FROM BENCH TO IMAGING Contrast enhanced ultrasound imaging Steven B. Feinstein, MD, FACC, a Blai Coll, MD, PhD, b Daniel Staub, MD, c Dan Adam, PhD, d Arend F. L. Schinkel, MD, PhD, e Folkert J. ten Cate, MD, e and Kai Thomenius, PhD f HISTORIC DEVELOPMENT Introduction The origins of contrast enhanced ultrasound imag- ing (CEUS) date to the earliest observations of Claude Joyner and publications of Gramiak and Shah in 1968. 1 Interest in the development of ultrasound contrast agents and associated clinical applications continues today, nearly 40 years after the first reports. The use of blood pool agents for enhancement of cardiovascular structures is ubiquitous, current clinical diagnostic imaging modalities utilize contrast agents to define anatomy and quantify tissue perfusion. Specifi- cally, with regard to ultrasound contrast agents, the unique physical properties of air-filled, microspheres serving as true intravascular indicators provide an unparalleled access to the intrinsic spatial and temporal heterogeneity of tissue perfusion. 2 Importantly, though initially developed for diag- nostic applications, novel therapeutic applications for the ultrasound contrast agents are forthcoming. Thus, while the use of ultrasound contrast agents today pro- vides important clinical information regarding chamber enhancement and myocardial perfusion, in the near future these agents will provide therapeutic options for site-specific, drug/gene delivery. Ultimately, ultrasound contrast agents may provide the opportunity to dramat- ically alter both the diagnosis and subsequent treatment of numerous diseases. Background Today, the clinical applications of CEUS occupy a unique position in the non-invasive imaging field as defined by these parameters: • Use of non-ionizing, acoustic energy • Unparalleled spatial and temporal resolution • Real-time processing • Established user base • Portability and economy During the formative years of CEUS development, researchers focused on the development of novel agents and the requisite validation of the concept that these air- filled, microspheres represented true, intravascular, non- diffusible indicators. The list of scientists/clinicians performing this pioneering work in the 1960-1980’s include many of the following names: Gramiak and Shah, 1 Reale et al, 3 Meltzer et al, 4 DeMaria et al, 5,6 Reisner, Schwartz, Kremkau, 7 Ziskin et al, 8 Bove et al, 9 Bommer et al, 10 McKay and coworkers, 11 Kort and Kronzon, 12 Goldberg 13 to list but a few of the innova- tors. The scientific investigations provided a foundation for the ensuing clinical applications of CEUS. Later, a second wave of CEUS development was spearheaded by the efforts of Armstrong et al, 14 Tei et al, 15 Feinstein et al, 16 Powsner et al, 17 Kaul et al, 18 Porter et al, 19 Kemper et al, 20 Zwehl et al, 21 to list only a few. Of note, the initial efforts designed to quantify the novel ‘‘contrast effect’’ can be attributed to DeMaria and Bommer, 6 Ong et al, 22 Meltzer et al. 23 Ultimately, the efforts culminated in the production of commercial ultrasound contrast agents (Levovist in Europe, Berlex, Schering, and Albunex in the USA, Molecular Biosystems Inc.). Today, implementation of sophisticated harmonic imaging systems and lower mechanical index imaging provide prolonged in vivo persistence and markedly enhanced, signal to noise ratios. Importantly, the appropriate and clinically indicated clinical uses of CEUS are reimbursed through third party insurers based on the proven safety and efficacy of use. The development of ‘‘second’’ generation con- trast agents generally utilized high molecular weight, low soluble gases, and resulted in the prolonged From the Rush University Medical Center, a Chicago, IL; DETMA, b Hospital Universitari Arnau de Vilanova, Lleida, Spain; Division of Angiology, c University Hospital Basel, Basel, Switzerland; Department of Biomedical Engineering, d Technion - Israel Institute of Technology, Haifa, Israel; The Thoraxcenter, e Rotterdam, The Netherlands; GE Global Research, f Niskayuna, NY. Reprint requests: Steven B. Feinstein, MD, FACC, Rush University Medical Center, Suite 1015 Jelke, 1653 West Congress Parkway, Chicago, IL 60612; [email protected]. J Nucl Cardiol 2010;17:106–15. 1071-3581/$34.00 Copyright Ó 2009 by the American Society of Nuclear Cardiology. doi:10.1007/s12350-009-9165-y 106

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

FROM BENCH TO IMAGING
Contrast enhanced ultrasound imaging
Steven B. Feinstein, MD, FACC,a Blai Coll, MD, PhD,b Daniel Staub, MD,c
Dan Adam, PhD,d Arend F. L. Schinkel, MD, PhD,e Folkert J. ten Cate, MD,e
and Kai Thomenius, PhDf
HISTORIC DEVELOPMENT
Introduction
The origins of contrast enhanced ultrasound imag-
ing (CEUS) date to the earliest observations of Claude
Joyner and publications of Gramiak and Shah in 1968.1
Interest in the development of ultrasound contrast agents
and associated clinical applications continues today,
nearly 40 years after the first reports.
The use of blood pool agents for enhancement of
cardiovascular structures is ubiquitous, current clinical
diagnostic imaging modalities utilize contrast agents to
define anatomy and quantify tissue perfusion. Specifi-
cally, with regard to ultrasound contrast agents, the
unique physical properties of air-filled, microspheres
serving as true intravascular indicators provide an
unparalleled access to the intrinsic spatial and temporal
heterogeneity of tissue perfusion.2
Importantly, though initially developed for diag-
nostic applications, novel therapeutic applications for
the ultrasound contrast agents are forthcoming. Thus,
while the use of ultrasound contrast agents today pro-
vides important clinical information regarding chamber
enhancement and myocardial perfusion, in the near
future these agents will provide therapeutic options for
site-specific, drug/gene delivery. Ultimately, ultrasound
contrast agents may provide the opportunity to dramat-
ically alter both the diagnosis and subsequent treatment
of numerous diseases.
Background
Today, the clinical applications of CEUS occupy a
unique position in the non-invasive imaging field as
defined by these parameters:
• Use of non-ionizing, acoustic energy
• Unparalleled spatial and temporal resolution
• Real-time processing
• Established user base
• Portability and economy
During the formative years of CEUS development,
researchers focused on the development of novel agents
and the requisite validation of the concept that these air-
filled, microspheres represented true, intravascular, non-
diffusible indicators. The list of scientists/clinicians
performing this pioneering work in the 1960-1980’s
include many of the following names: Gramiak and
Shah,1 Reale et al,3 Meltzer et al,4 DeMaria et al,5,6
Reisner, Schwartz, Kremkau,7 Ziskin et al,8 Bove et al,9
Bommer et al,10 McKay and coworkers,11 Kort and
Kronzon,12 Goldberg13 to list but a few of the innova-
tors. The scientific investigations provided a foundation
for the ensuing clinical applications of CEUS.
Later, a second wave of CEUS development was
spearheaded by the efforts of Armstrong et al,14 Tei
et al,15 Feinstein et al,16 Powsner et al,17 Kaul et al,18
Porter et al,19 Kemper et al,20 Zwehl et al,21 to list only a
few. Of note, the initial efforts designed to quantify the
novel ‘‘contrast effect’’ can be attributed to DeMaria
and Bommer,6 Ong et al,22 Meltzer et al.23
Ultimately, the efforts culminated in the production
of commercial ultrasound contrast agents (Levovist in
Europe, Berlex, Schering, and Albunex in the USA,
Molecular Biosystems Inc.).
Today, implementation of sophisticated harmonic
imaging systems and lower mechanical index imaging
provide prolonged in vivo persistence and markedly
enhanced, signal to noise ratios. Importantly, the
appropriate and clinically indicated clinical uses of
CEUS are reimbursed through third party insurers based
on the proven safety and efficacy of use.
