Corticotropin-Releasing Hormone Prepubertal Major Depression Challenge in Boris Birmaher, Ronald E. Dahl, James Perel, Douglas E. Williamson, Beverly Nelson, Stacy Stull, Joan Kaufman, G. Scott Waterman, Uma Rao, Nga Nguyen, Joaquim Puig-Antich, and Neal D. Ryan This study investigates cortisol and ACTH (corticotropin) responses to an infusion of human CRH (corticotropin-releasing hormone) in prepubertal children with major depressive disorder (MDD). Following a period of 24 hours of adaptation to the laboratory environment with an intravenous catheter in place, 34 children with MDD and 22 healthy controls received 1 txg/kg of human CRH at 5:00 PM. Blood samples for cortisol and ACTH were measured at baseline and post-CRH. Overall, there were no significant differences between the MDD and the normal controls in baseline or post CRH stimulation values of either cortisol or ACTH. Melancholic (n = 4) patients had significantly higher baseline cortisol levels than nonmel- ancholic (n = 24) patients. Compared with the outpatients and the nonmelancholics, the inpatients (n = 10) and the melancholics showed significantly lower total ACTH secretion (effect size: 0.9 and 1.4, respectively) after CRH infusion. These results are consistent with a broad literature suggesting that the HPA axis abnormalities occur less frequently in early-onset depression than reported in adult studies. The pattern of results in the subgroups of inpatients and in melancholic children, however, raise questions about possible continuities with adult studies. Key Words: CRH, cortisol, ACTH, stress, child depression BIOL PSYCHIATRY1996;39:267--277 Introduction There is a considerable body of literature showing an association between adult major depressive disorder From the Department of Psychiatry, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, Pittsburgh, PA; the Department of Psychiatry, University of Texas Medical Branch, Department of Psychiatry and Behavioral Sciences, Galveston, TX (NN); and the Department of Psychiatry, University of Vermont, College of Medicine, Burlington, VT. Address reprint requests to Boris Birmaher, MD, Western Psychiatric Institute and Clinic, 3811 O'Hara Street Room #612BT, Pittsburgh, PA 15213. Received April 29, 1994; revised March 14, 1995. (MDD) and dysregulation of the hypothalamic-pituitary- adrenal (HPA) axis (Stokes and Sikes 1987; Arana and Baldessarini 1987). This work also indicates that excessive cortisol secretion is most likely to be present in depressed subjects who are inpatients, melancholic, severely de- pressed, and/or older (Sachar et al 1973; Carroll et al 1981; Halbreich et al 1985; Linkowski et al 1985; APA Task Force 1987; Arana and Baldessarini 1987; Rubin et al 1987; Stokes and Sikes 1987). More recent work has attempted to determine the mechanisms responsible for the HPA axis dysregulation associated with depression. © 1996 Society of Biological Psychiatry 0006-3223/96/$15.00 SSDI 0006-3223(95)00177-I

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Corticotropin-Releasing Hormone Prepubertal Major Depression
Challenge in
Boris Birmaher, Ronald E. Dahl, James Perel, Douglas E. Williamson, Beverly Nelson, Stacy Stull, Joan Kaufman, G. Scott Waterman, Uma Rao, Nga Nguyen, Joaquim Puig-Antich, and Neal D. Ryan
This study investigates cortisol and ACTH (corticotropin) responses to an infusion of human CRH (corticotropin-releasing hormone) in prepubertal children with major depressive disorder (MDD). Following a period of 24 hours of adaptation to the laboratory environment with an intravenous catheter in place, 34 children with MDD and 22 healthy controls received 1 txg/kg of human CRH at 5:00 PM. Blood samples for cortisol and ACTH were measured at baseline and post-CRH. Overall, there were no significant differences between the MDD and the normal controls in baseline or post CRH stimulation values of either cortisol or ACTH. Melancholic (n = 4) patients had significantly higher baseline cortisol levels than nonmel- ancholic (n = 24) patients. Compared with the outpatients and the nonmelancholics, the inpatients (n = 10) and the melancholics showed significantly lower total ACTH secretion (effect size: 0.9 and 1.4, respectively) after CRH infusion. These results are consistent with a broad literature suggesting that the HPA axis abnormalities occur less frequently in early-onset depression than reported in adult studies. The pattern of results in the subgroups of inpatients and in melancholic children, however, raise questions about possible continuities with adult studies.
Key Words: CRH, cortisol, ACTH, stress, child depression
BIOL PSYCHIATRY 1996;39:267--277
Introduction There is a considerable body of literature showing an association between adult major depressive disorder
From the Department of Psychiatry, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, Pittsburgh, PA; the Department of Psychiatry, University of Texas Medical Branch, Department of Psychiatry and Behavioral Sciences, Galveston, TX (NN); and the Department of Psychiatry, University of Vermont, College of Medicine, Burlington, VT.
Address reprint requests to Boris Birmaher, MD, Western Psychiatric Institute and Clinic, 3811 O'Hara Street Room #612BT, Pittsburgh, PA 15213.
Received April 29, 1994; revised March 14, 1995.
(MDD) and dysregulation of the hypothalamic-pituitary- adrenal (HPA) axis (Stokes and Sikes 1987; Arana and Baldessarini 1987). This work also indicates that excessive cortisol secretion is most likely to be present in depressed subjects who are inpatients, melancholic, severely de- pressed, and/or older (Sachar et al 1973; Carroll et al 1981; Halbreich et al 1985; Linkowski et al 1985; APA Task Force 1987; Arana and Baldessarini 1987; Rubin et al 1987; Stokes and Sikes 1987). More recent work has attempted to determine the mechanisms responsible for the HPA axis dysregulation associated with depression.
© 1996 Society of Biological Psychiatry 0006-3223/96/$15.00 SSDI 0006-3223(95)00177-I
268 BIOL PSYCHIATRY B. Birmaher et al 1996;39:267-277
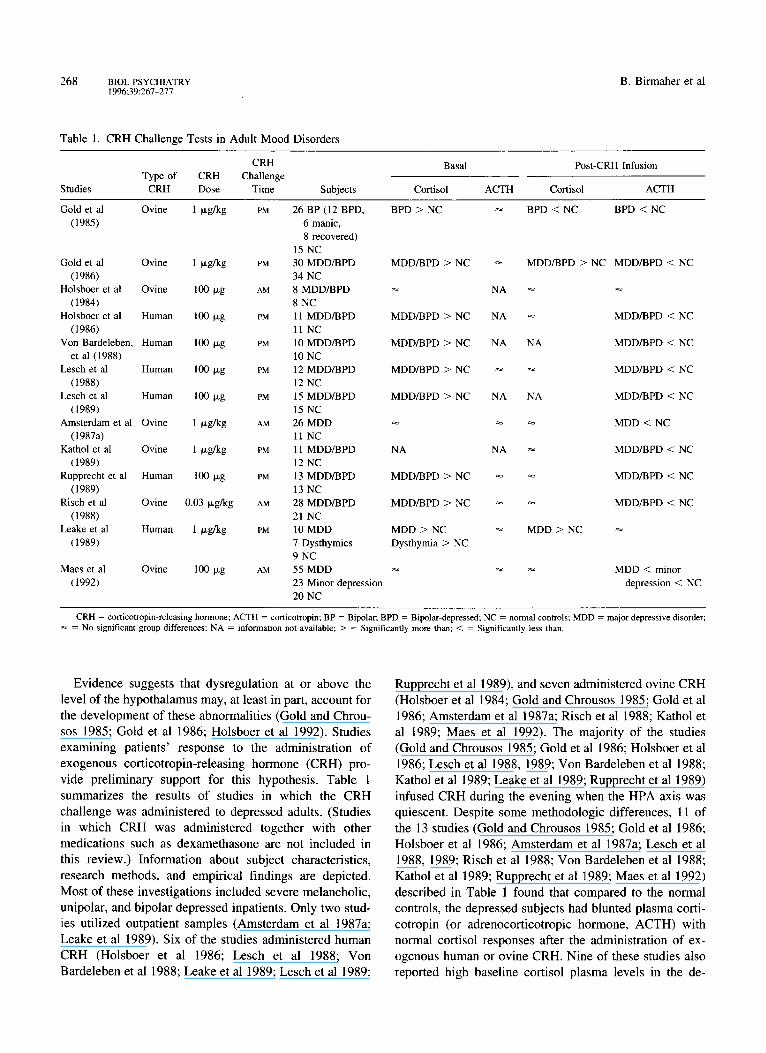
Table 1. CRH Challenge Tests in Adult Mood Disorders
CRH
Type of CRH Challenge
Studies CRH Dose Time Subjects
Basal Post-CRH Infusion
Cortisol A C T H Cortisol A C T H
Gold et al Ovine 1 I~g/kg PM 26 BP (12 BPD, BPD > NC ~ BPD < NC BPD < NC
(1985) 6 manic,
8 recovered)
15 NC
Gold et al Ovine 1 I.tg/kg PM 30 MDD/BPD MDD/BPD > NC ~ MDD/BPD > NC MDD/BPD < NC
(1986) 34 NC
Holsboer et al Ovine 100 i~g AM 8 MDD/BPD ~ NA ~
(1984) 8 NC
Holsboer et al Human 100 Ixg PM 11 MDD/BPD MDD/BPD > NC NA ~ MDD/BPD < NC
(1986) 11 NC
Von Bardeleben, Human 100 I~g PM 10 MDD/BPD MDD/BPD > NC NA NA MDD/BPD < NC
et al (1988) 10 NC
