ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S: COVID-19 Emergency Response Team ‘covERT’ Page 1 of 14 * UNCONTROLLED WHEN DOWNLOADED * COVID-19 Emergency Response Team ‘covERT’ Policy Policy Statement The best management for progressive hypoxic respiratory failure due to COVID-19 is early transfer to Intensive Care, intubation and ventilation. In patients with COVID-19, intubation places the patient and surrounding staff at risk. It is recommended that intubation be performed by the most experienced clinician available. The COVID-19 Emergency Response Team (covERT) fulfils this role. Related Clinical Documents COVID-19 Policies Objectives To outline the team membership of covERT To describe the roles and responsibilities of team members Scope This policy applies to staff working in The Department of Anaesthesia and Acute Pain Medicine, the Emergency Department (ED) and Intensive Care Unit (ICU) at St Vincent’s Hospital Melbourne (SVHM) and St Vincent’s Private Hospital Melbourne (SVPHM). Definitions COVID-19 Patient For the purpose of this policy, a COVID-19 patient refers to both confirmed positive and suspected positive patients. covERT Response The critical care response to a COVID-19 patient requiring intubation. covERT Team A consultant anaesthetist and an anaesthesia nurse available to facilitate intubation in COVID- 19 patients. Acronyms covERT COVID-19 Emergency Response Team PACU Post-Anaesthesia Care Unit PPE Personal protective equipment NGT Naso-gastric tube

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 1 of 14 * UNCONTROLLED WHEN DOWNLOADED *
COVID-19 Emergency Response Team ‘covERT’
Policy Policy Statement
The best management for progressive hypoxic respiratory failure due to COVID-19 is early transfer to Intensive Care, intubation and ventilation. In patients with COVID-19, intubation places the patient and surrounding staff at risk. It is recommended that intubation be performed by the most experienced clinician available. The COVID-19 Emergency Response Team (covERT) fulfils this role. Related Clinical Documents
COVID-19 Policies Objectives
To outline the team membership of covERT
To describe the roles and responsibilities of team members Scope
This policy applies to staff working in The Department of Anaesthesia and Acute Pain Medicine, the Emergency Department (ED) and Intensive Care Unit (ICU) at St Vincent’s Hospital Melbourne (SVHM) and St Vincent’s Private Hospital Melbourne (SVPHM). Definitions
COVID-19 Patient For the purpose of this policy, a COVID-19 patient refers to both confirmed positive and suspected positive patients. covERT Response The critical care response to a COVID-19 patient requiring intubation. covERT Team A consultant anaesthetist and an anaesthesia nurse available to facilitate intubation in COVID-19 patients. Acronyms
covERT COVID-19 Emergency Response Team PACU Post-Anaesthesia Care Unit PPE Personal protective equipment NGT Naso-gastric tube

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 2 of 14 * UNCONTROLLED WHEN DOWNLOADED *
Index
1 Responsibilities ............................................................................................................................. 3
1.1 Roles of the covERT Team .................................................................................................. 3 1.2 Anaesthesia ........................................................................................................................... 3 1.3 Intensive Care Unit ................................................................................................................ 3 1.4 Emergency Department ........................................................................................................ 3 1.5 St Vincent’s Private Hospital Melbourne (SVPHM) ............................................................ 4
2 Pathways ....................................................................................................................................... 6 2.1 Emergency Department Patient ........................................................................................... 6 2.2 Ward Patient .......................................................................................................................... 6 2.3 Patient at St Vincent’s Private Hospital Melbourne ............................................................ 7 2.4 Unintubated Patient in SVHM ICU ....................................................................................... 7
3 General Principles......................................................................................................................... 7 3.1 Clinical Leadership ................................................................................................................ 7 3.2 PPE / Donning and Doffing .................................................................................................. 8 3.3 Intubation ............................................................................................................................... 8 3.4 Preparation of Intubating Spaces......................................................................................... 9 3.5 Staff for the covERT Response in each Location ............................................................... 9 3.6 Roles of Staff ....................................................................................................................... 10 Appendix A - covERT Response Process .................................................................................... 11 Appendix B - covERT Team PPE Donning / Doffing ................................................................... 12

