2010 UpToDate, Inc.
References Top
1. Knowler, WC, Barrett-Connor, E, Fowler, SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346:393.
2. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352:854.
3. Kjos, SL, Peters, RK, Xiang, A, et al. Predicting future diabetes in Latino women with gestational diabetes: Utility of early postpartum glucose tolerance testing. Diabetes 1995; 44:586.

4. Selvin, E, Coresh, J, Golden, SH, et al. Glycemic control, atherosclerosis, and risk factors for cardiovascular disease in individuals with diabetes: the atherosclerosis risk in communities study. Diabetes Care 2005; 28:1965.
About Us | Privacy | Site Map
March 20, 2010
home > topics a-z list > diabetes article
FONT SIZE
A
A
A
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
Glossary
Next Page »
1

Diabetes
Type 2 Diabetes Slideshow
Diabetes and Foot Problems Slideshow
Are You At Risk for Diabetic Nerve Pain?
Diabetes Overview Diabetes Causes Diabetes Symptoms When to Seek Medical Care Exams and Tests Diabetes Treatment Self-Care at Home Medical Treatment Medications Next Steps Follow-up Prevention Outlook Support Groups and Counseling For More Information Web Links Synonyms and Keywords Authors and Editors Viewer Comments: Diabetes Treatment - Effective Treatments
Diabetes + Smoking = TroubleMedical Author: Ruchi Mathur, M.D. Medical Editor: William C. Shiel Jr., MD, FACP, FACR I can summarize this little article in one quick sentence: Smoking is bad. In the general population, and particularly in patients with diabetes.... Smoking is bad.
Cigarette smoking is the leading cause if avoidable death in the United States, and accounts for almost 500,000 deaths a year. Smoking plays a role in one out of every five deaths in the United States per year. Smoking is indeed bad.
Where the health of diabetic smokers is concerned, the statistics are even worse. There is an increased risk of premature death and the development of heart disease in patients who have diabetes and continue to smoke. There is also evidence that links cigarette smoking with microvascular disease (kidney and eye damage) in diabetes. Additionally, there is data that shows that smoking may actually play a role in the development of type 2 diabetes. Smoking is bad.

Read more on smoking and diabetes »
Top Searched Diabetes Terms
symptoms, gestational diabetes, diabetes and vision, type 1 diabetes, risk factors, diagnosis, prevention
Diabetes Overview
Diabetes mellitus (DM) is a set of related diseases in which the body cannot regulate the amount of sugar (specifically, glucose) in the blood.
Glucose in the blood gives you energy to perform daily activities, walk briskly, run for a bus, ride your bike, take an aerobic exercise class, and perform your day-to-day chores.
From the foods you eat, glucose in the blood is produced by the liver (an organ on the right side of the abdomen near your stomach).
In a healthy person, the blood glucose level is regulated by several hormones, including insulin. Insulin is produced by the pancreas, a small organ between the stomach and liver. The pancreas secretes other important enzymes that help to digest food.
Insulin allows glucose to move from the blood into liver, muscle, and fat cells, where it is used for fuel.
People with diabetes either do not produce enough insulin (type 1 diabetes) or cannot use insulin properly (type 2 diabetes), or both (which occurs with several forms of diabetes).
In diabetes, glucose in the blood cannot move into cells, so it stays in the blood. This not only harms the cells that need the glucose for fuel, but also harms certain organs and tissues exposed to the high glucose levels.
Type 1 diabetes: The body stops producing insulin or produces too little insulin to regulate blood glucose level.
Type 1 diabetes comprises about 10% of total cases of diabetes in the United States.
Type 1 diabetes is typically recognized in childhood or adolescence. It used to be known as juvenile-onset diabetes or insulin-dependent diabetes mellitus.
Type 1 diabetes can occur in an older individual due to destruction of pancreas by alcohol, disease, or removal by surgery. It also results from progressive failure of the pancreatic beta cells, which produce insulin.
People with type 1 diabetes require daily insulin treatment to sustain life.
Type 2 diabetes: The pancreas secretes insulin, but the body is partially or completely unable to use the insulin. This is sometimes referred to as insulin resistance. The body tries to overcome this resistance by secreting more and more insulin. People with insulin resistance develop type 2 diabetes when they do not continue to secrete enough insulin to cope with the higher demands.
At least 90% of patients with diabetes have type 2 diabetes.

