CLINICAL—LIVER, PANCREAS, AND BILIARY TRACT Peginterferon alfa-2b and Ribavirin: Effective in Patients With Hepatitis C Who Failed Interferon alfa/Ribavirin Therapy THIERRY POYNARD,* MASSIMO COLOMBO, ‡ JORDI BRUIX, § EUGENE SCHIFF, RUBEN TERG, ¶ STEVEN FLAMM, # RICARDO MORENO-OTERO,** FLAIR CARRILHO, ‡‡ WARREN SCHMIDT, §§ THOMAS BERG, THOMAS MCGARRITY, ¶¶ E. JENNY HEATHCOTE, ## FERNANDO GONÇALES,*** MOISES DIAGO, ‡‡‡ ANTONIO CRAXI, §§§ MARCELO SILVA, PIERRE BEDOSSA, ¶¶¶ PABAK MUKHOPADHYAY, ### LOUIS GRIFFEL, ### MARGARET BURROUGHS, ### CLIFFORD BRASS, ### and JANICE ALBRECHT ### For The Epic Study Group *Service d’hepatologie, Université Pierre et Marie Curie Liver Center, Hôpital La Pitié Salpêtrière, Paris, France; ‡ First Division of Gastroenterology, Fondazione IRCCS Maggiore Hospital, University of Milan, Milan, Italy; § Centro de Investigación Biomédica en Red de Enfermedades Hepaticas y Digestivas, Liver Unit, Hospital Clinic, University of Barcelona, Barcelona, Spain; University of Miami School of Medicine, Miami, Florida; ¶ Hospital Municipal de Gastroenterologia Dr. Bonorino Udaondo, Capital Federal, Argentina; # Northwestern University, Chicago, Illinois; **Hospital Universitario de la Princesa and Centro de Investigación Biomédica en Red de Enfermedades Hepaticas y Digestivas (Instituto de Salud Carlos III), Madrid, Spain; ‡‡ Department of Gastroenterology, University of São Paulo School of Medicine, São Paulo, Brazil; §§ University of Iowa Hospitals and Clinics, Iowa City, Iowa; Charité, Campus Virchow Klinikum, Universitätsmedizin Berlin, Germany; ¶¶ Milton S. Hershey Medical Center, Hershey, Pennsylvania; ## University Health Network, Toronto, ON, Canada; ***Department of Medical Clinical, Faculty of Medical Sciences, University of Campinas, Campinas, Brazil; ‡‡‡ Hospital General Universitario de Valencia, Valencia, Spain; §§§ GI and Liver Unit, DIBIMIS, University of Palermo, Palermo, Italy; Hospital Universitario Austral, Pilar, Argentina; ¶¶¶ Anatomie Pathologique, Hôpital Beaujon, Clichy, France; and ### Schering–Plough Research Institute, Kenilworth, New Jersey Background & Aims: Treatment with peginterferon alfa and ribavirin produces a sustained virologic re- sponse (SVR) in approximately 60% of hepatitis C virus (HCV)-infected patients. Alternate options are needed for patients who relapse or do not respond to therapy. Methods: This prospective, international, multicenter, open-label study evaluated efficacy and safety of peginterferon alfa-2b (1.5 g/kg/wk) plus weight-based ribavirin (800 –1400 mg/day) in 2333 chronic HCV-infected patients with significant fibro- sis/cirrhosis whose previous interferon alfa/ribavirin therapy failed. Patients with undetectable HCV-RNA at treatment week (TW) 12 received 48 weeks of ther- apy; patients with detectable HCV-RNA at TW12 could enter maintenance studies at TW18; 188 pa- tients with low/detectable HCV-RNA at TW12 contin- ued therapy at the investigator’s request. Results: Overall, 22% of the patients attained SVR (56% with undetectable HCV-RNA and 12% with low/detectable HCV-RNA at TW12). SVR was better in relapsers (38%) than nonresponders (14%), regardless of previ- ous treatment, and in patients previously treated with interferon-alfa/ribavirin (25%) than peginterferon alfa-ribavirin (17%). Predictors of response in patients with undetectable HCV-RNA at TW12 were genotype (2/3 vs 1, respectively; odds ratio [OR] 2.4; P < .0001), fibrosis score (F2 vs F4; OR, 2.2; F3 vs F4; OR, 1.7; P < .0001), and baseline viral load (<600,000 vs >600,000 IU/mL; OR, 1.4; P .0223). These factors plus previous treatment and response were overall predictors of SVR. Safety was similar among fibrosis groups. Conclusions: Peginterferon alfa-2b plus weight-based ribavirin is effective and safe in patients who failed interferon alfa/ribavirin therapy. Geno- type, baseline viral load, and fibrosis stage were pre- dictors of response. T reatment of hepatitis C virus (HCV)-infected patients with pegylated interferon (PEG-IFN) alfa and ribavirin, the current standard of care, results in successful outcomes approximately 60% of the time. Patients infected with HCV genotype 2 or 3 (G2/3) are more likely to attain sustained virologic response (SVR) (70%–75%) than those infected with HCV G1 (40%– 45%). 1,2 Patients who attain SVR gen- erally do not experience progression of fibrosis and may experience regression of established fibrosis. 3–5 Survival rates are significantly higher in patients with cirrhosis who attain SVR than nonresponders in terms of liver failure and hepatocellular carcinoma. 6,7 Therefore, the primary goal of treating these patients is viral eradication. For nonre- sponders, strategies that prevent the progression of liver disease and hepatocellular carcinoma are being explored. To Abbreviations used in this paper: EPIC, Evaluation of PegIntron in Control of Hepatitis C Cirrhosis; EVR, early virologic response; HCV, hepatitis C virus; IFN, interferon; LLD, lower limit of detection; PCR, polymerase chain reaction; PEG-IFN, peginterferon; SVR, sustained virologic response; WBD, weight-based dose. © 2009 by the AGA Institute 0016-5085/09/$36.00 doi:10.1053/j.gastro.2009.01.039 CLINICAL–LIVER, PANCREAS, AND BILIARY TRACT GASTROENTEROLOGY 2009;136:1618 –1628

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CT
PW
TREPC
*MUCESHUPI
BasvntmswcstaactuOuH(oiaw(fiP>pp
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
GASTROENTEROLOGY 2009;136:1618–1628
LINICAL—LIVER, PANCREAS, AND BILIARYRACT
eginterferon alfa-2b and Ribavirin: Effective in Patients With Hepatitis Cho Failed Interferon alfa/Ribavirin Therapy
HIERRY POYNARD,* MASSIMO COLOMBO,‡ JORDI BRUIX,§ EUGENE SCHIFF,� RUBEN TERG,¶ STEVEN FLAMM,#
ICARDO MORENO-OTERO,** FLAIR CARRILHO,‡‡ WARREN SCHMIDT,§§ THOMAS BERG,� � THOMAS MCGARRITY,¶¶
. JENNY HEATHCOTE,## FERNANDO GONÇALES,*** MOISES DIAGO,‡‡‡ ANTONIO CRAXI,§§§ MARCELO SILVA,� ��
IERRE BEDOSSA,¶¶¶ PABAK MUKHOPADHYAY,### LOUIS GRIFFEL,### MARGARET BURROUGHS,###
LIFFORD BRASS,### and JANICE ALBRECHT### For The Epic Study Group
Service d’hepatologie, Université Pierre et Marie Curie Liver Center, Hôpital La Pitié Salpêtrière, Paris, France; ‡First Division of Gastroenterology, Fondazione IRCCSaggiore Hospital, University of Milan, Milan, Italy; §Centro de Investigación Biomédica en Red de Enfermedades Hepaticas y Digestivas, Liver Unit, Hospital Clinic,niversity of Barcelona, Barcelona, Spain; �University of Miami School of Medicine, Miami, Florida; ¶Hospital Municipal de Gastroenterologia Dr. Bonorino Udaondo,apital Federal, Argentina; #Northwestern University, Chicago, Illinois; **Hospital Universitario de la Princesa and Centro de Investigación Biomédica en Red denfermedades Hepaticas y Digestivas (Instituto de Salud Carlos III), Madrid, Spain; ‡‡Department of Gastroenterology, University of São Paulo School of Medicine,ão Paulo, Brazil; §§University of Iowa Hospitals and Clinics, Iowa City, Iowa; � �Charité, Campus Virchow Klinikum, Universitätsmedizin Berlin, Germany; ¶¶Milton S.ershey Medical Center, Hershey, Pennsylvania; ##University Health Network, Toronto, ON, Canada; ***Department of Medical Clinical, Faculty of Medical Sciences,niversity of Campinas, Campinas, Brazil; ‡‡‡Hospital General Universitario de Valencia, Valencia, Spain; §§§GI and Liver Unit, DIBIMIS, University of Palermo,
� �� ¶¶¶ ###
alermo, Italy; Hospital Universitario Austral, Pilar, Argentina; Anatomie Pathologique, Hôpital Beaujon, Clichy, France; and Schering–Plough Researchnstitute, Kenilworth, New Jerseygwwtd
Ttagvweerahtsd
Chpv
ackground & Aims: Treatment with peginterferonlfa and ribavirin produces a sustained virologic re-ponse (SVR) in approximately 60% of hepatitis Cirus (HCV)-infected patients. Alternate options areeeded for patients who relapse or do not respond to
herapy. Methods: This prospective, international,ulticenter, open-label study evaluated efficacy and
afety of peginterferon alfa-2b (1.5 �g/kg/wk) pluseight-based ribavirin (800 –1400 mg/day) in 2333
hronic HCV-infected patients with significant fibro-is/cirrhosis whose previous interferon alfa/ribavirinherapy failed. Patients with undetectable HCV-RNAt treatment week (TW) 12 received 48 weeks of ther-py; patients with detectable HCV-RNA at TW12ould enter maintenance studies at TW18; 188 pa-ients with low/detectable HCV-RNA at TW12 contin-ed therapy at the investigator’s request. Results:verall, 22% of the patients attained SVR (56% withndetectable HCV-RNA and 12% with low/detectableCV-RNA at TW12). SVR was better in relapsers
38%) than nonresponders (14%), regardless of previ-us treatment, and in patients previously treated with
nterferon-alfa/ribavirin (25%) than peginterferonlfa-ribavirin (17%). Predictors of response in patientsith undetectable HCV-RNA at TW12 were genotype
2/3 vs 1, respectively; odds ratio [OR] 2.4; P < .0001),brosis score (F2 vs F4; OR, 2.2; F3 vs F4; OR, 1.7;
< .0001), and baseline viral load (<600,000 vs600,000 IU/mL; OR, 1.4; P � .0223). These factors
lus previous treatment and response were overall
redictors of SVR. Safety was similar among fibrosisroups. Conclusions: Peginterferon alfa-2b pluseight-based ribavirin is effective and safe in patientsho failed interferon alfa/ribavirin therapy. Geno-
ype, baseline viral load, and fibrosis stage were pre-ictors of response.
