COLORECTAL NSSG (Lancs & South Cumbria) Constitution and Terms of Reference 2015

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

COLORECTAL NSSG (Lancs & South Cumbria)
Constitution and Terms of Reference 2015
2 | P a g e
Agreements:
Agreed by: Mr Tom Raymond, Consultant Colorectal Surgeon, University Hospitals of Morecambe Bay NHS Trust and Chair of NSSG
Date: 29/09/2015
Agreed by: Members of the Colorectal NSSG
Date: 29/09/2015
Agreed by: Dr Gerry Skailes, Clinical Lead for Cancer, GML&SC SCN
Date: Not validated – self assessment undertaken by the NSSG
Review date: March 2016
3 | P a g e
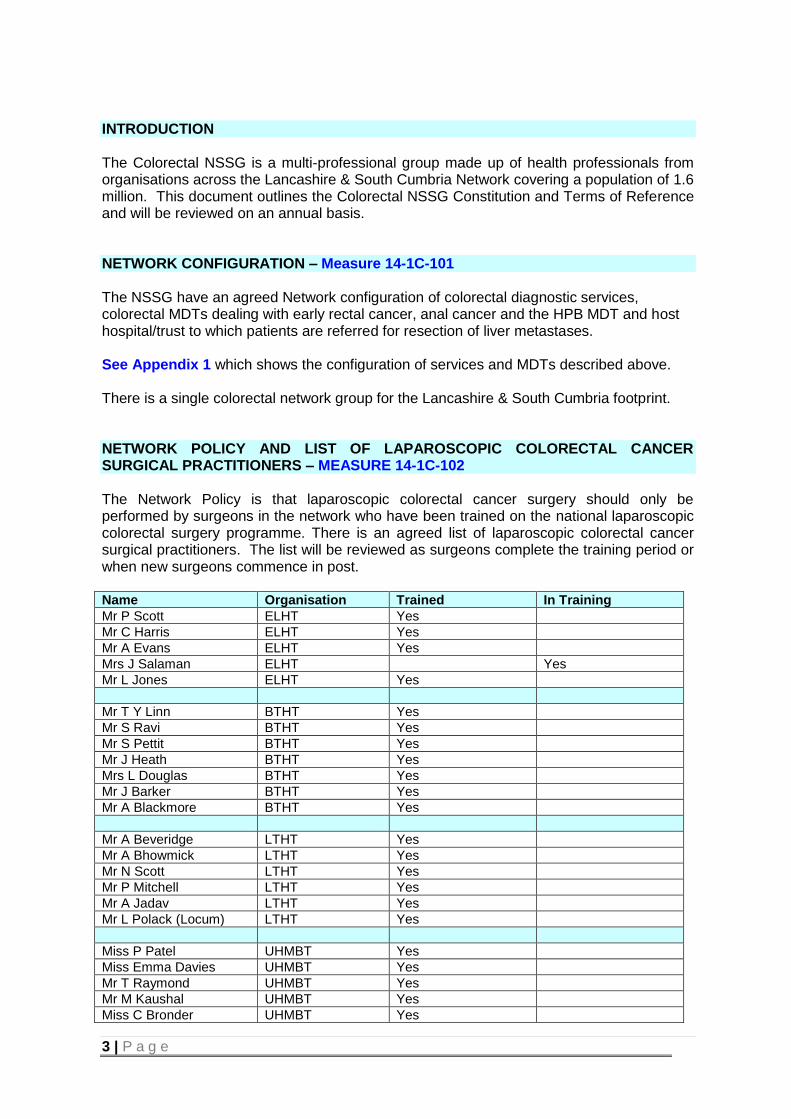
INTRODUCTION The Colorectal NSSG is a multi-professional group made up of health professionals from organisations across the Lancashire & South Cumbria Network covering a population of 1.6 million. This document outlines the Colorectal NSSG Constitution and Terms of Reference and will be reviewed on an annual basis. NETWORK CONFIGURATION – Measure 14-1C-101 The NSSG have an agreed Network configuration of colorectal diagnostic services, colorectal MDTs dealing with early rectal cancer, anal cancer and the HPB MDT and host hospital/trust to which patients are referred for resection of liver metastases. See Appendix 1 which shows the configuration of services and MDTs described above. There is a single colorectal network group for the Lancashire & South Cumbria footprint. NETWORK POLICY AND LIST OF LAPAROSCOPIC COLORECTAL CANCER SURGICAL PRACTITIONERS – MEASURE 14-1C-102 The Network Policy is that laparoscopic colorectal cancer surgery should only be performed by surgeons in the network who have been trained on the national laparoscopic colorectal surgery programme. There is an agreed list of laparoscopic colorectal cancer surgical practitioners. The list will be reviewed as surgeons complete the training period or when new surgeons commence in post. Name Organisation Trained In Training
Mr P Scott ELHT Yes
Mr C Harris ELHT Yes
Mr A Evans ELHT Yes
Mrs J Salaman ELHT Yes
Mr L Jones ELHT Yes
Mr T Y Linn BTHT Yes
Mr S Ravi BTHT Yes
Mr S Pettit BTHT Yes
Mr J Heath BTHT Yes
Mrs L Douglas BTHT Yes
Mr J Barker BTHT Yes
Mr A Blackmore BTHT Yes
Mr A Beveridge LTHT Yes
Mr A Bhowmick LTHT Yes
Mr N Scott LTHT Yes
Mr P Mitchell LTHT Yes
Mr A Jadav LTHT Yes
Mr L Polack (Locum) LTHT Yes
Miss P Patel UHMBT Yes
Miss Emma Davies UHMBT Yes
Mr T Raymond UHMBT Yes
Mr M Kaushal UHMBT Yes
Miss C Bronder UHMBT Yes
4 | P a g e
NETWORK COLORECTAL STENTING POLICY AND NAMED PERSONNEL COMPETENT FOR COLORECTAL STENTING - Measure 14-1C-103
STENTING FOR COLORECTAL CANCER OBSTRUCTION
Given the hazards of presentation with malignant large bowel obstruction we now outline
what we believe constitutes a reasonable approach to the management of this condition.
