www.wjpps.com Vol 5, Issue 10, 2016. 315 Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences COMPLICATED MALARIA INDUCED SEVERE ACUTE RENAL FAILURE: A CASE STUDY Sai Kiran Polamarasetti*, Uma Sankar Viriti, Sumanjali Podugu, Swetha Gandreti Avanthi Institute of Pharmaceutical Sciences, Bhogapuram, Vizianagaram, Andhra Pradesh, India. ABSTRACT Malaria is a mosquito-borne infectious disease affecting humans and other animals caused by parasitic protozoans (a group of single- celled microorganisms) belonging to the Plasmodium type like P. vivax, P. falciparum, P.malariae, or P. ovale. If Malaria is neglected or not treated properly, it may further develop into a severe form effecting the brain resulting in Cerebral Malaria. Acute Kidney Injury (AKI) is a known complication of malaria which involves abrupt lose of kidney function. In this present case, a patient came with the complaint of fever associated with chills, rigors, altered sensorium and decreased urine output. He was diagnosed with Complicated malaria (Cerebral Malaria) induced Acute Kidney Injury, Hyperbilirubinemia and Cerebral dysfunction. He was given with appropriate treatment, symptomatically relieved and drug utilization review has been done. Patient was counseled regarding the disease, its complications, prevalance and importance of medication adherence. KEYWORDS: Sensorium, Hyperbilirubinemia, Cerebral dysfunction, Plasmodium falciparum. INTRODUCTION DEFINITIONS: 1. MALARIA: Malaria is a mosquito-borne infectious disease affecting humans and other animals caused by parasitic protozoans belonging to the Plasmodium type like P. vivax, P. falciparum, P.malariae, or P. ovale. [1] WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES SJIF Impact Factor 6.041 Volume 5, Issue 10, 315-340 Review Article ISSN 2278 – 4357 *Corresponding Author Sai Kiran Polamarasetti Avanthi Institute of Pharmaceutical Sciences, Bhogapuram, Vizianagaram, Andhra Pradesh, India. Article Received on 29 July 2016, Revised on 17 August 2016, Accepted on 06 Sept 2016 DOI: 10.20959/wjpps201610-7784

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
315
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
COMPLICATED MALARIA INDUCED SEVERE ACUTE RENAL
FAILURE: A CASE STUDY
Sai Kiran Polamarasetti*, Uma Sankar Viriti, Sumanjali Podugu, Swetha Gandreti
Avanthi Institute of Pharmaceutical Sciences, Bhogapuram, Vizianagaram,
Andhra Pradesh, India.
other animals caused by parasitic protozoans (a group of single-
celled microorganisms) belonging to the Plasmodium type like
P. vivax, P. falciparum, P.malariae, or P. ovale. If Malaria is neglected
or not treated properly, it may further develop into a severe form
effecting the brain resulting in Cerebral Malaria. Acute Kidney Injury
(AKI) is a known complication of malaria which involves abrupt lose
of kidney function. In this present case, a patient came with the
complaint of fever associated with chills, rigors, altered sensorium and
decreased urine output. He was diagnosed with Complicated malaria
(Cerebral Malaria) induced Acute Kidney Injury, Hyperbilirubinemia
and Cerebral dysfunction. He was given with appropriate treatment, symptomatically relieved
and drug utilization review has been done. Patient was counseled regarding the disease, its
complications, prevalance and importance of medication adherence.
KEYWORDS: Sensorium, Hyperbilirubinemia, Cerebral dysfunction, Plasmodium
falciparum.
INTRODUCTION
DEFINITIONS:
1. MALARIA: Malaria is a mosquito-borne infectious disease affecting humans and other
animals caused by parasitic protozoans belonging to the Plasmodium type like
P. vivax, P. falciparum, P.malariae, or P. ovale. [1]
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 6.041
Volume 5, Issue 10, 315-340 Review Article ISSN 2278 – 4357
*Corresponding Author
DOI: 10.20959/wjpps201610-7784
316
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
2. CEREBRAL MALARIA:- Malaria will develop a severe form, and in these case it effects
brain and diffuse encephalopathy associated with seizures and status epilepticus which can
occur in up to one-third of patients with severe malaria, particularly that caused
by Plasmodium falciparum [2]
3. ACUTE KIDNEY INJURY:- Acute kidney injury (AKI) is the abrupt loss of kidney
function that develops within 7 days. (ARF (serum creatinine level, ≥3 mg/dL or ≥265
μmol/L)). [3]
4. ACUTE TUBULAR NECROSIS (ATN):- This is a medical condition involving
the death of tubular epithelial cells that form the renal tubules of thekidneys. ATN presents
with acute kidney injury (AKI) and is one of the most common causes of AKI [4]
EPIDEMIOLOGY:- Malaria is a major public health problem in tropical countries.
According to the World Malaria Report 2010, there were 225 million cases of malaria and an
estimated 781 000 deaths worldwide in 2009. [5]
About 500 million people suffer from
malaria, leading to death in 1 to 3 million cases. As per World Health Organization criteria,
acute renal failure occurs as a complication of Plasmodium falciparum malaria in less than
1% of cases, but the mortality rate in these cases may be up to 45%. It is more common in
adults than children. [6]
Cerebral malaria (CM) forms part of the spectrum of severe malaria,
with a case fatality rate ranging from 15% in adults in southeast Asia. [7]
Cerebral malaria is
the most severe neurological manifestation of severe malaria. With an incidence of
1,120/100,000/year in the endemic areas of Africa. [8]
CAUSES OF MALARIA: Malaria can occur if a mosquito infected with the
Plasmodium parasite bites you. An infected mother can also pass the disease to her baby at
birth. This is known as congenital malaria. Malaria is transmitted by blood, so it can also be
transmitted through:
An organ transplant
Use of shared needles or syringes. [9]
In humans, malaria is caused by P. falciparum, P. malariae, P. ovale, P. vivax and
P. knowlesi. [10]
317
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
PATHOPHYSIOLOGY OF MALARIA:- Malaria infection develops via two phases: one
that involves the liver (exoerythrocytic phase), and one that involves red blood cells
Erythrocytic phase. These two phases involves rupturing of RBC and invasion hepatic cells
for parasite replication. The rupturing of RBC causes most of the symptoms associated with
malaria as it produces toxicv substances, as the host’s immune system responds to the waste
products produced by the malaria parasites. [12]
CEREBRAL MALARIA:-The P. falciparum parasite displays adhesive proteins on the
surface of the infected blood cells, causing the blood cells to stick to the walls of small blood
vessels, thereby sequestering the parasite from passage through the general circulation and
the spleen. [13]
Sequestered red blood cells can breach the blood–brain barrier and cause
cerebral malaria [14]
SIGNS AND SYMPTOMS OF MALARIA
Plasmodium vivax, ovale and malariae:- The initial symptoms are often similar to those of
influenza:
Plasmodium falciparum:- Malaria caused by Plasmodium falciparum is the most severe form
of malaria. Cerebral malaria is defined as a severe P. falciparum-malaria presenting with
neurological symptoms, including coma (with a Glasgow coma scale less than 11, or
a Blantyre coma scale greater than 3), or with a coma that lasts longer than 30 minutes after a
seizure. [15]
mild jaundice
KIDNEY FAILURE
coma that may last for three days at a stretch
www.wjpps.com Vol 5, Issue 10, 2016.
318
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
rise in intracranial pressure
delirium and seizures [16]
DIAGNOSIS
Laboratory diagnosis of malaria requires the identification of the parasite or its antigens/
products in the patient’s blood.
Current available techniques can be separated in three categories
1. Microscopy
a) THICK AND THIN BLOOD SMEAR STUDY
i) Thick and thin blood smear study:- It is the gold standard method for malaria diagnosis.
ii) Thick smear:- Thick smears are mainly used to detect infection and to estimate
parasitemia.
iii) Thin smear:-Thin smears allow the examiner to identify malaria species, quantify
parasitemia, and recognize parasite forms like schizonts and gametocytes. [17]
b) QUANTATIVE BUFFY COAT (QBC) TEST:- QBC test is easier and faster than
classic peripheral blood smear microscopy but the equipment required is expensive and
species identification and accurate enumeration are impossible.
2. IMMUNOLOGICAL TECHNIQUES
a) ANTIBODY-BASED TECHNIQUES
i) Indirect fluorescent antibody test (IFAT)
ii) Enzyme- linked immunosorbent assay (ELISA):- If the test is positive, the antibody
binds the antigen resulting in a visible colour change. When the test is negative, in the
absence of antibody, there is no change of colour of the substrate.
b) ANTIGEN-BASED TECHNIQUES
i) Rapid Diagnostic Test (RDT)
RDT is a device that can detect malaria antigen in a small amount of blood (5μl) by
immunochromatographic with monoclonal antibodies directed against the parasite antigen.
www.wjpps.com Vol 5, Issue 10, 2016.
319
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
3. MOLECULAR TECHNIQUES
a) Polymerase Chain Reaction (PCR):-Using PCR amplification, it is possible to detect all
4 species of malaria parasites with a reportedly 10-fold greater sensitivity than microscopy .[17]
OTHER TESTS
a) Subjective diagnosis:- Areas that cannot afford laboratory diagnostic tests often use only
a history of subjective fever as the indication to treat for malaria. [18]
b) Differential diagnosis:- In malaria-endemic areas, parasitemia does not ensure a diagnosis
of severe malaria, because parasitemia can be incidental to other concurrent disease. Recent
investigations suggest that malarial retinopathy is better (collective sensitivity of 95% and
specificity of 90%) than any other clinical or laboratory feature in distinguishing malarial
from non-malarial coma. [19]
c) Susceptibility testing:- It is done by testing the DNA of the parasite to detect markers that
indicate resistance.
CEREBRAL MALARIA(CM)
Advanced imaging devices have become increasingly accessible in elucidating the etiology of
CM [20]
damage attributable to inflammatory processes and allows the analysis of neuronal axon
injury during CM [21]
c) COMPUTED TOMOGRAPHY:- Determination of cerebral volume variation and the
detection of infarctions in large vessels [22]
2. INVESTIGATIVE NEURO-IMAGING TOOLS
a) In vivo bioluminescent imaging
In vivo bioluminescent imaging is a versatile and sensitive tool that is based on the detection
of light emission from cells or tissues. [23]
320
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
b) 18
f-fluorodeoxyglucose (fdg) positron emission tomography (pet)
FDG-PET is a non-invasive imaging tool used to map cerebral metabolic activity by
quantifying the uptake of a glucose analog by brain cells. [24]
3. NEW DIAGNOSTIC TOOLS
a) Malarial retinopathy
The sequestration of P. falciparum-infected red blood cells (PRBC) in the cerebral
microvasculature is the hallmark of CM. [25]
ii) Optical Coherence Tomography (OCT):-OCT is an in vivo imaging tool for the
detection of retinal changes. [26]
4. ELECTROENCEPHALOGRAPHY (EEG) AND MICRO-EEG
a) EEG
This non-invasive technique to record electrical impulses of the brain by measuring voltage
fluctuations. [27]
5. BIOMARKERS:- Biomarkers include tools and technologies that can facilitate the
prediction, cause, diagnosis, progression, regression, or outcome of treatment of disease. [28]
MANAGEMENT
Modes of Treatment: Two important concepts in the treatment of malaria are suppressive
and radical treatments.
i) SUPPRESSIVE TREATMENT: The symptoms of malaria can be alleviated by
suppressing the erythrocytic stage of the parasitic development. Suppressive therapy involves
administration of appropriate blood schizonticidal drugs.
ii) RADICAL TREATMENT: Radical treatment is administration of primaquine to all
confirmed cases of malaria.
In P. vivax malaria, 2 weeks’ therapy with primaquine completely cures the infection in
the host by its tissue schizonticidal activity and thereby prevents relapses.
In P. falciparum malaria, a single dose of primaquine destroys the gametocytes, thereby
prevents the spread of the infection into the mosquito [29]
The drugs available to treat malaria include: Chloroquine, Quinine,
Hydroxychloroquine (Plaquenil), Artemether and lumefantrine (Coartem), Atovaquone
321
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
(Mepron), Proguanil (sold as a generic), Mefloquine, Clindamycin (Cleocin) and
Doxycycline.
People with falciparum malaria have the most severe symptoms. People
with falciparum malaria may need to be monitored in the intensive care unit of a hospital
during the first days of treatment because the disease can cause breathing failure, coma
and kidney failure [30]
TREATMENT FOR SEVERE OR COMPLICATED MALARIA
i) ANTIMALARIALS:- All patients with any form of complicated or severe disease should
be treated parenterally. The choice of drugs, according to availability and licensing, lies
between the cinchona alkaloids, i.e. quinine or quinidine (in the USA), or one of the
artemisinin derivatives, preferably intravenous artesunate. [31]
ii) QUININE:- Since the advent of chloroquine resistance, quinine has been the drug of
choice for the parenteral treatment of malaria. Quinine is given by slow intravenous infusion
but in an emergency may be given intramuscularly in split doses as has been done in
children. [32]
iii) ARTEMISININ AND ITS DERIVATIVES:- Artemisinin derivatives are increasingly
being used in the treatment of malaria of all degrees of severity. Artemisinins, especially
artesunate and artemether, result in more rapid parasite clearance (being active on the
immature parasite forms. [33]
In children with cerebral malaria and evidence of raised intracranial pressure, mannitol (1 g
kg −1
infused over 30 min as a 10 or 20% solution) has been shown to control intermediate
intracranial hypertension, but not when severe (>40 mmHg) 34
.
