CLINICAL STUDIES Contribution of ribavirin transporter gene polymorphism to treatment response in peginterferon plus ribavirin therapy for HCV genotype 1b patients Akihito Tsubota 1,2 , Noritomo Shimada 3 , Kai Yoshizawa 4 , Tomomi Furihata 5 , Rie Agata 1 , Yoko Yumoto 1 , Hiroshi Abe 4 , Makiko Ika 3 , Yoshihisa Namiki 1 , Kan Chiba 5 , Kiyotaka Fujise 2 , Norio Tada 1 and Yoshio Aizawa 3 1 Institute of Clinical Medicine and Research (ICMR), Jikei University School of Medicine, Kashiwa, Chiba, Japan 2 Division of Gastroenterology and Hepatology, Kashiwa Hospital, Jikei University School of Medicine, Kashiwa, Chiba, Japan 3 Department of Gastroenterology, Shinmatsudo Central General Hospital, Matsudo, Chiba, Japan 4 Division of Gastroenterology and Hepatology, Aoto Hospital, Jikei University School of Medicine, Katsushika-ku, Tokyo, Japan 5 Laboratory of Pharmacology and Toxicology, Graduate School of Pharmaceutical Sciences, Chiba University, Chuo-ku, Chiba, Japan Keywords chronic hepatitis C virus infection – nucleoside transporter – pegylated interferon – ribavirin – single nucleotide polymorphism Correspondence Akihito Tsubota, MD, Institute of Clinical Medicine and Research (ICMR), Jikei University School of Medicine, 163-1 Kashiwa-shita, Kashiwa, Chiba 277-8567, Japan Tel: +81-4-7164-1111 Fax: +81-4-7166-8638 e-mail: [email protected] Received 27 September 2011 Accepted 20 November 2011 DOI:10.1111/j.1478-3231.2011.02727.x Abstract Background: Standard-dose ribavirin is crucial for the standard-of-care treat- ment of chronic hepatitis C virus (HCV) infection. Equilibrative nucleoside transporter 1 (ENT1), encoded by SLC29A1 gene, is the main transporter that imports ribavirin into human hepatocytes. Aims: To determine whether single nucleotide polymorphisms (SNPs) at the SLC29A1 gene could influence the probability of treatment response compared with other baseline and host genetic factors. Methods: A total of 526 East Asian patients mono- infected with HCV genotype 1b who had received pegylated interferon alpha plus ribavirin therapy were enrolled in this study. They were assigned randomly to the derivation and confirmatory groups. SNPs related to the IL28B, ITPA and SLC29A1 genes were genotyped using real-time detection polymerase chain reaction. Factors associated with sustained virological response (SVR) were analysed using multiple logistic regression analy- sis. Results: Multivariate analysis for the derivation group identified six baseline variables significantly and independently associated with SVR: age [P = 0.023, odds ratio (OR) = 0.97], gender (P = 0.0047, OR = 2.25), plate- let count (P = 0.00017, OR = 1.11), viral load (P = 0.00026, OR = 0.54), IL28B SNP rs12979860 (P = 1.09 9 10 7 , OR = 8.68) and SLC29A1 SNP rs6932345 (P = 0.030, OR = 1.85). Using the model constructed by these independent variables, positive and negative predictive values and predictive accuracy were 73.3, 70.1 and 71.9% respectively. For the confirmatory group, they were 71.4, 84.6 and 75.3% respectively. The SLC29A1 and IL28B SNPs were also significantly associated with rapid virological response. Conclusions: The SNP at the major ribavirin transporter ENT1 gene SLC29A1 was one of significantly independent factors influencing treat- ment response, although the impact on the prediction was small. Pegylated interferon (peg-IFN) alpha in combination with weight-based doses of ribavirin is currently recom- mended as a standard-of-care treatment for chronic hepatitis C virus (HCV) infection (1). The addition of ribavirin to peg-IFN alpha elicits the synergistic antiviral activity against HCV (2–4), even though monotherapy with ribavirin clinically shows minimal efficacy on the viral load decline and almost no efficacy on the viral clearance (5). Recent clinical trials of specifically targeted antiviral therapy for HCV (STAT-C) agents, PROVE for telaprevir and SPRINT for boceprevir (6–8), showed that treatment arms without ribavirin in the PROVE2 trial and with low-dose ribavirin in the SPRINT-1 trial had increased viral breakthrough, higher relapse, and had lowered sustained virological response (SVR), sug- gesting that standard-dose ribavirin is required as a cru- cial component even in new combination regimens with the first-generation protease inhibitors. Therefore, riba- virin appears to remain the backbone of these combina- tion therapies in the foreseeable future. Ribavirin is a synthetic guanosine analogue, and the possible antiviral mechanisms have been proposed, such Liver International (2012) © 2011 John Wiley & Sons A/S 826 Liver International ISSN 1478-3223

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CL IN ICAL STUDIES
Contribution of ribavirin transporter gene polymorphism to treatmentresponse in peginterferon plus ribavirin therapy for HCV genotype 1bpatientsAkihito Tsubota1,2, Noritomo Shimada3, Kai Yoshizawa4, Tomomi Furihata5, Rie Agata1, Yoko Yumoto1,Hiroshi Abe4, Makiko Ika3, Yoshihisa Namiki1, Kan Chiba5, Kiyotaka Fujise2, Norio Tada1 and Yoshio Aizawa3
1 Institute of Clinical Medicine and Research (ICMR), Jikei University School of Medicine, Kashiwa, Chiba, Japan
2 Division of Gastroenterology and Hepatology, Kashiwa Hospital, Jikei University School of Medicine, Kashiwa, Chiba, Japan
3 Department of Gastroenterology, Shinmatsudo Central General Hospital, Matsudo, Chiba, Japan
4 Division of Gastroenterology and Hepatology, Aoto Hospital, Jikei University School of Medicine, Katsushika-ku, Tokyo, Japan
5 Laboratory of Pharmacology and Toxicology, Graduate School of Pharmaceutical Sciences, Chiba University, Chuo-ku, Chiba, Japan
Keywords
chronic hepatitis C virus infection –
nucleoside transporter – pegylated interferon
– ribavirin – single nucleotide polymorphism
Correspondence
Akihito Tsubota, MD, Institute of Clinical
Medicine and Research (ICMR), Jikei
University School of Medicine, 163-1
Kashiwa-shita, Kashiwa, Chiba 277-8567,
Japan
Tel: +81-4-7164-1111
Fax: +81-4-7166-8638
e-mail: [email protected]
Received 27 September 2011
Accepted 20 November 2011
DOI:10.1111/j.1478-3231.2011.02727.x
AbstractBackground: Standard-dose ribavirin is crucial for the standard-of-care treat-ment of chronic hepatitis C virus (HCV) infection. Equilibrative nucleosidetransporter 1 (ENT1), encoded by SLC29A1 gene, is the main transporterthat imports ribavirin into human hepatocytes. Aims: To determinewhether single nucleotide polymorphisms (SNPs) at the SLC29A1 gene couldinfluence the probability of treatment response compared with other baselineand host genetic factors. Methods: A total of 526 East Asian patients mono-infected with HCV genotype 1b who had received pegylated interferon alphaplus ribavirin therapy were enrolled in this study. They were assignedrandomly to the derivation and confirmatory groups. SNPs related to theIL28B, ITPA and SLC29A1 genes were genotyped using real-time detectionpolymerase chain reaction. Factors associated with sustained virologicalresponse (SVR) were analysed using multiple logistic regression analy-sis. Results: Multivariate analysis for the derivation group identified sixbaseline variables significantly and independently associated with SVR: age[P = 0.023, odds ratio (OR) = 0.97], gender (P = 0.0047, OR = 2.25), plate-let count (P = 0.00017, OR = 1.11), viral load (P = 0.00026, OR = 0.54),IL28B SNP rs12979860 (P = 1.09 9 10�7, OR = 8.68) and SLC29A1 SNPrs6932345 (P = 0.030, OR = 1.85). Using the model constructed by theseindependent variables, positive and negative predictive values and predictiveaccuracy were 73.3, 70.1 and 71.9% respectively. For the confirmatorygroup, they were 71.4, 84.6 and 75.3% respectively. The SLC29A1 andIL28B SNPs were also significantly associated with rapid virologicalresponse. Conclusions: The SNP at the major ribavirin transporter ENT1gene SLC29A1 was one of significantly independent factors influencing treat-ment response, although the impact on the prediction was small.