We begin with the acceptance that this is an unpredictable condition that in the large
majority of patients presents through the emergency room.
History, examination and plain abdominal films suggest the diagnosis of obstruction. At
this point a small minority of patients (13/1094 - Tekkis et al 2004) will not be fit for any
technical intervention and should be managed without surgery.
Similarly a small number of patients (about 1% - Deen et al 1998) will have signs of
peritonitis and will need to proceed through resuscitation to an emergency laparotomy
(13.1% - Tekkis et al 2004).
The large majority of patients who present with malignant large bowel obstruction,
however, should be stable enough to undergo CT confirmation (within 12 -24 hours of
admission) of the site and the nature of the obstruction along with assessment of distant
metastatic disease. Thereafter the following options should be considered:
The current evidence supports the large majority of patients with malignant
obstruction proximal to the splenic flexure, being dealt with by laparotomy, resection
of the obstructing lesion and ileocolonic anstomosis (Lee et al 2001). Only a
minority of patients with proximal obstruction will be suitable for self expanding
metal stents (Khot et al 2002).
Patients with malignant obstruction distal to the splenic flexure should be
considered for stenting of the obstructing tumour within 24 hours of admission.
Successful stenting in those patients with systemic disease should be regarded as
the definitive palliative therapy. Oncological referral and palliative chemotherapy if
appropriate should be considered.
Patients with successful stenting and no sytemic disease should be subjected to an
elective colonic resection (Mainar et al 1999 , Meisner et al 2004, Saida et al 2003)
with the aim of restoration of continuity – having been optimised, received stoma
counselling and elective bowel preparation.
Unsuccessful or complicated stenting requires urgent surgical intervention. The
options include simply raising a proximal stoma, resection with exteriorisation,
resection with on table lavage and anastomosis with or without a proximal stoma.
5 | P a g e
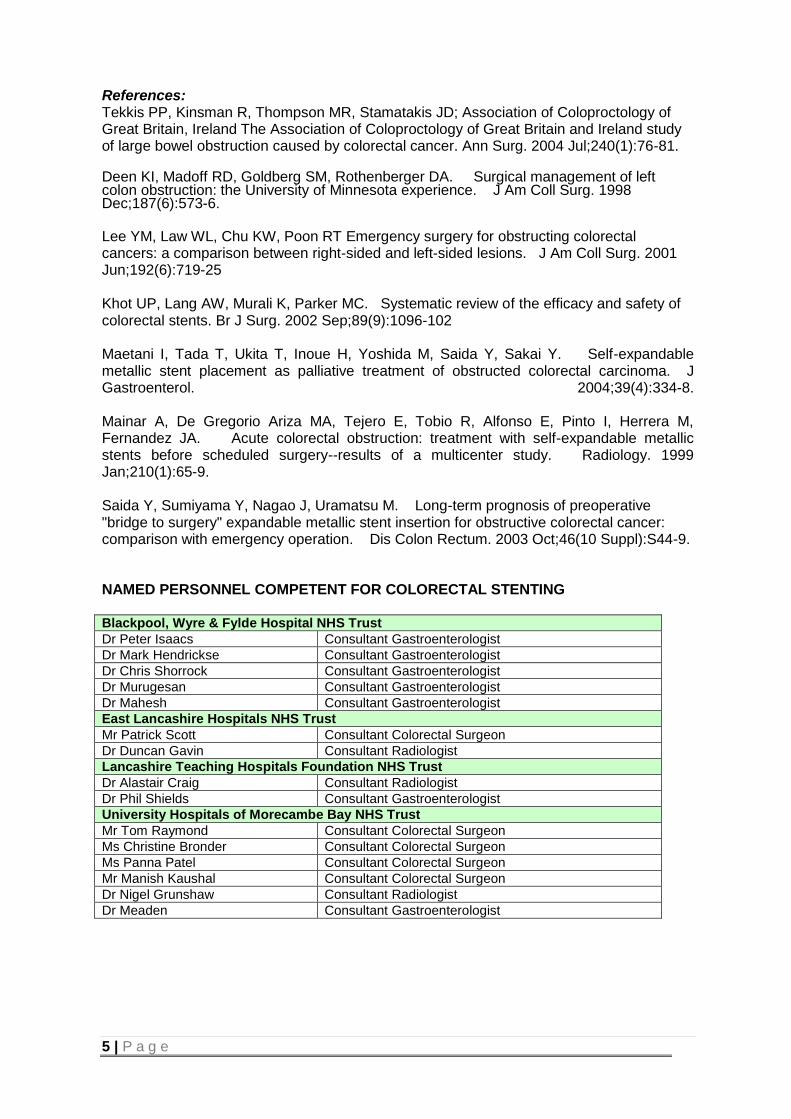
References: Tekkis PP, Kinsman R, Thompson MR, Stamatakis JD; Association of Coloproctology of Great Britain, Ireland The Association of Coloproctology of Great Britain and Ireland study of large bowel obstruction caused by colorectal cancer. Ann Surg. 2004 Jul;240(1):76-81. Deen KI, Madoff RD, Goldberg SM, Rothenberger DA. Surgical management of left colon obstruction: the University of Minnesota experience. J Am Coll Surg. 1998 Dec;187(6):573-6. Lee YM, Law WL, Chu KW, Poon RT Emergency surgery for obstructing colorectal cancers: a comparison between right-sided and left-sided lesions. J Am Coll Surg. 2001 Jun;192(6):719-25 Khot UP, Lang AW, Murali K, Parker MC. Systematic review of the efficacy and safety of colorectal stents. Br J Surg. 2002 Sep;89(9):1096-102 Maetani I, Tada T, Ukita T, Inoue H, Yoshida M, Saida Y, Sakai Y. Self-expandable metallic stent placement as palliative treatment of obstructed colorectal carcinoma. J Gastroenterol. 2004;39(4):334-8. Mainar A, De Gregorio Ariza MA, Tejero E, Tobio R, Alfonso E, Pinto I, Herrera M, Fernandez JA. Acute colorectal obstruction: treatment with self-expandable metallic stents before scheduled surgery--results of a multicenter study. Radiology. 1999 Jan;210(1):65-9. Saida Y, Sumiyama Y, Nagao J, Uramatsu M. Long-term prognosis of preoperative "bridge to surgery" expandable metallic stent insertion for obstructive colorectal cancer: comparison with emergency operation. Dis Colon Rectum. 2003 Oct;46(10 Suppl):S44-9. NAMED PERSONNEL COMPETENT FOR COLORECTAL STENTING Blackpool, Wyre & Fylde Hospital NHS Trust