reatment of hepatitis C virus (HCV)-infected patientswith pegylated interferon (PEG-IFN) alfa and ribavirin,
he current standard of care, results in successful outcomespproximately 60% of the time. Patients infected with HCVenotype 2 or 3 (G2/3) are more likely to attain sustainedirologic response (SVR) (70%–75%) than those infectedith HCV G1 (40%–45%).1,2 Patients who attain SVR gen-
rally do not experience progression of fibrosis and mayxperience regression of established fibrosis.3–5 Survivalates are significantly higher in patients with cirrhosis whottain SVR than nonresponders in terms of liver failure andepatocellular carcinoma.6,7 Therefore, the primary goal ofreating these patients is viral eradication. For nonre-ponders, strategies that prevent the progression of liverisease and hepatocellular carcinoma are being explored. To
Abbreviations used in this paper: EPIC, Evaluation of PegIntron inontrol of Hepatitis C Cirrhosis; EVR, early virologic response; HCV,epatitis C virus; IFN, interferon; LLD, lower limit of detection; PCR,olymerase chain reaction; PEG-IFN, peginterferon; SVR, sustainedirologic response; WBD, weight-based dose.
© 2009 by the AGA Institute0016-5085/09/$36.00
doi:10.1053/j.gastro.2009.01.039

de
CchwavprKPttea
ewwatpr
CsniraitusetawsaHvfrcspp�n
mcBhspi
dLP(�wwnmoi
iewa�11aipp
wps9t(adctCtsMdRtPp
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
May 2009 RESPONSE TO PEG-IFN alfa-2b/RBV RETREATMENT 1619
ate, these strategies may be most effective in preventingvents associated with portal hypertension.8
The Evaluation of PegIntron in Control of Hepatitis Cirrhosis (EPIC3) study—a large, prospective, multiphase
linical program—is evaluating the retreatment of chronicepatitis C patients with significant fibrosis/cirrhosis inhom previous treatment with nonpegylated or PEG-IFNlfa plus ribavirin was ineffective (ie, patients experiencedirologic nonresponse or relapse). Patients entering thisrogram were first offered retreatment with an optimalegimen of PEG-IFN alfa-2b (PegIntron, Schering–Plough,enilworth, NJ) plus weight-based dose (WBD) ribavirin.atients who did not respond to retreatment by week 12 ofherapy were offered the opportunity to participate in main-enance studies addressing the clinical and histologic ben-fits of low-dose (0.5 �g/kg/wk), long-term PEG-IFNlfa-2b treatment.
The EPIC3 program includes the largest study to date tovaluate the retreatment of chronic hepatitis C patientsith significant fibrosis or cirrhosis for whom at least 12eeks of previous therapy with nonpegylated or PEG-IFNlfa/ribavirin therapy was ineffective. This report describeshe efficacy and safety of retreatment with PEG-IFN alfa-2blus WBD ribavirin of the 2333 patients enrolled in theetreatment study.
Patients and MethodsPatient SelectionPatients 18 to 65 years of age with chronic hepatitis
and significant hepatic fibrosis/cirrhosis (METAVIRcore F2, F3, or F4) who failed combination therapy withonpegylated or PEG-IFN alfa/ribavirin therapy were el-
gible to enroll. All patients in this study previouslyeceived a minimum of 12 weeks of combination therapynd did not attain SVR. Patients were categorized accord-ng to previous response (nonresponder, relapser, orreatment failure) to combination therapy based on doc-mented HCV-RNA polymerase chain reaction (PCR) re-ults. Nonresponders had detectable HCV-RNA at thend of therapy. Relapsers had undetectable HCV-RNA athe end of treatment (EOT) and had subsequent detect-ble HCV-RNA during posttreatment follow-up. Patientsho did not meet the protocol definition for nonre-
ponder or relapser because documentation of HCV-RNAssays did not fulfill these definitions but had detectableCV-RNA more than 1 week after the end of their pre-
ious therapeutic regimen were designated as treatmentailures. These patients likely represented a mixture ofelapsers and nonresponders. Additional major inclusionriteria included HCV-RNA PCR positivity, hepatic fibro-is documented by historical biopsy showing at leastortal fibrosis with few septa (METAVIR score, F2), com-ensated liver disease (Child–Pugh class A), hemoglobin
12 g/dL for women and � 13 g/dL for men, absolute
eutrophil count � 1500/mm3, platelet count � 80,000/ Tm3, and body weight of 40 to 125 kg. Major exclusionriteria included known coinfection with HIV or hepatitis
virus, decompensated liver disease, and history ofepatocellular carcinoma. Additionally, patients werecreened for hepatocellular carcinoma by serum �-feto-rotein determination and review of available radiologic
maging.
Study Design and ConductThis prospective, open-label, clinical trial was con-
ucted at 133 sites in the United States, Canada, Europe,atin America, Taiwan, and Australia. Patients receivedEG-IFN alfa-2b 1.5 �g/kg/wk and daily WBD ribavirin
800 mg for �65 kg; 1000 mg for �65–85 kg; 1200 mg for85–105 kg, and 1400 mg for �105–125 kg) for up to 48eeks. Patients with detectable HCV-RNA at treatmenteek (TW) 12 were offered randomization into mainte-ance studies. Waivers requesting continuation of treat-ent to 48 weeks for patients with decreases in HCV-RNA
f �2 log10 at TW12 compared with baseline were given tonvestigators.
Guidelines for discontinuing, interrupting, or decreas-ng the dose of study medication because of adversevents and hematologic or biochemical abnormalitiesere prespecified in the protocol. Study drug was reducednd discontinued as follows: hemoglobin values of10 and 8.5 g/dL, absolute neutrophil counts of 0.75 �
09/L and 0.50 � 109/L, and platelet counts of �50 �09/L and �25 � 109/L, respectively. The study waspproved by the ethics committee at each participatingnstitution and was conducted according to good clinicalractice and the Declaration of Helsinki. All patientsrovided written informed consent.
AssessmentsPlasma HCV-RNA was measured at screening; at
eeks 12, 24, and 48 of treatment; and at 12 and 24 weeksosttreatment. HCV-RNA analyses (TaqMan; Applied Bio-ystems, Foster City, CA; lower limit of detection [LLD] for5% sensitivity of 125 IU/mL) were performed centrally athe Schering–Plough Research Institute (SPRI) LaboratoryKenilworth, New Jersey). Samples below the LLD for which
signal was detected were characterized as low positive oretectable; those for which no signal was detected wereharacterized as negative or undetectable. Confirmatoryesting (Quest Nichols Laboratory, San Juan Capistrano,A) using TaqMan was performed on a subset of samples
ested at the SPRI Laboratory. Pretreatment liver biopsypecimens were scored by a single pathologist (P. B.) using
ETAVIR criteria.10 Early virologic response (EVR) wasefined as HCV-RNA below the LLD (125 IU/mL) at TW12.elapse rates were calculated based on patients with unde-
ectable HCV-RNA at EOT, and available 24-week follow-upCR results were calculated based on the percentage ofatients who had detectable HCV-RNA during follow-up.
