COGNITIVE DEFICITS AND PSYCHIATRIC REHABILITATION OUTCOMES IN SCHIZOPHRENIA Steven M. Silverstein, Ph.D., Lindsay S. Schenkel, Carolyn Valone, M.A., and Scott W. Nuernberger Many patients with schizophrenia are characterized by cognitive deficits that limit their ability to benefit from psychiatric rehabilitation interventions. While this suggests that cognitive rehabilitation is important, more needs to be known about which cognitive deficits interfere with which aspects of outcome and func- tioning before effective interventions are developed. We report data on cognitive predictors of three types of outcome: acquisition and performance of skills in a skills training group; aspects of daily ward functioning; and ability to be dis- charged from a state hospital. Our data indicate that poorer outcomes in each of these areas are associated with different, but somewhat overlapping, profiles of cognitive deficits. These data are relevant for designing both ward-based and individualized interventions. Integrating traditional psychiatric rehabilitation approaches with targeted cognitive interventions is necessary to maximize the impact of psychiatric rehabilitation services on individuals with chronic schizo- phrenia. In recent years, increased attention has been paid to the role of cognitive deficits (e.g., impairments in perception, attention, memory, reasoning) in schizophrenia. This is due to a number of factors, including: 1) cognitive deficits have been identified as sta- ble aspects of the disorder, are found in unaffected relatives sug- Address correspondence to Steven M. Silverstein, Ph.D., University Services Psychiatric Rehabilitation Program, Rochester Psychiatric Center, 1111 Elmwood Avenue, Rochester, NY 14620; e-mail: [email protected]. PSYCHIATRIC QUARTERLY, Vol. 69, No. 3, Fall 1998 0033-2720/98/0900-0169$15.00/0 © 1998 Human Sciences Press, Inc. 169

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

COGNITIVE DEFICITS AND PSYCHIATRICREHABILITATION OUTCOMES IN
SCHIZOPHRENIA
Steven M. Silverstein, Ph.D., Lindsay S. Schenkel,Carolyn Valone, M.A., and Scott W. Nuernberger
Many patients with schizophrenia are characterized by cognitive deficits thatlimit their ability to benefit from psychiatric rehabilitation interventions. Whilethis suggests that cognitive rehabilitation is important, more needs to be knownabout which cognitive deficits interfere with which aspects of outcome and func-tioning before effective interventions are developed. We report data on cognitivepredictors of three types of outcome: acquisition and performance of skills ina skills training group; aspects of daily ward functioning; and ability to be dis-charged from a state hospital. Our data indicate that poorer outcomes in eachof these areas are associated with different, but somewhat overlapping, profilesof cognitive deficits. These data are relevant for designing both ward-based andindividualized interventions. Integrating traditional psychiatric rehabilitationapproaches with targeted cognitive interventions is necessary to maximize theimpact of psychiatric rehabilitation services on individuals with chronic schizo-phrenia.
In recent years, increased attention has been paid to the role ofcognitive deficits (e.g., impairments in perception, attention,memory, reasoning) in schizophrenia. This is due to a number offactors, including: 1) cognitive deficits have been identified as sta-ble aspects of the disorder, are found in unaffected relatives sug-
Address correspondence to Steven M. Silverstein, Ph.D., University ServicesPsychiatric Rehabilitation Program, Rochester Psychiatric Center, 1111Elmwood Avenue, Rochester, NY 14620; e-mail: [email protected].
PSYCHIATRIC QUARTERLY, Vol. 69, No. 3, Fall 19980033-2720/98/0900-0169$15.00/0 © 1998 Human Sciences Press, Inc. 169

gesting that they are a genetically transmitted aspect of the ill-ness, and are viewed as vulnerability factors in the developmentof the disorder; and 2) they have been found to be among thebest predictors of level of functioning and eventual outcome, withbetter predictive ability than symptomatology in many cases (1,2). While cognitive deficits are related to poorer outcomes in ageneral psychiatric population (3), in schizophrenia they are oftenquite severe, and outcomes across a wide range of domains (e.g.,community tenure, work, school) are often poor (1, 2).
Although enough evidence now exists to confidently state thatcognitive deficits are related to lower levels of current and futurefunctioning in schizophrenia, it is not entirely clear which cog-nitive deficits are related to which outcomes. One reason for thisis that studies have varied in their definition of outcome as wellas in their choices of cognitive measures. Moreover, to the extentthat there is consistency across studies, it appears as if at leasttwo types of relationships exist: a class of relationships between"low level" processes such as response preparedness (assessed byreaction time) and certain outcomes, and another class of rela-tionships between higher level processes such as memory andconcept formation and other outcomes. For example, in theschizophrenia literature, there is a long history of looking at therelationships between performance on reaction time (RT) tasksand outcome variables such as hospital length of stay and relapserates. In general, this literature suggests that longer RT on ad-mission predicts poorer eventual outcome (e.g., longer hospitali-zations, faster relapses, etc; 4, 5). These data have beeninterpreted to indicate that a reduction in the ability to respondquickly and consistently to relevant environmental stimuli, or toestablish a "preparatory set" (leading to longer RTs in the labo-ratory), is associated with reduced clinical stability. There is alsoa newer literature, however, that is focusing on the relationshipsbetween other cognitive processes, such as attention and memory,and outcomes such as acquisition of skills in skills training, andin vocational rehabilitation. This literature generally indicatesthat poorer attention and memory leads to less learning of newskills (1, 2). These literatures suggest that different forms ofadaptive behavior may be subserved by unique profiles of cogni-tive functioning. Stated differently, specific behaviors targeted for
PSYCHIATRIC QUARTERLY170
psychiatric rehabilitation intervention may be mediated by variedcognitive functions. This is important because it implies that dif-ferent cognitive remediation strategies may be needed to improvedifferent outcomes. Prior to developing cognitive rehabilitation in-terventions, however, the nature of the cognition-outcome rela-tionships must be clarified.