Lesch et al Human 100 tzg PM 12 MDD/BPD MDD/BPD > NC ~ ~ MDD/BPD < NC
(1988) 12 NC
Lesch et al Human 100 o,g PM 15 MDD/BPD MDD/BPD > NC NA NA MDD/BPD < NC
(1989) 15 NC
Amsterdam et al Ovine 1 i~g/kg AM 26 MDD ~- ~ ~ MDD < NC
(1987a) 11 NC
Kathol et al Ovine 1 ~,g/kg PM 11 MDD/BPD NA NA ~ MDD/BPD < NC
(1989) 12 NC
Rupprecht et al Human 100 p,g PM 13 MDD/BPD MDD/BPD > NC ~ ~ MDD/BPD < NC
(1989) 13 NC
Risch et al Ovine 0.03 I~g/kg AM 28 MDD/BPD MDD/BPD > NC ~ ~ MDD/BPD < NC
(1988) 21 NC
Leake et al Human 1 ~xg/kg PM 10 M DD MDD > NC ~ MDD > NC
(1989) 7 Dysthymics Dysthymia > NC
9 NC
Maes et al Ovine 100 ta, g AM 55 MDD ~- ~ ~ MDD < minor
(1992) 23 Minor depression depression < NC
20 NC
CRH = corticotropin-releasing hormone; ACTH = corticotropin; BP - Bipolar; BPD = Bipolar-depressed; NC = normal controls; MDD = major depressive disorder; = No significant group differences; NA = information not available; > = Significantly more than; < = Significantly less than.
Evidence suggests that dysregulation at or above the level of the hypothalamus may, at least in part, account for the development of these abnormalities (Gold and Chrou- sos 1985; Gold et al 1986; Holsboer et al 1992). Studies examining patients' response to the administration of exogenous corticotropin-releasing hormone (CRH) pro- vide preliminary support for this hypothesis. Table 1 summarizes the results of studies in which the CRH challenge was administered to depressed adults. (Studies in which CRH was administered together with other medications such as dexamethasone are not included in this review.) Information about subject characteristics, research methods, and empirical findings are depicted. Most of these investigations included severe melancholic, unipolar, and bipolar depressed inpatients. Only two stud- ies utilized outpatient samples (Amsterdam et al 1987a; Leake et al 1989). Six of the studies administered human CRH (Holsboer et al 1986; Lesch et al 1988; Von Bardeleben et al 1988; Leake et al 1989; Lesch et al 1989;
Rupprecht et al 1989), and seven administered ovine CRH (Holsboer et al 1984; Gold and Chrousos 1985; Gold et al 1986; Amsterdam et al 1987a; Risch et al 1988; Kathol et al 1989; Maes et al 1992). The majority of the studies (Gold and Chrousos 1985; Gold et al 1986; Holsboer et al 1986; Lesch et al 1988, 1989; Von Bardeleben et al 1988; Kathol et al 1989; Leake et al 1989; Rupprecht et al 1989) infused CRH during the evening when the HPA axis was quiescent. Despite some methodologic differences, 11 of the 13 studies (Gold and Chrousos 1985; Gold et al 1986; Holsboer et al 1986; Amsterdam et al 1987a; Lesch et al 1988, 1989; Risch et al 1988; Von Bardeleben et al 1988; Kathol et al 1989; Rupprecht et al 1989; Maes et al 1992) described in Table 1 found that compared to the normal controls, the depressed subjects had blunted plasma corti- cotropin (or adrenocorticotropic hormone, ACTH) with normal cortisol responses after the administration of ex- ogenous human or ovine CRH. Nine of these studies also reported high baseline cortisol plasma levels in the de-

CRH Challenge in Prepubertal Depression SlOL PSYCHIATRY 269 1996:39:267-277
pressed patients (Gold et al 1985, 1986; Holsboer et al 1986; Lesch et al 1988, 1989; Risch et al 1988; Von Bardeleben et al 1988; Leake et al 1989; Rupprecht et al 1989). The mechanisms responsible for these findings are not yet clear. It has been suggested that the blunted ACTH response to CRH may be due to the downregulation of pituitary postsynaptic CRH receptors induced by central hypersecretion of CRH (Gold and Chrousos 1985; Gold et al 1986; Holsboer et al 1992). Alternatively, some studies, but not all, have reported that pituitary hypersensitivity to may also explain the blunted nous CRH (Amsterdam et al Young et al 1990a; Holsboer tion of the HPA axis may also
high basal cortisol levels or cortisol negative feedback ACTH responses to exoge- 1987a; Lisanski et al 1989; et al 1992). The dysregula- be related to disturbances in
other neurotransmitters (e.g., norepinephrine), and neu- ropeptides (e.g., arginine-vasopressin) known to be asso- ciated with the regulation of CRH (Gillies et al 1982; Young et al 1990a; Holsboer et al 1992).
Our research group has been interested in early devel- opmental influences on HPA axis dysregulation associated with depression. In a number of previously published studies, we examined 24-hour baseline cortisol measures (Puig-Antich et al 1989; Dahl et al 1989, 1991) and cortisol response to dexamethasone (Birmaher et al 1992a, 1992b; Dahl et al 1992a). The depressed subjects in these studies were predominantly outpatient, and the measures (serum cortisol) were focused at the peripheral end of the HPA axis. The current study utilizes a CRH challenge test with measurement of cortisol and ACTH and includes both inpatient and outpatient MDD children and healthy normal controls. Thus, this study examines more central aspects of the HPA axis and includes a heterogeneous sample of children with MDD. To our knowledge, this is the first study measuring plasma cortisol and ACTH levels following the administration of intravenous CRH in chil- dren with MDD. Additionally, this study provides data from subjects who were primarily in theirfirst depressive episode, permitting an examination of the HPA axis in the early stages of depression.
Methods
Subjects Depressed children, aged 6-13 and in Tanner stage I or II of sexual development (Marshall and Tanner 1969, 1970), were recruited through the inpatient and outpatient Child and Adolescent Depression Program of Western Psychi- atric Institute and Clinic, University of Pittsburgh Medical Center. Children were evaluated by a research nurse using the School Age Schedule for Schizophrenia and Affective
Disorders Present Episode and Epidemiological (K- SADS-P and K-SADS-E, respectively) (Chambers et al 1985; Orvashel and Puig-Antich 1987) interviews, with both parent(s) and child as informants. In all cases a psychiatrist interviewed the child, confirmed the presence of each of the criteria symptoms for depressive disorder with the child and family, and reviewed all other diagnos- tic information. The diagnoses of affective disorders were made using unmodified adult Research Diagnostic Criteria (RDC) (Spitzer and Endicott 1978). The diagnoses of melancholic subtype and other nonaffective emotional disorders conformed to DSM-III criteria (APA 1980). The child was included in the study if he/she met medical inclusion/exclusion criteria described in the following, signed an assent form, and the parent(s) or guardian(s) signed informed consent. All children were reinterviewed using a short version of K-SADS-P for the past week during the psychobiologic protocol to confirm continued presence of MDD.