Dr Peter Isaacs Consultant Gastroenterologist
Dr Mark Hendrickse Consultant Gastroenterologist
Dr Chris Shorrock Consultant Gastroenterologist
Dr Murugesan Consultant Gastroenterologist
Dr Mahesh Consultant Gastroenterologist
East Lancashire Hospitals NHS Trust
Mr Patrick Scott Consultant Colorectal Surgeon
Dr Duncan Gavin Consultant Radiologist
Lancashire Teaching Hospitals Foundation NHS Trust
Dr Alastair Craig Consultant Radiologist
Dr Phil Shields Consultant Gastroenterologist
University Hospitals of Morecambe Bay NHS Trust
Mr Tom Raymond Consultant Colorectal Surgeon
Ms Christine Bronder Consultant Colorectal Surgeon
Ms Panna Patel Consultant Colorectal Surgeon
Mr Manish Kaushal Consultant Colorectal Surgeon
Dr Nigel Grunshaw Consultant Radiologist
Dr Meaden Consultant Gastroenterologist

6 | P a g e
NETWORK GROUP MEMBERSHIP AND TERMS OF REFERENCE Measure 14-1C-104 Mr Tom Raymond Consultant Colorectal Surgeon (NSSG Chair) UHMBT
Ms Christine Bronder Consultant Colorectal Surgeon (MDT Lead Clinician) (Vice Chair) UHMBT
Miss Panna Patel Consultant Colorectal Surgeon UHMBT
Mr Manish Kaushal Consultant Colorectal Surgeon UHMBT
Mrs Emma Davies Consultant Colorectal Surgeon UHMBT
Jayne Scothern Colorectal Nurse Specialist UHMBT
Suzanne Thompson Colorectal Nurse Specialist UHMBT
Mr Thu Linn Consultant Colorectal Surgeon (MDT Lead Clinician) BTHT
Mr Ravi Consultant Colorectal Surgeon BTHT
Mr Jonathan Heath Consultant Colorectal Surgeon BTHT
Ms Lynn Douglas Consultant Colorectal Surgeon BTHT
Mr A Blackmore Consultant Colorectal Surgeon BTHT
Dr Sin Lau Consultant Oncologist BTHT
Gill Towers Colorectal Nurse Specialist BTHT
Sharon Iddon Colorectal Nurse Specialist BTHT
Shelly Gregson Colorectal Nurse Specialist BTHT
Nickie Ritchie Colorectal Nurse Specialist BTHT
Mr Alan Beveridge Consultant Colorectal Surgeon (MDT Lead Clinician) LTHT
Mr Nigel Scott Consultant Colorectal Surgeon LTHT
Mr Peter Mitchell Consultant Colorectal Surgeon LTHT
Dr Mike Dobson Consultant Radiologist LTHT
Dr Mark Pitt Consultant Pathologist LTHT
Dr Marcus Wise Consultant Oncologist LTHT
Dr Deborah Williamson Consultant Oncologist LTHT
Dr Shabbir Susnerwala Consultant Oncologist LTHT
Kim Moxham Colorectal Nurse Specialist LTHT
Cath Boyle Colorectal Nurse Specialist LTHT
Maria McEneaney Colorectal Nurse Specialist LTHT
Mrs Judith Salaman Consultant Colorectal Surgeon (MDT Lead Clinician) ELHT
Mr Patrick Scott Consultant Colorectal Surgeon (Deputy for JS) ELHT
Mr David Chang Consultant HPB Surgeon ELHT
Andrea Darbyshire Colorectal Nurse Specialist ELHT
Miranda Darbyshire Colorectal Nurse Specialist ELHT
Tracy Hacking Colorectal Nurse Specialist ELHT
Joanne Thomas HPB Specialist Nurse ELHT
Pat Lord Patient representative
Scott Alker Quality Improvement Manager (Peer Review) SCN
Vicki Wagstaff NSSG Administrator SCN
Extended Members:
Dr Mark Hendrickse Consultant Gastroenterologist/Lead Clinician Lancs Bowel Screening Prog
BTHT
Dr Colin Brown Consultant Gastroenterologist/Lead Clinician Cumbria Bowel Screening Prog
UHMBT
Linda Pickles Colorectal Nurse Specialist UHMBT

7 | P a g e
Role and Function of Group The role and purpose of the Colorectal NSSG is to improve the experience and outcomes of cancer care for colorectal patients in the Lancashire & South Cumbria Network. This involves consideration of strategies and plans for service improvement and service development across the patient pathway, incorporating all aspects of care at appropriate stages of the patient’s journey. The aim is to achieve the best possible outcomes and best quality of life for all patients who use colorectal cancer services within the Network.
The Colorectal NSSG: Is the Network’s primary source of clinical opinion on issues relating to colorectal
cancer for the Network
Is the group with corporate responsibility for co-ordination and consistency across the Network for policy, practice guidelines, audit, research and service improvement relating to colorectal cancer.
Will consult with the relevant cross-cutting Network groups on issues involving chemotherapy, cancer imaging, histopathology and laboratory investigation and specialist palliative care; and with the Head of Service on issues involving radiotherapy.
Members of the NSSG will be responsible for feeding back information/decisions from the NSSG to their clinical and managerial colleagues.
NETWORK GROUP MEETINGS – MEASURE 14-1C-105
The group will meet three times per year (two business meetings and one educational event). Notes of the meeting will be produced and attendance recorded. The group will be deemed to be quorate if there is representation from three of the four localities or five of the member groups. A deputy should be sent. The Colorectal NSSG will have a Chair elected from within the membership of the NSSG and the period of tenure will be for an initial period of two years then reviewed every two years after. Election of the Chair will be through a process of expressions of interest. The current Chair is Mr Tom Raymond, Consultant Colorectal Surgeon, University Hospitals of Morecambe Bay NHS Trust. Miss Christine Bronder, Consultant Colorectal Surgeon, University Hospitals of Morecambe Bay NHS Trust is the nominated Vice-Chair. One of the NHS employed members will be nominated as having specific responsibility for user issues and information for patients/carers. The nominated member is Kim Moxham, Colorectal Nurse Specialist, Lancashire Teaching Hospitals Trust. One of the NHS employed members will be nominated as having responsibility recruitment into trials and other well designated studies is integrated into the function of the NSSG. The nominated member is Dr Deborah Williamson, Consultant Oncologist, Lancashire Teaching Hospitals Trust.
Extended membership - the group will identify and recommend membership of other appropriate professionals as required, to achieve the objectives of the group. In instances where only one user representative is available, the Cancer Partnership Group have agreed to provide additional advice as and when required to the NSSG meetings. NSSG ANNUAL REPORT AND WORK PROGRAMME – MEASURE 14-1C-106 The NSSG will produce an annual report and work programme.

