-
8/9/2019 Copy of vitamin A guidebook.pdf
1/40
SIGHT AND LIFE Guidebookon Vitamin A
in Health and Disease
by
Donald S. McLaren, MD, PhD, FRCP
and
Martin Frigg, PhD
Second Edition
2001
-
8/9/2019 Copy of vitamin A guidebook.pdf
2/40
-
8/9/2019 Copy of vitamin A guidebook.pdf
3/40
3
SIGHT AND LIFE
Guidebook on Vitamin A
Introduction
This booklet has been designed forhealth workers and other professionalsfor whom an understanding of the basic
facts and most recent advances in thefield of vitamin A is of great relevancein their work. It is not primarily for thoseconcerned with nutrition, for whom theSIGHT AND LIFE Manual on Vitamin A Deficiency Disorders (VADD) may bemore appropriate.
In structure this Guidebook follows
fairly closely the new second edition ofthe SIGHT AND LIFE Manual on Vitamin A Deficiency Disorders (VADD) . It contains the key messagesfrom the Manual but gives less em-phasis to details.
The reader might ask why vitamin A hasbeen singled out from among all thevarious vitamins and the many otherimportant aspects of nutrition. Com-ments to this question are given in thefollowing paragraphs.
Vitamin A deficiency is among the mostcommon and serious of all nutritionaldeficiency diseases and also probablythe one for which there is the greatest
hope of it being brought under controlwithin the forseeable future.
In recent years startling scientificdiscoveries have been made that haverevealed how vitamin A functions as ahormone at the cellular level in manysystems of the body.
Some years ago it was believed thatdisease resulted only from severevitamin A deficiency and that it was
confined to being a major cause ofblindness in young children (xeroph-thalmia). Although xerophthalmia ismuch less common than it used to be,due in part to the many preventionprogrammes that have been set up,many children still go blind every year.However, over and above this we nowknow that deficiency of vitamin A canlead to a much greater risk of deathand also predispose to suffering frommany infectious diseases. Of greatimportance is the fact that these risksoccur when the level of vitamin Adeficiency is what is called “subclinical”
– that is to say there is no clinicaldisease and the deficiency can berevealed only by carrying out bio-
-
8/9/2019 Copy of vitamin A guidebook.pdf
4/40
4
SIGHT AND LIFE
Guidebook on Vitamin A
chemical or other laboratory tests. Thissubclinical deficiency is very muchmore common and widespread thanclinical deficiency like xerophthalmia.It affects mainly young children andtheir mothers during pregnancy andlactation. This means that the greatestemphasis now needs to be switchedaway from blindness and the eye to thearea of Maternal and Child Health(MCH). Because many systems areaffected by vitamin A deficiency itseems appropriate to use a term thatcovers all aspects, and vitamin Adeficiency disorders (VADD) is nowbeing generally accepted for thispurpose.
That having been said, all healthworkers need to be aware of what is
going on in the field of vitamin A.Compared to the common occurrence
of deficiency, excess of vitamin A is veryrare, however, it can also lead todisease and the danger should be keptin mind. A careful and controlled use ofsupplements is important.
A link is also being made in Section 8to carotenoids that are closely relatedto β-carotene and vitamin A. In recentyears they have been shown to haveantioxidant and other functions thatmay prove to be important in theprevention of some common dis-eases.
It is hoped that some readers willbecome fascinated with the unfoldingstory of vitamin A and wish to go onlearning about it – for them the SIGHT AND LIFE Manual on Vitamin A De-
ficiency Disorders (VADD) is waiting. Itcan be obtained from SIGHT AND LIFE.
-
8/9/2019 Copy of vitamin A guidebook.pdf
5/40
5
SIGHT AND LIFE
Guidebook on Vitamin A
Almost wherever we happen to be weare surrounded by vitamin A in someform or another. Vitamin A itself(retinol), and the closely related acidform (retinoic acid), which carries outmost of the functions of vitamin A inthe body, are hidden away inside thebodies of animals and humans.However, closely related to vitamin A
are hundreds of compounds be-longing to the group called carot-enoids. They readily attract ourattention as yellow, red and brownpigments, which are responsible forthe bright colours of many fruits,vegetables and leaves of trees aswell as the brilliant colours of manybirds, fish and other animals.
