Dr. Veerabhadrudu. K MBBS, DNB Paediatrics--III

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr. Veerabhadrudu. K
MBBS, DNB Paediatrics--III

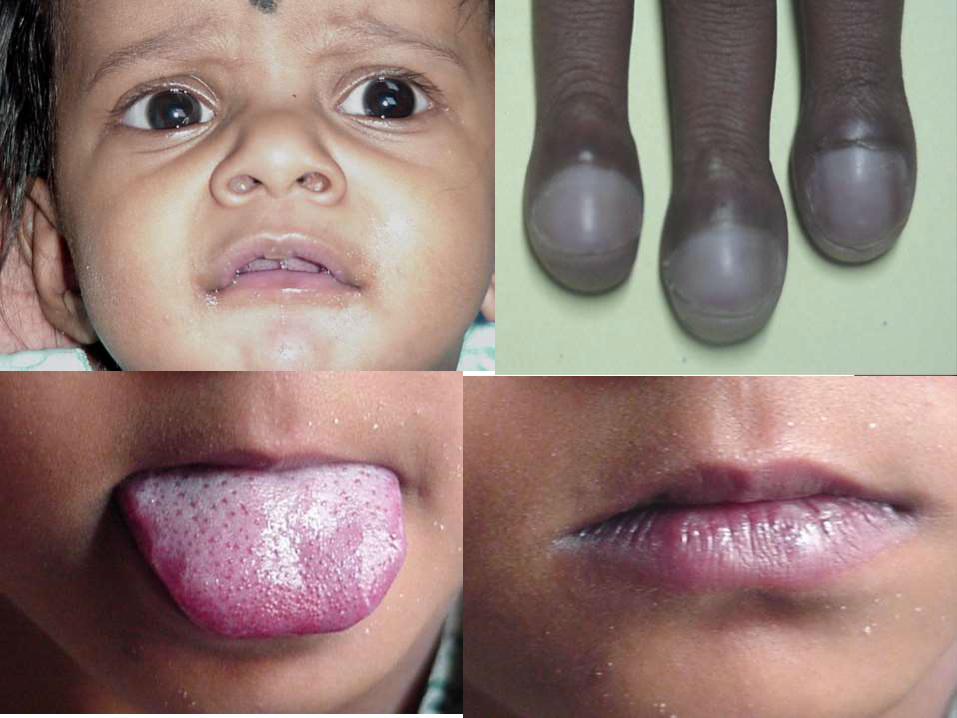
Cyanosis is a bluish or purplish tinge of the skin and mucous membranes.
Clinically detectable only when reduced Hb
is >5g% or saturation is <85%.
Cyanosis is recognized at a higher level of oxygen saturation in patients with polycythemia and at a lower level of oxygen saturation in patients with anemia.

Pulmonary RDS Pneumothorax Pneumonia MAS CDH TTNB PPHN
• CVS
– Cyanotic HD
• Pulm blood flow
• Pulm blood flow
• With CHF
– CHF alone
• CNS– Maternal
meds
– Asphyxia
– ICH
– NMD
• Metabolic– Hypoglycemia
– Adrenogenital syndrome
• Hematologic– Acute blood loss
– Chronic blood loss
– Polycythemia
– Methemoglobinemia
• Infectious– SEPSIS

Central – cyanotic CHD Peripheral – hypothermia, CCF Mixed Cyanosis – CHD in Shock
Differential cyanosis – PDA with reversal Reversed differential cyanosis – TGA with PDA
with reversal
Intermittent Cyanosis – Ebstein’s anomaly
Circum oral cyanosis
Cyclical cyanosis – Bilateral choanal atresia

Pseudo cyanosis : a bluish tinge to the skin and/or
mucous membranes that is not associated with
either hypoxemia or peripheral vasoconstriction.
Most causes are related to metals (e.g., silver
nitrate, silver iodide, silver, lead) or drugs (e.g.,
Phenothiazines, amiodarone, chloroquine
hydrochloride).

True Cyanosis
Associated with
clubbing
ABG - confirms
Cyanosis like
conditions
Not associated
with clubbing
Lab estimation of
Meth Hb and Sulph
Hb Confirms

Acrocyanosis Central cyanosis
Involves peripheries tongue, nail beds and
mucosal membranes
Peripheries Cold Warm
CRT Delayed Normal
Crying Decreases Increases
Part of normal
transition
May last upto 72 hrs