8 | P a g e
CLINICAL GUIDELINES FOR COLORECTAL CANCER Measure 14-1C-107
The NSSG agreed to adopt the NICE Clinical Guidelines 131 on the diagnosis and management of colorectal cancer (November 2011) as the Network Clinical Guidelines. http://www.nice.org.uk/guidance/CG131. These are supported by local guidelines for the clinical management of patients with anal cancer, early rectal cancer and liver metastases. CLINICAL GUIDELINES FOR ANAL CANCER Measure 14-1C-108 The NSSG have an agreed set of clinical guidelines for the clinical management of patients with anal cancer. See separate document – Clinical Guidelines and Pathways CHEMOTHERAPY TREATMENT ALGORITHMS Measure 14-1C-109 The NSSG have an agreed set of acceptable chemotherapy treatment algorithms which have been agreed with the Chemotherapy network group. See Appendix 2 for Chemotherapy Treatment Algorithms PATIENT PATHWAYS FOR COLORECTAL CANCER Measure 14-1C-110 The NSSG has developed patient pathways which identify the named services, hospitals and MDTs which a patient should be referred to according to named indications, during their investigation, treatment, psychological and social support, rehabilitation and follow-up). PATIENT PATHWAYS FOR ANAL CANCER Measure 14-1C-111 The NSSG has developed patient pathways which identify the named services, hospitals and MDTs which a patient should be referred to according to named indications, during their investigation, treatment, psychological and social support, rehabilitation and follow-up). See separate document – Clinical Guidelines and Pathways REFERRAL TO DIAGNOSTIC SERVICES AND ONWARD REFERRAL Measure 14-1C-112 Referral to Diagnostic Services: The NSSG have produced a set of network-wide guidelines for primary care practitioners on the referral for diagnosis of patients with potential colorectal cancer. The guidelines require practitioners to refer to a network agreed colorectal diagnostic service, not a named individual consultant, and to use a network-agreed referral pro-forma. The pro-forma specifies which type of presentation should be referred with which level of priority. The guidelines contain the single referral contact point for each trust hosting a colorectal diagnostic service. The primary care guidelines were distributed to all primary care practices in the network via the Lancs & South Cumbria Agency.
9 | P a g e
Onward Referral from the Diagnostic Service: The NSSG have agreed a policy governing onward referral from the colorectal diagnostic service when a diagnosis is made of either malignant disease or non-malignant disease. This policy will ensure that timely and appropriate communication is in place between clinicians and with the patient. This covers onward referral of patients diagnosed with colorectal cancer or non-malignant disease. Members of the colorectal diagnostic service are part of the MDT. Details of the policy are as follows: Patients who are unexpectedly diagnosed with colorectal cancer or known patients who
are diagnosed with recurrent or metastatic disease will be referred to a core member of the MDT within one full working day of the diagnosis being made. In most cases this will be the Colorectal Nurse Specialist.
The core member of the MDT will ensure that such patients are discussed at the next
MDT. If cancer is detected, the Radiology Department (Radiologist/Radiographer) or
Pathologist will report the result to the referring clinician. The Clinical Nurse Specialist/MDT Co-ordinator will be alerted by a cancer “flag” on the hospital PAS system or by a list generated from the laboratory computer system.
The referring clinician (or Team) (ie clinician requesting the image) is responsible for
informing the patient of their diagnosis verbally. If the image has been undertaken following GP direct access, the Clinical Nurse
Specialist will contact the GP by telephone to discuss further investigations as appropriate. The GP is responsible for informing the patient of the diagnosis.
If a patient has been diagnosed via endoscopy, the performing endoscopist is
responsible for informing the patient of the diagnosis and onward referral to the MDT. The performing endoscopist is also responsible for informing the GP of the diagnosis.
If non-malignant disease is diagnosed and further investigation or treatment is required,
the report is sent to the referring clinician who will inform the patient and organise further investigation.
The GP will be informed of a diagnosis of malignancy by the following working day after
the patient has been informed. This will normally be undertaken by the clinical nurse specialist and details are communicated via fax.
Clinical Nurse Specialists may be contacted by bleep, via Hospital Trust switchboards. When non-colorectal cancer is detected, then the Clinical Nurse Specialist in the other
specialty is contacted within one working day.

10 | P a g e
Primary Care Referral Guidelines for patients with potential colorectal cancer Primary Care Practitioners should urgently refer all patients with symptoms suspicious of colorectal malignancy using the current two-week wait referral process established within their locality. Each Trust has a single point for receipt of referrals using locally agreed 2 week wait referral forms. The following protocol outlines the priority that should be given to the different types of clinical presentation for investigation of large bowel problems. The clinical presentations are in accord with the NICE Referral Guidelines for Suspected Cancer 2015 as reflected in the two week wait Urgent Suspected Cancer Pro-forma.
Urgent referrals – patients who present with the following symptoms should be referred urgently using the locally agreed 2ww referral form:
They are aged 40 and over with unexplained weight loss and abdominal pain or;
They are aged 50 and over with unexplained rectal bleeding or;
They are aged 60 and over with: o Iron-deficiency anaemia or o Changes in their bowel habit, or
Tests show occult blood in their faeces (see final recommendation in this list for who should be offered a test for occult blood in faeces) (new 2015)
Consider a suspected cancer pathway referral (for an appointment within 2 weeks) for colorectal cancer in people with rectal or abdominal mass. (new 2015) Consider a suspected cancer pathway referral (for an appointment within 2 weeks) for colorectal cancer in adults aged under 50 with rectal bleeding and any of the following unexplained symptoms or findings:
Abdominal pain
Change in bowel habit
Weight loss
Iron deficiency anaemia (new 2015) Offer testing for occult blood in faeces to assess for colorectal cancer in adults without rectal bleeding who:
Are aged 50 and over with unexplained: o Abdominal pain or o Weight loss, or
Are aged under 60 with o Changes in their bowel habit or o Iron-deficiency anaemia or
Are aged 60 and over and have anaemia even in the absence of iron deficiency (new 2015)
Consider a suspected cancer pathway referral (for an appointment within 2 weeks) for anal cancer in people with an unexplained anal mass or unexplained anal ulceration (new 2015)
11 | P a g e
Referral of patients with symptoms of colorectal pathology but at low risk of cancer: Referral on the Choose and Book System should be considered for patients with the following symptoms and no abdominal or rectal mass who are thus at a very low risk of colorectal cancer: Rectal bleeding with anal symptoms (pain, prolapse, pruritis) Change in bowel habit to decreased frequency of defaecation and harder stools Abdominal pain without clear evidence of intestinal obstruction It is always good practice to perform a rectal examination.