The development of ‘‘second’’ generation con-
trast agents generally utilized high molecular weight,
low soluble gases, and resulted in the prolonged
From the Rush University Medical Center,a Chicago, IL; DETMA,b
Hospital Universitari Arnau de Vilanova, Lleida, Spain; Division
of Angiology,c University Hospital Basel, Basel, Switzerland;
Department of Biomedical Engineering,d Technion - Israel Institute
of Technology, Haifa, Israel; The Thoraxcenter,e Rotterdam, The
Netherlands; GE Global Research,f Niskayuna, NY.
Reprint requests: Steven B. Feinstein, MD, FACC, Rush University
Medical Center, Suite 1015 Jelke, 1653 West Congress Parkway,
Chicago, IL 60612; [email protected].
J Nucl Cardiol 2010;17:106–15.
1071-3581/$34.00
Copyright � 2009 by the American Society of Nuclear Cardiology.
doi:10.1007/s12350-009-9165-y
106
in vivo persistence. These second generation agents
fulfilled the required clinical expectations for safe,
efficient, and economical non-invasive imaging of the
left-sided cardiac chambers (i.e., left ventricular
opacification, Doppler enhancement, and myocardial
perfusion).
The ‘‘third’’ generation of contrast agents may be
considered as ‘‘designer’’ agents for molecular imaging.
These agents are uniquely and specifically labeled
and, as such, are designed to provide quantitative,
physiologic localization (‘‘molecular imaging’’) of
inflammation, and related disease states. The leaders in
this field include Jonathan Lindner, Lisa Villanueva,
Thomas Porter, Evan Unger, Samuel Wickline, David
McPherson, to name but a few.
Ultimately, the ‘‘fourth generation’’ CEUS appli-
cations break new ground in the area of therapy. These
agents are designed as ultrasound-directed, site-specific
drug/gene therapeutic systems. The pioneers in this
field include Ishihara,24 Unger et al,25 Grayburn and
coworkers,26 and an ever-expanding cadre of
researchers.
Reflecting back to the early years of CEUS, it is
clear that the dedicated work of many clinicians/
researchers cannot be underestimated. Their research
efforts directly contributed to the development of a
novel, safe, and efficacious non-invasive imaging
modality which improves patient care and reduces
downstream testing expenses and risk.
Table 1 (Ultrasound contrast agents) lists the cur-
rent ultrasound agents.
CEUS CLINICAL APPLICATIONS: LEFTVENTRICULAR OPACIFICATION
In the USA, two FDA ultrasound contrast agents are
currently approved for clinical use: Optison, GE Medi-
cal Diagnostics, Princeton, NJ; Definity (Lantheus
Medical Imaging, Billerica, MA). Several additional
agents are approved for clinical use outside of the USA
and include: Sonazoid, Sonovue, and Levovist.
Generally, direct visualization of the left ventricular
chamber and endocardial surfaces permits sonographers
and physicians to make clinical judgments regarding left
ventricular systolic function, filling status, and intra-
cavitary anatomy. Fundamentally, if health care pro-
fessionals cannot visualize the full extent of the left
ventricle, the diagnostic accuracy of the test is limited
and the physician’s confidence is reduced.
Therefore, ultrasound contrast agents are indicated in
patients who possess technically limited, suboptimal
echocardiograms. The American Society of Echocardiog-
raphy in 200027 and 200828 and the European Association
of Echocardiography 200929 recognized the clinical value
of using ultrasound contrast agents and issued position
papers providing guidelines. The following list of indica-
tions was abstracted from the ASE and EAE guidelines:
• Improve endocardial visualization: The resting state
echocardiography revealed reduced image quality (i.e.,
two contiguous left ventricular endocardial segments
were not observed in the non-contrast images).
• Reduce variability and increase accuracy in assessing
LV volume and LV ejection fraction.
Table 1. Ultrasound contrast agents (present and past agents)
Manufacturer Name Type Development stage
Accusphere Polymer/perfluorocarbon Clinical development
Alliance/Schering Imavist Encapsulated perfluorocarbon Clinical development
Andaris Quantison Albumin/low solubility gas Clinical development?
Bracco Sonovue Lipid/sulfur hexafluoride Approved for clinical use
Byk-Gulden BY963 Lipid/air (BY963) Clinical development
Cavcon Filmix Lipid/air Pre-clinical development
Lantheus Medical Imaging Definity Pentane/octafluoropropane Approved for clinical use
GE Healthcare Optison Sonicated albumin/octafluoropropane Approved for clinical use
GE Healthcare Sonazoid Lipid/perfluorocarbon Approved for clinical use
Point Biomedical Bisphere Perfluorocarbon/polymer bilayer Clinical development
Porter MD/University of
Nebraska
PESDA Sonicated albumin/perfluoropropane Not commercially available
Schering Echovist Approved for clinical use
Schering Levovist Lipid/air Approved for clinical use
Schering Sonavist Polymer/air Clinical development
Sonus Echogen Surfactant/perfluorocarbon Withdrawn from development
Journal of Nuclear Cardiology Feinstein et al 107
Volume 17, Number 1;106–15 Contrast enhanced ultrasound imaging

• Increase reader confidence for the interpretation of
left ventricle functional, structure, and filling status;
at rest and in stress echocardiography
• Confirm or exclude left ventricular structural abnor-
malities: apical variant of hypertrophic cardiomyop-
athy, ventricular non-compaction, apical thrombus,
aneurysm, pseudoaneurysm, myocardial rupture, and
intracardiac masses (tumors and thrombi).
In 2000-2002, shortly after the initial FDA approval
of ultrasound contrast agent, the initial clinical reports
described the value of CEUS for identifying left-sided,
cardiac chambers, particularly in patients with techni-
cally limited echocardiogram examinations.30-32 These
early studies provided a strong clinical base from which
future guidelines were developed.
Today, the use of CEUS is an accepted standard of
care. Notwithstanding the implementation of harmonic
imaging systems, experts generally agree that approxi-
mately 10-30% of all transthoracic echo images are
considered technically difficult or uninterpretable. In
fact, the value of CEUS is increasingly relevant in
today’s healthcare climate where efficiency, safety, and
utility are at a premium.
As an example, in a recent study from Senior et al,33
the authors used CEUS for determination of left ven-
tricular remodeling after acute myocardial infarction.
The addition of CEUS to the clinical study provided an
independent, incremental value for the prediction of late
mortality. This recent study reinforced the concept that
contrast echocardiography provides clinical utility for
the determination of left ventricular function and clinical
outcomes following an acute myocardial infarction.
Importantly, in 2009 Kurt et al,34 published a
landmark study in which they reported that the routine
use of CEUS for left ventricular chamber enhancement
significantly impacted diagnostic accuracy and resource
utilization; directly benefiting patient management. In
this large, prospective study, ultrasound contrast agents
were clinically indicated in 14.5% of the cohort (632/
4362). The impact of CEUS imaging was reflected in a
change in therapy (drugs), procedures or both in 35.6%
while the most benefit accrued to those patients who
were in the surgical intensive care unit. In this critically
ill population, the authors noted a change in therapy and
procedures in 62.7% of the patients. Additionally, the
authors commented on a reduction in subsequent testing
which included exposure to ionizing radiation and
invasive testing.
