BARNET PRIMARY CARE TRUST COMMISSIONING PROSPECTUS 2007/8 5 th December 2006

Commissioning Prospectus 2007 / 08
Aug 20, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
BARNET PRIMARY CARE TRUST
COMMISSIONING PROSPECTUS 2007/8
5th December 2006
BPCT Commissioning Prospectus 2007/8
BPCT COMMISSIONING PROSPECTUS 2007/8
CONTENTS
Page
1. Introduction 3
2. The PCT’s Vision and Approach 4
3. Local Health Needs and Funding 6
4. Strategic Context 7
5. Key Priorities 14
6. The Commissioning Process for 2007/8 15
Appendix A The Commissioning Cycle
Appendix B Barnet GP Referral Matrix
Appendix C Commissioning Priorities
Appendix D London Planning and Commissioning Arrangements
Appendix E Summary of Commissioning Intentions
2
BPCT Commissioning Prospectus 2007/8
PCT COMMISSIONING PROSPECTUS 2007/8
1. INTRODUCTION
In July 2006 the Department of Health produced an update on health reforms that focussed on key changes designed to strengthen the commissioning of NHS services and in particular hospital services.
One key component of the changes is the requirement for PCTs’ to produce a Prospectus each year as an integral part of the commissioning cycle. Final guidance on Prospectus contents in due out from the DoH at the end of 2006, with a view to the first full Prospectus being made available by each PCT well ahead of 2008/9.
The Prospectus allows commissioners to set out, in a clear way, the changes they intend to make to local health services delivery in the following full financial year. Any changes are based on an assessment of needs, past service delivery performance and local health priorities within the overall funding available.
In any PCT, the term ‘commissioners’ refers both to the professionals employed to invest in the full spectrum of health services wisely for their local population and to the GPs who take responsibility for commissioning a selection of services directly for their practice populations. It is essential that all commissioners work together against a common strategic background to ensure the best possible outcomes for patients and, in Barnet, the proposals in this document represent a joint approach by all commissioners. The relationship between different stages of the commissioning cycle, and where the Prospectus fits in, is set out as a diagram at Appendix A.
Although final guidance is still awaited, it is clear from information available already that the document should be commissioning driven and should allow local residents the opportunity to input to the PCT’s proposals for service change in an informed way. Barnet PCT has therefore decided that it would be helpful to its residents and service providers to produce its commissioning intentions for the coming year, ahead of full Prospectus publication, and has produced this Commissioning Prospectus in response to a desire to inform.
This Commissioning Prospectus relates to the year 2007/8. It is available in a précised version for wider distribution. For those who do not wish to read the narrative text, a summary of commissioning intentions has been incorporated at Appendix E. This appendix has been designed to be read as a stand-alone version if required.
Although the Commissioning Prospectus is not being circulated as part of a formal consultation process in this year, any comments on its contents and the service changes proposed are welcomed and should be directed to:
Dominic WrightDirector of Strategic Commissioning and Planning
3
BPCT Commissioning Prospectus 2007/8
2nd Floor, Westgate HouseEdgware Community HospitalBurnt Oak BroadwayEdgware, Middlesex HA8 0AD
2. THE PCT’S VISION AND APPROACH
2.1 The PCT’s Vision
Barnet PCT will improve the health of the local population. The PCT will ensure there are good quality, appropriate health services available, so the right treatment can be delivered, at the right time, in the right place, by suitably skilled staff.
Services will
• foster personal responsibility for health and independence;
• be based on prevention and tackle the root cause of ill health;
• be directed to reduce inequalities in people’s health;
• be patient centred by being built around the needs of the individual;
• be accessible – provided in the most appropriate location, at the
most convenient times, using the most appropriate technology;
• integrate with other health and social care services across care
pathways;
• focus on quality – making sure people get the most appropriate,
best possible care and treatment and are involved in choosing the
location that might not always be geographically the closest;
• be supported by a well motivated, empowered, equipped and skilled
workforce who have responsibility for their actions;
• be developed in line with evidence and value for money;
• be innovative and creative to develop the best practice and models
of care;
• through the promotion of healthy lifestyles, empower and
encourage individuals to retain their independence;
• encourage a culture of openness, honesty and transparency
throughout the organisation.
To ensure that our vision becomes a reality, the PCT will support and develop staff so they can provide a high quality service to our local community.
2.2 Approach
4
BPCT Commissioning Prospectus 2007/8
An important component of achieving our vision and applying our values is using our resources in the most appropriate way to enable the greatest good for the greatest number of people. As demand in the NHS has always outstripped supply, this inevitably means that it is not possible for everyone to receive precisely what they might want, or necessarily where or when they want it. When determining service priorities for individual people or for the whole population of Barnet we use a framework based on a number of ‘principles’. In brief, these are that:
our resources should be used in the most clinically effective way; our resources should be used in the most cost effective way we can only provide, contract for or commission the services that
we consider are appropriate if we have enough money or other resources to do so; and our resources should be used in an equitable way
We also seek to take an ethical approach to service prioritisation, and this includes considering:
respect for patient autonomy – which requires that we help people to make their own decisions (e.g. by providing important information), and respect those decisions (even when we or health professionals may believe that a patient’s or a group of people’s decision may be wrong, noting that this does not require us to provide a specific treatment just because someone wants it, but only if it satisfactorily meets the other criteria in this framework) and only requires us to provide a treatment in a particular place of their choice if that meets the requirements of the national ‘Patient Choice’ initiative or other NHS regulations;
beneficence – which emphasises the moral importance of ‘doing good’ to others, entailing doing what is ‘best’ for the patient or group of people (the question of who should be the judge of what is ‘best’ is often interpreted as focusing on what an objective assessment by a relevant health professional would determine as in the patient’s best interests, with the patient’s own views being considered through the principle of respect for patient autonomy, the two only conflicting when a competent patient chooses a course of action that might be thought of as not in their best interests);
non-maleficence – which requires that we should not harm patients, and, because most treatments carry some risk of doing some harm as well as good, the potential goods and harms and their probabilities must be weighed up to decide what, overall, is in the patient’s or group of patients’ best interests (but it must also be noted that we have a duty of non-maleficence to others – we could indirectly harm others because a decision to provide treatment to one person or group of people could prevent others from receiving other care of proven clinical and cost-effectiveness; and
5
BPCT Commissioning Prospectus 2007/8
distributive justice – which recognises that time and resources do not allow every patient to have the ‘best possible’ treatment and that decisions must be made about which treatments can be offered within a health care system. This principle of justice emphasises two points:
people in similar situations should normally have access to similar health care, and
when determining what level of health care should be available for one group, we must take into account the effect of such a use of resources on others (i.e. the opportunity costs).
2.3 User input
The Introduction to this document sets out that in future years the Commissioning Prospectus should be commissioning driven and should allow local residents the opportunity to input to the PCTs proposals in an informed way. Because this is the first annual prospectus, it has not been possible to gather extensive user input owing to timing constraints. It is planned to incorporate extensive input, in a co-ordinated manner, in successive years.
However, the PCT has held one users’ event immediately prior to production of this document and was able to gather useful feedback on service delivery. The most significant elements of feedback, such as the need for extended practice opening hours in primary care, have been incorporated into planned review work in the coming year. In addition, access to elective procedures such as hip replacement, where chronic and debilitating conditions may be treated effectively, was signalled by users as a priority and will be addressed as part of the speeding up of the patients pathway to an 18-week maximum in 2008.
Further user input will be gathered as the year progresses.
3. LOCAL HEALTH NEEDS AND FUNDING
3.1 Local Health Needs
The population of Barnet was estimated at 329,700 for 2005. This is expected to increase by 2016 to 366,000. Although, the population is likely to increase in 2007/2008 the largest increases are not expected until after 2010. The population is very diverse with over 27% coming from black and minority ethnic communities. Generally the population is relatively wealthy and in better health than most other London boroughs.
The Public Health White Paper Choosing Health (Nov 2004) lays out proposals to change ‘a national sickness service’ into ‘a national health service’ and there is now a much increased emphasis in the NHS on improving health and not just treating disease.
6
BPCT Commissioning Prospectus 2007/8
Smoking not only increases the risk of lung disease and a number of different types of cancer, it also increases the risk of heart disease, delayed bone healing after a fracture, miscarriage, osteoporosis, hair loss, premature skin ageing and kidney disease – among other things. Passive smoking increases the risk of many of these conditions in non-smokers.
Barnet PCT’s top health improvement activity therefore is, and will continue to be, helping smokers to quit. It’s health promotion activities around smoking were commended in the recent Healthcare Commission report. This activity is especially important in terms of reducing ‘health inequalities’, i.e. the differences in health (and especially death rates) between different groups in the population.
In Barnet, as elsewhere in the country, someone living in one of the more deprived parts of the borough is much more likely to die before they reach 75 years of age than someone living in one of the more affluent areas. In men, smoking is responsible for more than 50% of this difference. But here are other health inequalities in Barnet, some attributable to lifestyle (such as obesity) and others to factors such as poverty or ethnic background.
The PCT’s greatest inequality gaps are demonstrated in prevalence of coronary heart disease (CHD) and uptake of breast screening. Although Barnet still has lower than the national average deaths due to heart disease in its population, there is a marked difference within the borough on death rates due to CHD, depending on the ward of residence. Those wards with the greatest deprivation also demonstrate a proportionately high death rate due to CHD and the reverse is true of areas with low deprivation. The higher rate is almost 50% more than the lower rate.
In the latest national comparison, Barnet demonstrated the greatest rise in teenage pregnancy in the country. Whilst of great concern, the rise was calculated on a relatively small baseline and therefore appears more significant than is really is.
Breast cancer is the single most common life-threatening cancer diagnosed and the leading cause of cancer deaths among women living with cancer in Barnet. For breast screening to make a significant impact on reducing deaths from breast cancer it has been estimated that at least 70% of the relevant population need to be screened. In Barnet the average across the borough is around 60% uptake, with a broad spread of results across GP practices. This inequitable uptake is the cause significant concern.
3.2 Funding
Every year a certain amount of funding is allocated to all PCTs by the Department of Health, based on the outcome of a formula using size and needs of the local population. In the past PCTs have sometimes received an allocation that does not match the outcome of the formula as it is currently applied so, instead of removing funding all at once from some PCTs and potentially destabilising local services, the government has set a
7

BPCT Commissioning Prospectus 2007/8
‘pace of change’ policy. This means that over time PCTs are brought to the correct level of funding.
In the case of Barnet, the PCT has been relatively over-funded by about 8% (this is approximately £32million per year). As a result the PCT will receive a lower proportion of additional funds allocated to the NHS in 2007/8 than the national average. For the coming year this will mean approximately £5 million less income in real terms and a similar trend will continue for Barnet over the next few years.