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 3 of 14 * UNCONTROLLED WHEN DOWNLOADED *
Procedure
Responsibilities
1.1 Roles of the covERT Team
Airway management to facilitate mechanical ventilation in COVID-19 patients.
Transport of intubated COVID-19 patients from site of intubation, to intensive
care bed when necessary.
Insertion of invasive monitoring, venous-access and wide bore naso-gastric
tube (NGT) placement in discussion with ICU team, to facilitate assessment
with a single chest x-ray.
1.2 Anaesthesia
Provide an anaesthetist and anaesthesia nurse to staff the covERT team
o In hours (Monday to Friday 0800-1800) this will be provided by in house
staff
o Out of hours, this service will be provided by an on-call anaesthetist
o To respond to Code Blue PPE in the inpatient services building (Building
A), with equipment to facilitate intubation.
Provide clinical leadership in the period immediately surrounding airway
management.
Constantly review the staffing of the covERT team, in the context of patient load
and adjust staffing as appropriate.
1.3 Intensive Care Unit
Provide a consultant led service to triage all requests for intubation and
admission to ICU.
To be aware of COVID-19 patients who are at risk of deterioration and to
facilitate elective intubation of patients wherever possible.
To provide clinical assistance (doctor and nursing staff) with airway
management.
To provide a specified area for intubation of COVID-19 patients
o To provide pre-specified airway equipment
o To provide pre-specified medications to facilitate airway management and
potential consequences.
To provide clinical leadership in the airway management of COVID-19 patients,
except in the immediate period
1.4 Emergency Department
To identify COVID-19 patients in the Emergency Department for whom
intubation and ventilation is an appropriate form of treatment.
To communicate with on-call ICU consultant about the need for intubation.
To make and communicate a decision about the most appropriate location for
airway management to occur.
If intubation is to occur in the ICU (preferred), the ED team will communicate
with the ICU and the coVERT team, and transport the patient to the ICU.
If intubation needs to occur in the ED

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 4 of 14 * UNCONTROLLED WHEN DOWNLOADED *
o If emergent intubation is required and the covERT team has not arrived, the
most experienced airway physician will undertake intubation in Level 4 PPE
o If the covERT team (preferred) is going to intubate
Provide clinical assistance (doctor and nursing staff) with airway
management
Provide a specified area for intubation of COVID-19 patients
Provide pre-specified airway equipment
Provide pre-specified medications to facilitate airway management
and potential consequences
Provide clinical leadership in airway management of COVID-19 patients
except in the immediate period around
1.5 St Vincent’s Private Hospital Melbourne (SVPHM)
Early and constant assessment of all COVID-19 patients to identify those at risk
of hypoxic respiratory failure.
Early transport of COVID-19 patients at risk of hypoxic respiratory failure to St
Vincents Hospital Melbourne.
SVPHM ICU consultant consults with SVHM ICU consultant.
SVPHM ICU consultant contacts the covERT team on 9231 4471, if emergency
intubation of a COVID-19 patient is required to facilitate safe transport to the
public ICU
Provide clinical assistance (doctor and nursing staff) with airway
management
Provide a specified area for intubation of COVID-19 patients
Provide pre-specified airway equipment
Provide pre-specified medications to facilitate airway management
and potential consequences
Provide clinical leadership in the management of COVID-19 patients except
in the immediate period around airway management
Ensure all covERT responders are capable of donning and doffing PPE as
described in departmental guidelines.