Pegylated interferon (peg-IFN) alpha in combinationwith weight-based doses of ribavirin is currently recom-mended as a standard-of-care treatment for chronichepatitis C virus (HCV) infection (1). The addition ofribavirin to peg-IFN alpha elicits the synergistic antiviralactivity against HCV (2–4), even though monotherapywith ribavirin clinically shows minimal efficacy on theviral load decline and almost no efficacy on the viralclearance (5). Recent clinical trials of specifically targetedantiviral therapy for HCV (STAT-C) agents, PROVE fortelaprevir and SPRINT for boceprevir (6–8), showed
that treatment arms without ribavirin in the PROVE2trial and with low-dose ribavirin in the SPRINT-1 trialhad increased viral breakthrough, higher relapse, andhad lowered sustained virological response (SVR), sug-gesting that standard-dose ribavirin is required as a cru-cial component even in new combination regimens withthe first-generation protease inhibitors. Therefore, riba-virin appears to remain the backbone of these combina-tion therapies in the foreseeable future.
Ribavirin is a synthetic guanosine analogue, and thepossible antiviral mechanisms have been proposed, such
Liver International (2012)© 2011 John Wiley & Sons A/S826
Liver International ISSN 1478-3223

as direct inhibition of the viral RNA-dependent RNApolymerase, anti-replication efficiency by depletion ofintracellular guanosine triphosphate pools, viral errorcatastrophe through increased mutagenesis in a dose-dependent manner, immunomodulatory action by shift-ing host T-cell response phenotype from Th2 to Th1and upregulation of IFN-stimulated genes (9–11),although not entirely elucidated. Most of these pro-posed mechanisms require import of ribavirin into cellsfor the antiviral activity. In mice infected with viral hep-atitis, selectively targeted delivery of ribavirin to the liverincreases antiviral activity and consequently improvesthe clinical events (12, 13). In patients with chronic hep-atitis C, higher serum/plasma concentrations and moreexposure of ribavirin and more severe degree of anaemiacould yield higher SVR rate (14–20). These studies sug-gest that sufficient import levels of ribavirin intohepatocytes and high intracellular ribavirin concentra-tions would be required to augment the virucidal effectof treatment on HCV within cells.
Ribavirin and other synthetic analogs are transportedinto cells by nucleoside transporters (NTs), which aretransmembrane glycoproteins that localize to the plasmaand mitochondrial membranes and transport physiolog-ical nucleoside substrates and synthetic analogs acrossthe membranes from the surrounding medium (10, 21–23). There are two known families of NTs, equilibrativenucleoside transporters (ENTs) and concentrativenucleoside transporters (CNTs). Four known ENTs,ENT 1–4, are, respectively, encoded by the solute carrier(SLC) 29A 1–4 genes in humans, and mediate facilitatedbidirectional diffusion of nucleosides and nucleobasesbased on electrochemical gradients. Three known CNTs,CTN 1–3, are, respectively, encoded by the SLC28A 1–3genes, and mediate unidirectional flux against the elec-trochemical gradient by coupling a sodium gradientinterchange. Of these NTs, ENT1, ENT2, CNT2 andCNT3 could transport ribavirin to human placental epi-thelial cells and Xenopus oocytes, although the efficiencyof ribavirin uptake by each NT is various between thesecells (24). In the human liver, mRNA and proteins ofENT1, ENT2, CNT1 and CNT2 are expressed (25). Ofthem, ENT1 is a major ribavirin uptake transporter inhuman hepatocytes and erythrocytes, which are themain cellular compartments for ribavirin accumulation(26–30). More recently, a specific SNP (rs760370) at theSLC29A1 gene was reported to influence treatmentresponse significantly in peg-IFN plus ribavirin therapyfor Spanish patients co-infected with HIV and HCVgenotype 1 or 4 (31).
The aim of the present study was to assess whetherSNPs at the SLC29A1 gene could contribute significantlyto treatment response or clinical events such as treat-ment-induced haemolytic anaemia in peg-IFN plusribavirin therapy for East Asian chronic hepatitis Cpatients monoinfected with HCV genotype 1b, indepen-dent of other SNPs nearby the interleukin 28B (IL28B)gene, which are the strongest predictors of treatment
outcome (32–34), and those at the inosine triphospha-tase (ITPA) gene, which are correlated with treatment-induced haemolytic anaemia (35–37).
Materials and methods
Study population and assessment
Between April 2005 and March 2010, 526 East Asianpatients chronically monoinfected with HCV genotype1b were enrolled in this study at Shinmatsudo CentralGeneral Hospital and Aoto Hospital and Kashiwa Hos-pital, the Jikei University School of Medicine. Patientsreceived subcutaneous peg-IFN alpha-2a (PEGASYS®;Roche, Basel, Switzerland) at a dose of 180 lg or peg-IFN alpha-2b (PEG-Intron®; MSD, Tokyo, Japan) at adose of 1.5 lg/kg once weekly, and oral ribavirin (CO-PEGUS®; Roche or Rebetol®; MSD) at a dose of 600–1000 mg twice daily; the dose was adjusted according tobody weight (600 mg for weight 60 kg or less, 800 mgfor weight above 60–80 kg or less, and 1000 mg forweight above 80 kg). The standard treatment durationlasted 48 weeks, although patients who achieved rapidvirological response (RVR) could be shortened to24 weeks and those with undetectable HCV RNA atweek 16 or later were recommended to extend the dura-tion period to 72 weeks. When serum HCV RNA levelwas decreased by less than 2 logs at week 12 or whenqualitative HCV RNA was detectable at week 24 of treat-ment, treatment was recommended to discontinue pre-maturely. Leading inclusion criteria were HCV genotype1b confirmed using the conventional polymerase chainreaction (PCR)-based method, acquisition of writteninformed consent from each individual, availability ofgenetic DNA for genotyping SNPs, adherence of morethan two-thirds to the scheduled dose of peg-IFN andribavirin for patients with relapse and more than 80%for those with non-virological response (NVR), absenceof liver cancer, liver failure or other forms of liver dis-ease, lack of concurrent treatment with any other antivi-ral or immunomodulatory agent and a negative test forhepatitis B surface antigen and human immunodefi-ciency virus. Patients who discontinued treatmentwithin 24 weeks of treatment for reasons other thanvirological failure were excluded from this study.On-treatment dose reduction, modification and discon-tinuation of PEG-IFN or ribavirin followed the criteriaand procedures with some modification or patient con-dition to reduce or avoid adverse effects (38). This studyprotocol was conducted in accordance with the provi-sions of the Declaration of Helsinki and Good ClinicalPractice guidelines, and was approved by the Institu-tional Review Boards of all participating sites.
Clinical and laboratory data were assessed at leastonce weekly during the first 4 weeks, and thereafter atleast every 4 weeks until 24 weeks post-treatment. Viro-logical data were assessed by monitoring serum HCVRNA levels at least every 4 weeks during and off treatment
Liver International (2012)© 2011 John Wiley & Sons A/S 827
Tsubota et al. Transporter gene SNP in peg-IFN and ribavirin

until 24 weeks post-treatment. Serum HCV RNA loadswere measured using a quantitative PCR assay (Ampli-cor HCV Monitor version 2.0 or Amplicor HCV version2.0; Roche Diagnostics, Basel, Switzerland). The pres-ence or absence of serum HCV RNA was assessed usinga qualitative PCR assay (Amplicor HCV version 2.0;Roche Diagnostics). Virological response (VR) wasdefined as undetectable serum HCV RNA by the end oftreatment. RVR and SVR were defined as serum HCVRNA undetectable at week 4 of treatment and 24 weekspost-treatment. NVR was defined as persistent presenceof serum HCV RNA throughout the treatment. VR withrelapse was defined as VR during treatment, but reap-pearance of serum HCV RNA during the follow-up per-iod. All liver biopsy specimens were reviewed using theestablished ranking system for staging of fibrosis andgrading of necroinflammation activity (39).