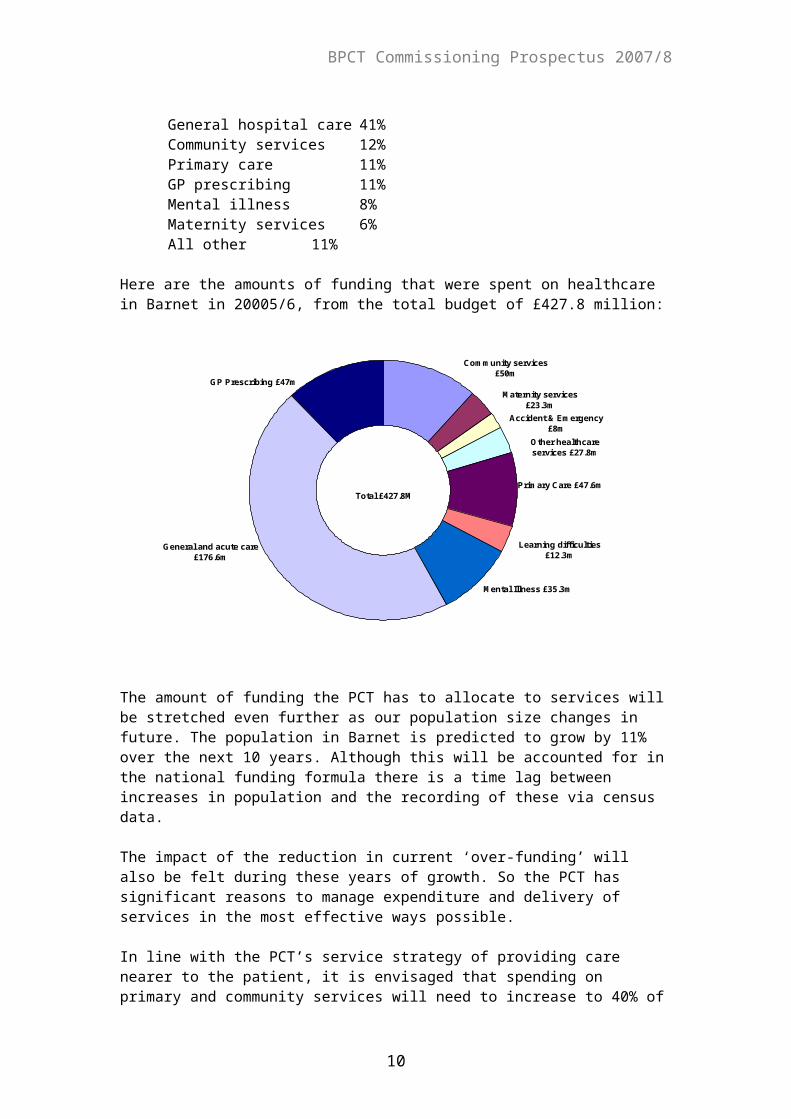
This means that the PCT needs to be very clear about what the priorities are for funding services for its community. During 2005/6 the annual £427.8 million funding for Barnet was allocated roughly as follows:
General hospital care 41%Community services 12%Primary care 11%GP prescribing 11%Mental illness 8%Maternity services 6%All other 11%
Here are the amounts of funding that were spent on healthcare in Barnet in 20005/6, from the total budget of £427.8 million:
Mental Illness £35.3m
Learning difficulties £12.3m
Primary Care £47.6m
Other healthcare services £27.8m
Accident & Emergency £8m
Maternity services £23.3m
Community services £50m
GP Prescribing £47m
General and acute care £176.6m
Total £427.8M
The amount of funding the PCT has to allocate to services will be stretched even further as our population size changes in future. The population in Barnet is predicted to grow by 11% over the next 10 years. Although this will be accounted for in the national funding formula there is a time lag between increases in population and the recording of these via census data.
The impact of the reduction in current ‘over-funding’ will also be felt during these years of growth. So the PCT has significant reasons to
8
BPCT Commissioning Prospectus 2007/8
manage expenditure and delivery of services in the most effective ways possible.
In line with the PCT’s service strategy of providing care nearer to the patient, it is envisaged that spending on primary and community services will need to increase to 40% of the PCT’s overall budget by 2017. In addition, the PCT’s spending on mental health is below the London average and we aim to increase investment from 8% to 10% in the future.
In order to make this shift possible, the PCT be focussing on areas where spending is relatively high compared to local and national benchmarks.
The PCT will have to make some difficult decisions and will not be in a position to invest in service development unless funds are released from elsewhere or the development itself demonstrates service improvement allied to cost reduction.
3.3 Health Priorities
The PCT is working with a number of neighbouring PCTs on potential areas for consideration of disinvestment at some stage in the future. Any decisions will be based on a systematic approach to assessing clinical and cost ineffectiveness. Areas to be considered in a systematic way are:
HomeopathyVaricose vein managementTonsillectomy and adenoidectomyGrommet insertionHip and knee replacementDental implantsWisdom teeth removalCaesarean sectionManagement of obesityUse of some drugs
The prioritisation process will be ongoing and a list of further topics for consideration, once these have been investigated, is being agreed.
4. STRATEGIC CONTEXT
4.1 Barnet Strategic Service Development Plan 2005-8
The Barnet Strategic Service Development Plan (SSDP) for 2005-8 was published recently and it provides a concise and cohesive planning strategy for primary, community and acute care in Barnet over the next few years. The plan is built on a foundation of several key planning processes that were already in existence and provides continuity into the future. A review of the Strategic Plan is expected to be produced in the spring of 2007. This will need to take account of Barnet Enfield and Haringey Clinical Strategy and the Strategy for London.
9
BPCT Commissioning Prospectus 2007/8
The SSDP will form the strategic backdrop for all aspects of work carried out across the PCT, as it does for this Commissioning Prospectus. Underpinning all the PCTs plans is the shifting of services and activity from secondary to primary and social care enabling patients to receive the right care, in the right place from the most appropriate professional.
Of particular significance are the commitments (both national and local) due to be delivered by the PCT over the next three years in section 3 of the SSDP. The key influencing policies underpinning the SSDP are echoed below in this section (para 4.3) in the detail of the government White Paper (‘Our health, our care, our say’).
4.2 The PCT’s Financial Position
During 2006/7 the PCT has faced a difficult financial position following the 3% top slice of its revenue allocation. A challenging savings plan has been put into place to offset the predicted year end shortfall in funding. Incorporated into the saving plan is a series of demand management schemes that were initiated to establish pathways to care for the longer term that are compatible with DoH strategic guidelines and that ensure care is provided in the most appropriate setting.
Mid year analysis of expenditure demonstrates that the demand management schemes have had a long introductory phase and have not yet delivered the benefits that were predicted at this stage in implementation. The savings plan as a whole has therefore slipped and there is little potential to retrieve the situation fully in mid year. In addition, extra funding amounting to £1 million has been taken from the PCT by the London Strategic Health Authority as part of a London wide move to top up their contingency reserves.
The PCT is now predicted a ‘likely’ forecast deficit of £7 million at year end 2006/7, with a possible reduction by 50% if the savings plan and accompanying demand management schemes begin to deliver tangible benefits. This will leave the PCT with an unfunded deficit of £3.5 million at year end that will have a detrimental impact on 2007/8 funding. The PCT will nevertheless still aim to achieve balance by ensuring full implementation of savings plans. The existing demand management schemes (see Section 4.6 ) are now intended to be implemented on a permanent basis.
It is likely that further schemes will have to be introduced next year and these do not feature yet in this document as discussions are at an early stage. Service providers and the public will be informed once they have been shaped within the PCT.
A top slice of 3.6% is envisaged for 2007/2008 with repayment of any 2006/2007 over-spending also being deducted. Developments for the year will be minimal. Most improvements to services, working towards NSFs and other national targets will have to come from service redesign.
4.3 ‘Our health, our care, our say’
10
BPCT Commissioning Prospectus 2007/8
The government White Paper ‘Our health, our care, our say’ was published at the beginning of 2006 and sets a new direction for social care and community health services, with four main goals:
a. Better prevention and early intervention for improved health, independence and well-being.
b. More choice and a stronger voice for individuals and communities.
c. Tackling inequalities and improving access to services.
d. More support to people with long term needs.
This guidance reaffirms the direction of travel that the PCT was already engaged in, by seeking to move out services wherever possible from an acute hospital base and make them available nearer to the patient using settings such as health centres and the GP’s surgery. In this way there is easier access for the patient and better coordination of the care provided.
In a move to parallel publication of the White Paper, the DoH announced that some capital funding would be made available to develop a new generation of community hospitals to meet new models of care closer to the patient. At present, the PCT is in the process of bidding for consideration of funding via this initiative in order to redevelop Finchley Memorial Hospital.4.4 Local Delivery Plan (LDP)
The PCT’s Local Delivery Plan relates to the years 2005-8 and sets out clear plans and milestones for delivery of the DoH’s national targets, covering a number of different service areas. The LDP is reviewed and updated annually (the latest review is expected by end November 2006) by PCT staff in joint working with partners (service provider and Local Authority).
The most significant task facing the PCT, in terms of LDP targets, is delivery of the 18-week ‘referral to procedure’ target for all GP referrals by December 2008. As the target time subsumes waiting for first outpatient consultation, any tests necessary to aid diagnosis and then waiting for any elective procedure required it is a difficult one for service providers to deliver. The November 2006 reworking of the LDP may result in milestones for commissioners to work to, with local health partners, to ensure delivery of the December 2008 target.
The aim for the PCT will be to achieve the staged reduction of waiting time without incurring a rise in activity levels above those predicted as part of the LDP and FT Diagnostic planning process.
4.5 Barnet, Enfield and Haringey Clinical Strategy
Barnet, Enfield and Haringey PCTs and local hospital trusts (Barnet and Chase Farm Hospitals and North Middlesex University Hospital) are engaged in a strategic planning process with their staff and local
11
BPCT Commissioning Prospectus 2007/8
residents, on the pattern of services to be provided within local hospitals in future. At the moment, four different scenarios are being considered in a structured process that should deliver a clear direction for any service changes by the beginning of 2007/8.
4.6 Demand Management Plans
The PCT’s financial position in the early part of 2006/7 made the implementation of a series of demand management measures imperative. In common with most other PCTs, Barnet has seen consistent rises over the years in the numbers of patients attending A/E departments, short non-elective stays associated with this service and outpatients generally.
The rise in demand would be difficult enough to accommodate and fund in itself, but it is accompanied by a gradual tightening of access targets to acute services and the whole scenario is not sustainable. Therefore the PCT has adopted a series of demand management initiatives, some have already been implemented, others are still in development.
The schemes are:
1) Orthopaedic referrals triage2) Dermatology referrals triage3) Gynaecology referrals triage4) Management of diabetic patients in primary care5) Diabetic retinopathy screening in the community6) ENT pilot clinic in primary care7) Emergency care practitioners preventing admissions8) Consultant to consultant referral management guide9) Direct GP access to MRI scanning10) Reduction in long lengths of stay 11) Increased primary care to support A/E 12) Community matrons13) Telecare14) Disinvesting in uneconomic services15) Investing only in service changes that deliver demonstrable
service improvements and are cost neutral or cost saving16) Unbundling current service tariffs to achieve service
improvements
Where schemes will have an impact that does not come into effect until 2007/8, they have been embedded in the contents of Appendices C and E.
The development of care pathways across many specialties and individual conditions is underway within the PCT and is an important accompanying strategy to most of the demand management initiatives above.
4.7 Annual Performance Ratings
12

BPCT Commissioning Prospectus 2007/8
In October 2006 the Healthcare Commission published its findings on the PCT’s performance during 2005/6. The Trust was rated ‘fair’ for use of resources (managing finances and demonstrating value for money in the services it offers to patients). It was graded as ‘weak’ for quality of services, with failure to meet some existing national targets the cause for concern. As the PCT is responsible for commissioning services from other bodies, they also share responsibility for the other bodies’ performance against targets (e.g. LAS).
Those existing targets that were failed or under achieved in 2005/6 were:
• Crisis resolution services for mental health needs
• Thrombolysis for heart attack patients
• LAS response times to Category B calls
• Sustained success of smoking quitters
• Total time in A/E (target – four hours or less)
• Appointments booked via Patients Choice
Rectifying action has been taken where possible in 2006/7 but a more strategic approach via commissioning is being incorporated into individual service areas for the coming year (2007/8) to ensure sustained improvement into the longer term. It is interesting to note that, using a different set of criteria to assess tobacco control, the PCT achieved an ‘excellent’ score in a different section of the report.
Where new national targets are concerned, the PCT was graded as ‘fair’.
Areas for concern were:
• Teenage conception rates
• Access to GUM clinics within 24 hours
• Number of high intensity users
• Delivery of community equipment
• Number of community matrons
• Ongoing diabetic monitoring
4.8 Practice Based Commissioning Clusters
Barnet has four practice based commissioning (PbC) clusters. The strategic backdrop for commissioning of services by these clusters is provided by PCT wide strategic direction. In turn, some of the PCT wide priorities are derived from the focal points of the clusters. All GP practices in Barnet are part of a PbC cluster. In 2006/7 the clusters had the following service developments as common priorities:
13
BPCT Commissioning Prospectus 2007/8
1. Moving the provision of dermatology services into the community wherever possible.
2. The use of the Referrals Assessment Service to direct musculo-skeletal referrals to the most appropriate setting for diagnosis and treatment.
3. Prescribing statins in line with NICE guidance.
There is in addition a locality element to their priorities, based on local health need. These are:
North Locality - A/E access and preparatory work on diabetes, COPD and ENTSouth Locality - Access to diagnosticsWest Locality (Edgware/Mill Hill) - Diabetes management and data collectionWes Locality (Burnt Oak/ Hendon) - Gynaecology care pathway and data
collection
In 2007/8 the clusters will consolidate progress made the previous year and will implement schemes in preparation at present. Data collection falls into this category as it will be used to make informed strategic decisions about the future of services.
4.9 Diagnostic Services
From April 2007 the PCT will be able to access increased diagnostic capacity via the national DoH initiative to introduce new independent sector provision to work alongside the NHS. This will offer shorter waiting times in some diagnostic areas and help commissioners to deliver the 18-week referral to procedure target by December 2007.