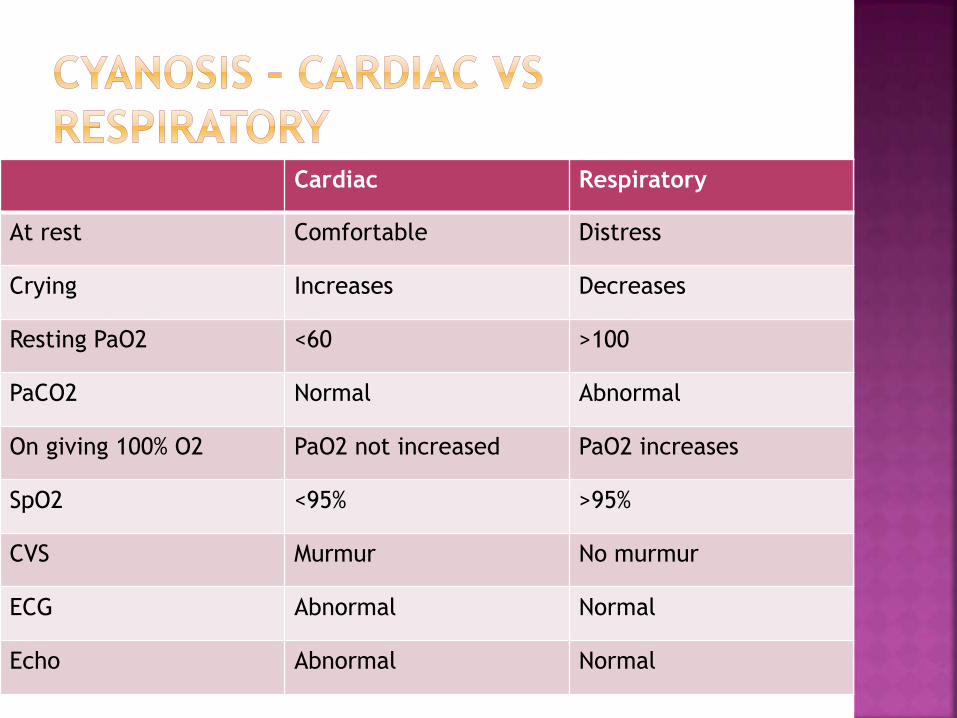
Cardiac Respiratory
At rest Comfortable Distress
Crying Increases Decreases
Resting PaO2 <60 >100
PaCO2 Normal Abnormal
On giving 100% O2 PaO2 not increased PaO2 increases
SpO2 <95% >95%
CVS Murmur No murmur
ECG Abnormal Normal
Echo Abnormal Normal
Most sensitive and specific tool for
evaluation of a neonate with suspected CHD
especially in the absence of ECHO.
Helps to differentiate the cardiac and non
cardiac causes of cyanosis.
Pulse oximetry is not reliable, but in resource limited settings, it can be used.
Both pre and post ductal sites are used.
Rt radial ABG in air after administration
of 100% O2 for 5-10min.

Rt radial ABG in air after 10 min 100% O2
paO2 > 250mmHg - excludes CCHD
paO2 > 150 to 250 - CCHD unlikely (mixing lesions)
paO2 < 150 - CCHD likely (shunting lesions)
< 150 mmHg most likely duct dependent lesions, so PGE1 can be started until anatomic lesion is defined
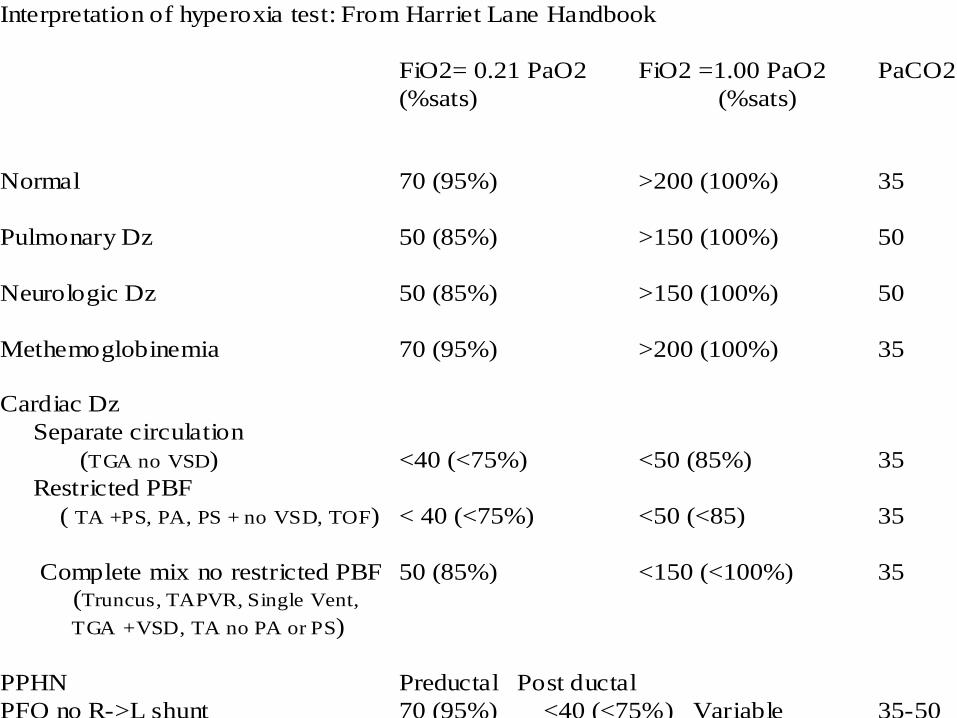
Interpretation of hyperoxia test: From Harriet Lane Handbook
FiO2= 0.21 PaO2 FiO2 =1.00 PaO2 PaCO2
(%sats) (%sats)
Normal 70 (95%) >200 (100%) 35
Pulmonary Dz 50 (85%) >150 (100%) 50
Neurologic Dz 50 (85%) >150 (100%) 50
Methemoglobinemia 70 (95%) >200 (100%) 35
Cardiac Dz
Separate circulation
(TGA no VSD) <40 (<75%) <50 (85%) 35
Restricted PBF
( TA +PS, PA, PS + no VSD, TOF) < 40 (<75%) <50 (<85) 35
Complete mix no restricted PBF 50 (85%) <150 (<100%) 35 (Truncus, TAPVR, Single Vent,
TGA +VSD, TA no PA or PS)
PPHN Preductal Post ductal
PFO no R->L shunt 70 (95%) <40 (<75%) Variable 35-50
PFO + R->L shunt <40 (<75%) <40 (75%) Variable 35-50