CEUS SAFETY
In September 2007, following the passage of House
Resolution (H.R. 3580), the FDA officials were provided
with additional authority for monitoring of phase-IV,
post-approval surveillance of ethical drugs. Subse-
quently, in October of 2008, following a series of self-
reported adverse events, the FDA officials issued a
‘‘Black Box’’ warning for Perflutren ultrasound contrast
agents affecting two previously FDA approved ultra-
sound contrast agents: Optison (approved in 1997; GE
Medical Diagnostics, Princeton, NJ) and Definity
(approved in 2001; Lantheus Medical Imaging, Bille-
rica, MA). The revised product label included new
contraindications. The sequence of events leading up to
these labeling were identified as follows:
• Post-marketing reports of *190 serious adverse
events and four deaths shortly following administra-
tion of the contrast agents (all self-reported cases)
• ‘‘Safety signal’’ appeared to be identified in animal
study resembling serious cardiopulmonary reactions
observed in humans
• The safety issues associated with Sonvue in Europe
• Lack of pulmonary hemodynamic data in humans
• A pre-marketing database that generally excluded
patients with unstable cardiopulmonary conditions
• Lack of a systematic risk assessment and management
plan
• Failure of a manufacturer to initiate an ‘‘important
post-marketing clinical study commitment to assess
its product’s safety.’’
Shortly following the revised product labeling,
an international grassroots organization of physicians,
sonographers, nurses, and interested parties strongly
requested reconsideration of the newly applied restric-
tions. Additionally, professional guilds (the American
Society of Echocardiography and the European Asso-
ciation of Echocardiography) similarly voiced concern
over the new labeling limitations on the ultrasound
contrast agents.
In direct response to the October 2007 FDA label
changes, clinicians promptly responded with a series of
peer-reviewed, publications focused on the proven
clinical safety record of ultrasound contrast agents. As
of May 2009, published reports cited over 228,611
patient cases in which ultrasound contrast agents were
safely used.
In May 2008, the FDA officials revised the labeling
changes to reflect the well-established, clinical safety
record of ultrasound contrast agents.
Continuing today, the clinical community, grass-
roots organizations, and professional societies provide
leadership highlighting the important clinical utility and
safety of ultrasound contrast agents. In fact, based on
intense response of the community, a new international,
not-for-profit organization was created to provide
interdisciplinary and international information for those
108 Feinstein et al Journal of Nuclear Cardiology
Contrast enhanced ultrasound imaging January/February 2010
interested in CEUS. The International Ultrasound Con-
trast Society (www.icus-society.org) provides monthly
newsletters and timely updates to all members at no
charge. Currently, ICUS provides updates to several
thousand subscribers in [57 countries. (For a list of the
recently published reports see references.32-39)
VASCULAR IMAGING APPLICATIONS
Overview
Today, the clinical vascular applications for the use
of CEUS are legion. Similar to the chamber enhance-
ment applications for echocardiography, the vascular
applications include enhancement of aorta, carotid
arteries, and peripheral venous systems.
Mattrey and Kono initially identified the clinical
value of using CEUS as an alternative to more invasive
imaging technologies.35,36 Although, ultrasound contrast
agents are not currently FDA approved in the USA, this
is not the case in Europe, Asia, and South America. In
the autumn of 2009, it is expected that vascular FDA-
approved, clinical trials will be initiated in the USA.
Recently the use of CEUS has been identified as a
novel imaging system capable of producing high reso-
lution, real-time, images of microvascular perfusion,
including tumor angiogenesis. Specifically, imaging of
the neovasculature (vasa vasorum) within the carotid
artery atherosclerotic plaque has captured world-wide
attention.37,38,39 Thus, the unifying concept is that arte-
rial wall inflammation/hypoxia provides a source for the
generation of VEGF proteins and subsequent neovas-
cularization growth. Hypoxia and inflammation events
are routinely observed in diverse disease states including
diabetes, atherosclerosis, connective tissue diseases, and
cancer. And with great prescience, Judah Folkman
realized that neovascularization provides the requisite
tumor nutrient blood supply commonly observed in a
variety of disease states.40
VASCULAR APPLICATIONS
Currently, the applications for the use of ultrasound
contrast agents include the following: (1) Enhancement
of the carotid artery lumen (plaque/ulcer), (2)
Enhancement of the intima-media-thickness (IMT), and
(3) Identification of adventitial/intra-plaque angiogene-
sis (vasa vasorum).
Enhancement of the Carotid Artery Lumen
Ultrasound contrast agents serve as blood pool
agents and consequently provide enhancement of the
carotid arterial luminal surface which includes the
common, bifurcation, and internal carotid arteries. Often
the case, the ability to clearly define extent of the carotid
vascular tree eludes the examiner. The image quality is
often compromised by the physical habitus of the sub-
ject. Importantly, CEUS provides a non-ionizing
radiation alternative to more invasive and higher risk
procedures.36
Over the last few years, there are numerous reports
from international centers which described the use of
CEUS for vascular imaging, specifically for the ana-
tomic enhancement of the luminal structures leading to
the diagnosis of irregular surface lesions, ulcers, soft
plaque, etc.2,35,37,41-45
At Rush University Medical Center in Chicago,
Illinois, we have performed over 1000 CEUS clinical
carotid examinations since 2001. All the studies were
performed under physician supervision with appropriate
institutional approvals. No adverse events or untoward
occurrences were noted. Remarkably, over the last
9 years, frequently, luminal irregularities (i.e., ulcers
and ‘‘soft plaque’’) were not observed without the use of
ultrasound contrast agents (see Figures 1, 2, 3, and 4). In
order to confirm the value of CEUS for routine vascular
imaging, multi-center, prospective clinical trials will be
required to ascertain the value of using these agents for
enhanced lesion detection in ‘‘at risk’’ populations.37
Enhancement of the Carotid Intima-Media-Thickness (IMT)
The use of the ultrasound-derived c-IMT as a sur-
rogate marker of systemic atherosclerosis was first
described by Pignoli in 1986.46 Subsequently, over the
last 23 years, the use of c-IMT has become a widely
accepted clinical standard for the detection of premature
atherosclerosis. Numerous FDA approved clinical trials
utilized c-IMT as an efficient marker for therapeutic
efficacy.47
Traditionally, clinicians and researchers readily
acknowledge the technical limitations which surround
the precise measurement of c-IMT measurements, par-
ticularly associated with identification of the carotid
artery near wall IMT.48-50 The primary technical issues
revolve around acoustic physics and include the rever-
berant acoustic noise generated from the overlying soft
tissues; all of which limit a clear acoustic definition of
the near wall. In distinction to the near wall, the acoustic
definition of the carotid artery far wall is regularly and
routinely visualized. This is due, in part, to the overlying
presence of the uniform media (blood) and lack of tissue
reflectance and interference. Due to the fact that the
carotid artery far wall remains an acoustically strong
acoustic reflector, this target is generally used in most
clinical studies and related pharmaceutical trials.
Journal of Nuclear Cardiology Feinstein et al 109
Volume 17, Number 1;106–15 Contrast enhanced ultrasound imaging
However, based on recently published data, CEUS
provides a reliable and precise measurement of the near
c-IMT, particularly when compared to similar c-IMT
measurements performed without the use of ultrasound
contrast agents.51,52,45 In fact, and wholly consistent
with this data, previous pathology studies indicate that
the near wall is consistently thicker (20%) than the far
wall of the c-IMT; thus, implying that systemic athero-
sclerosis is preferentially distributed on the near wall
structures.53
Generally, the procedure for performing CEUS is
routine and straightforward. Specifically, after a patient
is referred for a clinically indicated carotid ultrasound
examination, it is reasonable to develop a consent form
for ‘‘off-label’’ use of ultrasound contrast agents. The
performance of a CEUS study requires a peripheral
intravenous injection of 0.5-1.0 mL of an FDA
approved contrast agent. Standard vascular imaging of
the carotid artery is routinely performed with a linear
array transducer. The mechanical index used for CEUS
is set at levels that are considerably lower levels than
those required for non-contrast studies (0.1-0.2 MI vs
0.3-0.5 MI, respectively). In order to measure the
c-IMT, it is recommended that one uses a readily
available semi-automated, computer-assisted c-IMT
software program.