Procurement and contract negotiation have been carried out by the DoH on behalf of PCTs and Amicus in Health will be the provider for this region. It is anticipated that the service will be provided from the Garden Hospital, Edgware Hospital and Barnet MRI but under the terms of the agreement patients can access Amicus’ services wherever they are provided in London if they prefer.
It is anticipated that the following services will be provided and pathway arrangements from referral to reporting are being finalised at present:
MRI, ultrasound, radiography (may be reporting only), sigmoidoscopy, echocardiogram, electrocardiogram, phlebotomy.
Given the lack of capacity in some areas, such as ultrasound, it may be that the additional capacity provided by the IS is necessary to meet the 18 week access target without reducing any current activity levels.
14

BPCT Commissioning Prospectus 2007/8
The PCT will also be working with its practice based commissioners on the development of one-stop assessment services for a range of different conditions.
For further detail, see section 2 in Appendix C.
5. KEY PRIORITIES
The PCT has identified a small number of key priorities for 2007/2008 that will inform and direct its operational planning. These reflect national and local policy drivers. These are:
Returning to financial balance Successfully Implementing demand management plans to
reduce acute sector activity Achieve the required reductions in waiting times from referral to
treatment Meet smoking cessation and access to genitor urinary medicine
targets Ensure health services are safe minimising the risks of acquired
infections Deliver the systems and support to the public and patients to
enable them to make informed choices concerning their care Develop community and primary care services in line with the
direction of travel outlined in ‘Our health, Our Care, Our Say’. Take forward the outcome of the Barnet, Enfield and Haringey
clinical strategy.
Proposed commissioned services for 2007/8, by provider, are set out at Appendix B.
Specific changes proposed for individual services are identified at Appendix C.
A summary of proposed commissioning changes, with indicative targets where applicable, is set out at Appendix E.
6. THE COMMISSIONING PROCESS 2007/8
The PCT will adhere to the recently published Department of Health guidance on the application of Payment by Results for 2007/8 and on any successive guidance which follows. Commissioners will discuss the implications of roadtesting an unbundled tariff with acute and community providers, where appropriate, particularly where diagnostic or rehab services are concerned.
The PCT will also adhere to the London-wide financial and commissioning terms, as set in the document entitled ‘London Wide Commissioning - Primary Care Trust business intentions/terms of business for 2007/8’. A summary of these terms is set out at Appendix D.
15
BPCT Commissioning Prospectus 2007/8
The PCT wishes to move away from block contracts for non-PbR services wherever possible and will put in place shadow cost and volume contracts during 2007/8 for Barnet PCT provider services and diagnostic services provided by BCFH and RFH, with a view to establishing full cost and volume contracts in 2008/9 at locally negotiated prices.
(BCFH, RFH and Barnet PCT provider services please note)
16
BPCT Commissioning Prospectus 2007/8
APPENDIX A
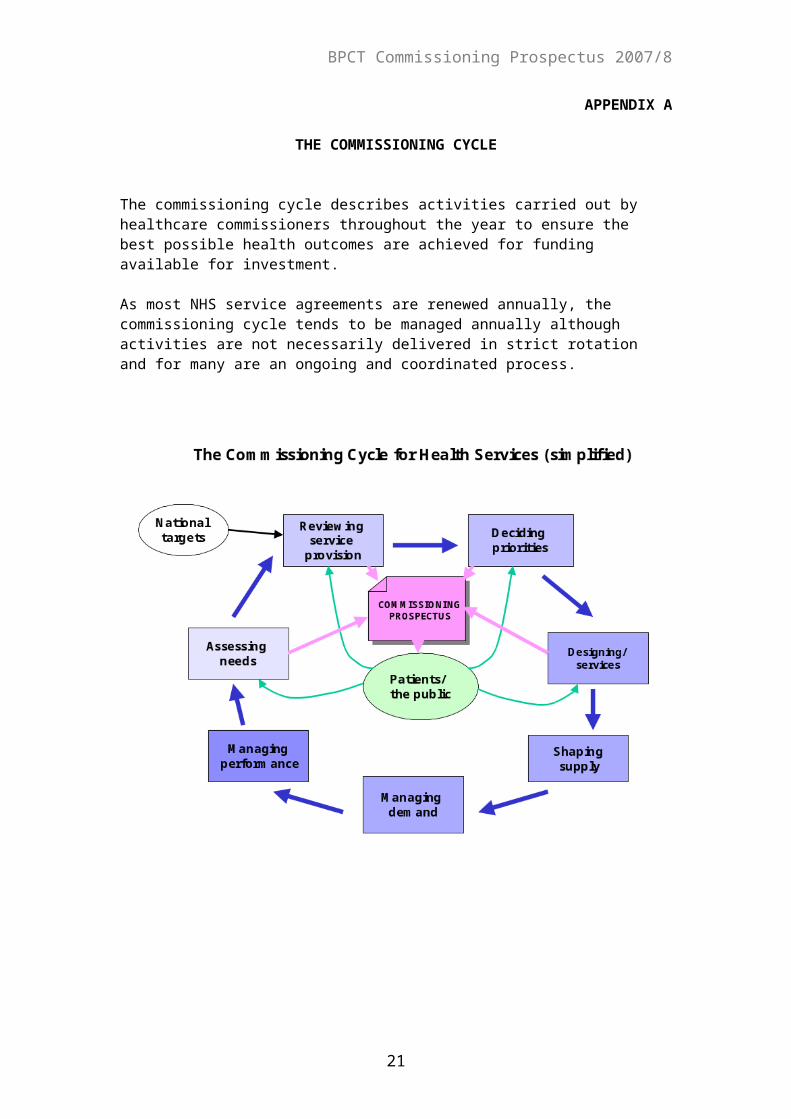
THE COMMISSIONING CYCLE
The commissioning cycle describes activities carried out by healthcare commissioners throughout the year to ensure the best possible health outcomes are achieved for funding available for investment.
As most NHS service agreements are renewed annually, the commissioning cycle tends to be managed annually although activities are not necessarily delivered in strict rotation and for many are an ongoing and coordinated process.
17
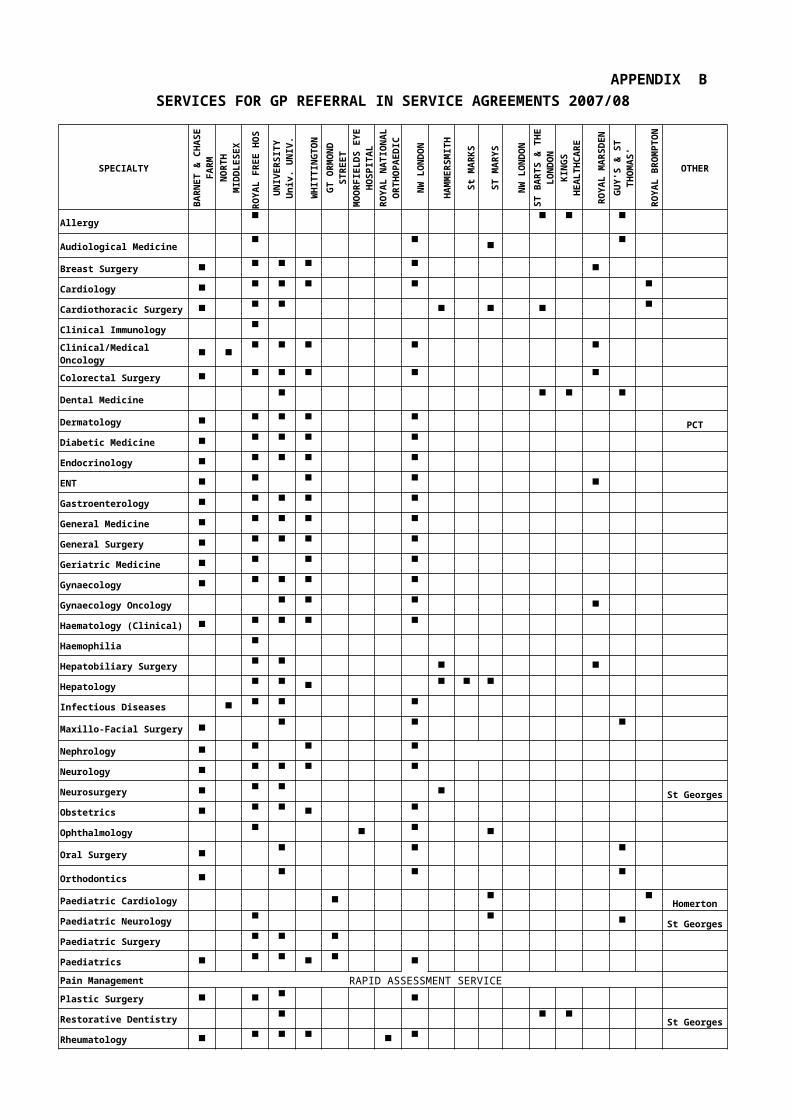
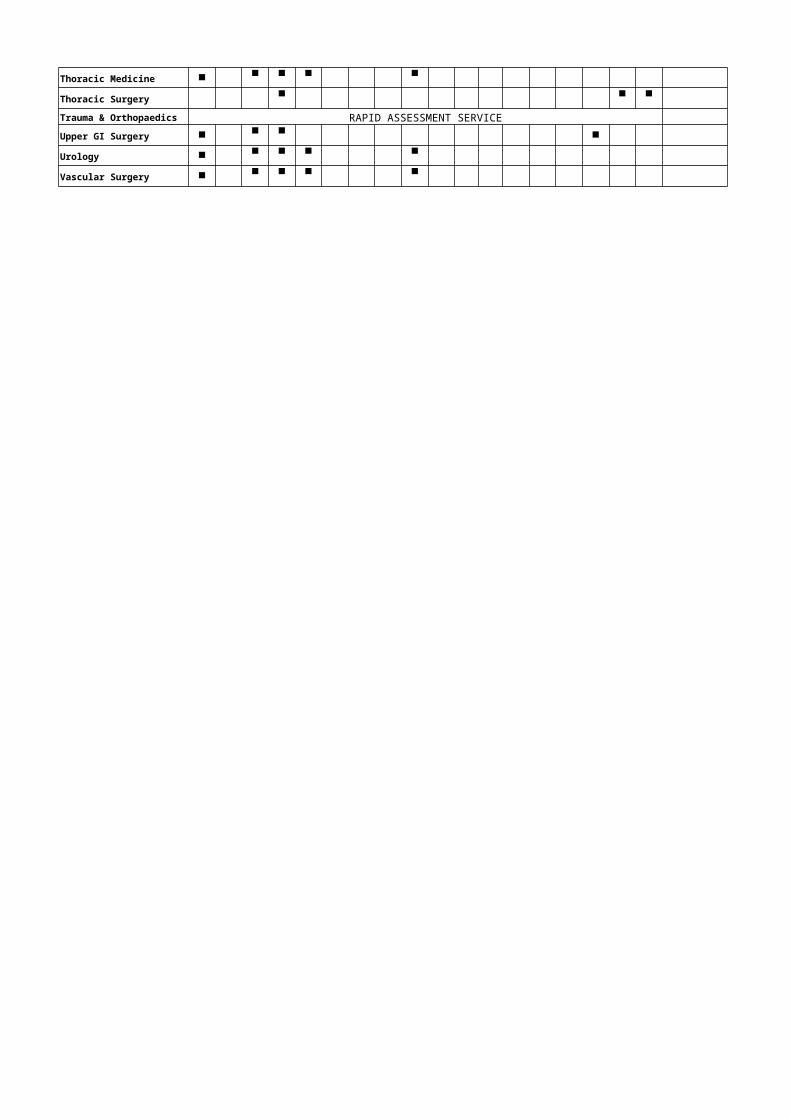
APPENDIX BSERVICES FOR GP REFERRAL IN SERVICE AGREEMENTS 2007/08
SPECIALTY
BA
RN
ET
&
CH
AS
E F
AR
M
NO
RT
H
MID
DL
ES
EX
U
NIV
ER
SIT
Y
RO
YA
L F
RE
E H
OS
UN
IVE
RS
ITY
Un
iv.
UN
IV.