Clubbing
Cyanotic spell
Depressed IQ
Infective endocarditis
Polycythemia
Embolic phenomenon
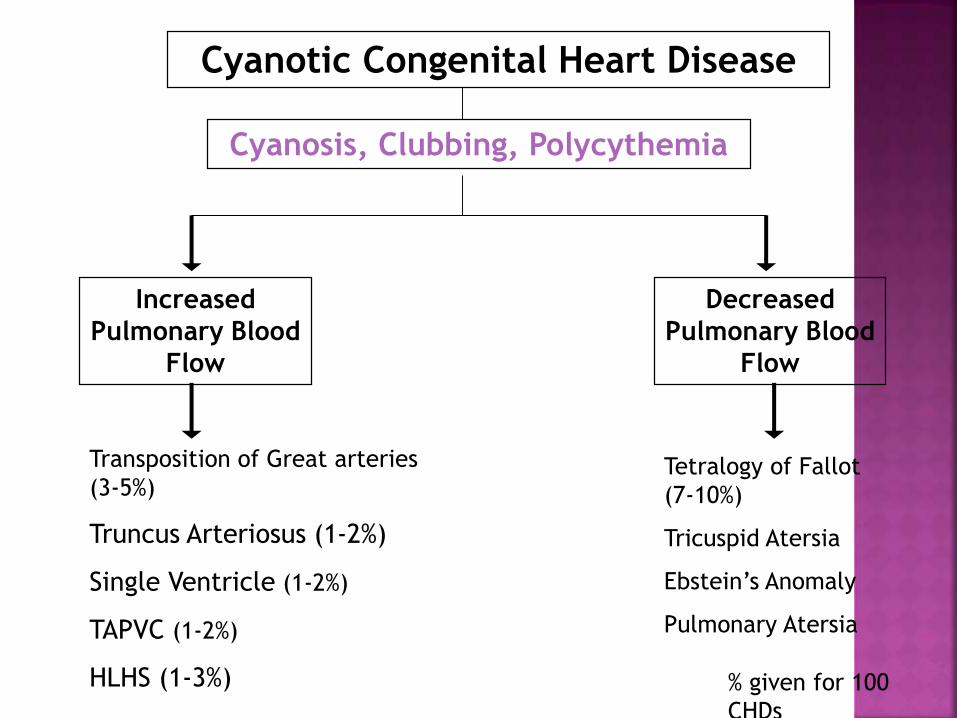
Cyanotic Congenital Heart Disease
Increased
Pulmonary Blood
Flow
Cyanosis, Clubbing, Polycythemia
Decreased
Pulmonary Blood
Flow
Transposition of Great arteries
(3-5%)
Truncus Arteriosus (1-2%)
Single Ventricle (1-2%)
TAPVC (1-2%)
HLHS (1-3%)
Tetralogy of Fallot
(7-10%)
Tricuspid Atersia
Ebstein’s Anomaly
Pulmonary Atersia
% given for 100
CHDs

Clinical sub types:
Tetrology of Fallot
Tricuspid atresia with PS
DORV with VSD and PS
Single ventricle with PS
TGA and VSD with PS
AVSD with PS