Type 2 diabetes is typically recognized in adulthood, usually after age 45 years. It used to be called adult-onset diabetes mellitus, or non-insulin-dependent diabetes mellitus. These names are no longer used because type 2 diabetes does occur in younger people, and some people with type 2 diabetes need to use insulin.
Type 2 diabetes is usually controlled with diet, weight loss, exercise, and oral medications. More than half of all people with type 2 diabetes require insulin to control their blood sugar levels at some point in the course of their illness.
Gestational diabetes is a form of diabetes that occurs during the second half of pregnancy.
Although gestational diabetes typically goes away after delivery of the baby. Women who have gestational diabetes are more likely than other women to develop type 2 diabetes later in life.
Women with gestational diabetes are more likely to have large babies.
Metabolic syndrome (also referred to as syndrome X) is a set of abnormalities in which insulin-resistant diabetes (type 2 diabetes) is almost always present along with hypertension, high fat levels in the blood (increased serum lipids, predominant elevation of LDL cholesterol, decreased HDL cholesterol, and elevated triglycerides), central obesity, and abnormalities in blood clotting and inflammatory responses. A high rate of cardiovascular disease is associated with the metabolic syndrome.
Pre-diabetes is a common condition related to diabetes. In people with pre-diabetes, the blood sugar level is higher than normal but not high enough to be considered diabetic.
Pre-diabetes increases your risk of developing type 2 diabetes and of heart disease or stroke.
Pre-diabetes can typically be reversed without insulin or medication by losing a modest amount of weight and increasing your physical activity. This weight loss can prevent, or at least delay, the onset of type 2 diabetes.
An international expert committee of the American Diabetes Association redefined the criteria for pre-diabetes, lowering the blood sugar level cut-off point for pre-diabetes. Approximately 20% more adults are now believed to have this condition and may develop diabetes within 10 years if they do not exercise or maintain a healthy weight.
About 17 million Americans (6.2% of adults in North America) are believed to have diabetes. About one third of diabetic adults do not know they have diabetes.
About 1 million new cases occur each year, and diabetes is the direct or indirect cause of at least 200,000 deaths each year.
The incidence of diabetes is increasing rapidly. This increase is due to many factors, but the most significant are the increasing incidence of obesity and the prevalence of sedentary lifestyles.
Complications of diabetes

Both forms of diabetes ultimately lead to high blood sugar levels, a condition called hyperglycemia. Over a long period of time, hyperglycemia damages the retina of the eye, the kidneys, the nerves, and the blood vessels.
Damage to the retina from diabetes (diabetic retinopathy) is a leading cause of blindness.
Damage to the kidneys from diabetes (diabetic nephropathy) is a leading cause of kidney failure.
Damage to the nerves from diabetes (diabetic neuropathy) is a leading cause of foot wounds and ulcers, which frequently lead to foot and leg amputations.
Damage to the nerves in the autonomic nervous system can lead to paralysis of the stomach (gastroparesis), chronic diarrhea, and an inability to control heart rate and blood pressure during postural changes.
Diabetes accelerates atherosclerosis, (the formation of fatty plaques inside the arteries), which can lead to blockages or a clot (thrombus). Such changes can then lead to heart attack, stroke, and decreased circulation in the arms and legs (peripheral vascular disease).
Diabetes predisposes people to high blood pressure and high cholesterol and triglyceride levels. These conditions independently and together with hyperglycemia increase the risk of heart disease, kidney disease, and other blood vessel complications.
In the short run, diabetes can contribute to a number of acute (short-lived) medical problems.
Many infections are associated with diabetes, and infections are frequently more dangerous in someone with diabetes because the body's normal ability to fight infections is impaired. To compound the problem, infections may worsen glucose control, which further delays recovery from infection.
Hypoglycemia, or low blood sugar, occurs from time to time in most people with diabetes. It results from taking too much diabetes medication or insulin (sometimes called an insulin reaction), missing a meal, doing more exercise than usual, drinking too much alcohol, or taking certain medications for other conditions. It is very important to recognize hypoglycemia and be prepared to treat it at all times. Headache, feeling dizzy, poor concentration, tremors of hands, and sweating are common symptoms of hypoglycemia. You can faint or have a seizure if blood sugar level gets too low.
Diabetic ketoacidosis is a serious condition in which uncontrolled hyperglycemia (usually due to complete lack of insulin or a relative deficiency of insulin) over time creates a buildup in the blood of acidic waste products called ketones. High levels of ketones can be very harmful. This typically happens to people with type 1 diabetes who do not have good blood glucose control. Diabetic ketoacidosis can be precipitated by infection, stress, trauma, missing medications like insulin, or medical emergencies like stroke and heart attack.
Hyperosmolar hyperglycemic nonketotic syndrome is a serious condition in which the blood sugar level gets very high. The body tries to get rid of the excess blood sugar by eliminating it in the urine. This increases the amount of urine significantly and often leads to dehydration so severe that it can cause seizures, coma, and even death. This syndrome typically occurs in people with type 2 diabetes