SNP genotyping of IL28B, ITPA, and SLC29A1
Genomic DNA was extracted from whole blood usingthe MagNA Pure LC and the DNA Isolation Kit (RocheDiagnostics). Genetic polymorphisms, rs8099917 andrs12979860 nearby the IL28B gene (32–34), rs1127354 atthe ITPA gene (35–37), rs6051702 at the C20orf194 gene(35, 37), and rs760370, rs3734703, rs3734704,rs1057985, rs9394992, rs6932345, rs324148, rs324149,rs693955, rs1886884, rs507964, rs55725328, rs9462977and rs3734701 at the SLC29A1 gene (Fig. 1)(31, 40)were genotyped by real-time detection PCR using theTaqMan SNP Genotyping Assays and the 7500Fast Real-Time PCR System (Applied Biosystems, Foster City, CA,USA). Except for notable SNPs in the previous reports(31, 40), SNPs at the SLC29A1 gene with an allelic fre-quency > 0.2 (31) among the East Asian populationwere selected based on the HapMap-JPT database.
Ribavirin serum concentrations
At week 4 of treatment, blood samples were collectedbefore the morning dosing of ribavirin, which was 12 hafter the evening dosing on the preceding day. Troughconcentrations of serum ribavirin were determined by avalidated high-performance liquid chromatography/tan-
dem mass spectrometric assay using 13C-ribavirin as aninternal standard (14, 41). The assay was validated withrespect to linearity in the range from 50 to 5005 ng/ml,specificity, accuracy and precision (within 15% for allruns).
Statistical analysis
Pearson or Mantel–Haenszel chi-square test, Fisher’sexact test, or Mann–Whitney test was used to comparefrequencies in categorical data or differences in continu-ous data between two groups respectively. Possiblevariables influencing treatment response and treatment-induced haemolytic anaemia included baseline features(Table 1) and host genetic characteristics (Table 2).Variables that reached statistical significance (P < 0.05)or marginal significance (P < 0.10) in univariate com-parisons were subsequently entered into multiple logis-tic regression analysis using forward and backwardstepwise selection method to identify significantly inde-pendent factors associated with treatment response.Based on the final-step results, score (S) was constructedby the exposure of some set of independent factors (x1,x2, …, xp):
S ¼ b0 þ b1x1 þ b2x2 þ . . .þ bpxp ðb0 : intercept;b1; b2; . . .; bp : regression coefficientsÞ
The model could be expressed as:
P = 1/[1 + exp ( - S)], where P > 0.5 was SVR andP < 0.5 was non-SVR
Hosmer–Lemeshow test and likelihood-ratio chi-square test were used and positive/negative predictivevalues, and predictive accuracy were calculated to evalu-ate the fitness of the model. Split-group validation wasused to develop and validate the best fitness of themodel. Patients were randomly divided into two groupsapproximately in the ratio of 2:1 using a computer-gen-erated random number list: 64.1% of the patients (337patients) were assigned to the derivation group and35.9% (189 patients) to the confirmatory group. Thereproducibility of the resulting model based on datafrom the derivation group was assessed with the data
SLC29A1
rs3734704
(Chromosome 6, 44187242..44201888)
rs760370rs9394992
rs1057985rs3734703
rs6932345rs324148
rs324149
rs3734701
rs507964
rs9462977 rs693955rs1886884
rs55725328
Fig. 1. Genetic analysis of SNPs at the SLC29A1 gene. Association of these SLC29A1 SNPs with treatment outcome and haemolytic anaemiawere analysed in the present study.
Liver International (2012)© 2011 John Wiley & Sons A/S828
Transporter gene SNP in peg-IFN and ribavirin Tsubota et al.
from the validation group. All P values for statisticaltests were two tailed, and the values of less than 0.05denoted the presence of a statistically significant differ-ence. All data analyses were performed using the SPSSstatistical package for Windows, version 17.0 (IBM-SPSS, Chicago, IL, USA).
For SNPs, Hardy–Weinberg equilibrium was assessedusing chi-square test with one degree of freedom. Link-
age disequilibrium (LD) between pairs of SNPs withavailable genotype data of more than 50% and haplo-type maps were analysed by calculating parameters D’and r2, implemented in Haploview software version 4.2(Broad Institute, Cambridge, MA, USA). Frequencies ofhaplotype were estimated using the EM algorithm inHaploview.
Ethnic approval
This study was conducted with the approval of the JikeiUniversity Ethics Committee and Shinmatsudo CentralGeneral Hospital Ethnics Committee.
Results
Patient profiles and response rate
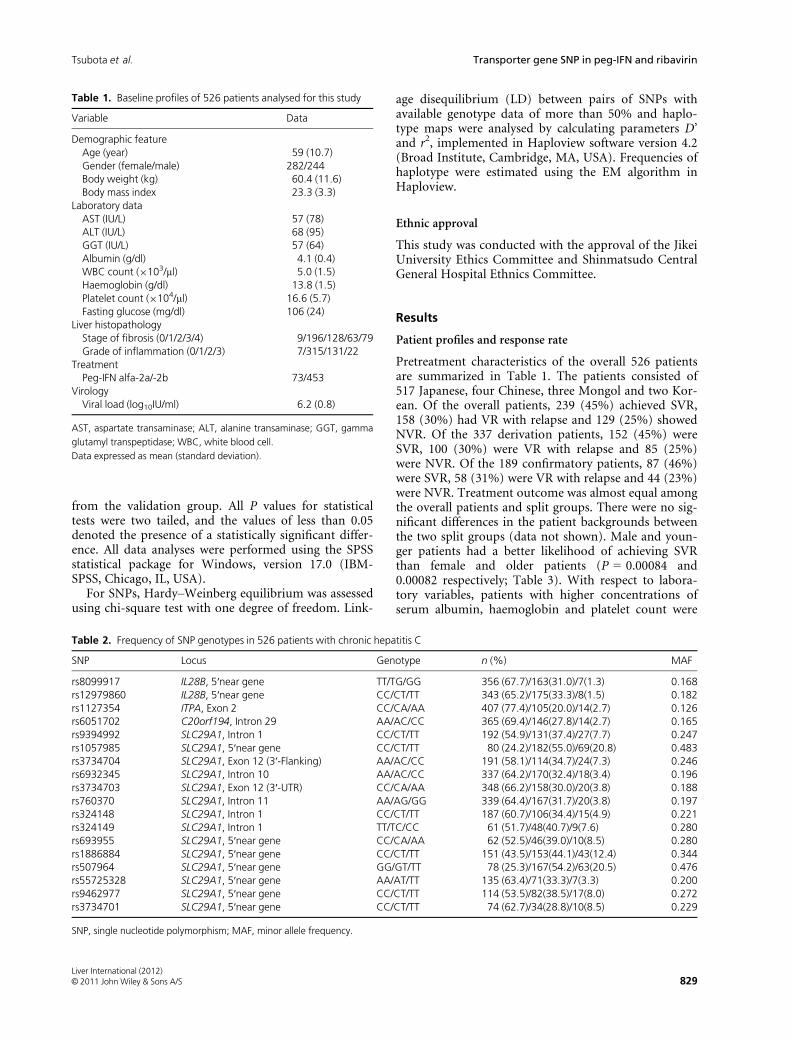
Pretreatment characteristics of the overall 526 patientsare summarized in Table 1. The patients consisted of517 Japanese, four Chinese, three Mongol and two Kor-ean. Of the overall patients, 239 (45%) achieved SVR,158 (30%) had VR with relapse and 129 (25%) showedNVR. Of the 337 derivation patients, 152 (45%) wereSVR, 100 (30%) were VR with relapse and 85 (25%)were NVR. Of the 189 confirmatory patients, 87 (46%)were SVR, 58 (31%) were VR with relapse and 44 (23%)were NVR. Treatment outcome was almost equal amongthe overall patients and split groups. There were no sig-nificant differences in the patient backgrounds betweenthe two split groups (data not shown). Male and youn-ger patients had a better likelihood of achieving SVRthan female and older patients (P = 0.00084 and0.00082 respectively; Table 3). With respect to labora-tory variables, patients with higher concentrations ofserum albumin, haemoglobin and platelet count were
Table 1. Baseline profiles of 526 patients analysed for this study
Variable Data
Demographic featureAge (year) 59 (10.7)Gender (female/male) 282/244Body weight (kg) 60.4 (11.6)Body mass index 23.3 (3.3)
Laboratory dataAST (IU/L) 57 (78)ALT (IU/L) 68 (95)GGT (IU/L) 57 (64)Albumin (g/dl) 4.1 (0.4)WBC count (9103/ll) 5.0 (1.5)Haemoglobin (g/dl) 13.8 (1.5)Platelet count (9104/ll) 16.6 (5.7)Fasting glucose (mg/dl) 106 (24)
Liver histopathologyStage of fibrosis (0/1/2/3/4) 9/196/128/63/79Grade of inflammation (0/1/2/3) 7/315/131/22
TreatmentPeg-IFN alfa-2a/-2b 73/453
VirologyViral load (log10IU/ml) 6.2 (0.8)
AST, aspartate transaminase; ALT, alanine transaminase; GGT, gamma
glutamyl transpeptidase; WBC, white blood cell.
