Received: 26.06.2010 Accepted: 21.07.2010 J Gastrointestin Liver Dis September 2010 Vol.19 No 3, 295-202 Address for correspondence: Dr. Angelo Zullo Gastroenterologia ed Endoscopia Digestiva PTP Nuovo Regina Margherita Roma, Italy Email: [email protected] Cyclic Antibiotic Therapy for Diverticular Disease: a Critical Reappraisal Angelo Zullo 1 , Cesare Hassan 1 , Giovanni Maconi 2 , Gianpiero Manes 2 , Gianfranco Tammaro 3 , Vincenzo De Francesco 4 , Bruno Annibale 5 , Leonardo Ficano 6 , Luigi Buri 7 , Giovanni Gatto 8 , Roberto Lorenzetti 1 , Salvatore M. Campo 1 , Enzo Ierardi 4 , Fabio Pace 9 , Sergio Morini 1 1) Gastroenterology Unit, “Nuovo Regina Margherita” Hospital, Rome; 2) Dept. of Clinical Sciences, Division of Gastroenterology, “L. Sacco” University Hospital, Milan; 3) Gastroenterology Unit, “Sant’Eugenio” Hospital, Rome; 4) Section of Gastroenterology, Department of Medical Sciences, University of Foggia, Foggia; 5) Dept. of Digestive and Liver Diseases, University “La Sapienza”, Sant’Andrea Hospital Rome; 6) Department of Oncology, Division of General and Oncological Surgery, University of Palermo, Palermo; 7) Gastroenterology and Digestive Endoscopy Unit, “Cattinara’’ Hospital, Trieste; 8) Gastroenterology and Digestive Endoscopy Unit “Villa Sofia” Hospital Palermo; 9) Gastroenterology, “Bolognini” Hospital, Seriate, Italy Abstract Different symptoms have been attributed to uncomplicated diverticular disease (DD). Poor absorbable antibiotics are largely used for uncomplicated DD, mainly for symptom treatment and prevention of diverticulitis onset. Controlled trials on cyclic administration of rifaximin in DD patients were evaluated. Four controlled, including 1 double-blind and 3 open-label, randomized studies were available. Following a long-term cyclic therapy, a significant difference emerged in the global symptoms score (range: 0-18) between rifaximin plus fibers (from 6-6.5 to 1-2) and fibers alone (from 6.7 to 2-3.8), although the actual clinically relevance of such a very small difference remains to be ascertained. Moreover, a similar global symptom score reduction (from 6 to 2.4) can be achieved by simply recommending an inexpensive high-fiber diet. Current data suggest that cyclic rifaximin plus fibers significantly reduce the incidence of the first episode of acute diverticulitis as compared to fibers alone (1.03% vs 2.75%), but a cost-efficacy analysis is needed before this treatment can be routinely recommended. The available studies have been hampered by some limitations, and definite conclusions could not be drawn. The cost of a long-life, cyclic rifaximin therapy administered to all symptomatic DD patients would appear prohibitive. Key words Diverticular disease – therapy – symptoms – rifaximin – diverticulitis – haemorrhage. Diverticular disease symptoms: a puzzling interpretation Diverticular disease (DD) is a very common condition in western countries, and its incidence has greately increased in the last decades. It is well known that DD prevalence rises with age, being relatively infrequent (5-10%) in subjects younger than 40 years and present in as many as 50-66% of people older than age 80 years [1]. Although DD remains asymptomatic in a large part of subjects, nearly 20% of patients develop some symptoms during their life-time [2]. Different symptoms have been attributed to uncomplicated DD, such as abdominal pain, bloating, and changes in bowel habit (constipation and/or diarrhoea) [2]. However, such a symptoms combination may be indistinguishable from that of the irritable bowel syndrome (IBS), a condition that is also highly prevalent in western populations [3, 4]. In addition, several alterations recognized as a possible cause of symptoms in the colon of DD patients are equally encountered in IBS. These include abnormal colonic motility, visceral hypersensitivity, low-grade inflammation, and increased circulating levels of either substance P or vasoactive intestinal polypeptide (VIP) [5, 6]. Currently, there is no reliable test to discriminate whether symptoms are actually caused by presence of diverticula in the colon or by an underlying IBS. On one hand, it has been proposed that gastrointestinal symptoms may precede the onset of DD in a proportion of subjects and, on the other hand, it is still unclear why up to 80% of cases of DD patients remain asymptomatic despite the presence of diverticula in their colon [7]. Such uncertainty is further increased by the observation that IBS prevalence has increased in elderly people in the last decades. Moreover, a recent population- based study found a significant association between the two conditions, the risk of DD being 9.4-fold increased (95% CI = 5.8-15.1) in patients >65 years with IBS as compared to age-matched control subjects without IBS [8]. Therefore, the overlap between IBS and DD may be expected to be

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Received: 26.06.2010 Accepted: 21.07.2010J Gastrointestin Liver DisSeptember 2010 Vol.19 No 3, 295-202Address for correspondence: Dr. Angelo Zullo Gastroenterologia ed Endoscopia Digestiva PTP Nuovo Regina Margherita Roma, Italy Email: [email protected]
Cyclic Antibiotic Therapy for Diverticular Disease: a Critical ReappraisalAngelo Zullo1, Cesare Hassan1, Giovanni Maconi2, Gianpiero Manes2, Gianfranco Tammaro3, Vincenzo De Francesco4, Bruno Annibale5, Leonardo Ficano6, Luigi Buri7, Giovanni Gatto8, Roberto Lorenzetti1, Salvatore M. Campo1, Enzo Ierardi4, Fabio Pace9, Sergio Morini1
1) Gastroenterology Unit, “Nuovo Regina Margherita” Hospital, Rome; 2) Dept. of Clinical Sciences, Division of Gastroenterology, “L. Sacco” University Hospital, Milan; 3) Gastroenterology Unit, “Sant’Eugenio” Hospital, Rome; 4) Section of Gastroenterology, Department of Medical Sciences, University of Foggia, Foggia; 5) Dept. of Digestive and Liver Diseases, University “La Sapienza”, Sant’Andrea Hospital Rome; 6) Department of Oncology, Division of General and Oncological Surgery, University of Palermo, Palermo; 7) Gastroenterology and Digestive Endoscopy Unit, “Cattinara’’ Hospital, Trieste; 8) Gastroenterology and Digestive Endoscopy Unit “Villa Sofia” Hospital Palermo; 9) Gastroenterology, “Bolognini” Hospital, Seriate, Italy
AbstractDifferent symptoms have been attributed to uncomplicated
diverticular disease (DD). Poor absorbable antibiotics are largely used for uncomplicated DD, mainly for symptom treatment and prevention of diverticulitis onset. Controlled trials on cyclic administration of rifaximin in DD patients were evaluated. Four controlled, including 1 double-blind and 3 open-label, randomized studies were available. Following a long-term cyclic therapy, a significant difference emerged in the global symptoms score (range: 0-18) between rifaximin plus fibers (from 6-6.5 to 1-2) and fibers alone (from 6.7 to 2-3.8), although the actual clinically relevance of such a very small difference remains to be ascertained. Moreover, a similar global symptom score reduction (from 6 to 2.4) can be achieved by simply recommending an inexpensive high-fiber diet. Current data suggest that cyclic rifaximin plus fibers significantly reduce the incidence of the first episode of acute diverticulitis as compared to fibers alone (1.03% vs 2.75%), but a cost-efficacy analysis is needed before this treatment can be routinely recommended. The available studies have been hampered by some limitations, and definite conclusions could not be drawn. The cost of a long-life, cyclic rifaximin therapy administered to all symptomatic DD patients would appear prohibitive.
