c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489 j o ur nal homep age : w ww.intl.elsevierhealth.com/journals/cmpb Computer-aided optimal design of custom scoliosis braces considering clinical and patient evaluations Daniel Visser a , Deyi Xue a,∗ , Janet L. Ronsky a , James Harder b,c , Ronald F. Zernicke a,c a Department of Mechanical and Manufacturing Engineering, University of Calgary, 2500 University Drive N.W., Calgary, AB, Canada T2N 1N4 b Department of Orthopaedic Surgery, Alberta Children’s Hospital, Calgary, AB, Canada c Department of Surgery, University of Calgary, Calgary, AB, Canada a r t i c l e i n f o Article history: Received 17 March 2009 Received in revised form 4 July 2010 Accepted 29 December 2010 Keywords: Scoliosis Brace CAD CAM Multi-objective optimization a b s t r a c t Scoliosis causes an abnormal three dimensional curvature of the spine that is often treated by an orthotic device called brace. The objective of this research was to develop a new approach to automatically identify the optimal design of custom-built brace, based on clin- ical and patient evaluations. In this approach, torso geometry of the scoliosis patient was achieved using a 3-D imaging system that generated a 3-D torso surface model, which was modified using a custom CAD system to design the 3-D brace surface model. Two design parameters, a translational correction factor and a rotational correction factor, were selected to design the brace geometry from the torso geometry. The 3-D digital brace was evalu- ated by three clinical evaluation measures (imbalance, rib hump and principal axis angle reduction) and one patient evaluation measure (discomfort). A multi-objective optimization method was employed to identify the optimal design parameters considering both clinical and patient evaluations. © 2011 Elsevier Ireland Ltd. All rights reserved. 1. Introduction 1.1. Scoliosis and scoliosis braces Scoliosis is a condition with abnormal 3-dimensional curva- ture of the spine (Fig. 1(a)). The most common form of scoliosis, adolescent idiopathic scoliosis (AIS), frequently presents dur- ing the adolescent growth spurt. The rapid growth during this time period may cause imbalance in the spine, and the curve usually develops quickly. The severity of scoliosis is traditionally recorded with a pla- nar clinical measure called the Cobb angle (Fig. 1(a)). For a mild case (Cobb angle <25 ◦ ), the curve is monitored with biannual X-rays without other treatment. If the curve progresses to a moderate level (Cobb angle: 25–40 ◦ ), the patient is treated with ∗ Corresponding author. Tel.: +1 403 220 4168. E-mail address: [email protected] (D. Xue). an orthotic brace. If brace treatment is not effective and the curve progresses to a severe level (Cobb angle >40 ◦ ), surgery is required to arrest or minimize the curve progression. Among various scoliosis treatment braces, the Boston brace (Fig. 1(b)) is the most popular. The Boston brace uses a prefabri- cated module to apply transverse loads to the patient’s torso to reduce the curvature. The prefabricated standard brace mod- ule is ordered from a manufacturing company based on a series of measurements from the patient. The relief areas of the brace module are removed, and comfort pads are added inside the brace. The mass-produced standard braces fit only 70% of the scoliosis patients. For the scoliosis patients who cannot use the standard braces, custom-built braces have to be manu- factured to satisfy their special needs. Current methods for producing custom-built braces depend on extensive manual 0169-2607/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.cmpb.2010.12.017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489
j o ur nal homep age : w ww.int l .e lsev ierhea l th .com/ journa ls /cmpb
Computer-aided optimal design of custom scoliosis bracesconsidering clinical and patient evaluations
Daniel Vissera, Deyi Xuea,∗, Janet L. Ronskya, James Harderb,c, Ronald F. Zernickea,c
a Department of Mechanical and Manufacturing Engineering, University of Calgary, 2500 University Drive N.W., Calgary, AB, CanadaT2N 1N4b Department of Orthopaedic Surgery, Alberta Children’s Hospital, Calgary, AB, Canadac Department of Surgery, University of Calgary, Calgary, AB, Canada
a r t i c l e i n f o
Article history:
Received 17 March 2009
Received in revised form 4 July 2010
Accepted 29 December 2010
Keywords:
Scoliosis
Brace
a b s t r a c t
Scoliosis causes an abnormal three dimensional curvature of the spine that is often treated
by an orthotic device called brace. The objective of this research was to develop a new
approach to automatically identify the optimal design of custom-built brace, based on clin-
ical and patient evaluations. In this approach, torso geometry of the scoliosis patient was
achieved using a 3-D imaging system that generated a 3-D torso surface model, which was
modified using a custom CAD system to design the 3-D brace surface model. Two design
parameters, a translational correction factor and a rotational correction factor, were selected
to design the brace geometry from the torso geometry. The 3-D digital brace was evalu-
CAD
CAM
Multi-objective optimization
ated by three clinical evaluation measures (imbalance, rib hump and principal axis angle
reduction) and one patient evaluation measure (discomfort). A multi-objective optimization
method was employed to identify the optimal design parameters considering both clinical
and patient evaluations.