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 5 of 14 * UNCONTROLLED WHEN DOWNLOADED *
Figure 1. A graphic overview of the covERT response
Medications

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 6 of 14 * UNCONTROLLED WHEN DOWNLOADED *
Pathways
2.1 Emergency Department Patient
COVID-19 patients who are likely to benefit from intubation and ventilation
should be discussed at a consultant level in the ED, considering functional
state, frailty, major co-morbidities and age, as per the Patient Triage flowchart.
The ICU consultant on call should be contacted via the switchboard and a
decision about treatment options made, considering the patient factors and
hospital resources available.
If the decision to progress with intubation and airway management is made, the
ED physician should make a recommendation about whether the patient can be
transported to ICU or whether the intubation should occur in the ED.
The ED physician should contact the covERT team by phoning 4471, during the
day this will reach the Anaesthetist in charge, afterhours it will reach the after
hours anaesthesia registrar
o If the patient requires immediate intubation, this should be performed by the
most experienced airway physician available, following the guidelines for
intubation of COVID-19 patients listed later in this document and wearing
Level 4 PPE
o If the patient is too unstable to be transferred to the ICU but can wait for the
arrival of the covERT team
The covERT team will arrive in Level 4 PPE, having donned PPE in the
PACU
The Emergency Department should prepare the space around the
patient, pre-specified medications and airway equipment
The covERT response will require the covERT team, a senior ED
physician to act as second physician, an ED nurse to act as a runner,
an ED nurse to act as an outside runner and someone to control the
scene
Intubation and insertion of a large bore NGT should be performed
simultaneously wherever possible
Following successful intubation of the patient and stabilisation of their
condition, the covERT team will transport the patient to the ICU. If the
ED team is available to participate in this transport they will. It is
expected that they will frequently have other clinical duties.
o If the patient can be transported to the ICU before intubation, the transport
will be performed by the ED team. The covERT team will meet the patient
in the ICU and will work in tandem with ICU staff.
2.2 Ward Patient
In an ideal situation, COVID-19 patients on the ward will be carefully monitored
and those who might require intubation will be identified early allowing
intubation to occur in an elective fashion.
Should an acute deterioration occur on the ward necessitating emergency
intubation a ‘Code Blue/PPE’ should be called via the switchboard
o Basic life support as per Basic Life Support in the COVID-19 Patient
o The covERT team will attend a ‘Code Blue/PPE’ after donning PPE in
PACU
o The decision to intubate the patient and transfer the patient to ICU will be
made by the ICU consultant wherever practical