Key words Diverticular disease – therapy – symptoms – rifaximin
– diverticulitis – haemorrhage.
Diverticular disease symptoms: a puzzling interpretation Diverticular disease (DD) is a very common condition in
western countries, and its incidence has greately increased in the last decades. It is well known that DD prevalence rises with age, being relatively infrequent (5-10%) in subjects younger than 40 years and present in as many as 50-66% of people older than age 80 years [1]. Although DD remains asymptomatic in a large part of subjects, nearly 20% of patients develop some symptoms during their life-time [2]. Different symptoms have been attributed to uncomplicated DD, such as abdominal pain, bloating, and changes in bowel habit (constipation and/or diarrhoea) [2]. However, such a symptoms combination may be indistinguishable from that of the irritable bowel syndrome (IBS), a condition that is also highly prevalent in western populations [3, 4]. In addition, several alterations recognized as a possible cause of symptoms in the colon of DD patients are equally encountered in IBS. These include abnormal colonic motility, visceral hypersensitivity, low-grade inflammation, and increased circulating levels of either substance P or vasoactive intestinal polypeptide (VIP) [5, 6]. Currently, there is no reliable test to discriminate whether symptoms are actually caused by presence of diverticula in the colon or by an underlying IBS. On one hand, it has been proposed that gastrointestinal symptoms may precede the onset of DD in a proportion of subjects and, on the other hand, it is still unclear why up to 80% of cases of DD patients remain asymptomatic despite the presence of diverticula in their colon [7]. Such uncertainty is further increased by the observation that IBS prevalence has increased in elderly people in the last decades. Moreover, a recent population-based study found a significant association between the two conditions, the risk of DD being 9.4-fold increased (95% CI = 5.8-15.1) in patients >65 years with IBS as compared to age-matched control subjects without IBS [8]. Therefore, the overlap between IBS and DD may be expected to be

296 Zullo et al
present in a large part of elderly patients complaining of abdominal symptoms. Finally, a possible role for small intestinal bacterial overgrowth (SIBO) on abdominal symptoms, particularly bloating, has been also suggested [9]. Indeed, SIBO could be detected in both DD and IBS patients, further acerbating the problem. Consequently, the question remains - what are we treating when a patient with diverticula complains of abdominal symptoms?
Antibiotic therapy in uncomplicated diverticular disease
Antibiotics are largely used for uncomplicated DD, mainly for symptoms treatment and prevention of diverticulitis onset [10]. The rationale of such an approach is based on the assumption that changes in gut microbiota could contribute to symptom development and onset of DD complications, although no specific bacteria have been identified as causing either abdominal symptoms or diverticulitis. Therefore, a scheduled cyclic therapy with antibiotics has been proposed in patients with DD. In order to avoid systemic effects, non-absorbable or poorly absorbable antibiotics with a proved efficacy on intestinal bacteria have been utilized. In the past, either neomycin and paramomycin have been used, but their long-term use is limited by ototoxicity and nephrotoxicity effects therapy have been reported [10]. More recently, rifaximin therapy has been proposed.
Rifaximin is a poorly-absorbable derivative of rifamycin with a broad-spectrum bactericidal activity – including anaerobes – which inhibit bacterial ribonucleic acid synthesis [11]. In contrast to aminoglycosides (neomycin and paramomycin), rifaximin possesses a good tolerability profile [10, 11]. Its use was firstly approved in Italy in 1987, and it is currently commercialized in over 30 countries with the following indications: gastrointestinal infections, travellers diarrhoea, hepatic encephalopathy, perioperative prophylaxis for gastrointestinal surgery, and small bowel intestinal overgrowth [12]. Rifaximin is also approved for treatment of uncomplicated DD in Austria, Georgia, Kazakhstan, Mexico, Moldavia, Russia, Slovak Republic, Tajikistan, Turkey, Turkmenistan, Uzbekistan and for acute, uncomplicated diverticulitis in Hungary, Spain, and Ukraine [12]. In Italy, such an antibiotic is commercialized - on a National Health System charge - but only for travellers diarrhoea, hepatic encephalopathy, and prophylaxis for gastrointestinal surgery; thus indication for DD is not allowed. However, the use of this drug in Italy has largely exceeded the approved indications. Indeed, it is widely used in clinical practice - not only by general practitioners but also by many gastroenterologists - for the treatment of symptomatic DD patients. In this setting, it is generally prescribed at a dose of 800 mg/day (2 tablets twice daily) for 5-7 days each month on a long-term basis.