scoliosis patients. For the scoliosis patients who cannot use
1. Introduction
1.1. Scoliosis and scoliosis braces
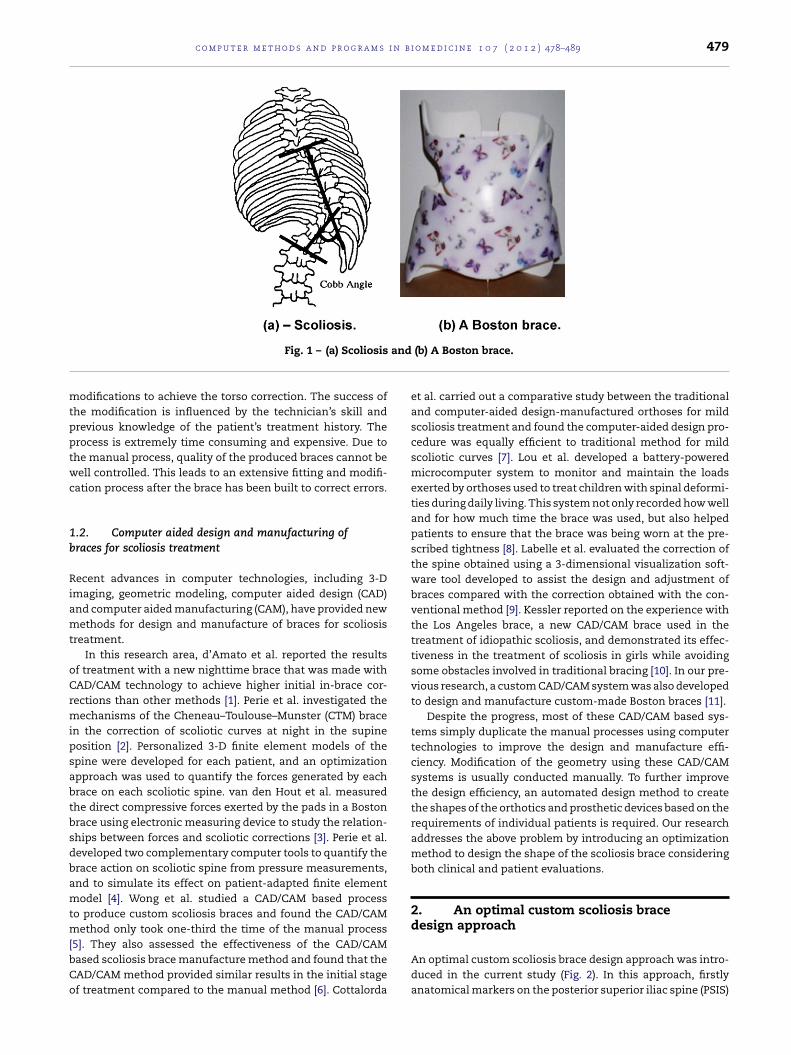
Scoliosis is a condition with abnormal 3-dimensional curva-ture of the spine (Fig. 1(a)). The most common form of scoliosis,adolescent idiopathic scoliosis (AIS), frequently presents dur-ing the adolescent growth spurt. The rapid growth during thistime period may cause imbalance in the spine, and the curveusually develops quickly.
The severity of scoliosis is traditionally recorded with a pla-nar clinical measure called the Cobb angle (Fig. 1(a)). For a mild
◦
case (Cobb angle <25 ), the curve is monitored with biannualX-rays without other treatment. If the curve progresses to amoderate level (Cobb angle: 25–40◦), the patient is treated with∗ Corresponding author. Tel.: +1 403 220 4168.E-mail address: [email protected] (D. Xue).
0169-2607/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights resdoi:10.1016/j.cmpb.2010.12.017
© 2011 Elsevier Ireland Ltd. All rights reserved.
an orthotic brace. If brace treatment is not effective and thecurve progresses to a severe level (Cobb angle >40◦), surgery isrequired to arrest or minimize the curve progression.
Among various scoliosis treatment braces, the Boston brace(Fig. 1(b)) is the most popular. The Boston brace uses a prefabri-cated module to apply transverse loads to the patient’s torso toreduce the curvature. The prefabricated standard brace mod-ule is ordered from a manufacturing company based on aseries of measurements from the patient. The relief areas ofthe brace module are removed, and comfort pads are addedinside the brace.
The mass-produced standard braces fit only 70% of the
the standard braces, custom-built braces have to be manu-factured to satisfy their special needs. Current methods forproducing custom-built braces depend on extensive manual
erved.
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489 479
and
mtpptwc
1b
Riamt
oCrmipsabtbsdbamtm[bCo
Fig. 1 – (a) Scoliosis
odifications to achieve the torso correction. The success ofhe modification is influenced by the technician’s skill andrevious knowledge of the patient’s treatment history. Therocess is extremely time consuming and expensive. Due tohe manual process, quality of the produced braces cannot beell controlled. This leads to an extensive fitting and modifi-
ation process after the brace has been built to correct errors.
.2. Computer aided design and manufacturing ofraces for scoliosis treatment
ecent advances in computer technologies, including 3-Dmaging, geometric modeling, computer aided design (CAD)nd computer aided manufacturing (CAM), have provided newethods for design and manufacture of braces for scoliosis
reatment.In this research area, d’Amato et al. reported the results
f treatment with a new nighttime brace that was made withAD/CAM technology to achieve higher initial in-brace cor-ections than other methods [1]. Perie et al. investigated the
echanisms of the Cheneau–Toulouse–Munster (CTM) bracen the correction of scoliotic curves at night in the supineosition [2]. Personalized 3-D finite element models of thepine were developed for each patient, and an optimizationpproach was used to quantify the forces generated by eachrace on each scoliotic spine. van den Hout et al. measuredhe direct compressive forces exerted by the pads in a Bostonrace using electronic measuring device to study the relation-hips between forces and scoliotic corrections [3]. Perie et al.eveloped two complementary computer tools to quantify therace action on scoliotic spine from pressure measurements,nd to simulate its effect on patient-adapted finite elementodel [4]. Wong et al. studied a CAD/CAM based process
o produce custom scoliosis braces and found the CAD/CAMethod only took one-third the time of the manual process
5]. They also assessed the effectiveness of the CAD/CAMased scoliosis brace manufacture method and found that theAD/CAM method provided similar results in the initial stagef treatment compared to the manual method [6]. Cottalorda
(b) A Boston brace.