Referral of patients in known high risk groups who develop symptoms: High risk patients who are undergoing screening and surveillance as described in the
national guidance (GUT 2002) who develop symptoms should be referred urgently. Contact details for Colorectal MDTs:
Trust Hospital sites Local MDT
Lancashire Teaching Hospitals Foundation Trust
Royal Preston Hospital
Local Colorectal MDT MDT Co-ordinator Tel 01772 523519
Blackpool Teaching Hospitals Trust
Blackpool Victoria Hospital
Local Colorectal MDT MDT Co-ordinator Tel 01253 303915
East Lancashire Hospitals Trust
Royal Blackburn Hospital
Local Colorectal MDT MDT Co-ordinator Tel 01254 85965
University of Morecambe Bay Hospitals Trust
Royal Lancaster Infirmary Furness General Hospital
Local Colorectal MDT (VC MDT RLI/FGH) MDT Co-ordinator Tel 01524 512493
NETWORK POLICY ON NAMED MEDICAL PRACTITIONER WITH CLINICAL RESPONSIBILITY - Measure 14-1C-113 The NSSG have agreed, in consultation with the MDTs, a policy specifying the medical practitioner (whether primary care practitioner, consultant surgeon, gastroenterologist or investigational consultant) who is considered to be responsible for the patient at each stage from referral from primary care to the treatment planning decision of the colorectal MDT.
The policy in the Network is as follows: Referral - the referring GP has responsibility for the patient until the receipt of the referral by the named service.

12 | P a g e
The GP may refer the patient to an acute named Trust, bowel screening programme or CATS for investigation.
Referral to the hospital On receipt of the GP referral the Trust will allocate a named registered hospital surgeon or investigational Consultant who will be responsible for the patient until the patient is seen. Pooling arrangements are in place and there is an agreed responsibility of care; the named surgeon or investigational consultant who sees the patient initially will have responsibility for the patient’s care throughout the investigational part of their journey; that consultant may not be the named registered consultant who will ultimately assume care for the patient. On referral to imaging colleagues for investigation, the named surgeon or investigational consultant will remain responsible for the patient’s management. CATS & Bowel screening programme Patients who are referred to CATS or bowel screening programme remain the responsibility of the GP at this investigation stage until a diagnosis is made. If a diagnosis of cancer is made and the patient is referred to a colorectal surgical MDT then the named surgical consultant will be responsible for the patient.
Consultant to consultant referral A patient who is admitted under the care of a consultant and who is referred for investigation to a consultant surgeon, investigational gastro-enterologist or imaging consultant, will remain under the care of the referring consultant. NSSG/MDT agreed Guidelines for Surgical Emergencies Measure 14-1C-114 The NSSG have an agreed a set of Guidelines for Surgical Emergencies. See separate document – Clinical Guidelines and Patient Pathways PATIENT EXPERIENCE Measure 14-1C-115 In the course of the regular meetings, the NSSG will annually review patient feedback of their associated MDTs and any actions implemented, and will agree an improvement programme with them. This detail will be recorded in the Annual Report. CLINICAL OUTCOMES INDICATORS AND AUDITS Measure 14-1C-116 In the course of the regular meetings, the NSSG will annually review the progress (or discuss the completed results, as relevant) of their associated MDTs’ outcome indicators and audits, which will have been carried out, or the data examined across all the MDTs.

13 | P a g e
DISCUSSION OF CLINICAL TRIALS Measure 14-1C-117 The Colorectal MDTs feed into two Clinical Research Networks. LTHT, BTHT and UHMBT link into the North West Coast Clinical Research Network and ELHT links into the Greater Manchester Clinical Research Network. Trial recruitment reports are discussed at NSSG meetings and improvement plans agreed. A full year trial recruitment report is included in the Annual Report.

14 | P a g e
Appendix 1 Measure 14-1C-101 : Network Configuration; List of Colorectal MDTs including those dealing with Rectal Cancer, Anal Cancer and Liver Resection The following table lists the local colorectal diagnostic teams, local colorectal MDTs, Network MDTs for Early Rectal, Anal and Liver Resection and their referring catchment populations.