The clinical utilization of the c-IMT as a surrogate
marker for the diagnosis of premature atherosclerosis is
increasing based on published clinical data bases.
Accordingly, the American Society and the Society for
Vascular Medicine have provided guidelines for clinical
use.54
Clearly, a current limitation for the use of per-
forming serial c-IMT measurements in individuals
remains the inherent error of measurement due to the
lack of a truly volumetric ultrasound scanner. While the
value if two-dimensional c-IMT analyses is unques-
tioned, the issues surrounding the routine clinical use
remain. Ultimately, with the introduction of real-time,
three-dimensional ultrasound scanners, the technical
issues associated with image alignment and registration
will be reduced.
Identification of Adventitial and Intra-Plaque Angiogenesis (Vasa Vasorum)
Historically, clinicians and researchers have repor-
ted upon the association of plaque vascularity and
‘‘vulnerability.’’39,55-74 Recently, CEUS imaging of the
carotid artery provided a novel, non-invasive method for
directly examining plaque vascularity; perhaps provid-
ing a ‘‘window’’ into plaque vulnerability.
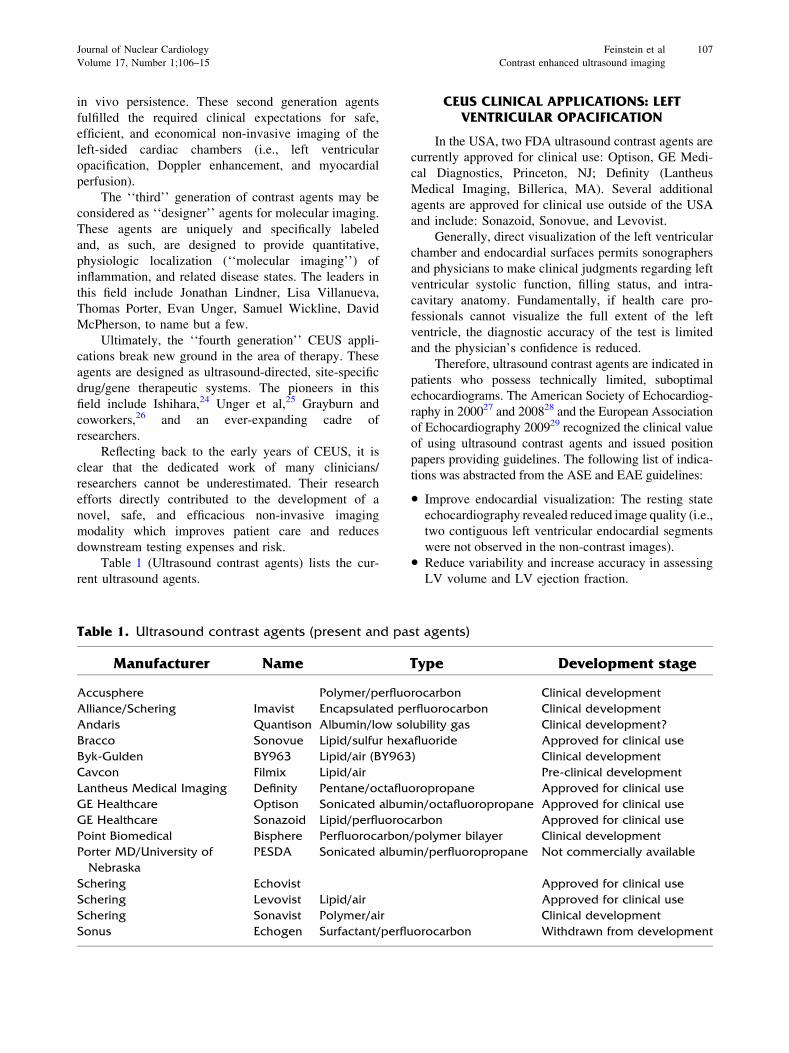
Figure 1. Contrast-enhanced carotid ultrasound imaging—intra-luminal plaque. A, C Twodifferent carotid arteries with intra-luminal plaque on B-mode ultrasound imaging. B, DCorresponding arteries on contrast-enhanced ultrasound. The carotid intima-media complex(c-IMT) is depicted as a hypoechoic line and the adventitial layer appears echogenic.
110 Feinstein et al Journal of Nuclear Cardiology
Contrast enhanced ultrasound imaging January/February 2010
Historical consideration of the vasa vaso-rum. Atherosclerotic plaques are believed to develop
from an initial endothelial cell insult often precipitated
by mechanical shearing, oxidative, and/or hypoxia
stresses from noxious substances. Following the initiat-
ing event, the subsequent deposition of intra-cellular
matter promotes focal migration of inflammatory cells
(monocyte derived macrophages), smooth muscle cells,
and fibroblasts, accumulating in the intracellular space
often resulting in foam cell development, raised lesions
and release of tissue hypoxic factors, and VEGF
proteins.
Sluimer et al, provided insight into the mechanism
surrounding the ongoing development of the tissue
hypoxia based on a description of the incomplete
endothelial junctions and inadequate structural integrity
of the immature and thin-walled microvessels.72 The
presence of the immature microvessels (‘‘leaky’’ ves-
sels) contribute inflammation materials by providing a
source of noxious plasma components (hemoglobin,
oxidized low-density lipoprotein cholesterol, lipopro-
tein[a], glucose, advanced glycation end products AGE)
and inflammatory cells.73,74
Ultimately, the atherosclerotic plaque, similar to the
other abnormal tumor growths, requires nutrient blood
flow supplied by arterial and venous vasa vasorum.
The anatomic structure of the vasa vasorum as
related to the growth of atherosclerotic plaques has been
well characterized by pathologists over 100 years ago.65
Based on a series of autopsy reports, intra-plaque
angiogenic vessels were identified within the vessel wall
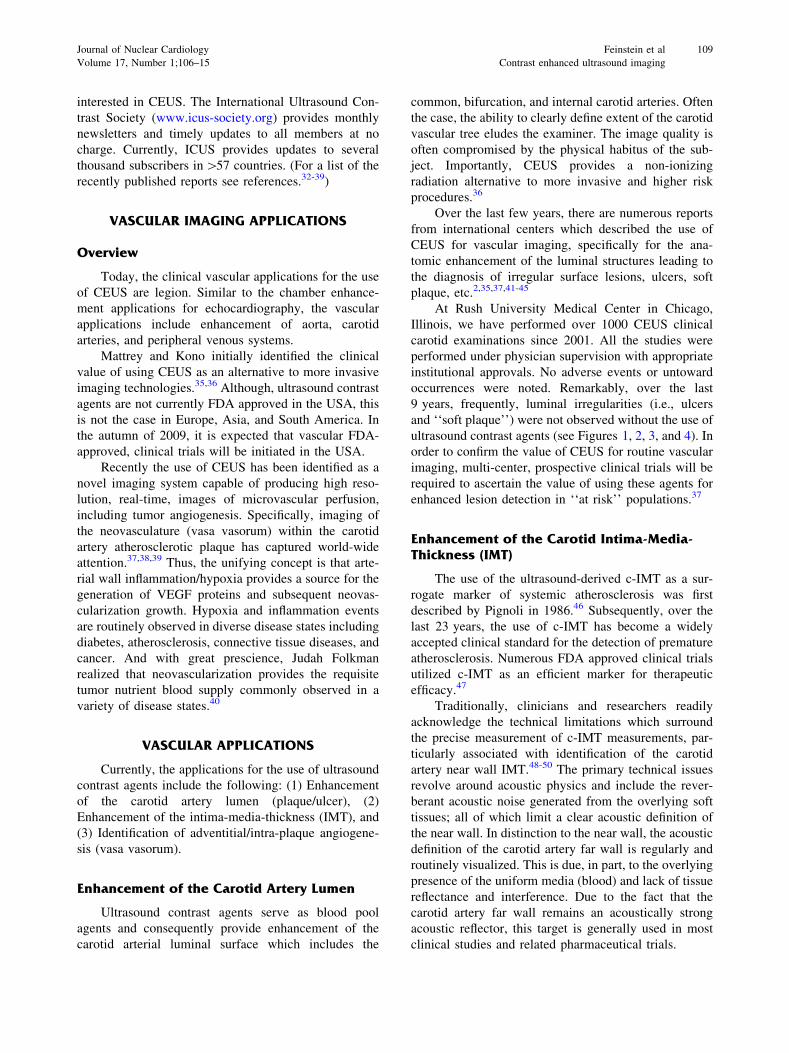
Figure 2. Contrast-enhanced carotid ultrasound imaging—plaque ulceration. A, C Two differentcarotid arteries with plaque ulceration on B-mode ultrasound imaging. B, D Corresponding arterieson contrast-enhanced ultrasound.
