Critically Appraised Critically Appraised Topic: Topic: Fluid Loading in Right Ventricular Fluid Loading in Right Ventricular Infarction Infarction Mounir Mounir Basalus Basalus Critically Appraised Critically Appraised Topic: Topic: Fluid Loading in Right Ventricular Fluid Loading in Right Ventricular Infarction Infarction Mounir Mounir Basalus Basalus

Critically Appraised Topic: Fluid Loading in Right Ventricular Infarction
Jul 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Critically Appraised Critically Appraised Topic: Topic:
Fluid Loading in Right Ventricular Fluid Loading in Right Ventricular
InfarctionInfarction
MounirMounir BasalusBasalus
Critically Appraised Critically Appraised Topic: Topic:
Fluid Loading in Right Ventricular Fluid Loading in Right Ventricular
InfarctionInfarction
MounirMounir BasalusBasalus

Patient with acute chest pain Patient with acute chest pain Patient with acute chest pain Patient with acute chest pain
• 60 y/o patient presented with acute chest pain.
• No past medical history,
• Smoker, family history of CVD.
• A/
• Acute chest pain (since 1 hour).
• Nausea and diaphoresis.

PhyscialPhyscial examination examination PhyscialPhyscial examination examination
• P: 90/min, BP: 90/50 mmHg.
• Jugular vein not congested
• Heart: normal heart sounds no additional
sounds.
• Lung: Vesicular breath sounds. No additional
sounds
• No oedema.

ECG: STEMI ECG: STEMI inferior inferior infarctioninfarction and right and right ventricularventricular MI.MI.ECG: STEMI ECG: STEMI inferior inferior infarctioninfarction and right and right ventricularventricular MI.MI.
CAGCAGCAGCAG
prepre

PCIPCIPCIPCI
GPIIbIIIa inhibitor; thrombus aspiratie RCA: 1 stent (3.5/23mm @14 atm); postdilatationNC ballon (3.5mm @24atm)
Voor thrombusaspiratie
finalfinal

Clinical Clinical questionquestionClinical Clinical questionquestion
• Persistent hypotension.
• Fluid loading? Or not?
• What is the effect of “volume loading” on the
hemodynamics of patients suffering from
right ventricular myocardial infarction (RVMI).
PICOPICOPICOPICO
P: patients suffering from right ventricular
myocardial infarction and low cardiac
output/hypotension.
I : Volume loading.
C: no volume loading, dobutamine
O: improvement in hemodynamic parameter.

Search strategy Search strategy Search strategy Search strategy
• Search terms:
• Right ventricle infarction AND volume
loading/infusion
• Right ventricle infarction AND treatment
• Human studies

Search strategy Search strategy Search strategy Search strategy

Search strategy Search strategy Search strategy Search strategy
3 Reviews
` 7 Clinical studies
ESC
ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1984JACC 1984ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1984JACC 1984
• 53 patients with acute inferior transmural
myocardial infarction were studied.
• To evaluate the potential occurrence of right
ventricular infarction.
• Cardiac output/index was measure before and
after volume loading in a Subpopulation (n=27).

ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1984 JACC 1984 ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1984 JACC 1984
RVI

ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1984 JACC 1984 ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1984 JACC 1984
RVI
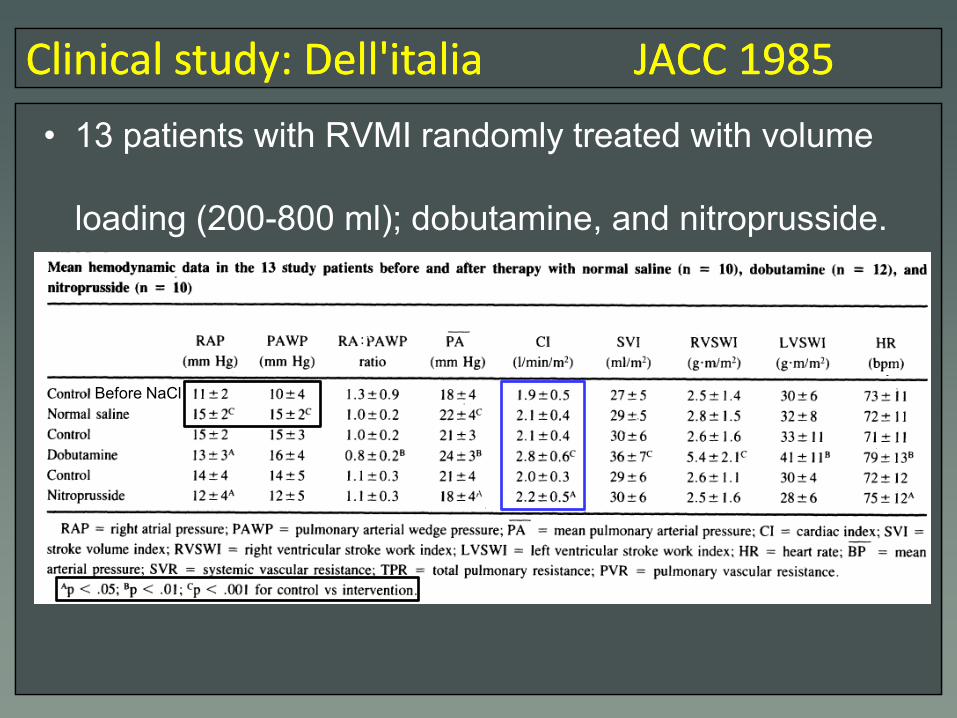
ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1985JACC 1985ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1985JACC 1985
• 13 patients with RVMI randomly treated with volume
loading (200-800 ml); dobutamine, and nitroprusside.
Before NaCl

ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1985JACC 1985ClinicalClinical studystudy: : Dell'italiaDell'italia JACC 1985JACC 1985
• 13 patients with RVMI randomly treated with volume
loading (200-800 ml); dobutamine, and nitroprusside.
Before NaCl

ClinicalClinical studystudy: : ShahShah JACC 1985JACC 1985ClinicalClinical studystudy: : ShahShah JACC 1985JACC 1985
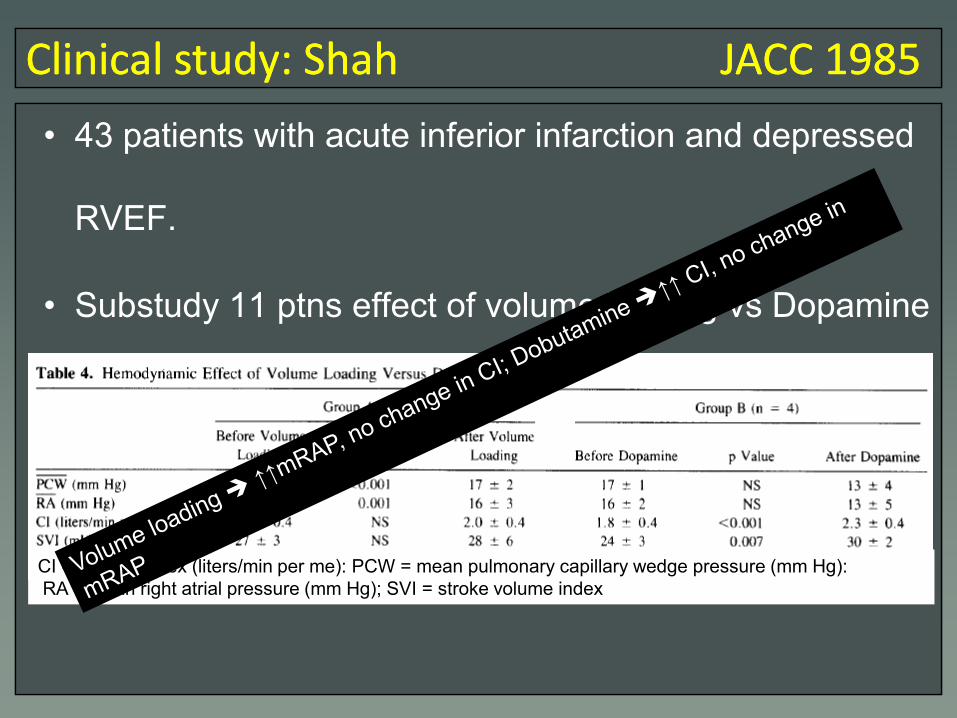
• 43 patients with acute inferior infarction and depressed
RVEF.
• Substudy 11 ptns effect of volume loading vs Dopamine
CI = cardiac index (liters/min per me): PCW = mean pulmonary capillary wedge pressure (mm Hg):
RA = mean right atrial pressure (mm Hg); SVI = stroke volume index
ClinicalClinical studystudy: : ShahShah JACC 1985JACC 1985ClinicalClinical studystudy: : ShahShah JACC 1985JACC 1985
• 43 patients with acute inferior infarction and depressed
RVEF.
• Substudy 11 ptns effect of volume loading vs Dopamine
CI = cardiac index (liters/min per me): PCW = mean pulmonary capillary wedge pressure (mm Hg):
RA = mean right atrial pressure (mm Hg); SVI = stroke volume index

