CVD Mortality in Brazil: SOCESP/SBC/IDPC/HAOC Proposal for Effective Reduction Álvaro Avezum, MD, PhD, FESC, FACC São Paulo, Brazil Director, Research Division, Dante Pazzanese Institute of Cardiology Professor, São Paulo University International Associate Researcher, PHRI, McMaster University, Canada Health Systems Research Workshop MRC and CONFAP Brasilia June 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CVD Mortality in Brazil:SOCESP/SBC/IDPC/HAOC Proposal
for Effective Reduction
Álvaro Avezum, MD, PhD, FESC, FACC
São Paulo, Brazil
Director, Research Division, Dante Pazzanese Institute of Cardiology
Professor, São Paulo University
International Associate Researcher, PHRI, McMaster University, Canada
Health Systems Research Workshop MRC and CONFAP
Brasilia June 2017

AGENDA
– Scope of the problem and Brazilian CVD landscape
(the real challenge)
– SOCESP/SB/C/IDPC/HAOC Roadmaps
(focus on Health System Component)
– Coalition for CVD mortality reduction
(Saving lives and generating relevant knowledge)
The Team
Alvaro Avezum (IDPC)
SOCESP/SBC
HAOC (Jefferson Fernandes)
LSH - UK (Pablo Perel)
PHRI – Canada (Salim Yusuf)
WHF - Geneve (David Wood)
Brazilian Cardiovascular Network
Primary Care Units (Family Health Strategy)