In this report, we discuss ongoing research at the Universityof Rochester Medical Center and Rochester Psychiatric Centerthat has systematically explored these relationships. We have ex-plored the associations between cognitive deficits and three typesof outcomes thus far: 1) performance and skill acquisition in so-cial skills training groups; 2) aspects of ward functioning thatare relevant to successful placement in the community (e.g.,grooming, mealtime behaviors, lateness, bizarre behavior, hostil-ity, etc.); and 3) success in being discharged from the hospital.By looking at multiple forms of outcome and using a battery ofmeasures that covers many of the cognitive processes hypothe-sized to be involved in the disabilities of patients with schizo-phrenia, our eventual goal is to develop "profiles of cognitivefunctioning" relevant to different outcomes and to developing spe-cific and effective cognitive interventions.
BATTERY OF COGNITIVE MEASURES
All of the outcomes were studied as a function of their relation-ships to a core group of cognitive measures, completed by patientson admission to a long-term inpatient psychiatric rehabilitationprogram (see below). In some cases, studies of specific aspects ofcognition that were being conducted at the same time as the out-come study allowed us to explore the predictive strength of anew variable in relation to one form of outcome. The core batteryincluded measures that had demonstrated a strong ability to pre-dict outcome in past studies (6) as well as tests whose predictiveability was unknown, but that assessed cognitive functions be-lieved to mediate skill acquisition. It included measures of: per-ceptual organization (7); simple auditory reaction time, assessingresponse preparedness and response inhibition (8); visual infor-mation processing (UCLA Degraded Stimulus Continuous Per-
SILVERSTEIN ET AL. 171
formance Test-1 DSCPT; 9); sustained visual attention (SustainedAttention Test; 10); verbal memory (Rey Auditory Verbal Learn-ing Test; 11); conceptual flexibility (Wisconsin Card Sorting Test;12); and verbal intelligence (13).
RESEARCH SETTING
Participants were chronic schizophrenia patients on the Univer-sity Services Psychiatric Rehabilitation Program (USPRP) at theRochester Psychiatric Center, a state psychiatric facility. This isa 30 bed long-term, behavioral inpatient unit focusing on skillstraining (14) and other psychiatric rehabilitation interventions(15-17). The USPRP opened in June 1993. All patients admittedto this program came from other units at the Rochester Psychi-atric Center, where they had already been hospitalized for a con-siderable length of time. Participants in this research metDSM-III-R (before 1994) or DSM-P7 criteria for schizophrenia asdetermined by a psychologist (SMS) and a psychiatrist, and bythe Structured Clinical Interview for either DSM-III-R (SCID- P;18) or DSM-IV Diagnosis (SCID-I/P; 19) conducted by trained re-search assistants.
OUTCOMES IN SOCIAL SKILLS TRAINING
Skill Performance
Our earliest studies examined performance at the end of theUCLA Basic Conversation Skills (BCS) module, a form of socialskills training. We studied this variable because some previousstudies of cognition-outcome relationships used module perform-ance as their dependent variable, and in some of those studies,performance was conceptualized as "total skill acquisition" (20).We believe the concept of performance at the end of the moduleis a relevant variable, although not necessarily the most relevantone. That is, because "performance" does not tell you anythingabout how much was actually learned, we see it more as a meas-ure of overall functioning than as an index of skill acquisition.Nevertheless, because it would be useful to know in advance that
172 PSYCHIATRIC QUARTERLY
a given person, due to their cognitive deficits, would be able todemonstrate few if any skills after six months of treatment, theidentification of cognitive predictors of performance is seen as aclinically relevant issue. In this research, performance was meas-ured with the UCLA Comprehensive Module Tests for the BCSmodule, which assess both knowledge of the material taught andthe ability to demonstrate the skills in role plays (14). The per-formance score is the sum of scores on the post-tests given aftereach skill area.