In 1888, Fallot described the anatomy of TOF
Incidence 7-10 % of all forms of congenital
heart disease
The most common cardiac malformation
responsible for cyanosis after 1 year of age.
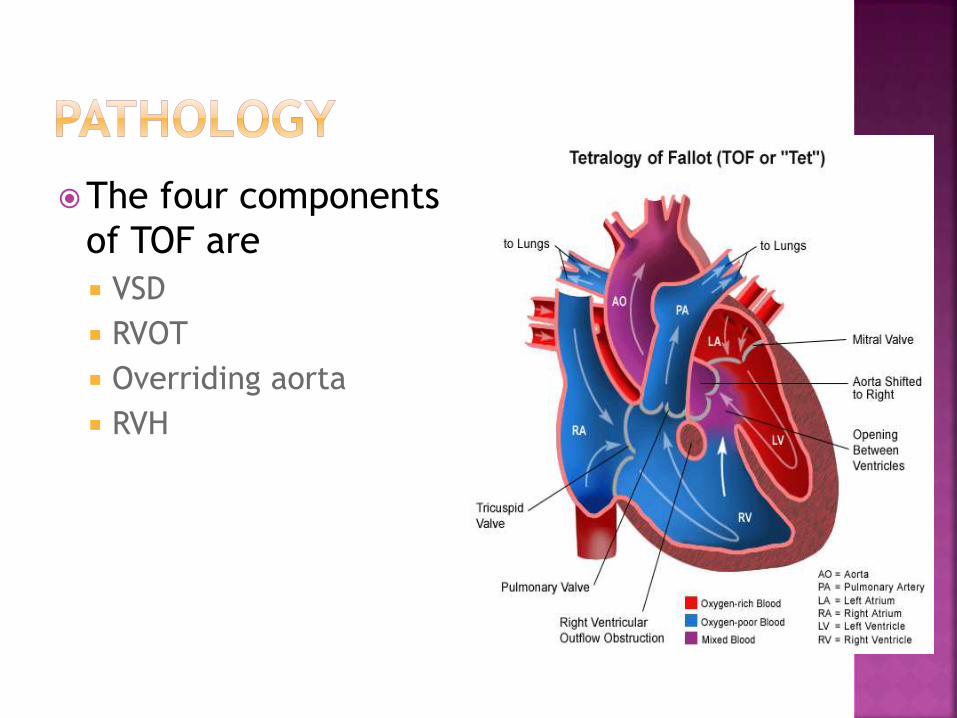
The four components
of TOF are
VSD
RVOT
Overriding aorta
RVH

Only two abnormalities are required A VSD large enough to equalize pressures in both
ventricles
A right ventricular outflow tact obstruction
RVH is secondary to right ventricular outflow tract obstruction (RVOT) and VSD
Over riding of aorta varies
VSD is perimembranous defect with extension into the subpulmonary region
VSD is non restrictive and large

RVOT obstruction can be in the form of
Infundibular stenosis - 45%
Pulmonary valve stenosis - 10%
Combination - 30%
Pulmonary atresia - 15%

Pulmonary annulus and MPA are hypoplastic
Right aortic arch in 25% of TOF
Abnormal coronary arteries in about 5% of
TOF patients

Enlarged, overriding aorta and hypoplasia of
pulmonary flow results from septation of the
conus and truncus arteriosus with anterior
deviation of the conus into the RV outflow
Experimental lesions in specific loci of
ectodermal tissue that migrate to the conus
can reproduce the defects seen in TOF

* PS increased RV
pressure, RVH
*pressures in both RV&LV ---
EQUAL
*RT LT shunt occurs
*flow across PS results in ESM
*the more severe the PS the
more the
RT LT shunt, so, more
cyanosis.
HAEMODYNAMICS:
Appearance of cyanosis
After neonatal period
Exception TOF with Pulmonary atresia
Hypoxemic Spells
Low birth weight or development delay or
easy fatigability
Cyanosis
Clubbing
Polycythemia
Squatting position
Tachypnea


Increased activity
Increased respiration
Increased venous return
Fixed pulmonary blood flow
Increased (RV) to (LV) shunt
Increased cyanosis

Decreased venous return
Increased systemic vascular resistance
Increased pulmonary blood flow
Decreased cyanosis
Squating Equivalent – Knee Chest position,
child sitting with flexed limbs, mother
carrying the child with folded limbs and
others

RV tap in left sternal borderSystolic thrill in upper and mid left
sternal bordersEjection click which originates from aortaS2 is single due to absent pulmonary
component A loud ejection type systolic murmur
heard at the mid and upper left sternal border
This murmur originates from the Pulmonary stenosis and may be confused with the pansystolic murmur of VSD

Intensity of the murmur depends of the severity of RVOT obstruction
More severe the obstruction, shorter and softer murmur will be heard
In Pulmonary atresia, murmur is either absent or very soft
Auscultation of back is important to find the presence of MAPCAs ( Major AortoPulmonary Collateral Arteries)
Acyanotic or pink TOF – RVOT obstruction is mild, so clinical picture resembles VSD
Pentalogy of Fallot – TOF with ASD
Tetralogy of Fallot with Pulmonary atresia
Tetralogy of Fallot with Absent Pulmonary Valve
Tetralogy of Fallot with absence of branch pulmonary artery

Fetal hydantoin syndrome
Fetal carbamazepine syndrome
Fetal alcohol syndrome
Maternal phenylketonuria (PKU)
CATCH 22 – Cardiac defects, abnormal facies,
thymic hypoplasia, cleft palate,
hypocalcemia
Anemia
Infective Endocarditis
Valvular Regurgitation
Surgically created or naturally occurring
large left to right shunts
Systemic hypertension
Unrelated or coincidental myocardial disease