Life-threatening situations because of malaria infection with P. falciparum may include:
Severe infection of the brain (cerebral malaria), with seizures, confusion, and increasing
tiredness leading to coma and death.
Fluid in the lungs (pulmonary edema)
Abnormal liver function
Low blood sugar (hypoglycemia).
Altered blood chemistry, including low sodium and lowered pH (lactic acidosis)
322
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
Blackwater fever
MALARIA INDUCED ACUTE KIDNEY INJURY/ACUTE KIDNEY FAILURE
This is also indicated as ‘Malarial Nephropathy’. Acute kidney injury (AKI) is a known
complication of malaria, and is reported to occur in up to 40 % of adult patients with a
severe Plasmodium falciparum infection in endemic regions. [36]
Infection with the
urinary abnormalities and mild electrolyte imbalance to acute renal failure. Renal failure is
multifactorial and carries a high mortality and morbidity [37]
Over a decade ago, cerebral
malaria was the predominant manifestation of severe malaria, where as today the
combination of jaundice and renal failure are more common. [38]
PREVALANCE:- Prevalence of ARF in malaria all over the world has been reported as
0.57% to 60% . In Southeast Asia there is an upsurge in the overall incidence of malarial
ARF and has been reported in between 13% to 17.8%. [39]
RISK FACTORS OF OCCURING AKI IN MALARIAL PATIENTS
Immuno-compromised patients (Elderly or infants)
Pathogen/Parasitic overload
Kidney trauma or injury
Pregnant women
Poor people due to lack of effective treatment
Over use of medicines that are highly burden to the kidneys
Multi-organ dysfunction. [40]
PATHOGENESIS:- The pathogenesis of AKI in falciparum malaria is not clearly known.
Several factors; including various chemical mediators, catecholamine release, cytoadherence
of parasitized erythrocytes, dehydration, intravascular haemolysis, intravascular coagulation,
sepsis hyprebilirubinaemia and hyperparasitaemia have been implicated in the pathogenesis
of ARF in malaria. [41]
Malarial complications possibly are caused by the interaction of the
323
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
parasite with the host, resulting in mechanical, immunologic, and humoral responses. These
responses, while attempting to eliminate the parasites, may also injure the host tissues. [42]
CYTOADHERENCE
The pathogenesis of severe P falciparum malaria is attributed in part to the cytoadherence of
parasitized red blood cells (PRBCs) to the vascular endothelial cells in different host
organs. [43]
Parasite proteins referred to as variant surface antigens expressed on the PRBC
surface mediate the adhesion of infected erythrocytes to host vascular endothelial
receptors. [44]
PRBCs preferentially sequester in the deep vascular beds of vital organs,
including the brain, liver, lung, spleen, intestine, and kidney. [45]
Sequestration of PRBCs in
glomerular and tubulointerstitial capillaries has been shown, although at a lesser degree than
the cerebral vessels. [46]
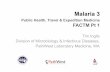
features in plasmodium infections: hemodynamic, immunologic, and metabolic
perturbations. [47]
Principal pathogenic pathways in severe falciparum malaria was mentioned in the above
fig.1. [48]
CYTOKINES, REACTIVE OXYGEN SPECIES, AND NITROGEN SPECIES
Literature on the influence of cytokine concentrations on renal pathology in malaria is scanty
although cytokines, reactive oxygen intermediates, and nitrogen intermediates (ROI and NO)
play an important role in both protection against malaria and pathogenesis of severe malaria.
Levels of inflammatory cytokines, such as tumor necrosis factor (TNF-α), interferon- γ, and
interleukins 1-α, -6, and -8 are increased in malaria. [49]
Higher blood concentrations of
proinflammatory cytokines have been observed in severe complications of malaria. [50]
Anti–
TNF-α and anti–interferon γ- antibodies are reported to abolish the onset of cerebral
www.wjpps.com Vol 5, Issue 10, 2016.
324
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
malaria [51]
However, in contrast to observations in the murine model, monoclonal antibodies
to Malaria and AKI 397 TNF- ameliorate fever but not the manifestations of human cerebral
malaria [52]
An early increase in NO stimulates the helper T-cell-1 (Th1) response to control
parasitemia similar to natural immunization during malaria infection. [53]
Whereas a late
increase in NO production in the liver and spleen appear to have pathologic consequences.
Regulatory functions of NO are dependent on the presence of various isoforms of the enzyme
nitric oxide synthase (NOS). Physiologic function of NO is regulated by low basal
concentrations synthesized by constitutive NOS isoforms. A high concentration of NO
usually is produced by inducible NOS isoforms (iNOS), which play a crucial role in
pathologic consequences. Increased iNOS activity and production of NO have been observed
in severe malaria. [54]
RESTRICTED LOCAL BLOOD FLOW IN THE KIDNEYS:- This is considered as a
major contributor for malarial ARF. Low intake of fluids, loss of fluids because of vomiting
and pyrexial sweating may be responsible for dehydration and renal ischemia. Administration
of intravenous fluids often worsens the general condition of the patient by inducing
pulmonary edema, a situation similar to shock like syndrome. A generalized vasodilatation
with an associated decrease in systemic vascular resistance is considered an important
contributor for septic shock as well as malarial ARF. Vasodilatation leads to activation of
sympathetic nervous system, rennin-angiotensin-aldosterone axis (RAAA), and release of
vasopressin for maintaining the falling blood pressure. Unfortunately, these compensatory
mechanisms may worsen the renal pathology leading to overt ARF. [55,56]
LOW INTAKE OF FLUIDS, LOSS OF FLUIDS:-Because of vomiting and pyrexial
sweating, cytokine and NO mediated arterial vasodilatation specifically organ specific release
of NO, resistance to vasoactive hormones, cytopathic hypoxia leading to decreased ATP
synthesis, cytoadherence of PRBCs, etc all may contribute singly or in combination towards
malarial ARF. Increased fluid administration, oxygen toxicity, and yet unidentified factors
may contribute to pulmonary edema, acute respiratory distress syndrome (ARDS), multiorgan
failure and death. [57]
SIGNS AND SYMPTOMS
An absolute increase in serum creatinine level of 0.3 mg/dL or more (26.4 mol/L)
A percentage increase in serum creatinine level of 50% or more (1.5-fold from baseline)
www.wjpps.com Vol 5, Issue 10, 2016.
325
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
A reduction in urine output (documented oliguria of 0.5 mL/kg/h for 6 hours). [58]
Swelling in legs, ankles, and around the eyes
nausea and vomiting
Chest pain or pressure
Fluid imbalances. [60]
DIAGNOSIS
The following tests can aid in the diagnosis and assessment of AKI:
Kidney function studies: Increased levels of blood urea nitrogen (BUN) and creatinine are
the hallmarks of renal failure
Complete blood count
Fractional excretion of sodium and urea
Bladder pressure: Patients with a bladder pressure above 25 mm Hg should be suspected
Ultrasonography
Aortorenal angiography : Can be helpful in establishing the diagnosis of renal vascular
diseases, such as renal artery stenosis, renal atheroembolic disease, atherosclerosis with
aortorenal occlusion, and certain cases of necrotizing vasculitis (eg, polyarteritis nodosa)
Renal biopsy: Can be useful in identifying intrarenal causes of AKI. [61]
urinalysis
Estimated glomerular filtration rate (eGFR)
AKI can be diagnosed if any one of the following is present:
Increase in SCr by ≥0.3 mg/dl (≥26.5 μmol/l) within 48 hours; or
Increase in SCr to ≥1.5 times baseline, which have occurred within the prior 7 days; or
Urine volume < 0.5 ml/kg/h for 6 hours. [62]
www.wjpps.com Vol 5, Issue 10, 2016.
326
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
MANAGEMENT
The management of MAKI needs careful and meticulous management of several problems.
Early and prompt decisions and institutions are the hallmark of a better prognosis. The
outlines of treatment guidelines include the following:
1. institution of appropriate antimalarials
2. maintenance of fluid and electrolyte levels
3. renal replacement therapy as indicated
4. treatment of associated complications and
5. management of infection including pneumonia.
ANTIMALARIA DRUGS:- The preferred antimalarial is artesunate or quinine given
parenterally. Intravenous quinine has remained as the time-tested first-line drug. The dose is
10 mg/kg/body weight. If quinine has not been given in the previous 7 days, a loading dose
may be given. But it is very diffi- cult to get a definite history, hence it is advisable to start a
maintenance dose of 10 mg/kg of body weight every 8 hours. The dose for the initial 48 hours
should never be modified, even in the presence of AKI. [63,64]
The use of other drugs, namely
chloroquine or sulfadoxine pyrimethamine, should be avoided owing to widespread
resistance from areas where CM and AKI are common.
FLUID CHALLENGE
Many patients with oligura are dehydrated. They should receive fluid, up to 20 mL/kg of
0.9% saline infused over 60 minutes. To prevent fluid overload, auscultation of the lungs and
jugular venous pressure measurements (and, if possible, CVP measurements) should be
performed after every 200 mL of fluid. The CVP should always be kept between 0 and ±5. If
there is no urine output after fluid replacement, an intravenous diuretic challenge may be
given. [58]
DOPAMINE CHALLENGE
The use of dopamine for the prevention and treatment of AKI has not yet been established. Its
use is based on the understanding that selective renal vasodilatation will occur when it is
infused at a low dose. In a prospective, controlled, cross-over trial in an intensive care unit of
an infectious diseases hospital in Vietnam, dopamine at a renal dose (2.5 g/kg/min) was
associated with a mean (95% confidence interval) fractional increase in the absolute renal
blood flow (RBF) index of 37% (13% to 61%) and in RBF as a fraction of cardiac output of
35% (10%-59%; P = .007 and P = .014, respectively). [65]
www.wjpps.com Vol 5, Issue 10, 2016.
327
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
VASOPRESSIN THERAPY
As discussed in the pathogenesis, there appears to be a future role for the use of vasopressin
in the management of malarial shock as well as MAKI.
ALBUMIN INFUSION
The administration of albumin for volume expansion reduces mortality rates. [66]
DIURETIC CHALLENGE
The loop diuretic (frusemide 40 mg or bumetanide 1 mg) is given initially. If urination does
not occur, further diuretic challenge can be tried at every 30-minute intervals with
incremental doses (frusemide 100, 200, and 400 mg or bumetanide 2, 4, and 6 mg). If there is
still no urine flow, dopamine 2.5 to 5 g/kg/min may be tried [67]
RENAL REPLACEMENT THERAPY:- It should be initiated if any of the following is
present
b. Uraemic symptoms (Encephalopathy or pericarditis)
c. Fluid overload, pulmonary edema, congestive heart failure or Pericardial rub [68]
DIALYSIS:- Dialysis has improved the survival of the AKI cases when instituted early in the
course. It can be intermittent haemodialysis (daily or alternate day), or continuous
venovenous haemofiltration (CVVH) or arteriovenous haemofiltration (CAVH). Often
haemodialysis (HD) is performed in patients with AKI as Peritoneal dialysis (PD) is
considered to be less effective in controlling biochemical abnormalities than HD. Thus,
whenever RRT is indicated, either PD or HD should be started as early as possible.
FREQUENCY OF DIALYSIS:-
Intermittent HD should be performed daily for better prognosis in acute renal failure.
Mortality is reduced in patients receiving six dialyses per week as opposed to those receiving
HD every other day. [69,70]
MANAGEMENT OF DIURETIC PHASE:-
Diuretic phase may return gradually or in a few hours. Careful attention needs to be given
towards fluid and electrolyte requirements. In addition, repeated estimation of Na, K and
bicarbonate is essential.
328
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
NUTRITION: Suppressing endogenous protein catabolism by providing fat and
carbohydrates is recommended. In patients without dialysis, protein restriction is advised,
whereas those undergoing daily HD may require additional proteins. [75]
CASE STUDY
A patient of age 60years male was admitted in King George Hospital Visakhapatnam, Andhra
Pradesh, India, with a complaint of fever since 10 days and altered sensorium since 1day.
History of present illness: Patient was apparently normal 10 days before. Later he developed
fever and yellowish discoloration from 10days. Fever was found to be high grade,
intermittent and associated with chills and rigors, associated with headache. There is
decreased output of urine from 4days. Last day urine output increased. Altered sensorium is
observed last day.
Patient experienced cough with expectoration since 5 days and breathlessness since 3 days.
On examination patient experienced altered seizures.
There is no history of hematuria/pyuria/dysuria/vomiting/diarrhea/pedal edema/facial
puffiness.
Patient didn’t experience any of the above present complaints in the past.
Personal history was found to be alcoholic, smoker and takes mixed diet.
On the day of admission, patient’s blood pressure was found to be 140/50mm of Hg, Pulse
rate 80/min, Respiratory rate 15/min and temperature was afebrile.