Control children were recruited through advertisement and personal contacts. They were aged 6-13, in Tanner stage I or II of sexual development, at low familial risk for depression, without medical illnesses, and without lifetime episode of any major psychiatric disorder. If an initial telephone screening of the family was promising, the child's psychiatric symptomatology was assessed using the K-SADS-E (Orvashel and Puig-Antich 1987) with both child and parent(s) or guardian(s) as informants. First- and second-degree relatives were interviewed using the K-SADS-E for relatives ages 6-18, and the Schedule for Schizophrenia and Affective Disorders-Life Time (SADS-L) (Endicott and Spitzer 1978) was used for adult relatives. Unavailable adult first- and second-degree rela- tives were assessed using the Family History--RDC technique with the child's parent(s) serving as the infor- mant(s). Low familial risk for depression was operation- ally defined as having no first-degree relative with a lifetime episode of any affective disorder, having no first- or second-degree relative with a lifetime episode of mania, schizoaffective disorder or schizophrenia, and having no more than 20% of second-degree relatives with a lifetime episode of MDD.
Exclusionary criteria were: (1) the use or presence of medication with central nervous system or hypothalamic- pituitary effects within the past 2 weeks; (2) neurologic, endocrinologic, or other significant medical illness; (3) gross obesity (weight greater than 150% of ideal body weight) or growth failure (height or weight under third percentile); (4) IQ less than 70; (5) anorexia nervosa, autism, or schizophrenia by DSM-III criteria; (6) inordi- nate fear of intravenous (IV) needles; (7) specific learning disabilities; and (8) Tanner stage III or greater of either breast or genital development.
270 BIOL PSYCHIATRY B. Birmaher et al 1996;39:267-277
Table 2. Demographics
MDD Normal (n = 34) (n = 22) Statistic p
Sex
Male/female 26/8 11/11 X 2 = 3.08 .08
Race
White/black/other 26/1/7 21/0/1 FET ~ NS
Age
(mean _+ SD) 10.4 -- 1.5 10.1 _+ 1.6 ta4 = 0.77 NS
SES
(mean _+ SD) 37.1 +_ 15.2 47.0 _+ 13.1 U = 493.5 .02
BMI
(mean ± SD) 18.8 _ 3.5 17.9 +_ 3.2 U = 309.0 NS
Percent Tanner II 47% 57% X 2 = 0.08 NS
MDD = major depressive disorder; SES = socioeconomic status; BMI = body mass index (kg/mZ); Tanner = Tanner stage of sexual development; FET = Fisher's Exact Test; U = Mann-Whitney U test; NS = nonsignificant.
Sample
A total of 56 prepubertal children, 34 with MDD and 22 normal controls, received CRH infusion. The cortisol measurements of all 56 subjects were available for data analysis; however, due to technical problems with the ACTH assay early in the study, only 42 subjects (28 MDDs and 14 normals) had ACTH data available. Demo- graphic characteristics of the sample are depicted in Table 2. The MDD and control groups were not significantly different with respect to age, race, sex, and body mass index (BMI) (kg/m2). The two groups differed on socio- economic status (SES) as measured by the Hollingshead four-factor index (Hollingshead 1975) (p = .03).
Within the MDD group, there were 13 inpatients and 21 outpatients; 4 met DSM-III criteria for melancholia (3 of these were inpatients); 11 met RDC criteria for definite endogenous subtype; and 9 were suicidal (defined as a patient with a definite suicidal plan or an attempt). Five depressed children had one previous MDD episode. The mean duration of the current episode was 34.4 ___ 30.9 weeks. The Hamilton depression rating scale (HDRS) (17 items) (Hamilton 1960) was extracted from the K-SADS-P as described by Williamson et al (1992). The mean extracted HDRS score was 17.2 _ 4.9. All patients were medication free prior to entry into the study.
The rate of comorbidity in the MDD population was relatively low: 2 subjects met criteria for conduct disorder, 3 met criteria for anxiety disorder, and 2 had lifetime diagnoses of attention deficit disorder with hyperactivity. These disorders preceded the onset of MDD.
Protocol
The CRH challenge was part of a comprehensive psycho- biological study of childhood MDD (e.g., Ryan et al
1992). All subjects (inpatients, outpatients, and healthy controls) came to the child and adolescent sleep/psycho- biology laboratory for a 5-day study. Sleep data have been reported by Dahl et al (1991, 1994). The actual protocol was split into two segments (each lasting 2-3 days) to permit the protocol to be conducted over 2 weekends, thus minimizing interference with school schedules.
The CRH challenge test occurred during the first seg- ment of the protocol. All subjects came to the laboratory and had an intravenous catheter placed in an antecubital vein, which was then kept open by a slow drip of heparinized saline with a mobile system allowing a free range of activities. The first evening and night were strictly for adaptation. Children participated in numerous age-appropriate activities in a pleasant, low-stress envi- ronment. On the second night, baseline EEG and plasma sampling were collected with subjects following their usual home schedule, which was determined by sleep logs during the previous week. At 9:00 AM on the following morning, the subjects had a growth hormone releasing hormone (GHRH) challenge test. The remainder of the day was spent at leisure on the unit, including movies and games with staff. At 5:00 PM ( a time when HPA activity is relatively quiescent) (Puig-Antich et al 1989), 1.0 Ixg/kg of human CRH was given as an IV infusion over 2 minutes. Basal blood samples for cortisol and ACTH were obtained at - 30 , - 15 , and 0 minutes pre-CRH infusion. Following CRH infusion, blood samples were obtained at +15, +30, +60, +90, +120, +150, and +180 minutes. Blood samples were immediately centrifuged under refrig- eration, and plasma was carefully separated and stored at - 80°C until assayed. There were no significant side effects from the CRH infusion. A few children had a mild transient tingling sensation in their arms while the CRH was infused, but most subjects were completely unaware of the infusion. Two children had mild facial flushing during or immediately after the infusion.
It is important to mention that the indwelling catheter by itself may cause stress and influence the CRH challenge test; however, as described above, in this study the CRH challenge test was done after subjects adapted to the laboratory environment and the indwelling catheter. A previous report of subjects who had participated in a similar protocol found that the degree of subjective stress experienced was quite low and that the indwelling catheter as a rule caused little discomfort (Townsend et al 1988).
Hormone Assays
CORTISOL Cortisol levels were determined from 25 ixl sample assayed in duplicate. The procedure used was the Diagnostic Products solid phase 1251 radioimmunoas- say for cortisol. This method is sensitive to 13.79 nmol/L
CRH Challenge in Prepubertal Depression BIOL PSYCHIATRY 271 1996;39:267-277
(0.5 Ixl/dL) of cortisol. Patient duplicates exceeding a 5.0% coefficient of variation were reassayed. The intraas- say coefficient of variation ranged from 1.3%-2.7% with a mean of 1.9%. Interassay variation ranged from 11.7% CV at 103.7 nmol/L (3.76 Ixl/dL) to 7.0% CV at 839.0 nmol/L (30.4 txl/dL).
ACTHo TO optimize the sensitivity with small plasma samples, the procedure used for determination of adreno- corticotropic hormone (ACTH) was a slightly modified version of the double antibody, 12sI radioimmunoassay developed by Radioassay Systems Laboratories, Inc. This assay detected both the 1-39 and 1-24 molecular forms of human ACTH. The sample size used for determination of ACTH was approximately 100 ixl. Blood samples were collected with EDTA, aprotinin for protease inhibition, and n-ethylmaleimide for stability, and frozen at -80°C.