Milestones
From EMERAS to COMPASS (60 RCTs – 28 yr)
From OASIS-Registry to PURE (20 Epi-Studies)
Key relevant areas in CVD research (AMI, ACS, HF, AF,
1ary & 2ary CV prevention, DM, Obesity, PCI, CABG, etc)
Consolidated Research Network (300 hospitals: in- and
outpatient research + 700 private offices + 500 PCUs)
Beyond Institutional borders
Publication policy – always focusing on high-impact journals
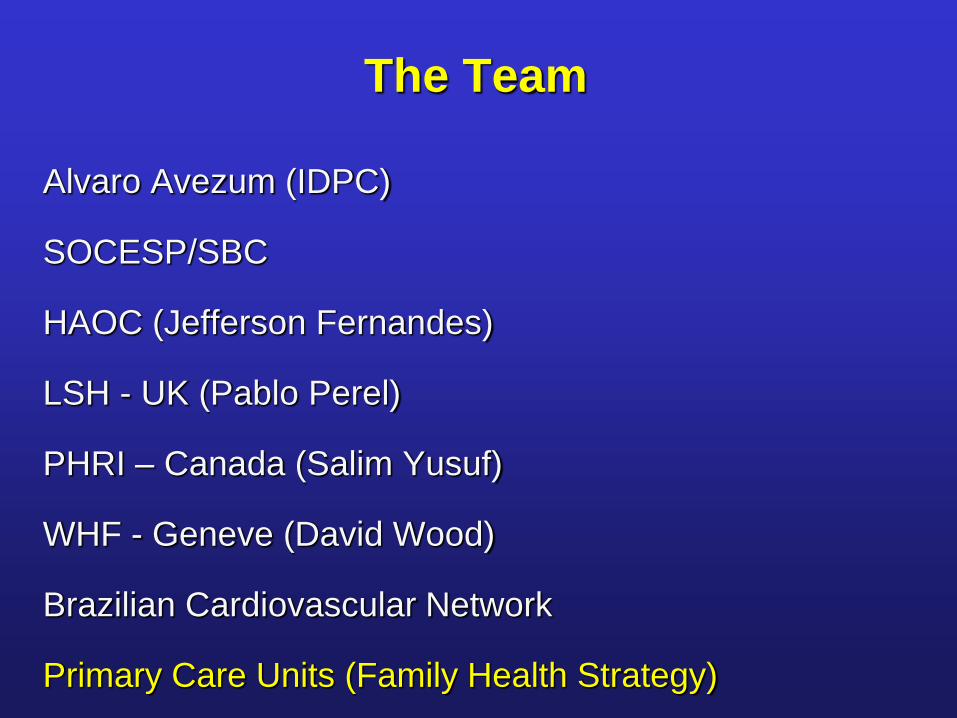
BRAZIL: MI Mortality CoefficientRelative Variation - 2003/2012
Colombo F, Magalhaes C, Gagliardi S, Avezum A. Submitted 2016
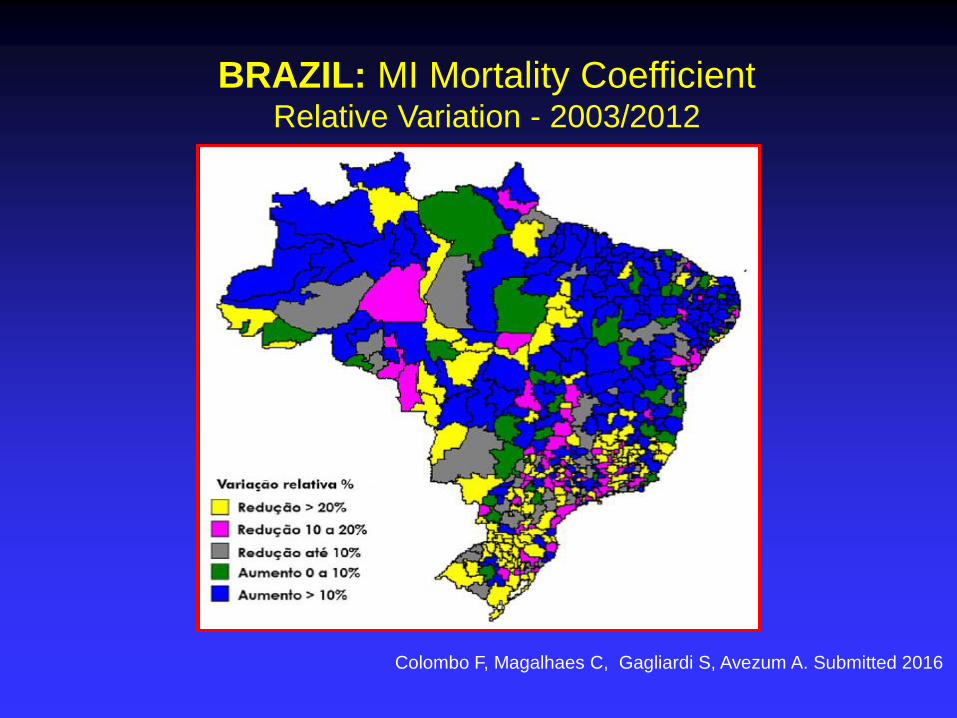
Força da Associação e Impacto Clínico do risco
de IAM na América do Sul, por países
Lanas F, Avezum A, Bautista L, Yusuf S, et al. Circulation 2007;115:1067-1074

ESTUDO INTERSTROKE: FATORES DE RISCO PARA
TODOS OS TIPOS DE AVC (TODAS REGIÕES)
Overall PAR 90.2% (88.0-92.1)
0.25 0.5 1 2 4 8
Odds ratio (99% CI)
Risk Factor Control(%) Ischemic(%) ICH(%) OR(99% CI) PAR(99% CI)
ApoB/ApoA1 (T3 vs T1)
Cardiac Causes
Psychosocial
High Alcohol Intake
Diabetes Mellitus
Physical Activity
modified AHEI (T3 vs T1)
Waist-to-Hip Ratio (T3 vs T1)
Current Smoker
Hypertension
33.0
5.0
2.5
22.0
16.3
33.0
32.9
22.4
47.4
46.4
16.8
5.3
30.7
11.1
28.9
42.0
30.6
72.0
38.0
4.4
4.3
19.2
7.9
24.2
35.0
29.3
74.8
1.84(1.65 to 2.06)
3.17(2.68 to 3.75)
2.20(1.78 to 2.72)
2.09(1.64 to 2.67)
1.16(1.05 to 1.30)
0.60(0.52 to 0.70)
0.60(0.53 to 0.67)
1.44(1.27 to 1.64)
1.67(1.49 to 1.87)
2.98(2.72 to 3.28)
26.8(22.2 to 31.9)
9.1(8.0 to 10.2)
17.4(13.1 to 22.6)
5.8(3.4 to 9.7)
3.9(1.9 to 7.6)
35.8(27.7 to 44.7)
23.2(18.2 to 28.9)
18.6(13.3 to 25.3)
12.4(10.2 to 14.9)
47.9(45.1 to 50.6)
Overall PAR 90.7% (88.7 to 92.4)
O´Donnel M,….Avezum A, ….Yusuf S. Lancet 2016, in press