Hematology Polycythemia secondary to cyanosis (hematocrit
>65%)
Anemia – due to relative iron deficiency
Electrocardiography
X-ray
Echocardiography
Angiogram
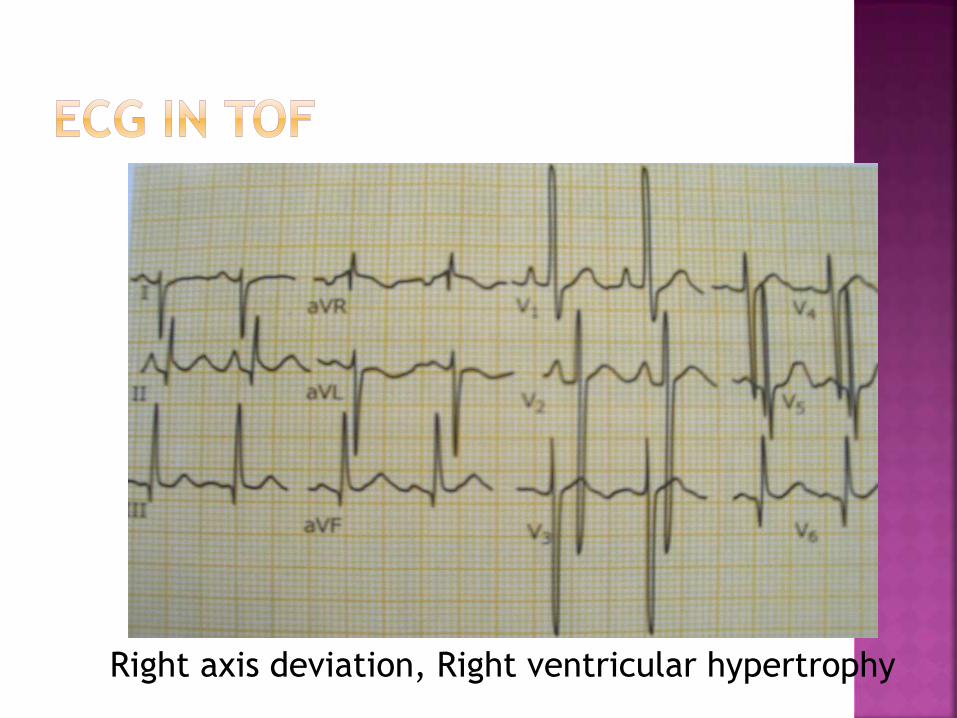
Right axis deviation, Right ventricular hypertrophy
Normal size heart
Pulmonary vascular markings are decreased
Concave main pulmonary artery segment with an
upturned apex – BOOT shaped heart or coeur en
sabot
Right atrial enlargement (25%)
Right aortic arch (25%)

Typical - Fallot CXR
Pulmonary bay
RV apex
Pulmonary
oligaemia

TOF-boot ,no cardiomegaly, oligaemia

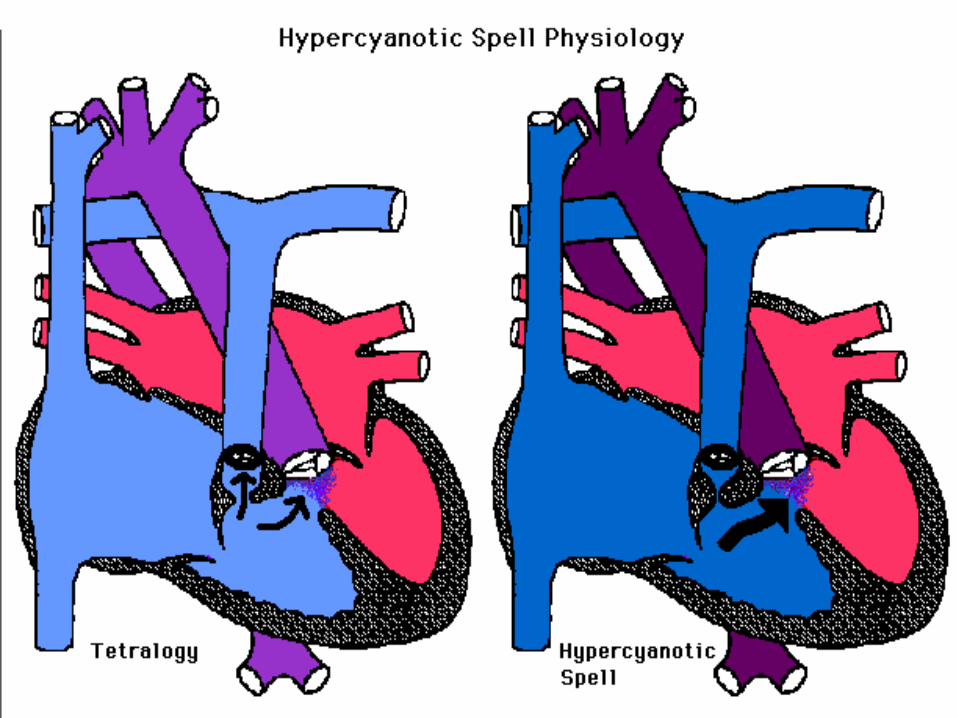
Hyper cyanotic or Tet or cyanotic or hypoxic spell
Peak incidence 2 - 4 months
Usually occurs in morning after crying, feeding or defecation
Severe spell may lead to limpness, convulsions, CVA or even death