he primary efficacy end point was SVR, defined as unde-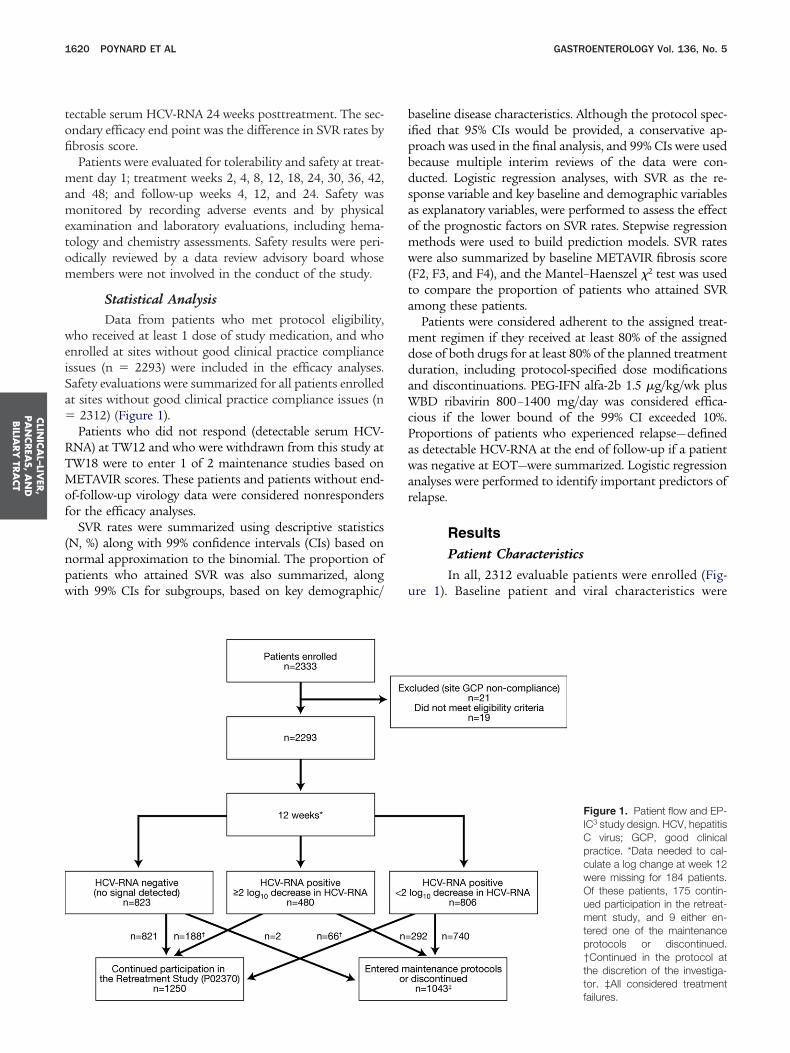
tofi
mametom
weiSa�
RTMof
(npw
bipbdsaomw(ta
mddaWcPawar
u
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1620 POYNARD ET AL GASTROENTEROLOGY Vol. 136, No. 5
ectable serum HCV-RNA 24 weeks posttreatment. The sec-ndary efficacy end point was the difference in SVR rates bybrosis score.Patients were evaluated for tolerability and safety at treat-ent day 1; treatment weeks 2, 4, 8, 12, 18, 24, 30, 36, 42,
nd 48; and follow-up weeks 4, 12, and 24. Safety wasonitored by recording adverse events and by physical
xamination and laboratory evaluations, including hema-ology and chemistry assessments. Safety results were peri-dically reviewed by a data review advisory board whoseembers were not involved in the conduct of the study.
Statistical AnalysisData from patients who met protocol eligibility,
ho received at least 1 dose of study medication, and whonrolled at sites without good clinical practice compliancessues (n � 2293) were included in the efficacy analyses.afety evaluations were summarized for all patients enrolledt sites without good clinical practice compliance issues (n
2312) (Figure 1).Patients who did not respond (detectable serum HCV-
NA) at TW12 and who were withdrawn from this study atW18 were to enter 1 of 2 maintenance studies based onETAVIR scores. These patients and patients without end-
f-follow-up virology data were considered nonrespondersor the efficacy analyses.
SVR rates were summarized using descriptive statisticsN, %) along with 99% confidence intervals (CIs) based onormal approximation to the binomial. The proportion ofatients who attained SVR was also summarized, alongith 99% CIs for subgroups, based on key demographic/
aseline disease characteristics. Although the protocol spec-fied that 95% CIs would be provided, a conservative ap-roach was used in the final analysis, and 99% CIs were usedecause multiple interim reviews of the data were con-ucted. Logistic regression analyses, with SVR as the re-ponse variable and key baseline and demographic variabless explanatory variables, were performed to assess the effectf the prognostic factors on SVR rates. Stepwise regressionethods were used to build prediction models. SVR ratesere also summarized by baseline METAVIR fibrosis score
F2, F3, and F4), and the Mantel–Haenszel �2 test was usedo compare the proportion of patients who attained SVRmong these patients.
Patients were considered adherent to the assigned treat-ent regimen if they received at least 80% of the assigned
ose of both drugs for at least 80% of the planned treatmenturation, including protocol-specified dose modificationsnd discontinuations. PEG-IFN alfa-2b 1.5 �g/kg/wk plusBD ribavirin 800–1400 mg/day was considered effica-
ious if the lower bound of the 99% CI exceeded 10%.roportions of patients who experienced relapse—defineds detectable HCV-RNA at the end of follow-up if a patientas negative at EOT—were summarized. Logistic regressionnalyses were performed to identify important predictors ofelapse.
ResultsPatient CharacteristicsIn all, 2312 evaluable patients were enrolled (Fig-
re 1). Baseline patient and viral characteristics were
Figure 1. Patient flow and EP-IC3 study design. HCV, hepatitisC virus; GCP, good clinicalpractice. *Data needed to cal-culate a log change at week 12were missing for 184 patients.Of these patients, 175 contin-ued participation in the retreat-ment study, and 9 either en-tered one of the maintenanceprotocols or discontinued.†Continued in the protocol atthe discretion of the investiga-tor. ‡All considered treatment
failures.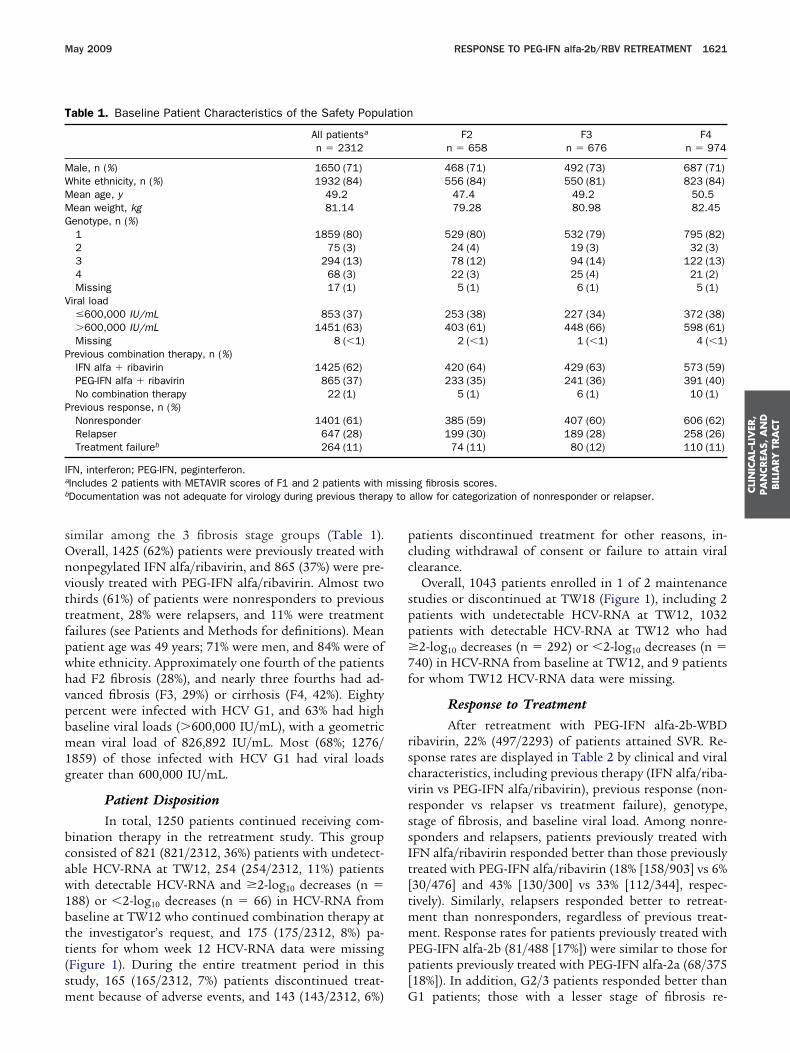
sOnvttfpwhvpbm1g
bcaw1btt(sm
pcc
spp�7f
rscvrssIt[tmmPp[
T
MWMMG
V
P
P
Ia
b y to
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
May 2009 RESPONSE TO PEG-IFN alfa-2b/RBV RETREATMENT 1621
imilar among the 3 fibrosis stage groups (Table 1).verall, 1425 (62%) patients were previously treated withonpegylated IFN alfa/ribavirin, and 865 (37%) were pre-iously treated with PEG-IFN alfa/ribavirin. Almost twohirds (61%) of patients were nonresponders to previousreatment, 28% were relapsers, and 11% were treatmentailures (see Patients and Methods for definitions). Meanatient age was 49 years; 71% were men, and 84% were ofhite ethnicity. Approximately one fourth of the patientsad F2 fibrosis (28%), and nearly three fourths had ad-anced fibrosis (F3, 29%) or cirrhosis (F4, 42%). Eightyercent were infected with HCV G1, and 63% had highaseline viral loads (�600,000 IU/mL), with a geometricean viral load of 826,892 IU/mL. Most (68%; 1276/
859) of those infected with HCV G1 had viral loadsreater than 600,000 IU/mL.