The limit of detectability was 1.1 pmol/L (5 pg/mL); the range of the coefficient of variation (CV) was 1.5-9.0% with an upper limit of 11.0 pmol/L (50 pg/mL) for linearity. The ACTH samples were diluted and measured with reliability at 1.1-22.0 pmol/L (5-100 pg/mL). The interday variation for the assay ranged from 9.3% CV (mean of 11.8 pmol/L) to 19.9% CV (mean of 1.9 pmol/L).
Statistical Methods
Sample characteristics were compared using t, X 2, and Fisher' s Exact tests as appropriate. The cortisol and ACTH data were analyzed with linear interpolation to fill in occasional missing values. The cortisol measurements of all 56 subjects (34 MDD and 22 normals) were available for data analysis. As stated in the sample description, data on ACTH consisted of a total of 42 subjects (28 MDD and 14 normals). In those subjects who had cortisol and ACTH data available, problems with missing data were minimal (for cortisol = 0.2%; for ACTH measurements 2.3%).
Between-group differences in cortisol and ACTH were assessed using analysis of variance (ANOVA) on the following variables: baseline, total post-CRH, peak, and net response. The baseline values were computed by determining the mean of the three cortisol and ACTH samples taken at - 30 , - 1 5 , and 0 minutes pre-CRH infusion. The total post-CRH scores were computed by determining the area under the curve (AUC) using the five cortisol and ACTH samples obtained between 0 and 120 minutes post-CRH infusion. The peak scored was the highest cortisol and ACTH value after the administration of CRH. The net response scores were computed by subtracting the mean baseline values from the five post- CRH draws and calculating an AUC of the difference scores. AUCs were calculated using the trapezoidal rule.
Data distributions were examined for normality using the Shapiro and Wilkes W statistic (Shapiro and Wilkes 1965); where significantly non-normal distributions were found, logarithmic transformations were performed to normalize the distributions before applying parametric tests. In cases where no transformation normalized the data, nonparametric tests (Mann-Whitney rank sum test, Spearman correlation) were used. Analysis of covariance (ANCOVA) was used to test effects of age, sex, body mass index (BMI), Tanner stage, and SES. All values in the text are reported as means ___ standard deviations (SD). All p values are based on two-tailed tests.
R e s u l t s
A CTH Measures
MDD VS. NORMAL CONTROLS. Human CRH reliably increased ACTH secretion in both MDDs and normal controls. Peak ACTH levels occurred at the 15-minute sample and returned to baseline levels at approximately 90 minutes. In depressed adults, the peak and return to baseline have been reported at approximately 30-45 and 90 minutes, respectively (Holsboer et al 1986; Muller and yon Werder 1991). In normal children and adults, the ACTH peak has been reported to occur 10 minutes after human CRH administration (Attansio et al 1987). Overall, there were no significant differences between the MDDs and the normal controls on baseline, total post-CRH, peak, or net ACTH secretion (Figure 1, Table 3). Also, there were no between-group differences in ACTH time to peak or time to return to baseline after CRH infusion (Figure 1).
CONTRASTS AMONG SUBGROUPS OF C H I L D H O O D DEPRES-
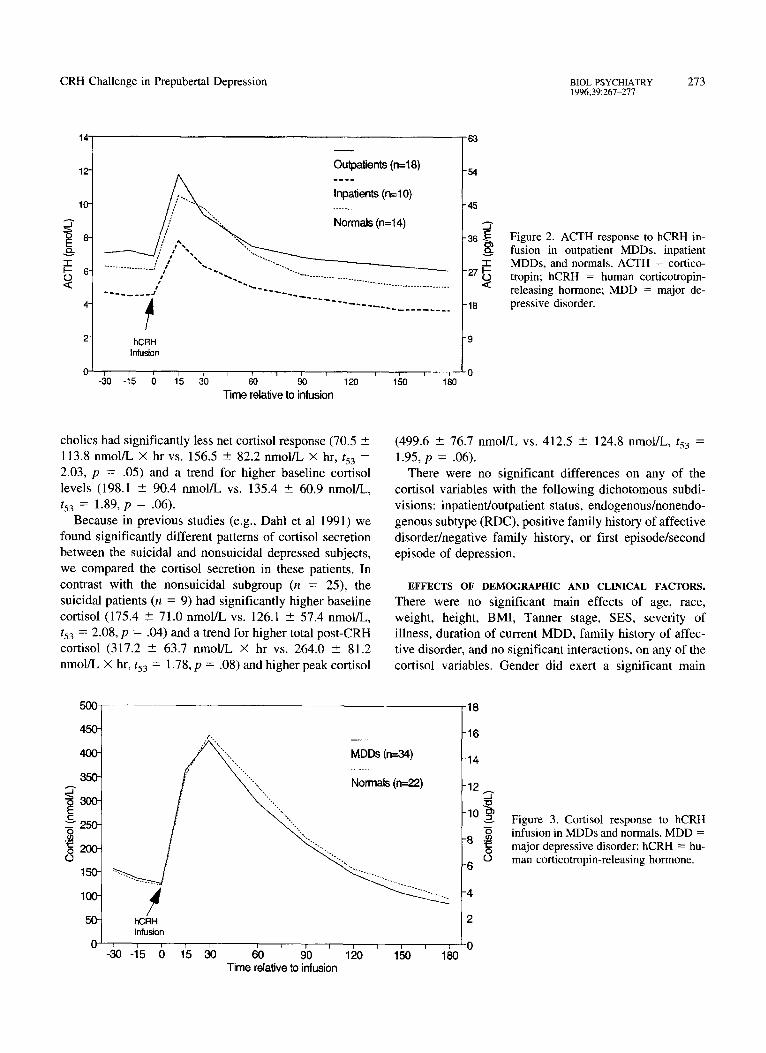
SIVES. Because most of the HPA abnormalities reported in the adult MDD literature were mainly reported in the inpatient and melancholic depressed subgroups, we con- ducted post hoc analysis in these subgroups. In contrast with the outpatient subgroup (n = 18), the inpatients (n = 10) (Figure 2) had significantly lower total post-CRH ACTH (5.3 -+ 1.3 pmol/L × hr vs. 8.0 - 3.4 pmol/L × hour, t39 = 2.20, p = 0.03) (effect size: 0.90), and trends toward lower baseline ACTH (4.6 - 0.8 pmol/L vs. 7.0 -+ 3.7 pmol/L, /39 = 1.95, p = .06), and lower peak ACTH (7.9 --- 3.6 pmol/L vs. 11.8 - 6.1 pmol/L, t39 = 1.95, p = .06). There were no statistically significant differences in the net ACTH response parameter (0.7 --- 0.7 pmol/L × hr vs. 1.0 _+ 1.4 pmol/L X hr, t39 = -0 .6 , p = NS). Compared with the normal controls, the inpatients tended to have lower ACTH secretion across all ACTH measures. None of these comparisons reached statistical significance, which may have been attributable to the small sample sizes.

272 BIOL PSYCHIATRY B. Birmaher et al 1996;39:267 277
14
12-
10-
0 8" E
-1-
,<
2-
MDDs (n--28)
. . . . . 1 4 ) hCRH
Infusion
~o 15 6 15 ~o ~o 9o 1~o 1~o 1~o "time relative to infusion
63
-54
-45
-36
-27 <0 ~
-18
-9
0
Figure 1. ACTH response to hCRH in- fusion in MDDs and normals. ACTH = corticotropin; hCRH = human cortico- tropin-releasing hormone; MDD = ma- jor depressive disorder.