Data expressed as mean (standard deviation).
Table 2. Frequency of SNP genotypes in 526 patients with chronic hepatitis C
SNP Locus Genotype n (%) MAF
rs8099917 IL28B, 5′near gene TT/TG/GG 356 (67.7)/163(31.0)/7(1.3) 0.168rs12979860 IL28B, 5′near gene CC/CT/TT 343 (65.2)/175(33.3)/8(1.5) 0.182rs1127354 ITPA, Exon 2 CC/CA/AA 407 (77.4)/105(20.0)/14(2.7) 0.126rs6051702 C20orf194, Intron 29 AA/AC/CC 365 (69.4)/146(27.8)/14(2.7) 0.165rs9394992 SLC29A1, Intron 1 CC/CT/TT 192 (54.9)/131(37.4)/27(7.7) 0.247rs1057985 SLC29A1, 5′near gene CC/CT/TT 80 (24.2)/182(55.0)/69(20.8) 0.483rs3734704 SLC29A1, Exon 12 (3′-Flanking) AA/AC/CC 191 (58.1)/114(34.7)/24(7.3) 0.246rs6932345 SLC29A1, Intron 10 AA/AC/CC 337 (64.2)/170(32.4)/18(3.4) 0.196rs3734703 SLC29A1, Exon 12 (3′-UTR) CC/CA/AA 348 (66.2)/158(30.0)/20(3.8) 0.188rs760370 SLC29A1, Intron 11 AA/AG/GG 339 (64.4)/167(31.7)/20(3.8) 0.197rs324148 SLC29A1, Intron 1 CC/CT/TT 187 (60.7)/106(34.4)/15(4.9) 0.221rs324149 SLC29A1, Intron 1 TT/TC/CC 61 (51.7)/48(40.7)/9(7.6) 0.280rs693955 SLC29A1, 5′near gene CC/CA/AA 62 (52.5)/46(39.0)/10(8.5) 0.280rs1886884 SLC29A1, 5′near gene CC/CT/TT 151 (43.5)/153(44.1)/43(12.4) 0.344rs507964 SLC29A1, 5′near gene GG/GT/TT 78 (25.3)/167(54.2)/63(20.5) 0.476rs55725328 SLC29A1, 5′near gene AA/AT/TT 135 (63.4)/71(33.3)/7(3.3) 0.200rs9462977 SLC29A1, 5′near gene CC/CT/TT 114 (53.5)/82(38.5)/17(8.0) 0.272rs3734701 SLC29A1, 5′near gene CC/CT/TT 74 (62.7)/34(28.8)/10(8.5) 0.229
SNP, single nucleotide polymorphism; MAF, minor allele frequency.
Liver International (2012)© 2011 John Wiley & Sons A/S 829
Tsubota et al. Transporter gene SNP in peg-IFN and ribavirin
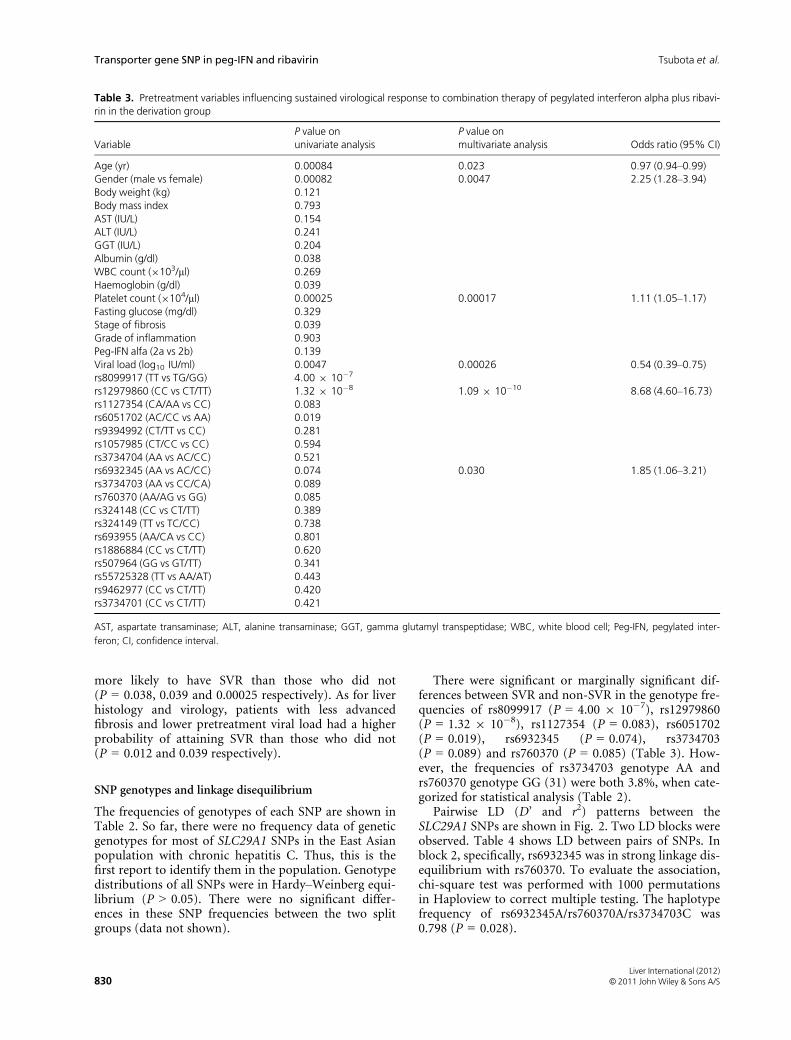
more likely to have SVR than those who did not(P = 0.038, 0.039 and 0.00025 respectively). As for liverhistology and virology, patients with less advancedfibrosis and lower pretreatment viral load had a higherprobability of attaining SVR than those who did not(P = 0.012 and 0.039 respectively).
SNP genotypes and linkage disequilibrium
The frequencies of genotypes of each SNP are shown inTable 2. So far, there were no frequency data of geneticgenotypes for most of SLC29A1 SNPs in the East Asianpopulation with chronic hepatitis C. Thus, this is thefirst report to identify them in the population. Genotypedistributions of all SNPs were in Hardy–Weinberg equi-librium (P > 0.05). There were no significant differ-ences in these SNP frequencies between the two splitgroups (data not shown).
There were significant or marginally significant dif-ferences between SVR and non-SVR in the genotype fre-quencies of rs8099917 (P = 4.00 9 10�7), rs12979860(P = 1.32 9 10�8), rs1127354 (P = 0.083), rs6051702(P = 0.019), rs6932345 (P = 0.074), rs3734703(P = 0.089) and rs760370 (P = 0.085) (Table 3). How-ever, the frequencies of rs3734703 genotype AA andrs760370 genotype GG (31) were both 3.8%, when cate-gorized for statistical analysis (Table 2).