Section 1
Vitamin A in the world around us
all- trans β-carotene
all- trans retinol
retinyl palmitate
all- trans retinoic acid
11- cis retinalCHO
COOH
O
CH 2 OCC 15 H 31
CH 2 OH
Figure 1. Chemistry of vitamin A (retinol) and some related compounds
-
8/9/2019 Copy of vitamin A guidebook.pdf
6/40
6
SIGHT AND LIFE
Guidebook on Vitamin A
Leafy plants and trees have the abilityto remove carbon dioxide from theatmosphere and to combine it withwater to form carbohydrates, richsources of energy. This process isknown as photosynthesis and requireslight from the sun and the presence inthe leaf of the green pigment chlo-rophyll, which acts as a catalyst.Carotenoids also need to be presentto help to harvest the light. In this waythe sun ’s energy is captured and storedto make all of life possible on earth. Thedarker the green colour of leaves themore chlorophyll they contain and alsothe more carotenoid. This is why darkgreen leaves are more nutritious thanpale ones. Out of the hundreds ofcarotenoids in nature only a smallnumber are present in our food and
these are of two kinds. One kind, ofwhich β-carotene is the most important,can be converted in the body to retinol.This source of vitamin A fromcarotenoids in vegetables and fruits is
the main source for most people indeveloping countries, it makes up70 – 90% of all their dietary vitamin Aintake. Figure 1 shows the formulaeof β-carotene, retinol, and some of itsmost important related retinoids. Thelong chain of β-carotene is usually splitin the middle by an enzyme in theintestine to produce two molecules ofretinol, although in practice much lessthan this is available to the body (seepage 8). The other kind of carotenoid,including lutein and lycopene andothers, cannot form vitamin A but recentresearch suggests that they may haveother important functions (see page32). Laboratory methods are nowavailable for measuring the amounts ofdifferent forms of retinol, knowncollectively as retinoids, and also
individual carotenoids. HPLC (high-performance liquid chromotography)has replaced most other methods butis expensive and requires high-qualityfacilities.
-
8/9/2019 Copy of vitamin A guidebook.pdf
7/40
7
SIGHT AND LIFE
Guidebook on Vitamin A
Before we consider the kinds of foodsthat provide us with the vitamin A werequire it is necessary to discuss theunits of measurement used for theexpression of vitamin A activity infoodstuffs and also in body tissues.Weight for weight β-carotene has lessvitamin A activity than preformedvitamin A (retinol) itself. It has alsobeen found that other provitamin Acarotenoids, like α -carotene, γ -caro-
tene and cryptoxanthin, have onlyabout half the activity of β-carotene.Consequently the term RetinolEquivalent (RE) was coined to make
possible comparison between differentsources of vitamin A activity. It wasdecided that retinol is 6 times moreeffective than β-carotene, which istwice as effective as the otherprovitamin A carotenoids. Table 1indicates these relationships.
In recent years research has cast doubton these values as they apply to thebioavailability of carotenoids to
humans. In general it has been foundthat provitamin A carotenoids in darkgreen leafy vegetables are much lessreadily available than from other
Section 2
Where we get our vitamin A
Table 1. International Units (IU) and Retinol Equivalents (RE)
Compound µg/IU IU/ µg RE/ µg µg/RE
all-trans retinol 0.300 3.33 1.000 1.0
all-trans retinyl acetate 0.344 2.91 0.873 1.15
all-trans retinyl palmitate 0.549 1.82 0.546 1.83
all-trans β-carotene 1.800 0.56 0.167 6.0
Mixed carotenoids* 3.600 0.28 0.083 12.0
* Provitamin A carotenoids other than β-carotene
-
8/9/2019 Copy of vitamin A guidebook.pdf
8/40
8
SIGHT AND LIFE
Guidebook on Vitamin A
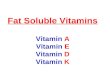
sources and that the relationships inTable 1 overestimate the activity ofcarotenoids in the body (Figure 2).Among the many factors that decreasethe bioavailability of carotenoids themost important probably are:• the matrix in which the carotenoid
is incorporated in the food,• the presence and amount of
substances that affect absorption,such as fat, vitamin E, fibre, chlo-rophyll, and nonprovitamin Acarotenoids,
• the nutritional status of the hostand
• parasites such as roundworm andgiardia.
It has recently been proposed that theprevious RE values for provitamin Acarotenoids be halved. This wouldmake β-carotene 1/12 as active asretinol (up to now 1:6), and otherprovitamin A carotenoids 1/24 (up tonow 1:12). Some studies have showngreat variability between individuals intheir ability to respond to dosing withβ-carotene.
Syntheticcarotenoids in oil
Red palm oil
Yellow or green fruits
Yellow or green tubers
Lightly cooked yellow, orange
or green vegetables or fruit juices
Fresh vegetable juices
Raw yellow or orange vegetables
Raw green leafy vegetables
Figure 2. Hierarchy of carotenoid bioavailability.
-
8/9/2019 Copy of vitamin A guidebook.pdf
9/40
-
8/9/2019 Copy of vitamin A guidebook.pdf
10/40
10
SIGHT AND LIFE
Guidebook on Vitamin A
red palm oil into parts of the worldwhere previously it was unknown isincreasing.
Other sources of provitamin AcarotenoidsHen ’s eggs are rich in carotenoids, butthese are mostly nonprovitamin A.Natural extracts containing carotenoidshave long been used to colourfoodstuffs and make them moreattractive. β-carotene is sometimesused for this purpose and then alsocontributes to the nutrient intake.
Sources of preformedvitamin A
Table 3 shows some common sources.Fish liver oils are the most concentratedsources and are often used medicinally.Dairy products, usually quite ex-pensive, are only moderate sources.