What are the evidence-based data of controlled studies supporting such a therapeutic approach? In our search of the literature, we identified 4 controlled trials on the cyclic administration of rifaximin in DD patients, all carried
out in Italy, including 1 double-blind and 3 open-label, randomized studies [13-16]. In all these studies, patients with symptomatic, uncomplicated DD were randomized to receive rifaximin plus fiber or fiber supplementation alone. Unfortunately, no study compared rifaximin alone to identical placebo tablets in order to accurately detect its efficacy as a single therapy – i.e. the regimen largely used in clinical practice. Moreover, in none of these studies the score used for the symptoms score was previously validated. Data of a further controlled Italian study was not taken into account because the rifaximin plus fibers therapy was compared to mesalazine therapy instead of placebo or fibers alone [17].
In the single double-blind, placebo controlled study available [13], 168 patients were enrolled in 9 Italian centres and randomized (ratio 1:1) to receive either rifaximin (800 mg/day) plus glucomannan (2 g/day) or placebo (4 tablets/day) plus glucomannan (2 g/day), all given for 7 days every month. Clinical evaluation was performed at entry and at 3-month intervals for 12 months by using a questionnaire on the following symptoms: 1) upper abdominal pain/discomfort; 2) bloating; 3) lower abdominal pain/discomfort; 4) tenesmus; 5) diarrhoea; and 6) abdominal tenderness. Each symptom was graded using a simple score system as follows: 0 (absence), 1 (mild), 2 (moderate), and 3 (severe) symptoms (score range: 0-18). Overall, 151 patients were evaluated at 1 year, whilst 17 patients (9 in rifaximin plus fiber and 8 in placebo plus fiber group) were withdrawn. Both treatments equally reduced symptoms at 3 months. At 12-month follow-up, the global score decreased from the initial level of 6.5 to 2 in the rifaximin plus fiber and to 3 in the placebo plus fiber groups. Difference between the treatments was statistically significant starting from 6 months of therapy. In detail, among the 6 considered symptoms, a statistically significant difference emerged only for bloating (at 6 months), lower abdominal pain (at 9 months), and abdominal tenderness (at 12 months), whilst no significant modifications were observed for diarrhoea, upper abdominal pain, and tenesmus. At the end of follow-up, 68.9% (52/84, 61.9% at ITT analysis) of patients in the rifaximin plus fiber group were either symptom-free or mildly symptomatic (global score = 0-1), as compared to 39.5% (30/84, 35.7% at ITT analysis) in the placebo plus fiber group (P = 0.001). These results indicate that, when rifaximin is added to fiber supplementation the therapeutic response is increased from 39.5% to 68.9%, with an absolute therapeutic gain of 29.4% at PP analysis (26.2% at ITT analysis).
There are some limitations of this study that deserve to be mentioned. The first observation is that the success rate achieved in the placebo plus fiber arm (39.5%) in this study would appear quite similar to the 24-29.2% observed in other studies with fiber supplementation alone [14,16], quoting the placebo effect in DD patients as low as 10-15%. This would appear as an unexpectedly low result when dealing with functional symptoms, particularly by considering that the placebo effect in IBS was observed in up to 71.4% of patients with a population-weighted average of 40.2% [18].

Cyclic antibiotic therapy for diverticular disease 297
Moreover, it should be noted that the placebo was able to improve ulcerative colitis symptoms including rectal bleeding in up to 40-63.3% of cases and to induce clinical remission of active Crohn’s disease in up to 33% [19-21]. Another limitation is that at the 12-month follow-up, symptoms-free patients and those with mild symptoms were arbitrarily grouped together for statistical comparison between the two therapeutic arms. Therefore, it remains unclear how many patients really became asymptomatic following therapy, and whether a difference between the asymptomatic (score 0) and symptomatic (score 1) distribution between the two treatment groups did occur. This would be an important aspect, as the study emphasized that a significant difference in the global score was observed between the two therapies at 12 months, the final symptomatic score decreasing from the initial 6.5 to 3 following placebo plus fibres and to only 2 following rifaximin plus fibres. Why should the same 1 point score modification be considered clinically irrelevant from 0 to 1 - so that patients were cumulatively grouped - and clinically relevant from 2 to 3? Based on a global symptom score ranging from 0 to 18, a score of 3 would appear unlikely to be meaningfully different from a score of 2, since no inference of symptoms on quality of life was considered in this trial. Therefore, it remains uncertain how patients were really able to distinguish from a “mild” to a “moderate” bloating or the physician from a “mild” to a “moderate” abdominal tenderness. In addition, criteria for diarrhoea are lacking. Therefore, the qualitative score used for diarrhoea (i.e. mild or severe) would appear ambiguous, whilst the number of daily bowel movements would have appeared surely more objective. In addition, DD patients with diarrhoea, but not those with constipation, were enrolled, even if both therapeutic arms included fiber supplementation, which is generally indicated for treating constipation but not diarrhoea. Finally, data (number of patients enrolled, symptoms changes, etc.) observed in each participating centre was not declared, so that we remain unaware whether different results emerged in different centres, as well as whether a heterogeneity test before pooling data has been performed. In addition, the randomization procedure is not provided, and compliance to therapy has been not assessed.