Pairwise LD (D’ and r2) patterns between theSLC29A1 SNPs are shown in Fig. 2. Two LD blocks wereobserved. Table 4 shows LD between pairs of SNPs. Inblock 2, specifically, rs6932345 was in strong linkage dis-equilibrium with rs760370. To evaluate the association,chi-square test was performed with 1000 permutationsin Haploview to correct multiple testing. The haplotypefrequency of rs6932345A/rs760370A/rs3734703C was0.798 (P = 0.028).
Table 3. Pretreatment variables influencing sustained virological response to combination therapy of pegylated interferon alpha plus ribavi-rin in the derivation group
VariableP value onunivariate analysis
P value onmultivariate analysis Odds ratio (95% CI)
Age (yr) 0.00084 0.023 0.97 (0.94–0.99)Gender (male vs female) 0.00082 0.0047 2.25 (1.28–3.94)Body weight (kg) 0.121Body mass index 0.793AST (IU/L) 0.154ALT (IU/L) 0.241GGT (IU/L) 0.204Albumin (g/dl) 0.038WBC count (9103/ll) 0.269Haemoglobin (g/dl) 0.039Platelet count (9104/ll) 0.00025 0.00017 1.11 (1.05–1.17)Fasting glucose (mg/dl) 0.329Stage of fibrosis 0.039Grade of inflammation 0.903Peg-IFN alfa (2a vs 2b) 0.139Viral load (log10 IU/ml) 0.0047 0.00026 0.54 (0.39–0.75)rs8099917 (TT vs TG/GG) 4.00 9 10�7
rs12979860 (CC vs CT/TT) 1.32 9 10�8 1.09 9 10�10 8.68 (4.60–16.73)rs1127354 (CA/AA vs CC) 0.083rs6051702 (AC/CC vs AA) 0.019rs9394992 (CT/TT vs CC) 0.281rs1057985 (CT/CC vs CC) 0.594rs3734704 (AA vs AC/CC) 0.521rs6932345 (AA vs AC/CC) 0.074 0.030 1.85 (1.06–3.21)rs3734703 (AA vs CC/CA) 0.089rs760370 (AA/AG vs GG) 0.085rs324148 (CC vs CT/TT) 0.389rs324149 (TT vs TC/CC) 0.738rs693955 (AA/CA vs CC) 0.801rs1886884 (CC vs CT/TT) 0.620rs507964 (GG vs GT/TT) 0.341rs55725328 (TT vs AA/AT) 0.443rs9462977 (CC vs CT/TT) 0.420rs3734701 (CC vs CT/TT) 0.421
AST, aspartate transaminase; ALT, alanine transaminase; GGT, gamma glutamyl transpeptidase; WBC, white blood cell; Peg-IFN, pegylated inter-
feron; CI, confidence interval.
Liver International (2012)© 2011 John Wiley & Sons A/S830
Transporter gene SNP in peg-IFN and ribavirin Tsubota et al.

Pretreatment factors associated with SVR
Multiple logistic regression analysis identified six inde-pendent variables that were significantly associated with
SVR (Table 3): age [P = 0.023, odds ratio (OR) = 0.97,95% confidence interval (CI) = 0.94–0.99], gender(P = 0.0047, OR = 2.25, 95% CI = 1.28–3.94), plateletcount (P = 0.00017, OR = 1.11, 95% CI = 1.05–1.17),pretreatment viral load (P = 0.00026, OR = 0.54, 95%CI = 0.39–0.75), rs12979860 (P = 1.09 9 10�7, OR =8.68, 95% CI = 4.60–16.73) and rs6932345 (P = 0.030,OR = 1.85, 95% CI = 1.06–3.21). The model wasexpressed as: S = �1.238�0.031 9 Age (by year)+ 0.809 9 Gender (where male was 1 and female was 0)+ 0.104 9 Platelet count (by 1.0 9 104/lL) � 0.614 9Viral load (by log10 IU/ml) + 2.161 9 rs12979860(where genotype CC was 1 and CT/TT was 0) + 0.6149 rs6932345 (where genotype AA was 1 and AC/CC was0). P values were 0.476 and 2.29 9 10�17 in Hosmer–Lemeshow test and likelihood-ratio chi-squaretest respectively. Positive and negative predictive valuesand predictive accuracy were 73.3, 70.1 and 71.9%respectively.
Validation of the model
When the model was used for the confirmatory group,positive and negative predictive values and predictiveaccuracy were 71.4, 84.6 and 75.3% respectively. For theoverall patients, they were 71.6, 75.2 and 73.1% respec-tively.
Association of SLC29A1 SNP with RVR
RVR, an on-treatment factor, is one of the strongestindependent predictors of SVR (42–45). Using data ofthe overall 526 patients, only 74 (14%) achieved RVR.Of the 74 RVR patients, 69 (93%) achieved SVR. Of theremaining 452 non-RVR patients, 170 (38%) achievedSVR (P = 6.62 9 10�15). This variable, strongly predic-tive of SVR together with pretreatment variables, wasincorporated into multiple logistic regression analysis,and the statistical analysis was re-performed: age(P = 0.013, OR = 0.97, 95% CI = 0.95–0.99), gender(P = 0.0075, OR = 1.81, 95% CI = 1.17–2.81), RVR(lack vs attainment, P = 6.47 9 10�7, OR = 13.4, 95%CI = 4.82–37.16), rs12979860 (P = 8.09 9 10�17,OR = 10.17, 95% CI = 5.89–17.55), rs6932345(P = 0.045, OR = 1.57, 95% CI = 1.01–2.45), plateletcount (P = 0.00014, OR = 1.08, 95% CI = 1.04–1.13)and pretreatment viral load (P = 0.010, OR = 0.66,95% CI = 0.49–0.91).
Next, the association of SLC29A1 SNP with RVR wasevaluated, because its significance was recently reported(31). On univariate analyses, five variables were signifi-cantly or marginally associated with RVR: pretreatmentviral load (P = 3.21 9 10�13), rs12979860 (P = 3.39 910�5), rs8099917 (P = 6.35 9 10�5), rs6932345 (P =0.012) and serum albumin concentration (P = 0.066).Multiple logic regression analysis identified four signifi-cantly independent variables: pretreatment viral load(P = 1.11 9 10�12, OR = 0.29, 95% CI = 0.21–0.41),
Fig. 2. Pairwise linkage disequilibrium diagrams for SLC29A1. Theblock structure was constructed by calculating D′ and r2. In the D’diagram (upper), regions with high values are deep red, and thosewith low values are lighter shades of red. In the r2 diagram (lower),regions with high values are dark grey, and those with low valuesare lighter shades of grey.
Table 4. Linkage disequilibrium between pairs of SNPs within hap-lotype blocks
SNP1 SNP2 D’ (95% CI) r2
Block 1rs1057985 rs507964 0.99 (0.96–1.00) 0.975Block 2rs6932345 rs760370 0.98 (0.95–1.00) 0.953rs6932345 rs3734703 0.97 (0.93–0.99) 0.873rs6932345 rs3734704 0.95 (0.89–0.98) 0.696rs760370 rs3734703 0.96 (0.92–0.99) 0.861rs760370 rs3734704 0.96 (0.90–0.99) 0.706rs3734703 rs3734704 1.00 (0.96–1.00) 0.711
CI, confidence interval.
Liver International (2012)© 2011 John Wiley & Sons A/S 831
Tsubota et al. Transporter gene SNP in peg-IFN and ribavirin

rs12979860 (P = 1.70 9 10�5, OR = 5.78, 95% CI =2.60–12.86), rs6932345 (P = 0.0082, OR = 2.44, 95%CI = 1.26–4.73) and serum albumin concentration(P = 0.00029, OR = 5.21, 95% CI = 2.13–12.74).