In an initial study with 21 persons with schizophrenia (10),performance on the Sustained Attention Test significantly pre-dicted performance at the end of the BCS module. As our dataset has expanded, we are finding that performance is predictedsignificantly by pre-treatment levels of three cognitive variables:1) immediate memory span, or the number of words, from a listof 15, that could be remembered after hearing them for the firsttime on the Key Auditory Verbal Learning Test (RAVLT), r(21)= .62, p < .01; 2) IQ, calculated as a WAIS-R full scale estimatebased on performance on the Shipley Institute of Living ScaleVocabulary subtest, r(22) = .61, p < .01; and 3) the number ofcorrect responses on the Wisconsin Card Sorting Test (WCST),r(25) = .42, p < .05. In addition, there was a trend towards asignificant relationship between number of commission errors onthe simple RT task and module performance. That is, on a taskwhere you had to press a button after you heard a tone, themore times you responded when there was no signal to respond,the poorer your performance was at the end of the BCS module.This finding likely reflects an inability to maintain a mental setand appropriate engagement to the relevant task as mediatingfactors in both task and module performance. Due to charac-teristics of the distribution of commission error scores and theoverall relationship between these scores and module perform-ance, correlational methods were not used in the analysis of thisrelationship. Instead, patients were divided into two groups:those who made no commission errors (i.e., "normal" perform-ance), and those who made at least one. Patients who made atleast one commission error demonstrated skill levels at the endof the module that were approximately 36% lower than patientswho did not make commission errors, t(21) = 2.07, p < .06.
SILVERSTEIN ET AL. 173
Taken together as a group, the three significant predictors ac-counted for 40% of the variance in performance at the end ofthe module (R = .63, p < .01). These data indicate that verbalintelligence, verbal memory, and the ability to shift mental setare associated with a better ability to demonstrate the skills andinformation taught in the module. In addition, the commissionerror data suggest that a reduced ability to inhibit context-inap-propriate responses is also associated with a reduced ability toperform the skills that are taught.
Skill Acquisition
Next, we looked at learning in the BCS module, defined as thedegree of change from skill level before the module to skill levelafter it, again assessed using the UCLA Comprehensive ModuleTests. In our most recent data analysis, the combination of per-formance on RAVLT Trial 5 (amount of words recalled after hear-ing the list 5 consecutive times) and number of omission errorson the simple RT task (i.e., the number of auditory signals towhich the person should have responded but did not) accountedfor 42% of the variance in amount of learning, with the omissionerror index being the best overall predictor (16). Omission errorsare commonly interpreted as reflecting lapses in attention, witha higher rate indicating more difficulty sustaining continuous at-tention to a task. Therefore, these data suggest that the combi-nation of auditory attention span and verbal memory skills iscritical in learning skills in psychiatric rehabilitation treatment.
Summary of Skills Training Outcome Data
The data sets on cognitive predictors of module performance andskill acquisition share some similarities but are not identical. Thedata summarized above suggest that some form of attention spanappears to be required for both performance of skills and learningof new skills. It appears that the largest difference between thetwo data sets involves intelligence and inhibition of inappropriateresponses being relevant to skill performance, but verbal learningbeing predictive of degree of learning in the module. At the veryleast, these data suggest that the way in which outcome is de-fined can impact on the results that are obtained. At another
174 PSYCHIATRIC QUARTERLY

level, they suggest that the cognitive abilities subserving per-formance of social skills are not identical to those mediatinglearning of social (and presumably other) skills. This is importantbecause it points to the need to address different cognitive func-tions at different stages of the rehabilitation process.
Corrigan and McCracken (21) noted that a successful rehabili-tation program must include methods for helping patients to ac-quire new skills (e.g., skills training), methods for reinforcingperformance of these skills (e.g., a token economy); methods topromote generalization of these skills to new settings; and meth-ods to address cognitive deficits that may interfere with the firstthree processes. From within this framework, our data suggestthat attentional and memory impairments must be addressedeither prior to (via rehabilitation) or during (using compensatorystrategies) skills acquisition interventions. Following successfulskill acquisition, attention span, verbal ability, response inhibi-tion, and cognitive flexibility are cognitive abilities that must betargeted in the effort to assist patients to perform new skills tothe best of their ability.
A New Measure of Responsiveness to Skills Training
Charles Wallace, Ph.D. and colleagues at the UCLA ClinicalResearch Center for Schizophrenia and Psychiatric Rehabilita-tion (Robert Liberman, M.D., Principal Investigator) have re-cently developed a measure to rapidly assess responsiveness toskills training. The Micro-Module Learning Test (MMLT) is abrief measure of responsiveness to the three core componentsinvolved in skills training: verbal instruction, modeling, androle play. The MMLT was developed, in part, because there wasa need for a relatively brief and accurate assessment tool thatwould predict a patient's performance before being placed inskills training modules, which often last from 3 to 6 or moremonths. While successful prediction of performance in skillstraining has been achieved using traditional neuropsychologicalmeasures, an assumption driving the development of theMMLT was that it uses a basic structure and content that aresimilar to skills training procedures, and that this wouldachieve greater ecological and predictive validity than previous
SILVERSTEIN ET AL. 175
measures when used as a predictor variable. In addition, theMMLT can be used as a dependent variable, as an analogue toperformance in a full-length module. This is important for com-pleting research studies on predictors of skill acquisition since atypical module on a long-term inpatient unit can take six monthsto complete and a single skill area can take several weeks tofinish. Moreover, on a typical treatment unit, during the monthsthat it takes to complete a module, patients who began it maybe discharged, leaving the investigator without the chance to ob-tain post-test data. Also, new patients admitted to the unit mayenter the previously started group and finish it, but without pro-viding data on all skill areas. This loss of data can prolong evenfurther the time it takes to complete a study of skill acquisitionor predictors.