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 7 of 14 * UNCONTROLLED WHEN DOWNLOADED *
o Once the patient is intubated they will be transported to the ICU by the
covERT team and further invasive monitoring and lines placed as
necessary.
2.3 Patient at St Vincent’s Private Hospital Melbourne
The SVPHM ICU consultant can call the covERT team (9231 4471) to assist in
the emergency intubation of COVID-19 patients.
The covERT team will meet in the PACU, don their PPE and travel to SVPHM
via the tunnels. They will be met by a security officer at the lift and a nurse on
exiting the lift on the second floor of SVPHM, where the operating theatre is
located.
The intubating space should be prepared with specified airway equipment,
medications and staff in appropriate PPE.
The covERT team will work in conjunction with the SVPHM ICU consultant and
SVPHM nursing staff to safely intubate the patient and place a large bore NGT.
The covERT team will take responsibility for the transport of the patient to
SVHM ICU, utilising the portable ventilator provided by the SVPHM ICU. The
patient will be transported on a SVPHM bed and transferred to a SVHM bed on
arrival in our ICU.
Once in our ICU the covERT team will place any other invasive monitoring and
lines that are required.
2.4 Unintubated Patient in SVHM ICU
When a decision is made to intubate a patient already in the ICU, the ICU
consultant should call the covERT team on 4471.
The covERT team will meet in PACU and don PPE.
The covERT team will attend the ICU.
The ICU will prepare the intubating area including specified staff, airway
equipment and medications.
The covERT response will involve at least, the covERT team, ICU consultant,
an ICU nurse in the room, an external nurse and someone to perform scene
control.
Following successful intubation and wide bore NGT placement the covERT
team will place appropriate invasive monitoring and lines.
General Principles
Clinical Leadership
When the covERT team arrives, clinical leadership will be held by an ED
physician, ICU physician or anaesthetist, depending on the patient’s location.
Once the covERT team has assessed the patient and formulated a plan, they
should formally assume clinical leadership and receive a response from the
existing clinical leader.
The covERT team retain clinical leadership until the airway is declared secure
unless they are involved with transport of the intubated patient or have further
procedures to perform.
The transfer of clinical leadership should be openly discussed and clearly
communicated.
See Appendix A.
ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 8 of 14 * UNCONTROLLED WHEN DOWNLOADED *
PPE / Donning and Doffing
Intubation is considered an aerosol-generating procedure (AGP). During the
covERT response AGP may create a viral plume that could put staff at risk. All
staff in close proximity (2 m radius) to the patient during intubation should be
wearing level 4 PPE.
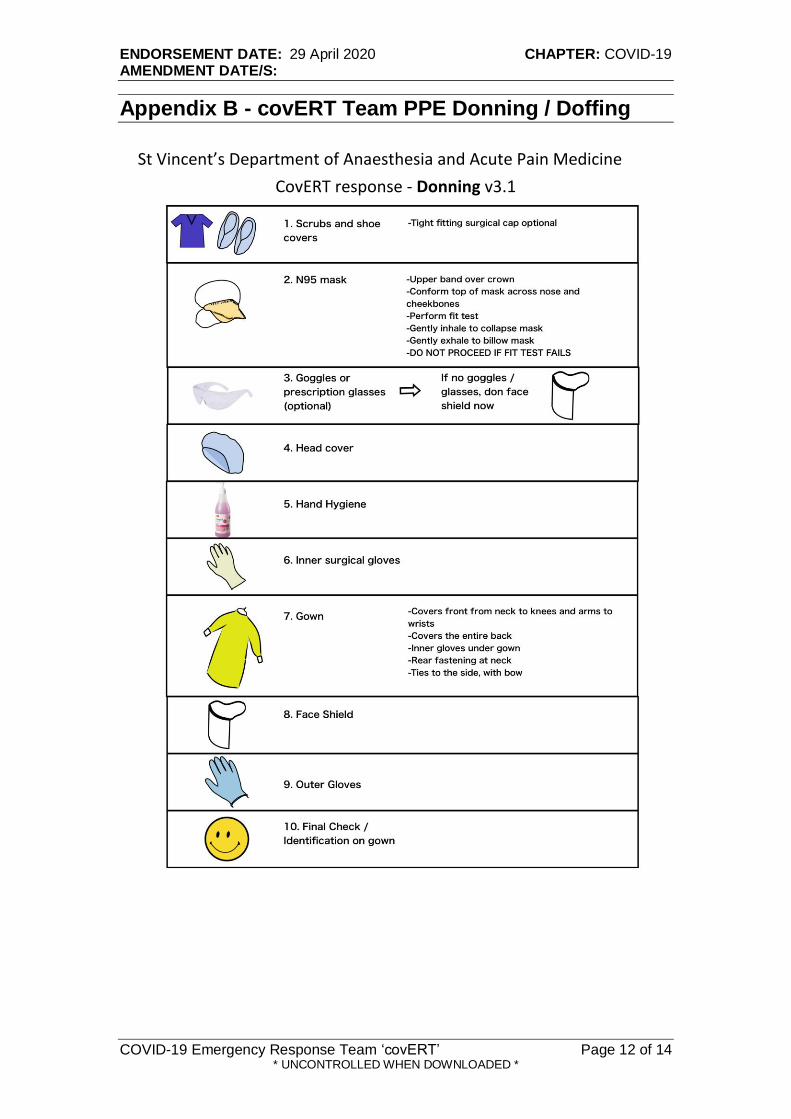
Meticulous attention to detail is required whilst donning or doffing PPE. During
donning and doffing the specified procedure should be followed exactly and an
observer used.
See Appendix B for the covERT donning and doffing guide.
Intubation
Ensure the patient is optimally positioned.
The airway physician and assistant will remove the patient’s O2 mask and
replace immediately with a mask attached to the circuit, obtaining the best
possible seal. A two handed technique is recommended to optimise the seal,
utilising end tidal CO2 (EtCO2) and observing a square wave form acts as
confirmation of a good mask seal.
Perform best possible pre-oxygenation.
Turn off bag valve mask (BVM) O2 prior to removing BVM to minimise aerosol
generation.
Induce with a rapid sequence induction avoiding positive pressure ventilation
wherever possible. Rapid muscle relaxation is preferred to minimise the chance
of cough and infectious aerosol
o Either suxamethonium (succinylcholine) or high dose rocuronium could be
utilised. Suxamethonium may produce marginally quicker intubating
conditions, however, it must be quickly followed by a longer acting agent to
ensure muscle relaxation is maintained and the chance of aerosol generation
is minimised.
Videolaryngoscopy utilising a system where the screen is separate from the
laryngoscope blade is preferable, this will usually be with a Glidescope. At
SVPHM there is a C-MAC® system.
The cuff of the endotracheal tube should be inflated before positive pressure
ventilation proceeds.
If in the operating room, the intubating physician should only touch the
adjustable pressure limiting (APL) valve and bag component of the anaesthesia
circuit, all other ventilator manipulations should be made by the observer under
instruction.
A large bore NGT should be placed and secured in all patients by the covERT
team at the time of intubation. The glidescope and McGill forceps may be a
useful adjunct to ensure the procedure is performed efficiently.
Once the airway is secure this should be declared. At this point clinical
leadership can be returned to the ‘home team’ if that is appropriate.
Once the airway is safely secured all disposable airway equipment should be
disposed of in the appropriate bin within the patient’s room.
Reusable equipment (e.g. glidescope stylet) should be placed in a sealed bag.
The bag should be wiped down within the room and then placed into a second
bag held by the outside runner.