ClinicalClinical studystudy: : DhainautDhainaut JACC 1990JACC 1990ClinicalClinical studystudy: : DhainautDhainaut JACC 1990JACC 1990
• 20 consecutive patients with RVI and low cardiac output
within 48 h of the onset of symptoms were prospectively
included. Evaluation after volume loading and Dobu.
• Volume loading slight ↑in CI, marked ↑↑ in RAP .
• Dobu marked ↑↑ in CI.

ClinicalClinical studystudy: : SlniorakisSlniorakis EHJ 1994EHJ 1994ClinicalClinical studystudy: : SlniorakisSlniorakis EHJ 1994EHJ 1994
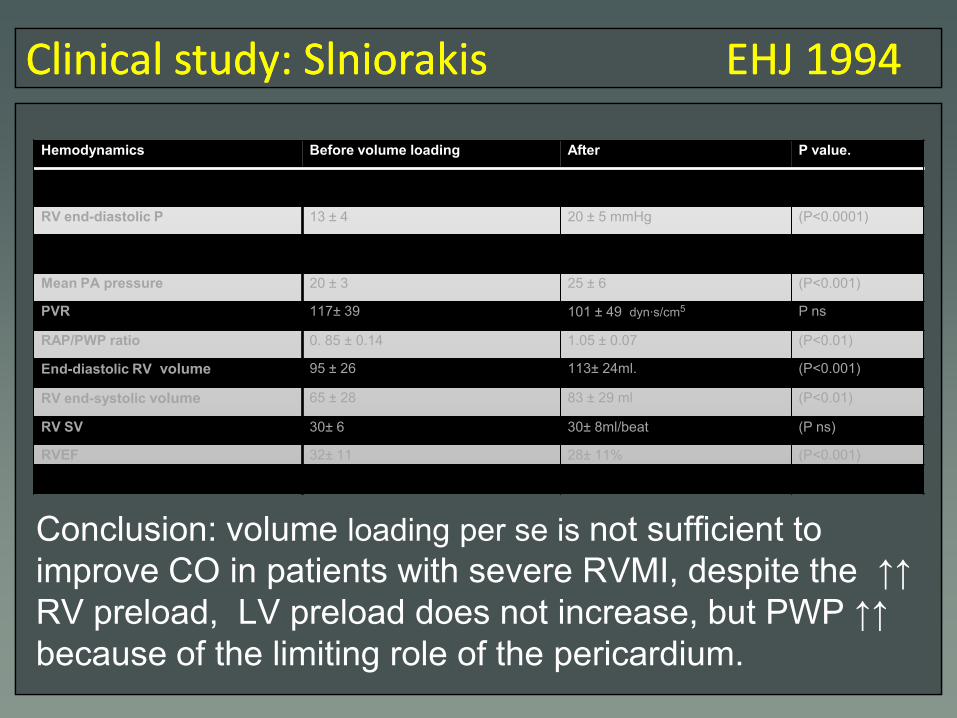
• Evaluation of the effect of volume loading in 11 patient
with severe RVMI. Used volume loading aiming @ PWP
(18-24mmHg). Hemodynamics were measure before
and after volume loading
Hemodynamics Before volume loading After P value.
Right atrial pressure 12 ± 4 19 ± 5 mmHg (P<0.0001)
RV end-diastolic P 13 ± 4 20 ± 5 mmHg (P<0.0001)
PWP 14 ± 3 20 ± 6 (P<0.0001)
Mean PA pressure 20 ± 3 25 ± 6 (P<0.001)
PVR 117± 39 101 ± 49 dyn·s/cm5 P ns
RAP/PWP ratio 0. 85 ± 0.14 1.05 ± 0.07 (P<0.01)
End-diastolic RV volume 95 ± 26 113± 24ml. (P<0.001)
RV end-systolic volume 65 ± 28 83 ± 29 ml (P<0.01)
RV SV 30± 6 30± 8ml/beat (P ns)
RVEF 32± 11 28± 11% (P<0.001)
Cardiac output 2. 3 ± 0.42 2.4± 0.62 l/ min (P ns)
ClinicalClinical studystudy: : SlniorakisSlniorakis EHJ 1994EHJ 1994ClinicalClinical studystudy: : SlniorakisSlniorakis EHJ 1994EHJ 1994
Conclusion: volume loading per se is not sufficient to
improve CO in patients with severe RVMI, despite the ↑↑
RV preload, LV preload does not increase, but PWP ↑↑
because of the limiting role of the pericardium.
Hemodynamics Before volume loading After P value.
Right atrial pressure 12 ± 4 19 ± 5 mmHg (P<0.0001)RV end-diastolic P 13 ± 4 20 ± 5 mmHg (P<0.0001)
PWP 14 ± 3 20 ± 6 (P<0.0001)
Mean PA pressure 20 ± 3 25 ± 6 (P<0.001)
PVR 117± 39 101 ± 49 dyn·s/cm5 P ns
RAP/PWP ratio 0. 85 ± 0.14 1.05 ± 0.07 (P<0.01)
End-diastolic RV volume 95 ± 26 113± 24ml. (P<0.001)
RV end-systolic volume 65 ± 28 83 ± 29 ml (P<0.01)
RV SV 30± 6 30± 8ml/beat (P ns)
RVEF 32± 11 28± 11% (P<0.001)
Cardiac index 2. 3 ± 0.42 2.4± 0.62 l/ min /m2 (P ns)
ClinicalClinical studystudy: : FerrarioFerrario AJC 1994AJC 1994ClinicalClinical studystudy: : FerrarioFerrario AJC 1994AJC 1994
• 11 consecutive patients with RVI (and inferior infarction
with low cardiac output.
• After baseline measurements, patients were randomly
treated with
• dobutamine infusion, 5 µkg/min over 10 minutes,
followed by 10 p&kg/minover 10 minutes or,
• alternatively, by rapid intravascular administration of
normal saline solution in 200 ml increments over 5
minutes. Interruption of volume : mRAP> 20; mean
pulmonary capillary pressure >20 mm Hg, or ↓↓ CO
• After return of hemodynamics to baseline volume
loading & dobutamine were repeated in a crossover.