CO
LL
EG
E
HO
SP
LO
ND
ON
WH
ITT
ING
TO
N
GT
OR
MO
ND
S
TR
EE
T
MO
OR
FIE
LD
S
EY
E H
OS
PIT
AL
RO
YA
L
NA
TIO
NA
L
OR
TH
OP
AE
DIC
NW
LO
ND
ON
HA
MM
ER
SM
ITH
St
MA
RK
S
ST
MA
RY
S
NW
LO
ND
ON
ST
BA
RT
S &
TH
E
LO
ND
ON
KIN
GS
H
EA
LT
HC
AR
E
RO
YA
L M
AR
SD
EN
GU
Y'S
& S
T
TH
OM
AS
'
RO
YA
L
BR
OM
PT
ON
OTHER
Allergy
Audiological Medicine
Breast Surgery
Cardiology
Cardiothoracic Surgery
Clinical Immunology
Clinical/Medical Oncology
Colorectal Surgery
Dental Medicine
Dermatology PCT
Diabetic Medicine
Endocrinology
ENT
Gastroenterology
General Medicine
General Surgery
Geriatric Medicine
Gynaecology
Gynaecology Oncology
Haematology (Clinical)
Haemophilia
Hepatobiliary Surgery
Hepatology
Infectious Diseases
Maxillo-Facial Surgery
Nephrology
Neurology
Neurosurgery St Georges
Obstetrics
Ophthalmology
Oral Surgery
Orthodontics
Paediatric Cardiology Homerton
Paediatric Neurology St Georges
Paediatric Surgery
Paediatrics
Pain Management RAPID ASSESSMENT SERVICE
Plastic Surgery
Restorative Dentistry St Georges
Rheumatology
Thoracic Medicine
Thoracic Surgery
Trauma & Orthopaedics RAPID ASSESSMENT SERVICE
Upper GI Surgery
Urology
Vascular Surgery
APPENDIX C
Commissioning Priorities 2007/2008
1. CANCER SERVICES
Breast Screening
The PCT is concerned that the uptake of routine breast screening has been assessed as relatively poor and efforts will be directed towards those women who, for whatever reason, do not accept the offer of routine screening. This may be due to personal choice, administrative error or cultural reasons. The PCT will work with primary care staff to encourage all relevant women to attend screening sessions. As the service is block funded, there will be no financial implications to commissioners.
(North London Breast Screening Service please note)
Specialist Palliative Care
The PCT is working with the North London Cancer network to produce a model of care and service specification for specialist palliative care (including hospice provision) with a view to full implementation from April 2008, although the model of care should be applicable from April 2007. The implementation of the new commissioning arrangements will depend upon the development of a specialist palliative care tariff and consideration of moving to full 100% NHS funding of services at some stage in the future.
(North London Hospice, Marie Curie Hampstead and St John’s Hospice please note)
General Palliative Care
The issue of reducing length of stay in the acute sector, with increasing reliance on community services, has grown over the past year or two. This is often laudable and in line with the Department of Health direction of travel for modernised services. However, the savings benefit to the acute sector has not been used to meet increased demands for funding in community based services.
A particular area of creeping LOS reduction concerns patients needing palliative care. Barnet PCTstill has comparably high proportions of patients receiving palliative care and then dying in hospital. Service redesign is expected to increase the community end of life care to allow more patients to be treated and cared for at home. This will see reductions in length of stay across many HRGs, a factor that will need to be reflected in reductions in tariff payment by the sum being used to support the community service. There is a national tariff being developed for palliative care that may help although this is not expected to be in place for 2007/8. The PCT will be discussing a partnership approach to this issue with its providers
(Local acute providers please note)

Cancer Drugs
Commissioners will develop a process that enables fast decision making on the use of drugs / devices associated with the delivery of cancer services, to work in tandem with the NICE and pre-NICE processes.
Mount Vernon
The PCT will continue to support Mount Vernon cancer services. However, it is expected that more clinical networks will be developed between Barnet and the Royal Free Hospital. This will lead to increasing numbers of patients being referred for radiotherapy and other cancer treatment to the Royal Free Hospital rather than Mount Vernon.
(Mount Vernon and RFH please note)
Urology / Gastro-intestinal Services
Both Urology and Gastro-intestinal Cancer Surgery Services are planned to move from the Royal Free Hospital to UCLH during 2007/8. The commissioners take the view that this move should be revenue neutral to them. One of the drivers behind the move is the need to maintain compliance with quality standards and this is part of a sector wide strategic direction overseen by the North London Cancer Network in conjunction with local commissioning PCTs.
( RFH, UCLH and Mount Vernon please note)
2 DIAGNOSTIC SERVICES
From April 2007 the PCT will be able to access increased diagnostic capacity via the national DoH initiative to introduce new independent sector provision to work alongside the NHS. This will offer shorter waiting times in some diagnostic areas and help commissioners to deliver the 18-week referral to procedure target by December 2007.
Procurement and contract negotiation have been carried out by the DoH on behalf of PCTs and Amicus in Health will be the provider for this region. It is anticipated that the service will be provided from the Garden Hospital, Edgware Hospital and Barnet MRI but under the terms of the agreement patients can access Amicus’ services wherever they are provided in London if they prefer.
It is anticipated that the following services will be provided and pathway arrangements from referral to reporting are being finalised at present:
MRI, ultrasound, radiography (may be reporting only), sigmoidoscopy, echocardiogram, electrocardiogram, phlebotomy.
Where the PCT has block arrangements for funding direct access diagnostic services at present, they will be reviewing the level of funding for next year in order to accommodate potential reductions in activity in the acute sector in future as a result of the independent sector (IS) capacity. This may take
BPCT Commissioning Prospectus 2007/8
the form of a shadow cost and volume contract being held with local providers for diagnostic services during 2007/8 with a view to formalising this arrangement in future years.
Given the lack of capacity in some areas, such as ultrasound, it may be that the additional capacity provided by the IS is necessary to meet the 18 week access target without reducing any current activity levels.
PBC is also a driver for the introduction of cost and volume contracts in direct access diagnostics, with the disaggregation of funding to practice level being the aim by 2008/9.
The issue of commissioners funding outpatient and elective activity through PbR (which includes diagnostic costs associated with that specialty) and also having to meet the additional costs of independent sector provision for the diagnostic capacity has yet to be resolved - guidance is awaited on the potential to manage this double funding.
(BCFH, RFH, NW London, Whittington please note)
During 2007/8 the direct GP access to diagnostics MRI at Edgware Community Hospital will be extended to cover patients with chronic headache.
The PCT will also be working with its practice based commissioners on the development of one-stop assessment services for a range of different conditions.
(Local acute providers please note)
3 MENTAL HEALTH SERVICES
The PCT has been working in partnership with local statutory and voluntary sector providers to review and modernise mental health services in Barnet. In line with government White Papers, the new mental health strategy aims to shift emphasis from mental illness to mental wellbeing. As such, more services are being provided out to the community wherever possible, to make them more accessible to patients and to link in to primary care services for greater continuity of care and to offer greater choice.
Primary Care Mental Health Teams (PCMHTs) have been established within the Barnet site of Barnet, Enfield and Haringey Mental HealthTrust (BEH MHT) that are linked to the Psychological Therapies Service and provide a more accessible and timely therapy pathway for patients. It is anticipated that at least 2 Star (Support, Time & Recovery Workers) and 3 Community Development Workers will be added to the teams in 2007/8.
The PCT and BEH Mental Health Trust is failing to meet the target levels of client coverage, as set out in the 2005-8 LDP. An action plan to address the shortfall is in place in 2006/7, including a specific performance improvement bonus of £50,000. This will be continued in 2007/8 with the funds deducted from the SLA and payable on successful completion of the target level. In continuing to apply a Performance Bond with BEH-MHT in 2007/8, the PCT wishes the trust to note that provision of provider activity data for commissioners is still a significant issue.
2
BPCT Commissioning Prospectus 2007/8
Following the creation of the PCMHTs Complex Community Mental Health Teams (CMHTs) will refocus and absorb more complex cases. In 2006/07, the CMHTs will absorb the caseloads previously managed by the Assertive Outreach Team and the Mentally Disordered Offenders Team which are now disbanded.
The PCT scored a ‘fail’ on the Healthcare Commission assessment of the Crisis Resolution service it commissions for Barnet residents. This was on the basis that the two teams across the borough were not reaching activity targets. The PCT expects that the teams will reach their target from now on and will consider including this in the performance bond for next year if they fail again.
The PCT will be extending the EIP service from the one pilot area operating in high Barnet to the whole of the borough. The areas of roll out will be determined by the expected health gain by population and the support of primary care and the primary mental health team functionality.
During 2007-8 the PCT in partnership with the King’s Fund will be reviewing services for older people with functional mental health needs. There may be some service changes that occur as a result during the year although most are anticipated to impact in 2008/9.
During 2007/08, The Holly Oak Unit which is on the Colindale site will be relocated on the newly refurbished site at Dennis Scott Unit to provide 12 beds for older people with chronic functional mental health problems in a modern setting.
During 2008/09, the fully refurbished East of Barnet Psychiatric Unit (BPU) is expected to be completed following a £12m capital refurbishment approved by the SHA in 2005. This will provide good quality accommodation in a comprehensively refurbished and upgraded BPU provide for 30 Adult inpatient and 12 older people ensuite beds with associated day and community services.
(BEH-MHT please note)
4 CHILDREN’S SERVICES
At present services for children are commissioned separately by health and social care staff, although they work together wherever possible on a common approach. The Children’s Plan for Barnet, produced as a result of partnership working at the beginning of 2006/7, provides a framework for delivery of the NSF for Children and Young People and includes workstreams around integration across health and social care of commissioning and of front-line services, whilst separating commissioning and service delivery functions. Although there should be little practical impact on the way that services are delivered during 2007-8, work on delivering the various workstream in the plan will continue and will probably impact from 2008-9 on.
We will be working with the Royal Free Hospital on the delivery of a consultant delivered paediatric service as outlined in the Healthy Starts Healthy Futures consultation. (RFH please note)
3
BPCT Commissioning Prospectus 2007/8
In parallel with moves around adult services to refocus care from hospitals to a community setting wherever possible, the PCT is working with acute providers to relocate outpatient care for children from a hospital setting, particularly for follow-up care. Consideration is also being given to managing appropriate paediatric A/E attenders in a different way. Draft proposals for remodelled outpatient and A/E services for children are being developed and directed at Barnet and Chase Farm Hospitals initially. It is not clear at this stage whether there will be an impact on 2007/8.
(Acute providers please note)
There is no separate service agreement with BEH-MHT for the Child and Adolescent Mental Health Service (CAMHS) at present, it is provided within an overall block contract for provision of a range of mental health services. As a first step towards creating a designated service agreement, the activity baseline needs to be established using historic activity information. The PCT will be working with the trust to establish this.
(BEH-MHT please note)
Access to CAMHS Tier 4 provision is being reviewed at present across London and any changes arising may impact on services next year. Existing providers will be informed at an early stage of any potential changes.
(CAMHS Tier 4 providers)
A new referral pathway for accessing the Tavistock and Portman Clinic is being considered at present and, once agreed, it is anticipated that it will be implemented from April 2007. The new pathway will include a single point of access to services.
(Tavistock and Portman Clinic please note)
Issues around transition within Children’s and Adult’s care in Mental Health and Learning Difficulties services are apparent, and it is intended to review these during 2007/8.
(London Borough of Barnet and BEH-MHT please note)
The PCT will be providing and additional £100k worth of annual CAMHS grant funding next year. This is in recognition of the Local Authority providing a similar level of extra money in 2006/2007.
(All CAMHS providers please note)
Service agreements with New Beginnings are being renegotiated for next year, to be implemented from April 2007.
(New Beginnings please note)
Where Northgate is concerned, a service redesign process is planned for the coming months and may be implemented, in part or wholly, in 2007-8.
(Northgate please note)
For children with sexualised behaviour, the PCT is working with LBB on a model of care based on Cognitive Behaviour Therapy which has proved very effective elsewhere.
(LBB and BEH-MHT please note)
A borough based Children’s Community Nursing Team will be established, as part of a borough based agreement across North Central London Sector.
4
BPCT Commissioning Prospectus 2007/8
It is likely that funding will transfer from the Royal Free Hospital to Barnet and Chase Farm Hospital to provide this service at some stage in the future.
(RFH and BCFH please note)
5 LOCAL PCT- PROVIDED SERVICES
As required by the reforms set out in ‘Commissioning a patient led NHS’ and the White Paper ‘Our health, our care, our say’ the PCT’s commissioning arm is establishing a more formal and separate relationship with services provided within the PCT in a community setting. An essential step towards achieving this more formalised relationship will be the introduction of a service specification ahead of 2007/8 and the creation of shadow unit pricing of services wherever possible during 2007/8, in order to inform a possible cost and volume contract in 2008/9.
In this way any changes in the profile of services delivered may be funded more appropriately in future, services can be better performance managed via service agreements and they can be benchmarked when operating in a more competitive environment. We will be working with the PCT’s provider services to implement the new national targets from the Healthcare Commission and this will be part of the service specification process.