On examination by using Glasgow coma scale, measures were done to estimate brain
function. Results were found to be E2, V1, M4. These scores explain that:
E2 - means eye opening to pain
V1- means no verbal response
M4 - means motor response withdraws to pain
On addition of scores of E.V and M we get 2+1+4=7, it shows that severe brain injury.
[3-8 = severe brain injury
9-12=moderate brain injury
13-15= mild brain injury]
329
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
RBC- normocytic, hypochromic with mild anisocytes
WBC- count is increased and neutrophilia is seen
Platelets- adequate
Basing on these it was found that normocytic, hypochromic anemia with neutrophilic
leukocytosis
Blood urea levels: 199 mg/dl (normal: 14-45)
Serum bilirubin total: 18.4 mg% (0.3 to 1.0 mg%)
SGOT: 74 U/L (Normal: 5-40 U/L)
SGPT: 50 U/L (Normal: 7-56 U/L)
Serum Alkaline Phosphate: 348 U/L (Normal level for 56-60 years: 46-118 U/L)
Patient exhibited sensorium, seizures (E2 V1 M4) and Plasmodium falsiparum positive. So he
was diagnosed as CEREBRAL MALARIA and CEREBRAL DYSFUNCTION.
Total Bilirubin levels are abnormal. So the patient was concluded of having
HYPERBILIRUBINEMIA.
Serum creatine levels are abnormally high. Previously patient has no complaint of Renal
problems. But after getting Malaria, he was tested for serum creatine levels and was
concluded that he is having renal impairment so that his serum creatine levels are abnormal.
Basing on this he was diagnosed of having ACUTE KIDNEY INJURY induced by
MALARIA.
FINAL DIAGNOSIS
By observing the above diagnostic tests patient was diagnosed as suffering with CEREBRAL
MALARIA WITH ACUTE KIDNEY INJURY, HYPERBILIRUBINEMIA, CEREBRAL
and DYSFUNCTION
TREATMENT
On the first day of treatment patient was given with Inj.falcigo( artesunate) 120mg IV BD ,
Inj.clindamycin 600mg IV BD, Inj.pantop(pantoprazole) 40mg IV OD, Tab.paracetamol
500mg QID, IVF( intravenous fluid) 25%dextrose IV TID.
On 2 nd
day, patient exhibited altered sensorium. Same drugs that are Inj.falcigo( artesunate)
120mg IV BD, Inj.clindamycin 600mg IV BD, Inj.pantop(pantoprazole) 40mg IV OD, Tab.
paracetamol 500mg QID, IVF( intravenous fluid) 25%dextrose IV TID were continued.
Dialysis is done by using bicarbonate dialysate.
www.wjpps.com Vol 5, Issue 10, 2016.
330
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
On 3 rd
day, BP-160/100mm of Hg, PR-96/min and abdominal examination shows diffuse
tenderness. Patient was given with drugs like Tab.Nicardia Retard( nifedipine) 10mg BD,
Tab.Falcigo 120mg IV OD, Tab.Clindamycin 600mg IV BD, Inj.Pantop 40 mg IV OD and
Tab. B complex OD.
On 4 th
day, patient is conscious and coherent and found to be afebrile. BP is 140/80 mm of
Hg and PR is 92/min. Same drugs continued, that are Tab.Nicardia Retard( nifedipine) 10mg
BD, Tab.Falcigo 120mg IV OD, Tab.Clindamycin 600mg IV BD, Inj.Pantop 40 mg IV OD
and Tab. B complex OD.
On 5 th
day, patient is conscious and coherent and found to be afebrile. BP is 140/90 mm of
Hg, PR is 72/min and abdomen is soft. Drugs like Tab.Nicardia Retard( nifedipine) 10mg
BD, Tab.Falcigo 120mg IV OD, Tab.Clindamycin 600mg IV BD, Inj.Pantop 40 mg IV OD
and Tab. B complex OD were given. Patient is given IVF ( intra venous fluid) 25% dextrose
in 100 ml. dialysis was done using bicarbonate dialysate.
On 6 th
day, patient is conscious and coherent and found to be afebrile. BP is 140/80 mm of
Hg, PR is 74/min and abdomen is soft. Drugs like Tab.Nicardia Retard( nifedipine) 10mg
BD, Tab.Falcigo 120mg IV OD, Tab.Clindamycin 600mg IV BD, Inj.Pantop 40 mg IV OD
and Tab. B complex OD were given. Patient is given IVF (intra venous fluid) 25% dextrose
in 100 ml. dialysis was done using bicarbonate dialysate. Syrup.lactulose 15ml TID and
Inj.opitneuron 10 ml in 100 ml normal saline IV OD is given.
On 7 th
day, patient exhibited fever, BP is 120/80 mm of Hg and PR is 78/min. same drugs
were continued. But dialysis is not done.
On 8 th
day, patient was found to be afebrile, BP is 120/80 mm of Hg and PR is 82/min. same
drugs were continued but syrup lactulose is replaced with syrup duphalac 15ml TID.
On 9 th
day, BP is 120/80 mm of Hg and PR is 90/min. Drugs like Inj.falcigo 120mg IV OD,
Inj.clinamycin 600mg IV BD, Inj.pantop 40 mg OD, Tab.Nicardia Retard 20 mg BD, Tab.
Bcomplex and Tab. Calcium.
On 10 th
day, patient was given with Tab. Nicardia Retard 20 mg BD, Tab. B complex OD,
Tab. Calcium BD and Tab. IFA ( iron folic acid) OD were given.
On 11 th
day, patient vitals are normal and was given with Tab. Nicardia Retard 20 mg BD,
Tab. B complex OD, Tab. Calcium BD and Tab. IFA ( iron folic acid) OD were given.
On 12 th
day, patient was given with Tab. Nicardia Retard 20 mg BD, Tab. B complex OD,
Tab. Calcium BD and Tab. IFA ( iron folic acid) OD were given.
www.wjpps.com Vol 5, Issue 10, 2016.
331
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
On 13 th
day, patient exhibited fever. So Tab. Paracetomol 500mg SOS along with Tab.
Nicardia Retard 20 mg BD, Tab. B complex OD, Tab. Calcium BD and Tab. IFA ( iron folic
acid) OD were given.
On 14 th
day, patient exhibited fever, BP is 130/90 mm of Hg and PR is 78/min and RR is
20/min. His urine output is >600ml. Blood pressure was controlled so nicardia retard drug has
stopped. Tab. B complex OD, Tab. Calcium+ vit D3 OD, Tab. IFA ( iron folic acid) OD, Tab.
Pantop 40 mg OD and Tab. Paracetomol 500mg SOS are given. Dialysis was done using
bicarbonate dialysate.
On 15 th
day, patient vitals are normal i.e., BP is 130/80 mm of Hg and PR is 84/min and RR
is 18/min. Paracetomol was withdrawn and same drugs are given. But dialysis is not done.
On 16 th
day, patient vitals are normal and his urine output is 1 liter.Drugs like Tab. B
complex OD, Tab. Calcium+ vit D3 OD, Tab. IFA ( iron folic acid) OD, Tab. Pantop 40 mg
OD and Tab. Paracetomol 500mg SOS are given.
On 17 th
day, patient vitals are normal i.e., BP is 120/80 mm of Hg and PR is 82/min and RR
is 22/min. His urine output is 1.8 liters. So drugs like Tab. B complex OD, Tab. Calcium+ vit
D3 OD, Tab. IFA ( iron folic acid) OD, Tab. Pantop 40 mg OD and Tab. Paracetomol 500mg
SOS are given.
On 18 th
day, patient was prescribed with Tab. B complex OD, Tab.Calcium+ vit D3 OD, Tab.
IFA ( iron folic acid) OD, Tab. Pantop 40 mg OD.
On 19 th
day, patient vitals are normal and his urine output is 1.6 liters. Same drugs were
continued.
On 20 th
day, patient is conscious and coherent and found to be afebrile. BP is 120/70 mm of
Hg, PR is 84/min and abdomen is soft. His Urine Output is 1.8 liters.He was prescribed with
Tab. B complex OD, Tab.Calcium+ vit D3 OD, Tab. IFA ( iron folic acid) OD, Tab. Pantop
40 mg OD..
On 21 st
day, patient vitals are normal and his urine output is 1.2 liters. On 22 nd
day, patient’s
Urine output was 2 liters and was given with Tab. Rantac 150mg BD, Cap. IFA ( iron folic
acid) OD, Tab.Calcium+ vit D3 OD and Tab. B complex OD.
On 23 rd
day, patient’s Urine output was 1.8 liters. Drugs like Tab. Rantac 150mg BD, Cap.
IFA ( iron folic acid) OD, Tab.Calcium+ vit D3 OD and Tab. B complex OD were given.
On 24 th
day, patient’s Sr.Cr. levels are 1.7mg/dl and blood urea was 45mg/dl. Patient was
generally improved, vitals are stabilized and urine output is also improved. So, he was
discharged under stable, general conditions and advised to attend nephrology OPD at regular
follow ups.
332
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
DISCUSSION: A 60 years old male patient came with a complaint of fever since 10 days
and altered sensorium since 1 day. He was diagnosed as suffering with Cerebral Malaria with
Acute Kidney Injury, Hyperbilirubinemia and Cerebral dysfunction. So he was given with
Inj.Falcigo 120mg IV. Falcigo (Aetesunate) is an anti-malarial drug. Artemisinins and
cinchona alkaloids are the only classes used to treat severe malaria. So intravenous artesunate
was given to treat cerebral malaria. Clindamycin 600mg IV BD was given inorder to treat the
Complicated Malaria. Tab. Paracetomol 500mg QID is given as the patient exhibited Fever.
Nicardia Retard (Nifedepine) 10mg BD is given in order to treat blood pressure due to Acute
Kidney Injury(AKI) which relaxes smooth muscle and produces vasodilation, which in turn
improves blood flow and oxygen delivery. Pantop (Pantoprazole) is a proton pump
inhibitor that decreases the amount of acid produced in the stomach. Tab B complex, Iron
folic acid supplements are mainly given as having chronic kidney disease changes the need
for some nutrients, their absorption or their utility and some may lost during dialysis.
Optineuron is for relaxing the nerve signals to the brain. Patient was haemodialysed 5 times
along with packed cell transfusion. Patient general condition was improved, vitals are
stabilized and urine output is improved after 20 days of hospital admission. He was
discharged with medications Tab. B complex OD, Tab.Calcium+ vit D3 OD and Tab. IFA (
iron folic acid) OD.
333
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
2. HOSPITAL CONSENT FORM
334
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
5. CONSENT FORM
CONCLUSION
Malaria is a mosquito-borne infectious disease which is a major public health problem caused
by parasitic protozoans belonging to the Plasmodium type like P. vivax, P. falciparum,
P.malariae, or P. ovale. If this condition is neglected or untreated it may get complicated and
effects brain(Cerebral Malaria). Acute kidney injury (AKI) is the abrupt loss of kidney
function which is also a complication of malaria. Present case was apparently normal 10 days
before. Later he developed fever, decreased urine output and altered sensorium. He was
diagnosed as suffering with Cerebral malaria with acute kidney injury, hyperbilirubinemia
and cerebral dysfunction. Given with appropriate treatment, the patient was found to be
relieved from symptoms. Patient was explained about the disease condition and its
assosciated complications, importance of medication adherence and discharged with
medication.From this case, it is cleared that if Malaria is neglected, it becomes complicated
and may be fatal. In every malaria case, serum creatinine levels should be checked
compulsorily. If it is correctly treated in right time with right medication, the quality and well
being of the patient can be improved.
www.wjpps.com Vol 5, Issue 10, 2016.
335
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
ACKNOWLEDGEMENT
The author likes to express his gratitude towards the Physicians of King George Hospital
especially Nephrology Department, King George Hospital and Avanthi Institute of
Pharmaceutical Sciences for continuous support.
REFERENCES:-
1. "Malaria Fact sheet N°94". WHO. March 2014. Retrieved 28 August 2014.
2. Indian J Crit Care Med. 2008 Oct-Dec; 12(4): 204–205. doi: 10.4103/0972-5229.45084.
3. Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, Levin A
(2007). "Acute Kidney Injury Network: report of an initiative to improve outcomes in
acute kidney injury". Critical Care (London, England). 11 (2):
R31. doi:10.1186/cc5713.PMC 2206446 . PMID 17331245.
4. "Acute Tubular Necrosis (ATN)". Nephrology Channel. HealthCommunities.com. 2008.
Retrieved 2008-09-23.
5. World Malaria Report. 2010; p. 60.
6. Mishra SK, Das BS.Malaria and acute kidney injury. Semin Nephrol. 2008 Jul;28(4):395-
408. doi: 10.1016/j.semnephrol.2008; 04: 007.
7. Georges Emile Raymond Grau; Alister Gordon Craig. Cerebral Malaria Pathogenesis.
Future Microbiol. 2012; 7(2): 291-302. Medscape.
8. Breman JG, Am J . The ears of the hippopotamus: manifestations, determinants, and
estimates of the malaria burden. Trop Med Hyg. 2001 Jan-Feb; 64(1-2 Suppl): 1-11.