The melancholics (n = 4) also had a significantly lower total post-CRH ACTH levels (4.3 _ 1.0 pmol/L x hr vs. 7.5 _ 3.1 pmol/L x hr, t39 = 2.21, p = .03) (effect size: 1.4), and a trend toward lower ACTH peak values (6.5 -_+ 3.2 pmol/L vs. 11.1 ± 5.7 pmol/L, t39 = 1.90, p = .06) compared to the nonmelancholics (n = 24). There were no statistically significant differences in the net ACTH re- sponse (melancholics: 0.3 ± 0.9 pmol/L X hr vs. nonmel- ancholics: 1.0 ___ 1.2 pmol/L x hr). Compared with the normal controls, the melancholics had a trend for lower ACTH peak (6.5 -+ 3.2 pmol/L vs. 11.0 --- 5.7 pmol/L, t39 = 1.80, p = .08). Because three of the four melancholics were inpatients, to determine if the inpatient differences were accounted for by the effects of melancholia, the melancholics were removed from both the inpatient and outpatient groups and the analyses reconducted. There was a trend for the inpatients (n = 7) from this reduced sample to have lower total post-CRH ACTH (5.6 -+ 1.3 pmol/L X hr vs. 8.3 ± 3.3 pmol/L X hr, t35 = 1.88, p = .07) and a trend for lower peak levels (8.1 + 4.0 pmol/L vs. 12.3 ___ 6.0 pmol/L, t35 = 1.95, p = 0.06) than the reduced outpatient sample (n = 17).
Table 3. ACTH Summary Variables: Comparison between MDDs and Normal Controls
MDD Normal
(n = 28) (n = 14) Statistic p
Baseline (pmol/L) 6.2 -+ 3.2 6.1 -+ 3.3 t4o = 0.01 NS
Total post-CRH 7.0 -+ 3.1 7.4 -+ 3.7 t4o = 0.32 NS (pmol/L × hr)
Peak (pmol/L) 10.4 _+ 5.6 11.0 _+ 5.7 t4o = 0.43 NS
Net A C T H response 0.9 -+ 1.2 1.2 -+ 0.9 t40 = 1.00 NS
(pmol/L × hr)
ACTH = corticotropin; MDD = major depressive disorder; CRH = human corticotropin-releasing hormone; AUC = area under the curve; NS = nonsignifi- cant.
The following dichotomous subdivisions of the MDD children failed to detect any significant differences on the ACTH measures: endogenous/nonendogenous subtype (RDC), suicidal/nonsuicidal, or first episode/second epi- sode of depression.
EFFECTS OF DEMOGRAPHIC AND CLINICAL FACTORS.
There were no significant main effects of age, gender, race, BMI, Tanner stage, SES, severity of illness, duration of current MDD, family history of affective disorder, and no significant interactions, on any of the ACTH variables.
Cortisol Measures
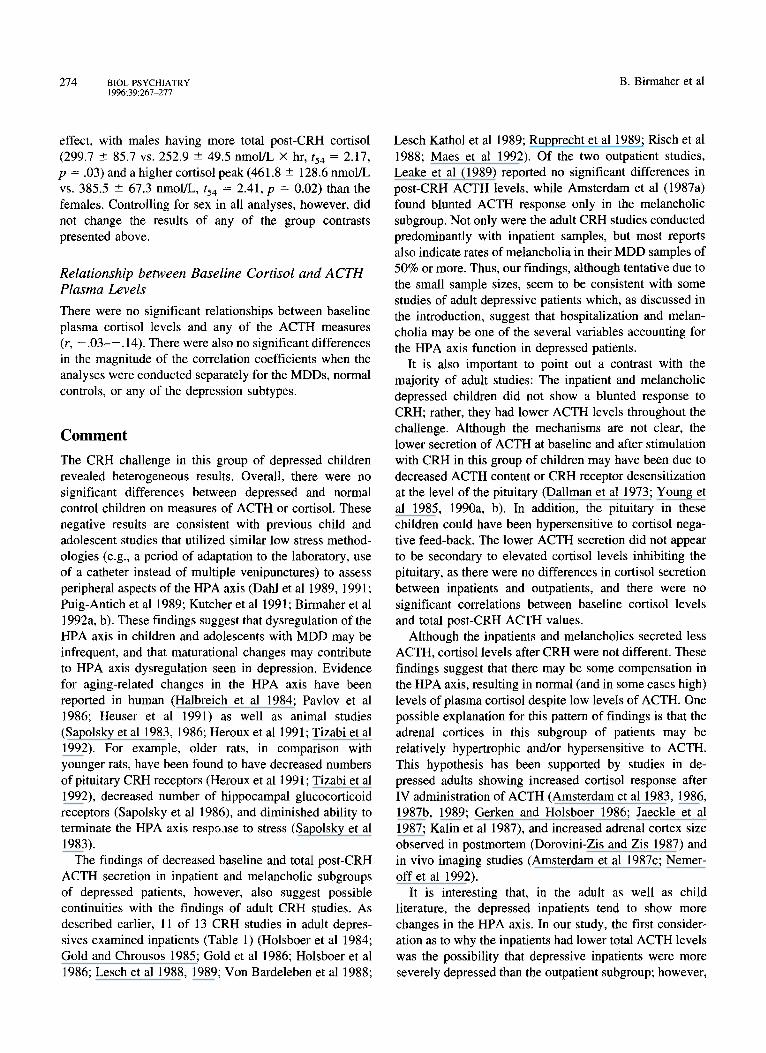
MDD VS, NORMAL CONTROLS, CRH reliably increased cortisol secretion in both MDDs and normal controls. Cortisol reached the peak and returned to baseline levels approximately at 30 and 120 minutes, respectively. In adults, the peak and return to baseline have been reported at approximately 4 5 - 6 0 and 90 minutes, respectively (Holsboer et al 1986, Muller and von Werder 1991). There were no significant differences on any of the cortisol variables between the MDD and the normal control groups (Figure 3). In addition, there were no between-group differences in cortisol time to peak and time to return to baseline after the CRH infusion.
CONTRASTS AMONG SUBGROUPS OF C H I L D H O O D DEPRES-
SIVES. In contrast with the MDD nonmelancholic sub- group, the melancholies (n = 4) had significantly higher baseline cortisol (198.1 + 90.4 nmol/L vs. 131.3 ± 57.3 nmol/L, t53 = -2 .06 , p = .04) (effect size: 0.85) and a trend lower net cortisol response (70.5 -+ 113.8 nmol/L x hr vs. 148.1 + 69.6 nmol/L X hr, t53 = 1.87, p = .07). In comparison with the normal control group, the melan-
CRH Challenge in Prepubertal Depression BIOL PSYCHIATRY 273 1996;39:267-277
14
12"
tO-
"l- I-- 6"- o <
4-
2
O'
Outpatients (n=18)
" . Normals (n=14)
hCRH Infusion
-~o-~s 6 t'5 ~o ' ~o ' ~o ' 120 ' Time relative to infusion
"9
1--50 , --r--180 "0
63
-54
-45
-36
"27 <
-18
Figure 2. ACTH response to hCRH in- fusion in outpatient MDDs, inpatient MDDs, and normals. ACTH = cortico- tropin; hCRH = human corticotropin- releasing hormone; MDD = major de- pressive disorder.
cholics had significantly less net cortisol response (70.5 ___ 113.8 nmol/L X hr vs. 156.5 - 82.2 nmol/L × hr, t 5 3 :
2.03, p = .05) and a trend for higher baseline cortisol levels (198.1 ___ 90.4 nmol/L vs. 135.4 ± 60.9 nmol/L, t53 : 1.89, p = .06).
Because in previous studies (e.g., Dahl et al 1991) we found significantly different patterns of cortisol secretion between the suicidal and nonsuicidal depressed subjects, we compared the cortisol secretion in these patients. In contrast with the nonsuicidal subgroup (n = 25), the suicidal patients (n = 9) had significantly higher baseline cortisol (175.4 ± 71.0 nmol/L vs. 126.1 ___ 57.4 nmol/L, t53 = 2.08, p = .04) and a trend for higher total post-CRH cortisol (317.2 --- 63.7 nmol/L X hr vs. 264.0 --- 81.2 nmol/L x hr, t53 = 1.78, p = .08) and higher peak cortisol
(499.6 ___ 76.7 nmol/L vs. 412.5 -4- 124.8 nmol/L, t53 = 1.95, p --- .06) .
There were no significant differences on any of the cortisol variables with the following dichotomous subdi- visions: inpatient/outpatient status, endogenous/nonendo- genous subtype (RDC), positive family history of affective disorder/negative family history, or first episode/second episode of depression.