who are not controlling their blood sugar levels, who have become dehydrated, or who have stress, injury, stroke, or are taking certain medications, like steroids.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
Glossary
Next Page »
Next: Diabetes Causes »
Share | | | | | More
Viewer Comments & Reviews
Diabetes Treatment - Effective Treatments
The eMedicineHealth physician editors ask:Please describe what treatments have been effective for your diabetes.
Anonymously share your comment to help others.
See 2 Viewer Comments & Reviews
Submit Your Review
Privacy Policy
Diabetes
Find tips and advances in treatment.
DiabetesWMD http://w w w .emed http://w w w .emed Enter email address

null
2/5
From WebMD
Diabetes Resources
Safe Ways to Exercise With Diabetes
Featured Centers
Foods That Can Trigger Bedwetting Is Your Emphysema Under Control? 8 Ways to Boost Your Fertility
Health Solutions From Our Sponsors
Depression Med for You? Fibromyalgia Center MS Rx Options
DiabetesDiabetic Eye Disease »Diabetic Eye Disease Overview
Diabetes mellitus is one of the leading causes of irreversible blindness worldwide, and, in the United States, it is the most
common cause of blindness in people younger than 65 years of age.
In addition to being a leading cause of blindness, diabetic eye disease encompasses a wide range of problems that can
affect the eyes.

Diabetes mellitus may cause a reversible, temporary blurring of the vision, or it can cause a severe, permanent loss of vision.
Diabetes mellitus increases the risk of developing cataracts and glaucoma.
Some people may not even realize they have had diabetes mellitus for several years until they begin to experience problems with their eyes or vision. Severe diabetic eye disease most commonly develops in people who have had diabetes mellitus for many years and who have had little or poor cont...
Read the Diabetic Eye Disease article »
Read What Your Physician is Reading on eMedicine
Diabetes Mellitus, Type 2 »
Type 2 diabetes mellitus is a group of disorders characterized by hyperglycemia and associated with microvascular (ie,
retinal, renal, possibly neuropathic), macrovascular (ie, coronary, peripheral vascular), and neuropathic (ie, autonomic,
peripheral) complications.
Read More on eMedicine »
Featured Topics Is Sleepiness Hurting You? Depression Tips Slideshow Causes of Fatigue Slideshow Are You at Risk for Diabetic Nerve Pain? Trouble Breathing? Take the COPD Health Check
Topics Related to Diabetes
Diabetic Eye Disease Diabetic Foot Care Diabetic Ketoacidosis Heart Attack High Blood Sugar (Hyperglycemia) High Cholesterol Hypoglycemia (Low Blood Sugar) Leg Pain Night Sweats ObesityMedical Dictionary
or A-Z List
Search for Medical Terms

First Aid & Emergencies | Topics A-Z | Picture Slideshows | Medications | eTools | Medical Dictionary Definitions
About Us | Privacy | Terms of Use | Advertising Policy | Site Map
eMedicine® | WebMD® | Medscape® | MedicineNet® | RxList®
This site complies to the HONcode standard fortrustworthy health information: Verify here.
©2010 WebMD, Inc. All rights reserved.eMedicineHealth does not provide medical advice, diagnosis or treatment.
See Additional Information.
Related Documents