As the development will depend on robust data collection and analysis, there will be a time delay on shadow cost and volume arrangements until the RIO community data collection system is fully operational (should be by end 2006/7).
(Barnet PCT Provider Services please note)
6 SUBSTANCE MISUSE
Drug misuse Barnet has seen a steady increase in the number of people accessing structured tier 3 and tier 4 treatment which includes specialist prescribing, counselling, Psychology, inpatient detoxification, rehabilitation and shared care. The numbers in treatment rose to 725 in 05/06. This years estimated target is 834 and the Borough is already showing signs that this will be achieved. However, Home Office prevalence data estimates that Barnet has around 1290 level opiate or crack cocaine problem drug users in total and the aim is to keep increasing the numbers in treatment in future.
Beyond 2008 it is not yet known whether the Pooled Treatment Funding will exist in its current format and whether there will be continued investment in the sector, so we plan to consolidate existing services in 2007/8. The following are the priorities for the next 2-3 years.
- Set up a North London Drug and Alcohol Detox Centre with Islington, Haringey, Enfield and Herts if a current bid to the DoH for capital funding is successful.
5
BPCT Commissioning Prospectus 2007/8
- Develop Hepatitis B/C testing and ensure robust services are in place to for Hep B vaccinations and Hep C treatment pathways for IV drug users.
- Implement a Borough wide Harm Reduction Strategy and reduce drug related deaths
- Increase delivery of prescribing services in the Community through shared care with GP’s
- Develop an aftercare service for those exiting treatment, maintain their stability and enable them to renter their community as fully contributing members return as fully functioning as full members of their community.
- Continue to support and develop user and carer services
Alcohol Misuse Alcohol Concern completed a needs assessment on behalf of the Borough in Feb 2005 estimating that 47,000 adults in Barnet are drinking at levels that risk harm to their health and of which 14% are at high risk of alcohol related health problems. There has been little investment in alcohol services for some years. The report makes several recommendations and the following could be considered in terms of needing some urgent attention from the PCT:
- Increase the investment in specialist community based alcohol services
- Develop primary care response to identify early, treat and support patients who are risking their health through drinking and reduce longer term harm
- Ensure all health and social care staff routinely receive training on recognising an managing alcohol issues
- Implementation of the model of care for alcohol misusers (MoCAM) best practice guidance for health organisations in delivering planned and integrated local treatment system for adult alcohol users.
(Providers of drug and alcohol misuse services please note)
- Identify those presenting at A&E and for inpatient admission with symptoms and conditions associated with alcohol abuse. The PCT will work with local providers on the use of clinical coding to identify those at risk and the development of clear pathways for referral to follow up care.
(All local providers please note)
7 LEARNING DISABILITIES
Barnet Learning Disability Partnership Board recently produced a joint health and social care plan for services for clients with learning disabilities (‘A Small Plan to Make a Big Difference’). This plans sets the strategic context for changes in service provision over the next three years.
The PCT jointly commissions services for patients with learning disabilities with LBB. In 2007/8 it is proposed that the 8 Specialist Residential Services (SRS) beds at Harperbury Hospital, that are used by Barnet will be decommissioned and patients will be provided with alternative services.
Forensic and assessment and treatment beds will remain at Harperbury but those in the specialist residential services will move locally to community
6
BPCT Commissioning Prospectus 2007/8
accommodation that meets their assessed individual needs. It is recognised that more robust assessment and treatment services must be developed locally to support his move.
(Hertfordshire Partnership NHS Trust please note)
Recommendations for a commissioning strategy for Learning Disabilities services are being drawn up as part of a review being carried out by LBB. The outcome of the strategy will be published in January 2007 and may impact on the commissioning of health services in future.
The strategic direction of Learning Disabilities services is being considered as part of the longer-term commissioning strategy and will address the issues of increasing numbers of children with complex health needs and severe learning disabilities, an increase aging population of people with learning disabilities who all have a higher prevalence of developing dementia and an increase of children with diagnosed autistic spectrum disorders.
A review of sub-commissioning arrangements between the Barnet LD provider arm and BEH-MHT for provision of psychology and psychiatry support will take place ahead of 2007/8.
(BEH-MHT please note)
8 OLDER PEOPLE’S SERVICES / STROKE SERVICES
The PCT is strengthening the commissioning of continuing care by increasing manpower and the use of technology. There will be a focus on value for money in negotiating placements and greater joint commissioning with London Borough of Barnet in order to manage the care market where appropriate. In addition, the PCT is considering linking to the procurement and contracting hub for continuing care, currently being established in North-West London.
The PCT is reviewing stroke accommodation across acute and community providers because current capacity does not meet need appropriately. There will be an emphasis on establishing the number of acute or rehab designated beds required – at present patients are managed wherever there are spare beds in times of high demand. It may be that the Strategic Outline Case for redevelopment of the Finchley Memorial site offers a longer term solution to the issues of dedicated stroke services accommodation. Until then it may be necessary to rebalance existing accommodation. Of particular concern is the lack of local rehab accommodation for younger stroke victims, who have to be managed out of borough at present.
(BCFH and Barnet PCT Provider please note)
The Intermediate Care Team will be expected to improve their response rate to the discharge of patients from acute trusts and to develop expertise in areas such as stroke to facilitate earlier discharge.
(Barnet PCT provider please note)
9 LONG TERM CONDITIONS
The PCT has already set in place a new model of care to meet the needs of patients with long term conditions and the caseloads managed by specialist
7
BPCT Commissioning Prospectus 2007/8
staff are rising. This trend will continue in 2007/8 with the focus on preventing hospital admission where possible by closer clinical management in the community. This has already been an effective approach to managing patients with respiratory disease in Barnet. Many of the schemes outlined in the rest of this section also benefit those with long term conditions.
10 SEXUAL HEALTH
The PCT is looking at the provision of GUM services from all of its providers. The currently hosted GUM service by Barnet and Chase Farm will be reviewed to assess where services can be provided within a primary care setting. The patient pathway will be developed according to this model including assessment of primary care contribution from GP practices, family planning and the appropriate use of secondary care. Key to this work is the careful planning of how the national target of 48 hour access is met, including the understanding of demand and capacity for GUM provision.
(BCFH please note)
11 PLASTIC SURGERY / BURNS SERVICES
Plastic Surgery and Burns services will be relocated from West Herts Hospital to RFH from April 2007 as part of a planned strategic development to strengthen these services. There will be no financial implications for commissioners.
(West Herts Hosp and RFH please note)
12 REFERRAL ASSESSMENT CENTRE
The Barnet Referral Assessment Centre (RAS) currently assesses referrals from GPs for musculo-skeletal opinion and sends them on to the most appropriate service for management, which may be an acute hospital outpatient service, a community based service or increasingly an alternative in primary care.
During 2007/8 the RAS will expand its function to cover referrals for paediatrics, pain management and direct access to MRI scanning. It is anticipated that the range of specialties covered by this service may expand further in 2008/9.
From December 2007 the PCT will be commissioning one provider to run the triage service with an expectation that this will be operationally independent of any acute organisations to avoid possible conflicts of interest.
For more detail on individual specialties please see points 4-6 in the table at Appendix E.
(All acute providers please note)
13 DERMATOLOGY
Pathway development for dermatology referrals has been supported by the creation of additional GP Specialists in Barnet, so that patients only need to
8
BPCT Commissioning Prospectus 2007/8
access secondary care when higher level intervention is required. Although this service has been in developmental phase during 2006/7 it will impact fully on secondary providers for the whole of 2007/8.
For more detail please see the entry at point 7 in the table at Appendix E.
(Secondary providers of Dermatology services please note)
14 GYNAECOLOGY
During 2006/7 a GP with Special Interest in Gynaecology has been involved in a pilot gynaecology triage service in primary care, for referrals requiring specialist opinion, for one of the PBC commissioning clusters. The PCT will be looking to introduce a fuller primary care based triage service, via a tendering process. It is anticipated that current providers of secondary care services will be excluded from tendering, to ensure no conflicts of interest.
(Secondary providers of Gynaecology services please note)
15 IVF
Barnet PCT currently follows DoH guidance and funds one cycle of treatment per eligible couple. One important aspect of eligibility is the age of the woman and NICE guidance is followed (this excludes women aged over 39 being treated on effectiveness grounds). The average waiting time for treatment is currently around 2 years and there are issues with patients who are approaching the upper threshold for eligibility when they are put onto the waiting list exceeding it before they are treated. In addition, service monitoring demonstrates that there may be alternative providers in London with better outcomes.
IVF provision is being reviewed at the moment with a view to potentially switching the preferred provider arrangement at King’s College Hospital to another hospital with better outcomes. However, the PCT needs to be assured that equitable access to services will not be diminished if alternative arrangements are made. Although consideration will be given to increasing the amount invested in IVF, in order to reduce waiting times, this will have to be considered along with competing priorities.
(Kings College Hospital please note)
16 URGENT CARE
The PCT has been running a pilot scheme providing primary care expertise in the local A/E department which has proven to be successful in providing patients with more appropriate clinical care. It has been estimated nationally that between 30-50% of all attenders at A/E departments are for primary care management. It has been decided that the pilot will be fully implemented in 2007/8 and should be self-funding from April. Work on a longer-term model for primary care in A/E will continue.
(BCFH and RFH please note)
17 NEUROLOGY
9
BPCT Commissioning Prospectus 2007/8
The direct GP access to diagnostic MRI at ECH will be extended fully to cover patients with chronic headache. This will be included in a specific service specification and patient pathway for the management of this condition.
Further appropriate neurological conditions will be added in year including the development of improved services for people with or at risk of epilepsy.
(Local acute providers please note)
18 HOMEOPATHY
The PCT will cease commissioning all homeopathic treatments from April 2007, unless patient referrals has been approved by the Individual Treatment Panel (ITP). All existing patients under treatment will be reviewed. The ITP will consider referral where there is proven and substantiated evidence of clinical and cost effectiveness.
(UCLH – Royal Homeopathic Hospital please note)
19 REDUCING LENGTH OF ACUTE STAY
There has been a measurable reduction in length of inpatient stay in local acute providers over the past year or two. This is highly laudable and compatible with the direction of travel required by the Department of Health. However, the trend has put an increasing pressure and cost on community service provision, as patients are accessing the service at a higher level of need. The revenue savings associated with a reducing length of stay (LoS) have been retained by acute providers to date, but this situation cannot continue.
The structure of the national tariff currently rewards acute Trusts for reducing LoS but gives no compensatory reward to community based services to cover increasing demands. Early indications from the DoH are that local negotiations around splitting national tariffs are to be allowed for 2007/8. In the meantime the PCT expects all local acute providers to indicate where further LoS reductions are planned, together with the support required from community services to achieve them. A proportion of savings achieved can then be properly attributed to community and/or social care. Where schemes begin without this consultation and agreement there will be a high chance of failure because of insufficient capacity in place outside of hospitals.
(Local acute providers please note)
20 PERFORMANCE BOND
The PCT will be applying a Performance Bond to local acute providers of services, which will contain financial penalties if benchmarked consultant-to-consultant referral rates and first to follow-up outpatient attendance ratios are not met.
(BCFH and RFH please note)21 PRIMARY CARE
Consideration is being given to the role that wider (i.e. non-GP) primary care can play in supporting the strategic direction of the PCT to move the
10
BPCT Commissioning Prospectus 2007/8
focus of care away from acute and into a community setting. The role of pharmacists, dentists and optometrists is being explored to assess potential to expand their role in this respect.
An initial Users’ Forum for service planning in the future has indicated that poor access to primary care in the evenings and at weekends is a significant concern. The PCT will be carrying out a study of demand for services and the best way that requirements can be met so that a more specific target can be established around access for our local services. The PCT will work with practice based commissioners on urgent access out of hours, alternatives to primary care and issues such as benchmarking the number of planned appointments per patient. It is anticipated that specific targets for primary care access will be developed during 2007/8.
22 CHOOSE AND BOOK
The PCT has an LDP target of 90% of all GP referrals to be booked electronically by end February 2007. At present, only 15% of these referrals are booked this way. A significant block to progress has been the lack of capacity at RFH to handle patient bookings in this way at present, either on their site or at outreach clinics on the Edgware Hospital site, although the staffing and technology solutions should be in place by end December. Certain BCFH sub-specialties are not available electronically yet.
Both providers must ensure that their services are fully bookable via the electronic route before 2007/8.