et al. carried out a comparative study between the traditionaland computer-aided design-manufactured orthoses for mildscoliosis treatment and found the computer-aided design pro-cedure was equally efficient to traditional method for mildscoliotic curves [7]. Lou et al. developed a battery-poweredmicrocomputer system to monitor and maintain the loadsexerted by orthoses used to treat children with spinal deformi-ties during daily living. This system not only recorded how welland for how much time the brace was used, but also helpedpatients to ensure that the brace was being worn at the pre-scribed tightness [8]. Labelle et al. evaluated the correction ofthe spine obtained using a 3-dimensional visualization soft-ware tool developed to assist the design and adjustment ofbraces compared with the correction obtained with the con-ventional method [9]. Kessler reported on the experience withthe Los Angeles brace, a new CAD/CAM brace used in thetreatment of idiopathic scoliosis, and demonstrated its effec-tiveness in the treatment of scoliosis in girls while avoidingsome obstacles involved in traditional bracing [10]. In our pre-vious research, a custom CAD/CAM system was also developedto design and manufacture custom-made Boston braces [11].
Despite the progress, most of these CAD/CAM based sys-tems simply duplicate the manual processes using computertechnologies to improve the design and manufacture effi-ciency. Modification of the geometry using these CAD/CAMsystems is usually conducted manually. To further improvethe design efficiency, an automated design method to createthe shapes of the orthotics and prosthetic devices based on therequirements of individual patients is required. Our researchaddresses the above problem by introducing an optimizationmethod to design the shape of the scoliosis brace consideringboth clinical and patient evaluations.
2. An optimal custom scoliosis bracedesign approach
An optimal custom scoliosis brace design approach was intro-duced in the current study (Fig. 2). In this approach, firstlyanatomical markers on the posterior superior iliac spine (PSIS)

480 c o m p u t e r m e t h o d s a n d p r o g r a m s i n
Scoliosis Patient
3-D Torso
3-D Imaging
3-D Brace
Design Modification (T,R)
Rib Hump:
E2 (T,R)
Imbalance:
E1 (T,R)
Principal Axis Angle
Reduction: E3 (T,R)
Discomfort:
E4 (T,R)
Index:
I2 (T,R)
Index:
I1 (T,R)
Index:
I3 (T,R)
Index:
I4 (T,R)
Overall Evaluation Index: I(T,R)
Scoliosis Brace
Brace Patient Fitting
Clinical Evaluation Patient Evaluation
Brace Fabrication
Fig. 2 – An optimal custom scoliosis brace design approach.
toward the center of the pelvic section. The rotation aroundthe center of mass was used to align the principal axis towardthe reference PSIS axis. The ideal center of mass and the ideal
of the scoliosis patient were used to provide a reference coordi-nate system. The 3-D torso surface of a scoliosis patient wasachieved using a 3-D imaging system. The 3-D geometry ofthe torso was sectioned into many layers, and each layer wasmodeled by a 2-D profile. Due to the dark color of the pos-terior superior iliac spine (PSIS) markers, locations of thesemarkers in the 3-D geometric model were also modeled usingdark intensity values. For each 2-D profile, the actual center ofmass and the actual principal axis were calculated from the2-D geometry. The ideal center of mass and the ideal principalaxis of the 2-D section were obtained from the PSIS markers.By translating and rotating the 2-D section, the actual centerof mass and the actual principal axis were aligned to the idealcenter of mass and the ideal principal axis. Different sectionsrequired different translational and rotational measures forthe alignment.
Mapping from the 3-D geometry of torso to the 3-D geom-etry of brace was accomplished by changing values of twodesign variables: translational correction factor, T, and rota-tional correction factor, R. These two design variables weredescribed by percentage measures representing the degreesof corrections by translation and rotation. These two designvariables were applied to each of the 2-D sections to modifythe 2-D torso profile to create the 2-D brace profile.
The 3-D brace geometry, modeled by layers of 2-D profiles,was subsequently evaluated. In this research, three clinicalevaluation measures (i.e., imbalance, rib hump and principalaxis angle reduction) and one patient evaluation measure (i.e.,discomfort) were used to evaluate the 3-D brace shape. Sincethese evaluation measures were modeled by different units,the measures were converted into comparable evaluationindices representing degrees of satisfaction in the relevant
evaluation aspects. The overall evaluation index was achievedfrom the four individual evaluation indices and weighting fac-tors of these evaluation indices.b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489
When the evaluation criteria were satisfied, the 3-D bracegeometry was used to fabricate the brace. Otherwise furthermodification of the two design variables was required. In thisresearch, the optimization approach was employed by select-ing the translation and rotation correction factors as designvariables and the overall evaluation index as the objectivefunction. Change of the two design variables was conductedcontinuously until no further improvement of the overall eval-uation index was achieved.
Details on modeling of custom scoliosis braces, evaluationof scoliosis braces, and optimal design of scoliosis braces areintroduced in Sections 3, 4 and 5, respectively.