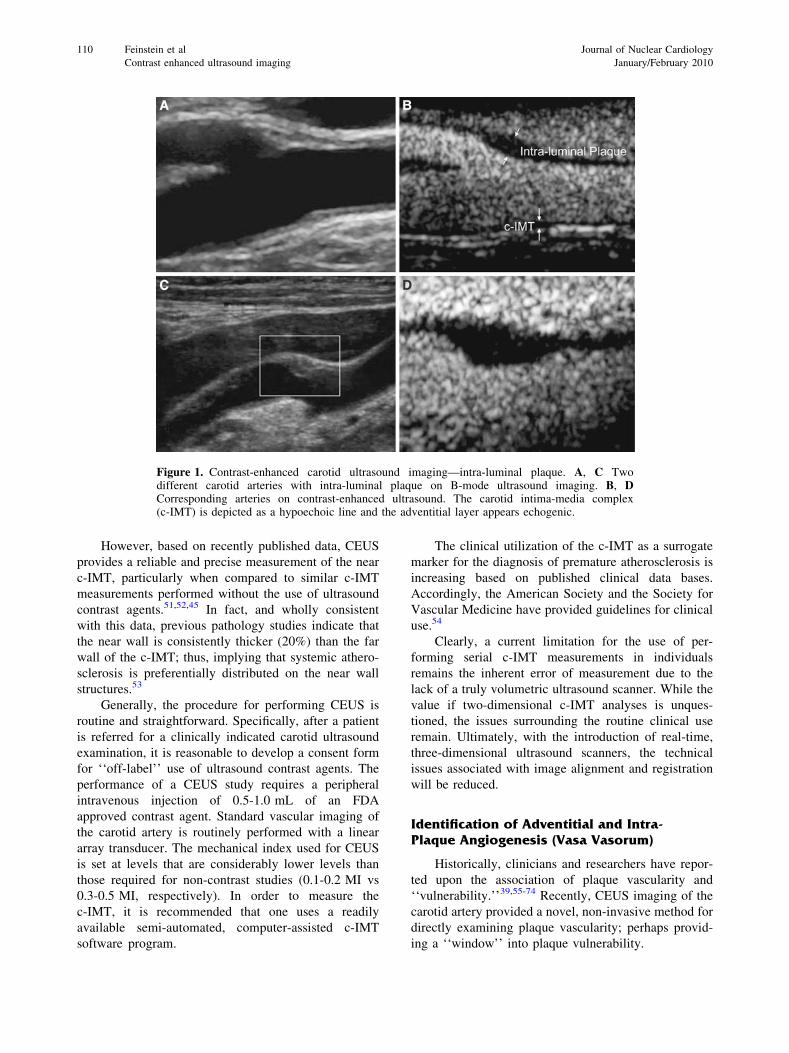
Figure 3. Contrast-enhanced carotid ultrasound imaging—intraplaque neovascularization. Carotid artery with intra-lumi-nal plaques and intra-plaque neovascularization (arrow).
Journal of Nuclear Cardiology Feinstein et al 111
Volume 17, Number 1;106–15 Contrast enhanced ultrasound imaging
(media and intima) in subjects with known systemic
atherosclerosis.65,75 The seminal articles of Barger
et al55 and Beeuwkes et al56 and Winternitz in 1876,
provided important evidence directly linking adventitial
and intra-plaque vasa vasorum to the atherosclerotic
disease processes.
In 2004, Fleiner et al75 observed that the presence
and degree of neovascularization within vulnerable
plaque was associated with plaque rupture and clinical
occlusive cardiovascular events.
Similarly, Kumamoto et al in 1995 observed:
There was a significant positive correlation
between the density of new vessels in the intima
and the incidence of luminal stenosis, the extent of
chronic inflammatory infiltrate, the formation of
granulation tissue, or the atheromatous changes,
whereas the vascular density decreased in the
extensively hyalinized and calcified intima. The
newly formed intimal vessels originated mainly
from the adventitial vasa vasorum and also partly
from the proper coronary lumen. The intimal
vessels that originated from the adventitia occurred
approximately 28 times more frequently than those
that originated from the luminal side.65
In addition, Moreno and Fuster reported findings
which directly linked atherosclerosis and diabetes to the
formation of vulnerable plaques.76 Recently, Mauriello
et al examined 544 coronary segments in 16 patients
who experienced fatal coronary events.77 The results
revealed the presence of diffuse, active inflammation in
the entire coronary vascular system, in patients with
both stable and vulnerable plaques.
Using experimental animal models with dietary-
induced atherosclerosis, Williams et al showed regres-
sion of intima and media neovascularization after a
reduction of cholesterol feeding.78 In addition, Wilson
et al79 used micro-computed tomography techniques to
observe the induction of coronary adventitial vasa
vasorum in the pig and, subsequently, revealed regres-
sion after initiating statin therapy. Importantly, the
authors noted that the excessive growth of adventitial
vasa vasorum preceded the development of luminal
plaques. Similarly, Moulton et al studied anti-angio-
genesis therapies in an experimental animal model of
atherosclerosis.80
In 2007, Shah et al, at Rush University Medical
Center, in Chicago, published a clinical validation study
based on pathology specimens of subjects who under-
went CEUS prior to undergoing carotid endarterectomy
surgery.81 The results revealed a direct, positive corre-
lation between CEUS images and the surgically derived,
tissue specimens with regard to presence and degree of
angiogenesis within the human carotid plaques. For this
study, the histology consisted of hematoxylin and eosin
stains, with immunohistochemical markers: CD31,
CD34, von Willebrand factor, CD68, and were evalu-
ated for degree of vascularity.