Hypertension Control accross HIC/MIC/LIC – PURE Study
25
32
27
8
3943
37
12
4951
47
15
0
10
20
30
40
50
60
Hipertension HT aware HT treated HT controlled
no risk factor ≥1 risk factor ≥2 risk factors
Risk factors: diabetes, smoking, obesity, male and age>65 anos
Chow CK, Teo KK,…Avezum A,…Yusuf S, PURE Study Investigators. JAMA 2013;310:959-68

% receiving proven medications in CAD (154,000 people from 17 countries: PURE Prospective Study)
0
10
20
30
40
50
60
70
80
90
100
Overall HIC UMIC LMIC LIC
0 1 2 3 4
5593 671 1338 2879
Yusuf S, Rangarajan S, Avezum A, et al. The Lancet, August 28, 2011

Proportion of medication use in individuals
with CHD by countries in South America
Avezum A, ..., Yusuf S. Global Heart 2016, Oct 20
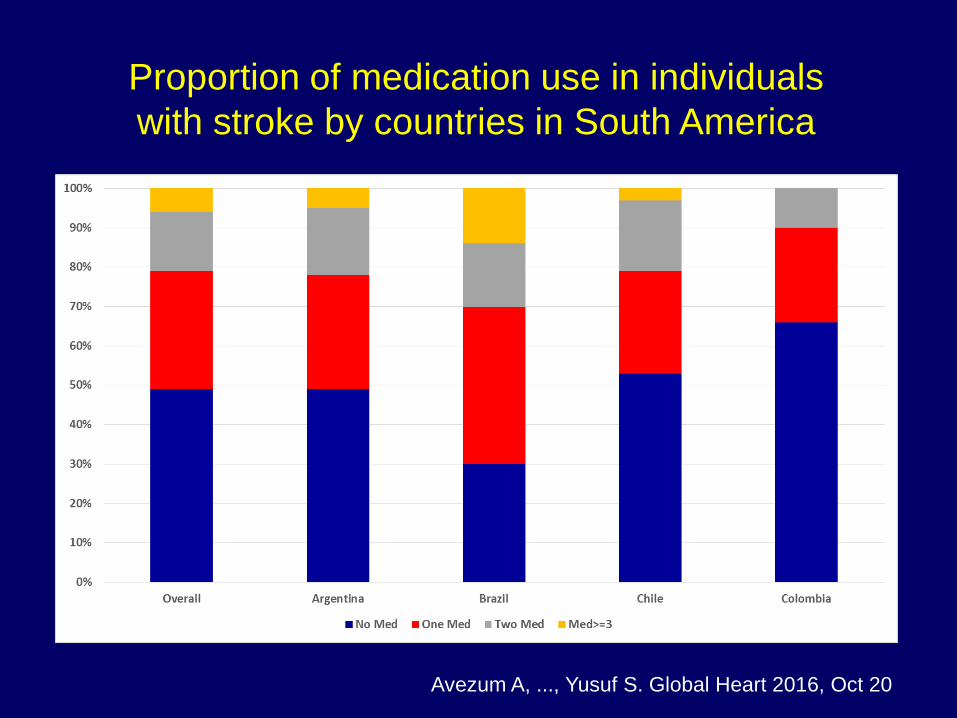
Proportion of medication use in individuals
with stroke by countries in South America
Avezum A, ..., Yusuf S. Global Heart 2016, Oct 20
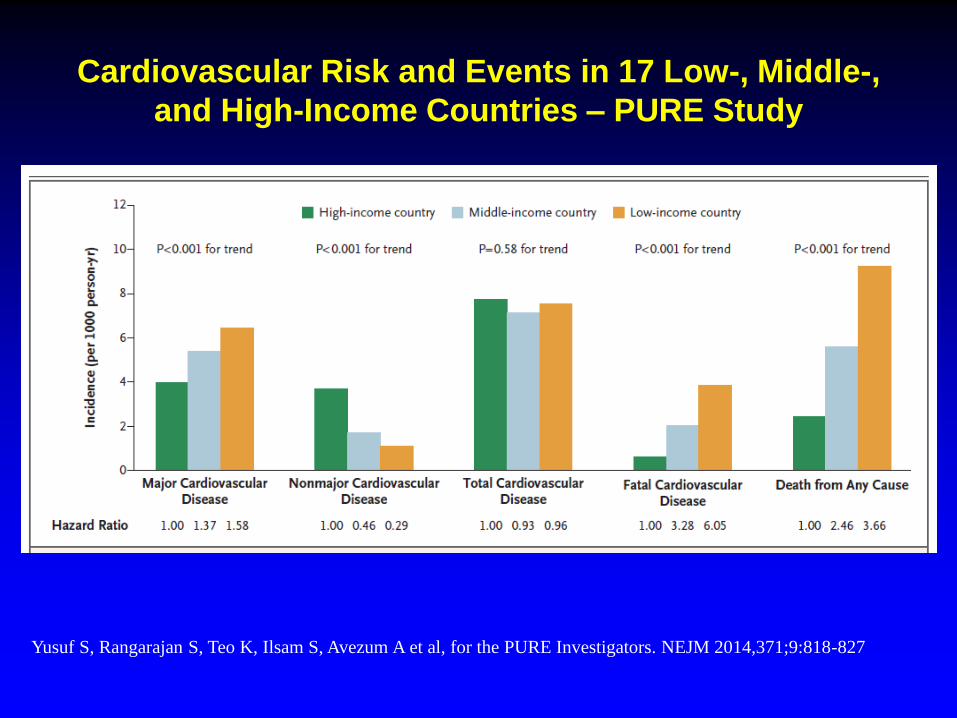
Cardiovascular Risk and Events in 17 Low-, Middle-,
and High-Income Countries – PURE Study
Yusuf S, Rangarajan S, Teo K, Ilsam S, Avezum A et al, for the PURE Investigators. NEJM 2014,371;9:818-827