3. Modeling of custom scoliosis braces
Anatomical markers on the posterior superior iliac spine (PSIS)of the scoliosis patient were used to provide a reference coordi-nate system. The 3-D torso geometry and texture informationof the scoliosis patient were quantified using an INSPECK 3-Dimaging system (InSpeck Inc., Montreal, Canada). The tex-ture information was used to identify the markers placedon the torso surface. The geometric information was con-verted into a cloud of data points with XYZ coordinates. Acustom CAD system was developed using MATLAB to modelthe 3-D geometry. This system was used to sort data cloudsinto multiple layers with each layer containing 360 points(Fig. 3). PSIS markers were modeled using different intensityvalues.
The torso correction was based on the current practice ofshaping the brace to realign the center and orientation of thetorso over the center and orientation of the pelvis. This mod-ification stabilized the spine by reducing the eccentricity ofthe mass center in each section. Two types of operations werecarried out for the correction of a torso shape (Fig. 4). Thetranslation of the section was used to align the center of mass
Fig. 3 – 3-D geometry with many layers of 2-D profiles.

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i
(a) – Translation modification.
Center of Mass
for the Section Reference Center
of Mass from the
Pelvis Section V: Translation
Vector
Original Profile Modified Profile
: Rotation
Angle
Principal Axis
PSIS Axis
(b) – Rotation modification.
Center of Mass
for the Section
Original Profile
Modified Profile
pm
3
Oectttmtgp
TihtsST(in
⎡⎣
were originally developed to predict the Cobb angle using a
Fig. 4 – (a) Translation and (b) rotation modifications.
rincipal axis at the pelvis section were obtained from the PSISarkers.
.1. Translational modification
ne of the main goals for brace treatment is to reduce theccentricity of the spinal column. That was achieved, in theurrent study, using a brace to translate the torso section inhe medial-lateral direction to align the mass center of the sec-ion toward the pelvic center. Existing methods for obtaininghis correction were based on hand measurement and esti-
ation of the pelvic center to derive the required amounts oforso translation in different positions. In our approach, a 3-Deometric model was used to obtain the precise translationarameters in different sections.
Firstly, the center of mass was obtained for the 2-D section.he area centroid was used as the center of mass by assum-
ng that the differences in tissue densities and distributionsad no influence on the calculation of the mass center. Theranslation vector was obtained from the mass center of theection and the mass center of the pelvic section (Fig. 4(a)).uppose the translation vector was described as (Vx,Vy), and
was the translation correction factor in unit of percentage0% for no translation, and 100% for full translation), a pointn the original torso profile, P = (X,Y), was then translated to aew point on the brace profile, P′ = (X′,Y′), using
⎤ ⎡ ⎤ ⎡ ⎤
X′Y′
1
⎦ = ⎣1 0 TVx
0 1 TVy
0 0 1
⎦ ⎣X
Y
1
⎦ , 0% ≤ T ≤ 100% (1)
o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489 481
Since 2-D profiles in different sections were different, thetranslation vectors for different sections were usually differ-ent.
3.2. Rotational modification
The rotation of the torso was used to align the actual principalaxis of the 2-D section toward the ideal principal axis definedby PSIS markers. Firstly, the principal axis was obtained basedon the moment of inertia (Fig. 4(b)). That principal axis wascompared with the PSIS axis to obtain the rotation angle �.Suppose R was the rotation correction factor in unit of per-centage (0% for no rotation, and 100% for full rotation), a pointin the original torso profile, P = (X,Y), was rotated to a new pointon the brace profile, P′ = (X′,Y′), using
⎡⎣
X′
Y′
1
⎤⎦ =
⎡⎣
cos(R�) − sin(R�) 0sin(R�) cos(R�) 00 0 1
⎤⎦
⎡⎣
X
Y
1
⎤⎦ , 0% ≤ R ≤ 100% (2)
Since 2-D profiles in different sections were different, the rota-tion angles for different sections were usually different.
4. Evaluation of patient-specific customscoliosis braces
Braces are intended to correct the abnormal spinal curvatureand to prevent further progression of the curvature. Evaluationof the brace is usually conducted by a comparison betweenX-rays of the patient with and without the brace [12]. Thebrace treatment has good potential to stop the curve pro-gression if the Cobb angle is reduced considerably when thebrace is worn. The in-brace X-ray is an adequate method todemonstrate how the brace reduces the curvature in the coro-nal plane. However it does not evaluate the 3-D nature of thecorrection. Since scoliosis is a disease with abnormal 3-D cur-vatures of the spine, evaluation based on a single plane doesnot provide sufficient information to accurately describe thebrace correction effectiveness.
The second major requirement for successful brace treat-ment is high brace-wear compliance. This factor is stronglydependent on the patient’s comfort when wearing a brace.Most brace evaluation methods have considered comfort asecondary goal. Neglecting patient comfort during brace eval-uation has resulted in poor compliance to brace treatment.Development of measures to evaluate patient comfort isessential for providing a well fitting brace that will be wornappropriately.
4.1. Clinical evaluation measures
Three clinical evaluation measures: imbalance, rib hump, andprincipal axis angle reduction (Fig. 5) were introduced to eval-uate the effectiveness of the scoliosis brace. These measures
neural network, which was trained to model the relationsbetween these geometric measures and the Cobb angle basedon the collected clinical data, to avoid the use of X-ray [13].

482 c o m p u t e r m e t h o d s a n d p r o g r a m s i n
Fig. 5 – Three clinical evaluation measures: (a) imbalance ofleft side and right side about the PSIS axis, (b) rib hump
(Pedar-X, NOVEL Technologies, Germany) with arrays of pres-
area, and (c) reduction of principal axis angle.