9. Darla Burke. Malaria. Reference Library. Healthline. December 14, 2015.
10. Collins WE (2012). "Plasmodium knowlesi: A malaria parasite of monkeys and
humans". Annual Review of Entomology. 57: 107–21. doi:10.1146/annurev-ento-121510-
133540. PMID 22149265.
11. Bledsoe GH (2005). "Malaria primer for clinicians in the United States". Southern
Medical Journal. 98(12): 1197–204; quiz 1205, 1230.
doi:10.1097/01.smj.0000189904.50838.eb. PMID 16440920.
12. Vaughan AM, Aly AS, Kappe SH (2008). "Malaria parasite pre-erythrocytic stage
infection: Gliding and hiding". Cell Host & Microbe. 4(3): 209–18.
doi:10.1016/j.chom.2008.08.010. PMC 2610487. PMID 18779047
13. Tilley L, Dixon MW, Kirk K (2011). "The Plasmodium falciparum-infected red blood
cell". International Journal of Biochemistry and Cell Biology. 43(6): 839-42. Doi:
10.1016/j.biocel.2011.03.012. PMID 21458590.
336
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
14. Rénia L, Wu Howland S, Claser C, Charlotte Gruner A, Suwanarusk R, Hui Teo T,
Russell B, Ng LF (2012). "Cerebral malaria: mysteries at the blood-brain
barrier". Virulence. 3(2):193201.doi:10.4161/viru.19013. PMC 3396698.
PMID 22460644.
15. WHO (2010). Guidelines for the Treatment of Malaria (PDF) (Report) (2nd ed.). World
Health Organization. ISBN 978-9-2415-4792-5.
16. Bushra Kafeel. Malaria-Symptoms of cerebral malaria. Blood diseases; Only my health.
http://www.onlymyhealth.com/signs-symptoms-cerebral-malaria-1300864141
http://www.malwest.gr/enus/malaria/informationforhealthcareprofessionals/laboratorydia
gnosis.aspx
18. Redd S, Kazembe P, Luby S, Nwanyanwu O, Hightower A, Ziba C, Wirima J, Chitsulo
L, Franco C, Olivar M (2006). "Clinical algorithm for treatment ofPlasmodium
falciparum malaria in children". Lancet. 347(8996): 223–7. doi: 10.1016/S0140-
6736(96)90404-3.PMID 8551881.
19. Beare NA, Taylor TE, Harding SP, Lewallen S, Molyneux ME (November
2006). "Malarial retinopathy: a newly established diagnostic sign in severe malaria". Am.
J. Trop. Med. Hyg. 75(5): 790–7.PMC 2367432 . PMID 17123967.
20. Praveen K. Sahu 1 , Sanghamitra Satpathi
2 et al., Pathogenesis of cerebral malaria: new
diagnostic tools, biomarkers, and therapeutic approaches. Front. Cell. Infect. Microbiol.,
27 October 2015 http://dx.doi.org/10.3389/fcimb.2015.00075
21. Kennan, R. P., Machado, F. S., Lee, S. C., Desruisseaux, M. S., Wittner, M., Tsuji, M., et
al. (2005). Reduced cerebral blood flow and N-acetyl aspartate in a murine model of
cerebral malaria. Parasitol. Res. 96, 302–307. doi: 10.1007/s00436-005-1349-z
22. Potchen, M. J., Birbeck, G. L., Demarco, J. K., Kampondeni, S. D., Beare, N., Molyneux,
M. E., et al. (2010). Neuroimaging findings in children with retinopathy-confirmed
cerebral malaria. Eur. J. Radiol. 74, 262–268. doi: 10.1016/j.ejrad.2009; 02: 010
23. Franke-Fayard, B., Waters, A. P., and Janse, C. J. (2006). Real-time in vivo imaging of
transgenic bioluminescent blood stages of rodent malaria parasites in mice. Nat. Protoc. 1,
476–485. doi: 10.1038/nprot.2006; 69
24. Sugiyama, M., Ikeda, E., Kawai, S., Higuchi, T., Zhang, H., Khan, N., et al. (2004).
Cerebral metabolic reduction in severe malaria: fluorodeoxyglucose-positron emission
337
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
tomography imaging in a primate model of severe human malaria with cerebral
involvement. Am. J. Trop. Med. Hyg. 71, 542–545.
25. Beare, N. A., Taylor, T. E., Harding, S. P., Lewallen, S., and Molyneux, M. E. (2006).
Malarial retinopathy: a newly established diagnostic sign in severe malaria. Am. J. Trop.
Med. Hyg. 75, 790–797. doi: 10.1016/j.idcr.2014; 10: 003
26. Sakata, L. M., Deleon-Ortega, J., Sakata, V., and Girkin, C. A. (2009). Optical coherence
tomography of the retina and optic nerve - a review. Clin. Exp. Ophthalmol. 37, 90–99.
doi: 10.1111/j.1442-9071.2009.02015.x
27. Thumasupapong, S., Tin, T., Sukontason, K., Sawaddichi, C., and Karbwang, J. (1995).
Electroencephalography in cerebral malaria.Southeast Asian J. Trop. Med. Public
Health 26: 34–37.
28. Smith, J. D., Craig, A. G., Kriek, N., Hudson-Taylor, D., Kyes, S., Fagan, T., et al.
(2000). Identification of a Plasmodium falciparumintercellular adhesion molecule-1
binding domain: a parasite adhesion trait implicated in cerebral malaria. Proc. Natl. Acad.
Sci. U.S.A.97, 1766–1771. doi: 10.1073/pnas.040545897
29. Srinivas. Cerebral Malaria; Malaria site Complications; February 27, 2015
30. Malaria- Treatment. Harvard Health Topics. Drugs.com https://www.drugs.com/health-
guide/malaria.html
31. Geoffrey Pasvol. The treatment of complicated and severe malaria. Oxford Journals;
Medicine & Health; British Medical Bulletin; Volume 75-76, Issue 1; Pp. 29-47
32. Pasvol G, Newton CR, Winstanley PA et al. Quinine treatment of severe falciparum
malaria in African children: a randomized comparison of three regimens. Am J Trop Med
Hyg 1991; 45: 702–13.
33. Ter Kuile F, White NJ, Holloway P et al. Plasmodium falciparum: in vitro studies of the
pharmacodynamic properties of drugs used for the treatment of severe malaria. Exp
Parasitol 1993; 76: 85–95.
34. Newton CR, Crawley J, Sowumni A et al. Intracranial hypertension in Africans with
cerebral malaria. Arch Dis Child 1997; 76: 219–26.
35. Bartoloni A, Zammarchi L (2012). "Clinical aspects of uncomplicated and severe
malaria". Mediterranean Journal of Hematology and Infectious Diseases. 4(1):
e2012026. doi:10.4084/MJHID.2012.026.PMC 3375727. PMID 22708041
338
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
36. Liese C. Koopmans, # Marlies E. van Wolfswinkel et.al., Acute kidney injury in
imported Plasmodium falciparum malaria. Malar J. 2015; 14: 523.Published online 2015
Dec 24. doi: 10.1186/s12936-015-1057-9
37. Naqvi R, Ahmed E, Akhtar F, Naqvi A, Rizvi A. Out come in severe acute renal failure
associated with malaria. Nephrology Dialysis Transplantation 2003; 18:1820-1823.
38. Nand N, Aggarwal H, Sharma M, Singh M. Systemic manifestations of malaria. JIACM
2001; 2:189-94.
39. Mehta KS, Halankar AR, Makwana PD, Torane PP, Satija PS, Shah VB. Severe acute
renal failure in malaria. J Postgrad Med 2001; 47: 24 – 6
40. Panda SK, Das MC, Meher LK, Rathod PK. Risk factors for acute renal failure in severe
falciparum malaria. Indian J Nephrol 2003; 13: 55–8.
41. Eiam-Ong S, Sitprija V. Falciparum malaria and the kidney: a model of inflammation.
Am J Kidney Dis 1998; 32:361-75
42. Saroj Mishra, Bhabani S Das. Malaria and Acute Kidney Injury. Seminars in Nephrology
· July 2008 DOI: 10.1016/j.semnephrol.2008.04.007 · Source: PubMed
43. Kyes S, Horrocks P, Newbold C. Antigenic variation at the infected red cell surface in
malaria. Ann Rev Microbiol. 2001; 55: 673-707.
44. Baruch DI, Pasloske BL, Singh HB, Xiahui B, Ma XC, Feldman M, et al. Cloning of the
P. falciparum gene encoding PfEMP 1, a malarial variant antigen and adherence receptor
on the surface of parasitized human erythrocyte. Cell. 1995; 82: 77-87
45. Pongponratan E, Riganti M, Punpoowong B, Aikawa M. Microvascular sequestration of
parasitized erythrocytes in human falciparum malaria: a pathological study. Am J Trop
Med Hyg. 1991; 44: 168-75
46. MacPherson GG, Warrell MJ, White NJ, Looareesuwan S, Warrell DA. Human cerebral
malaria: a quantitative ultrastructural analysis of parasitized erythrocyte sequestration.
Am J Pathol. 1985; 119: 385-401.
47. RASHAD S. BARSOUM, Malarial Acute Renal Failure. Journal of American Society of
Nephrology. vol. no. 11 2147-2154; November 1, 2000 .
48. Barsoum R: Malarial nephropathies. Nephrol Dial Transplant 13:1588-1597, 1998
49. Mshana RN, Boulandi J, Mshana NM, Mayombo J, Mendome G. Cytokines in the
pathogenesis of malaria: levels of IL-1, IL-4, IL-6, TNF-, and IFN in plasma of healthy
individuals and malaria patients in a holoendemic area. J Clin Lab Immunol. 1991; 34:
131-9.
339
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
50. Day NP, Hien TT, Schollaardt T, Loc PP, Chuong LV, Chau TT, et al. The prognostic
and pathophysiologic role of pro- and anti-inflammatory cytokines in severe malaria. J
Infect Dis. 1999; 180: 1288-97
51. Grau GE, Heremans H, Piguet PF, Pointaire P, Lambert PH, Billiau A, et al. Monoclonal
antibody against interferon gamma can prevent experimental cerebral malaria and its
associated overproduction of tumor necrosis factor. Proc Natl Acad Sci U S A. 1989; 86:
5572-4.
52. Kwiatkowski D, Molyneux ME, Stephens S, Curtis N, Klein N, Pointaire P, et al. Anti-
TNF therapy inhibits fever in cerebral malaria. QJM. 1993; 86: 91-8.
53. Nahrevanian H, Dascombe MJ. Nitric oxide and reactive nitrogen intermediates in lethal
and nonlethal strains of murine malaria. Parasite Immunol. 2001; 23: 491-501.
54. Nahrevanian H, Dascombe MJ. Expression of inducible nitric oxide synthase (iNOS)
mRNA in target organs of lethal and non-lethal strains of murine malaria. Parasite
Immunol. 2002; 24: 471-8.
55. Cumming AD, Driedger AA, McDonald JW, Lindsay RM, Solez K, Linton AI.
Vasoactive hormones in the renal response to systemic sepsis. Am J Kidney Dis 1988; 11:
23–32. 82.
56. Benedict CR, Rose JA. Arterial norepinephrine changes in patients with septic shock.
Circ Shock 1992; 38: 165–72.
57. Pulido-Méndez M, Finol HJ, Girón ME, Aguilar I. Ultrastructural pathological changes in
mice kidney caused by Plasmodium berghei infection. J Submicrosc Cytol Pathol 2006;
38: 143–8.
58. WHO. Severe falciparum malaria. Trans R Soc Trop Med Hyg. 2000; 94 Suppl 1:s1-90
59. Skorecki K, Green J, Brenner BM (2005). "Chronic renal failure". In Kasper DL,
Braunwald E, Fauci AS, et al. Harrison's Principles of Internal Medicine (16th ed.). New
York, NY: McGraw-Hill. pp. 1653-63. ISBN 0-07-139140-1.
60. Tierney, Lawrence M.; Stephen J. McPhee; Maxine A. Papadakis (2004).
"22". CURRENT Medical Diagnosis and Treatment 2005 (44th ed.). McGraw-Hill.
p. 871. ISBN 0-07-143692-8.
61. Biruh T Workeneh, MD, PhD. Acute kidney injury. Oct 31, 2015. MEDSCAPE.
62. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work
Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl
2012; 2:1.
340
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
63. White NJ, Miller KD, Marsh K, Berry CD, et al. Hypoglycemia in African children with
severe malaria. Lancet. 1987; i: 708-11. 97.
64. Das BS, Satpathy SK, Mohanty D, Mohanty S, Mishra SK, Satapathy PC, et al.
Hypoglycaemia in severe falciparum malaria. Trans R Soc Trop Med Hyg. 1988; 82: 197-
201
65. Day NJ, Phu NH, Bethel DP, et al. The effects of dopamine and adrenaline infusions on
acid-base balance and systemic haemodynamics in severe infection. Lancet. 2000; 348:
219-23.
66. Maitland K, Pamba A, English M, Peshu N, Marsh K, Newton C, et al. Randomized trial
of volume expansion with albumin or saline in children with severe malaria: preliminary
evidence of albumin benefit. Clin Infect Dis. 2005; 40: 538-45.