Table 3. Examples of common animalvitaminA sources ( µµµµµg retinol/100 g edibleportion)
Fatty fish liver oils
Halibut 900,000 Cod 18,000 Shark 180,000 Herring and mackerel 50
Dairy produce Butter 830 Margarine, vitaminized 900 Eggs 140 Milk 40 Cheese, fatty type 320
Meats Liver of sheep and ox 15,000 Beef, mutton, pork 0 – 4
Vitamin A has been added to food for a
long time and fortification is one of themajor long-term approaches to thecontrol of the problem of VAD (seepage 33).
-
8/9/2019 Copy of vitamin A guidebook.pdf
11/40
11
SIGHT AND LIFE
Guidebook on Vitamin A
Vitamin A (retinol) in the body comesfrom two sources, preformed vitamin Ain animal foods and from β-caroteneand other provitamin A carotenoids inplant sources. Both of these arereleased from protein in the stomachand like all other lipids are taken up inthe wall of the small intestine andbecome part of chylomicrons that enter
the blood circulation. From there theyare taken to the liver, where storagetakes place as retinyl ester mainly inspecial cells called stellate cells. Fortransport to other parts of the bodyretinol is attached to its own protein,the retinol-binding protein (RBP), andanother protein called transthyretin(TTR, see Figure 3).
Section 3
What vitamin A doesand how it works
Liver
Retinol
Small intestine
β-Carotene
+ RBP
Parenchymalcells
Chylomicrons
Othercells
Epithelia
Stellate cell(retinyl palmitate)
Eye(11- cis retinal)
____________
T T R
T T R
R B P
R
Figure 3. Physiology of vitamin A
-
8/9/2019 Copy of vitamin A guidebook.pdf
12/40
12
SIGHT AND LIFE
Guidebook on Vitamin A
all over the body it is RA that is theactive form of vitamin A. It has beenshown that many genes are activatedby RAR or RXR nuclear receptors(Figure 4). These receptors act likehormones, such as steroids and thyroidhormones, with which they are closelylinked. It is through this mechanism thatthe functions of vitamin A are broughtabout, with one exception, vision. In therod and cone cells of the retinaresponsible for vision the functionalform of vitamin A is not RA but 11- cis retinal (see page 13).
At the cell membrane retinol is takenup by receptors (RBP receptors).Within cells there are cellular retinoid-binding proteins (CRBPs) that directretinoids to specific enzymes and, mostimportantly, to the nucleus of the cell.
In recent years it has been discoveredthat within the cell nucleus there aretwo sets of three nuclear receptors(known as RARs and RXRs). Thesenuclear receptors are activated by anacidic form of retinol, such as retinoicacid (RA). In cells of organs and tissues
Extracellular
RBP-ROH
ROH-CRBP
ROH
Receptor
RA
Nucleus
Regulatedgenetranscription
Intracellular
RA-CRABP
RA
RA-RXR RAR-RA
Target cell
D N A
ROH = RetinolRA = Retinoic acidRBP = Retinol-binding
proteinCRBP = Cellular retinol-
binding protein
CRABP = Cellular retinoic acid-binding protein
RXR, RAR = Nuclear retinoic acid receptors
Figure 4. Molecular biology of vitamin A
-
8/9/2019 Copy of vitamin A guidebook.pdf
13/40
13
SIGHT AND LIFE
Guidebook on Vitamin A
Functions of vitamin A
Table 4 outlines some of the mainfunctions of vitamin A in the body.
Vision
The rods cells of the retina contain aprotein, opsin, attached to a form ofvitamin A, 11- cis retinal, to form acompound that is sensitive to light,rhodopsin or visual purple. Onexposure to light 11- ci s retinal isconverted back to all -trans retinal anda nerve impulse is generated. In VADthe supply of retinal is reduced and rodfunction is impaired.
Cell differentiation
In VAD mucus-secreting cells in manyepithelial tissues are replaced bykeratin-producing cells. This is
Vision (night, day, colour)
Epithelial cell integrity against infections
Immune response
Haemopoiesis
Skeletal growth
Fertility (male and female)
Embryogenesis
responsible for the xerosis andkeratinization of the conjunctiva andcornea and other tissues.
Embryogenesis
Reference is made elsewhere (seepage 32) to the evidence in animals thatboth deficiency or excess of vitamin Acan cause congenital malformations.Humans appear to be more resistant.
Immune response
Healthy epithelial tissues are barriersto infection, but in VAD these cells aredamaged and invasion by pathogensbecomes easier. Vitamin A appears tobe involved more in cell-mediatedrather than humoral aspects of theimmune response.
Table 4. Functions of vitamin A
-
8/9/2019 Copy of vitamin A guidebook.pdf
14/40
14
SIGHT AND LIFE
Guidebook on Vitamin A
Reproduction
Studies in animals show the involve-ment of vitamin A in spermatogenesisin the male and the prevention ofplacental necrosis and fetal absorptionin the female.
Haemopoiesis
There is a link between iron and vitaminA in erythropoiesis. Iron deficiencyanaemia responds more completely ifvitamin A is added to iron therapy thanif it is not. The mechanism is not yetunderstood.