Sets of stained slides were examined microscopi-
cally for evidence of neovascularization and inflam-
mation using a grading system as reported by Jeziorska
in 1999.61
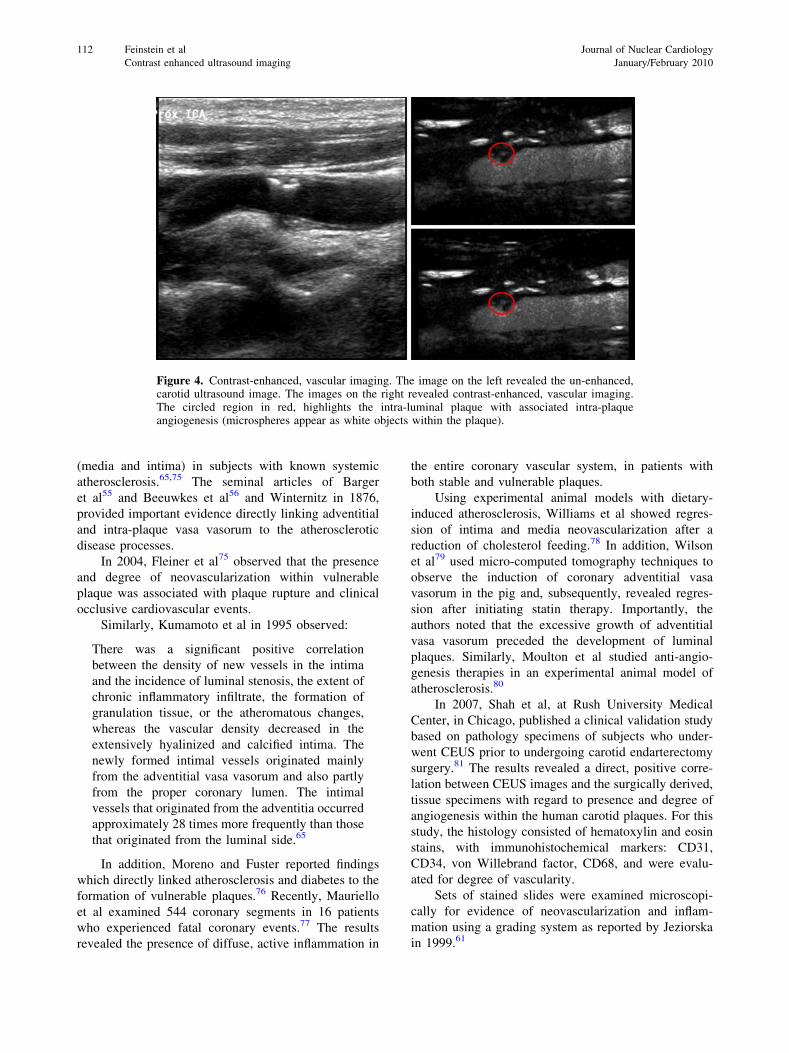
Figure 4. Contrast-enhanced, vascular imaging. The image on the left revealed the un-enhanced,carotid ultrasound image. The images on the right revealed contrast-enhanced, vascular imaging.The circled region in red, highlights the intra-luminal plaque with associated intra-plaqueangiogenesis (microspheres appear as white objects within the plaque).
112 Feinstein et al Journal of Nuclear Cardiology
Contrast enhanced ultrasound imaging January/February 2010

Similar to the limitation mentioned in performing
serial c-IMT measurements in the individual patient, the
ability to accurately quantify adventitial and intra-plaque
vasa vasorum, will necessitate the construction of an
ultrasound system with true, volumetric, image acquisi-
tion. Figure 5 is an image obtained from a real-time, 3D
mechanical ultrasound system during a clinical study
using CEUS. As noted, one can identify the luminal sur-
faces and the presence of the adventitial vasa vasorum.
FUTURE THERAPEUTIC APPLICATIONS
The current clinical applications of CEUS are
exclusively approved for diagnostic imaging. However,
future applications include a paradigm shift and will
include therapeutic options. Thus, the microscopic, gas-
filled, intravascular sphere that currently serves as a
‘‘stealth’’ agent has the potential to become an ideal
vehicle for delivering site-specific, drugs and/or genes to
the target organs. In fact, the ubiquitous presence of
angiogenesis in tumor growths provides an important
vascular conduit for the delivery of therapeutic
payloads.
The transformation of CEUS form a diagnostic
modality to a therapeutic option is created when in vivo
microspheres are acoustically disrupted via externally
applied acoustic energy resulting in a disruption of the
microspheres and subsequent, release of payload at a
target site. Based on published studies, which date to at
least 1995, Tochibana used ultrasound-directed therapy
for thrombolysis. More recently, the uses of CEUS
include site-specific delivery of drugs/genes.82-84
Thus, an entirely new field of non-viral, ultrasound-
mediated drug delivery appears to be unfolding. Leading
scientists throughout the world have successfully dem-
onstrated non-viral transduction through sonoporation in
a variety of pre-clinical scenarios. Clearly, the bur-
geoning scientific advancements in therapeutic options
are beyond the scope of this brief mention and command
future attention.
To imagine that the vascular conduits provide a
direct assess to tumor (or plaque) allows one’s imagi-
nation to speculate on the future of combined diagnostic
and therapeutic applications of CEUS. Stay tuned…
References
1. Gramiak R, Shah PM. Echocardiography of the aortic root. Invest
Radiol 1968;3:356-66.
2. Feinstein SB. The powerful microbubble: From bench to bedside,
from intravascular indicator to therapeutic delivery system, and
beyond. Am J Physiol Heart Circ Physiol 2004;287:H450-7.
3. Reale A, Pizzuto F, Gioffre PA, et al. Contrast echocardiography:
Transmission of echoes to the left heart across the pulmonary
vascular bed. Eur Heart J 1980;1:101-6.
4. Meltzer RS, Tickner EG, Popp RL. Why do the lungs clear
ultrasonic contrast? Ultrasound Med Biol 1980;6:263-9.
5. DeMaria AN, Bommer W, Takeda P, Mason DT, Kwan OL, Rasor
J. Value and limitations of contrast echocardiography in cardiac
diagnosis. J Cardiogr 1983;13:1-13.
6. DeMaria AN, Bommer W, Kwan OL, Riggs K, Smith M, Waters
J. In vivo correlation of thermodilution cardiac output and vid-
eodensitometric indicator-dilution curves obtained from contrast
two-dimensional echocardiograms. J Am Coll Cardiol 1984;3:999-
1004.
7. Kremkau FW, Gramiak R, Carstensen EL, Shah PM, Kramer DH.
Ultrasonic detection of cavitation at catheter tips. Am J Roent-
genol Radium Ther Nucl Med 1970;110:177-83.
8. Ziskin MC, Bonakdarpour A, Weinstein DP, Lynch PR. Contrast
agents for diagnostic ultrasound. Invest Radiol 1972;7:500-5.
9. Bove AA, Ziskin MC, Mulchin WL. Ultrasonic detection of in
vivo cavitation and pressure effects of high-speed injections
through catheters. Invest Radiol 1969;4:236-40.
10. Bommer WJ, Shah PM, Allen H, Meltzer R, Kisslo J. The safety of
contrast echocardiography: Report of the Committee on Contrast
Echocardiography for the American Society of Echocardiography.
J Am Coll Cardiol 1984;3:6-13.
11. Rubissow GJ, Mackay RS. Ultrasonic imaging of in vivo bubbles
in decompression sickness. Ultrasonics 1971;9:225-34.
12. Kort A, Kronzon I. Microbubble formation: In vitro and in vivo
observation. J Clin Ultrasound 1982;10:117-20.
13. Goldberg BB. Ultrasonic measurement of the aortic arch, right
pulmonary artery, and left atrium. Radiology 1971;101:383-90.
14. Armstrong WF, Mueller TM, Kinney EL, Tickner EG, Dillon JC,
Feigenbaum H. Assessment of myocardial perfusion abnormalities
with contrast-enhanced two-dimensional echocardiography.
Circulation 1982;66:166-73.
15. Tei C, Sakamaki T, Shah PM, et al. Myocardial contrast echocar-
diography: A reproducible technique of myocardial opacification
for identifying regional perfusion deficits. Circulation 1983;
67:585-93.
16. Feinstein SB, Ten Cate FJ, Zwehl W, et al. Two-dimensional
contrast echocardiography. I. In vitro development and
Figure 5. Contrast-enhanced, 3D vascular imaging. Thelumen of the carotid artery is opacified following theintravenous injection of an ultrasound contrast agent (white).Note that the luminal-intima interface is highlighted. Theadventitial vasa vasorum are highlighted at the level of carotidbulb (white arrows).