(RFH and BCFH please note)
23 SPECIALISED SERVICES
The commissioning of very specialised services (e.g. bone marrow transplants) is carried out on behalf of the PCT by a team of commissioners who work across the five PCTs in North Central London. This team is responsible to the PCTs for the strategic direction of the specialised services.
Proposals for 2007/8 include:
• Activity plans for 2007/8 will be the baseline plan for 2006/7. The exception will be where commissioning consortia apply a 3-year rolling average, which will continue to be applied.
• Commissioning consortia will undertake a price audit and benchmarking exercise to ensure value for money. No service developments will be considered for funding unless they are implemented on a cost neutral or cost saving basis.
• Services being considered for inclusion in the specialised commissioning portfolio, rather than that of PCTs, include burns and neurorehabilitation.
• A referral pathway, including gate keeping procedure, has been agreed for patients accessing the Personality Disorder Treatment Service at the Henderson Hospital. Patients will be funded on a cost
11
BPCT Commissioning Prospectus 2007/8
and volume basis, and only when compliance with the referral pathway has been demonstrated.
• Development of plans for a low secure mental health unit in the sector, so that patients do not have to be placed at risk on routine wards or at a great distance from home.
The first formal specialised commissioning plan for the sector is expected to be issued in mid-December and service providers should consider it a companion document to this one.
(All providers of specialised services please note)
12
BPCT Commissioning Prospectus 2007/8
APPENDIX D
LONDON PLANNING and COMMISSIONING ARRANGEMENTS 2007/8
NHS London has recently published the 2007/8 Planning Framework for London, ahead of the London Commissioning Regime which will be published in December 2006. The Planning Framework acknowledges that national targets and the current financial challenges faced by PCTs will drive service reforms via the commissioning process.
The new commissioning regime will require PCT’s to produce the following:
1. A Strategic Plan (produced every 3 years with a 5-10 year outlook) to establish direction and set priorities. This plan will drive and inform the Operating and Organisational capability Development Plans. The Strategic Plan will overlap with the PCT’s Prospectus and will be aggregatable to sector and London-wide level.
2. An annual Operating Plan, with a 3 year horizon. In the first year this will contain detailed targets and financial plans. It incorporates elements of the existing LDP and Local Area Agreements. The Operating Plan will set targets by month and form the basis for financial and risk rating.
3. An Organisational Capability Development Plan produced in line with the Strategic Plan which establishes the capability needs and gaps in delivering on strategy and operations, and sets out to address these. Will be based initially on the PCT’s FfP development plans.
The next tranche of guidance will also address PCT risk-rating and incentives systems. There will also be details of the arbitration process for 2007/8 contracts, with financial penalties incorporated.
Timetable for 2007/8
November 2006 – PCTs finalise FfP Development Plan Commence development of LDP and Operating Plans
December 2006 – DoH publishes National Operating Framework 2007/8
London Commissioning Regime issuedArbitration process announced
2nd January 2007 – PCTs submit LDP, Operating Plan, FfP PlanTurnaround Plans submitted where required
February 2007 - Contracts to be signed by 28th Feb
March 2007 1st – 9th Arbitration for unsigned contracts
13
BPCT Commissioning Prospectus 2007/8
16th All Plans finalised for NHS London Board approval
28th PCT Plans signed off by NHS London
Key Financial Planning Assumptions 2007/8
1. PCT top-slice across London will be between 2.6% and 3.6%. Planning should be on the basis of 3.6% at present.
2. £70m risk reserve and 2006/7 PCT surpluses to be repaid in full in 2007/8.
3. Repayment of the initial 2006/7 3% top-slice to be deferred beyond 2007/8 (to be repaid in full by 2010).
4. All unplanned deficits to be repaid in 2007/8
5. Tariff inflation at 2.5% (5% inflation net of 2.5% cost improvement programme)
6. PPA on the same basis as 20006/7, albeit reduced by 25%.
7. Prescribing uplift of 8%, GMS uplift of 2.5%.
8. Unbundling of the PbR tariff may be road tested locally and set at locally negotiated levels.
Key Service Planning Assumptions 2007/8
The top priorities will be:
Delivering the 18-week wait milestones
Maintaining the 98% A/E 4 hour maximum wait
Maintaining the cancer wait targets
Healthcare associated infections (i.e. MRSA and C-diff)
High priorities will be:
Smoking cessation
Obesity
GUM waits
Patient choice
Choose and book
Points to note
PCTs in financial balance should deliver the other LDP targets for 2007/8 as well as local targets.
14
BPCT Commissioning Prospectus 2007/8
Providers’ service plans should reflect PCTs commissioning intentions, which should be incorporated in contracts between PCTs and Trusts.
15
BPCT Commissioning Prospectus 2007/8
APPENDIX E
COMMISSIONING INTENTIONS SUMMARY
The table on the following 8 pages represents a summation of the PCT’s commissioning intentions for 2007/8 and may be read as a stand-alone compendium, without reference to the rest of this document.
In some instances, entries contain specific targets for service delivery against which commissioning performance may be monitored as the year progresses.
16
Barnet PCT 2007/08 Commissioning Intentions - DRAFT
Key: Barnet & Chase Farm (B&CF), Royal Free (RF), University College Hospital (UCLH), PCT Provider Arm (PCTPA), Barnet Enfield and Haringey Mental Health Trust (BEHMHT), Tavistock and Portman (T&P).
All of the PCTs providers should note that the PCT will be conforming and adopting the London wide business rules as agreed with the new London Strategic Health Authority. This will include the application of a new and updated standard contract. For Foundation Trusts the PCT will act in accordance with the new contract that is being negotiated to begin from 1st April 2007.
No. Type of Action Outline of Proposal/Purpose Expected Outcomes Trusts/Providers Affected
General Acute
1General Acute Waiting
Times
To achieve the staged reduction in waiting times making progress towards the December 2008 target of having no patient waiting longer than 18 weeks between referral and treatment. The aim for the PCT will be to achieve the staged reduction without seeing a rise in activity levels above the LDP/FT diagnostic predicted activity levels.
Trusts will be expected to achieve the reduction in waiting times through more efficient working including:
o Maximising capacity through reviewing outpatient new to follow up rates. 95% of specialties will be expected to be at least compliant with the national average with 25% of specialties in the top 25% band of England performance. Baseline will be 2005/2006 national data.
o Unbundling elective tariffs to segregate the diagnostic test elements.
o Complying with Barnet PCTs and applicable London wide Commissioners policy governing consultant to consultant referrals. Where this is not complied with the PCT will not reimburse the trust for activity generated.
All acute with whom Barnet PCT has an SLA.
2General Acute Homeopathy
To cease commissioning all Homeopathic treatments unless the patients referral has been agreed by the PCTs ITP. This will also include a review of all patients currently being
Overall PCT spend at the National Homeopathic Hospital will be reduced by £300,000 in a full year.
UCLH/National Homeopathic Hospital
BPCT Commissioning Prospectus 2007/8
treated. The ITP will consider referral where there is proven and substantiated evidence of clinical and cost effectiveness.
3General Acute Stroke
The commissioner wishes to see the feasibility explored for developing greater capacity in the community for increased stroke rehabilitation facilities. Currently too many patients with CVA are remaining in general hospital wards and acute stroke units when rehabilitation in a specialist community based rehabilitation unit might speed their progress. The supporting analysis will be developed in conjunction with the Strategic Outline Business Case to support the redevelopment of Finchley Memorial Hospital. It will need to also fit with any outcomes generated by the acute hospitals consultation across Barnet, Enfield & Haringey.
The HRG tariff for CVA will need to be unbundled at secondary care level to ensure that cash transfers will be made recognising reductions in length of stay. Currently the tariff is based on a completed inpatient spell. Benefits accrued through length of stay reductions accrue entirely with the acute trust this militate against greater community and social care provision.
Depending upon the background feasibility and increase in community facilities length of stay for patients with a diagnosis of stroke will fall from the 2006 calendar year average of x days to x days. (to be added at year end).
.
B&CF, RF and PCTPA
4General Acute Musculoskele
tal
The PCT will continue to refine the Rapid Assessment Service (RAS) including the extension of the triage function to cover paediatrics and to develop a clinical assessment and treatment service in line with the musculo-skeletal framework.
The PCT will be commissioning one provider to run the triage service from December 2007 with an expectation that this will be operationally run and staffed independently of any acute hospital organisation to avoid possible conflicts of interest when guiding patients to secondary care treatment.
The PCT provider has been commissioned to run all direct GP physiotherapy referral activity. It is expected that this will decrease the current waiting time of 30 weeks to below 15 by the end of December 2007.
Expected that 85% of all adult non trauma orthopaedic referrals from GPs to secondary care will be sent via the RAS. Of these it will be expected that 50% will be removed a directed to other community based treatments.
The PCTs Public Health Department will carry out an annual review of the clinical effectiveness of the RAS and recommend any changes to the specification on numbers of referrals expected to be diverted.
Patients’ satisfaction will continue to be measured via the specific survey mechanism in place. There will be an expected level of increase in satisfaction from Level four (reasonably satisfied to level two (good) of 10%.
Direct access physiotherapy waits will fall from 30 to 15 weeks by December 2007.
All general and acute providers with whom the PCT has an SLA
5General Acute Rheumatolog
The PCT will continue to roll out the pathway for rheumatology referrals that will include
It is expected that 20% of new and 35% of follow up appointments will be diverted form the 2006 calendar
All general and acute providers with
1
BPCT Commissioning Prospectus 2007/8
y incorporation into the RAS infrastructure..Rheumatology will be included in the specification for the commissioned triage service with the same expectation in place to avoid conflicts of interest.
year secondary care activity base.. whom the PCT has an SLA
6General Acute Chronic Pain
The PCT will continue to roll out the pathway for chronic pain referrals. This will be incorporated into the RAS infrastructure..Chronic pain will be included in the specification for the commissioned triage service with the same expectation in place to avoid conflicts of interest.
It is expected that 25% of current new referrals will be diverted into community settings from April and 35% of follow ups.
B&CF and RF
7General Acute Dermatology
The PCT will be looking to introduce a fuller triage service to support primary care. This will include increased levels of practitioners with a special interest support. This will be done via tendering and commissioning a triage service.
The commissioner will wish to see the PCT provider progress in developing community based dermatology services including dedicated consultant sessions in the community transferred out of current job plan commitments.
The expectation is that 50% of 2006 calendar year new outpatient referrals and 60% of follow ups will be managed outside the acute hospital structure.
95% of GPs will have attended dedicated educational sessions to improve the management of acne, eczema and psoriasis.
Four dedicated consultant sessions based in Edgware Community and Finchley Memorial Hospital to support the primary care management of acne, psoriasis and eczema. This will achieve through the PVT provider arm or PbC Clusters directly contracting for the sessions. No additional resources will be put into secondary care to compensate for this transfer.
A clinical effectiveness evaluation will be carried out in-year by the PCTs Public Health Department. Highlighted modifications/recommendations will be acted upon.
B&CF and RF & PCTPA.
8General Acute Gynaecology
The PCT will be looking to introduce a fuller primary care based triage service This will be done via tendering and commissioning a triage service. It is expected that current providers of secondary care services will be excluded form tendering to ensure no conflicts of interest arise when directing patients for onward specialist treatment.
It is expected that 30% of new and 35% of follow up general gynaecology referrals will be diverted to community based infrastructure.
At least three sessions of consultant gynaecologist time will be engaged by the PCT provider arm to carry out primary care based activity. This transfer of sessional commitment from secondary care will be expected to be revenue neutral.
B&CF and RF
9General Acute Neurology
The direct GP access to diagnostic MRI at ECH will be extended fully to cover patients with
5% of existing neurology new and follow up referrals will be diverted or have their care maintained in primary
B&CF and RF
2
BPCT Commissioning Prospectus 2007/8
chronic headache.. This will be included in a specific service specification and patient pathway for the management of this condition. Further appropriate neurology conditions will be added in year including the development of improved services for people with or at risk of epilepsy.
care as a result of the direct access provision. Quality control will continue to be monitored by the
scanners operator Alliance Medical. Inappropriate referrals from GPs kept below 2% as
measured by the agreed criteria. A clinical effectiveness evaluation will be carried out in-
year by the PCTs Public Health Department. Highlighted modifications/recommendations will be acted upon
10General Acute Diagnostics
The PCT will be expected to fully utilise the nationally procured Independent Sector (IS) diagnostic network, to enable this to work effectively all trusts with whom the PCT has an SLA will need to unbundled the cost of diagnostic procedures from the national and local price tariffs.