Growth
Vitamin A is known to be involved in
normal growth of the musculo-skeletal
system. Several field studies haveprovided evidence that growth isimpaired in children if severe VAD ispresent.
Human requirements for vitamin A
These are usually expressed in termsof recommended dietary intake (RDI)values according to age, sex andphysiological state such as pregnancyand lactation. Table 5 gives somerepresentative values which tend to beon the lower side. It will be noted thatthe requirements are relatively muchgreater in early life. This is mainly be-cause of the increased needs forgrowth, over and above those formaintenance.
Table 5. Vitamin A requirements
-
8/9/2019 Copy of vitamin A guidebook.pdf
15/40
15
SIGHT AND LIFE
Guidebook on Vitamin A
There are varying degrees of VAD asshown in outline in Table 6. Differenttests are appropriate for detectingdifferent stages of this process. Theyall measure the state of vitamin Anutriture in the body or what isusually called vitamin A status. The
measurement of dietary intake of vi-tamin A over a given period of time,usually per day, does not measurestatus but does give a good generalindication in a population whether ornot there is a serious VAD problem.
Section 4
How to test for vitamin Adeficiency
SubclinicalIncreasing reducing stores
deficiency
lowering serum levelmetaplasia
Clinicalxerophthalmia- non-blinding- blinding
Table 6. Stages of vitamin A deficiency
-
8/9/2019 Copy of vitamin A guidebook.pdf
16/40
-
8/9/2019 Copy of vitamin A guidebook.pdf
17/40
17
SIGHT AND LIFE
Guidebook on Vitamin A
Serum retinol does not fall appreciablyuntil body stores have been virtuallyexhausted. Even so, serum retinolvalues for large population groups havebeen found to be a reliable indicationof their overall vitamin A status and areespecially useful for comparing onepopulation with another (Table 8). It isnow generally recognized that in thepresence of inflammation, infection ortrauma the acute phase responsecauses serum retinol to fall, sometimesdramatically. During this phase serumretinol does not reflect vitamin A status.
Serum RBP is easier to measure thanserum retinol and is coming into greater
use. However, it is also lowered in theacute phase response. Breast milkretinol has been found useful to assessthe vitamin A status of lactating womenand might be of value for comparingdifferent groups. It has the advantageover other biochemical tests of notrequiring blood sampling. The relativedose response (RDR) and modifiedrelative dose response (MRDR) testsassess indirectly the level of livervitamin A stores, which under mostconditions are a truer reflection ofvitamin A status than serum retinol.They are mainly used as researchtests, as is the more recent stableisotope dilution test.
Table 8. Ranges of prevalence of serum retinol to define a public health problem of
subclinical vitamin A deficiency of varying importance in young children
Prevalence below cut-offs to define a publichealth problem and its level of importance
Indicator(cut-off) Mild Moderate Severe
Serum retinol ≥2 –
-
8/9/2019 Copy of vitamin A guidebook.pdf
18/40
-
8/9/2019 Copy of vitamin A guidebook.pdf
19/40
19
SIGHT AND LIFE
Guidebook on Vitamin A
The term xerophthalmia is used to in-clude all signs and symptoms affect-ing the eye that can be attributed tovitamin A deficiency. Table 9 lists thesechanges and gives their shorthandsymbols. In a general way they arelisted in order of appearance with in-creasing severity of deficiency.
Night blindness (XN)
As we saw earlier (see page 12) therod cells of the retina require vitamin Ato fulfil their function of vision at night.There are instruments to test rodfunction but they require thecooperation of the subject and are
unsuitable for use in young children, inwhom VAD is most common. A simplemethod is in use in the field to gain anidea of the vitamin A status of acommunity. In areas where VAD iscommon there is usually one or morephrase in the local language for theinability to see well at night. Thisinformation and some other questionsabout a child ’s night vision form a shortquestionnaire (Table 10).
Conjunctival xerosis (X1A)
In extreme cases the dryness,thickening and wrinkling of theconjunctiva are very obvious. Lesserdegrees are much more common andin these cases it is very difficult to be
sure that the conjunctiva is abnormal.
Section 5
Eye diseases due to vitamin Adeficiency
Table 9. Xerophthalmia classification byocular signs
Night blindness (XN)
Conjunctival xerosis (X1A)
Bitot’s spot (X1B)
Corneal xerosis (X2)Corneal ulceration/keratomalacia
< 1 / 3 of corneal surface (X3A)
Corneal ulceration/keratomalacia ≥ 1 / 3 of corneal surface (X3B)
Corneal scar (XS)
Xerophthalmic fundus (XF)
-
8/9/2019 Copy of vitamin A guidebook.pdf
20/40
20
SIGHT AND LIFE
Guidebook on Vitamin A
Consequently it was decided toexclude this sign from use in fieldsurveys. Unfortunately it is stillsometimes being used in somesurveys and the results are notreliable.