There are seven alternate forms of the MMLT, each using con-tent specifically drawn from the UCLA Social and IndependentLiving Skills modules (3 tests from the Basic Conversation Skillsmodule, 2 from the Recreation for Leisure module, and one eachfrom the Medication Management and Symptom modules). Psy-chometrically, the MMLT has adequate internal consistency andtest retest reliability. In a sample of 13 patients, coefficient al-phas ranged from .75 to .86 for the verbal instruction section,.77 to .89 for the modeling section, and .68 to .87 for the roleplay section. Test-retest reliabilities for 8 patients over a 3 monthor longer period were .58 for verbal instruction, .72 for modeling,and .68 for role play (22).
We investigated the relationship between performance on theMMLT and the cognitive battery described earlier. In additionto the core battery, measures of verbal fluency (FAS; 23) andinferential reasoning (using a theory of mind task; 24) were in-cluded as predictors for this study. Lastly, we determined thedegree to which MMLT performance predicted performance in afull-length module.
During test administration, the material from each section(e.g., verbal instruction, modeling, role play) is presented andthen questions are asked or role plays initiated. An incorrect re-sponse results in up to 2 trials of simple training procedures thatmimic what is done in a typical skills training procedure. On
176 PSYCHIATRIC QUARTERLY

learning trials, relevant material is re-presented with materialnot directly related to the correct response removed. This formatwas adopted from "dynamic" methods of assessing intelligence,which assume that providing information about how a person im-proves when given explicit training or hints provides a betterassessment of intellectual capabilities than static methods. Thespecific format adopted for the MMLT most closely resembles the"learning potential assessment" (25).
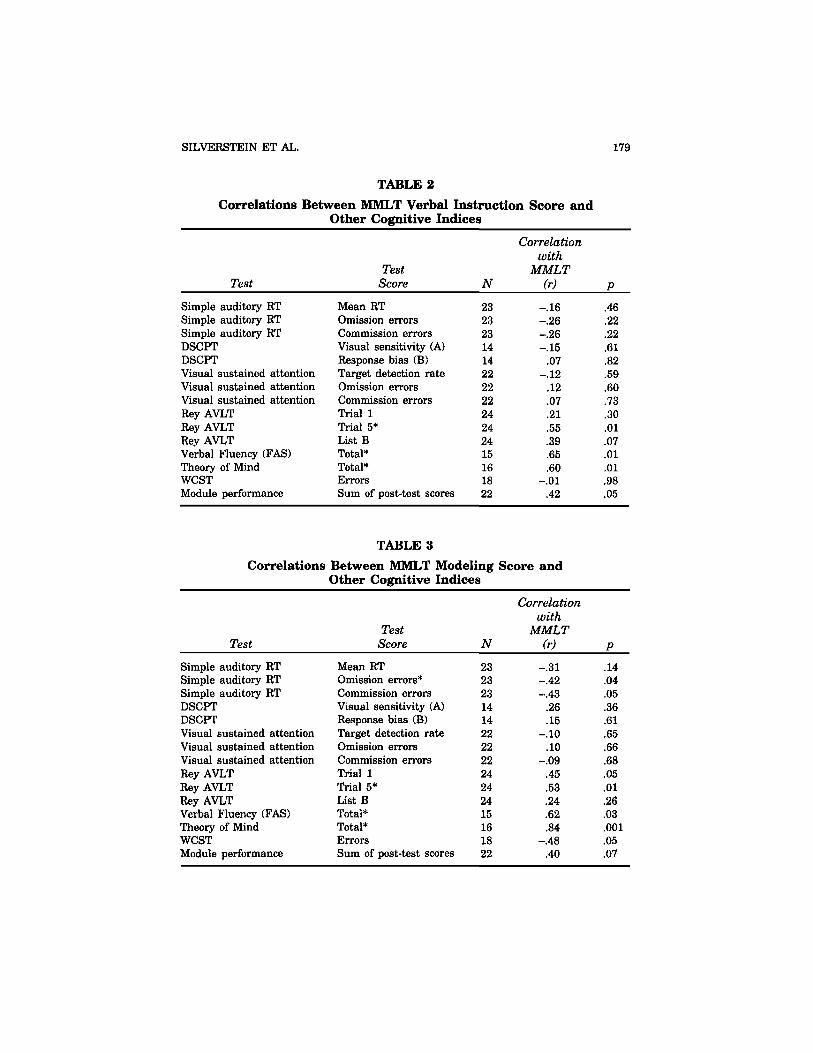
Twenty-six medicated chronic schizophrenia patients (15 M,11 F) completed the MMLT. Correlations between the MMLTand the cognitive measures and module performance are pre-sented in Tables 1-4. A consistent pattern emerged across thethree test components indicating that performance on the MMLT"interventions" was related to verbal memory, verbal fluency, andinferential reasoning (theory of mind) ability. Data from only themodeling component indicated, in addition, a trend (p = .05) to-wards a significant relationship between responsiveness to thisprocedure and conceptual flexibility, as measured by the WCST.Performance on the MMLT was not predicted significantly bymeasures of RT or visual information processing. AlthoughMMLT performance was not significantly related to performancein the Basic Conversation Skills Module, strong correlations as-sociated with statistical trends (ps = .05 or .07) were evident inall cases except one, suggesting that as our sample size increases,significant prediction may be observed.