Patient DispositionIn total, 1250 patients continued receiving com-
ination therapy in the retreatment study. This grouponsisted of 821 (821/2312, 36%) patients with undetect-ble HCV-RNA at TW12, 254 (254/2312, 11%) patientsith detectable HCV-RNA and �2-log10 decreases (n �88) or �2-log10 decreases (n � 66) in HCV-RNA fromaseline at TW12 who continued combination therapy athe investigator’s request, and 175 (175/2312, 8%) pa-ients for whom week 12 HCV-RNA data were missingFigure 1). During the entire treatment period in thistudy, 165 (165/2312, 7%) patients discontinued treat-
able 1. Baseline Patient Characteristics of the Safety Popul
All patientsa
n � 2312
ale, n (%) 1650 (71)hite ethnicity, n (%) 1932 (84)ean age, y 49.2ean weight, kg 81.14enotype, n (%)1 1859 (80)2 75 (3)3 294 (13)4 68 (3)Missing 17 (1)
iral load�600,000 IU/mL 853 (37)�600,000 IU/mL 1451 (63)Missing 8 (�1)
revious combination therapy, n (%)IFN alfa � ribavirin 1425 (62)PEG-IFN alfa � ribavirin 865 (37)No combination therapy 22 (1)
revious response, n (%)Nonresponder 1401 (61)Relapser 647 (28)Treatment failureb 264 (11)
FN, interferon; PEG-IFN, peginterferon.Includes 2 patients with METAVIR scores of F1 and 2 patients withDocumentation was not adequate for virology during previous therap
ent because of adverse events, and 143 (143/2312, 6%) G
atients discontinued treatment for other reasons, in-luding withdrawal of consent or failure to attain virallearance.
Overall, 1043 patients enrolled in 1 of 2 maintenancetudies or discontinued at TW18 (Figure 1), including 2atients with undetectable HCV-RNA at TW12, 1032atients with detectable HCV-RNA at TW12 who had2-log10 decreases (n � 292) or �2-log10 decreases (n �
40) in HCV-RNA from baseline at TW12, and 9 patientsor whom TW12 HCV-RNA data were missing.
Response to TreatmentAfter retreatment with PEG-IFN alfa-2b-WBD
ibavirin, 22% (497/2293) of patients attained SVR. Re-ponse rates are displayed in Table 2 by clinical and viralharacteristics, including previous therapy (IFN alfa/riba-irin vs PEG-IFN alfa/ribavirin), previous response (non-esponder vs relapser vs treatment failure), genotype,tage of fibrosis, and baseline viral load. Among nonre-ponders and relapsers, patients previously treated withFN alfa/ribavirin responded better than those previouslyreated with PEG-IFN alfa/ribavirin (18% [158/903] vs 6%30/476] and 43% [130/300] vs 33% [112/344], respec-ively). Similarly, relapsers responded better to retreat-
ent than nonresponders, regardless of previous treat-ent. Response rates for patients previously treated with
EG-IFN alfa-2b (81/488 [17%]) were similar to those foratients previously treated with PEG-IFN alfa-2a (68/375
18%]). In addition, G2/3 patients responded better than
F2n � 658
F3n � 676
F4n � 974
468 (71) 492 (73) 687 (71)556 (84) 550 (81) 823 (84)
47.4 49.2 50.579.28 80.98 82.45
529 (80) 532 (79) 795 (82)24 (4) 19 (3) 32 (3)78 (12) 94 (14) 122 (13)22 (3) 25 (4) 21 (2)
5 (1) 6 (1) 5 (1)
253 (38) 227 (34) 372 (38)403 (61) 448 (66) 598 (61)
2 (�1) 1 (�1) 4 (�1)
420 (64) 429 (63) 573 (59)233 (35) 241 (36) 391 (40)
5 (1) 6 (1) 10 (1)
385 (59) 407 (60) 606 (62)199 (30) 189 (28) 258 (26)74 (11) 80 (12) 110 (11)
ing fibrosis scores.allow for categorization of nonresponder or relapser.
ation
miss
1 patients; those with a lesser stage of fibrosis re-

salvrssbGI(I
riqG(c43apr
sPPrro
glswcmwM1IlPsfi
T
OP
N
T
G
G
B
NCa
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1622 POYNARD ET AL GASTROENTEROLOGY Vol. 136, No. 5
ponded better than those with a greater stage of fibrosis;nd those with a low (�600,000 IU/mL) baseline viraload responded better than those with a high baselineiral load (Table 2). No significant differences in responseates were observed in patients with no or little (0%–5%)teatosis (23% SVR; 306/1331) and patients with �30%teatosis (20% SVR; 91/466). A combination of factorsest predicted response; for example, 67% (954/81) of2/3 patients who experienced relapse after previous
FN/ribavirin treatment attained SVR, whereas only 4%19/431) of G1 patients who were nonresponders to PEG-FN alfa/ribavirin attained SVR.
Although the EOT response was 39% (891/2293), theelapse rate (43% [374/865]) was high. However, patientsnfected with HCV G1 experienced relapse more fre-uently (53% [297/563]) than patients infected with HCV2 (17% [9/53]), G3 (27% [57/214]), or G4 (32% [9/28])
Table 3). Additionally, patients with advanced fibrosis orirrhosis had higher relapse rates (F4, 53% [176/335]; F3,1% [103/249]) than those with moderate fibrosis (F2,4% [95/281]) (Table 3). Based on multivariate regressionnalysis using a backward selection method, significantredictors of relapse were genotype (G2/3 vs G1; odds
able 2. Sustained Virologic Response Rates Based on Prev
Total population
SVR, % (n/N) 99% CI
verall 22 (497/2293) 20–24revious responseRelapser 38 (243/645) 33–43G1 27 (123/452) 22–33G2/3 61 (106/173) 52–71
onresponder 14 (188/1385) 11–16G1 10 (117/1198) 8–12G2/3 46 (63/137) 35–57
reatment failure 25 (66/263) 18–32G1 15 (30/196) 9–22G2/3 60 (34/57) 43–76
enotype1 15 (270/1846) 13–172 59 (44/75) 44–733 55 (159/292) 47–624 28 (19/67) 14–43
enotype and METAVIR scoreG1 F2 21 (110/525) 16–26G1 F3 16 (82/529) 11–20G1 F4 10 (78/790) 7–13G2/3 F2 68 (69/102) 56–80G2/3 F3 55 (61/112) 42–67G2/3 F4 48 (73/153) 37–58
aseline viral load, IU/mLHVL (�600,000) 17 (239/1441) 14–19LVL (�600,00) 30 (256/848) 26–34
OTE. Data not available for all subjects for all data points. Sum ofI, confidence interval; G, genotype; HVL, high viral load; LVL, low virInsufficient patient numbers for accurate determination.
atio [OR], 0.295; P � .0001), baseline METAVIR fibrosis a
core (F2 vs F4; OR, 0.407; P � .0001; F3 vs F4; OR, 0.588;� .0030), and baseline viral load (OR, 0.681; P � .0112).atients with multiple predictors of relapse had low SVRates. G1 patients with cirrhosis had an EOT responseate of 28% and a relapse rate of 64%, resulting in an SVRf only 10%.
Predictors of ResponseUnivariate logistical regression analyses identified
enotype, baseline METAVIR fibrosis score, baseline viraload, previous therapy regimen, previous response, region,ex, and age as significant predictors of SVR. In the step-ise multivariate regression analysis, significant patient
haracteristics that were predictors of response after adjust-ent for the factors identified by the univariate analysesere genotype (G2/3 vs G1; OR, 4.9; P � .0001), baselineETAVIR fibrosis score (F2 vs F4; OR, 2.2; F3 vs F4; OR,
.4; P � .0001), baseline viral load (�600,000 vs �600,000U/mL; OR, 1.9; P � .0001), previous treatment (nonpegy-ated IFN alfa/ribavirin vs PEG-IFN alfa/ribavirin: OR, 2.0;
� .0001), and previous response (relapser vs nonre-ponder: OR, 3.8; P � .0001). A graded decrease in SVR asbrosis score increased from F2 to F3 to F4 was observed,
Therapy
Previous therapy
IFN alfa/ribavirin PEG-IFN alfa/ribavirin
SVR, % (n/N) 99% CI SVR, % (n/N) 99% CI
25 (348/1423) 22–27 17 (149/863) 14–21
43 (130/300) 36–51 33 (113/344) 26–3932 (67/208) 24–41 23 (56/243) 16–3067 (54/81) 53–80 57 (52/92) 43–7018 (158/903) 14–21 6 (30/476) 3–913 (98/761) 10–16 4 (19/431) 2–749 (53/109) 36–61 36 (10/28) NAa
27 (60/220) 20–35 14 (6/43) 0–2816 (27/166) 9–24 10 (3/30) 0–2464 (32/50) 47–82 29 (2/7) NAa
17 (192/1135) 14–20 11 (78/704) 8–1458 (28/48) 40–77 59 (16/27) 35–8458 (111/192) 49–67 48 (48/100) 35–6133 (13/40) 13–52 22 (6/27) 2–43
24 (79/328) 18–30 16 (31/196) 9–2319 (63/339) 13–24 10 (19/188) 4–1611 (50/466) 7–14 9 (28/320) 5–1373 (53/73) 59–86 55 (16/29) 31–7954 (39/72) 39–69 55 (22/40) 35–7550 (47/95) 36–63 45 (26/58) 28–62
20 (170/864) 16–23 12 (69/573) 9–1632 (178/557) 27–37 27 (78/288) 20–34
oups may not equal “total population.”d; SVR, sustained virologic response.
ious
subgral loa
nd the differences were significant (P � .0001; Figure 2).