Bitot’s spot (X1B)
Figure 5 shows a typical example. Thelesion consists of a local heaping upof keratinized material on the surfaceof the conjunctiva. It is usually presenton the temporal (outer) side of theconjunctiva and on the area notnormally covered by the lids. It is reallyan extreme example of X1A in onearea. Bitot ’s spot is rare in infants, andthe kind that responds to treatment
with vitamin A is most commonly seen
Table 10. Scheme for the classification ofnight blindness by interview (WHO, 1996)
1) Does your child have any problem seeingin the daytime?
2) Does your child have any problem seeingat nighttime?
3) If (2) = yes, is this problem different fromother children in your community? (Note:this question is particularly appropriatewhere VAD is not very prevalent.)
4) Does your child have night blindness (uselocal term that describes the symptom)?
Figure 5. Bitot ’s spot (X1B) on temporal aspect of bulbar conjunctiva in inter-palpebral fissure. Bubbles of foam are clearly visible.
-
8/9/2019 Copy of vitamin A guidebook.pdf
21/40
21
SIGHT AND LIFE
Guidebook on Vitamin A
in older preschool age children. Afterthat age, in older children and adultsBitot’s spots are usually not due to VADand these spots should not be used asan indicator of VAD.
Corneal xerosis (X2)
This is dryness of the cornea just likethat of the conjunctiva. This stage ofhaziness on its own is short-lived anduncommon. Prompt treatment withvitamin A (see page 34) at this stagewill result in complete cure of the eyelesion.
Keratomalacia (X3A, X3B)
This is the final stage of xerophthalmiaand results in partial (X3A) or greateror total (X3B) melting and destructionof the cornea. Both eyes are usuallyaffected but not necessarily equally(Figure 6). Blindness is inevitable andmortality is high. In any communitykeratomalacia is very uncommon andyoung children are almost alwaysthose affected.
Figure 6. Colliquative necrosis (keratomalacia) affecting the greater part of thecornea (X3B).The relative sparing of the superior aspect is typical. PlasmavitaminA was 4 µg/dL in this case.
-
8/9/2019 Copy of vitamin A guidebook.pdf
22/40
22
SIGHT AND LIFE
Guidebook on Vitamin A
Figure 7. Bilateral corneal scars (leucomataXS) in an anaemic and generally malnour-ished infant. The inferior situation of the scarsis typical.
Corneal scars (XS)
The cornea may be damaged by injuryand many infections as well as byxerophthalmia. In survivors of ker-atomalacia scars of varying sizes maybe left on one or both corneas. They
are usually situated in thelower part of the cornea andcentrally placed; in a “sixo’clock ” position (Figure 7). Adiagnosis of XS should not bemade unless the scars relateto a period of malnutrition inthe past. These inactivelesions are more commonthan active keratomalacia andcan be used in surveys withcare. All the eye signs do notnecessarily appear in theorder given above andkeratomalacia in very youngchildren may develop rapidlywith no evidence of xerosis.
Xerophthalmic fundus is veryrare and not useful for surveys.
-
8/9/2019 Copy of vitamin A guidebook.pdf
23/40
23
SIGHT AND LIFE
Guidebook on Vitamin A
Soon after vitamin A was discovered in1913 it became known as the “anti-infective vitamin ”. This was because inanimals and humans vitamin A,especially in the form of cod liver oil,was found to have a beneficial effectin a number of infectious diseases,
especially respiratory infections,measles, and puerperal fever (afterchildbirth). Some years later effectivedrugs against many infections wereintroduced and the benefit fromvitamin A was largely forgotten.
Section 6
Vitamin A deficiency as a cause of death and disease
-60
-50
-40
-30
-20
-10
0 -
+10
-34
-45
-54
-6
-30 -29
+6
-19 %
C h a n g e
Indonesia India Nepal Africa
19901988 1988 1990 1991 1991 1992 1992
T. NaduAceh Java A. Prad. Sarlahi Jumla Sudan Ghana
Figure 8. Impact of vitamin A on child mortality
-
8/9/2019 Copy of vitamin A guidebook.pdf
24/40
-
8/9/2019 Copy of vitamin A guidebook.pdf
25/40
25
SIGHT AND LIFE
Guidebook on Vitamin A
like the common causes of infectiousdiarrhoea, malaria and meningococcaldisease.
Research results all tend to agree thatthe various forms of acute lower res-piratory tract infection (ALRI), unlikemost infections, do not appear torespond to vitamin A supple-mentation. The reasons for this arenot understood, especial ly asexperimental animals with VADusually die with respiratory infections,but all agree that patients should begiven vitamin A to improve theirvitamin A status.
Infants born to women with HIVinfection have a higher mortality and
poorer growth, and morbidity andmortality among these are reduced byvitamin A supplementation. It wasoriginally suggested that vitamin Amay reduce the transfer of HIVinfect ion from mothers to theiroffspring but more recently severaltrials failed to confirm this.
It has been calculated that improve-ment of vitamin A status would reducethe all-cause mortality rate in youngchildren by about 23% and would beexpected to prevent 1.3 – 2.5 milliondeaths per year in children agedunder 5 years. Vitamin A supple-mentation is one of the most effectiveand inexpensive of all public healthinterventions (see page 33).