The target will be that the PCT fully utilises the expected and reserved capacity in the IS facilities.
Patients will be able to choose the location of the diagnostic tests
All trusts with whom the PCT has an SLA.
11General Acute Low priority
procedures
All trusts with whom the PCT has an SLA will need to comply with the specific access to treatment protocols for the following conditions: Varicose Veins Wisdom tooth extraction Tonsillectomy and Adenoidectomy Grommet insertion
Any recorded activity for the above will be validated by the PCTs Public Health Department to ensure compliance with the protocol. If the results of the audit of selected records shows non compliance the assumption shall be made that all patients admitted under the relevant HRGs were inappropriate admissions and will therefore not be reimbursed.
Only expect to treat 50 VVs. 200 complex wisdom teeth treated in a daycase hospital
setting with only 10 to be treated as inpatients. Accords to the British Association of Day Surgery (BADS) expectations.
60 tonsillectomy procedures only to be carried out across the population of Barnet. 50|% of children >19 will be treated as a daycase with an expectation that from 2008/2009 this will move to 85%.
Only 40 grommet insertions are expected across all SLAs based on current population/intervention rate estimates.
ALL OF THESE SPECIFIC DIAGNOSES REDUCTIONS NEED PUBLIC HEALTH INPAUT TO AGREE THAT THE EXPECTED REDUCTIONS AND DAYCASE RATES ARE REALISTIC AND ACHIEVABLE LOCALLY.
All Trusts with whom the PCT has an SLA
12General AcuteHip and knee arthroplasty
To manage within available resources the PCT will be working with its GPs and monitoring via the RAS the threshold for operative treatment for hip and knee arthroplasty. It will aim to introduce the Salisbury or similar scoring methodology and set referral thresholds at a
Reduction of 20% in hip and knee arthroplasty referrals to secondary care during 2007/2008.
The PCT Public Health Department will carry out a clinical review of the effects of the revised intervention thresholds in January 2007.
All acute trusts with whom the PCT has a contract
3
BPCT Commissioning Prospectus 2007/8
level that will see a reduction in referrals in 2007/2006 for both hip and knee replacements. The scoring methodology will be reviewed for appropriateness as there is variable evidence at present.
13General AcuteCons to Cons Referrals
Ensuring appropriate referral practices are in place to limit the numbers of unnecessary patient journeys.
Ensure compliance with the PCT PbC Clusters consultant to consultant policy. This will be audited by the Clusters to ensure compliance.
All acute trusts with whom the PCT has a contract
14General AcuteDiabetes
Diabetes is one of the most debilitating chronic diseases that is prevalent across the population in Barnet. It leads to premature death, morbidity from heart disease, renal disease and peripheral vascular disease.
30% reduction in new referrals to secondary care during 2007/08
10% Reduction in FUPs to secondary care during 2007/08
Revised Diabetes guidelines and pathways in place by 1 April 2007
GPwSI led educational support programme in Diabetes Management in place by 1 April 2007
All acute trusts with whom the PCT has a contract
15General AcuteBreast Screening
The national Breast Screening service is in place to detect early stage breast cancer in women. The rates of attendance across the eligible cohort of women in Barnet is significantly below the national target level.
Increase the screening rate to 80% of eligible women screened in 2007/2008.
The inequalities gap for coverage rates in breast screening by Barnet general practices to fall to 30%.
BCFH
16 Reducing Length of Stay
The PCT will be discussing with local acute providers splitting the national tariff where LoS has demonstrably fallen and greater service demands are is being absorbed by community services.
The PCT will be piloting a range of split tariffs during 2007/8 with a view to implementing them formally in 2008/9.
Mental Health
17Early Intervention in Psychosis (EIP)
The PCT will be extending the EIP service from the one pilot area operating in High Barnet to the whole of the borough. The areas of roll out will be determined by the expected health gain by population and the support of primary care and the primary mental health team functionality.
The number of the population to be covered will be set in early 2007 with an expectation of having specific contact and admission avoidance targets in place by 1st April.
The PCT public health department in conjunction with Barnet, Enfield and Haringey Mental Health Trust will carry out detailed clinical effectiveness audit and review
BEH MHT
4
BPCT Commissioning Prospectus 2007/8
during 2007/2008 to assess the value for money of the service.
18Crisis Resolution and Home Treatment
The PCT and Mental Health Trust is failing to meet the target levels of clients coverage as set in the 2005/2008 Local delivery Plan (LDP). An action plan to address the shortfall is in place in 2006/2007 including a specific performance improvement bonus of £50,000. This will be continued in 2007/2008 with the funds deducted from the SLA payable on successful completion of the target level.
655 clients to be in receipt of crisis resolution and home treatment contact.
BEH MHT
19Referrals to the Tavistock and Portman
All self referred patients to the Tavistock and Portman services should be reviewed by primary care to ensure that only those referrals that meet PCT protocols remain within their care.
Expectation that there will be a 15% reduction in activity in the family liaison and counselling services
T&P
Primary Care
20Urgent Care Embed the GP in A/E scheme. Funding for pilot withdrawn at year end and expect to be
self-funding from April 2007.Will also be considering a longer-term model for primary care in A/E.
BCFH
21Non-GP services Support to relocation of patient care Will be looking at potential to expand role of dentists,
pharmacists and optometrists in moving focus of patient care from acute to community setting.
All acute trusts with whom the PCT has a contract
22GP Services Demand and capacity modelling Will be undertaking demand and capacity modelling to
identify inequities and look at potential to extend opening hours in PMS practices.
All acute trusts with whom the PCT has a contract
Older People
23Continuing Care All Category 1 full health funded continuing
care clients and all those on Category 2 joint packages of care will be reviewed to ensure that appropriate packages of care are being provided and that all care is being funded in line with the legal guidance from Capsticks. Extra nursing capacity will be commissioned to carry out regular reviews of those on Cat 1 and Cat 2 packages. The PCT will manage the
Expectation that regular reviews of continuing care clients, particularly in adult mental health, will lead to a number of clients being found no longer eligible for continuing care.
Expectation that joint packages of care will be funded on an assessed health needs basis only. A reduction in spend of over £1m on joint packages of care is expected.
Expectation that more effective market management of surrounding PCTs and LAs will maintain a fair price for
All providers of services for Older People
5
BPCT Commissioning Prospectus 2007/8
market by first managing the placement of patients by out of borough PCTs and LAs. The PCT will also manage the market by opposing planning applications for additional nursing and residential homes. Continuing care clients with the highest levels of need e.g. EMI and those with multiple complex/intense needs will receive the care they need through up-skilling of nursing home staff, or through in house provision. All palliative care patients will have the choice of receiving their end of life care at home, in line with the palliative care quality marker below. The PCT will explore the commissioning of more cost-effective night care services to enable those that live alone the choice to die at home.
placements in Barnet. By preventing further care homes from opening in
Barnet this will reduce the influx of residents from other boroughs and thus prevent significant rises in RNCC and continuing care spend.
Expectation that the costs of care for those with the highest level need could be reduced by more directed commissioning.
Expectation that by unbundling the acute tariff for palliative patients, the savings from shorter stays in hospital can be passed to the community to provide for more cost-effective care at home.
24Intermediate Care Team
Although there the PCT now a single point of access to the Intermediate Care Team, the service is struggling to meet demand and is currently operating at over capacity. The PCT wishes to explore the feasibility of increasing the capacity of the ICT and needs to ensure that there is a stroke specialist on the team.
By increasing the capacity of the intermediate care team the PCT will be in a position to provide a more rapid response. A fast response will aid hospital discharge and prevent unnecessary admissions to hospital. Increased capacity will help more people to improve faster from illness, and maximise their independent living.
All providers of services for Older People
25Community Stroke Services
The PCT wishes to explore extending community services for stroke survivors and their carers, particularly focusing on improving access to information, to support groups, to psychological support and to Carer’s assessments and respite, as set out in the National Audit Office report, November 2005. One excellent example is the “Stroke Survivor’s Project” run in Hackney by a stroke survivor and the Family Support Service run by the Stroke Association.
Enhanced community support for stroke survivors and their carers will reduce the number of stroke patients who have a further stroke, assist younger stroke survivors to return to work, reduce the number who enter expensive long term care and assist carers to continue caring for their loved ones at home, thus greatly reducing the costs to the PCT and Social Services.
All providers of services for Older People
26Community Therapy Services
Community therapy support, such as podiatry, dietetics and diabetic chiropody, is difficult to access in Barnet, and physiotherapy is
Access to community therapy support can be life changing for older people. Individuals will have fewer falls, respiratory conditions, tissue viability problems and
All providers of services for Older People
6
BPCT Commissioning Prospectus 2007/8
currently only available on a short-term basis because demand outstrips capacity. Should any individual require ongoing ‘maintenance’ physiotherapy, for example, the community physiotherapy service does not have the capacity to provide this.
physical disability issues, and through an improved nutritional status will rely less on prescribed nutritional support products which are costly to the PCT. Better access to such services will lead to a reduction in hospital admissions, improve mental well-being and aid independent living.
27Older People’s Mental Health
Mental health is arguably the most neglected area of development in the NSF for Older People to date. With support from the King’s Fund, the PCT and LA aims to develop a joint mental health commissioning strategy for older people and their carers.
The expected outcomes are currently being developed alongside work on needs analysis, carer and user feedback, financial allocations, and an audit of current mental health provision.
Childrens Services
.
28Complex Care Children’s community nursing
The PCT will specify and commission a sole provider of community care for children with complex needs. To develop a PCT skill mix team to work with the home Care nursing from B&C
Set up, employ, train and develop team 2007. April 2007 implement. Initial set up costs but savings from 2008 £77,000 per yearDelivering complex nursing care in children’s homes for 5-6 cases.
All care currently provided from Agency
To develop as agreed in the North London Sector a borough based Children’s community nursing team, (Home Care Team in (HCT) B&C)
Give notice to RFH to redirect Barnet PCT funding to B&C.Teams to develop agreed criteria for care and pathways and protocols.Linking work with and becoming part of the above home Care Team.Develop standards and care across Barnet & Enfield developing a net work.Provide care across the borough. No children to be in hospital who meet the criteria for discharge to the HCT.
Currently there is a geographical gap where approximately 7,000 children & young people would not receive a service. This has stopped some children being discharged home.All cases that meet the criteria will be appropriately discharged home.
29Paediatric acute Develop new paediatric model Paediatric re modelling to reduce the use of out patients by
25-50%, developing new community service – dependent on financial modelling making this viable as qualified paediatric
Currently 25% new patient referrals seen in OPD do not
7
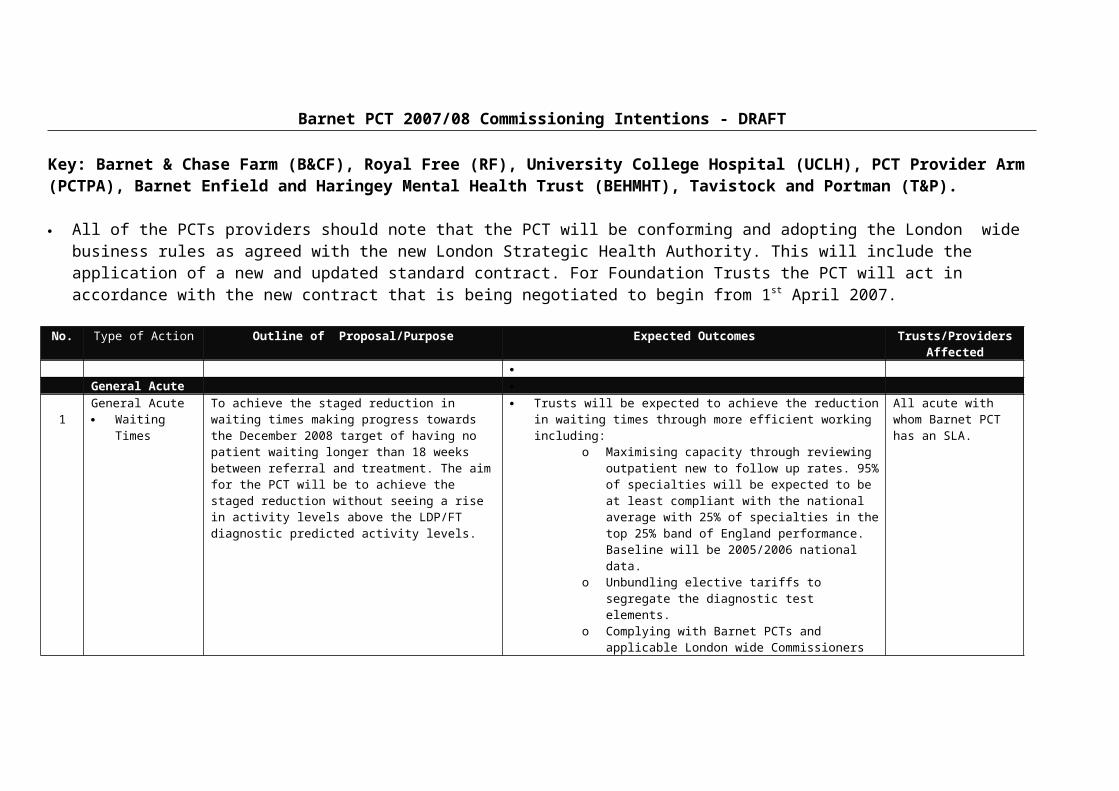
BPCT Commissioning Prospectus 2007/8
professionals will need to be available to deliver the service. receive any diagnosis, investigation or treatment.