67. Cantarovich F, Rangoonwala B, Lorenz H, Verho M, Esnault VL, High-Dose Furosemide
in Acute Renal Failure Study Group. High-dose furosemide for established ARF: a
prospective, randomized, doubleblind, placebo-controlled, multicenter trial. Am J Kidney
Dis. 2004; 44: 402-9.
68. Kellum JA, Bellomo R, Ronco C. Kidney attack. JAMA. 2012; 307: 2265-66.
69. Korbet SM. Acute peritoneal dialysis prescription. In Handbook of Dialysis. Eds: JT
Dougirdas, Peter G Black, Todd S Ing, 4a Edn. Walters Kluwer- Lippincott Williams &
Wilkins, 4a~dn, 2007; 376-85.
70. Schiff H, Lang SM, Fischer R. Daily dialysis and the outcome of acute renal failure. N
Eng J Med 2002; 346: 305-10.
71. Saroj K ~ishra', Kishore C Mahantaz et.al., Acute Kidney Injury In Malaria - Challenges
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
COMPLICATED MALARIA INDUCED SEVERE ACUTE RENAL
FAILURE: A CASE STUDY
Sai Kiran Polamarasetti*, Uma Sankar Viriti, Sumanjali Podugu, Swetha Gandreti
Avanthi Institute of Pharmaceutical Sciences, Bhogapuram, Vizianagaram,
Andhra Pradesh, India.
other animals caused by parasitic protozoans (a group of single-
celled microorganisms) belonging to the Plasmodium type like
P. vivax, P. falciparum, P.malariae, or P. ovale. If Malaria is neglected
or not treated properly, it may further develop into a severe form
effecting the brain resulting in Cerebral Malaria. Acute Kidney Injury
(AKI) is a known complication of malaria which involves abrupt lose
of kidney function. In this present case, a patient came with the
complaint of fever associated with chills, rigors, altered sensorium and
decreased urine output. He was diagnosed with Complicated malaria
(Cerebral Malaria) induced Acute Kidney Injury, Hyperbilirubinemia
and Cerebral dysfunction. He was given with appropriate treatment, symptomatically relieved
and drug utilization review has been done. Patient was counseled regarding the disease, its
complications, prevalance and importance of medication adherence.
KEYWORDS: Sensorium, Hyperbilirubinemia, Cerebral dysfunction, Plasmodium
falciparum.
INTRODUCTION
DEFINITIONS:
1. MALARIA: Malaria is a mosquito-borne infectious disease affecting humans and other
animals caused by parasitic protozoans belonging to the Plasmodium type like
P. vivax, P. falciparum, P.malariae, or P. ovale. [1]
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 6.041
Volume 5, Issue 10, 315-340 Review Article ISSN 2278 – 4357
*Corresponding Author
DOI: 10.20959/wjpps201610-7784
316
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
2. CEREBRAL MALARIA:- Malaria will develop a severe form, and in these case it effects
brain and diffuse encephalopathy associated with seizures and status epilepticus which can
occur in up to one-third of patients with severe malaria, particularly that caused
by Plasmodium falciparum [2]
3. ACUTE KIDNEY INJURY:- Acute kidney injury (AKI) is the abrupt loss of kidney
function that develops within 7 days. (ARF (serum creatinine level, ≥3 mg/dL or ≥265
μmol/L)). [3]
4. ACUTE TUBULAR NECROSIS (ATN):- This is a medical condition involving
the death of tubular epithelial cells that form the renal tubules of thekidneys. ATN presents
with acute kidney injury (AKI) and is one of the most common causes of AKI [4]
EPIDEMIOLOGY:- Malaria is a major public health problem in tropical countries.
According to the World Malaria Report 2010, there were 225 million cases of malaria and an
estimated 781 000 deaths worldwide in 2009. [5]
About 500 million people suffer from
malaria, leading to death in 1 to 3 million cases. As per World Health Organization criteria,
acute renal failure occurs as a complication of Plasmodium falciparum malaria in less than
1% of cases, but the mortality rate in these cases may be up to 45%. It is more common in
adults than children. [6]
Cerebral malaria (CM) forms part of the spectrum of severe malaria,
with a case fatality rate ranging from 15% in adults in southeast Asia. [7]
Cerebral malaria is
the most severe neurological manifestation of severe malaria. With an incidence of
1,120/100,000/year in the endemic areas of Africa. [8]
CAUSES OF MALARIA: Malaria can occur if a mosquito infected with the
Plasmodium parasite bites you. An infected mother can also pass the disease to her baby at
birth. This is known as congenital malaria. Malaria is transmitted by blood, so it can also be
transmitted through:
An organ transplant
Use of shared needles or syringes. [9]
In humans, malaria is caused by P. falciparum, P. malariae, P. ovale, P. vivax and
P. knowlesi. [10]
317
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
PATHOPHYSIOLOGY OF MALARIA:- Malaria infection develops via two phases: one
that involves the liver (exoerythrocytic phase), and one that involves red blood cells
Erythrocytic phase. These two phases involves rupturing of RBC and invasion hepatic cells
for parasite replication. The rupturing of RBC causes most of the symptoms associated with
malaria as it produces toxicv substances, as the host’s immune system responds to the waste
products produced by the malaria parasites. [12]
CEREBRAL MALARIA:-The P. falciparum parasite displays adhesive proteins on the
surface of the infected blood cells, causing the blood cells to stick to the walls of small blood
vessels, thereby sequestering the parasite from passage through the general circulation and
the spleen. [13]
Sequestered red blood cells can breach the blood–brain barrier and cause
cerebral malaria [14]
SIGNS AND SYMPTOMS OF MALARIA
Plasmodium vivax, ovale and malariae:- The initial symptoms are often similar to those of
influenza:
Plasmodium falciparum:- Malaria caused by Plasmodium falciparum is the most severe form
of malaria. Cerebral malaria is defined as a severe P. falciparum-malaria presenting with
neurological symptoms, including coma (with a Glasgow coma scale less than 11, or
a Blantyre coma scale greater than 3), or with a coma that lasts longer than 30 minutes after a
seizure. [15]
mild jaundice
KIDNEY FAILURE
coma that may last for three days at a stretch
www.wjpps.com Vol 5, Issue 10, 2016.
318
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
rise in intracranial pressure
delirium and seizures [16]
DIAGNOSIS
Laboratory diagnosis of malaria requires the identification of the parasite or its antigens/
products in the patient’s blood.
Current available techniques can be separated in three categories
1. Microscopy
a) THICK AND THIN BLOOD SMEAR STUDY
i) Thick and thin blood smear study:- It is the gold standard method for malaria diagnosis.
ii) Thick smear:- Thick smears are mainly used to detect infection and to estimate
parasitemia.
iii) Thin smear:-Thin smears allow the examiner to identify malaria species, quantify
parasitemia, and recognize parasite forms like schizonts and gametocytes. [17]
b) QUANTATIVE BUFFY COAT (QBC) TEST:- QBC test is easier and faster than
classic peripheral blood smear microscopy but the equipment required is expensive and
species identification and accurate enumeration are impossible.
2. IMMUNOLOGICAL TECHNIQUES
a) ANTIBODY-BASED TECHNIQUES
i) Indirect fluorescent antibody test (IFAT)
ii) Enzyme- linked immunosorbent assay (ELISA):- If the test is positive, the antibody
binds the antigen resulting in a visible colour change. When the test is negative, in the
absence of antibody, there is no change of colour of the substrate.
b) ANTIGEN-BASED TECHNIQUES
i) Rapid Diagnostic Test (RDT)
RDT is a device that can detect malaria antigen in a small amount of blood (5μl) by
immunochromatographic with monoclonal antibodies directed against the parasite antigen.
www.wjpps.com Vol 5, Issue 10, 2016.
319
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
3. MOLECULAR TECHNIQUES
a) Polymerase Chain Reaction (PCR):-Using PCR amplification, it is possible to detect all
4 species of malaria parasites with a reportedly 10-fold greater sensitivity than microscopy .[17]
OTHER TESTS
a) Subjective diagnosis:- Areas that cannot afford laboratory diagnostic tests often use only
a history of subjective fever as the indication to treat for malaria. [18]
b) Differential diagnosis:- In malaria-endemic areas, parasitemia does not ensure a diagnosis
of severe malaria, because parasitemia can be incidental to other concurrent disease. Recent
investigations suggest that malarial retinopathy is better (collective sensitivity of 95% and
specificity of 90%) than any other clinical or laboratory feature in distinguishing malarial
from non-malarial coma. [19]
c) Susceptibility testing:- It is done by testing the DNA of the parasite to detect markers that
indicate resistance.
CEREBRAL MALARIA(CM)
Advanced imaging devices have become increasingly accessible in elucidating the etiology of
CM [20]
damage attributable to inflammatory processes and allows the analysis of neuronal axon
injury during CM [21]
c) COMPUTED TOMOGRAPHY:- Determination of cerebral volume variation and the
detection of infarctions in large vessels [22]
2. INVESTIGATIVE NEURO-IMAGING TOOLS
a) In vivo bioluminescent imaging
In vivo bioluminescent imaging is a versatile and sensitive tool that is based on the detection
of light emission from cells or tissues. [23]
320
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
b) 18
f-fluorodeoxyglucose (fdg) positron emission tomography (pet)
FDG-PET is a non-invasive imaging tool used to map cerebral metabolic activity by
quantifying the uptake of a glucose analog by brain cells. [24]
3. NEW DIAGNOSTIC TOOLS
a) Malarial retinopathy
The sequestration of P. falciparum-infected red blood cells (PRBC) in the cerebral
microvasculature is the hallmark of CM. [25]
ii) Optical Coherence Tomography (OCT):-OCT is an in vivo imaging tool for the
detection of retinal changes. [26]
4. ELECTROENCEPHALOGRAPHY (EEG) AND MICRO-EEG
a) EEG
This non-invasive technique to record electrical impulses of the brain by measuring voltage
fluctuations. [27]
5. BIOMARKERS:- Biomarkers include tools and technologies that can facilitate the
prediction, cause, diagnosis, progression, regression, or outcome of treatment of disease. [28]
MANAGEMENT
Modes of Treatment: Two important concepts in the treatment of malaria are suppressive
and radical treatments.
i) SUPPRESSIVE TREATMENT: The symptoms of malaria can be alleviated by
suppressing the erythrocytic stage of the parasitic development. Suppressive therapy involves
administration of appropriate blood schizonticidal drugs.
ii) RADICAL TREATMENT: Radical treatment is administration of primaquine to all
confirmed cases of malaria.
In P. vivax malaria, 2 weeks’ therapy with primaquine completely cures the infection in
the host by its tissue schizonticidal activity and thereby prevents relapses.
In P. falciparum malaria, a single dose of primaquine destroys the gametocytes, thereby
prevents the spread of the infection into the mosquito [29]
The drugs available to treat malaria include: Chloroquine, Quinine,
Hydroxychloroquine (Plaquenil), Artemether and lumefantrine (Coartem), Atovaquone
321
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
(Mepron), Proguanil (sold as a generic), Mefloquine, Clindamycin (Cleocin) and
Doxycycline.
People with falciparum malaria have the most severe symptoms. People
with falciparum malaria may need to be monitored in the intensive care unit of a hospital
during the first days of treatment because the disease can cause breathing failure, coma
and kidney failure [30]
TREATMENT FOR SEVERE OR COMPLICATED MALARIA
i) ANTIMALARIALS:- All patients with any form of complicated or severe disease should
be treated parenterally. The choice of drugs, according to availability and licensing, lies
between the cinchona alkaloids, i.e. quinine or quinidine (in the USA), or one of the
artemisinin derivatives, preferably intravenous artesunate. [31]
ii) QUININE:- Since the advent of chloroquine resistance, quinine has been the drug of
choice for the parenteral treatment of malaria. Quinine is given by slow intravenous infusion
but in an emergency may be given intramuscularly in split doses as has been done in
children. [32]
iii) ARTEMISININ AND ITS DERIVATIVES:- Artemisinin derivatives are increasingly
being used in the treatment of malaria of all degrees of severity. Artemisinins, especially
artesunate and artemether, result in more rapid parasite clearance (being active on the
immature parasite forms. [33]
In children with cerebral malaria and evidence of raised intracranial pressure, mannitol (1 g
kg −1
infused over 30 min as a 10 or 20% solution) has been shown to control intermediate
intracranial hypertension, but not when severe (>40 mmHg) 34
.
Life-threatening situations because of malaria infection with P. falciparum may include:
Severe infection of the brain (cerebral malaria), with seizures, confusion, and increasing
tiredness leading to coma and death.
Fluid in the lungs (pulmonary edema)
Abnormal liver function
Low blood sugar (hypoglycemia).