(i) ImbalanceImbalance evaluated the amount of lateral asymmetry ofthe spinal shape. Suppose the areas at the left side and theright side of the PSIS center axis for the i-th 2-D sectionwere obtained as ALHS,i and ARHS,i (Fig. 5(a)), the imbalanceof the i-th 2-D section was then calculated by
E1,i = |ALHS,i − ARHS,i|ALHS,i + ARHS,i
× 100% (3)
The imbalance considering all the n 2-D sections wasachieved by
E1 = 1n
n∑i=1
E1,i (4)
For the ideal spine, there would be no spinal imbalance.So the ultimate goal of correction (perfect correction) forthe scoliosis patient was to reduce the spinal imbalanceto zero. The spinal imbalance measure was reduced byboth translation and rotation of the section points.
(ii) Rib HumpOne of the major considerations in scoliosis treatment isto reduce the visible deformity of the torso. In many cases,
the most noticeable deformity is known as rib hump(Fig. 5(b)), a deformity caused by torsion and imbalancedgrowth of the ribcage.b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489
To achieve the rib hump evaluation measure, firstly a cut-ting plane was created parallel to the PSIS reference planefor the i-th 2-D section. The cutting plane was positionedat the point closest to the torso profile at the oppositeside of the rib hump. The area above the cutting line wasdefined as the rib hump area, Arib-hump,i. The rib-humpevaluation measure for the i-th 2-D section was calculatedby
E2,i = Arib-hump,i
ALHS,i + ARHS,i× 100% (5)
The rib hump considering all the n 2-D sections was quan-tified by
E2 = 1n
n∑i=1
E2,i (6)
The goal of the correction was to minimize the rib humpmeasurement. Since the rib hump was dependent on thetorso section orientation relative to the PSIS referenceaxis, this measure was strongly influenced by the rota-tional correction parameter.
(iii) Principal Axis Angle ReductionThe rotational spinal deformity in scoliosis can be mea-sured by calculating the principal axis angle of each 2-Dsection (Fig. 5(c)). Suppose for the i-th 2-D section, theinitial principal axis angle before the modification wasdescribed by �initial,i, and the final principal axis angleafter the modification was described by �final,i, then theprincipal axis angle reduction for the i-th 2-D section wasmodeled by:
E3,i = �final,i
�initial,i× 100% (7)
The principal axis angle reduction considering all the n2-D sections was achieved by
E3 = 1n
n∑i=1
E3,i (8)
4.2. Patient evaluation measures
The discomfort was used to evaluate the scoliosis brace fromperspective of patient. Measuring discomfort or pain was dif-ficult due to the subjective nature of discomfort or pain. TheVisual Analog Scale (VAS) [14] was used in the current studyto measure the personal discomfort. The VAS method used aline with two ends labeled as “no discomfort” and “severe dis-comfort” (Fig. 6). The patient was asked to place a mark on theVAS to rate the discomfort. The VAS method has been provento be effective and valid for rating pain and discomfort [14].
The discomfort measures of the patient were directly influ-enced by the levels of interface pressures at different locationsof the torso. In the current study, a pressure acquisition system
sure sensors quantified pressure data at different locations.Since the discomfort evaluation measure must be predictedbefore the brace was actually fabricated, the discomfort eval-

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489 483
Fig. 6 – A sample discomfort survey page.
uofpitda
p
ation measure was obtained based on the geometric shapesf the brace and torso. Here, the relation between the discom-ort and the displacement the torso moved from its normalosition to the braced position was first studied. Since scol-
osis braces have specific design goals for different regions ofhe torso, three key design regions were selected to study theisplacement–discomfort relations. These three areas were:
bdomen, ribcage, and lumbar areas (Fig. 6).In each of these key areas, displacement pads (Fig. 7) werelaced on the torso, and the brace was put on. A displacement
Table 1 – A sample data set collected by discomfort survey.
Location Pad
Standing
Max.pressure(N/cm2)
Ave.pressure(N/cm2)
Disco(1–10)
Abdomen 0 mm 1 0.0582 0.8
10 mm 1 0.1496 2.2
20 mm 1 0.3081 3.9
30 mm 1 0.3033 6.5
Ribcage 0 mm 2 0.5387 0.2
10 mm 2 0.8419 1.5
20 mm 3 1.7626 4.5
30 mm 5 2.3283 8.9
Lumbar 0 mm 1 0.1419 1.7
10 mm 3 0.7871 2.5
20 mm 2 1.3748 3.7
30 mm 3 0.7032 8.9
pad was shaped to fit each of the key areas. The displace-ment pads had different heights of 10 mm, 20 mm, or 30 mmand were used to obtain the discomfort measures at differentlocations.
After each pad was placed on the torso, the brace was fit andtightened appropriately. The subject was asked to complete acomfort evaluation, and pressure data were recorded for each
of the instrumented locations. The subject was required tocomplete the evaluation for two postures: sitting and stand-ing. The discomfort survey was composed of torso picturesPosture
Sitting
mfort Max.pressure(N/cm2)
Ave.pressure(N/cm2)
Discomfort(1–10)
1 0.0775 1.81 0.1909 2.81 0.2733 4.31 0.2901 7.32 0.7326 1.42 1.0713 1.83 1.4871 3.85 1.9526 8.23 0.7561 1.52 0.5806 2.22 1.24 4.83 0.7954 8.1

484 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489
Fig. 7 – Different displacement pads used in different locations.
from four views with the identified key areas and the VAS dis-comfort scale for each of the areas (Fig. 6). The patient wasrequired to mark the VAS to rate the discomfort in each ofthe three key areas for each of the two postures with each ofthe three pad thicknesses. The discomfort was measured bya value between 0 (no discomfort) and 10 (severe discomfort)(Table 1).