Performance Measures
Adherence Rates
PERFORMANCE MEASURES N %
Blood Pressure Control (<140/90 mmHg) 695 22.0
LDL-c < 100 mg/dL 450 14.3
Smoking Cessation Program Referral 0 0
Antiplatelet Therapy 817 74.3
ACEi/ARB (DM and/or systolic dysfuncion)
Betablocker Therapy (systolic dysfuncion)
Oral Anticoagulation (AF patients – CHADS2>2)
521
92
153
67.0
22.0
33.0

Real-World Scenario
• Epidemic increase on CVD mortality (varying from region to region)
• Regional Heterogeneity and lack of common applicable guidelines and
Intrinsic limitation of guidelines to improve clinical practice
• Urgent need for KT strategies (regional and locally applicable) – policy
implementation science
• Health system not considered for health care improvement
• Possibly, shift from guidelines to EB practical recommendations
• Lack of community (primary care) interventions
• Urgent need for building a nationwide coalition for better CVD care

Need for comprehensive approach-coalition
for fighting CVD
• Inclusive and comprehensive strategy: medical societies,
government (all levels), hospitals, universities, NGOs, funding
agencies, private stakeholders.
• Platform: Brazilian Health Family Strategy (70% coverage)
• Indicators to be monitored (metrics): CV death, MI, stroke, HF,
Risk Factors (awareness/treated/controlled), 2ary prevention
• Roadmaps Interventions customized for Brazil – HS component