Altered blood chemistry, including low sodium and lowered pH (lactic acidosis)
322
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
Blackwater fever
MALARIA INDUCED ACUTE KIDNEY INJURY/ACUTE KIDNEY FAILURE
This is also indicated as ‘Malarial Nephropathy’. Acute kidney injury (AKI) is a known
complication of malaria, and is reported to occur in up to 40 % of adult patients with a
severe Plasmodium falciparum infection in endemic regions. [36]
Infection with the
urinary abnormalities and mild electrolyte imbalance to acute renal failure. Renal failure is
multifactorial and carries a high mortality and morbidity [37]
Over a decade ago, cerebral
malaria was the predominant manifestation of severe malaria, where as today the
combination of jaundice and renal failure are more common. [38]
PREVALANCE:- Prevalence of ARF in malaria all over the world has been reported as
0.57% to 60% . In Southeast Asia there is an upsurge in the overall incidence of malarial
ARF and has been reported in between 13% to 17.8%. [39]
RISK FACTORS OF OCCURING AKI IN MALARIAL PATIENTS
Immuno-compromised patients (Elderly or infants)
Pathogen/Parasitic overload
Kidney trauma or injury
Pregnant women
Poor people due to lack of effective treatment
Over use of medicines that are highly burden to the kidneys
Multi-organ dysfunction. [40]
PATHOGENESIS:- The pathogenesis of AKI in falciparum malaria is not clearly known.
Several factors; including various chemical mediators, catecholamine release, cytoadherence
of parasitized erythrocytes, dehydration, intravascular haemolysis, intravascular coagulation,
sepsis hyprebilirubinaemia and hyperparasitaemia have been implicated in the pathogenesis
of ARF in malaria. [41]
Malarial complications possibly are caused by the interaction of the
323
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
parasite with the host, resulting in mechanical, immunologic, and humoral responses. These
responses, while attempting to eliminate the parasites, may also injure the host tissues. [42]
CYTOADHERENCE
The pathogenesis of severe P falciparum malaria is attributed in part to the cytoadherence of
parasitized red blood cells (PRBCs) to the vascular endothelial cells in different host
organs. [43]
Parasite proteins referred to as variant surface antigens expressed on the PRBC
surface mediate the adhesion of infected erythrocytes to host vascular endothelial
receptors. [44]
PRBCs preferentially sequester in the deep vascular beds of vital organs,
including the brain, liver, lung, spleen, intestine, and kidney. [45]
Sequestration of PRBCs in
glomerular and tubulointerstitial capillaries has been shown, although at a lesser degree than
the cerebral vessels. [46]
features in plasmodium infections: hemodynamic, immunologic, and metabolic
perturbations. [47]
Principal pathogenic pathways in severe falciparum malaria was mentioned in the above
fig.1. [48]
CYTOKINES, REACTIVE OXYGEN SPECIES, AND NITROGEN SPECIES
Literature on the influence of cytokine concentrations on renal pathology in malaria is scanty
although cytokines, reactive oxygen intermediates, and nitrogen intermediates (ROI and NO)
play an important role in both protection against malaria and pathogenesis of severe malaria.
Levels of inflammatory cytokines, such as tumor necrosis factor (TNF-α), interferon- γ, and
interleukins 1-α, -6, and -8 are increased in malaria. [49]
Higher blood concentrations of
proinflammatory cytokines have been observed in severe complications of malaria. [50]
Anti–
TNF-α and anti–interferon γ- antibodies are reported to abolish the onset of cerebral
www.wjpps.com Vol 5, Issue 10, 2016.
324
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
malaria [51]
However, in contrast to observations in the murine model, monoclonal antibodies
to Malaria and AKI 397 TNF- ameliorate fever but not the manifestations of human cerebral
malaria [52]
An early increase in NO stimulates the helper T-cell-1 (Th1) response to control
parasitemia similar to natural immunization during malaria infection. [53]
Whereas a late
increase in NO production in the liver and spleen appear to have pathologic consequences.
Regulatory functions of NO are dependent on the presence of various isoforms of the enzyme
nitric oxide synthase (NOS). Physiologic function of NO is regulated by low basal
concentrations synthesized by constitutive NOS isoforms. A high concentration of NO
usually is produced by inducible NOS isoforms (iNOS), which play a crucial role in
pathologic consequences. Increased iNOS activity and production of NO have been observed
in severe malaria. [54]
RESTRICTED LOCAL BLOOD FLOW IN THE KIDNEYS:- This is considered as a
major contributor for malarial ARF. Low intake of fluids, loss of fluids because of vomiting
and pyrexial sweating may be responsible for dehydration and renal ischemia. Administration
of intravenous fluids often worsens the general condition of the patient by inducing
pulmonary edema, a situation similar to shock like syndrome. A generalized vasodilatation
with an associated decrease in systemic vascular resistance is considered an important
contributor for septic shock as well as malarial ARF. Vasodilatation leads to activation of
sympathetic nervous system, rennin-angiotensin-aldosterone axis (RAAA), and release of
vasopressin for maintaining the falling blood pressure. Unfortunately, these compensatory
mechanisms may worsen the renal pathology leading to overt ARF. [55,56]
LOW INTAKE OF FLUIDS, LOSS OF FLUIDS:-Because of vomiting and pyrexial
sweating, cytokine and NO mediated arterial vasodilatation specifically organ specific release
of NO, resistance to vasoactive hormones, cytopathic hypoxia leading to decreased ATP
synthesis, cytoadherence of PRBCs, etc all may contribute singly or in combination towards
malarial ARF. Increased fluid administration, oxygen toxicity, and yet unidentified factors
may contribute to pulmonary edema, acute respiratory distress syndrome (ARDS), multiorgan
failure and death. [57]
SIGNS AND SYMPTOMS
An absolute increase in serum creatinine level of 0.3 mg/dL or more (26.4 mol/L)
A percentage increase in serum creatinine level of 50% or more (1.5-fold from baseline)
www.wjpps.com Vol 5, Issue 10, 2016.
325
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
A reduction in urine output (documented oliguria of 0.5 mL/kg/h for 6 hours). [58]
Swelling in legs, ankles, and around the eyes
nausea and vomiting
Chest pain or pressure
Fluid imbalances. [60]
DIAGNOSIS
The following tests can aid in the diagnosis and assessment of AKI:
Kidney function studies: Increased levels of blood urea nitrogen (BUN) and creatinine are
the hallmarks of renal failure
Complete blood count
Fractional excretion of sodium and urea
Bladder pressure: Patients with a bladder pressure above 25 mm Hg should be suspected
Ultrasonography
Aortorenal angiography : Can be helpful in establishing the diagnosis of renal vascular
diseases, such as renal artery stenosis, renal atheroembolic disease, atherosclerosis with
aortorenal occlusion, and certain cases of necrotizing vasculitis (eg, polyarteritis nodosa)
Renal biopsy: Can be useful in identifying intrarenal causes of AKI. [61]
urinalysis
Estimated glomerular filtration rate (eGFR)
AKI can be diagnosed if any one of the following is present:
Increase in SCr by ≥0.3 mg/dl (≥26.5 μmol/l) within 48 hours; or
Increase in SCr to ≥1.5 times baseline, which have occurred within the prior 7 days; or
Urine volume < 0.5 ml/kg/h for 6 hours. [62]
www.wjpps.com Vol 5, Issue 10, 2016.
326
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
MANAGEMENT
The management of MAKI needs careful and meticulous management of several problems.
Early and prompt decisions and institutions are the hallmark of a better prognosis. The
outlines of treatment guidelines include the following:
1. institution of appropriate antimalarials
2. maintenance of fluid and electrolyte levels
3. renal replacement therapy as indicated
4. treatment of associated complications and
5. management of infection including pneumonia.
ANTIMALARIA DRUGS:- The preferred antimalarial is artesunate or quinine given
parenterally. Intravenous quinine has remained as the time-tested first-line drug. The dose is
10 mg/kg/body weight. If quinine has not been given in the previous 7 days, a loading dose
may be given. But it is very diffi- cult to get a definite history, hence it is advisable to start a
maintenance dose of 10 mg/kg of body weight every 8 hours. The dose for the initial 48 hours
should never be modified, even in the presence of AKI. [63,64]
The use of other drugs, namely
chloroquine or sulfadoxine pyrimethamine, should be avoided owing to widespread
resistance from areas where CM and AKI are common.
FLUID CHALLENGE
Many patients with oligura are dehydrated. They should receive fluid, up to 20 mL/kg of
0.9% saline infused over 60 minutes. To prevent fluid overload, auscultation of the lungs and
jugular venous pressure measurements (and, if possible, CVP measurements) should be
performed after every 200 mL of fluid. The CVP should always be kept between 0 and ±5. If
there is no urine output after fluid replacement, an intravenous diuretic challenge may be
given. [58]
DOPAMINE CHALLENGE
The use of dopamine for the prevention and treatment of AKI has not yet been established. Its
use is based on the understanding that selective renal vasodilatation will occur when it is
infused at a low dose. In a prospective, controlled, cross-over trial in an intensive care unit of
an infectious diseases hospital in Vietnam, dopamine at a renal dose (2.5 g/kg/min) was
associated with a mean (95% confidence interval) fractional increase in the absolute renal
blood flow (RBF) index of 37% (13% to 61%) and in RBF as a fraction of cardiac output of
35% (10%-59%; P = .007 and P = .014, respectively). [65]
www.wjpps.com Vol 5, Issue 10, 2016.
327
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
VASOPRESSIN THERAPY
As discussed in the pathogenesis, there appears to be a future role for the use of vasopressin
in the management of malarial shock as well as MAKI.
ALBUMIN INFUSION
The administration of albumin for volume expansion reduces mortality rates. [66]
DIURETIC CHALLENGE
The loop diuretic (frusemide 40 mg or bumetanide 1 mg) is given initially. If urination does
not occur, further diuretic challenge can be tried at every 30-minute intervals with
incremental doses (frusemide 100, 200, and 400 mg or bumetanide 2, 4, and 6 mg). If there is
still no urine flow, dopamine 2.5 to 5 g/kg/min may be tried [67]
RENAL REPLACEMENT THERAPY:- It should be initiated if any of the following is
present
b. Uraemic symptoms (Encephalopathy or pericarditis)
c. Fluid overload, pulmonary edema, congestive heart failure or Pericardial rub [68]
DIALYSIS:- Dialysis has improved the survival of the AKI cases when instituted early in the
course. It can be intermittent haemodialysis (daily or alternate day), or continuous
venovenous haemofiltration (CVVH) or arteriovenous haemofiltration (CAVH). Often
haemodialysis (HD) is performed in patients with AKI as Peritoneal dialysis (PD) is
considered to be less effective in controlling biochemical abnormalities than HD. Thus,
whenever RRT is indicated, either PD or HD should be started as early as possible.
FREQUENCY OF DIALYSIS:-
Intermittent HD should be performed daily for better prognosis in acute renal failure.
Mortality is reduced in patients receiving six dialyses per week as opposed to those receiving
HD every other day. [69,70]
MANAGEMENT OF DIURETIC PHASE:-
Diuretic phase may return gradually or in a few hours. Careful attention needs to be given
towards fluid and electrolyte requirements. In addition, repeated estimation of Na, K and
bicarbonate is essential.
328
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
NUTRITION: Suppressing endogenous protein catabolism by providing fat and
carbohydrates is recommended. In patients without dialysis, protein restriction is advised,
whereas those undergoing daily HD may require additional proteins. [75]
CASE STUDY
A patient of age 60years male was admitted in King George Hospital Visakhapatnam, Andhra
Pradesh, India, with a complaint of fever since 10 days and altered sensorium since 1day.
History of present illness: Patient was apparently normal 10 days before. Later he developed
fever and yellowish discoloration from 10days. Fever was found to be high grade,
intermittent and associated with chills and rigors, associated with headache. There is
decreased output of urine from 4days. Last day urine output increased. Altered sensorium is
observed last day.
Patient experienced cough with expectoration since 5 days and breathlessness since 3 days.
On examination patient experienced altered seizures.
There is no history of hematuria/pyuria/dysuria/vomiting/diarrhea/pedal edema/facial
puffiness.
Patient didn’t experience any of the above present complaints in the past.
Personal history was found to be alcoholic, smoker and takes mixed diet.
On the day of admission, patient’s blood pressure was found to be 140/50mm of Hg, Pulse
rate 80/min, Respiratory rate 15/min and temperature was afebrile.
On examination by using Glasgow coma scale, measures were done to estimate brain
function. Results were found to be E2, V1, M4. These scores explain that:
E2 - means eye opening to pain
V1- means no verbal response
M4 - means motor response withdraws to pain
On addition of scores of E.V and M we get 2+1+4=7, it shows that severe brain injury.
[3-8 = severe brain injury
9-12=moderate brain injury
13-15= mild brain injury]
329
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
RBC- normocytic, hypochromic with mild anisocytes
WBC- count is increased and neutrophilia is seen
Platelets- adequate
Basing on these it was found that normocytic, hypochromic anemia with neutrophilic
leukocytosis
Blood urea levels: 199 mg/dl (normal: 14-45)
Serum bilirubin total: 18.4 mg% (0.3 to 1.0 mg%)
SGOT: 74 U/L (Normal: 5-40 U/L)
SGPT: 50 U/L (Normal: 7-56 U/L)
Serum Alkaline Phosphate: 348 U/L (Normal level for 56-60 years: 46-118 U/L)
Patient exhibited sensorium, seizures (E2 V1 M4) and Plasmodium falsiparum positive. So he
was diagnosed as CEREBRAL MALARIA and CEREBRAL DYSFUNCTION.