Once the displacement and discomfort data were collected,those data were used to generate displacement–discomfortrelations (e.g., displacement–discomfort relations for theabdomen region considering standing and sitting postures asshown in Fig. 8).
The discomfort measure of the 3-D brace was achieved bythe displacements from the torso to the brace in the selectedthree key regions. Firstly, markers were placed in the keyregions of the patient torso, and those markers were scannedinto a custom CAD system. For each region, the displacementwas obtained from the original torso shape and the braceshape that represented the modified torso shape. The discom-fort measure was calculated from the displacement measureusing the displacement–discomfort relation through function
interpolation.When the discomfort measures for the i-th region consider-ing standing and sitting postures were predicted as Di,standing
0
1
2
3
4
5
6
7
8
100 20 30 40
Displacement (mm)
Dis
com
fort
(0-
10)
Standing
Sittin g
Fig. 8 – Displacement–discomfort relation for abdomenarea.
and Di,sitting from the 3-D model, the discomfort measure forthe i-th region was then calculated by
Di = Di,standing + Di,sitting
2(9)
The overall discomfort measure considering all the 3 keyregions was achieved by
E4 = Dabdomen + Dribcage + Dlumbar
3(10)
5. Optimal design of custom scoliosisbraces
The optimization method was incorporated into the process ofscoliosis brace design once techniques to evaluate the digitalbrace shape were developed. Optimization used evaluation ofthe brace shape as feedback to determine the values of designvariables. Optimization for scoliosis brace design was basedon evaluation of the digital brace shape rather than the actualmanufactured scoliosis brace.
The first step to implement the optimization method forbrace design was to select the design variables. Two correctionfactors – translation correction factor T and rotation correctionfactor R – were selected as the design variables.
D = (T, R), 0% ≤ T, R ≤ 100% (11)
For each 2-D section of the digital torso, the maximal trans-lational correction vector was achieved as (Vx,i,Vy,i), and themaximal rotational angle was obtained as �i using the meth-ods introduced previously in Section 3. Eqs. (1) and (2) wereused to modify the coordinates of the points on the 2-D profileof the torso to create the 2-D profile of the brace. The 3-D bracegeometry was created by modifying all 2-D profiles of the torsoshape. An example is provided (Fig. 9) to show actual transla-
tional and rotational modifications for different sections withthe same design variables of T and R.The 3-D brace geometry was evaluated using the previouslyintroduced four evaluation measures, which were modeled as

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489 485
d ro
f
(
(
cmtmw
Fig. 9 – Translational an
unctions of the two design variables.
1) Clinical evaluation measures:• Imbalance: E1(T,R)• Rib hump: E2(T,R)• Principal axis angle reduction: E3(T,R)
2) Patient evaluation measure:• Discomfort: E4(T,R)
One goal of scoliosis treatment is to provide substantialurve correction, but that can result in high torso displace-
ents and high discomfort levels. The discomfort can leado reduced brace compliance and negatively influence treat-ent effectiveness. Therefore the goal of this optimizationas to achieve the maximal amount of correction while keep-
0
0.2
0.4
0.6
0.8
1
50 10 15 20
0
0.2
0.4
0.6
0.8
1
0 20 40 60 100 80
Imbalance (%)
Sat
isfa
ctio
n
Imbalance - Satisfaction
Principal Axis Angle Reduction - Satisfaction
Principal Axis Angle Reduction (%)
Sat
isfa
ctio
n
Fig. 10 – Relations between evaluation
tational modifications.
ing patient discomfort to the minimum. The optimizationconsidering multiple and sometimes opposing objectives iscalled multi-objective optimization [15].
Presently many methods have been developed to solvemulti-objective optimization problems [15]. These methodsare primarily classified into three categories [16]. The methodsin the first category convert a multi-objective optimiza-tion problem into a single-objective optimization problemby assigning weights, preferences, or utilities to the differ-ent objective functions. The methods in the second categoryare used to first identify the multiple Pareto set points (i.e.,
the optimal solutions) and then allow the decision mak-ers to select one based upon their selection criteria. Themethods in the third category try to model each singleobjective function and then explore the Pareto optimal fron-0
0.2
0.4
0.6
0.8
1
0 0.05 0.1 0.15 0.2 0.2 5 0.3
0
0.2
0.4
0.6
0.8
1
6420 8
Rib Hump (%)
Sat
isfa
ctio
n
Sat
isfa
ctio
n
Discomfort - Satisfaction
Discomfort
Rib Hump - Satisfaction
measures and evaluation indices.

486 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489
Fig. 11 – Optimization considering two design variables.
tier using surrogate models or directly approximating thePareto optimal functions. In this research, the approachto convert the multi-objective optimization problem into asingle-objective optimization problem is employed due to itssimplicity and uniqueness to obtain the optimization solu-tion.
Since different evaluation measures in multi-objectiveoptimization are usually modeled in different units (e.g.,efficiency and cost), these individual evaluation measuresmust be converted into comparable evaluation measuresfirst. Here, the method for modeling the non-linear relationbetween an evaluation measure and its satisfaction indexintroduced in [17] was employed to convert all the evalua-tion measures into evaluation indices (Fig. 10). A least squarecurve-fitting method was used to obtain the non-linear rela-tions.