ClinicalClinical studystudy: : FerrarioFerrario AJC 1994AJC 1994ClinicalClinical studystudy: : FerrarioFerrario AJC 1994AJC 1994
• Volume loading(VL)↑↑RAP&PCWP BUT no change CI
• Dobutamine(d)no change RAP&PCWP BUT↑↑CI.
ClinicalClinical studystudy: : BerishaBerisha BMJ 1990BMJ 1990ClinicalClinical studystudy: : BerishaBerisha BMJ 1990BMJ 1990
• 41 patients with RVMI
• What is the optimal filling pressure for the RV?
• Used volume loading or NTG to modify the right
ventricular filling pressure.
• Used right ventricular stroke work index (RVSWI) and CI
endpoints.
• RVSWI=0.0144*SVI*MPAP (the amount of work that
the right ventricle does during each contraction)

ClinicalClinical studystudy: : BerishaBerisha BMJ 1990BMJ 1990ClinicalClinical studystudy: : BerishaBerisha BMJ 1990BMJ 1990
Baseline
mRAP<10mmHg <10mmHg 10-14mmHg 10-14mmHg >14mmHg
mRAP after
intervention10-14mmHg >14mmHg 10-14mmHg >14mmHg RA Perssure
lowered
• Similarly, optimal PWP 16 mmHg.
summary summary clinicalclinical studies studies (n=7)(n=7)summary summary clinicalclinical studies studies (n=7)(n=7)
• Volume loading has no effect on CI : 5
• Volume loading has a modest effect on CI: 1
• Volume loading has an effect on CI within limits : 1