In the largest, open-label trial currently available [14], consecutive patients with symptomatic, uncomplicated DD were initially enrolled in 16 Italian centres over 3 years. Patients were randomized (ratio 2:1) to receive either rifaximin 800 mg/day plus glucomannan 4 g/day (595 patients) or glucomannan 4 g/day (373 patients), all for 7 days a month. Clinical evaluation was performed at entry and at 4-month intervals for 12 months by using a questionnaire evaluating the same 6 symptoms of the previous study [13]. Each symptom was graded using a score system including 0 (no symptom), 1 (symptoms easily tolerated), 2 (symptoms sufficient to cause interference with normal activities), and 3 (inability to perform normal activities) symptoms (global score range: 0-18). Overall, 904 patients were evaluated at 1 year, whilst 64 patients (37 in the rifaximin plus fiber and 27
in the placebo plus fiber) withdrew due to either side-effects or DD complications. Both treatments equally reduced symptoms at 3 months. At 12-month follow-up, the global score decreased from the initial 6.5 to 1 in the rifaximin plus fiber group and from 6.3 to 2 in the fiber group. Difference between treatments was statistically significant starting from 4 months at both ITT and PP analyses. In contrast to the previous study [13], all the 6 considered symptoms (upper abdominal pain, lower abdominal pain, tenesmus, bloating, diarrhoea, and abdominal tenderness) improved with therapy. Rifaximin plus fiber achieved significantly better results than fiber alone. Moreover, 56.5% of patients in the rifaximin plus fiber group were symptom-free (global score = 0) as compared to 29.2% in the fiber group (P < 0.001), accounting for an absolute therapeutic gain of 27.3% at PP analysis.
Based on these data, it could be speculated that rifaximin alone would not be superior to fiber supplementation alone (27.3% vs 29.2%) in DD patients after a 1-year treatment, but it is surely more expensive. In this study, all the considered symptoms significantly improved following therapy, including upper abdominal pain, diarrhoea and tenesmus which remained unmodified in the double-blind trial [13]. However, based on the open-label design, this observation should be considered with caution. Although a clear definition of diarrhoea was not provided in this study, 44.4% and 38.1% of patients with diarrhoea at entry were treated with fibers plus rifaximin or fibers alone, respectively. The choice of this therapeutic approach would appear questionable, fiber supplementation being generally suitable for constipation. Therefore, a diarrhoea rate reduction from 38.1% to near 10% following fiber supplementation alone represents an unexpected finding deserving interpretation. Many limitations found in the previous trial are still present in this study [13]. In detail, the clinical relevance of a difference between a final symptom score of 1 (rifaximin plus fiber) and 2 (fiber alone) on a scale of 0-18 remains questionable, and opportune cost-efficacy aspects should be also considered. Finally, if results among the 16 participating centres are homogeneous before pooling, data is not declared.
In another open-label trial [15], 307 patients with symptomatic, uncomplicated DD were enrolled in 3 Italian centres. Patients were randomized (ratio 3:2) to receive either rifaximin 800 mg/day plus dietary fibers supplementation (at least 20 g/day) or dietary fibers supplementation (at least 20 g/day) alone, with rifaximin given for 7 days every month. Clinical evaluation was performed at entry and at 2-month intervals for 24 months by using a symptom questionnaire similar to that in the previous studies [13,14], with the exception of inclusion of upper abdominal pain evaluation. Symptoms were scored as in the other study [14], and the global score ranged from 0 to 15 (5 instead of 6 symptoms). Overall, 259 patients were evaluated at 24 months, whilst 48 patients (25 in rifaximin plus fibers and 23 in fibers groups) dropped out. Both treatments equally reduced symptoms at 2 months. At the 24-month follow-up, the global score decreased from the initial 6 to 1 in the rifaximin plus fibers and to 2.4 in the fibers group. The difference between

298 Zullo et al
treatments was statistically significant starting from 3 months of treatment. However, at 24 months, a significant difference in symptoms frequency between the two intervention groups was observed only for bloating (21.9% vs 40.3%; P <0.002) and abdominal tenderness (6.5% vs 21.2%; P <0.001), whilst no significant change occurred for lower abdominal pain (12.9% vs 19.2%; P = 0.05), tenesmus (3.9% vs 9.6%; P = 0.05), and diarrhoea (3.9% vs 2.9%; P = NS).
Besides the open-label design, a possible limitation is that dietary fiber supplementation was advised in both treatment arms, but it is unclear how the actual intake of at least 20 mg/day fibers - as well as compliance to rifaximin therapy - was controlled during a 24 month period. Similarly to the previously mentioned studies [13,14], patients with constipation were not included in this trial. Surprisingly, even in this study, a large number of patients (35.9% and 32.5% in the two arms) were asked to increase fiber intake, irrespective of presence of a diarrheic bowel habit. As in the previous study [14], a clear definition of diarrhoea was not provided, and fiber supplementation alone resulted in a marked reduction of diarrhoea, from 32.5% to 1.0% and 2.9% at 12 and 24-month follow-up. Once again, the clinical relevance of an adjunctive reduction of the global symptom score from 2.4 to 1 (in a range score of 0-15) achieved by adding rifaximin therapy to dietary fibers supplementation is questionable, and cost-effective considerations have to be taken into account dealing with a virtually long-life therapy. Unfortunately, the rate of symptom-free (global score = 0) patients in the two treatment groups is not clearly provided so that a comparison with a previous, similar study is unfeasible [14].
Finally, the first published study on such a topic [16] was a multicentre, open-label, pilot trial enrolling 217 DD patients randomized (ratio 1:1) to receive either rifaximin (800 mg/day) plus glucomannan (2 g/day) or placebo (4 tablets/day) plus glucomannan (2 g/day), all for 7 days every month. Overall, 8 symptoms were considered - i.e. the same 6 symptoms of other studies [13,14] plus low grade fever and chills and fever - with a global symptoms score ranging from 0 to 24. Although both treatments determined a clinical improvement, after 12 months the global symptoms score decreased from 6.46 to 1.8 in patients treated with glucomannan plus rifaximin and from 6.78 to 3.8 in those receiving glucomannan only (P < 0.001). Limitations already discussed for the other double-blind trial by the same authors are also applicable to this study which, in addition, was open-label [13].
As far as side-effects is concerned, data are lacking in 1 study [16], no side-effects were observed in another trial [13], whilst they ranged from 1.68% and 2.5% and from 1.34% and 3% following rifaximin plus fiber and fibers alone, respectively, including nausea, headache, and weakness [14, 15].