Journal of Nuclear Cardiology Feinstein et al 113
Volume 17, Number 1;106–15 Contrast enhanced ultrasound imaging
quantitative analysis of echo contrast agents. J Am Coll Cardiol
1984;3:14-20.
17. Powsner SM, Keller MW, Saniie J, Feinstein SB. Quantitation of
echo-contrast effects. Am J Physiol Imaging 1986;1:124-8.
18. Kaul S, Pandian NG, Okada RD, Pohost GM, Weyman AE.
Contrast echocardiography in acute myocardial ischemia: I. In
vivo determination of total left ventricular ‘‘area at risk’’. J Am
Coll Cardiol 1984;4:1272-82.
19. Porter TR, Pretlow R, D’Sa A, Nixon JV. In vitro study of the
effects of volume changes on parameters of the radiofrequency
amplitude versus time curve with sonicated albumin. J Am Soc
Echocardiogr 1993;6:564-9.
20. Kemper AJ, O’Boyle JE, Sharma S, et al. Hydrogen peroxide
contrast-enhanced two-dimensional echocardiography: Real-time
in vivo delineation of regional myocardial perfusion. Circulation
1983;68:603-11.
21. Zwehl W, Areeda J, Schwartz G, Feinstein S, Ong K, Meerbaum
S. Physical factors influencing quantitation of two-dimensional
contrast echo amplitudes. J Am Coll Cardiol 1984;4:157-64.
22. Ong K, Maurer G, Feinstein S, Zwehl W, Meerbaum S, Corday E.
Computer methods for myocardial contrast two-dimensional
echocardiography. J Am Coll Cardiol 1984;3:1212-8.
23. Meltzer RS, Tickner EG, Sahines TP, Popp RL. The source of
ultrasound contrast effect. J Clin Ultrasound 1980;8:121-7.
24. Ishihara K. Ultrasonic control of drug releasing. Jpn J Artificial
Organs 1984;13:1205-8.
25. Unger EC, Hersh E, Vannan M, Matsunaga TO, McCreery T.
Local drug and gene delivery through microbubbles. Prog Car-
diovasc Dis 2001;44:45-54.
26. Shohet RV, Chen S, Zhou YT, et al. Echocardiographic destruc-
tion of albumin microbubbles directs gene delivery to the
myocardium. Circulation 2000;101:2554-6.
27. Mulvagh SL, DeMaria AN, Feinstein SB, et al. Contrast echo-
cardiography: Current and future applications. J Am Soc
Echocardiogr 2000;13:331-42.
28. Mulvagh SL, Rakowski H, Vannan MA, et al. American Society of
Echocardiography Consensus Statement on the clinical applica-
tions of ultrasonic contrast agents in echocardiography. J Am Soc
Echocardiogr 2008;21:1179-201, quiz 1281.
29. Senior R, Becher H, Monaghan M, et al. Contrast echocardiog-
raphy: Evidence-based recommendations by European Association
of Echocardiography. Eur J Echocardiogr 2009;10:194-212.
30. Reilly JP, Tunick PA, Timmermans RJ, Stein B, Rosenzweig BP,
Kronzon I. Contrast echocardiography clarifies uninterpretable
wall motion in intensive care unit patients. J Am Coll Cardiol
2000;35:485-90.
31. Yong Y, Wu D, Fernandes V, et al. Diagnostic accuracy and cost-
effectiveness of contrast echocardiography on evaluation of car-
diac function in technically very difficult patients in the intensive
care unit. Am J Cardiol 2002;89:711-8.
32. Daniel C. Echocardiographic imaging of technically difficult
patients in the ICU. J Am Soc Echocardiogr 2001;14:917-20.
33. Anantharam B, Chahal N, Chelliah R, Ramzy I, Gani F, Senior R.
Safety of contrast in stress echocardiography in stable patients and
in patients with suspected acute coronary syndrome but negative
12-hour troponin. Am J Cardiol 2009;104:14-8.
34. Kurt M, Shaikh KA, Peterson L, et al. Impact of contrast echo-
cardiography on evaluation of ventricular function and clinical
management in a large prospective cohort. J Am Coll Cardiol
2009;53:802-10.
35. Mattrey RF, Kono Y. Contrast-specific imaging and potential
vascular applications. Eur Radiol 1999;9:S353-8.
36. Kono Y, Pinnell SP, Sirlin CB, et al. Carotid arteries: Contrast-
enhanced US angiography—preliminary clinical experience.
Radiology 2004;230:561-8.
37. Feinstein SB. Contrast ultrasound imaging of the carotid artery
vasa vasorum and atherosclerotic plaque neovascularization. J Am
Coll Cardiol 2006;48:236-43.
38. Coli S, Magnoni M, Sangiorgi G, et al. Contrast-enhanced ultra-
sound imaging of intraplaque neovascularization in carotid
arteries: Correlation with histology and plaque echogenicity. J Am
Coll Cardiol 2008;52:223-30.
39. Xiong L, Deng YB, Zhu Y, Liu YN, Bi XJ. Correlation of carotid
plaque neovascularization detected by using contrast-enhanced US
with clinical symptoms. Radiology 2009;251:583-9.
40. Folkman J. Tumor angiogenesis: Therapeutic implications. N Engl
J Med 1971;285:1182-6.
41. Chugh A, Patel SN, Rajaram V, Neems R, Feinstein M, Goldin M,
Feinstein SB. The clinical use of noninvasive modalities in the
assessment of atherosclerosis. In: Davidson M, Toth P, Maki K,
editors. Therapeutic lipidology, chap 18. Humana Press; 2007.
p. 389-408.
42. Coli S, Magnoni M, Meslisurgo G, Cianfione D, Feinstein SB.
Contrast ultrasound for vasa vasorum imaging: Can we improve
plaque risk stratification? In: Sangiorgi G, Homes D Jr, Rosenfield
K, Nelson Hopkins L, Spagnoli L, editors. Carotid atherosclerotic
disease: Pathologic basis for treatment, chap 15. Informa Health-
care; in press.
43. Coll B, Feinstein SB. Carotid intima-media thickness measure-
ments: Techniques and clinical relevance. Curr Atheroscler Rep
2008;10:444-50.
44. Granada JF, Feinstein SB. Imaging of the vasa vasorum. Nat Clin
Pract Cardiovasc Med 2008;5:S18-25.
45. Macioch JE, Katsamakis CD, Robin J, et al. Effect of contrast
enhancement on measurement of carotid artery intimal medial
thickness. Vasc Med 2004;9:7-12.
46. Pignoli P, Tremoli E, Poli A, Oreste P, Paoletti R. Intimal plus
medial thickness of the arterial wall: A direct measurement with
ultrasound imaging. Circulation 1986;74:1399-406.
47. Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Pre-
diction of clinical cardiovascular events with carotid intima-media
thickness: A systematic review and meta-analysis. Circulation
2007;115:459-67.
48. Pignoli P, Longo T. Ultrasound evaluation of atherosclerosis.
Methodological problems and technological developments. Eur
Surg Res 1986;18:238-53.
49. van Swijndregt ADM. An in vitro evaluation of the line pattern of
the near and far walls of carotid arteries using B-mode ultrasound.
Ultrasound Med Biol 1996;22:1007-15.
50. Swijndregt Mv. An in vivo evaluation of the reproducibility of
intima-media thickness: B-mode ultrasound. Ultrasound Med Biol
1999;25:323-30.
51. Patel SN, Rajaram V, Pandya S, et al. Emerging, noninvasive
surrogate markers of atherosclerosis. Curr Atheroscler Rep
2004;6:60-8.