These data confirm past findings on the role of verbal short-term memory in skill acquisition, and also indicate that verbalfluency and inferential reasoning, which are two processesknown to be impaired in schizophrenia but rarely investigatedin the context of skills training, are also related to responsive-ness to skills training procedures. These data suggest that re-sponsiveness to the components of skills training involves acombination of higher-level cognitive functions including mem-ory, fluency, and reasoning abilities. This is consistent with mod-els of skills training (26) that posit the need to address threeoverall processes in skills training: encoding/receiving (short-term memory), processing (reasoning), and sending/communicat-ing (fluency).
SILVERSTEIN ET AL. 177

178 PSYCHIATRIC QUARTERLY
COGNITIVE FACTORS ASSOCIATED WITHWARD FUNCTIONING
To explore cognitive factors associated with ward functioning, weexplored relationships between performance indices from the cog-nitive battery (including theory of mind and verbal fluency meas-ures), and observational ratings of 28 behaviors that are rateddaily by staff on the USPRP. Three month averages for each be-havior were computed for each patient and used as the dependentvariables. Because correlating all task indices and behaviorsleads to an extremely large number of correlations, and thus ahigh risk of Type I error, whereas adjusting the alpha level basedon this large a number of tests would lead to an unacceptablystringent significance criterion for an exploratory study such asthis, we used replicability as the criterion for reporting signifi-cance. Specifically, the correlational analyses were performed fortwo consecutive three month periods, and only relationships thatwere significant during both periods were considered robust. Us-ing this procedure, only on time behavior (to both groups and
TABLE 1Correlations Between MMLT Total Score and Other Cognitive Indices
Test
Simple auditory RTSimple auditory RTSimple auditory RTDSCPTDSCPTVisual sustained attentionVisual sustained attentionVisual sustained attentionRey AVLTRey AVLTRey AVLTVerbal Fluency (FAS)Theory of MindWCSTModule performance
TestScore
Mean RTOmission errorsCommission errorsVisual sensitivity (A')Response bias (B)Target detection rateOmission errorsCommission errorsTrial 1Trial 5*List BTotal*Total*ErrorsSum of post-test scores
N
232323141422222224242415161822
Correlationwith
MMLT(r)
-.24-.36-.39
.09
.26-.07
.07-.06
.46
.60
.32
.66
.77-.48
.42
P
.17
.09
.06
.76
.37
.74
.75
.76
.05
.01
.12
.01
.001
.05
.05
SILVERSTEIN ET AL. 179
TABLE 2Correlations Between MMLT Verbal Instruction Score and
Other Cognitive Indices
Test
Simple auditory RTSimple auditory RTSimple auditory RTDSCPTDSCPTVisual sustained attentionVisual sustained attentionVisual sustained attentionRey AVLTRey AVLTRey AVLTVerbal Fluency (FAS)Theory of MindWCSTModule performance
TestScore
Mean RTOmission errorsCommission errorsVisual sensitivity (A)Response bias (B)Target detection rateOmission errorsCommission errorsTrial 1Trial 5*List BTotal*Total*ErrorsSum of post-test scores
N
232323141422222224242415161822
Correlationwith
MMLT(r)
-.16-.26-.26-.15
.07-.12
.12
.07
.21
.55
.39
.65
.60-.01
.42
P
.46
.22
.22
.61
.82
.59
.60
.73
.30
.01
.07
.01
.01
.98
.05
TABLE 3Correlations Between MMLT Modeling Score and
Other Cognitive Indices
Test
Simple auditory RTSimple auditory RTSimple auditory RTDSCPTDSCPTVisual sustained attentionVisual sustained attentionVisual sustained attentionRey AVLTRey AVLTRey AVLTVerbal Fluency (FAS)Theory of MindWCSTModule performance
TestScore
Mean RTOmission errors*Commission errorsVisual sensitivity (A)Response bias (B)Target detection rateOmission errorsCommission errorsTrial 1Trial 5*List BTotal*Total*ErrorsSum of post-test scores
N
232323141422222224242415161822
Correlationwith
MMLT(r)
-.31-.42-.43
.26
.15-.10
.10-.09
.45
.53
.24
.62
.84-.48
.40
P
.14
.04
.05
.36
.61
.65
.66
.68
.05
.01
.26
.03
.001
.05
.07

180 PSYCHIATRIC QUARTERLY
meals) and keeping room clean were significantly related to cog-nitive variables. On time behavior was predicted by mean reac-tion time on both the simple RT task and the Sustained AttentionTest. This suggests that response preparedness, as measuredeither by visual or auditory tasks, is involved in getting to re-quired activities on time. Passing daily room checks was in-versely related to commission errors on the RT task, suggestingthat patients who have difficulty inhibiting context inappropriateresponses are more likely to have difficulty keeping their livingarea clean.