Factors influencing haemolytic anaemia
Changes in haemoglobin concentrations from baselineto week 4 of treatment ranged from 0.1 to 6.9 g/dl(median, 2.3 g/dl) for the overall patients. They were0.1–6.9 g/dl (median, 2.3 g/dl) in patients withrs6932345 genotype AC/CC, and 0.1–6.6 g/dl (median,2.4 g/dl) in those with rs6932345 genotype AA(P = 0.248). In contrast, they were 0.1–6.9 g/dl (med-ian, 2.6 g/dl) in patients with rs1127354 genotype CC,and 0.1–4.4 g/dl (median, 1.0 g/dl) in those withrs1127354 genotype CA/AA (P = 8.40 9 10�19). Weanalysed factors affecting clinically significant anaemia,defined either as a decline in haemoglobin concentra-tions of more than 3 g/dl or haemoglobin concentra-tions of less than 10 g/dl at week 4 of treatment, whichis the threshold at which ribavirin dose reduction is rec-ommended (35). None of SLA29A1 SNPs showed signif-icant or marginal association with treatment-inducedhaemolytic anaemia in univariate analyses. Multiplelogistic regression analysis identified only two variablesas significantly independent factors associated with clin-ically significant anaemia: gender (female vs male, P =0.029, OR = 1.64, 95% CI = 1.05–2.56) and rs1127354(CA/AA vs CC, P = 4.13 9 10�7, OR = 14.37, 95%CI = 5.12–40.32).
Serum ribavirin concentration
Trough concentrations of serum ribavirin at week 4 oftreatment were preliminarily measured using availableserum samples obtained from patients with rs6932345genotype AA (n = 40) and AC/CC (n = 30). Troughribavirin concentrations ranged from 844 to 3812 ng/ml(median, 2150 ng/ml). There were marginally signifi-cant differences between patients with rs6932345 geno-type AA (range, 1319–3812 ng/ml; median, 2359 ng/ml) and AC/CC (844–2488 ng/ml and 2027 ng/mlrespectively; P = 0.052, Fig. 3).
Discussion
Identification of factors predictive of treatmentresponse, including host-, virus- and treatment-relatedfeatures, provides insights into the development oftreatment algorism and the clarification of antiviralmechanisms. So far, numerous studies have identifiedvarious factors that could influence the probability oftreatment response. As shown by several genome-wideassociation studies (32–34), treatment response of HCVgenotype 1 patients is strongly linked to host geneticfactors, such as SNPs nearby the IL28B gene[rs12979860 (32), rs12980275 and rs8099917 (33, 34)].
At present, the SNPs are one of the strongest indepen-dent baseline predictors of SVR or NVR to peg-IFNalpha plus ribavirin or triple combination therapyincluding STAT-C agents, in addition to HCV genotype.This multiple logistic regression analysis for the EastAsian cohort also showed that rs12979860, but notrs8099917, yielded the lowest or lower P values ofachieving both SVR and RVR compared with otherbaseline variables. The findings that the frequencies ofrs12979860 C-allele and the favourable genotype CCwere high (82 and 65% respectively, Table 2) supportthe close correlation between rs12979860 and ethnicity:its frequency is the highest in East Asians among diverseethnic groups (32). Despite the highly prevalent distri-bution of the favourable SNP genotype, only 45% of thisEast Asian cohort achieved SVR. The unexpected out-come might result from the fact that the SVR rate wasnot necessarily high in the East Asian patients withgenotype CC (60%, 206/343) compared with those ofthe Caucasian (69–82%) and African-American (48–53%) populations with the same genotype CC (32, 46).The racial differences in the SVR rate among genotypeCC patients suggest that any factors other than thestrongest predictor IL28B SNP would influence thetreatment response. Therefore, it remains highly unli-kely that IL28B SNP is used alone to decide differenttreatment strategies.
The SNP rs760370 genotype GG at the SLC29A1 genelocated at chromosome 6 was recently reported to asso-ciate significantly and independently with an increasedlikelihood of RVR (> 15-fold, P = 0.007), comparedwith genotype AA/AG, in patients coinfected with HCVand HIV (31). In the White-predominant population,
(ng/ml)
Tro
ugh
conc
entr
atio
ns o
f ser
um r
ibav
irin
AA AC/CC
Fig. 3. Trough concentrations of serum ribavirin at week 4 of treat-ment according to SLC29A1 SNP rs6932345. There were marginallysignificant differences in trough concentrations of serum ribavirinat week 4 of treatment between patients with rs6932345 genotypeAA (range, 1319–3812 ng/ml; median, 2359 ng/ml) and AC/CC(844–2488 ng/ml and 2027 ng/ml respectively; P = 0.052).
Liver International (2012)© 2011 John Wiley & Sons A/S832
Transporter gene SNP in peg-IFN and ribavirin Tsubota et al.

the frequencies of genotype AA, AG and GG were 39%(43/109), 46% (50/109) and 15% (16/109) respectively.They differ considerably from those observed in thisstudy (Table 2): the favourable genotype GG frequencywas only 3.8% (20/526) in the HCV-monoinfected EastAsian population, suggesting that other SLC29A1 SNPsmay differ between different ethnics. To the best of ourknowledge, this is the first report to provide frequencydata of genetic genotypes for SLC29A1 SNPs in the EastAsian population with chronic hepatitis C. Multivariateanalysis in this study identified SLC29A1 SNP rs6932345as a significantly independent factor of both RVR andSVR, even when analysed along with host genetic factors(IL28B and ITPA SNPs) strongly influencing treatmentresponse. Of note, this study revealed that rs6932345was in strong linkage disequilibrium with rs760370.However, the impact of SNP rs6932345 on SVR wasmarginally significant on univariate analysis, and rela-tively weak compared with other independent pretreat-ment factors on the final step of multivariate analysis.The lower association between the SLC29A1 SNPs andSVR was also recognized in other study (31). Moreintensive treatment such as prolongation of treatmentto 72 weeks might diminish the significance of somebaseline factors including the SLC29A1 SNPs in predict-ing the probability of SVR. Alternatively, there weresome limitations in these studies. As selection criteriafor the analysis (an allelic frequency > 0.2) restrictedpart of the registered SNPs on the database, there is thepossibility that other important SNPs at the SLC29A1gene might be lost. Furthermore, the function or impli-cation of most of the SLC29A1 SNPs is not yet under-stood fully.
This study suggested the possibility that SLC29A1SNP rs6932345 might be partly associated with troughconcentrations of serum ribavirin, although marginallysignificant. Recently, ENT1 mRNA expression levelswere reported to differ among hepatocyte lines derivedfrom healthy individuals (30). Characterization of theSLC29A1 gene structure clarified the existence of severalENT1 mRNA isoforms in the human liver. The differentENT1-mediated ribavirin uptake levels were associatedwith different expression levels of specific isoforms ofENT1 mRNA (30). Some SLC29A1 SNPs, such asrs6932345, might be related to the expression and/orisoforms of ENT1 mRNA, thereby influencing the activ-ity and the function, although the mechanism remainsunknown. In pharmacokinetics and pharmacodynamicsof ribavirin, it remains unclear as to how SLC29A1 SNPsare involved in the cellular uptake at absorption andexcretion sites, because ENT1 is also expressed in en-terocytes (25, 29, 47, 48) and renal epithelial cells (25,49). Furthermore, there may be some contributionof other ribavirin transports or yet unidentified addi-tional systems (27, 30). Currently, we are developing anin vitro experimental system and investigating whetherSLC29A1 SNPs or the mRNA isoforms could cause thedifference in the hepatic expression, activity and/or
function, and influence hepatocellular uptake levels andintra- and extracellular concentrations of ribavirin.
RVR is highly predictive of SVR, and thus a strongindependent on-treatment predictor (42–45). Response-guided therapy based on RVR has been also utilized inrecent trials of triple combination therapy with peg-IFNalpha, ribavirin and the protease inhibitor telaprevir inHCV genotype 1 patients (6, 7). When achievement ofRVR was incorporated into the model for SVR in thisstudy, it yielded the high odds ratio, independent ofIL28B SNP rs12979860, which was a significantly inde-pendent predictor of RVR. Caucasian patients with thefavourable rs12979860 CC genotype were more likely tohave RVR (28%) than African Americans with the samegenotype (15%)(46). In this East Asian cohort, 64 of343 CC genotype patients (19%) achieved RVR. Thus,racial disparities were still evident in that the RVR ratesdiffered among African Americans, Caucasians and EastAsians with the same favourable genotype CC. However,patients with RVR appear to have consistently high SVRrates, irrespective of IL28B genotype and race. Con-versely, these data further underscore the acceptednotion that achievement of RVR is strongly associatedwith a high likelihood of SVR and the most stable mile-stone in the response-guided treatment across IL28Bgenotypes and races.