Achieving 25x25 together
• In September 2011, the United Nations
launched a Political Declaration which led to a
common goal of 25 percent reduction in
premature mortality from CVD and other non-
communicable diseases by 2025.
• This declaration represents a tremendous
opportunity and challenge for the medical
profession, multinational corporations,
advocacy groups, governments and other
stakeholders.
The WHF has adopted the overall goal for premature
CVD mortality and has identified three targets as being of
highest priority for CVD control: Roadmap
1. Preventing AMI and stroke through drug therapy and
counseling for high risk individuals (known CVD);
2. Reducing tobacco use by 30%
3. Increasing hypertension control by 25%

Roadblocks and potential solutions

Situational AnalysisSmoker Ex-Smoker
Never
Smoke
17% 26% 58%
Cigarrettes/day>10 10-20 > 20
59% 17% 24%
Awareness of the risk 88%
Sim Não
Attempts for quitting smoking 78% 22%
Successful quitting 25% 75%
Seeking specialized service 20% 80%
Scheduled appointment 64% 36%
Specific medication use 5% 95%
% of monthly family income 35% 65%

43%Hypertensives
33% Diagnosis > 10yr
28% Diagnosis< 5 yr
71% Regular appointments
82%Awareness of hypertension
relevance
30% Uncorrect medication use
5%Not using a single
medication
43%Hypertension
Awareness
35% BP<140x90mmHg
65% BP>140x90mmHg
20% Hypertensives unware of the hypertension diagnosis
Treatment
48% Hidroclorotiazide
26% Losartan
24% Enalapril
20% Atenolol
20% Anlodipine
Reasons for treatment non-adherence
61% Forgetfulness
30% Preference for not using
7% Highh cost
Eventos (20,3%)IAM AVC
Angin
aStent
Rev.
CirúrgicaDAOP
72% 53% 33% 29% 10% 5%
MedicaçõesAAS
Beta-
BloqueadorIECA Estatina BRA 4 Med.
38% 29% 19% 18% 15% 20%
Indivíduos com evento
prévio e sem nenhuma
medicação
28%
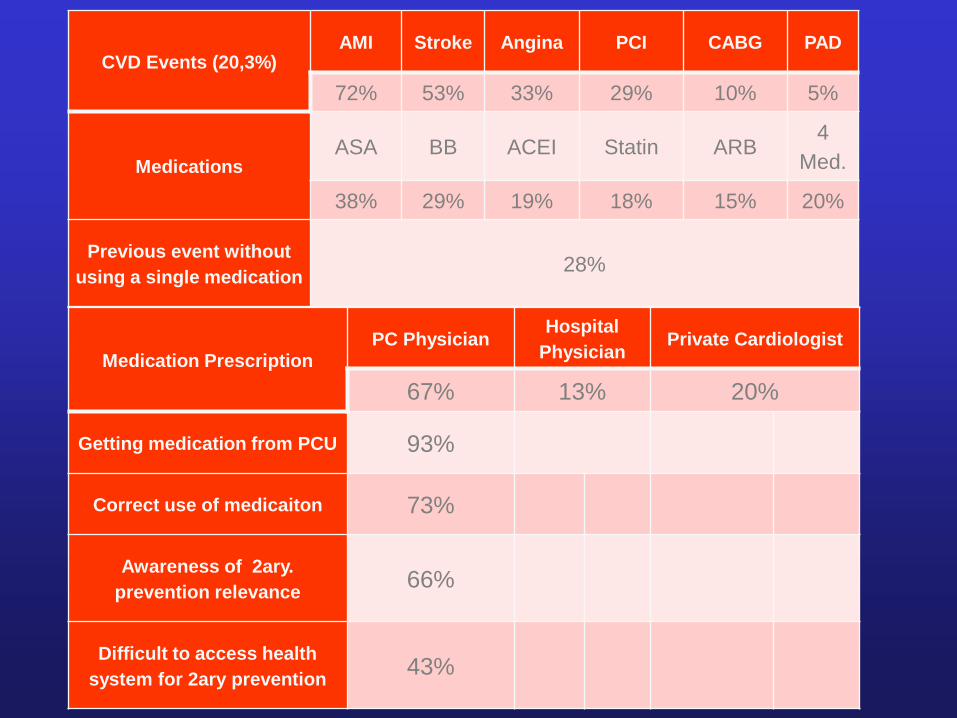
Medication PrescriptionPC Physician
Hospital
PhysicianPrivate Cardiologist
67% 13% 20%
Getting medication from PCU 93%
Correct use of medicaiton 73%
Awareness of 2ary.
prevention relevance66%
Difficult to access health
system for 2ary prevention43%
CVD Events (20,3%)AMI Stroke Angina PCI CABG PAD
72% 53% 33% 29% 10% 5%
MedicationsASA BB ACEI Statin ARB
4
Med.
38% 29% 19% 18% 15% 20%
Previous event without
using a single medication28%