30Long Term Conditions As part of the re modelling of paediatric out patient new and
follow up patients – redirecting service’s into community, improving the management in community avoiding hospital referral will include long term conditions such as:DermatologyRespiratory DiabetesAim to deliver up to 25% care in a community setting.
Work to be researched. To improve community care.
Learning and Physical Disability
31The reprovision of NHS Campus Services
Currently there are 8 people with a learning disability living in NHS campus provision on the Harperbury site. In accordance with Valuing People, all remaining NHS Campus provision should be reprovided into a community setting, and a Project Board will be established to manage the tendering process and reprovision of these individuals into community services in Barnet by April 2008.
Successful delivery of Valuing People with increased quality of life within a community setting.
Hertfordshire Partnership NHS Trust
32Effectively managing Assessment and Treatment
Currently Assessment and Treatment are provided within a hospital setting at high cost. A review will be conducted to consider local community based options through an outreach service from Ballards Lane and avoid future admissions.
A reduction in the number of admissions and duration of the assessment period.
Hertfordshire Partnership NHS Trust/Barnet and Chase Farm NHS Trust
33
A review of psychology and psychiatry support
A review of the sub-commissioning arrangements in relation to psychology and psychiatry LD services.
A revised SLA that ensures that the structure of thee service is aligned with people’s needs and expectations.
Barnet, Enfield and Haringey NHS Trust
Quality Markers
Q1 Quality marker Reduce unnecessary patient journeys Reduce the number of outpatient follow ups to ensure that 95% of specialties are operating at or above the
All acute and mental health trusts
8

BPCT Commissioning Prospectus 2007/8
national average performance level as set using the 2005/2006 England position.
with whom the PCT has an SLA.
Q2 Quality marker Quality of clinical care and planned and appropriate discharge.
Reduce the number of readmissions within 28 days following discharge for patients>65 by 10% on the 2006 year position for the HRGs covering all ages : fractured neck of femur with/& without
complications Stroke (CVA) with/without complications COPD with/without complications
Expect a reduction in the readmissions to acute hospitals within 7 days from the PCTs two community hospitals.
Rate for #NOF CVA COPD
Specific metrics to be set based on the 2006 calendar year position.
Reduce by 10% at Finchley and 15% at Edgware Community Hospitals the level of readmissions within 7 days over the levels recorded in 2006 calendar year.
Q3 Quality markers Reduce unnecessary patient journeys Reduce the number of outpatient follow ups to ensure that 95% of specialties are operating at or above the national average performance level as set using the 2005/2006 England position.
All acute and mental health trusts with whom the PCT has an SLA.
Q4 Quality marker Quality of clinical care and planned and appropriate discharge.
Reduce the number of readmissions within 28 days following discharge for patients>65 by 10% on the 2006 year position for the HRGs covering all ages : fractured neck of femur with/& without
complications Stroke (CVA) with/without complications COPD with/without complications
Expect a reduction in the readmissions to acute hospitals within 7 days from the PCTs two community hospitals.
Rate for #NOF CVA COPD
Specific metrics to be set based on the 2006 calendar year position.
Reduce by 10% at Finchley and 15% at Edgware Community Hospitals the level of readmissions within 7 days over the levels recorded in 2006 calendar year.
Q5 Quality marker Provide improved care and services for Reduce by 10% from the 2006 calendar year
9
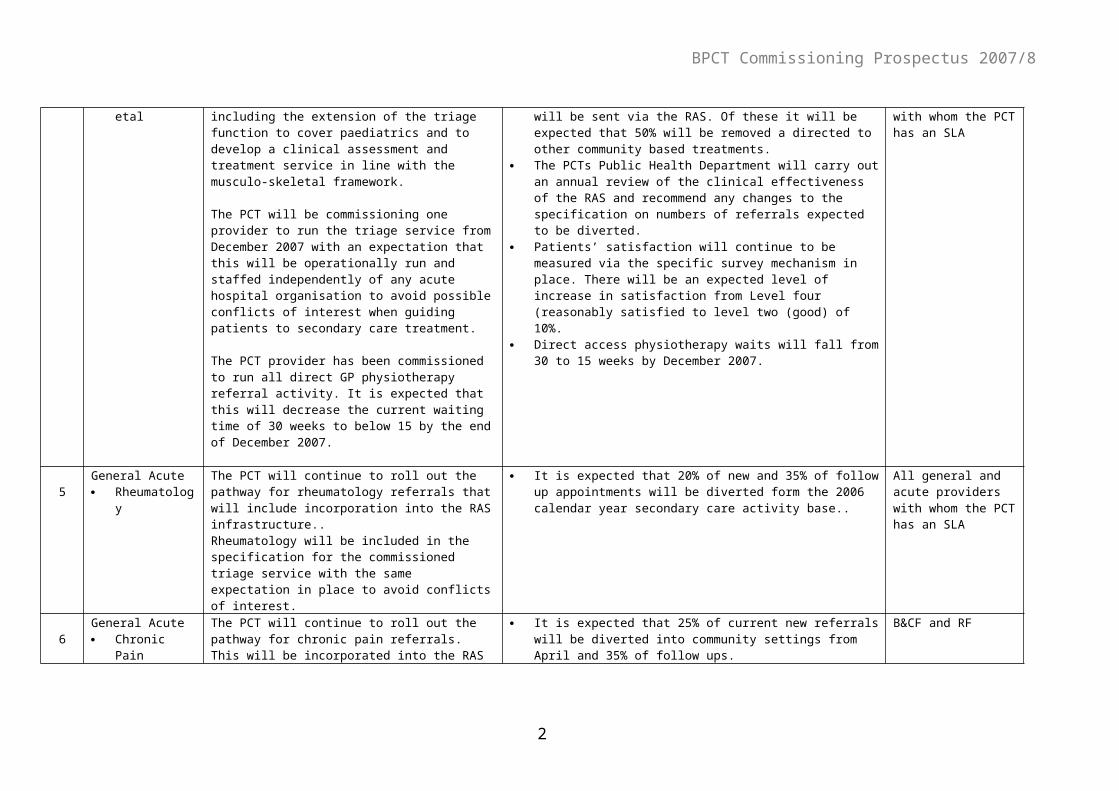
BPCT Commissioning Prospectus 2007/8
patients who area terminally ill baseline the number of patients with a diagnosis of cancer dying in hospital
Increase the number of cancer patients receiving palliative care in the community from the 2006 calendar year baseline.
Q6 Quality marker NHS Funded Continuing care and assuring that all patients in receipt of approved care packages receive at least two annual reviews by a specialist nurse practitioner.
All patients on a NHS funded continuing care package receive an appropriate face to face case review. This will be audited by the PCTs Commissioning quality adviser
Q7 Quality Marker Patient satisfaction survey indicators at the lead acute and mental health trusts and community and primary care facilities will each have a clear target of improvement assigned to one areas each.
Improve the information patients receive, in a way they can understand, about their condition, care and/or treatment by 10%.
Improve the privacy, dignity and respect patients receive when being treated by 5%
Increase compliance with hand hygiene and improve environmental cleanliness by 10%
B&CF, RF and BEHMHT B&CF, RF and BEHMHT B&CF and RF
Q8 Quality Marker Primary care improvement Detailed lists of performance targets are incorporated into the performance frameworks for the following areas in primary care:
General Practice – GMS and PMSGeneral Dental Services and PDSPharmacists
Specific quality indicators and measurable targets are included and are monitored annually.
A specific target around access to primary care is being considered at present. Evidence is being reviewed on the number of appointments practices should plan for per annum, for each patient, together with a study of the opening hours and general patient access needs.
Q9 Quality Marker Children & Young People
All self-referred patients to the Tavistock and Portman services should be reviewed by
Expectation that there will be a 12% reduction in activity in the Children and Young People's departments. All self and carer referrals will require prior agreement with the appropriate commissioner (GP, of PCT
Tavistock and Portman Services
10
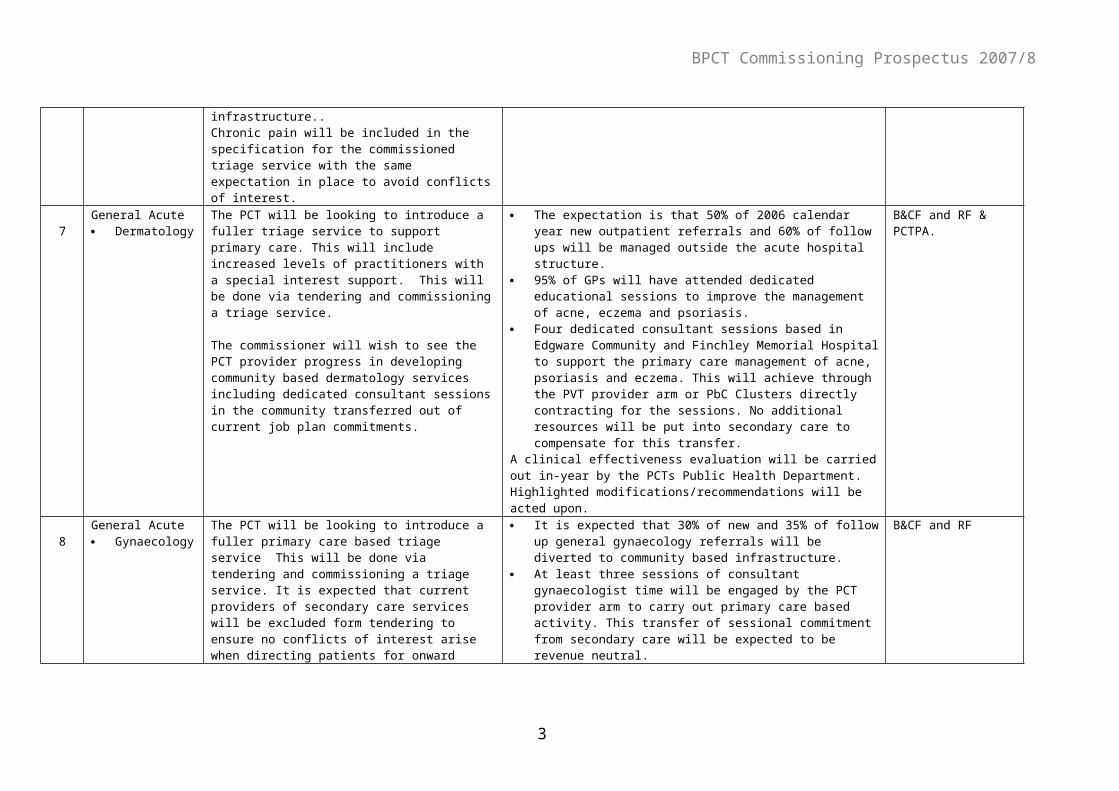
BPCT Commissioning Prospectus 2007/8
primary care to ensure that only those referrals that meet PCT protocols remain within their care.
representative). All referrals to the Young Person and Parent Consultation service to be limited to the agreed number of interventions (4 sessions).
This approach has been implemented with adult services and in this year with the children and families team, this commissioning decision will be of particular relevance to adolescent services (individual therapy, the young person's consultation service, parents service and trauma unit) .
Q10 Quality Marker Fit for Purpose workforce:
Obtain assurances that provider Trusts have action plans in place in response to annual NHS Staff Attitude Survey findings from questionnaire domains relating to access to training and development.
Action plans being implemented to ensure staff are appropriately qualified and trained to deliver services in line with commissioner requirements.
Staff Attitude survey results on responses to training and development issues show progress between 2006 and 2007 findings for each Trust and in comparison to similar Trusts nationally.
11
Related Documents