Rifaximin therapy for primary prevention of diverticulitis and other complications During a life-span period, nearly 20% of symptomatic
DD patients develop a complication, including acute diverticulitis and diverticular bleeding [3, 4]. In the majority of patients, acute diverticulitis presents as a single episode, but it may recur in nearly 20% of cases with a single or multiple episodes [22]. Moreover, some patients with diverticulitis may develop bowel perforation, obstruction, abscesses and fistulas [4]. Patients with uncomplicated diverticulitis generally present with acute pain in the left lower abdominal quadrant, fever, sometimes associated with a change in bowel habits or other symptoms such as anorexia, nausea, and vomiting [3,22]. Increased values of both blood white cells and ESR are usually detectable. An imaging study with CT or ultrasonography reveals inflammatory bowel wall thickening (> 5 mm) and peri-colic fat infiltration in the diverticular tract [23-25].
The importance of the imaging study has been highlighted in a study showing that a suspected diagnosis of acute diverticulitis only based on the clinical feature (abdominal pain and/or fever, and/or leukocytosis, and/or rebound tenderness) was excluded in as many as 57% of cases following CT study [23]. Therefore, acute uncomplicated diverticulitis may be suspected when prolonged (>24 hours) - presumed inflammatory - pain is present [26], but only when a compatible clinical feature together with fever >38° C, leukocytosis above 12,000 µL, and imaging signs of diverticulitis without complications (e.g., abscess, fistula, overt perforation) are present, as suggested in the literature [22-25]. The other major complication of DD is diverticular haemorrhage which generally presents as an sudden, painless bowel haemorrhage with the urge to defecate large volumes of blood or clots [3]. Providentially, the bleeding stop itself in near 80% of cases, but a recurrence occurs in 20-40% of cases, and a third episode occurs in further half of the patients [3]. Diagnosis includes angiography or scintigraphy, but colonoscopy with bowel preparation has been found to be accurate, also allowing endoscopic treatment in near 20% of cases [27]. Following a second diverticular haemorrhage episode a surgical approach is generally advised [3].
Can we prevent the onset of the first episode of acute diverticulitis and/or diverticular haemorrhage with cyclic, long-life, rifaximin therapy in symptomatic DD patients? Primary prevention of DD complications was specifically assessed in two prospective trials, in which cyclic therapy with rifaximin with fiber supplementation was compared to fibers alone for 12-24 months [14,15]. As reported in Table 1, an acute diverticulitis episode occurred in 1% and 2.9% (P = 0.0068) at 12 months and in 1.1% and 3.2% (P = 0.64) at 24 months following rifaximin plus fibers and fibers supplementation alone, respectively.
In the first study [14], acute diverticulitis was diagnosed based on clinical, laboratory, and radiological examination – although no clear criteria were disclosed as reported in other studies [23-25] – whilst in the other trial diverticulitis was not defined at all [15]. Moreover, no data on the management of the diverticulitis were provided, so that the actual severity of such a DD complication in the observed cases remains unclear. These observations suggest that the

Cyclic antibiotic therapy for diverticular disease 299
actual role of therapy in preventing diverticulitis should be addressed in future trials, accurately defining acute diverticulitis, including diverticulitis management (therapy, hospitalization, surgery, etc.), and possibly planning a therapeutic arm with only placebo aimed to assess how many acute diverticulitis cases would occur within 12–24 months without any treatment.
Data on the onset of acute diverticulitis during therapy were also reported in two further trials - although these aspects were not clear end-points of these studies [13,16]. In contrast to the open-label studies [14, 15], in the double-blind trial a 2.4% rate of diverticulitis at 12 months follow-up was reported without any difference between rifaximin plus fiber or placebo plus fiber therapy, although criteria for diagnosis of acute diverticulitis were not provided [13]. In another trial [16], diverticulitis requiring hospitalization was observed in 3 (2.7%) patients receiving glucomannan, whilst a recto-vaginal fistula requiring surgery occurred in 1 (0.9%) patient treated with rifaximin plus glucomannan. By pooling all available data [13-16], we calculated that diverticulitis occurred in 10 out of 970 patients receiving rifaximin plus fibers and in 19 out of 690 patients receiving fibers alone (1.03% vs 2.75%; P = 0.0083).
However, cost considerations should be also taken into account, before proposing rifaximin administration as a long-life cyclic therapy for a such a highly prevalent disease. Based on these data, we calculated that the number required to treat (NNT) to prevent 1 case of diverticulitis by adding rifaximin to fibers, is 58. In Italy, the cost of a 7-day/month cycle of 800 mg/day of rifaximin therapy for 12 months is 245.28 euros. Therefore, the cost is 14,226 euros to prevent 1 case of diverticulitis, in addition to the cost of fiber supplementation. Unfortunately, no data on diverticulitis management have been reported in 3 out 4 of these studies [13-15], so that we remain unaware if the 9 cases observed in these studies following rifaximin plus fiber therapy were simply treated with a systemic antibiotic and bowel rest or required hospitalization. Indeed, a direct cost comparison would allow the estimation of whether the cost of a short-term, systemic antibiotic therapy to only 9 patients was cheaper if compared to 14,226 euros of rifaximin therapy administered to 58 adjunctive patients to prevent 1 diverticulitis case. As reported in Fig. 1, we calculated that an adjunctive cost of more than 301 million euros every year should be spent in Italy by the National Health System by adding rifaximin therapy to fiber supplementation if all the estimated symptomatic patients with DD have to be treated to prevent diverticulitis. Obviously, such a huge cost also applies to rifaximin therapy aimed to simply treat symptoms attributed to DD. It is doubtful that our National Health System could sustain such an enormous cost every year simply to reduce bloating or abdominal pain to DD patients and, likely, these resources would be better employed for colorectal cancer management - from screening to therapy. Therefore, further well designed, controlled trials aimed to assess the actual benefits of rifaximin in the prevention of acute diverticultis are needed, before extending the indications of such a drug.