EFFECTS OF DEMOGRAPHIC AND CLINICAL FACTORS. There were no significant main effects of age, race, weight, height, BMI, Tanner stage, SES, severity of illness, duration of current MDD, family history of affec- tive disorder, and no significant interactions, on any of the cortisol variables. Gender did exert a significant main
5OO
450-
400-
35O-
E t - -
v 250-
0 150-
100-
5O-
0
Y hCl=llt Infusion
MDDs (n=34)
Normals (n--22)
-30 "15 () I~5 30 ~ ~ ) ' 9'0 ' 120 ' If~O ' I~30 Time relative to infusion
-18
1 6
-14
~12
10 ~
o 6
-4
2
0
Figure 3. Cortisol response to hCRH infusion in MDDs and normals. MDD = major depressive disorder; hCRH = hu- man corticotropin-releasing hormone.
274 BIOL PSYCHIATRY B. Birmaher et al 1996;39:267-277
effect, with males having more total post-CRH cortisol (299.7 ___ 85.7 vs. 252.9 _+ 49.5 nmol/L × hr, / 54 : 2.17, p = .03) and a higher cortisol peak (461.8 + 128.6 nmol/L vs. 385.5 _+ 67.3 nmol/L, t54 = 2.41, p = 0.02) than the females. Controlling for sex in all analyses, however, did not change the results of any of the group contrasts presented above.
Relationship between Baseline Cortisol and ACTH Plasma Levels
There were no significant relationships between baseline plasma cortisol levels and any of the ACTH measures (r, - . 0 3 - - . 14). There were also no significant differences in the magnitude of the correlation coefficients when the analyses were conducted separately for the MDDs, normal controls, or any of the depression subtypes.
Comment
The CRH challenge in this group of depressed children revealed heterogeneous results. Overall, there were no significant differences between depressed and normal control children on measures of ACTH or cortisol. These negative results are consistent with previous child and adolescent studies that utilized similar low stress method- ologies (e.g., a period of adaptation to the laboratory, use of a catheter instead of multiple venipunctures) to assess peripheral aspects of the HPA axis (Dahl et al 1989, 1991; Puig-Antich et al 1989; Kutcher et al 1991; Birmaher et al 1992a, b). These findings suggest that dysregulation of the HPA axis in children and adolescents with MDD may be infrequent, and that maturational changes may contribute to HPA axis dysregulation seen in depression. Evidence for aging-related changes in the HPA axis have been reported in human (Halbreich et al 1984; Pavlov et al 1986; Heuser et al 1991) as well as animal studies (Sapolsky et al 1983, 1986; Heroux et al 1991; Tizabi et al 1992). For example, older rats, in comparison with younger rats, have been found to have decreased numbers of pituitary CRH receptors (Heroux et al 1991; Tizabi et al 1992), decreased number of hippocampal glucocorticoid receptors (Sapolsky et al 1986), and diminished ability to terminate the HPA axis resp.vase to stress (Sapolsky et al 1983).
The findings of decreased baseline and total post-CRH ACTH secretion in inpatient and melancholic subgroups of depressed patients, however, also suggest possible continuities with the findings of adult CRH studies. As described earlier, 11 of 13 CRH studies in adult depres- sives examined inpatients (Table 1) (Holsboer et al 1984; Gold and Chrousos 1985; Gold et al 1986; Holsboer et al 1986; Lesch et al 1988, 1989; Von Bardeleben et al 1988;
Lesch Kathol et al 1989; Rupprecht et al 1989; Risch et al 1988; Maes et al 1992). Of the two outpatient studies, Leake et al (1989) reported no significant differences in post-CRH ACTH levels, while Amsterdam et al (1987a) found blunted ACTH response only in the melancholic subgroup. Not only were the adult CRH studies conducted predominantly with inpatient samples, but most reports also indicate rates of melancholia in their MDD samples of 50% or more. Thus, our findings, although tentative due to the small sample sizes, seem to be consistent with some studies of adult depressive patients which, as discussed in the introduction, suggest that hospitalization and melan- cholia may be one of the several variables accounting for the HPA axis function in depressed patients.
It is also important to point out a contrast with the majority of adult studies: The inpatient and melancholic depressed children did not show a blunted response to CRH; rather, they had lower ACTH levels throughout the challenge. Although the mechanisms are not clear, the lower secretion of ACTH at baseline and after stimulation with CRH in this group of children may have been due to decreased ACTH content or CRH receptor desensitization at the level of the pituitary (Dallman et al 1973; Young et al 1985, 1990a, b). In addition, the pituitary in these children could have been hypersensitive to cortisol nega- tive feed-back. The lower ACTH secretion did not appear to be secondary to elevated cortisol levels inhibiting the pituitary, as there were no differences in cortisol secretion between inpatients and outpatients, and there were no significant correlations between baseline cortisol levels and total post-CRH ACTH values.
Although the inpatients and melancholics secreted less ACTH, cortisol levels after CRH were not different. These findings suggest that there may be some compensation in the HPA axis, resulting in normal (and in some cases high) levels of plasma cortisol despite low levels of ACTH. One possible explanation for this pattern of findings is that the adrenal cortices in this subgroup of patients may be relatively hypertrophic and/or hypersensitive to ACTH. This hypothesis has been supported by studies in de- pressed adults showing increased cortisol response after IV administration of ACTH (Amsterdam et al 1983, 1986, 1987b, 1989; Gerken and Holsboer 1986; Jaeckle et al 1987; Kalin et al 1987), and increased adrenal cortex size observed in postmortem (Dorovini-Zis and Zis 1987) and in vivo imaging studies (Amsterdam et al 1987c; Nemer- off et al 1992).
It is interesting that, in the adult as well as child literature, the depressed inpatients tend to show more changes in the HPA axis. In our study, the first consider- ation as to why the inpatients had lower total ACTH levels was the possibility that depressive inpatients were more severely depressed than the outpatient subgroup; however,

CRH Challenge in Prepubertal Depression BIOL PSYCHIATRY 275 1996;39:267-277
comparing the total score from the HDRS, or the 12 items from the depression section from the K-SADS-P, revealed no significant between-group differences in severity of depression between inpatients and outpatients. Addit ion- ally, the inpatient depressed children were next compared to the outpatients on a variety of demographic and clinical variables (e.g., age, sex, race, SES, HDRS). Of these variables, only SES was significantly different, with the inpatients having lower SES on the Holl ingshead four- factor i tem (29.6 ± 15.2 vs. 41.9 ± 13.4; Mann-Whitney = 68.0; p = .02). After entering SES as a covariate, however, the inpatients still showed significantly lower ACTH levels compared to outpatients (for total post-CRH, p = .05; for peak, p --- .03). Thus, demographic and clinical variables failed to explain the effect of inpatient status on the total ACTH secretion.
CRH is one of the primary effectors of physiologic stress responses (Chrousos and Gold 1992). Further, the process of hospitalization (APA Task Force 1987; Casat et al 1989; Birmaher et al 1992a,b; Dahl et al 1992a), exposure to acute and chronic stressors (Breier et al 1988; Guerra et al 1993; DeBellis et al 1994), and stress in animals (Dallman and Jones 1973; DeSouza and Van
Loon 1982; Young and Akil 1985; Young et al 1990b) have been shown to influence the HPA axis (Traskman et al 1980; Calloway et al 1984; Dolan et al 1985; Roy et al 1987). Therefore, stress could, at least in part, account for some differences in the total ACTH secretion between inpatients and outpatients. Unfortunately, in this study we did not measure the children 's exposure and perception of stress before and during the first days of hospitalization. These issues and other variables, such as age, severity of depression, melancholic features, and their interactions, need to be carefully examined in future studies of the HPA axis system.
The authors would like to acknowledge the important contributions of the clinical interviewers from the Program Project and the staff of the Child and Adolescent Sleep Laboratory. The authors also would like to acknowledge Dr. David J. Kupfer and Dr. David A. Brent for their critical review and comments of this article. The authors thank Therese Delseroth and Deborah Small for their assistance in the preparation of this manuscript.
This paper is dedicated to the memory of Joaquim Puig-Antich, MD, who died in December 1989.
These data were presented at the 48th Annual meeting of The Society For Biological Psychiatry held in San Francisco, California, 1993.