Instituting a level system wherein weekly privilege levels arebased on the frequency of 28 behaviors for the past seven daysalso allowed an opportunity to examine cognitive predictors ofresponsiveness to this system (comparing baseline data to dataafter system inception). Instituting this system had generallypositive effects, with all activities of daily living and on- timebehaviors showing significant improvement (15). Interestingly,however, the level of disruptive behavior increased briefly after
TABLE 4
Correlations Between MMLT Role Play Score andOther Cognitive Indices
Test
Simple auditory RTSimple auditory RTSimple auditory RTDSCFTDSCFTVisual sustained attentionVisual sustained attentionVisual sustained attentionRey AVLTRey AVLTRey AVLTVerbal Fluency (FAS)Theory of MindWCSTModule performance
TestScore
Mean RTOmission errorsCommission errorsVisual sensitivity (A)Response bias (B)Target detection rateOmission errorsCommission errorsTrial 1Trial 5*List BTotal*Total*ErrorsSum of post-test scores
N
232323141422222224242415161822
Correlationwith
MMLT(r)
-.30-.27-.34
.16
.33
.01
.007-.11
.49
.61
.33
.62
.66-.36
.22
P
.16
.20
.11
.59
.24
.98
.97
.60
.03
.01
.11
.03
.005
.14
.23
the system was instituted. Increased disruptiveness after initia-tion of the level system was predicted by fewer correct responseson the WCST (rs(17) = -.47, p < .05) and lower scores on MMLT(rs(22) = -.44, p < .05), indicating that impaired conceptual flexi-bility and learning ability are associated with a poorer initialresponse to a social learning intervention. Further analysis re-vealed that the major increases in disruptive behavior occurredin a relatively small group of patients who had been charac-terized by such behavior prior to the start of the level system.Therefore, the combination of disruptive behavior tendenciesalong with a reduced ability to alter responses based on feedbackand/or to understand a new set of contingencies appears to be aformula for poor responsiveness to a ward-based interventionsuch as the one we instituted. Subsequent individualized behav-ior contracts for these patients led to reductions in the problembehaviors, suggesting that these interventions may be necessaryfor patients with this combination of cognitive and behavioral dif-ficulties.
A final point here is that these data overlap with data reportedabove on skill performance. That is, both actual on-ward per-formance of skills after initiation of a social- learning program,and skill performance in training groups were predicted by vari-ables such as conceptual flexibility, learning ability, and abilityto inhibit context-inappropriate responses. In addition, ward be-haviors involving on-time arrival to events was related to re-sponse preparedness, as measured by RT indices.
COGNITIVE FACTORS ASSOCIATED WITHHOSPITAL DISCHARGE
In order to determine which cognitive variables were related tothe ability to be discharged from a long-term inpatient program,we administered the core cognitive battery to all patients withschizophrenia who were admitted to the USPRP upon its incep-tion in late 1993. Three years later, the data of patients who hadbeen discharged were compared to data from patients who werestill in the hospital to determine which variables predicted inpa-tient vs. outpatient status. Only one variable differentiated the
SILVERSTEIN ET AL. 181
groups, performance on the perceptual organization task. The im-plications of this are discussed below. It is important to note here,however, that none of the variables that predicted skill perform-ance or acquisition (e.g., attention span, memory, intelligence) dif-ferentiated the discharged from nondischarged groups. There wasa trend indicating that patients who, on admission, demonstratedmore perseverative errors on the WCST were less likely to bedischarged within three years; £(19) = 2.00, p < .06. These datasuggest that patients who are characterized by a reduced abilityto adapt their response organization processes to current envi-ronmental demands, and who instead perseverate on context-in-appropriate responses, tend to have behavioral difficultiesrequiring extended treatment. The perceptual organization re-sults described below support this view.
Perceptual Organization and Hospital Discharge
Perceptual organization refers to the combining of stimulus fea-tures and components into object representations during the first200 milliseconds of information processing (7). It is thought topreattentively define objects in the visual field to facilitate sub-sequent attentional allocation to relevant stimuli. Several studieshave demonstrated that schizophrenia patients are deficient intheir perceptual organization abilities (7, 27-30). Moreover, stud-ies indicate that perceptual organization dysfunction is foundmainly among schizophrenia patients with histories of poor pre-morbid social functioning (7, 31, 32), and that it is most pro-nounced among these patients when they are acutely psychotic(7) or characterized by high levels of disorganized symptoms (29).In addition, with the task used in this study, we have, in a sam-ple of 20 chronic schizophrenia patients, observed a significantassociation between abnormal perceptual organization and in-creased nailfold plexus visibility, a putative biological marker ofschizophrenia (33); rs(18) = -.50, p < .05. All of these data suggestthat abnormal perceptual organization is associated with a moresevere form of the illness, of which the need for extended inpa-tient care may be but one manifestation.