Suppose the evaluation indices of imbalance, rib hump,
principal axis angle reduction, and discomfort were describedas I1(T,R), I2(T,R), I3(T,R), and I4(T,R), and the weighting fac-tors representing the importance of these evaluation aspectsFig. 12 – Major manufacturing processes: (a) CNC machi
were modeled by W1, W2, W3, and W4, then the optimizationobjective function, I(T,R), was defined by
I(T, R) =∑4
i=1[WiIi(T, R)]∑4i=1Wi
(12)
The optimization problem was modeled as
Maxw.r.t. T,R
I(T, R)
subject to :0% ≤ T ≤ 100%0% ≤ R ≤ 100%
(13)
6. Case study and discussion
6.1. Case study
A test subject (15-year old scoliosis patient), who had diffi-culty time to find a right brace, volunteered for the study. The
ning of brace die, (b) blank area, and (c) final brace.

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489 487
Table 2 – Evaluation measures and evaluation indices.
Evaluationaspect
Evaluationmeasure
Evaluationindex
Imbalance 5.07% 0.95Rib hump 0.076% 0.43Principal axis
anglededuction
0.5% 1.0
Discomfort 2.0 0.80Overall 0.8017
sv2
IiLearmitso
oa
bTsp
Table 3 – Different optimal designs with different designobjectives.
Design Design 1 Design 2 Design 3
Weightingfactors
W1 0.5 1.0 0.1W2 0.6 1.0 0.1W3 0.5 1.0 0.1W4 0.9 0.1 1.0
Design T 65% 100% 0%
evaluationindex
ubject had a predominately right thoracic curve through theertebrae range, T5-T11, with a Cobb angle measurement of8.5◦.
The surface data of the subject were quantified using theNSPECK 3-D imaging system, and those geometric data weremported into the custom CAD system developed using MAT-AB. The 26,640 points were further sorted into 74 sectionsach containing 360 points. The locations of the markers werelso obtained using the 3-D imaging system to identify theeference coordinate system, PSIS axes, and key areas for esti-
ating the patient discomfort measures. Then, 1303 pointsn the abdomen, ribcage, and lumbar areas were selected torack the displacements from their original positions on theurface of the torso to the modified positions on the surfacef the brace.
The weighting factors of the four evaluation indices in theptimization objective function given in Eq. (12) were selecteds:
W1 = 0.5W2 = 0.6W3 = 0.5W4 = 0.9
ased on experience of the orthotist in scoliosis brace design.hese weighting factors are then entered into the custom CADystem. By optimization using Eq. (13), the optimal designarameters were achieved as (Fig. 11):
T = 65%R = 55%
Table 4 – Comparison between two brace construction methods
Phases Manual procedure
Procedure T
Torso acquisition Patient casting 3Torso replica molding 2
Torso modification Brace shape design 0Cast correction 4
Die fabrication
Brace construction Thermo forming 3Trimming 1
Fitting Brace adjustment 4Total 17
result R 55% 55% 0%
The corresponding evaluation measures and evaluationindices for the optimal design are provided in Table 2.
From this optimization result, we can see that the shapeof the brace is created by correcting the shape of the scoliosispatient’s torso partially. Since the shape of torso inside a braceis not exactly the same as the shape of the brace, even with anideal brace with 100% corrections in translation and rotation,the torso’s shape is usually corrected only partially.
After the two torso correction factors were optimized andthe final corrected shape was generated, the shape was used tofabricate the brace die using a CNC milling machine (Fig. 12(a)).The brace was fabricated using the brace die through athermo-molding process (Fig. 12(b)). The laminated plasticblank brace was trimmed according to guidelines created bythe orthotist. Material of the relief area was removed fromlocation opposite to the curve apex, and additional pads wereplaced inside the brace to increase the applied pressure andadd cushioning. Straps were added to the brace, and the edgeswere smoothed (Fig. 12(c)). The brace was subsequently fitto the patient. The patient was also very satisfied with thiscustom-built brace.
6.2. Discussions
Different design parameter values were identified whendifferent weighting factors of evaluation measures wereselected. Different optimal design results can achieve differ-ent design objectives (Table 3). When the clinical evaluationmeasures were primarily considered, as was the case ofdesign 2 (Table 3), large translational and rotational correctionparameter values were typically identified. When the patient
evaluation measure was primarily considered, as was the caseof design 3 (Table 3), small translational and rotational correc-tion parameter values were achieved..
Computer based procedure
ime (h) Procedure Time (h)
3-D Imaging 0.25 Image processing 1.5.5 Design optimization 0.5
CNC machining 3 Thermo forming 3 Trimming 1
.5 9.25

s i n
r
488 c o m p u t e r m e t h o d s a n d p r o g r a m
The saving of labor hours was assessed (Table 4). The pro-cedure for brace creation was broken into several phases, andthe time used in each phase was obtained. The manual pro-cedure took approximately 17.50 h to complete, while the newcomputer-based method required only 9.25 h to create a brace.The time savings found in this study agree with those reportedby Wong et al. [5].
7. Conclusions and future work
An automated design approach was developed to identifythe optimal custom brace to satisfy the clinical and patientrequirements for scoliosis treatment. Results of the approachwere:
(1) The CAD/CAM based method considerably improved theefficiency of design and manufacturing of scoliosis braces.
(2) Design of custom braces considering both clinical andpatient evaluations created braces with greater effective-ness for scoliosis treatment.
(3) Multi-objective optimization was a useful method to iden-tify the optimal design considering multiple evaluationmeasures.
The following issues need to be further addressed in ourfuture work:
(1) Our study is based on the assumption that variousrelationships (e.g., relationships between evaluation mea-sures and evaluation indices, and relationships betweendisplacements and discomfort levels) can be used for allthe patients. Since different patients can be classified intodifferent patterns based on their differences in genders,ages, torso sizes, etc., modeling of the relationships con-sidering different patterns of patients is required. Morepatients need to be recruited for creating more custombraces for this purpose.