Review: Review: MovahedMovahed ClinClin. . CardiolCardiol. 2000. 2000Review: Review: MovahedMovahed ClinClin. . CardiolCardiol. 2000. 2000
• Optimization of preload.
• Initial therapy of RVI (hypotension and no pulmonary
congestion) should start with volume expansion.
• If unresponsive to initial trial of fluids hemodynamic
monitoring, and subsequent volume challenge CVP < I5
mmHg.
• Any interventions that reduce the preload (diuretics,
nitrates, and vasodilators) should be avoided even in the
absence of hypotension.
Review: Review: MovahedMovahed ClinClin. . CardiolCardiol. 2000. 2000Review: Review: MovahedMovahed ClinClin. . CardiolCardiol. 2000. 2000
• When RVI is accompanied by severe LV dysfunction and
pulmonary congestion, the RV is further compromised by
increased afterload.
• In this circumstance, the use of afterload-reducing
agents such as sodium-nitroprusside or IABP is often
necessary to unload the LV and subsequently the RV.

Review: Review: GoldsteinGoldstein JACC 2002JACC 2002Review: Review: GoldsteinGoldstein JACC 2002JACC 2002
• Optimization of preload:
• RVI dilated noncompliant RV is exquisitely preload
dependent.
• factors that reducing preload tend to be detrimental,
• optimizing cardiac filling tend to be beneficial.
• Wide spectrum of initial volume status in acute RVI:
• relatively volume depleted benefiting from VL
• more replete flat response to fluid resuscitation.
Review: Review: GoldsteinGoldstein JACC 2002JACC 2002Review: Review: GoldsteinGoldstein JACC 2002JACC 2002
• An initial volume challenge is appropriate for patients
manifesting
• low output
• without pulmonary congestion,
• particularly if the estimated CVP <15 mm Hg.
• For those unresponsive to an initial trail of fluids,
• hemodynamically monitored volume challenge may
be appropriate.
• Avoid excessive volume administration (descending limb of starling curve).

Review: Review: InoharaInohara EHJEHJ--ACVC 2013ACVC 2013Review: Review: InoharaInohara EHJEHJ--ACVC 2013ACVC 2013
• Older (animal model) studies maintenance of the RV
preload with volume loading thought to resolve
accompanying hypotension.
• Later clinical studies variable responses to
aggressive fluid therapy.
• Some studies, showed that volume loading further
elevates right-sided filling pressure without improving CI
• Berisha et al: maximal RVSWI & CI @mRAP of 10–14
mmHg, and a mRAP of >14 mmHg ↓↓RVSWI/CI.
• Haemodynamics of RVI : extremely variable (influenced
by state of hydration and the degree of concomitant LV
involvement.)

GuidelinesGuidelines: ESC EHJ 2012: ESC EHJ 2012GuidelinesGuidelines: ESC EHJ 2012: ESC EHJ 2012
• Despite the jugular distension, fluid loading that
maintains right ventricular filling pressure is a key
therapy in avoiding or treating hypotension.*
• In addition, diuretics and vasodilators should be avoided,
as they may aggravate hypotension.*
* No references
ConslusionConslusionConslusionConslusion
• Patients suffering from RVMI appears to be very
sensitive for changes in volume status.
• In patients with RVMI and low cardiac
output/hypotension, low CVP, and no pulmonary
congestion it is prudent to administer boluses of
normal saline (200 cc) reaching a maximal of 1.5 ltr.
(voluven is frequently administered in the cathlab)
• This group of patients may be simply suffering from a
low circulating volume status.

ConslusionConslusionConslusionConslusion
• In case of no response on this initial “fluid challenge”,
invasive monitoring of CVP should be considered.
• CVP <10mmHg further volume loading.
• CVP 10-14Hg consider dobutamine/ LV unloading
devices.
• CVP >14mmHg modest dose
diuretics/±venodilators(beside dobu en LV
unloading).
Related Documents