-
8/9/2019 Copy of vitamin A guidebook.pdf
26/40
-
8/9/2019 Copy of vitamin A guidebook.pdf
27/40
27
SIGHT AND LIFE
Guidebook on Vitamin A
Recent calculations show that nearly250 million preschool children aresubclinically vitamin A deficient – thisis almost 50% of those in developingcountries. Three million have xe-rophthalmia at any one time; about90% of these suffer from nightblindness and other non-blinding
xerophthalmia. 10% or 300,000 areblind with keratomalacia and thisaccounts for about 10% of all blindchildren in the world. While it isencouraging to note that the rate ofblindness due to xerophthalmia issteadily decreasing, only in recentyears has it become evident howwidespread subclinical deficiency isand what an important cause ofmortality and morbidity it is. The map(Figure 10) indicates in outline thevi tamin A deficiency si tuat ionthroughout the world. The majority ofcases occur in south and east Asia,partly because of the vast populationsand also because most of the poor inthese countries depend heavily on
rice (devoid of carotene). Many arelandless and this means they have topurchase all their food and have nomeans to buy or grow their ownvegetables. Urban slum dwellers areespecially vulnerable, as are thosesubsisting in semi-deserts. Rapidsocial change, as in some Pacific
islands, and civil strife, wars andecologic destruction in much of Africaand elsewhere often precipitateVADD.
Risk factors for VADD
Age
Preschool age children are mostcommonly affected by VAD anddevelop the most severe degrees ofdeficiency. This may be due to acombination of factors such as rapidgrowth, adverse effect of infectionsand low vitamin A status at birth.
Section 7
Who is vitamin A-deficientand why
-
8/9/2019 Copy of vitamin A guidebook.pdf
28/40
28
SIGHT AND LIFE
Guidebook on Vitamin A
W H O / N H D
PublichealthimportanceofvitaminAdeficiencypercountry
(frominformationavailabletoWHO,2000)
Clinical deficiency
Subclinical deficiency
Insufficientdata,butpossibilityofVAD
Insufficientdata,butVADunlikely
The designation employed and the presentation of material on this map do not imply the expression of any opinion whatsoever on the part of the World Health
Organization concerning the legalstatus of any country, territory, city or area or its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines
represent approximate border lines for which there may not yet be full agreement.
WHO 00294
Figure 10. Global occurrence of vitamin A deficiency
-
8/9/2019 Copy of vitamin A guidebook.pdf
29/40
29
SIGHT AND LIFE
Guidebook on Vitamin A
Sex
It has been found that for all aspects ofVAD males are more susceptible thanfemales. The reasons have been muchdebated but are not fully understood.
Physiological status
Pregnant and lactating women haveincreased requirements for vitamin Aand often develop night blindness orBitot’s spots. School children, perhaps
Figure 11. The VitaminA Deficiency Disorders (VADD) cycle.
-
8/9/2019 Copy of vitamin A guidebook.pdf
30/40
-
8/9/2019 Copy of vitamin A guidebook.pdf
31/40
31
SIGHT AND LIFE
Guidebook on Vitamin A
While VADD, as described here, are aproblem to some degree in nearly alldeveloping countries there are anumber of aspects of the use andmisuse of vitamin A that may affect usall.
Secondary VAD
Secondary, or endogenous, VAD
occurs not because of lack of thevitamin in the diet but due to one of avariety of steps in its utilization by thebody that goes wrong. Table 12 showshow this kind of deficiency may occur.Fortunately in most cases deficiencydevelops rather slowly and does notoften proceed beyond the stage of nightblindness or Bitot ’s spot, whentreatment can be effective. However, itusually has to be continued throughoutlife unless the underlying disease canbe cured.
Hypervitaminosis A
Vitamin A is stored in the body and ifintake is excessive various systemscan be damaged. Very large doses of
vitamin A, especially in young children,
Section 8
Vitamin A in general medicine
may cause a rise in intracranialpressure that leads to headache,nausea and vomiting. Withdrawal of thevitamin results in a rapid return tonormal without harmful long-termeffects. More commonly a higher thannormal intake of vitamin A over aperiod of months or even several yearscan result in a syndrome that may bevery difficult to diagnose. Common
symptoms are headache, vomiting,double vision, skin disease, bone and joint pain and liver damage. Oncediagnosed and vitamin A intakereduced to normal, symptoms willgradually subside but damage to theliver and other organs may not bereversible.
Pharmacological use of synthetic retinoidsLarge numbers of vitamin A-likecompounds, retinoids, have beensynthesized for use in treatment ofvarious diseases, especially thosethat are due to abnormal dif-ferentiation of epithelial cells. Theseinclude acne, psoriasis and some
other skin diseases and also some
-
8/9/2019 Copy of vitamin A guidebook.pdf
32/40
32
SIGHT AND LIFE
Guidebook on Vitamin A
cancers that affect epithelial tissuessuch as breast, skin, colon, and pros-tate. One form of leukaemia respondsto retinoic acid.