SNPs within or nearby the ITPA gene, rs7270101,rs6051702 and rs1127354 possess genetic variants lead-ing to ITPA deficiency that confers protection againstribavirin-induced haemolytic anaemia (35–37). Thegenetic variants differ considerably among ethnicgroups or geographical areas (35–37). Indeed, the splic-ing variant-related SNP rs7270101 is not polymorphousin the Japanese population with chronic HCV genotype1b infection (36, 37, our unpublished data) as well ashealthy Japanese controls in the HapMap database, andwas thus excluded from this study. Multivariate analysisin this study reconfirmed that rs1127354, but notrs6051702 (35), is independently and strongly responsi-ble for protection against treatment-induced haemolyticanaemia in the East Asian genetic cohort, which meansthat the ITPA minor variant A is a protective allele forthe anaemia (36, 37). Despite less need for dose reduc-tion and greater cumulative exposure of ribavirin, mul-tivariate analysis in this study also showed that theseSNPs have no significant association with RVR (35) orSVR (35, 36, 50). Concerning SNPs at the SLC29A1gene, those analysed in this study had no significantimpact on treatment-induced anaemia. Further investi-gation is required to clarify the correlation of otherSLC29A1 SNPs, ENT1 function and intracellular ribavi-rin concentrations with ribavirin-induced haemolyticanaemia.
In this study, host factors other than host geneticSNPs, such as younger age, female gender and higherplatelet count, were significantly independent contribu-tors to favourable treatment response. These findingscoincide with those reported in a multicenter study
Liver International (2012)© 2011 John Wiley & Sons A/S 833
Tsubota et al. Transporter gene SNP in peg-IFN and ribavirin

from Japan (51). Patient age and thrombopoietin-stim-ulated thrombocyte production capacity may reflectliver condition and liver disease stage, including reactiv-ity to treatment, patient tolerance and pharmacologicalmetabolism. The underlying backgrounds and mecha-nism is not exactly understood. Certain factors associ-ated with a lower treatment response in female gendercould not be identified (51).
In conclusion, SNP rs6932345 at the major ribavirintransporter ENT1 gene SLC29A1 was one of signifi-cantly independent genetic factors associated withboth RVR and SVR in peg-IFN alpha plus ribavirintherapy for East Asian patients monoinfected withHCV genotype 1b, although the impact on the predic-tion of treatment response was small. The significantcontribution, independent of the singular predictorIL28B SNPs, may provide an important clue to under-stand the pharmacokinetics and pharmacodynamics ofribavirin and the mechanisms by which ribavirinexerts antiviral actions within cells, and to develop theindividual tailoring and optimization of ribavirin-related therapeutics.
Acknowledgments
We thank physicians and staff members at ShinmatsudoCentral General Hospital and Aoto Hospital and Kas-hiwa Hospital, the Jikei University School of Medicinefor their help.
Funding: This work was supported in part by ClinicalResearch Funds from Department of Gastroenterologyand Hepatology, Aoto Hospital, Jikei University Schoolof Medicine and Shinmatsudo Central General Hospital.
Competing interests: None declared.Provenance and peer review: Not commissioned;
externally peer reviewed.
Author contributions
Tsubota A, Shimada N and Aizawa Y designed research;Tsubota A, Shimada N, Yoshizawa K, Agata R, Abe H,Ika M, Fujise K and Aizawa Y performed clinicalresearch and collected data (Yoshizawa K, Abe H, Ika Mand Fujise K are clinical investigators); Tsubota A, Shi-mada N and Aizawa Y analysed and interpreted data;Agata R and Yumoto Y provided technical help; Furih-ata T, Namiki Y, Chiba K and Tada N were scientificadvisors and critically reviewed the paper; and TsubotaA, Shimada N and Aizawa Y wrote the paper.
References
1. Ghany MG, Strader DB, Thomas DL, et al. Diagnosis,management, and treatment of hepatitis C: an update.Hepatology 2009; 49: 1335–74.
2. Poynard T, Marcellin P, Lee SS, et al. Randomised trial ofinterferon alpha 2b plus ribavirin for 48 weeks or for
24 weeks versus interferon alpha 2b plus placebo for48 weeks for treatment of chronic infection with hepatitisC virus. Lancet 1998; 352: 1426–32.
3. Manns MP, McHutchison JG, Gordon SC, et al. Peginter-feron alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitisC: a randomised trial. Lancet 2001; 358: 958–65.
4. Fried MW, Shiffman ML, Reddy KR, et al. Peginterferonalfa-2a plus ribavirin for chronic hepatitis C virus infec-tion. N Engl J Med 2002; 347: 975–82.
5. Di Bisceglie AM, Conjeevaram HS, Fried MW, et al. Riba-virin as therapy for chronic hepatitis C. A randomized,double-blind, placebo-controlled trial. Ann Intern Med1995; 123: 897–903.
6. McHutchison JG, Everson GT, Gordon SC, et al. Telapre-vir with peginterferon and ribavirin for chronic HCVgenotype 1 infection. N Engl J Med 2009; 360: 1827–38.
7. Hezode C, Forestier N, Dusheiko G, et al. Telaprevir andpeginterferon with or without ribavirin for chronic HCVinfection. N Engl J Med 2009; 360: 1839–50.
8. Kwo PY, Lawitz EJ, McCone J, et al. Efficacy of bocepre-vir, an NS3 protease inhibitor, in combination with pegin-terferon alfa-2b and ribavirin in treatment-naive patientswith genotype 1 hepatitis C infection (SPRINT-1): anopen-label, randomised, multicentre phase 2 trial. Lancet2010; 376: 705–16.
9. Feld J, Hoofnagle J. Mechanism of action of interferonand ribavirin in treatment of hepatitis C. Nature 2005;436: 967–72.
10. Dixit NM, Perelson AS. The metabolism, pharmacokinet-ics and mechanisms of antiviral activity of ribavirin againsthepatitis C virus. Cell Mol Life Sci 2006; 63: 832–42.
11. Hofmann W, Herrmann E, Sarrazin C, et al. Ribavirinmode of action in chronic hepatitis C: from clinical useback to molecular mechanisms. Liver Int 2008; 28: 1332–43.
12. Di Stefano G, Colonna FP, Bongini A, et al. Ribavirin con-jugated with lactosaminated poly-L-lysine: selective deliv-ery to the liver and increased antiviral activity in mice withviral hepatitis. Biochem Pharmacol 1997; 54: 357–63.
13. Levy GA, Adamson G, Phillips MJ, et al. Targeted deliveryof ribavirin improves outcome of murine viral fulminanthepatitis via enhanced antiviral activity. Hepatology 2006;43: 581–91.
14. Tsubota A, Hirose Y, Izumi N, et al. Pharmacokinetics ofribavirin in combined interferon alpha-2b and ribavirintherapy for chronic hepatitis C virus infection. Br J ClinPharmacol 2003; 55: 360–7.
15. Shiffman ML, Di Bisceglie AM, Lindsay KL, et al. Pegin-terferon alfa-2a and ribavirin in patients with chronic hep-atitis C who have failed prior treatment. Gastroenterology2004; 126: 1015–23.
16. Bronowicki JP, Ouzan D, Asselah T, et al. Effect of ribavi-rin in genotype 1 patients with hepatitis C responding topegylated interferon alfa-2a plus ribavirin. Gastroenterol-ogy 2006; 131: 1040–8.
17. Reddy KR, Shiffman ML, Morgan TR, et al. Impact ofribavirin dose reductions in hepatitis C virus genotype 1patients completing peginterferon alfa-2a/ribavirin treat-ment. Clin Gastroenterol Hepatol 2007; 5: 124–9.
18. Morello J, Rodriguez-Novoa S, Jimenez-Nacher I, et al.Usefulness of monitoring ribavirin plasma concentra-tions to improve treatment response in patients with
Liver International (2012)© 2011 John Wiley & Sons A/S834
Transporter gene SNP in peg-IFN and ribavirin Tsubota et al.

chronic hepatitis C. J Antimicrob Chemother 2008; 62:1174–80.