52. Rajaram V, Pandhya S, Patel S, et al. Role of surrogate markers in
assessing patients with diabetes mellitus and the metabolic syn-
drome and in evaluating lipid-lowering therapy. Am J Cardiol
2004;93:32C-48C.
53. Wong M, Edelstein J, Wollman J, Bond MG. Ultrasonic-patho-
logical comparison of the human arterial wall. Verification of
intima-media thickness. Arterioscler Thromb 1993;13:482-6.
54. Stein JH, Korcarz CE, Hurst RT, et al. Use of carotid ultrasound to
identify subclinical vascular disease and evaluate cardiovascular
114 Feinstein et al Journal of Nuclear Cardiology
Contrast enhanced ultrasound imaging January/February 2010
disease risk: A consensus statement from the American Society of
Echocardiography Carotid Intima-Media Thickness Task Force.
Endorsed by the Society for Vascular Medicine. J Am Soc
Echocardiogr 2008;21:93-111, quiz 189-90.
55. Barger AC, Beeuwkes R 3rd, Lainey LL, Silverman KJ. Hypoth-
esis: Vasa vasorum and neovascularization of human coronary
arteries. A possible role in the pathophysiology of atherosclerosis.
N Engl J Med 1984;310:175-7.
56. Beeuwkes R, Barger C, Silverman K, Lainery LL. Cinemicro-
graphic studies of the vasa vasorum of the human coronary
arteries. In: Glagov S, Newman WP, Schaffer S, editors. Patho-
biology of the human atherosclerotic plaque. New York, NY:
Springer-Verlag; 1990. p. 425.
57. Clagett GP, Robinowitz M, Youkey JR, et al. Morphogenesis and
clinicopathologic characteristics of recurrent carotid disease.
J Vasc Surg 1986;3:10-23.
58. Dunmore BJ, McCarthy MJ, Naylor AR, Brindle NP. Carotid
plaque instability and ischemic symptoms are linked to immaturity
of microvessels within plaques. J Vasc Surg 2007;45:155-9.
59. Dvorak HF. Angiogenesis: Update 2005. J Thromb Haemost
2005;3:1835-42.
60. Fryer JA, Myers PC, Appleberg M. Carotid intraplaque hemor-
rhage: The significance of neovascularity. J Vasc Surg
1987;6:341-9.
61. Jeziorska M, Woolley DE. Neovascularization in early athero-
sclerotic lesions of human carotid arteries: Its potential
contribution to plaque development. Hum Pathol 1999;30:919-25.
62. Kerwin W, Hooker A, Spilker M, et al. Quantitative magnetic
resonance imaging analysis of neovasculature volume in carotid
atherosclerotic plaque. Circulation 2003;107:851-6.
63. Kerwin WS, Oikawa M, Yuan C, Jarvik GP, Hatsukami TS. MR
imaging of adventitial vasa vasorum in carotid atherosclerosis.
Magn Reson Med 2008;59:507-14.
64. Kolodgie FD, Gold HK, Burke AP, et al. Intraplaque hemorrhage
and progression of coronary atheroma. N Engl J Med
2003;349:2316-25.
65. Kumamoto M, Nakashima Y, Sueishi K. Intimal neovasculariza-
tion in human coronary atherosclerosis: Its origin and
pathophysiological significance. Hum Pathol 1995;26:450-6.
66. McCarthy MJ, Loftus IM, Thompson MM, et al. Angiogenesis and
the atherosclerotic carotid plaque: An association between symp-
tomatology and plaque morphology. J Vasc Surg 1999;30:261-8.
67. Mofidi R, Crotty TB, McCarthy P, Sheehan SJ, Mehigan D,
Keaveny TV. Association between plaque instability, angiogenesis
and symptomatic carotid occlusive disease. Br J Surg
2001;88:945-50.
68. Moreno PR, Purushothaman KR, Fuster V, et al. Plaque neovas-
cularization is increased in ruptured atherosclerotic lesions of
human aorta: Implications for plaque vulnerability. Circulation
2004;110:2032-8.
69. Moulton KS. Plaque angiogenesis and atherosclerosis. Curr Ath-
eroscler Rep 2001;3:225-33.
70. Vicenzini E, Giannoni MF, Puccinelli F, et al. Detection of carotid
adventitial vasa vasorum and plaque vascularization with
ultrasound cadence contrast pulse sequencing technique and echo-
contrast agent. Stroke 2007;38:2841-3.
71. Yamagishi M, Terashima M, Awano K, et al. Morphology of
vulnerable coronary plaque: Insights from follow-up of patients
examined by intravascular ultrasound before an acute coronary
syndrome. J Am Coll Cardiol 2000;35:106-11.
72. Sluimer JC, Kolodgie FD, Bijnens AP, et al. Thin-walled micro-
vessels in human coronary atherosclerotic plaques show
incomplete endothelial junctions relevance of compromised
structural integrity for intraplaque microvascular leakage. J Am
Coll Cardiol 2009;53:1517-27.
73. Sluimer JC, Gasc JM, van Wanroij JL, et al. Hypoxia, hypoxia-
inducible transcription factor, and macrophages in human ath-
erosclerotic plaques are correlated with intraplaque angiogenesis.
J Am Coll Cardiol 2008;51:1258-65.
74. Sluimer JC, Gasc JM, Hamming I, et al. Angiotensin-converting
enzyme 2 (ACE2) expression and activity in human carotid ath-
erosclerotic lesions. J Pathol 2008;215:273-9.
75. Fleiner M, Kummer M, Mirlacher M, et al. Arterial neovascular-
ization and inflammation in vulnerable patients: Early and late
signs of symptomatic atherosclerosis. Circulation 2004;110:2843-
50.
76. Moreno PR, Fuster V. The year in atherothrombosis. J Am Coll
Cardiol 2004;44:2099-110.
77. Mauriello A, Sangiorgi G, Fratoni S, et al. Diffuse and active
inflammation occurs in both vulnerable and stable plaques of the
entire coronary tree: A histopathologic study of patients dying of
acute myocardial infarction. J Am Coll Cardiol 2005;45:1585-93.
78. Williams JK, Sukhova GK, Herrington DM, Libby P. Pravastatin
has cholesterol-lowering independent effects on the artery wall of
atherosclerotic monkeys. J Am Coll Cardiol 1998;31:684-91.
79. Wilson SH, Herrmann J, Lerman LO, et al. Simvastatin preserves
the structure of coronary adventitial vasa vasorum in experimental
hypercholesterolemia independent of lipid lowering. Circulation
2002;105:415-8.
80. Moulton KS, Vakili K, Zurakowski D, et al. Inhibition of plaque
neovascularization reduces macrophage accumulation and pro-
gression of advanced atherosclerosis. Proc Natl Acad Sci USA
2003;100:4736-41.
81. Shah F, Balan P, Weinberg M, et al. Contrast-enhanced ultrasound
imaging of atherosclerotic carotid plaque neovascularization: A
new surrogate marker of atherosclerosis? Vasc Med 2007;12:
291-7.
82. Tachibana K, Tachibana S. Albumin microbubble echo-contrast
material as an enhancer for ultrasound accelerated thrombolysis.
Circulation 1995;92:1148-50.
83. Li T, Tachibana K, Kuroki M, Kuroki M. Gene transfer with echo-
enhanced contrast agents: Comparison between Albunex, Optison,
and Levovist in mice—initial results. Radiology 2003;229:423-8.
84. Duvshani-Eshet M, Adam D, Machluf M. The effects of albumin-
coated microbubbles in DNA delivery mediated by therapeutic
ultrasound. J Control Release 2006;112(2):156-66.
Journal of Nuclear Cardiology Feinstein et al 115
Volume 17, Number 1;106–15 Contrast enhanced ultrasound imaging
Related Documents