Concerning bleeding prevention, data showed no significant difference in bleeding episodes between DD patients treated with either rifaximin plus fibers or fibers alone (Table I). Surprisingly, in both studies ‘rectal bleeding’ episodes were recorded, but no definition was provided. Moreover, the source of bleeding was not ascertained in any case. Indeed, in one study [14], colonoscopy was repeated in the event of “rectal bleeding”, but the endoscopic findings were not provided, whilst in the other study [15], colonoscopy was not repeated at all when bleeding occurred. Therefore, we remain unaware whether a diverticular haemorrhage episode was the cause of the 6 rectal bleedings overall observed at 12-24 months follow-up [14,15]. In addition, the entity of bleeding is not provided as well as whether hospitalization, blood transfusion, endoscopic treatment, or surgery were required. Therefore, based on these data, no reliable clinical information is currently available on the possible role of rifaximin plus fiber therapy on diverticular haemorrhage prevention.
Fig 1. Therapeutic cost of rifaximin in Italy for symptomatic diverticular disease patients
Table I. Diverticular disease complications during therapy.
Study (reference) Latella et al (14) Colecchia et al. (15)
Rifaximin + fibers
Fibers Rifaximin + fibers
Fibers
Follow-up (months) 12 24
Patients 595 373 184 123
Diverticulitis (%) 6 (1.0) 11 (2.9)* 2 (1.1) 4 (3.2)
Rectal bleeding (%) 2 (0.3) 1 (0.26) 1 (0.5) 2 (1.6 )
*P <0.0068; no significant difference for the other comparisons.
Italian population on 2008(data from ISTAT)
>60 years old = 15,369 540 people
20% diverticular disease prevalence = 6,147 816 people
Rifaximin cost = 245.28 euros/year per patient
Overall: 301,587 212
Rationale for rifaximin use in diverticular disease patientsThe rationale for rifaximin use in DD is based on the
inhibitory effects of this drug on intestinal microbiota [10,11, 28]. This, in turn, may decrease intestinal gas production, hence reducing abdominal symptoms. However, there is little evidence for excessive gas production as a cause of bloating, gas distribution impairment most likely playing a major role as observed in IBS [29]. Gut flora is an extremely
300 Zullo et al
complex entity, including several bacterial species. Although intestinal microbiota is relatively stable over time, it may present wide inter-individual differences, also changing following several factors, including diet, bowel movements frequency, drugs. This enormous biological entity constantly produces gas in the colon, which is mainly reabsorbed or physiologically expelled. Although it is likely that during a 1-week rifaximin therapy both bacterial load and gas formation are reduced, it remain unclear how such a benefit could be maintained in the remaining 3 weeks without antibiotic treatment. Although rifaximin reduced faecal bacterial counts during oral intake, the effect is short-lasting since the bacterial population recovered within 1–2 weeks from the end of treatment [30]. A recent well-designed, double-blind, placebo-controlled, crossover study, showed that intestinal hydrogen production was significantly reduced during a 14 -16 day therapy with high-dose rifaximin (1200 mg/day) plus fibers, whilst it tended to increase following placebo plus fibers [31]. However, after a washout period, the H2 breath test values would appear similar to the initial levels (198 ± 134 vs 209 ± 153 H2 ppm). Moreover, a possible role for SIBO - detected in 36% of enrolled DD patients - rather than for colon flora has been highlighted in this study [31]. On the other hand, rifaximin therapy is administered to DD patients for diverticulitis prevention. However, the mechanism by which a 7 day/month cyclic therapy with rifaximin would prevent acute diverticulitis by reducing colonic bacterial load remains disputable. Indeed, gut flora is generally restored within a few days following an antibiotic therapy. Such a therapeutic approach may be regarded as implausible dental caries prevention by brushing the teeth only 7 days/month leaving bacteria to act in the remaining 21 days.
Another aspect of a long-life, cyclic administration of
rifaximin should be considered. Such a therapy is aimed to relief abdominal symptoms attributed to DD, but reliable data on the natural history of these symptoms are still lacking. Indeed, it is unclear whether all DD patients have symptoms every day for a long-term period. Therefore, a monthly rifaximin administration, indistinctly administered to all DD patients, would appear as a preventive treatment rather than a cure for actual symptoms. In other words, it may be compared to a long-life, 7-day/month analgesic administration to all osteoarthritis patients to prevent skeletal pain that could not recur at all or may appear only episodically.
Although rifaximin owns a excellent tolerability profile and it appears to be safe [10,11], it should be highlighted that studies on its carcinogenetic potential are lacking [10]. This could be a cause for concern when a cyclic, long-life therapy is administered to a vast number of subjects with a benign disease. Such a topic deserves further investigations, since a possible relationship between DD and colorectal cancer development has been observed in different studies [32].