The perceptual organization task used in this study makes useof the finding that in a visual search task using brief stimulus
182 PSYCHIATRIC QUARTERLY

exposure durations, the relative positioning of the target and dis-tractor elements influences the time it takes to identify the targetmore than the overall number of elements in the display. Thus,while the time it takes to locate and identify a prespecified targettypically increases linearly as the number of distractors is in-creased (i.e., a display size effect), this effect can be overriddenby grouping the distractors together and then placing this groupapart from the target (i.e., an organizational effect). Perceptualorganization ability can thus be determined by comparing per-formance in conditions with "easier" target- distractor groupingto those where it is more difficult. In this task, perceptual organi-zation ability was operationally defined as the RT difference be-tween two critical conditions (see Figure 1). In Condition 1, therewere four distractor elements and a target letter (T or F) arrangedin a symmetrical pattern. Condition 2 had six elements and atarget letter, with the target being grouped apart from the dis-tractors. The subject's task was to press one of two buttons oneach trial as soon as they identified which target letter, whichcould appear in any of the four corners, was present. Normally,even though Condition 2 has more elements, performance is bet-ter, because the symmetry in Condition 1 precludes rapid targetidentification, whereas the target separation in Condition 2 facili-tates performance (7, 34). In contrast, if perceptual organizationis deficient, then performance should be determined more by theoverall number of elements in the display than the amount ofgrouping, leading to better performance in Condition 1. Therefore,
FIGURE 1. Examples of stimuli from perceptual organizationtask. Source: Journal of Abnormal Psychology 105:412, 1996. Copy-right © 1996 by the American Psychological Association. Reprintedwith permission.
SILVERSTEIN ET AL. 183

the direction and magnitude of the difference between Conditions1 and 2 in this task reveal the intactness of perceptual grouping.
Data from 18 of the original 28 patients admitted to the USPRPwere included in analyses involving the ability of perceptual or-ganization performance on admission to discriminate those pa-tients who would be discharged within three years from thosewhose level of functioning necessitated continued inpatient treat-ment. Ten of the original 28 patients were excluded for the fol-lowing reasons: diagnosis other than schizophrenia (n = 5);mentally retarded (n = 2); unable to complete the task (n = 2);and prior familiarity with the task through having participated inan earlier study using it at another hospital less than one yearearlier (n = 1). The remaining 18 patients were all tested withthe task as soon as possible after the opening of the USPRP, inmost cases within the first month. After three years, seven of these18 patients had been discharged and 11 remained in the program.
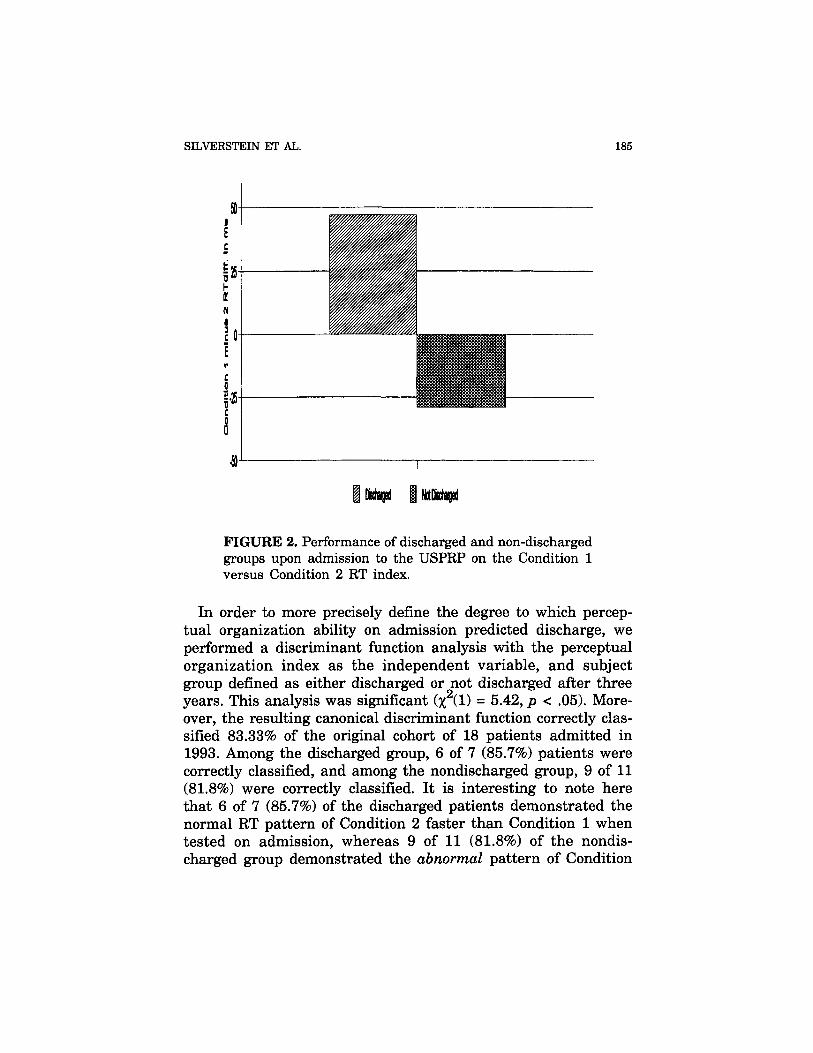
The discharged and non-discharged groups differed in theirperformance on the critical index from the perceptual organiza-tion task. The group that had been discharged during the firstthree years of the program demonstrated, when tested on admis-sion, the normal pattern of faster RTs in Condition 2 comparedto Condition 1 (2 faster than 1 by 47 ms, see Figure 2), £(6) =3.39, p < .05. As noted above, this pattern indicates a normalresponsivity to stimulus grouping, and the normal overriding ofdisplay size effects by organizational effects in this task. In con-trast, the group that was not discharged after three years dem-onstrated, when tested on admission, the abnormal pattern offaster RTs in Condition 1 compared to Condition 2 (2 slower than1 by 29 ms; see Figure 2), although the observed reversal didnot reach a level of statistical significance, £(10) = -1.32, p > .21.Despite this failure to demonstrate the strongest form of percep-tual organization impairment, the overall pattern of performancedemonstrated by the nondischarged group, and their failure toachieve significantly faster RTs in Condition 2, clearly indicatesa reduced responsivity to stimulus grouping and a tendency to-wards a reliance on serial processing. Most importantly, the dif-ference between the discharged and nondischarged groups on thedegree of the Condition 1 vs. Condition 2 difference was statis-tically significant, t(l6) = -2.59, p < .05.