Table 3. Response and Relapse Rates Based on Hepatitis C Virus RNA Status at Treatment Week 12
Patients with undetectablea
HCV-RNA at TW12, % (n/N)SVR of patients with undetectablea
HCV-RNA at TW12, % (n/N) 99% CI
SVR of patients with detectableHCV-RNA but �2-log10
decrease at TW12, % (n/N) 99% CI
Relapse of patients withundetectablea HCV-RNA
at TW12, % (n/N) 99% CI
Overall populationb 36 (823/2293) 56 (463/823) 52–61 12 (23/188) 6–18 38 (275/732) 33–42G1
All 28 (507/1846) 48 (245/507) 43–54 12 (20/171) 5–18 46 (201/442) 39–52HVL 24 (306/1267) 44 (135/306) 37–51 10 (12/126) 3–16 51 (134/265) 43–59LVL 35 (201/577) 55 (110/201) 46–64 18 (8/45) 3–33 38 (67/177) 29–47
G2/3All 77 (281/367) 70 (196/281) 63–77 14 (2/14) NAc 25 (65/259) 18–32HVL 75 (122/163) 68 (83/122) 57–79 14 (1/7) NAc 25 (28/111) 15–36LVL 78 (157/202) 71 (111/157) 61–80 14 (1/7) NAc 25 (37/146) 16–35
F2All 42 (271/653) 64 (174/271) 57–72 20 (10/50) 5–35 31 (76/245) 23–39G1 33 (174/525) 55 (95/174) 45–64 22 (10/46) 6–37 40 (62/154) 30–50G2/3 80 (82/102) 83 (68/82) 72–94 0 (0/4) NAc 14 (11/77) 4–25
F3All 36 (242/672) 59 (142/242) 51–67 9 (4/46) 0–19 35 (75/216) 26–43G1 28 (150/529) 53 (79/150) 42–63 8 (3/40) 0–18 41 (53/131) 29–52G2/3 76 (85/112) 71 (60/85) 58–83 0 (0/3) NAc 24 (19/79) 12–36
F4All 32 (309/966) 48 (147/309) 40–55 10 (9/92) 2–18 46 (124/271) 38–54G1 23 (182/790) 39 (71/182) 30–48 8 (7/85) 1–16 55 (86/157) 45–65G2/3 75 (114/153) 60 (68/114) 48–72 29 (2/7) NAc 34 (35/103) 22–46
HVLAll 30 (432/1441) 51 (220/432) 45–57 10 (13/134) 3–16 43 (163/379) 37–50F2 34 (135/400) 57 (77/135) 46–68 13 (5/40) 0–26 40 (49/123) 29–51F3 32 (142/445) 55 (78/142) 44–66 9 (3/33) 0–22 38 (48/125) 27–50F4 26 (155/595) 42 (65/155) 32–52 8 (5/61) 0–17 50 (66/131) 39–62
LVLAll 46 (389/848) 62 (241/389) 56–68 19 (10/54) 5–32 32 (112/351) 26–38F2 54 (135/252) 71 (96/135) 61–81 50 (5/10) NAc 22 (27/121) 13–32F3 44 (100/226) 64 (64/100) 52–76 8 (1/13) NAc 30 (27/91) 17–42F4 41 (153/369) 53 (81/153) 43–63 13 (4/31) 0–28 42 (58/139) 31–53
HCV, hepatitis C virus; SVR, sustained virologic response; G, genotype.aUndetectable, no HCV-RNA or signal below the LLD of the assay. To be conservative for the purposes of analysis, any sample that was below the LLD but for which a signal was detected wasconsidered detectable, or positive.bMissing data for 184 patients. Positive �2-log10 decrease at treatment week 12, n � 457,* 0% SVR. *Only 118 of these 457 patients continued in the retreatment study past treatment week22.cInsufficient patient numbers for accurate determination.
CLINICAL–LIVER,PANCREAS, ANDBILIARY TRACT
May
20
09
RES
PO
NS
ETO
PEG
-IFNalfa-2
b/RB
VR
ETREA
TMEN
T1
62
3

fRdsfvp
IuIwRoRh1tmH
asitilpgtSaOvvPvd
1
ceoatfaotaro6[�d9
owf(((e(pi
wmettiwTdste5[caoma
ri[
Fa1.ft
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1624 POYNARD ET AL GASTROENTEROLOGY Vol. 136, No. 5
Of the 342 patients who experienced relapse based onollow-up week 24 virology, 332 had detectable HCV-NA by follow-up week 12. This 97% concurrence rateemonstrated that virologic relapse occurred early anduggested that follow-up week 12 closely approximatesollow-up week 24 in assessment of the durability ofirologic response in a population for whom therapy hadreviously failed.
Response to treatment based on TW12 response.n total, 56% (463/823; 99% CI: 52– 61) of patients withndetectable HCV-RNA at TW12 attained SVR (Table 3).
n contrast, only 12% (23/188; 99% CI: 6 –18) of patientshose viral load decreased by 2 log10 but whose HCV-NA remained detectable attained SVR (Table 3). Mostf these patients (21/23) also had undetectable HCV-NA at TW24. At TW12, 65% (15/23) of these patientsad low positive (�125 IU/mL) HCV viral loads, and00% (23/23) had HCV viral loads of �750 IU/mL. Twenty-hree percent (15/65) of patients with low positive vire-
ia at TW12 attained SVR. No patient whose TW12CV-RNA was �750 IU/mL attained SVR.
Predictors of response in patients with undetect-ble HCV-RNA at TW12. The demographic factors con-idered (at a leave-in, leave-out significance level of .05)ncluded age, previous response to treatment, sex, geno-ype, previous therapy (pegylated interferon vs “standard”nterferon), fibrosis stage, geographic region, and base-ine viral load. Univariate logistical regression analysis ofatients with undetectable HCV-RNA at TW12 identifiedenotype, baseline METAVIR fibrosis score, previousherapeutic regimen, and age as significant predictors ofVR. However, in the stepwise multivariate regressionnalysis, only genotype (G2/3 vs G1; OR, 2.4; G4 vs G1;R, 1.4; P � .0001), baseline METAVIR fibrosis score (F2
s F4; OR, 2.2; F3 vs F4; OR, 1.7, P � .0001), and baselineiral load (�600,000 IU/mL vs �600,000 IU/mL; OR, 1.4;� .0223) remained significant predictors of SVR. Pre-
ious therapy and previous response were no longer pre-ictors of response at TW12.
Adherence to treatment. Most patients (76%;
igure 2. Sustained virologic response rates by METAVIR score over-ll and among patients with undetectable HCV-RNA at treatment week2. SVR, sustained virologic response. aData missing for 2 patients; P �0001 to each other based on Mantel–Haenszel �2 test. bData missingor 1 patient; P � .0004 to each other based on Mantel–Haenszel �2
est conducted on the group that was negative at treatment week 12.
746/2293) were adherent to study drug over the full F
ourse of the study; 92% (2121/2293) were �80% adher-nt to their assigned ribavirin dose in the first 12 weeksf therapy. Of these, 97% (2056/2121) were also compli-nt with their assigned PEG-IFN alfa-2b dose. Adherenceo therapy during the treatment period was importantor attaining SVR; 24.5% (428/1746) of patients who weredherent to study drugs attained SVR compared withnly 3.4% (12/349) of nonadherent patients. Adherenceo ribavirin in the first 12 weeks also was important inttaining SVR; patients who received at least 80% of theiribavirin dose in the first 12 weeks attained similar ratesf SVR regardless of PEG-IFN alfa-2b compliance (0%–0%, 40% [2/5]; 60% to �80%, 32% [19/60]; �80%, 38%780/2056]). Additionally, among patients who received
80% of their assigned ribavirin dose, SVR was depen-ent on PEG-IFN alfa-2b compliance (0%– 60%, 1% [1/4]; 60% to �80%, 10% [3/30]; �80%, 38% [18/48]).