Secondary to infundibular spasm and/or
decreased SVR with increased right-to-left
shunting at the VSD, resulting in diminished
pulmonary blood flow

Spasm of decrease SVR crying/feeding/defaecation
RVOT
Increase R…..L shunting
Increase systemic venous return DecreaseO2 Increase CO2 Decrease pH
Tachypneea

Sudden onset of cyanosis or deepening of
cyanosis
Sudden onset of dyspnea
Alterations in consciousness, encompassing a
spectrum from irritability to syncope
Decrease in intensity or even disappearance
of systolic murmur

Central cyanosis & anoxic spell (hyper cyanotic):

Knee chest position or squatting –decreases systemic venous return and increases systemic vascular resistance at femoral arteries
Morphine sulphate – 0.1 - 0.2mg/kg sc or im, suppresses the respiratory centre and abolishes hyperpnoea
Oxygen has little effect of arterial oxygen saturation
Acidosis should be treated with sodium bicarbonate 1mEq/kg administered intravenously
Preceding treatment, patient becomes less cyanotic, and heart murmur become louder
Indicates increased amount of blood flowing through stenotic right ventricular outflow tract
If Hypoxemic spell not fully respond Vasoconstrictor: Phenylephrine 0.02 mg/kg IV
Propranolol 0.01 to 0.25 mg/kg slow IV push, reduces the heart rate and may reverse the spell
Ketamine 1 – 3 mg/kg over 60 secs, increases systemic vascular resistance and sedates the patient

Prevention of Hypoxemic spell Oral Propranolol 0.5 to 1.5 mg/kg every 6 hours
Relative IDA should be detected and treated since anemic children are more susceptible to CVA
Maintenance of good dental hygiene and infective endocarditis prophylaxis
Hct has to maintained <65%, Phlebotomy may be needed to manage polycythemia

Neonates with TOF and pulmonary atresia
Infants with hypoplastic pulmonary annulus, which requires a transannular patch for complete repair
Children with hypoplastic pulmonary arteries
Severely cyanotic infants younger than 3 months of age
Infants younger than 3 to 4 months old who have medically unmanageable hypoxic spells
Systemic – Pulmonary Shunt
Blalock-Taussig: between subclavian artery and ipsilateral PA, preformed in infants older than 3 months
Gore-Tex Interposition shunt (modified BT): between subclavian and ipsilateral PA, done even in small infants younger than 3 months
Waterston: between ascending aorta right PA, no longer performed
Potts: between descending aorta and left PA, no longer performed


Symptomatic infants with favourable anatomy of the RVOT and PA
Asymptomatic and minimally cyanotic children may have repair between 3 and 24 months depending on the degree of annular and PA hypoplasia
Mildly cyanotic who had previous shunt surgery may have total repair 1 to 2 years after shunt operation
Asymptomatic and acyanotic children have the operation at 1 to 2 years of age
Asymptomatic children with coronary artery anomalies may have repair at 3 to 4 years of age

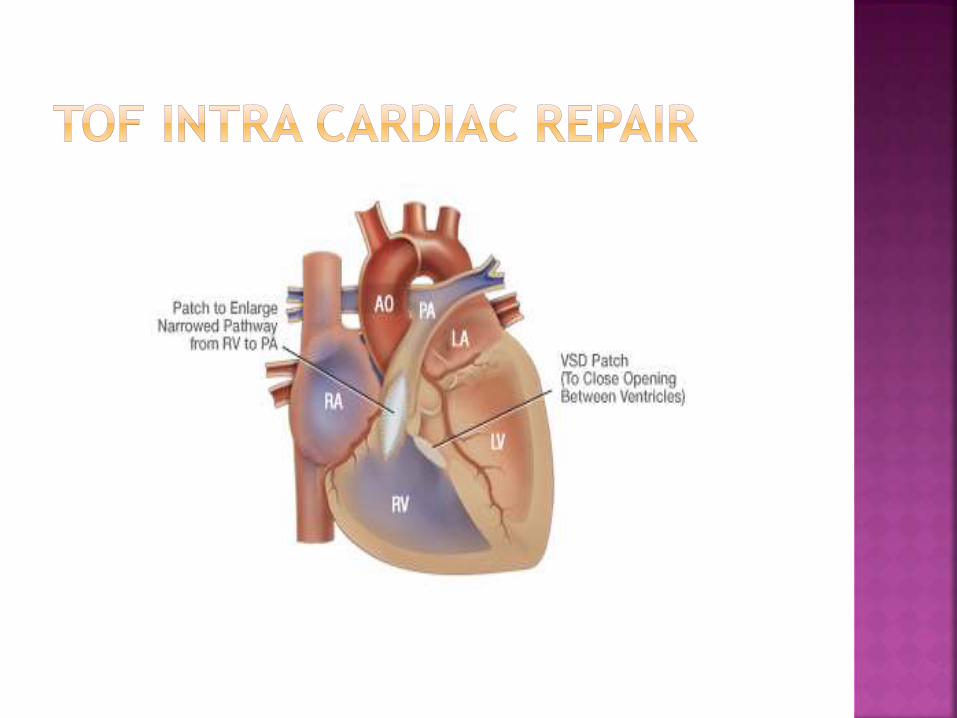
Patch closure of VSD
Widening of RVOT by resection of the
infundibular tissue and placement of a fabric
patch
Takedown of prior shunt (if done)