Total Bilirubin levels are abnormal. So the patient was concluded of having
HYPERBILIRUBINEMIA.
Serum creatine levels are abnormally high. Previously patient has no complaint of Renal
problems. But after getting Malaria, he was tested for serum creatine levels and was
concluded that he is having renal impairment so that his serum creatine levels are abnormal.
Basing on this he was diagnosed of having ACUTE KIDNEY INJURY induced by
MALARIA.
FINAL DIAGNOSIS
By observing the above diagnostic tests patient was diagnosed as suffering with CEREBRAL
MALARIA WITH ACUTE KIDNEY INJURY, HYPERBILIRUBINEMIA, CEREBRAL
and DYSFUNCTION
TREATMENT
On the first day of treatment patient was given with Inj.falcigo( artesunate) 120mg IV BD ,
Inj.clindamycin 600mg IV BD, Inj.pantop(pantoprazole) 40mg IV OD, Tab.paracetamol
500mg QID, IVF( intravenous fluid) 25%dextrose IV TID.
On 2 nd
day, patient exhibited altered sensorium. Same drugs that are Inj.falcigo( artesunate)
120mg IV BD, Inj.clindamycin 600mg IV BD, Inj.pantop(pantoprazole) 40mg IV OD, Tab.
paracetamol 500mg QID, IVF( intravenous fluid) 25%dextrose IV TID were continued.
Dialysis is done by using bicarbonate dialysate.
www.wjpps.com Vol 5, Issue 10, 2016.
330
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
On 3 rd
day, BP-160/100mm of Hg, PR-96/min and abdominal examination shows diffuse
tenderness. Patient was given with drugs like Tab.Nicardia Retard( nifedipine) 10mg BD,
Tab.Falcigo 120mg IV OD, Tab.Clindamycin 600mg IV BD, Inj.Pantop 40 mg IV OD and
Tab. B complex OD.
On 4 th
day, patient is conscious and coherent and found to be afebrile. BP is 140/80 mm of
Hg and PR is 92/min. Same drugs continued, that are Tab.Nicardia Retard( nifedipine) 10mg
BD, Tab.Falcigo 120mg IV OD, Tab.Clindamycin 600mg IV BD, Inj.Pantop 40 mg IV OD
and Tab. B complex OD.
On 5 th
day, patient is conscious and coherent and found to be afebrile. BP is 140/90 mm of
Hg, PR is 72/min and abdomen is soft. Drugs like Tab.Nicardia Retard( nifedipine) 10mg
BD, Tab.Falcigo 120mg IV OD, Tab.Clindamycin 600mg IV BD, Inj.Pantop 40 mg IV OD
and Tab. B complex OD were given. Patient is given IVF ( intra venous fluid) 25% dextrose
in 100 ml. dialysis was done using bicarbonate dialysate.
On 6 th
day, patient is conscious and coherent and found to be afebrile. BP is 140/80 mm of
Hg, PR is 74/min and abdomen is soft. Drugs like Tab.Nicardia Retard( nifedipine) 10mg
BD, Tab.Falcigo 120mg IV OD, Tab.Clindamycin 600mg IV BD, Inj.Pantop 40 mg IV OD
and Tab. B complex OD were given. Patient is given IVF (intra venous fluid) 25% dextrose
in 100 ml. dialysis was done using bicarbonate dialysate. Syrup.lactulose 15ml TID and
Inj.opitneuron 10 ml in 100 ml normal saline IV OD is given.
On 7 th
day, patient exhibited fever, BP is 120/80 mm of Hg and PR is 78/min. same drugs
were continued. But dialysis is not done.
On 8 th
day, patient was found to be afebrile, BP is 120/80 mm of Hg and PR is 82/min. same
drugs were continued but syrup lactulose is replaced with syrup duphalac 15ml TID.
On 9 th
day, BP is 120/80 mm of Hg and PR is 90/min. Drugs like Inj.falcigo 120mg IV OD,
Inj.clinamycin 600mg IV BD, Inj.pantop 40 mg OD, Tab.Nicardia Retard 20 mg BD, Tab.
Bcomplex and Tab. Calcium.
On 10 th
day, patient was given with Tab. Nicardia Retard 20 mg BD, Tab. B complex OD,
Tab. Calcium BD and Tab. IFA ( iron folic acid) OD were given.
On 11 th
day, patient vitals are normal and was given with Tab. Nicardia Retard 20 mg BD,
Tab. B complex OD, Tab. Calcium BD and Tab. IFA ( iron folic acid) OD were given.
On 12 th
day, patient was given with Tab. Nicardia Retard 20 mg BD, Tab. B complex OD,
Tab. Calcium BD and Tab. IFA ( iron folic acid) OD were given.
www.wjpps.com Vol 5, Issue 10, 2016.
331
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
On 13 th
day, patient exhibited fever. So Tab. Paracetomol 500mg SOS along with Tab.
Nicardia Retard 20 mg BD, Tab. B complex OD, Tab. Calcium BD and Tab. IFA ( iron folic
acid) OD were given.
On 14 th
day, patient exhibited fever, BP is 130/90 mm of Hg and PR is 78/min and RR is
20/min. His urine output is >600ml. Blood pressure was controlled so nicardia retard drug has
stopped. Tab. B complex OD, Tab. Calcium+ vit D3 OD, Tab. IFA ( iron folic acid) OD, Tab.
Pantop 40 mg OD and Tab. Paracetomol 500mg SOS are given. Dialysis was done using
bicarbonate dialysate.
On 15 th
day, patient vitals are normal i.e., BP is 130/80 mm of Hg and PR is 84/min and RR
is 18/min. Paracetomol was withdrawn and same drugs are given. But dialysis is not done.
On 16 th
day, patient vitals are normal and his urine output is 1 liter.Drugs like Tab. B
complex OD, Tab. Calcium+ vit D3 OD, Tab. IFA ( iron folic acid) OD, Tab. Pantop 40 mg
OD and Tab. Paracetomol 500mg SOS are given.
On 17 th
day, patient vitals are normal i.e., BP is 120/80 mm of Hg and PR is 82/min and RR
is 22/min. His urine output is 1.8 liters. So drugs like Tab. B complex OD, Tab. Calcium+ vit
D3 OD, Tab. IFA ( iron folic acid) OD, Tab. Pantop 40 mg OD and Tab. Paracetomol 500mg
SOS are given.
On 18 th
day, patient was prescribed with Tab. B complex OD, Tab.Calcium+ vit D3 OD, Tab.
IFA ( iron folic acid) OD, Tab. Pantop 40 mg OD.
On 19 th
day, patient vitals are normal and his urine output is 1.6 liters. Same drugs were
continued.
On 20 th
day, patient is conscious and coherent and found to be afebrile. BP is 120/70 mm of
Hg, PR is 84/min and abdomen is soft. His Urine Output is 1.8 liters.He was prescribed with
Tab. B complex OD, Tab.Calcium+ vit D3 OD, Tab. IFA ( iron folic acid) OD, Tab. Pantop
40 mg OD..
On 21 st
day, patient vitals are normal and his urine output is 1.2 liters. On 22 nd
day, patient’s
Urine output was 2 liters and was given with Tab. Rantac 150mg BD, Cap. IFA ( iron folic
acid) OD, Tab.Calcium+ vit D3 OD and Tab. B complex OD.
On 23 rd
day, patient’s Urine output was 1.8 liters. Drugs like Tab. Rantac 150mg BD, Cap.
IFA ( iron folic acid) OD, Tab.Calcium+ vit D3 OD and Tab. B complex OD were given.
On 24 th
day, patient’s Sr.Cr. levels are 1.7mg/dl and blood urea was 45mg/dl. Patient was
generally improved, vitals are stabilized and urine output is also improved. So, he was
discharged under stable, general conditions and advised to attend nephrology OPD at regular
follow ups.
332
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
DISCUSSION: A 60 years old male patient came with a complaint of fever since 10 days
and altered sensorium since 1 day. He was diagnosed as suffering with Cerebral Malaria with
Acute Kidney Injury, Hyperbilirubinemia and Cerebral dysfunction. So he was given with
Inj.Falcigo 120mg IV. Falcigo (Aetesunate) is an anti-malarial drug. Artemisinins and
cinchona alkaloids are the only classes used to treat severe malaria. So intravenous artesunate
was given to treat cerebral malaria. Clindamycin 600mg IV BD was given inorder to treat the
Complicated Malaria. Tab. Paracetomol 500mg QID is given as the patient exhibited Fever.
Nicardia Retard (Nifedepine) 10mg BD is given in order to treat blood pressure due to Acute
Kidney Injury(AKI) which relaxes smooth muscle and produces vasodilation, which in turn
improves blood flow and oxygen delivery. Pantop (Pantoprazole) is a proton pump
inhibitor that decreases the amount of acid produced in the stomach. Tab B complex, Iron
folic acid supplements are mainly given as having chronic kidney disease changes the need
for some nutrients, their absorption or their utility and some may lost during dialysis.
Optineuron is for relaxing the nerve signals to the brain. Patient was haemodialysed 5 times
along with packed cell transfusion. Patient general condition was improved, vitals are
stabilized and urine output is improved after 20 days of hospital admission. He was
discharged with medications Tab. B complex OD, Tab.Calcium+ vit D3 OD and Tab. IFA (
iron folic acid) OD.
333
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
2. HOSPITAL CONSENT FORM
334
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
5. CONSENT FORM
CONCLUSION
Malaria is a mosquito-borne infectious disease which is a major public health problem caused
by parasitic protozoans belonging to the Plasmodium type like P. vivax, P. falciparum,
P.malariae, or P. ovale. If this condition is neglected or untreated it may get complicated and
effects brain(Cerebral Malaria). Acute kidney injury (AKI) is the abrupt loss of kidney
function which is also a complication of malaria. Present case was apparently normal 10 days
before. Later he developed fever, decreased urine output and altered sensorium. He was
diagnosed as suffering with Cerebral malaria with acute kidney injury, hyperbilirubinemia
and cerebral dysfunction. Given with appropriate treatment, the patient was found to be
relieved from symptoms. Patient was explained about the disease condition and its
assosciated complications, importance of medication adherence and discharged with
medication.From this case, it is cleared that if Malaria is neglected, it becomes complicated
and may be fatal. In every malaria case, serum creatinine levels should be checked
compulsorily. If it is correctly treated in right time with right medication, the quality and well
being of the patient can be improved.
www.wjpps.com Vol 5, Issue 10, 2016.
335
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
ACKNOWLEDGEMENT
The author likes to express his gratitude towards the Physicians of King George Hospital
especially Nephrology Department, King George Hospital and Avanthi Institute of
Pharmaceutical Sciences for continuous support.
REFERENCES:-
1. "Malaria Fact sheet N°94". WHO. March 2014. Retrieved 28 August 2014.
2. Indian J Crit Care Med. 2008 Oct-Dec; 12(4): 204–205. doi: 10.4103/0972-5229.45084.
3. Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, Levin A
(2007). "Acute Kidney Injury Network: report of an initiative to improve outcomes in
acute kidney injury". Critical Care (London, England). 11 (2):
R31. doi:10.1186/cc5713.PMC 2206446 . PMID 17331245.
4. "Acute Tubular Necrosis (ATN)". Nephrology Channel. HealthCommunities.com. 2008.
Retrieved 2008-09-23.
5. World Malaria Report. 2010; p. 60.
6. Mishra SK, Das BS.Malaria and acute kidney injury. Semin Nephrol. 2008 Jul;28(4):395-
408. doi: 10.1016/j.semnephrol.2008; 04: 007.
7. Georges Emile Raymond Grau; Alister Gordon Craig. Cerebral Malaria Pathogenesis.
Future Microbiol. 2012; 7(2): 291-302. Medscape.
8. Breman JG, Am J . The ears of the hippopotamus: manifestations, determinants, and
estimates of the malaria burden. Trop Med Hyg. 2001 Jan-Feb; 64(1-2 Suppl): 1-11.
9. Darla Burke. Malaria. Reference Library. Healthline. December 14, 2015.
10. Collins WE (2012). "Plasmodium knowlesi: A malaria parasite of monkeys and
humans". Annual Review of Entomology. 57: 107–21. doi:10.1146/annurev-ento-121510-
133540. PMID 22149265.
11. Bledsoe GH (2005). "Malaria primer for clinicians in the United States". Southern
Medical Journal. 98(12): 1197–204; quiz 1205, 1230.
doi:10.1097/01.smj.0000189904.50838.eb. PMID 16440920.
12. Vaughan AM, Aly AS, Kappe SH (2008). "Malaria parasite pre-erythrocytic stage
infection: Gliding and hiding". Cell Host & Microbe. 4(3): 209–18.
doi:10.1016/j.chom.2008.08.010. PMC 2610487. PMID 18779047
13. Tilley L, Dixon MW, Kirk K (2011). "The Plasmodium falciparum-infected red blood
cell". International Journal of Biochemistry and Cell Biology. 43(6): 839-42. Doi:
10.1016/j.biocel.2011.03.012. PMID 21458590.