Congenital malformations
Studies in various animal species haveshown that both deficiency or excessof vitamin A during early fetal life mayresult in malformations in varioussystems of the body. In contrast to thisin humans there is no firm evidence thatmalformations in the fetus are causedby either lack or excess of vitamin A.Nevertheless, restrictions are placedon the amount of vitamin A that can besafely administered during pregnancyand lactation (see page 35).
Synthetic retinoids that are being usedto treat a number of skin and otherdiseases (see above) are known to behighly damaging to the fetus if con-tinued during pregnancy.
Carotenoids and chronicdiseasesThis is a very rapidly growing field forresearch and can only be touched onhere. It is probably the antioxidant andother effects of provitamin A andnonprovitamin A carotenoids in thebody that are responsible for beneficialresults. These have been reported insuch major diseases as coronary heartdisease, some cancers, and the eyediseases cataract and macular
degeneration.
Table 11. Secondary or endogenouscauses of vitaminA deficiency
Diseases Mechanisms
Coeliac disease, Impaired absorptionsprue, obstructive of lipids, including
jaundice, ascariasis, vitaminAgiardiasis, partial ortotal gastrectomy
Chronic pancreatitis In some casessecondary to zinc
deficiency
Chronic liver Storage impaireddisease, especially by damage tocirrhosis liver cells;
zinc deficiencyenhances theeffect
Severe infection Loss of RBP in urine
Cystic fibrosis Excessive faecalloss, unrelatedto degree of fat instools
Enzyme defect Failure to cleaveβ-carotene insmall intestine
Heterozygotic One case reported ofreduction of keratomalacia due toplasma RBP reduced transport
Mutations in the Biochemical but notgene for RBP clinical deficiency
-
8/9/2019 Copy of vitamin A guidebook.pdf
33/40
33
SIGHT AND LIFE
Guidebook on Vitamin A
There are three main types ofintervention that are being carried out.Each has been researched andpractised over the past severaldecades in many parts of the world.Each has its own particularcharacteristics, its disadvantages andits advantages. Frequently more than
one intervention is being used at thesame time. In addition, it must be re-membered that human communitiesare not like laboratory animals, capableof strict control. Many unknown and un-controllable variables exist. Im-provement or deterioration of vitaminA status in these circumstances cannotbe attributed directly or solely to anintervention.
Dietary modification
The vast majority of the world ’s peopleslive in an environment that is capableof meeting all their nutritionalrequirements, including that of vitaminA, without artificial supplementationof any kind. In the case of vitamin A
knowledge of its sources and the
consequent ordering of family lifeshould ensure normal vitamin A status.For example, home or school gardenscan not only meet family vitamin Arequirements but also provideadditional nutrients and income andhelp to raise the status of women. Suchprogrammes are difficult to start and to
sustain. The doubt recently cast on thebioavailability of provitamin A ca-rotenoids from dark green leaves andother sources suggests that somepreformed vitamin A from animalsources may be needed.
Recently rice has been geneticallymodified to contain β-carotene. Inten-sive efforts are under way to make this“golden rice ” widely available.
Supplementation
Large doses of vitamin A in capsuleor liquid form (200,000 IU) have beenadministered prophylactically at 4 – 6months intervals for many years in anumber of countries. Table 12 shows
the WHO-recommended schedule for
Section 9
What is being done to controlVADD
-
8/9/2019 Copy of vitamin A guidebook.pdf
34/40
34
SIGHT AND LIFE
Guidebook on Vitamin A
treatment of a patient with signs ofVAD. In a sense this is also a pre-ventive measure as the last dose isgiven with that aim in mind. Table 13indicates the preventive schedule rec-ommended by WHO. This should be astrictly emergency measure as it makesno contribution towards eradicating theproblem. Although easy to initiate, ex-perience has shown repeatedly that ina routine setting coverage falls dramati-cally to unacceptably low levels. Itshould not be considered in isolation,but thought should be given at thesame time to other long-term mea-sures. In recent years the national im-munization days (NIDs) and othermeasures as part of the worldwide Ex-panded Programme of Immunization
(EPI) of WHO has been utilized with
good effect for the distribution of vita-min A capsules. It is not immune fromthe criticisms mentioned above.
Evidence of transiently raised intra-cranial pressure has occasionally beennoted in vitamin A supplementationinvolving infants, but follow-up for 3years has found no long-term ill effect.Mention was made (see page 32) ofthe possibility of large doses of vita-min A in early pregnancy causingmalformations in the developingembryo. A number of studies haveprovided a consensus view thatsupplementation of vitamin A notexceeding 10,000 IU daily is perfectlysafe.