References American Psychiatric Association (1980): Diagnostic and Sta-
tistical Manual of Mental Disorders, 3rd ed. Washington DC: American Psychiatric Association.
APA Task Force on Laboratory Tests in Psychiatry (1987): The dexamethasone suppression test: An overview of its current status in psychiatry. Am J Psychiatry 144:1253-1262.
Amsterdam JD, Winokur A, Abelman E, Lucki I, Rickels K (1983): Cosyntropin (ACTH ~-2) stimulation test in depressed patients and healthy subjects. Am J Psychiatry 140:907-909.
Amsterdam JD, Maislin G, Abelman E, Bernish N, Winokur A (1986): Adrenocortical responsiveness to the ACTH stimula- tion test in depressed patients and healthy volunteers. J Affective Disord 11:265-274.
Amsterdam JD, Maislin G, Winokur A, Kling M, Gold P (1987a): Pituitary and adrenocortical responses to the ovine corticotropin releasing hormone in depressed patients and healthy volunteers. Arch Gen Psychiatry 44:775-781.
Amsterdam JD, Maislin G, Droba M, Winokur A (1987b). The ACTH stimulation test before and after clinical recovery from depression. Psychiatry Res 20:325-336.
Amsterdam JD, Marinelli DL, Arger P, Winokur A (1987c): Assessment of adrenal gland volume by computed tomogra- phy in depressed patients and healthy volunteers: A pilot study. Psychiatry Res 21:189-197.
Amsterdam JD, Maislin G, Berwish N, Phillips J, Winokur A (1989): Enhanced adrenocortical sensitivity to submaximal doses of cosyntropin ( t 1-24 corticotropin) in depressed pa- tients. Arch Gen Psychiatry 46:550-554.
Arana GW, Baldessarini J (1987): Clinical use of the dexameth- asone suppression test in psychiatry. In HY. Meltzer (ed),
Psychopharmacology: The Third Generation of Progress. New York: Raven Press, pp 609-615.
Attanasio A, Robkamp R, Bernasconi S, et al (1987): Plasma adreno-corticotropin, cortisol, and dehydroepiandrosterone response to corticotropin releasing factor in normal children during pubertal development. Pediatr Res 22:41-44.
Birmaher B, Ryan ND, Dahl R, et al (1992a): Dexamethasone suppression test in children with major depressive disorder. J Am Acad Child Adolesc Psychiatry 31:291-297.
Birmaher B, Dahl RE, Ryan ND, et al (1992b): Dexamethasone suppression test in adolescent outpatients with major depres- sive disorder. Am J Psychiatry 149:1040-1045.
Breier A, Kelsoe JR, Kirwin PD, Belier SA, Wolkowitz OM, Pickar D (1988): Early parental loss and development of adult psychopathology. Arch Gen Psychiatry 45:987-993.
Calloway SP, Dolan ILl, Fonagy P, DeSouzo VFA, Wakeling A (1984): Endocrine changes and clinical profiles in depression: I. The dexamethasone suppression test. Psychol Med 14:749-758.
Carroll BJ, Feinberg M, Greden JF, et al (1981): A specific laboratory test for the diagnosis of melancholia. Arch Gen Psychiatry 38:15-22.
Casat CD, Arana GD, Powel K (1989): The DST in children and adolescents with major depressive disorder. Am J Psychiatry 146:503-507.
Chambers WJ, Puig-Antich J, Hirsh M, et al (1985): The assessment of affective disorders in children and adolescents by semi-structured interview test-retest reliability. Arch Gen Psychiatry 42:696-702.
Chrousos GP, Gold PW (1992): The concepts of stress and stress
276 BIOL PSYCHIATRY B. Birmaher et al 1996;39:267-277
disorders: Overview of physical and behavioral homeostasis. JAMA 267:1244-1252.
Dahl RE, Puig-Antich J, Ryan ND, et al (1989): Cortisol secretion in adolescents with major depressive disorder. Acta Psychiatr Scand 80; 18-26.
Dahl RE, Ryan ND, Birmaher B, et al (1991): EEG sleep measures in prepubertal depression. Psychiatr Res 38:201-214.
Dahl RE, Kaufman J, Ryan ND, et al (1992): The dexamethasone suppression test in children and adolescents: A review and a controlled study. Biol Psychiatry 31(4):600-605.
Dahl RE, Ryan ND, Perel J, et al (1994): Cholinergic REM induction test with arecoline in depressed children. Psychiatry Res 51:269-282.
Dallman MF, Jones MT (1973): Corticosteroid feedback control of ACTH secretion: Effect of stress-induced corticosterone secretion on subsequent stress responses in the rat. Endocri- nology 92:1367-1375.
DeBellis MD, Chrousos GP, Dorn LD, et al (1994): Hypotha- lamic-pituitary-adrenal axis dysregulation in sexually abused girls. J Clin Endocrinol Metab 78:249-255.
deSouza EB, van Loon GR (1982): Stress-induced inhibition of the plasma corticosterone response to a subsequent stress in rats. A nonadrenocorticotropin-mediated mechanism. Endo- crinology 110:23-33.
Dolan RJ, Calloway SP, Fonagy P, DeSouza FVA, Wakeling A (1985): Life events, depression and hypothalamic-pituitary- adrenal axis function. Br J Psychiatry 147:429-433.
Doravini-Zis K, Zis A (1987): Increased adrenal weight in victims of violent suicide. Am J Psychiatry 144:1214-1216.
Endicott J, Spitzer RL (1978): Schedule for Affective Disorders and Schizophrenia--Lifetime version. Arch Gen Psychiatry 35:837-844.
Gerken A, Holsboer F (1986): Cortisol and corticosterone response after syncorticotropin in relationship to dexametha- sone suppressibility of cortisol. Psychoneuroendocrinology 11:185-194.
Guerra G, Caccavari R, Delsignore R, et al (1993): Parental divorce and neuroendocrine changes in adolescents. Acta Psychiatr Scand 87:350-354.
Gillies GE, Linton EA, Lowry PJ (1982): Corticotropin releasing activity of the new CRF is potentiated several times by vasopressin. Nature 299:355-357.
Gold PW, Chrousos GP (1985): Clinical studies with cortico- tropin releasing factor: Implications for the diagnosis and pathophysiology of depression, Cushing's disease, and adre- nal insufficiency. Psychoneuroendocrinology 10:410-419.
Gold PW, Loriaux L, Roy A, et al (1986): Responses to corti- cotropin-releasing hormone in the hypercortisolism of depres- sion and Cushing's disease. N Engl J Med 314:1329-1335.
Halbreich U, Asnis GM, Zumoff B, Nathan RS, Shindledecker R (1984): Effect of age and sex on cortisol secretion in depressives and normals. Psychiatr Res 13:221-229.
Halbreich U, Asnis GM, Shindledecker R, Zumoff B, Nathan RS (1985): Cortisol secretion in endogenous depression. Arch Gen Psychiatry 42:904-908.
Hamilton M (1960): A rating scale for depression. J Neurol Neurosurg Psychiatry 23:56-61.
Heroux JA, Grigoriades DE, DeSouza EB (1991): Age-related
diseases in corticotropin-releasing factor receptors in rat brain and anterior pituitary gland. Brain Res 542:155-158.
Heuser I, Wark HJ, Keul J, Holsboer F (1991): Altered pituitary- adrenocortical function in elderly endurance athletes. J Clin Endocrinol Metab 73:485-488.
Hollingshead AB (1975): Four-Factor Index of Social Status. New Haven, CT: Yale University Sociology Department.
Holsboer F, von Bardeleben U, Gerken A, Stalla GK, Muller OA, Steiger A (1984): Blunted corticotropin and normal cortisol response to human corticotropin-releasing factor in depres- sion. N Engl J Med 311 : 1127.
Holsboer F, Gerken A, von Bardeleben U, et al (1986): Human corticotropin-releasing hormone in depression. Biol Psychia- try 21:601-611.