Congestive heart failure (right or left),
residual outflow obstruction, VSD, and/or
pulmonic regurgitation
Atrial flutter, ventricular arrhythmias, RBBB,
or left anterior hemiblock
Infective endocarditis

Erythrocytosis
Brain abscess
Acute gouty arthritis
Infective endocarditis
Cerebrovascular thrombosis
Delayed puberty
Scoliosis

Pulmonary Atresia
- With VSD - Extreme form of TOF
- Without VSD - No egress of blood from Rt vent.
- Shunt through foramen ovale to Lt atrium
Left ventricle
systemic circulation
Aorta
pulmonic circulation
- Hypoplastic right ventricle (PDA)
61

62

Clinical Manifestation- Cyanosis at birth- Respiratory distress- Single 2nd heart sound- No murmur
Diagnosis- CXR - concave pulmonary artery segment
and apex tilted upward- ECG- Echocardiography
Treatment - PGE1
- Surgery
63

PA with IVS – LAD with RAE and LVH
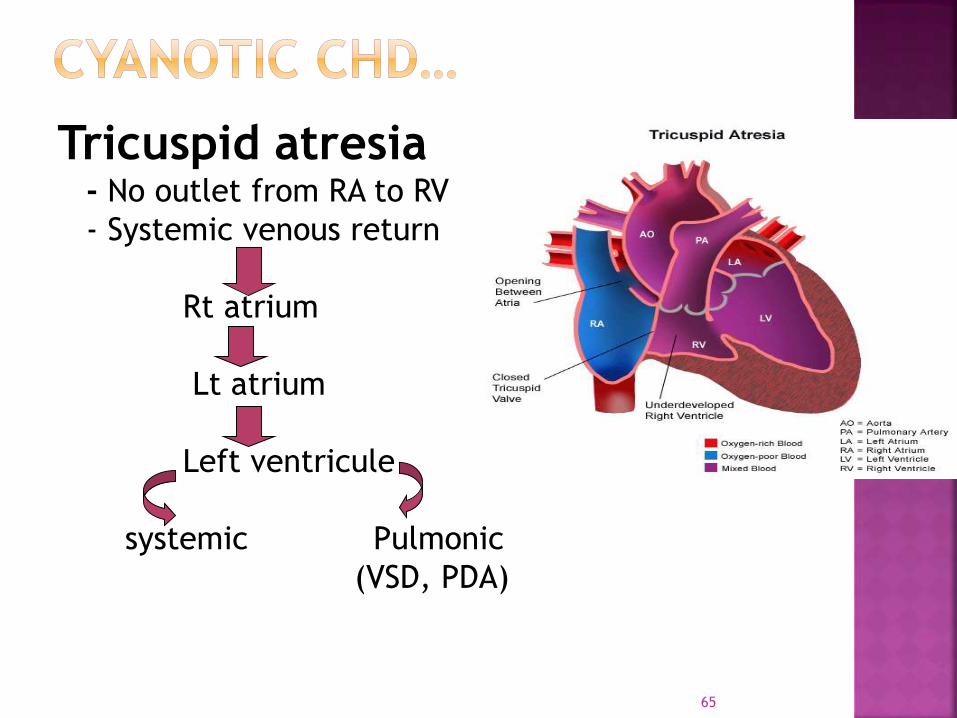
Tricuspid atresia- No outlet from RA to RV
- Systemic venous return
Rt atrium
Lt atrium
Left ventricule
systemic Pulmonic
(VSD, PDA)
65

66
Clinical Manifestation
- Cyanosis at birth
- Polycythemia
- Easily fatiguability
- Exertional dyspnea
Diagnosis
- CXR
- ECG – “superior” QRS axis with RAE and LVH
- Echocardiography
67
Pulmonary vascularity reduced.
Pulmonary artery segment – inconspicuous.
Heart size – normal.
LAO – Humped appearance of right cardiac
border and a prominent left cardiac
silhouette
Inferior border – flat or receding owing to
absence of RV.