Table 12. Recommended xerophthalmia treatment schedule Ð oil-miscible oral vitamin A
-
8/9/2019 Copy of vitamin A guidebook.pdf
35/40
35
SIGHT AND LIFE
Guidebook on Vitamin A
Fortification
Addition of a nutrient to a food impliesthat a significant proportion of apopulation is unable to obtain their dailyrequirement from natural food alone.Recent evidence suggests that thismay well be the case in manycommunities in the developing world.Foodstuffs used in developingcountries which can be fortified
include wheat, rice and other grainproducts, tea, dairy foods, margarine,edible oils, formula foods and specialityitems. Other micronutrients such asiron and zinc are also being added. Fora successful fortification programme tobe initiated and maintained a great dealof cooperation is required. Severalstudies have shown that in a researchsetting it can significantly improve thevitamin A status of a whole population.
Table 13. Universal vitaminA distribution schedule for preschool children and lactatingmothers
Children 1 – 6 years 200,000 IU of vitaminA orally every 3 – 6 months.
Infants 6 – 11 months 100,000 IU of vitaminA orally every 3 – 6 months.Immunization against measles provides a good
opportunity to give one of these doses (see note).
Lactating mothers 200,000 IU of vitaminA orally once: at deliveryor during the first 8 weeks postpartum if breast-feeding or during the first 6 weeks if not breast-feedingto protect the mother and raise breast milk vitaminA levels to help protect the breast-fed infant.
NOTE: When infants less than six months old are not being breast-fed, supplementation with 50,000 IUof vitaminA, as single dose or as divided doses of 25,000 IU, should be considered before they reachthe age of six months.
-
8/9/2019 Copy of vitamin A guidebook.pdf
36/40
-
8/9/2019 Copy of vitamin A guidebook.pdf
37/40
37
SIGHT AND LIFE
Guidebook on Vitamin A
Acute-phase reaction (or response)
(APR) A generalized reaction of thebody to acute infection, inflammationand injury. Certain proteins, positiveacute-phase proteins, increase inconcentration in plasma. Other pro-teins, which include retinol-bindingprotein (RBP) and transferrin, decreasein concentration in plasma and areknown as negative acute-phaseproteins.
Bioavailability In general the termrefers to the degree to which anysubstance in the diet is available afteringestion for utilization by the body. Inthe present context, bioavailabilityrelates to the degree to which dietaryprovitamin A carotenoids are utilizedafter ingestion.
BitotÕs spotHeaping up of keratinizedcells on bulbar conjunctiva. Anadvanced stage of conjunctival xerosis.The first description was attributed toa French physician of that name in themiddle of the 19th century. Not allBitot ’s spots are attributable todeficiency of vitamin A.
Carotenoids Yellow, orange, or red
pigments occurring in nature. About600 have been identified, of which lessthan 10 have provitamin A activity. Theyall have a basic C 40 skeleton which ismade up from successive additions ofC5 isoprene units.
Chlorophyll A green pigment thatimparts its colour to the leaves of plantsand many vegetables. It is mainlyresponsible for the process ofphotosynthesis, whereby in thepresence of sunlight carbon dioxidefrom the atmosphere and water areconverted to carbohydrate, and oxygenis given off.
Chloroplast This structure in leavescontains the chlorophyll and carot-
enoids, which act as catalysts in theprocess of photosynthesis.
Cis/trans See isomerization.
Conjunctiva The thin layer of tissuethat overlies the white part of the frontof the eye and also lines the inner partof the lids.
Glossary
-
8/9/2019 Copy of vitamin A guidebook.pdf
38/40
-
8/9/2019 Copy of vitamin A guidebook.pdf
39/40
39
SIGHT AND LIFE
Guidebook on Vitamin A
Recommended Dietary Allowance orIntake (RDA, RDI) This relates to thelevel of an essential nutrient consideredto be adequate to meet the knownnutritional needs of practically allhealthy persons in a population.
Relative dose response (RDR) Abiochemical test designed to assessvitamin A status by the indirect estimateof liver vitamin A stores.
Retinoids A class of compoundsconsisting of four isoprenoid units
joined together in a head-to-tail mannerand customarily containing fiveconjugated double bonds. The termvitamin A is used as a genericdescriptor for retinoids exhibitingqualitatively the biological activity of
retinol.
Retinol equivalent (RE) This term wascreated to express both preformedvitamin A and provitamin A carotenoidequivalents as a single nutritive value.One RE is equal to 1 µg of all- trans retinol, or to 6 µg of all- trans β-carotene,or to 12 µg of other provitamin A
carotenoids. It has recently been pro-posed that the previous RE values forprovitamin A carotenoids be halved.This would make β-carotene 1/12 asactive as retinol (up to now 1:6), andother provitamin A carotenoids 1/24(up to now 1:12).
Vitamin The word originally meant“vital amine ”. Vitamins are vital in thesense that they are organic com-pounds that must be included in thediet in sufficient amount for health.Their chemical structure varies andthey are not all amines as was firstthought.
Vitamin A As might be expected thiswas the first vitamin to be discovered,in 1913. Chemically it is known as
retinol. It is an alcohol with five carbon-carbon double bonds and a functionalβ-ionone ring.
Xerophthalmia A term that applies toall clinical stages of eye diseaseattributable to VAD.
Xerosis See keratinization.
-
8/9/2019 Copy of vitamin A guidebook.pdf
40/40