Holsboer F, Spengler D, Heuser I (1992): The role of cortico- tropin-releasing hormone in the pathogenesis of Cushing's disease, anorexia nervosa, alcoholism, affective disorders and dementia. Prog Brain Res 93:385-417.
Jaeckle RS, Kathol RG, Lopez JF, Meller WH, Krummel SJ (1987): Enhanced adrenal sensitivity to exogenous ACTH, 1-24 stimulation in major depression: Relationship to dexa- methasone suppression test results. Arch Gen Psychiatry 44:233-240.
Kalin NH, Dawson G, Torcot P, et al (1987): Function of the adrenal cortex in patients with major depression. Arch Gen Psychiatry 44:233-240.
Kathol RG, Jaeckle RS, Lopez JF, Miller WH (1989): Consistent reduction of ACTH responses to stimulation with CRH, vasopressin and hypoglycemia in patients with major depres- sion. Br J Psychiatry 155:468-478.
Kutcher S, Malkin D, Silverberg J, et al (1991): Nocturnal cortisol, thyroid stimulating hormone, and growth hormone secretory profiles in depressed adolescents. J Am Acad Child Adolesc Psychiatry 30:407-414.
Leake A, Griffiths AW, Ferrier IN (1989): Plasma N-POMC, ACTH and cortisol following hCRH administration in major depression and dysthymia. J Affective Disord 17:57-64.
Lesch KP, Laux G, Schulte HM, Pfuller H, Beckmann H (1988): Corticotropin and cortisol response to human CRH as a probe for HPA system integrity in major depressive disorder. Psychiatry Res 24:25-34.
Lesch KP, Muller U, Rupprecht R, Kruse K, Schulte HM (1989): Endocrine responses to growth hormone-releasing hormone, thyrotropin-releasing hormone and corticotropin-releasing hormone in depression. Acta Psychiatry Scand 79:597-602.
Linkowski P, Mendlewicz J, LeClerq R, et al (1985): The 24-hour profile of adrenocorticotropin and cortisol in major depressive illness. J Clin Endocrinol Metab 61:429-438.
Lisanski J, Peake GT, Strassman RJ, et al (1989): Augmented pituitary corticotropin response to a threshold dosage of human corticotropin-releasing hormone in depressives pre- treated with metyrapone. Arch Gen Psychiatry 46:641-649.
Maes M, Claes M, Vandewoude M, et al (1992): Adrenocorti- cotropin hormone, [3-endorphin and cortisol responses to oCRF in melancholic patients. Psychol Med 2:317-329.
Marshall WA, Tanner JM (1969): Variations in pattern of pubertal changes in girls. Arch Dis Child 44:291-293.
Marshall WA, Tanner JM (1970): Variations in pattern of pubertal changes in boys. Arch Dis Child 45:13-23.
CRH Challenge in Prepubertal Depression BIOL PSYCHIATRY 277 1996;39:267-277
Muller, OA, von Werder K (1991): Corticotropin-releasing hormone--Basic clinical aspects. In: Marcella Motta (ed), Brain Endocrinology, 2nd ed. New York: Raven Press Ltd, pp 351-373.
Nemeroff CB, Widerlov E, Bissette G, et al (1984): Elevated concentrations of CSF corticotropin-releasing factor-like im- munoreactivity in depressed patients. Science 226:1342- 1344.
Nemeroff CB, Krishnan KR, Reed D, Leder R, Beam C, Dunnick R (1992): Adrenal gland enlargement in major depression. Arch Gen Psychiatry 49:384-389.
Orvashel H, Puig-Antich J (1987): Schedule for Affective Disorders and Schizophrenia for School-Age Children (6- 18), Epidemiologic Version, K-SADS-E 4th Version.
Pavlov EP, Harman SM, Chrousos GP, Loriaux DC, Blackman MR (1986): Responses of plasma adrenocorticotropin, corti- sol, and dihydroepiandrosterone of ovine corticotropin-re- leasing hormone in healthy aging men. J Clin Endocrinol Metab 62:767-772.
Puig-Antich J, Dahl RE, Ryan ND, et al (1989): Cortisol secretion in prepubertal children with major depressive dis- order: Episode and recovery. Arch Gen Psychiatry 46:801- 809.
Risch SC, Golshan S, Rapaport MH, et al (1988): Neuroendo- crine effects of intravenous ovine corticotropin-releasing factor in affective disorder patients and normal controls. Biol Psychiatry 23:755-758.
Roy A, Pickar D, Linnoila M, Doran AR, Paul SM (1987): Cerebrospinal fluid monamine and monamine metabolite levels and the dexamethasone suppression test in depression. Arch Gen Psychiatry 43:356-360.
Rubin RT, Poland RE, Lesser IM, Winston RA, Blodgett N (1987): Neuroendocrine aspects of primary endogenous de- pression I. Cortisol secretory dynamics in patients and matched controls. Arch Gen Psychiatry 44:328-336.
Rupprecht R, Lesch KP, Muller U, Beck G, Beckmann H, Schulte HM (1989): Blunted adrenocorticotropin but normal B-endorphin release after human corticotropin-releasing hor- mone administration in depression. J Clin Endocrinol Metab 69:600-603.
Ryan N, Birmaher B, Perel J, et al (1992): Neuroendocrine response to L-5-hydroxytryptophan challenge in prepubertal major depression: Depressed versus normal children. Arch Gen Psychiatry 49:843- 851.
Sachar EJ, Hellman L, Roffwarg HP, Halpem FS, Fukushima DF, Gallagher DF (1973): Disrupted 24-hour pattern of
cortisol secretion in psychotic depression. Arch Gen Psychi- atry 28:19-25.
Sapolsky RM, Krey LC, McEwen BS (1983): The adrenocortical stress-response in the aged male rat: Impairment of recovery from stress. Exp Gerontol 18:55-64.
Sapolsky RM, Krey LC, McEwen BS (1986): The neuroendo- crinology of stress and aging: The glucocorticoid cascade hypothesis. Endocrinol Rev 7:284-304.
Shapiro SS, Wilk MB (1965): An analysis of variance test for normalcy (complete samples). Biometrika 52:591-611.
Spitzer RL, Endicott J, Robins E (1978): Research diagnostic criteria: Rationale and reliability. Arch Gen Psychiatry 35: 773-782.
Stokes PE, Sikes CR (1987): Hypothalamic-pituitary-adrenal axis in affective disorders. In: Meltzer HY (ed), Psychophar- macology: The Third Generation of Progress. New York: Raven Press, pp 589-608.
Tizabi Y, Aguilera G, Gilad GM (1992): Age-related reduction in pituitary corticotropin-releasing hormone receptors in two rat strains. Neurobiol Aging 13:227-230.
Townsend EM, Puig-Antich J, Nelson B, Krawiec V (1988): Well-being of children participating in psychobiological re- search: A pilot study. J Am Acad Child Adol Psychiatry 483-488.
Traskman L, Tybring G, Asberg M, Bertilsson L, Lantto, Schalling D (1980): Cortisol in the CSF of depressed and suicidal patients. Arch Gen Psychiatry 37:761-767.
von Bardeleben V, Stalla GK, Muller OA, Holsboer F (1988): Blunting of ACTH response to human CRH in depressed patients is avoided by metyrapone pretreatment. Biol Psychi- atry 24:782-786.
Williamson DE, Ryan ND, Dahl RE, Jeannette, L (1992): Hamilton depression scores can be extracted from K-SADS-P in adolescents. J Child Adolesc Psychopharmacology 2:175- 181.
Young EA, Akil H (1985): Corticotropin-releasing factor stim- ulation of adrenocorticotropin and [3-endorphin release: Ef- fects of acute and chronic stress. Endocrinology 117: 1:23-30.
Young EA, Watson S J, Kotun J, et al (1990a): [3-Lipotropin-13- Endorphin response to low-dose ovine corticotropin releasing factor in endogenous depression. Arch Gen Psychiatry 47: 449-457.
Young EA, Akana S, Dallman MF (1990b): Decreased sensitiv- ity to glucocorticoid fast feedback in chronically stressed rats. Neuroendocrinology 51:536-542.
Related Documents