Locality Trust Hospital sites Services /Local MDT/Network MDT Referring Catchment Population
Central Lancs Lancashire Teaching Hospitals Foundation Trust
Royal Preston Hospital
Diagnostic services Local Colorectal MDT Network Anal MDT * (1.6m pop) Early Rectal Cancer ** Radiotherapy Centre (1.6m pop) MDT contact no: 01772 523519
Central Lancs 449,000
Fylde Coast Blackpool Teaching Hospitals Trust Blackpool Victoria Hospital Diagnostic services Local Colorectal MDT MDT contact no: 01253 303915
Blackpool 143,000 North Lancs (Fylde/Wyre) 185,000
East Lancs East Lancashire Hospitals Trust Royal Blackburn Hospital
Diagnostic services Local Colorectal MDT MDT contact no: 01254 85965 Network VC Liver Resection MDT (1.6m pop) *** MDT contact no: 01254 734365
Blackburn with Darwen140,000 East Lancs 382,000
Morecambe Bay University of Morecambe Bay Hospitals Trust Royal Lancaster Infirmary Westmorland General Hospital Furness General Hospital
Diagnostic services (RLI/WGH/FGH) Local Colorectal MDT (VC MDT RLI/FGH)
MDT contact no: 01524 512493
Cumbria (South Lakeland) 173,000 North Lancashire (Lancaster) 137,000
* Referral between units will be as per the Anal Canal and Anal Margin Cancers MDT Guidelines. ** Referral as per the Early Rectal Cancer MDT Referral Guidelines *** Referral as per the Liver Resection MDT Referral Guidelines.
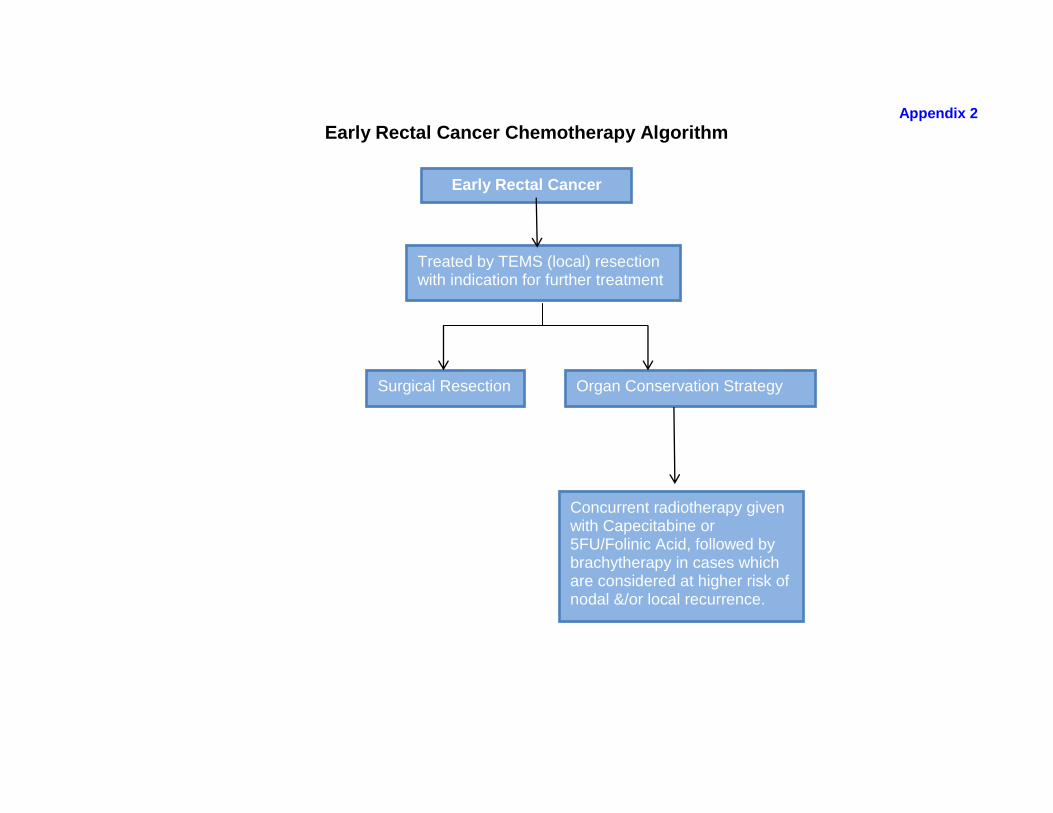
Early Rectal Cancer
Appendix 2
Early Rectal Cancer Chemotherapy Algorithm
Treated by TEMS (local) resection with indication for further treatment
Surgical Resection Organ Conservation Strategy
Concurrent radiotherapy given with Capecitabine or 5FU/Folinic Acid, followed by brachytherapy in cases which are considered at higher risk of nodal &/or local recurrence.