SafetyAdverse events were consistent with those previ-
usly reported for PEG-IFN alfa/ribavirin therapy1,2 andere reported by 97% of patients (Table 4). The most
requently reported adverse events included headache41%), fever (39%), fatigue (33%), myalgia (31%), nausea25%), insomnia (22%), influenza-like illness (21%), chills22%), and neutropenia (20%); most were mild or mod-rate in severity. The incidence of depression in this study12%) was lower than that reported in previous trials,robably because patients who developed depression dur-
ng their previous course were less likely to be retreated.As expected, hematologic adverse events associated
ith PEG-IFN alfa-2b plus ribavirin therapy were com-on in this study. The frequency of hematologic adverse
vents including thrombocytopenia was higher in pa-ients with cirrhosis than in F2 or F3 patients because ofhe lower initial platelet counts, not the greater decreasesn platelets with therapy. F4 patients entered the studyith lower baseline platelet levels than F2 or F3 patients.he decrease in platelet counts, expressed as a percentageecrease from baseline, was approximately 30% and wasimilar across fibrosis groups. The frequency of grade 3hrombocytopenia (25,000 – 49,000 cells/mm3) was high-st in F4 patients (F4, 70/974 [7%]; F3, 11/676 [2%]; F2,/658 [1%]). Three patients (F4, 1/974 [�1%]; F3, 1/676�1%]; F2, 1/658 [�1%]) experienced grade 4 thrombo-ytopenia (�25,000 cells/mm3). Bleeding events associ-ted with thrombocytopenia occurred in 19 patients, 17f whom had F4 fibrosis. All adverse events were mild oroderate except for a single occurrence of hematemesis
ssociated with a Mallory–Weiss tear.As expected, patients without cirrhosis had a very low
ate of clinical manifestations of end-stage liver disease,ncluding esophageal varices (F4, 55/974 [6%]; F3, 2/676�1%]; F2, 0/658 [0%]), splenomegaly (F4, 34/974 [3%];
3, 7/676 [1%]; F2, 2/658 [�1%]), portal hypertensive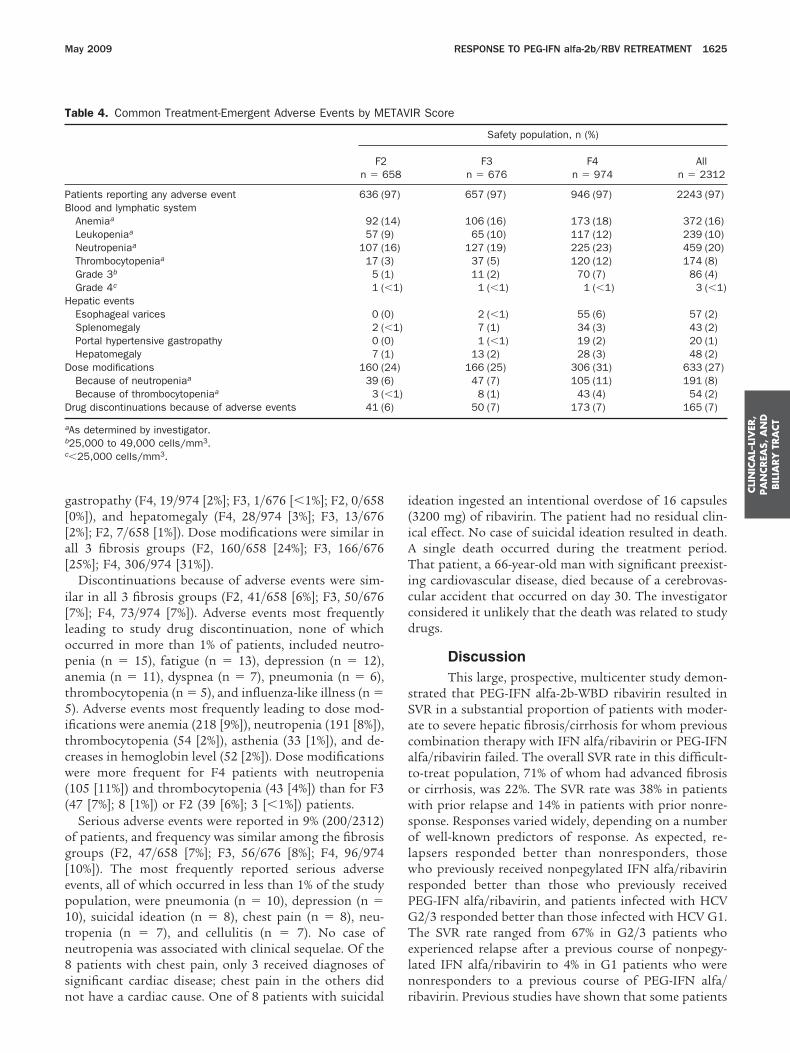
g[[a[
i[lopat5itcw((
og[ep1tn8sn
i(iATiccd
sSacatowsolwrPGTeln
T
PB
H
D
D
a
b
c
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
May 2009 RESPONSE TO PEG-IFN alfa-2b/RBV RETREATMENT 1625
astropathy (F4, 19/974 [2%]; F3, 1/676 [�1%]; F2, 0/6580%]), and hepatomegaly (F4, 28/974 [3%]; F3, 13/6762%]; F2, 7/658 [1%]). Dose modifications were similar inll 3 fibrosis groups (F2, 160/658 [24%]; F3, 166/67625%]; F4, 306/974 [31%]).
Discontinuations because of adverse events were sim-lar in all 3 fibrosis groups (F2, 41/658 [6%]; F3, 50/6767%]; F4, 73/974 [7%]). Adverse events most frequentlyeading to study drug discontinuation, none of whichccurred in more than 1% of patients, included neutro-enia (n � 15), fatigue (n � 13), depression (n � 12),nemia (n � 11), dyspnea (n � 7), pneumonia (n � 6),hrombocytopenia (n � 5), and influenza-like illness (n �). Adverse events most frequently leading to dose mod-
fications were anemia (218 [9%]), neutropenia (191 [8%]),hrombocytopenia (54 [2%]), asthenia (33 [1%]), and de-reases in hemoglobin level (52 [2%]). Dose modificationsere more frequent for F4 patients with neutropenia
105 [11%]) and thrombocytopenia (43 [4%]) than for F347 [7%]; 8 [1%]) or F2 (39 [6%]; 3 [�1%]) patients.
Serious adverse events were reported in 9% (200/2312)f patients, and frequency was similar among the fibrosisroups (F2, 47/658 [7%]; F3, 56/676 [8%]; F4, 96/97410%]). The most frequently reported serious adversevents, all of which occurred in less than 1% of the studyopulation, were pneumonia (n � 10), depression (n �0), suicidal ideation (n � 8), chest pain (n � 8), neu-ropenia (n � 7), and cellulitis (n � 7). No case ofeutropenia was associated with clinical sequelae. Of thepatients with chest pain, only 3 received diagnoses of
ignificant cardiac disease; chest pain in the others did
able 4. Common Treatment-Emergent Adverse Events by ME
F2n � 6
atients reporting any adverse event 636 (9lood and lymphatic systemAnemiaa 92 (1Leukopeniaa 57 (9Neutropeniaa 107 (1Thrombocytopeniaa 17 (3Grade 3b 5 (1Grade 4c 1 (�
epatic eventsEsophageal varices 0 (0Splenomegaly 2 (�Portal hypertensive gastropathy 0 (0Hepatomegaly 7 (1
ose modifications 160 (2Because of neutropeniaa 39 (6Because of thrombocytopeniaa 3 (�
rug discontinuations because of adverse events 41 (6
As determined by investigator.25,000 to 49,000 cells/mm3.�25,000 cells/mm3.
ot have a cardiac cause. One of 8 patients with suicidal r
deation ingested an intentional overdose of 16 capsules3200 mg) of ribavirin. The patient had no residual clin-cal effect. No case of suicidal ideation resulted in death.
single death occurred during the treatment period.hat patient, a 66-year-old man with significant preexist-
ng cardiovascular disease, died because of a cerebrovas-ular accident that occurred on day 30. The investigatoronsidered it unlikely that the death was related to studyrugs.
DiscussionThis large, prospective, multicenter study demon-
trated that PEG-IFN alfa-2b-WBD ribavirin resulted inVR in a substantial proportion of patients with moder-te to severe hepatic fibrosis/cirrhosis for whom previousombination therapy with IFN alfa/ribavirin or PEG-IFNlfa/ribavirin failed. The overall SVR rate in this difficult-o-treat population, 71% of whom had advanced fibrosisr cirrhosis, was 22%. The SVR rate was 38% in patientsith prior relapse and 14% in patients with prior nonre-
ponse. Responses varied widely, depending on a numberf well-known predictors of response. As expected, re-
apsers responded better than nonresponders, thoseho previously received nonpegylated IFN alfa/ribavirin
esponded better than those who previously receivedEG-IFN alfa/ribavirin, and patients infected with HCV2/3 responded better than those infected with HCV G1.he SVR rate ranged from 67% in G2/3 patients whoxperienced relapse after a previous course of nonpegy-ated IFN alfa/ribavirin to 4% in G1 patients who wereonresponders to a previous course of PEG-IFN alfa/
IR Score
Safety population, n (%)
F3n � 676
F4n � 974
Alln � 2312
657 (97) 946 (97) 2243 (97)
106 (16) 173 (18) 372 (16)65 (10) 117 (12) 239 (10)
127 (19) 225 (23) 459 (20)37 (5) 120 (12) 174 (8)11 (2) 70 (7) 86 (4)
1 (�1) 1 (�1) 3 (�1)
2 (�1) 55 (6) 57 (2)7 (1) 34 (3) 43 (2)1 (�1) 19 (2) 20 (1)
13 (2) 28 (3) 48 (2)166 (25) 306 (31) 633 (27)47 (7) 105 (11) 191 (8)8 (1) 43 (4) 54 (2)
50 (7) 173 (7) 165 (7)
TAV
58
7)
4))6)))1)
)1)))4))1))
ibavirin. Previous studies have shown that some patients

wwInpgrtr
oeuetiws2rvIrTwlwrsrtmtsspaoerrnr
wwPpSTprreTs
wbPllrmntapEvs
urp3ssae7p
MsocfiiFratrwpttatpnw
tffitbItw
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1626 POYNARD ET AL GASTROENTEROLOGY Vol. 136, No. 5
ho are nonresponsive to nonpegylated IFN alfa with orithout ribavirin can be successfully retreated with PEG-
FN alfa/ribavirin; SVR rates ranged from 4% to 20% inonresponders to 50% or more in relapsers.9 –19 In theresent study, in which previous treatment was nonpe-ylated IFN alfa/ribavirin or PEG-IFN alfa/ribavirin, SVRates were comparable with or better than the rates inhese studies, despite the inclusion of PEG-IFN alfa/ibavirin treatment failures.
Although several studies have evaluated retreatmentf patients for whom IFN alfa treatment failed, carefulvaluation of these studies reveals a heterogeneous pop-lation, including various permutations of those whoxperienced relapse or who did not respond to mono-herapy or combination therapy. Some of these studiesnvolved patients who received combination therapy andere comparable to patients enrolled in the current
tudy.11–21 Sherman et al13 reported overall SVR rates of3% for previous nonresponders and 41% for previouselapsers to nonpegylated IFN alfa with or without riba-irin; for those who had previously received nonpegylatedFN/ribavirin (n � 244), SVR rates were 22% and 38%,espectively. In the Hepatitis C Antiviral Long-termreatment Against Cirrhosis (HALT-C) study,21 patientsith bridging fibrosis or cirrhosis for whom nonpegy-
ated IFN alfa with or without ribavirin previously failedere retreated with standard doses of PEG-IFN alfa-2a/
ibavirin. The overall SVR rate was 18% in the HALT-Ctudy. Within that study, the population who previouslyeceived nonpegylated IFN with ribavirin (n � 385) at-ained an SVR rate of 12%.21 Although it is difficult to
ake cross-study comparisons, when considering onlyhose EPIC3 patients with similar fibrosis stages (cirrho-is or bridging fibrosis), the SVR rate was 17%. Smallertudies evaluated PEG-IFN alfa/ribavirin retreatment ofatients for whom nonpegylated IFN alfa/ribavirin ther-py failed. Taliani et al16 and Basso et al17 reportedverall SVR rates of 20% and 41%, respectively, in relaps-rs and nonresponders to nonpegylated IFN alfa/ribavi-in. Parise et al12 reported SVR rates of 51% and 26%,espectively, in a study (n � 134) in which relapsers andonresponders to nonpegylated IFN alfa/ribavirin wereetreated with PEG-IFN alfa-2a/ribavirin.