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 9 of 14 * UNCONTROLLED WHEN DOWNLOADED *
Preparation of Intubating Spaces
In order to facilitate the covERT response the following airway equipment and medications should be available on arrival of the covERT team, see Tables 1 and 2.
Airway Equipment
Inside Outside (brought by covERT team)
Videolaryngoscope
Airway Tray o Ambu bag / HME o Medium mask o Tracheostomy tape o 10 mL syringe o 7.5 ETT o MAC 4 VL blade o Satin slip stylet o Large bore NGT o McGill forcep o Lubricant o Plastic sheet o Nasofix / NGT spigot
ETT 6,7,8
3 sizes of guedel airway
iGel 3,4,5
Glidescope stylet
D blades, Mac 3 / 4 blades
Flexitip bougie
Frova bougie
Range of face masks
Oropharyngeal / nasopharyngeal airways
CICO kit
Table 1. Airway equipment required at the start of covERT intubation
Medications
Prepared
(CoVERT Intubation Kit A)
Immediately available
(CoVERT Intubation Kit B)
Fentanyl 200 microg in 4 mL (5mL syringe) Propofol 200 mg in 20mL (20mL syringe) Rocuronium 2 x 50 mg in 5mL (red 5mL syringe) Metaraminol 10 mg in 20mL (20mL syringe)
Midazolam 5 mg in 5mL Ketamine 200 mg in 2mL Vercuronium 10mg Water for Injection 10mLSuxamethonium 100 mg Atropine 2 x 600microg in 1mL Adrenaline 1 mg in 10mL
Infusion of morphine and midazolam and syringe pump Infusion of noradrenaline and syringe pump
Table 2. Pharmaceuticals required at the start of covERT intubation
Staff for the covERT Response in each Location
covERT team - Anaesthetist and Anaesthesia Nurse
Second Physician o ICU - ICU consultant o ED - Emergency physician o Ward - most senior physician available o SVPHM - SVPHM ICU consultant
In room assistant o ICU - patient’s ICU nurse o ED - ED nurse o Ward - ICU nurse from Code team o SVPHM - Anaesthesia nurse / ICU nurse supplied by SVPHM
Assistant outside room o ICU - ICU nurse o ED - ED nurse o Ward - ICU / ward nurse o SVPHM - Anaesthesia nurse / ICU nurse supplied by SVPHM