Next Steps
• Create a national coalition to achieve CVD mortality reduction
• Situation analysis • Epidemiological profile (CVD, risk factors)
• Health system assessment (resources, financing, governance,
delivery)
• Policy mapping (national plans, laws)
• Rapid reviews, secondary data analysis and interviews
• Produce a situation analysis report
• Policy dialogues• Stakeholders mapping
• Discuss roadmaps solutions (in the context of situation analysis)
• Produce a concrete plan of action “National Roadmap”

Brazilian Government Ministry of
Health
WHFMedical
Societies (SBC, SBMF, ABN, SBCM,
etc )
Health Professional
Societies (ABEN, SBP, SBAFS, SBF,
ABN)
Brazilian Government –
Ministry of Education
(municipal and state schools)
Media (viral dissemination):
TV, radio, newspaper
(major, minor, regional), websites
CVD Prevention-
aligned Private
Initiative Stakeholders
NGOs
Health Professional Organization
Medical Organization (AMB, APM)
Brazilian Coalition for CVD Prevention – Stakeholders Mapping

Key Messages
The problem
• Cardiovascular diseases are the leading cause of death and disability in Brazil
being responsible for one third of the total cause of mortality.
• Despite the availability for decades of evidence-based treatment to prevent
cardiovascular diseases, including anti-hypertensive, lipid lowering, and
secondary prevention medications there use is still very low.
• Recent data suggest that only 20% of post-MI and 30% of post-stroke patients
are not taking a single evidence-based medication and only 5% of post-MI
patients are taking four evidence-based therapies.
• The main challenge now is to develop and evaluate innovative models of care to
implement “what we know it works” for cardiovascular diseases.
Key Messages
Leadership in Brazil
• Dante Pazzanese Institute of Cardiology and Research Team in Sao Paulo is one
of the most recognized cardiovascular research group in Latin America.
• Dante Pazzanese Institute of Cardiology is one of the largest cardiovascular
institution in Latin America, 65 years old, with solid and meaningful contribution to
the Brazilian cardiovascular health, through clinical care, teaching and research
(about 100 randomized clinical trials and 20 epi-studies conducted in Brazil under
our coordination through a long-term established nationwide network in Brazil.
• Researcher has been a steering committee member of 60 studies (RCTs and Epi-
studies), author and co-author of 200 peer-reviewed scientific papers, h-index of
60, reviewer of key relevant journals and one of world´s most influential scientific
minds in clinical medicine by Thompson Reuters.
• Jointly with his team we have been working on better understanding existing
roadblocks to implementation of effective cardiovascular preventive treatments.
Key MessagesThe proposed area of work
• Under this call we propose to develop and evaluate an innovative and scalable
model of care at the primary care and community level for cardiovascular primary and
secondary prevention.
• Although the exact scope of the proposed model of care is still to be decided we
anticipate that it could include some of the following components: use of information
& communication technology, task sharing, and simplification of treatment by fixed
dose combination.
• Collaborative Institution: London School of Hygiene & Tropical Medicine Centre
for Global NCDs (Director: Pablo Perel, MD, PhD)
• MRC: Picking research that delivers, research to people, global research (global
science and population science)
• Newton Fund (neglected and emerging diseases and health systems research)
• CVD community; neglected and vulnerable (cutting edge policy-relevant research
for strengthening HS in Brazil is in perfect alignment with the proposed project)
Related Documents