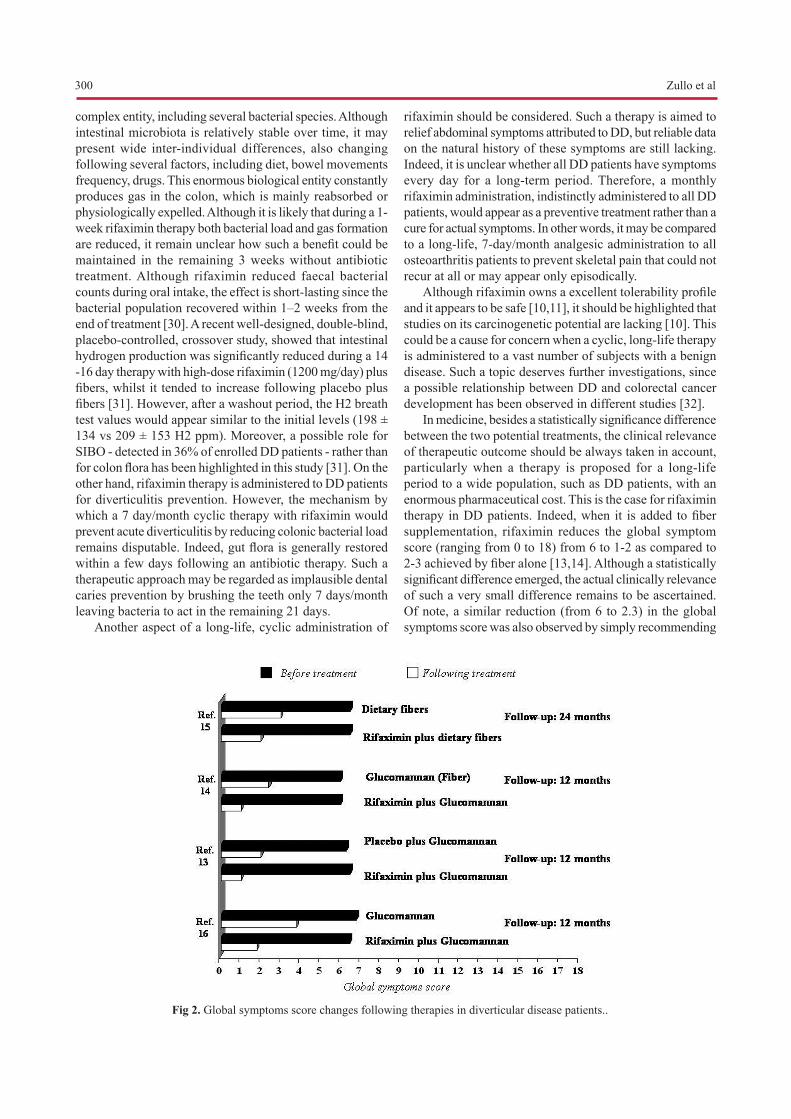
In medicine, besides a statistically significance difference between the two potential treatments, the clinical relevance of therapeutic outcome should be always taken in account, particularly when a therapy is proposed for a long-life period to a wide population, such as DD patients, with an enormous pharmaceutical cost. This is the case for rifaximin therapy in DD patients. Indeed, when it is added to fiber supplementation, rifaximin reduces the global symptom score (ranging from 0 to 18) from 6 to 1-2 as compared to 2-3 achieved by fiber alone [13,14]. Although a statistically significant difference emerged, the actual clinically relevance of such a very small difference remains to be ascertained. Of note, a similar reduction (from 6 to 2.3) in the global symptoms score was also observed by simply recommending
Fig 2. Global symptoms score changes following therapies in diverticular disease patients..

Cyclic antibiotic therapy for diverticular disease 301
a high dietary fiber intake (20 g/day) [15], suggesting that such a costless approach may achieve the same result of rifaximin or fiber supplementation in DD patients (Fig. 2). A recent study assessed the health-related Quality of Life (QoL) by using a SF-36 questionnaire in 58 symptomatic DD patients who were randomized to receive either rifaximin (200 mg or 400 mg b.i.d) or mesalazine (400 mg or 800 mg b.i.d) for 10 days/month together with high-fiber diet [33]. At 6 months, both treatments showed a significant improvement of both physical and mental performance. Unfortunately, this was not a double-blind, placebo-controlled study and, therefore, data should be interpreted with caution, dealing with completely subjective evaluations.
A timely evaluation of the actual role of rifaximin therapy in DD patients is now required and large, double-blind, placebo-controlled trials should be designed. Both symptom and bowel habit changes - recorded by using the Bristol stool scale [34] - should be recorded on daily basis, since recall of symptoms some months later is less accurate [35]. Patients should be classified according to different DD degrees (spastic colon diverticulosis, simple massed diverticulosis, right-sided diverticulosis, etc.) [36], and data analyzed accordingly. Criteria for DD complications (i.e. acute diverticulitis, diverticular haemorrhage) should be rigorously defined, and management of observed cases provided [37]. Moreover, a therapeutic arm with only a placebo - rather than fibres - should be included, to accurately evaluate the natural history of symptoms and complications in symptomatic DD patients. Finally, due to a possible overlapping between DD and IBS in the same patient as well as a possible response of IBS symptoms to rifaximin therapy [38], IBS patients should be also included.
While waiting for such trials, rifaximin therapy indistinctly prescribed to all DD patients would appear questionable.
Conflict of interest statementNone.
References 1. Martel J, Raskin JB. History, incidence, and epidemiology of
diverticulosis. J Clin Gastroenterol 2008; 42:1125–1127. 2. Colecchia A, Sandri L, Capodicasa S, et al. Diverticular disease of
the colon: new perspectives in symptom development and treatment. World J Gastroenterol 2003;9:1385-1389.
3. Stollman N, Raskin JB. Diverticular disease of the colon. Lancet 2004;363:631–639.
4. Sheth AA, Longo W, Floch MH. Diverticular disease and diverticulitis. Am J Gastroenterol 2008; 103:1550–1556.
5. Petruzziello L, Iacopini F, Bulajic M, Shah S, Costamanga G. Review article: uncomplicated diverticular disease of the colon. Aliment Pharmacol Ther 2006; 23:1379–1391.
6. Clemens CH, Samsom M, Roelofs J, van Berge Henegouwen GP, Smout AJ. Colorectal visceral perception in diverticular disease. Gut 2004;53: 717–722.
7. Otte JJ, Larsen L, Andersen JR. Irritable bowel syndrome and symptomatic diverticular disease – different diseases? Am J
Gastroenterol 1986;81:529–531. 8. Jung HK, Choung RS, Locke GR 3rd, Schleck CD, Zinsmeister
AR, Talley NJ. Diarrhea-predominant irritable bowel syndrome is associated with diverticular disease: a population-based study. Am J Gastroenterol 2010;105:652–661.