336
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
14. Rénia L, Wu Howland S, Claser C, Charlotte Gruner A, Suwanarusk R, Hui Teo T,
Russell B, Ng LF (2012). "Cerebral malaria: mysteries at the blood-brain
barrier". Virulence. 3(2):193201.doi:10.4161/viru.19013. PMC 3396698.
PMID 22460644.
15. WHO (2010). Guidelines for the Treatment of Malaria (PDF) (Report) (2nd ed.). World
Health Organization. ISBN 978-9-2415-4792-5.
16. Bushra Kafeel. Malaria-Symptoms of cerebral malaria. Blood diseases; Only my health.
http://www.onlymyhealth.com/signs-symptoms-cerebral-malaria-1300864141
http://www.malwest.gr/enus/malaria/informationforhealthcareprofessionals/laboratorydia
gnosis.aspx
18. Redd S, Kazembe P, Luby S, Nwanyanwu O, Hightower A, Ziba C, Wirima J, Chitsulo
L, Franco C, Olivar M (2006). "Clinical algorithm for treatment ofPlasmodium
falciparum malaria in children". Lancet. 347(8996): 223–7. doi: 10.1016/S0140-
6736(96)90404-3.PMID 8551881.
19. Beare NA, Taylor TE, Harding SP, Lewallen S, Molyneux ME (November
2006). "Malarial retinopathy: a newly established diagnostic sign in severe malaria". Am.
J. Trop. Med. Hyg. 75(5): 790–7.PMC 2367432 . PMID 17123967.
20. Praveen K. Sahu 1 , Sanghamitra Satpathi
2 et al., Pathogenesis of cerebral malaria: new
diagnostic tools, biomarkers, and therapeutic approaches. Front. Cell. Infect. Microbiol.,
27 October 2015 http://dx.doi.org/10.3389/fcimb.2015.00075
21. Kennan, R. P., Machado, F. S., Lee, S. C., Desruisseaux, M. S., Wittner, M., Tsuji, M., et
al. (2005). Reduced cerebral blood flow and N-acetyl aspartate in a murine model of
cerebral malaria. Parasitol. Res. 96, 302–307. doi: 10.1007/s00436-005-1349-z
22. Potchen, M. J., Birbeck, G. L., Demarco, J. K., Kampondeni, S. D., Beare, N., Molyneux,
M. E., et al. (2010). Neuroimaging findings in children with retinopathy-confirmed
cerebral malaria. Eur. J. Radiol. 74, 262–268. doi: 10.1016/j.ejrad.2009; 02: 010
23. Franke-Fayard, B., Waters, A. P., and Janse, C. J. (2006). Real-time in vivo imaging of
transgenic bioluminescent blood stages of rodent malaria parasites in mice. Nat. Protoc. 1,
476–485. doi: 10.1038/nprot.2006; 69
24. Sugiyama, M., Ikeda, E., Kawai, S., Higuchi, T., Zhang, H., Khan, N., et al. (2004).
Cerebral metabolic reduction in severe malaria: fluorodeoxyglucose-positron emission
337
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
tomography imaging in a primate model of severe human malaria with cerebral
involvement. Am. J. Trop. Med. Hyg. 71, 542–545.
25. Beare, N. A., Taylor, T. E., Harding, S. P., Lewallen, S., and Molyneux, M. E. (2006).
Malarial retinopathy: a newly established diagnostic sign in severe malaria. Am. J. Trop.
Med. Hyg. 75, 790–797. doi: 10.1016/j.idcr.2014; 10: 003
26. Sakata, L. M., Deleon-Ortega, J., Sakata, V., and Girkin, C. A. (2009). Optical coherence
tomography of the retina and optic nerve - a review. Clin. Exp. Ophthalmol. 37, 90–99.
doi: 10.1111/j.1442-9071.2009.02015.x
27. Thumasupapong, S., Tin, T., Sukontason, K., Sawaddichi, C., and Karbwang, J. (1995).
Electroencephalography in cerebral malaria.Southeast Asian J. Trop. Med. Public
Health 26: 34–37.
28. Smith, J. D., Craig, A. G., Kriek, N., Hudson-Taylor, D., Kyes, S., Fagan, T., et al.
(2000). Identification of a Plasmodium falciparumintercellular adhesion molecule-1
binding domain: a parasite adhesion trait implicated in cerebral malaria. Proc. Natl. Acad.
Sci. U.S.A.97, 1766–1771. doi: 10.1073/pnas.040545897
29. Srinivas. Cerebral Malaria; Malaria site Complications; February 27, 2015
30. Malaria- Treatment. Harvard Health Topics. Drugs.com https://www.drugs.com/health-
guide/malaria.html
31. Geoffrey Pasvol. The treatment of complicated and severe malaria. Oxford Journals;
Medicine & Health; British Medical Bulletin; Volume 75-76, Issue 1; Pp. 29-47
32. Pasvol G, Newton CR, Winstanley PA et al. Quinine treatment of severe falciparum
malaria in African children: a randomized comparison of three regimens. Am J Trop Med
Hyg 1991; 45: 702–13.
33. Ter Kuile F, White NJ, Holloway P et al. Plasmodium falciparum: in vitro studies of the
pharmacodynamic properties of drugs used for the treatment of severe malaria. Exp
Parasitol 1993; 76: 85–95.
34. Newton CR, Crawley J, Sowumni A et al. Intracranial hypertension in Africans with
cerebral malaria. Arch Dis Child 1997; 76: 219–26.
35. Bartoloni A, Zammarchi L (2012). "Clinical aspects of uncomplicated and severe
malaria". Mediterranean Journal of Hematology and Infectious Diseases. 4(1):
e2012026. doi:10.4084/MJHID.2012.026.PMC 3375727. PMID 22708041
338
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
36. Liese C. Koopmans, # Marlies E. van Wolfswinkel et.al., Acute kidney injury in
imported Plasmodium falciparum malaria. Malar J. 2015; 14: 523.Published online 2015
Dec 24. doi: 10.1186/s12936-015-1057-9
37. Naqvi R, Ahmed E, Akhtar F, Naqvi A, Rizvi A. Out come in severe acute renal failure
associated with malaria. Nephrology Dialysis Transplantation 2003; 18:1820-1823.
38. Nand N, Aggarwal H, Sharma M, Singh M. Systemic manifestations of malaria. JIACM
2001; 2:189-94.
39. Mehta KS, Halankar AR, Makwana PD, Torane PP, Satija PS, Shah VB. Severe acute
renal failure in malaria. J Postgrad Med 2001; 47: 24 – 6
40. Panda SK, Das MC, Meher LK, Rathod PK. Risk factors for acute renal failure in severe
falciparum malaria. Indian J Nephrol 2003; 13: 55–8.
41. Eiam-Ong S, Sitprija V. Falciparum malaria and the kidney: a model of inflammation.
Am J Kidney Dis 1998; 32:361-75
42. Saroj Mishra, Bhabani S Das. Malaria and Acute Kidney Injury. Seminars in Nephrology
· July 2008 DOI: 10.1016/j.semnephrol.2008.04.007 · Source: PubMed
43. Kyes S, Horrocks P, Newbold C. Antigenic variation at the infected red cell surface in
malaria. Ann Rev Microbiol. 2001; 55: 673-707.
44. Baruch DI, Pasloske BL, Singh HB, Xiahui B, Ma XC, Feldman M, et al. Cloning of the
P. falciparum gene encoding PfEMP 1, a malarial variant antigen and adherence receptor
on the surface of parasitized human erythrocyte. Cell. 1995; 82: 77-87
45. Pongponratan E, Riganti M, Punpoowong B, Aikawa M. Microvascular sequestration of
parasitized erythrocytes in human falciparum malaria: a pathological study. Am J Trop
Med Hyg. 1991; 44: 168-75
46. MacPherson GG, Warrell MJ, White NJ, Looareesuwan S, Warrell DA. Human cerebral
malaria: a quantitative ultrastructural analysis of parasitized erythrocyte sequestration.
Am J Pathol. 1985; 119: 385-401.
47. RASHAD S. BARSOUM, Malarial Acute Renal Failure. Journal of American Society of
Nephrology. vol. no. 11 2147-2154; November 1, 2000 .
48. Barsoum R: Malarial nephropathies. Nephrol Dial Transplant 13:1588-1597, 1998
49. Mshana RN, Boulandi J, Mshana NM, Mayombo J, Mendome G. Cytokines in the
pathogenesis of malaria: levels of IL-1, IL-4, IL-6, TNF-, and IFN in plasma of healthy
individuals and malaria patients in a holoendemic area. J Clin Lab Immunol. 1991; 34:
131-9.
339
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
50. Day NP, Hien TT, Schollaardt T, Loc PP, Chuong LV, Chau TT, et al. The prognostic
and pathophysiologic role of pro- and anti-inflammatory cytokines in severe malaria. J
Infect Dis. 1999; 180: 1288-97
51. Grau GE, Heremans H, Piguet PF, Pointaire P, Lambert PH, Billiau A, et al. Monoclonal
antibody against interferon gamma can prevent experimental cerebral malaria and its
associated overproduction of tumor necrosis factor. Proc Natl Acad Sci U S A. 1989; 86:
5572-4.
52. Kwiatkowski D, Molyneux ME, Stephens S, Curtis N, Klein N, Pointaire P, et al. Anti-
TNF therapy inhibits fever in cerebral malaria. QJM. 1993; 86: 91-8.
53. Nahrevanian H, Dascombe MJ. Nitric oxide and reactive nitrogen intermediates in lethal
and nonlethal strains of murine malaria. Parasite Immunol. 2001; 23: 491-501.
54. Nahrevanian H, Dascombe MJ. Expression of inducible nitric oxide synthase (iNOS)
mRNA in target organs of lethal and non-lethal strains of murine malaria. Parasite
Immunol. 2002; 24: 471-8.
55. Cumming AD, Driedger AA, McDonald JW, Lindsay RM, Solez K, Linton AI.
Vasoactive hormones in the renal response to systemic sepsis. Am J Kidney Dis 1988; 11:
23–32. 82.
56. Benedict CR, Rose JA. Arterial norepinephrine changes in patients with septic shock.
Circ Shock 1992; 38: 165–72.
57. Pulido-Méndez M, Finol HJ, Girón ME, Aguilar I. Ultrastructural pathological changes in
mice kidney caused by Plasmodium berghei infection. J Submicrosc Cytol Pathol 2006;
38: 143–8.
58. WHO. Severe falciparum malaria. Trans R Soc Trop Med Hyg. 2000; 94 Suppl 1:s1-90
59. Skorecki K, Green J, Brenner BM (2005). "Chronic renal failure". In Kasper DL,
Braunwald E, Fauci AS, et al. Harrison's Principles of Internal Medicine (16th ed.). New
York, NY: McGraw-Hill. pp. 1653-63. ISBN 0-07-139140-1.
60. Tierney, Lawrence M.; Stephen J. McPhee; Maxine A. Papadakis (2004).
"22". CURRENT Medical Diagnosis and Treatment 2005 (44th ed.). McGraw-Hill.
p. 871. ISBN 0-07-143692-8.
61. Biruh T Workeneh, MD, PhD. Acute kidney injury. Oct 31, 2015. MEDSCAPE.
62. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work
Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl
2012; 2:1.
340
Polamarasetti et al. World Journal of Pharmacy and Pharmaceutical Sciences
63. White NJ, Miller KD, Marsh K, Berry CD, et al. Hypoglycemia in African children with
severe malaria. Lancet. 1987; i: 708-11. 97.
64. Das BS, Satpathy SK, Mohanty D, Mohanty S, Mishra SK, Satapathy PC, et al.
Hypoglycaemia in severe falciparum malaria. Trans R Soc Trop Med Hyg. 1988; 82: 197-
201
65. Day NJ, Phu NH, Bethel DP, et al. The effects of dopamine and adrenaline infusions on
acid-base balance and systemic haemodynamics in severe infection. Lancet. 2000; 348:
219-23.
66. Maitland K, Pamba A, English M, Peshu N, Marsh K, Newton C, et al. Randomized trial
of volume expansion with albumin or saline in children with severe malaria: preliminary
evidence of albumin benefit. Clin Infect Dis. 2005; 40: 538-45.
67. Cantarovich F, Rangoonwala B, Lorenz H, Verho M, Esnault VL, High-Dose Furosemide
in Acute Renal Failure Study Group. High-dose furosemide for established ARF: a
prospective, randomized, doubleblind, placebo-controlled, multicenter trial. Am J Kidney
Dis. 2004; 44: 402-9.
68. Kellum JA, Bellomo R, Ronco C. Kidney attack. JAMA. 2012; 307: 2265-66.
69. Korbet SM. Acute peritoneal dialysis prescription. In Handbook of Dialysis. Eds: JT
Dougirdas, Peter G Black, Todd S Ing, 4a Edn. Walters Kluwer- Lippincott Williams &
Wilkins, 4a~dn, 2007; 376-85.
70. Schiff H, Lang SM, Fischer R. Daily dialysis and the outcome of acute renal failure. N
Eng J Med 2002; 346: 305-10.
71. Saroj K ~ishra', Kishore C Mahantaz et.al., Acute Kidney Injury In Malaria - Challenges
Related Documents