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 10 of 14 * UNCONTROLLED WHEN DOWNLOADED *
Scene control o Member of nursing or medical staff
Roles of Staff
Second Physician o Wears Level 4 PPE, ensures other members of the home team are
appropriately attired o Has clinical leadership of the patient in the time leading up to intubation o Gives clinical handover to covERT team o Cedes clinical leadership during intubation and takes on a role focusing on
situational awareness o Administers medications during intubation including induction medications
and medications to maintain haemodynamic stability o Takes back clinical leadership if appropriate once the airway is declared
secure o Meticulously doffs PPE, observed doffing by others
In Room Assistant o Wears Level 4 PPE o Ensures the intubating space, specified airway equipment and medications
are prepared and available o Assists covERT team when unfamiliar with ED / ward / ICU / SVPHM
environment o Obtains equipment from outside the intubating area by communication with
outside assistant o Meticulously doffs PPE, observed doffing by others
Outside assistant o Wears Level 3 PPE o Provides extra equipment or additional medications to the team in the
intubating area on request
Scene Control o Wears appropriate PPE o Minimises staff in the vicinity of the covERT response o Co-ordinates the response outside of the intubating area
Anaesthetist o Dons Level 4 PPE in the PACU, observes anaesthetic nurse donning o Travels to the site of intubation with anaesthesia nurse o Takes clinical handover from second physician o Assesses patients airway o Discusses airway plan with covERT response team in the intubating area o Pre-oxygenates patient o Intubates patient o Declares airway secure o Discusses with secondary physician whether it is appropriate to cede clinical
leadership o Meticulously doffs PPE, observed doffing by others
Anaesthesia Nurse o Dons Level 4 PPE in the PACU, observes anaesthetist donning o Travels to the site of intubation with the anaesthetist o Readies airway equipment o Assists in process of intubation o Assists in ensuring contaminated waste is correctly disposed of and reusable
equipment is correctly bagged to be sterilised o Meticulously doffs PPE, observed doffing by others

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 11 of 14 * UNCONTROLLED WHEN DOWNLOADED *
Appendix A - covERT Response Process
ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 12 of 14 * UNCONTROLLED WHEN DOWNLOADED *
Appendix B - covERT Team PPE Donning / Doffing
CovERTresponse-Donningv3.1
StVincent’sDepartmentofAnaesthesiaandAcutePainMedicine

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 13 of 14 * UNCONTROLLED WHEN DOWNLOADED *
CovERTresponse–DoffingGuidev3.1

ENDORSEMENT DATE: 29 April 2020 CHAPTER: COVID-19 AMENDMENT DATE/S:
COVID-19 Emergency Response Team ‘covERT’ Page 14 of 14 * UNCONTROLLED WHEN DOWNLOADED *
Authorship Details
Name: Position:
Primary Policy Author(s):
covERT response simulation group Representatives from critical care specialties
Stuart Dilley Emergency Physician
Alexander Handrinos Emergency Physician
Jonathan Karro Emergency Physician
Bernadette Hickey Intensive Care Physician
Yvette O’Brien Intensive Care Physician
Steven Musca Intensive Care Physician
Tim Haydon Intensive Care Physician
Ben Slater Anaesthetist
Tuong Phan Anaesthetist
Abarna Devapalasundaram Anaesthetist
Elizabeth Coyle Anaesthetist
Others Consulted, including Committees:
Joanne Cocks Co-ordinator infection control
John Santamaria Director, ICU
Andrew Walby Director, ED
David Scott Director, Anaesthesia
Medication Safety Committee
Head of Department Responsible for policy:
Antony Tobin Chief Medical Officer
Related Documents