9. Pimentel M. Review of rifaximin as treatment for SIBO and IBS. Expert Opin Investig Drugs 2009;18:349–358.
10. Latella G, Scarpignato C. Rifaximin in the management of colonic diverticular disease. Expert Rev Gastroenterol Hepatol 2009;3:585–589.
11. Ojetti V, Lauritano EC, Barbaro F, et al. Rifaximin pharmacology and clinical implications. Expert Opin Drug Metab Toxicol 2009;5:675–682.
12. Koo HL, DuPont HL. Rifaximin: a unique gastrointestinal-selective antibiotic for enteric diseases. Curr Opin Gastroenterol 2010;26:17–25.
13. Papi C, Ciaco A, Koch M, Capurso L. Efficacy of rifaximin in the treatment of symptomatic diverticular disease of the colon. A multicentre double-blind placebo-controlled trial. Aliment Pharmacol Ther 1995;9:33–39.
14. Latella G, Pimpo MT, Sottili S, et al. Rifaximin improves symptoms of acquired uncomplicated diverticular disease of the colon. Int J Colorectal Dis 2003;18:55–62.
15. Colecchia A, Vestito A, Pasqui F, et al. Efficacy of long term cyclic administration of the poorly absorbed antibiotic Rifaximin in symptomatic, uncomplicated colonic diverticular disease. World J Gastroenterol 2007;13:264–269.
16. Papi C, Ciaco A, Koch M, Capurso L. Efficacy of rifaximin on symptoms of uncomplicated diverticular disease of the colon. A pilot multicentre open trial. Diverticular Disease Study Group. Ital J Gastroenterol 1992;24:452–456.
17. Comparato G, Fanigliulo L, Cavallaro LG, et al. Prevention of complications and symptomatic recurrences in diverticular disease with mesalazine: a 12-month follow-up. Dig Dis Sci 2007;52: 2934–2941.
18. Patel SM, Stason WB, Legedza A, et al. The placebo effect in irritable bowel syndrome trials: a meta-analysis. Neurogastroenterol Motil 2005;17:332-340.
19. Scherl EJ, Pruitt R, Gordon GL, et al. Safety and efficacy of a new 3.3 g b.i.d. tablet formulation in patients with mild-to-moderately-active ulcerative colitis: a multicenter, randomized, double-blind, placebo-controlled study. Am J Gastroenterol 2009;104:1452–1459.
20. Celasco G, Papa A, Jones R, et al. Clinical trial: oral colon-release parnaparin sodium tablets (CB-01-05 MMX) for active left-sided ulcerative colitis. Aliment Pharmacol Ther 2010;31:375–386.
21. Prantera C, Lochs H, Campieri M, et al. Antibiotic treatment of Crohn’s disease: results of a multicentre, double blind, randomized, placebo-controlled trial with rifaximin. Aliment Pharmacol Ther 2006;23:1117–1125.
22. Jacobs DO. Clinical practice. Diverticulitis. N Eng J Med 2007;357:2057–2066.
23. Rao PM, Rhea JT, Novelline RA, et al. Helical CT with only colonic contrast material for diagnosing diverticulitis: prospective evaluation of 150 patients. AJR Am J Roentgenol 1998;170:1445–1449.
24. Lahat A, Menachem Y, Avidan B, et al. Diverticulitis in the young patient: is it different? World J Gastroenterol 2006;12:2932–2935.
25. Lahat A, Yanai H, Sakhnini E, Menachem Y, Bar-Meir S. Role of colonoscopy in patients with persistent acute diverticulitis. World J Gastroenterol 2008;14:2763–2766.
26. Simpson J, Neal KR, Scholefield JH, Spiller RC. Patterns of pain in diverticular disease and the influence of acute diverticulitis. Eur J Gastroenterol Hepatol 2003;15:1005-1010.

302 Zullo et al
27. Jensen DM, Machicado GA, Jutabha R, Kovacs TO. Urgent colonoscopy for the diagnosis and treatment of severe diverticular hemorrhage. N Engl J Med 2000;342:78–82.
28. Tursi A. Diverticular disease: what is the best long-term treatment? Nat Rev Gastroenterol Hepatol 2010;7:77–78.
29. Agrawal A, Whorwell PJ. Review article: abdominal bloating and distension in functional gastrointestinal disorders – epidemiology and exploration of possible mechanisms. Aliment Pharmacol Ther 2008;27:2–10.
30. Scarpignato C, Pelosini I. Experimental and clinical pharmacology of rifaximin, a gastrointestinal selective antibiotic. Digestion 2006;73 (suppl 1):13–27.
31. D’Incà R, Pomerri F, Vettorato MG, et al. Interaction between rifaximin and dietary fibre in patients with diverticular disease. Aliment Pharmacol Ther 2007;25:771–779.
32. Morini S, Zullo A, Hassan C, Tomao S, Campo SM. Diverticulosis and colorectal cancer: between lights and shadows. J Clin Gastroenterol 2008;42:763–770.
33. Comparato G, Fanigliulo L, Aragona G, et al. Quality of life in uncomplicated symptomatic diverticular disease: is it another good reason for treatment? Dig Dis 2007;25:252–259.
34. Heaton KW, Radvan J, Cripps H, Mountford RA, Braddon FE, Hughes AO. Defecation frequency and timing, and stool form in the general population: a prospective study. Gut 1992;33:818–824.
35. Bellini M, Bove A, Sormani MP, et al. The daily diary and the questionnaire are not equivalent for the evaluation of bowel habits. Dig Liver Dis 2010; 42:99–102.
36. Almy TP, Howell DA. Medical progress. Diverticular disease of the colon. N Engl J Med 1980;302:324–331.
37. Szojda MM, Cuesta MA, Mulder CM, Felt-Bersma RJ. Review article: Management of diverticulitis. Aliment Pharmacol Ther 2007;26 (Suppl 2):67–76.
38. Pimentel M, Park S, Mirocha J, Kane SV, Kong Y. The effect of a nonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritable bowel syndrome: a randomized trial. Ann Intern Med 2006;145:557–563.
Related Documents