19. Hiramatsu N, Oze T, Yakushijin T, et al. Ribavirin dosereduction raises relapse rate dose-dependently in genotype 1patients with hepatitis C responding to pegylated interferonalpha-2b plus ribavirin. J ViralHepat 2009; 16: 586–94.
20. Sulkowski MS, Shiffman ML, Afdhal NH, et al. HepatitisC virus treatment-related anemia is associated with highersustained virologic response rate. Gastroenterology 2010;139: 1602–11.
21. Griffiths M, Beaumont N, Yao SY, et al. Cloning of ahuman nucleoside transporter implicated in the cellularuptake of adenosine and chemotherapeutic drugs. NatMed 1997; 3: 89–93.
22. Baldwin SA, Beal PR, Yao SY, et al. The equilibrativenucleoside transporter family, SLC29. Eur J Physiol 2004;447: 735–43.
23. Molina-Arcas M, Casado FJ, Pastor-Anglada M. Nucleo-side transporter proteins. Current Vascular Pharmacology2009; 7: 426–34.
24. Yamamoto T, Kuniki K, Takekuma Y, et al. Ribavirinuptake by cultured human choriocarcinoma (BeWo) cellsand Xenopus laevis oocytes expressing recombinantplasma membrane human nucleoside transporters. Eur JPharmacol 2007; 557: 1–8.
25. Govindarajan R, Bakken AH, Hudkins KL, et al. In situhybridization and immunolocalization of concentrativeand equilibrative nucleoside transporters in the humanintestine, liver, kidneys, and placenta. Am J Physiol RegulIntegr Comp Physiol 2007; 293: R1809–22.
26. Jarvis S, Thorn J, Glue P. Ribavirin uptake by human ery-throcytes and the involvement of nitrobenzylthioinosine-sensitive (es)-nucleoside transporters. Br J Pharmacol1998; 123: 1587–92.
27. Govindarajan R, Endres C, Whittington D, et al. Expres-sion and hepatobiliary transport characteristics of the con-centrative and equilibrative nucleoside transporters insandwich-cultured human hepatocytes. Am J Physiol Gas-trointest Liver Physiol 2008; 295: G570–80.
28. Endres C, Moss A, Ke B, et al. The role of the equilibrativenucleoside transporter 1 (ENT1) in transport and metabo-lism of ribavirin by human and wild-type or Ent1(-/-)mouse erythrocytes. J Pharmacol Exp Ther 2009; 329: 387–98.
29. Endres C, Moss AM, Govindarajan R, et al. The role ofnucleoside transporters in the erythrocyte disposition andoral absorption of ribavirin in the wild-type and equilibra-tive nucleoside transporter 1-/- mice. J Pharmacol ExpTher 2009; 331: 287–96.
30. Fukuchi Y, Furihata T, Hashizume M, et al. Characteriza-tion of ribavirin uptake systems in human hepatocytes.J Hepatol 2010; 52: 486–492.
31. Morello J, Cuenca L, Soriano V, et al. Influence of a singlenucleotide polymorphism at the main ribavirin trans-porter gene on the rapid virological response to pegylatedinterferon-ribavirin therapy in patients with chronic hepa-titis C virus infection. J Infect Dis 2010; 202: 1185–91.
32. Ge D, Fellay J, Thompson A, et al. Genetic variation inIL28B predicts hepatitis C treatment-induced viral clear-ance. Nature 2009; 461: 399–401.
33. Suppiah V, Moldovan M, Ahlenstiel G, et al. IL28B isassociated with response to chronic hepatitis C interferon-a and ribavirin therapy. Nat Genet 2009; 41: 1100–4.
34. Tanaka Y, Nishida N, Sugiyama M, et al. Genome-wideassociation of IL28B with response to pegylated inter-feron-a and ribavirin therapy for chronic hepatitis C. NatGenet 2009; 41: 1105–9.
35. Fellay J, Thompson AJ, Ge D, et al. ITPA gene variantsprotect against anaemia in patients treated for chronichepatitis C. Nature 2010; 464: 405–8.
36. Ochi H, Maekawa T, Abe H, et al. ITPA polymorphismaffects ribavirin-induced anemia and outcomes of therapy–a genome-wide study of Japanese HCV virus patients.Gastroenterology 2010; 139: 1190–7.
37. Sakamoto N, Tanaka Y, Nakagawa M, et al. ITPA genevariant protects against anemia induced by pegylatedinterferon-a and ribavirin therapy for Japanese patientswith chronic hepatitis C. Hepatol Res 2010; 40: 1063–71.
38. Tsubota A, Arase Y, Someya T, et al. Early viral kineticsand treatment outcome in combination of high-doseinterferon induction vs. pegylated interferon plus ribavi-rin for naive patients infected with hepatitis C virus ofgenotype 1b and high viral load. J Med Virol 2005; 75:27–34.
39. Ichida F, Tsuji T, Omata M, et al. New inuyama classifica-tion; new criteria for histological assessment of chronichepatitis. Int Hepatol Commun 1996; 6: 112–9.
40. Kim SR, Saito Y, Maekawa K, et al. Thirty novel geneticvariations in the SLC29A1 gene encoding human equili-brative nucleoside transporter 1 (hENT1). Drug MetabPharmacokinet 2006; 21: 248–56.
41. Khakoo S, Glue P, Grellier L, et al. Ribavirin and inter-feron alfa-2b in chronic hepatitis C: assessment of possiblepharmacokinetic and pharmacodynamic interactions. Br JClin Pharmacol 1998; 46: 563–70.
42. Ferenci P, Fried MW, Shiffman ML, et al. Predicting sus-tained virological responses in chronic hepatitis C patientstreated with peginterferon alfa-2a (40 KD)/ribavirin. J Hep-atol 2005; 43: 425–33.
43. Jensen DM, Morgan TR, Marcellin P, et al. Early identifi-cation of HCV genotype 1 patients responding to24 weeks peginterferon alpha-2a (40 kd)/ribavirin therapy.Hepatology 2006; 43: 954–60.
44. Barcena R, Moreno A, del Campo S, et al. The magnitudeof week 4 HCV RNA decay on pegylated interferon/ribavi-rin accurately predicts virological failure in patients withgenotype 1. Antivir Ther 2007; 12: 401–6.
45. Fried MW, Hadziyannis SJ, Shiffman ML, et al. Rapidvirological response is the most important predictor ofsustained virological response across genotypes in patientswith chronic hepatitis C virus infection. J Hepatol 2011;55: 69–75.
46. Thompson AJ, Muir AJ, Sulkowski MS, et al. Interleukin-28B polymorphism improves viral kinetics and is thestrongest pretreatment predictor of sustained virologicresponse in hepatitis C virus-1 patients. Gastroenterology2010; 139: 120–9.
47. Patil S, Ngo L, Glue P, et al. Intestinal absorption ofribavirin is preferentially mediated by the Na + -nucle-oside purine (N1) transporter. Pharm Res 1998; 15:950–2.
48. Takaai M, Morishita H, Ishida K, et al. Contribution ofNa + -independent nucleoside transport to ribavirinuptake in the rat intestine and human epithelial LS180cells. Eur J Pharmacol 2008; 601: 61–5.
Liver International (2012)© 2011 John Wiley & Sons A/S 835
Tsubota et al. Transporter gene SNP in peg-IFN and ribavirin

49. Mangravite L, Badagnani I, Giacomini K. Nucleosidetransporters in the disposition and targeting of nucleo-side analogs in the kidney. Eur J Pharmacol 2003; 479:269–81.
50. Thompson AJ, Fellay J, Patel K, et al. Variants in the ITPAgene protect against ribavirin-induced hemolytic anemia
and decrease the need for ribavirin dose reduction. Gastro-enterology 2010; 139: 1181–9.
51. Okanoue T, Itoh Y, Hashimoto H, et al. Predictive valuesof amino acid sequences of the core and NS5A regions inantiviral therapy for hepatitis C: a Japanese multi-centerstudy. J Gastroenterol 2009; 44: 952–63.
Liver International (2012)© 2011 John Wiley & Sons A/S836
Transporter gene SNP in peg-IFN and ribavirin Tsubota et al.
Related Documents