(2) The current research focuses on feasibility study of thecomputer based method to design and manufacture cus-tomized braces. To improve the effectiveness of thisapproach, more design variables (e.g., different transla-tional and rotational parameters for thoracic position,thoracic-lumbar position, and lumbar position), moreclinical evaluation measures (e.g., rib prominence, andbalance of anterior-posterior inertia in sagittal direction),and more customer evaluation measures (e.g., easiness forsports, and good-looking) need to be considered.
(3) Development of a standard medical procedure, and a user-friendly computer system for customized brace design andmanufacture is also expected.
Conflict of interest statement
None declared.
b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489
Acknowledgments
This work was supported by Fraternal Order of Eagles(Alberta and Saskatchewan), Grand Aerie–Fraternal Order ofEagles–Lew Reed Spinal Cord Research Fund, Alberta Chil-dren’s Hospital, and the Canada Research Chairs program.
e f e r e n c e s
[1] C.R. d’Amato, S. Griggs, B. McCoy, Nighttime bracing withthe providence brace in adolescent girls with idiopathicscoliosis, Spine 26 (2001) 2006–2012.
[2] D. Perie, J.S. de Gauzy, M.C. Hobatho, Biomechanicalevaluation of Cheneau–Toulouse–Munster brace in thetreatment of scoliosis using optimisation approach andfinite element method, Medical & Biological Engineering &Computing 40 (2002) 296–301.
[3] J.A.A.M. van den Hout, L.W. van Rhijn, R.J.H. van denMunckhof, A. van Ooy, Interface corrective forcemeasurements in Boston brace treatment, European SpineJournal 11 (2002) 332–335.
[4] D. Perie, C.E. Aubin, Y. Petit, H. Labelle, J. Dansereau,Personalized biomechanical simulations of orthotictreatment in idiopathic scoliosis, Clinical Biomechanics 19(2004) 190–195.
[5] M.S. Wong, J.C.Y. Cheng, M.W. Wong, S.F. So, A work study ofthe CAD/CAM method and conventional manual method inthe fabrication of spinal orthoses for patients withadolescent idiopathic scoliosis, Prosthetics and OrthoticsInternational 29 (2005) 93–104.
[6] M.S. Wong, J.C.Y. Cheng, K.H. Lo, A comparison of treatmenteffectiveness between the CAD/CAM method and themanual method for managing adolescent idiopathicscoliosis, Prosthetics and Orthotics International 29 (2005)105–111.
[7] J. Cottalorda, R. Kohler, C. Garin, P. Genevois, C. Lecante, B.Berge, Orthoses for mild scoliosis: a prospective studycomparing traditional plaster mold manufacturing withfast, noncontact, 3-dimensional acquisition, Spine 30 (2005)399–405.
[8] E Lou, D.L. Hill, J.V. Raso, M.J. Moreau, J.K. Mahood, Smartorthosis for the treatment of adolescent idiopathic scoliosis,Medical & Biological Engineering & Computing 43 (2005)746–750.
[9] H. Labelle, C. Bellefleur, J. Joncas, C.E. Aubin, F. Cheriet,Preliminary evaluation of a computer-assisted tool for thedesign and adjustment of braces in idiopathic scoliosis—aprospective and randomized study, Spine 32 (2007) 835–843.
[10] J.I. Kessler, Efficacy of a new computer-aideddesign/computer-aided manufacture orthosis in thetreatment of adolescent idiopathic scoliosis, Journal ofPediatric Orthopaedics B 17 (2008) 207–211.
[11] H. Wu, D. Xue, J. Harder, J.L. Ronsky, P. Poncet, J. Jaremko, G.Clynch, A. Gyorffy, R.F. Zernicke, Design and manufacturingof customized braces for scoliosis treatment, in: Proceedingsof the 2002 ASME Design Engineering Technical Conferencesand Computers and Information in Engineering Conference,Montreal, Quebec, 2002.
[12] A.L. Nachemson, L.E. Peterson, Effectiveness of treatmentwith a brace in girls who have adolescent idiopathic
scoliosis—a prospective, controlled study based on datafrom the brace study of the scoliosis research society,Journal of Bone and Joint Surgery American 78(1996).
i n b i
c o m p u t e r m e t h o d s a n d p r o g r a m s[13] S.L. Swanson, Estimating Scoliosis Progression from ThreeDimensional Torso Shape, M.Sc. Thesis, Department ofMechanical and Manufacturing Engineering, University ofCalgary, Calgary, AB, 2008.
[14] K. Sriwatanakul, W. Kelvie, L. Lasagna, J.F. Calimlim, O.F.Weis, G. Mehta, Studies with different types of visual analogscales for measurement of pain, Clinical Pharmacology and
Therapeutics 34 (1983) 234–239.[15] B. Roman, J. Statnikov, J.B. Matusov, MulticriteriaOptimization and Engineering, Chapman and Hall, NewYork, 1995.
o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 478–489 489
[16] G.G. Wang, S. Shan, An efficient Pareto set identificationapproach for multiobjective optimization on black-boxfunctions, in: Proceedings of the 2004 ASME InternationalDesign Engineering Technical Conferences and Computersand Information in Engineering Conference, Salt Lake City,UT, 2004.
[17] H. Yang, D. Xue, Y.L. Tu, Modeling of the non-linear relations
among different design and manufacturing evaluationmeasures for multi-objective optimal concurrent design,Concurrent Engineering: Research and Applications 14(2006) 43–53.
Related Documents