In this retreatment study, HCV-RNA status at TW12as an important predictor of SVR; 56% of patientsith undetectable HCV-RNA at TW12 attained SVR.atients with �2-log10 decreases in viral load with lowositive HCV-RNA (�125 IU/mL) at TW12 attainedVR rates of 23% but had viral loads � 750 IU/mL.hese data establish a simple and effective decisionoint at TW12 for retreatment with PEG-IFN alfa-2b/ibavirin of patients who previously failed IFN alfa/ibavirin treatment. After considering patient and dis-ase factors, patients with HCV-RNA below the LLD atW12—those with negative or near negative results—
hould continue therapy (�50% chance of SVR), p
hereas others can be spared further drug exposureecause the likelihood of attaining an SVR is low.atients whose disease characteristics suggest a high
ikelihood of relapse (Table 3) may be candidates foronger durations of therapy. Whether TW4 and TW8esults could further refine this paradigm is undeter-
ined; this study was designed before 2002 and didot assess HCV-RNA levels at these time points. As inhe present study, Moucari et al22 found that EVR wasn important predictor of SVR in patients for whomrevious treatment failed; 49% of those who attainedVR attained SVR. In contrast, the negative predictivealue of the absence of EVR was 97% (66/68) in thattudy.
Despite the high response rate among patients withndetectable HCV-RNA at TW12 in the present study,elapse rates were also high, ranging from 64% in G1atients with cirrhosis to 14% in G2/3 F2 patients (Table). However, relapse was associated with advanced fibro-is and G1 infection, and one can speculate that exten-ion of therapy might have led to greater SVR ratesmong these patients. Several studies suggest that thextension of PEG-IFN alfa/ribavirin therapy from 48 to2 weeks is beneficial in a subset of treatment-naive G1atients who are slow to respond to therapy.23–27
As with treatment-naive patients, genotype, baselineETAVIR fibrosis score, and baseline viral load were
trong predictors of SVR in the present study. Althoughther studies2,3,13 have shown that significant fibrosis andirrhosis are negative predictors of SVR, the EPIC3 is therst large study to clearly demonstrate a graded decrease
n SVR rates as fibrosis score progresses from F2 to F3 to4. Previous treatment regimen and previous treatmentesponse also predicted SVR. As reported by Jacobson etl,28 weight-based ribavirin dosing might have abrogatedhe untoward effects of body mass index and weight onesponse rates. In the present study, adherence to therapyas high and was important for attaining SVR. Foratients with undetectable HCV-RNA at TW12, however,he only baseline patient characteristics that were predic-ors in the multivariate analysis were viral load, genotype,nd stage of fibrosis. These data demonstrate that unde-ectable HCV viral load at TW12 best defines an EVR thatredicts SVR among patients for whom previous combi-ation therapy with any IFN alfa/ribavirin failed andere retreated with PEG-IFN alfa-2b/ribavirin.Based on protocol-specified inclusion criteria, the pa-
ients in this study had at least 1 potential contributingactor (significant fibrosis/cirrhosis) to a poor safety pro-le and at least 1 potential contributing factor (previousreatment experience with any IFN alfa/ribavirin) to aetter safety profile. However, the safety profile of PEG-FN alfa-2b/WBD ribavirin in this population was similaro that previously observed.2,28 Overall, safety was notorse for patients with cirrhosis; fibrosis stage did not
redict rates of discontinuation, dose modifications, or
ad2cPibeosTtpfituidc
pvphtIopatttirwbbrbilhtbttmmpw
aG1
1
1
1
1
1
1
1
1
1
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
May 2009 RESPONSE TO PEG-IFN alfa-2b/RBV RETREATMENT 1627
dverse events, including serious adverse events. Theseata confirm the general observation that PEG-IFN alfa-b/ribavirin therapy is well tolerated in patients withompensated cirrhosis caused by chronic hepatitis C.atients with cirrhosis were more likely to require mod-
fied doses due to thrombocytopenia because of loweraseline platelet counts than F2 or F3 patients at studyntry. All 3 fibrosis stage groups had an approximatene-third reduction in platelet count, regardless of fibro-is score (F2, 30%; F3, 30%; F4 33% [data not shown]).hese data validate the widespread perception that pa-
ients with cirrhosis have lower (numeric) reductions inlatelet counts with IFN alfa-based therapies while de-ning the greater risk for these patients to acquirehrombocytopenia because of lower baseline platelet val-es. Although experiencing equal percentage reductions
n platelet count, these patients experience lower absoluteeclines as they begin treatment with lower plateletounts.
In summary, the results of this phase of the EPIC3
rogram demonstrate that PEG-IFN alfa-2b/WBD riba-irin is an effective and safe treatment option for severalopulations of patients with chronic hepatitis C andepatic fibrosis/cirrhosis for whom previous combina-ion therapy with any IFN alfa/ribavirin was ineffective.mportantly, this population can be defined by an arrayf treatment response predictors before therapy to morerecisely define the likelihood of an individual patientttaining SVR. Genotype and fibrosis stage were impor-ant predictors of response, even for patients with unde-ectable HCV-RNA at TW12. The results also suggesthat, after consideration of patient and disease character-stics, an effective approach is to treat patients until theesults of HCV-RNA PCR at TW12 are available; thoseho have HCV-RNA below the LLD at TW12 wouldenefit from continuing for a total of 48 weeks of com-ination therapy. In this study, the treatment paradigmesulted in a 56% SVR rate in patients with HCV-RNAelow the limit of detection at TW12. No new safety
ssues were identified in this study, which includes theargest group of patients with cirrhosis caused by chronicepatitis C studied to date. Based on HCV-RNA results,he population likely to respond to further treatment cane identified at TW12, thus limiting exposure to drug forhose unlikely to respond. The efficacy of long-term (upo 5 years) low-dose (0.5 �g/kg/wk) PEG-IFN alfa-2b
aintenance therapy in decreasing fibrosis progression,orbidity, and mortality is being assessed in the second
hase of the EPIC3 program; data from these 2 studiesill be available in 2009 and 2010.
Supplementary Data
Note: To access the supplementary materialccompanying this article, visit the online version ofastroenterology at www.gastrojournal.org, and at doi:
0.1053/j.gastro.2009.01.039.References
1. Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2aplus ribavirin for chronic hepatitis C virus infection. N Engl J Med2002;347:975–982.
2. Manns MP, McHutchison JG, Gordon SC, et al. Peginterferonalfa-2b plus ribavirin compared with interferon alfa-2b plus riba-virin for initial treatment of chronic hepatitis C: a randomised trial.Lancet 2001;358:958–965.
3. Poynard T, McHutchison J, Goodman Z, et al, and Albrecht J forthe ALGOVIRC Project Group. Is an “a la carte” combinationinterferon alfa-2b plus ribavirin regimen possible for the first linetreatment in patients with chronic hepatitis C? Hepatology 2000;31:211–218.
4. Shiratori Y, Imazeki F, Moriyama M, et al. Histologic improvementof fibrosis in patients with hepatitis C who have sustained re-sponse to interferon therapy. Ann Intern Med 2000;132:517–524.
5. Sobesky R, Mathurin P, Charlotte F, et al. Modeling the impact ofinterferon alfa treatment on liver fibrosis progression in chronichepatitis C: a dynamic view. Gastroenterology 1999;116:378–386.
6. Bruno S, Stroffolini T, Colombo M, et al. Sustained virologicresponse to interferon-� is associated with improved outcome inHCV-related cirrhosis: a retrospective study. Hepatology 2007;45:579–587.
7. Veldt BJ, Heathcote EJ, Wedemeyer H, et al. Sustained virologicresponse and clinical outcomes in patients with chronic hepatitisC and advanced fibrosis. Ann Intern Med 2007;147:677–684.
8. Afdhal NH, Levine R, Brown R, et al. Colchicine versus peg-interferonalfa 2b long-term therapy: results of the 4-year COPILOT Trial. Pre-sented at the 43rd Annual Meeting of the European Association forthe Study of the Liver (EASL 2008); April 23–27, 2008; Milan, Italy.
9. DiBisceglie AM, Shiffman ML, Everson GT, et al. Prolonged ther-apy of advanced chronic hepatitis C with low-dose peginterferon.N Engl J Med 2008;359:2429–2441.
0. Bedossa P, Poynard T for the METAVIR Cooperative Study Group.An algorithm for the grading of activity in chronic hepatitis C.Hepatology 1996;24:289–293.
1. Krawitt EL, Ashikaga T, Gordon SR, et al. Peginterferon alfa-2band ribavirin for treatment-refractory chronic hepatitis C. J Hepa-tol 2005;43:243–249.
2. Parise E, Cheinquer H, Crespo D, et al. Peginterferon alfa-2a(40KD) (PEGASYS) plus ribavirin (COPEGUS) in retreatment ofchronic hepatitis C patients, nonresponders and relapsers toprevious conventional interferon plus ribavirin therapy. Braz J In-fect Dis 2006;10:11–16.