TA - ECG – “superior” QRS axis with RAE and LVH
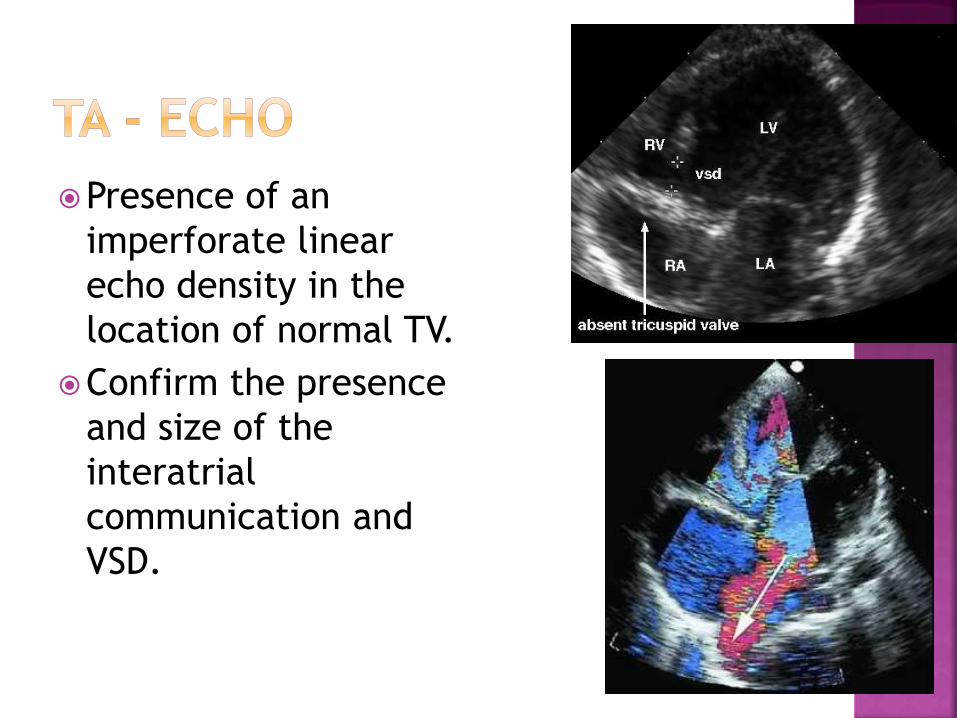
Presence of an
imperforate linear
echo density in the
location of normal TV.
Confirm the presence
and size of the
interatrial
communication and
VSD.

Limited role at present.
Therapeutic role for balloon atrial
septostomy.
Prior to a Fontan procedure for determining
pulmonary vascular resistance.

- PGE1, balloon atrial septostomy
- Surgery - Aortico - pulmonary Shunt
- Bidirectional Glenn shunt
- Modified Fontan operation
73

Displacement of abnormal tricuspid valve into right ventricle
Anterior cusp retains some attachment to the valve ring
Other leaflets are adherent to the valve of the right ventricle
Right atrium is huge -Atrialisation of Right Ventricle
Tricuspid valve is regurgitant

Clinical Manifestations- Easly fatiguability- Intermittent Cyanosis- Dysrhythmia- Rt to Lt shunt through formen ovale- Holosystolic Murmur at tricuspid area- Heart failure
- Multiple Clicks
Diagnosis- CXR - box shaped heart- ECG - Right BBB
- Superior axis deviationTreatment
- PGE1
- Surgery
75

Ebstein’s anomaly –BOX -heart
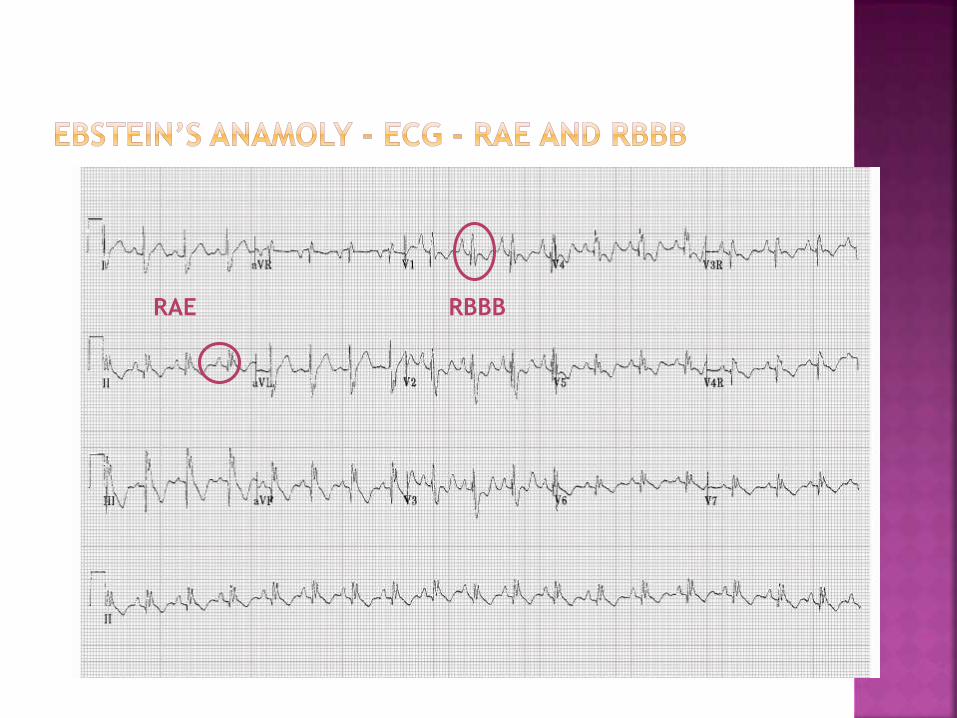
RBBBRAE

Ebstein’s with WPW Syndrome


TGA with VSD and PS; single ventricle with PS or
DORV with PS will have TOF picture

Thank you…
Related Documents