Locally Advanced Colorectal Cancer
Neoadjuvant Colorectal Cancer Chemotherapy Algorithm
Recruitment to clinical trials should be considered where appropriate
Unresectable Colorectal Cancer
Suitable for pre-operative CRT
3 months combination chemotherapy or clinical trial
Resection or consider chemotherapy for unresectable disease
Concurrent radiotherapy given with Capecitabine or 5FU/Folinic Acid or Irinotecan combination or clinical trial
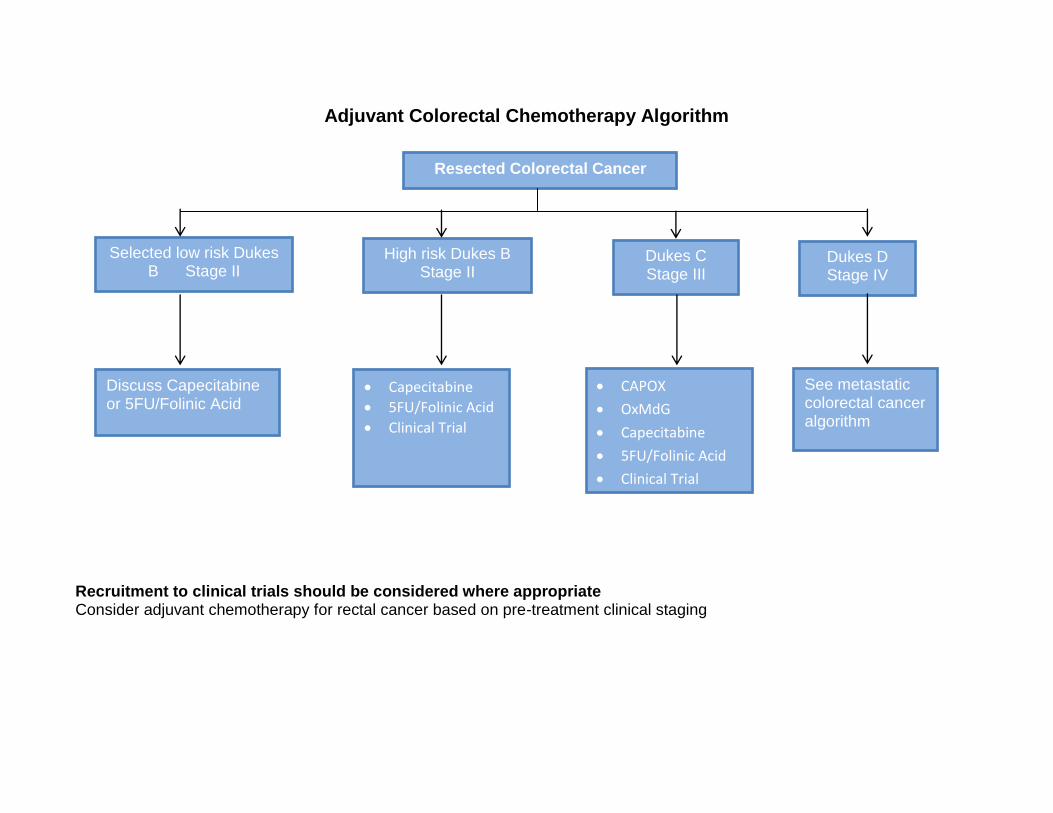
Resected Colorectal Cancer
Adjuvant Colorectal Chemotherapy Algorithm Recruitment to clinical trials should be considered where appropriate Consider adjuvant chemotherapy for rectal cancer based on pre-treatment clinical staging
Selected low risk Dukes B Stage II
High risk Dukes B Stage II
Dukes C Stage III
Dukes D Stage IV
Discuss Capecitabine or 5FU/Folinic Acid
Capecitabine
5FU/Folinic Acid
Clinical Trial
CAPOX
OxMdG
Capecitabine
5FU/Folinic Acid
Clinical Trial
See metastatic colorectal cancer algorithm

Metastatic Colorectal Cancer
Metastatic Colorectal Cancer Chemotherapy Algorithm
Potentially resectable metastatic disease Unresectable metastatic disease
Liver only metastatic disease Resection or 3 months combination chemotherapy prior to resection
Consideration of adjuvant chemotherapy depending on resection margins and histology
Oxaliplatin or Irinotecan based combination chemotherapy or + Cetuximab (if RAS wild type and disease not initially
resectable)1
Resection
Consideration of adjuvant chemotherapy depending on resection margins and histology
1st line chemotherapy
Oxaliplatin or Irinotecan
based combination
chemotherapy +/-
Cetuximab / Panitumumab
(if RAS wild type)3
Clinical Trial
Capecitabine
5FU/Folinic Acid
Raltitrexed2
2nd line chemotherapy
Switch to alternative
Irinotecan or
Oxaliplatin
combination therapy
Oxaliplatin
combination +
Bevacizumab5
Clinical trial
3rd/Subsequent chemotherapy
Previously unused regimen
Cetuximab/ Panitumumab
monotherapy (if RAS wild type)4
Rechallenge with previous
effective regime, clinical trial or
Mitomycin C + Capecitabine or
5FU/Folinic Acid

Recruitment to clinical trials should be considered where appropriate
1. As per NICE recommendation TA176
2. Raltitrexed is not recommended for people with advanced colorectal
cancer outside of clinical trials (NICE recommendation TA93) and may
be considered only in patients intolerant or unsuitable for 5FU or
capecitabine
3. 1st line Cetuximab or Panitumumab (used in combination) funding
available through CDF
4. 3rd or 4th line Cetuximab or Panitumumab monotherapy as per CDF
guidelines
5. 2nd line oxaliplatin combination + Bevacizumab funding available
through CDF
Related Documents