3. Sherman M, Yoshida EM, Deschenes M, et al. Peginterferonalfa-2a (40KD) plus ribavirin in chronic hepatitis C patients whofailed previous interferon therapy. Gut 2006;55:1631–1638.
4. Shiffman ML. Management of patients with chronic hepatitis Cvirus infection and previous nonresponse. Rev Gastroenterol Dis2004;4(Suppl 1):S22–S30.
5. Veldt BJ, Brouwer JT, Adler M, et al. Retreatment of hepatitis Cnon-responsive to interferon: a placebo controlled randomizedtrial of ribavirin monotherapy versus combination therapy withribavirin and interferon in 121 patients in the Benelux. BMCGastroenterol 2003;3:24.
6. Taliani G, Gemignani G, Ferrari C, et al. Pegylated interferonalfa-2b plus ribavirin in the retreatment of interferon-ribavirin non-responder patients. Gastroenterology 2006;130;1098–1106.
7. Basso M, Torre F, Grasso A, et al. Pegylated interferon andribavirin in retreatment of non-responder-relapser HCV patients.Dig Liver Dis 2007;39:47–51.
8. Cornberg M, Hadem J, Herrmann E, et al. Treatment with dailyconsensus interferon (CIFN) plus ribavirin in non-responder pa-tients with chronic hepatitis C: a randomized open-label pilot
study. J Hepatol 2006;44:291–301.
1
2
2
2
2
2
2
2
2
2
R
HCP1
A
JAPt
i
(oMDD
C
FSAsDGrsNHcAROnc
F
Rmpps
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1628 POYNARD ET AL GASTROENTEROLOGY Vol. 136, No. 5
9. Jacobson IM, Gonzalez SA, Ahmed F, et al. A randomized trial ofpegylated interferon �-2b plus ribavirin in the retreatment ofhepatitis C. Am J Gastroenterol 2005;100:2453–2462.
0. Sagir A, Heintges T, Akyazi Z, et al. Relapse to prior therapy is themost important factor for the retreatment response in patientswith chronic hepatitis virus infection. Liver Int 2007;27:954–959.
1. Shiffman ML, Di Bisceglie AM, Lindsay KL, et al. Peginterferonalfa-2a and ribavirin in patients with chronic hepatitis C who havefailed prior treatment. Gastroenterology 2004;126:1015–1023.
2. Moucari R, Ripault M, Oulès V, et al. High predictive value of earlyviral kinetics in retreatment with peginterferon and ribavirin ofchronic hepatitis C patients non-responders to standard combi-nation therapy. J Hepatol 2007;46:596–604.
3. Berg T, von Wagner M, Nasser S, et al. Extended treatmentduration for hepatitis C virus type 1: comparing 48 versus 72weeks of peginterferon-alfa-2a plus ribavirin. Gastroenterology2006;130:1086–1097.
4. Sanchez-Tapias JM, Diago M, Escartin P, et al. Peginterferon-alfa2a plus ribavirin for 48 versus 72 weeks in patients with detect-able hepatitis C virus RNA at week 4 of treatment. Gastroenter-ology 2006;131:451–460.
5. Pearlman BL, Ehleben C, Saifee S. Treatment extension to 72weeks of peginterferon and ribavirin in hepatitis C genotype1-infected slow responders. Hepatology 2007;46:1688–1694.
6. Marcellin P, Heathcote EJ, Craxi A. Which patients with genotype1 chronic hepatitis C can benefit from prolonged treatment withthe “accordion” regimen? J Hepatol 2007;47:580–587.
7. Mangia A, Minerva N, Bacca D, et al. Individualized treatmentduration for hepatitis C genotype 1 patients: a randomized con-trolled trial. Hepatology 2008;47:43–50.
8. Jacobson IM, Brown RS, Freilich B, et al. Peginterferon alfa-2band weight-based or flat-dose ribavirin in chronic hepatitis Cpatients: a randomized trial. Hepatology 2007;46:971–981.
Received December 21, 2007. Accepted January 15, 2009.
eprint requestsAddress requests for reprints to: Thierry Poynard, MD, PhD,
ôpital La Pitié Salpêtrière, Université Pierre et Marie Curie Liverenter, Service d’hepatologie, 47-83 boulevard de l’hôpital, 75651aris CEDEX 13, France. e-mail: [email protected]; fax: (11) 33-
42-16-14-25. icknowledgmentsThe authors thank Weiping Deng, Nicole Stauffer, Luminita
ustice, Michele Sauer, Misti Linaberry, Victoria Rizvi, Stefanielfano, Peter Savino, Michael Salman, and Becky Liou of Schering–lough Research Institute for their contributions to the conduct ofhe study.
The complete list of the EPIC Study Group membership appearsn the online Appendix.
Presented in part at the 55th (2004), 56th (2005), and 57th2006) Annual Meetings of the American Association for the Studyf Liver Diseases; the 40th (2005) and 43rd (2008) Annualeetings of the European Association for the Study of the Liver;igestive Diseases Week 2005; and HEP DART 2007: Frontiers inrug Development for Viral Hepatitis.
onflicts of InterestThe authors disclose the following: T. Poynard, M. Colombo, S.
lamm, T. Berg E. Schiff, E. J. Heathcote, A. Craxi, M. Silva, and W.chmidt are members of the speakers bureau for Schering–Plough;. Craxi, E. J. Heathcote, and W. Schmidt are members of thepeakers bureau for Roche; T. Poynard, M. Colombo, E. Schiff, M.iago, S. Flamm, T. Berg, A. Craxi, M. Silva, E. J. Heathcote, and F.onçales receive research support from Schering–Plough; A. Craxi
eceives research support from Roche; S. Flamm receives researchupport from Valeant and serves on the speakers bureau forovartis; M. Colombo, E. Schiff, A. Craxi, J. Bruix, and E. J.eathcote are consultants for Schering–Plough; A. Craxi is aonsultant for Roche; L. Griffel, M. Burroughs, C. Brass, J. K.lbrecht, and P. Mukhopadhyay are employees of Schering–Ploughesearch Institute and stock holders of Schering–Plough; R. Moreno-tero, F. Carrilho, R. Terg, P. Bedossa, and T. McGarrity haveothing to disclose. Study participants were told of investigators’onflicts of interests.
undingSchering–Plough Research Institute fully supported the study.
ole of study sponsor: Schering–Plough Research Institute played aajor role in the study design. They collected, analyzed, and
erformed the initial interpretation of all data. All the authorsrovided input and agreed to the final interpretation. The decision toubmit the report was made by Schering–Plough Research Institute
n conjunction with the publication committee.
ARFLKTHMJHPKJFAWXWHLDAJJMMGRRHSMSRRAJFSKDENHYRIGKPPMBL
AEMPPLAMATJCLRBDMCMKRALMJFRTMJRAMSHWDMVJEWWOKWMCUMHRRDE
May 2009 RESPONSE TO PEG-IFN alfa-2b/RBV RETREATMENT 1628.e1
Appendix: EPIC3 Study Group
lfredo Albertiamon Perez Alvarezrank Andersonuis Balartarl Barangehomas Bergenry Bodenheimerarc Bourliere
ean-Pierre Bronowickiarald Brunnereter Buggischelly Warren Burak
ose Luis Callejalair Carrilhormando Carvalhoolfgang Caselmann
avier Causseendy Chengenrique Sergio Moraes Coelhouis Colombatoarrell Crawfordntonio Craxi
ose Curciarelloean Delwaide
iguel Angel Serra Desfilisoises Diagoeoffrey Dusheikoobert Ennsafael Esteban-Murugo Fainboim
aya Victor Feinmanaria Lucia Gomes Ferraz
teven Flammaymundo Parana Ferreira Filhooberto Focacciadrian Gadano
acob Georgeernando Lopes Goncalestuart Gordonlaus Siegfried Gutfreundieter Haussinger. Jenny Heathcoteir Hilzenratolger Hinrichsenves Horsmansolf Hultcrantz
ra Jacobsonary Jeffreyelly Kaitaaul Kingaul Kwoing-Yang Lai
arbara Leggett
uiz Lyra Gndreas Maieronmanuel K. Manesisichael Manns
atrick Marcellinaul Marottauis Marsanongelo Mattosarcos Mauad
rthur J. McCulloughhomas McGarrity
ohn McHutchisonarlos Brandao Melloindsay Millisonicardo Moreno-Oteroeat Muellhauptominique Araujo Muzzilloeng Ngu
laus Niederauary Pat Pauly
evork Peltekianobert Perrillontonino Picciottoeonardo Pinchukauro Podda
orge-Luis Poored Poordadaoul Pouponhierry Poynardayra Ramos-Gomez
urg Reichenobert Reindollarlvaro Reymundeario Rizzetto
tuart Robertseitor Rosailliam Rosenbergouglas Routleyaria Grazia Rumi
inod Rustgiose Sanchez-Tapiasugene Schiffarren Schmidtolfgang Schmidtbaid S. Shaikhenneth Shermanilliam Sievertarcelo Silva
oleman Smithlrich Spenglerark Sulkowskiugo Tannoosangela Teixeirauben Tergoris Torosther Torres
regorio Castellanos Tortajada
ACNAAR
EHFRS
1628.e2 POYNARD ET AL GASTROENTEROLOGY Vol. 136, No. 5
lbert Tranhristian Trepoaoky Tsaina Maria Valedriana Varon
amon Planas Vila Arica Villa. Van Vlierberghelorence Wongeinhart Zachovaltefan Zeuzem
nna Linda Zignego
Related Documents