184 PSYCHIATRIC QUARTERLY
SILVERSTEIN ET AL. 185
FIGURE 2. Performance of discharged and non-dischargedgroups upon admission to the USPRP on the Condition 1versus Condition 2 RT index.
In order to more precisely define the degree to which percep-tual organization ability on admission predicted discharge, weperformed a discriminant function analysis with the perceptualorganization index as the independent variable, and subjectgroup defined as either discharged or not discharged after threeyears. This analysis was significant (%2(1) = 5.42, p < .05). More-over, the resulting canonical discriminant function correctly clas-sified 83.33% of the original cohort of 18 patients admitted in1993. Among the discharged group, 6 of 7 (85.7%) patients werecorrectly classified, and among the nondischarged group, 9 of 11(81.8%) were correctly classified. It is interesting to note herethat 6 of 7 (85.7%) of the discharged patients demonstrated thenormal RT pattern of Condition 2 faster than Condition 1 whentested on admission, whereas 9 of 11 (81.8%) of the nondis-charged group demonstrated the abnormal pattern of Condition

1 faster than Condition 2. This further supports the validity ofthe RT index as an outcome predictor, and suggests that the di-rection of the theoretically derived RT difference was the criticalfactor in the discriminant function analysis.
To explore whether the two groups differed on other variablesthat may have influenced the above results, we compared themon a number of standard demographic variables. The dischargedand non-discharged groups did not differ in age (means of 38.14(SD = 10.09) versus 41.27 (SD = 8.31), £(16) = 0.72, p > .48) orage at first hospitalization (means of 20.29 (SD = 3.40) versus18.64 (SD = 2.62), £(16) = -1.16, p > .26). The length of stayduring the current admission for the non-discharged group (in-cluding time prior to admission to the USPRP), however, wasover twice as long in duration as was the length of stay for thepatients who were eventually discharged (110 months (SD =44.20) versus 52 months (SD = 35.83); £(16) = 2.89, p < .05).Interestingly, the length of stay prior to admission to the USPRPdid not differ significantly between the two groups, even thoughthe eventually discharged group had been hospitalized for abriefer period of time (64 months (SD = 42.46) versus 36.6months (SD = 34.7); £(16) = 1.43, p > .17). Overall, these datasupport the hypothesis that abnormal perceptual organization isrelated to poorer prognosis and a more chronic course.
To determine whether other cognitive factors may have ac-counted for these results, we determined whether the dischargedand non-discharged groups differed on other relevant aspects ofcognitive task performance. The two groups did not differ in theiroverall RTs to either Condition 1 (£(16) - -0.63, p > .53) or Con-dition 2 (£(16) = 0.27, p > .75) in the perceptual organizationtask. To further explore the issue of potential cognitive con-founds, we compared the groups on RT performance in both thesimple reaction time task (8) and the Sustained Attention Test(10), also completed upon admission to the USPRP. The groupsdid not differ in their overall RTs in either the simple RT (£(16)= 0.86, p > .40) or the Sustained Attention Test (£(16) = 0.13, p> .89). Moreover, on the target detection index of the SustainedAttention Test, an indicator of vigilance, the two groups did notdiffer significantly (£(16) = -1.14, p > .27). Finally, the groupsdid not differ in their performance on the Shipley Institute of
186 PSYCHIATRIC QUARTERLY
Living Scale, a measure that correlates highly with WAIS-R IQscore (13), f(16) = 0.15, p > .88. These data indicate that thedifference between the eventually discharged and non-dischargedgroups in perceptual organization performance upon admissionto the program is not a function of either IQ, attention span orRT, but is specifically related to perceptual organization ability.
Because abnormal performance on this perceptual organizationtask can be reversed by contextual manipulations, suggestingthat a failure to adopt appropriate task strategies is associatedwith abnormal performance (7), it may be that a reduced abilityto benefit from context, rather than impaired perceptual proc-esses, is the operative factor associated with the need for ex-tended treatment. Support for this hypothesis comes from thefinding reported above that patients with perseverative tenden-cies were less likely to be discharged after three years.
CONCLUSIONS
It is well known that adaptive functioning involves multiple cog-nitive processes. What is important for practitioners of psychiat-ric rehabilitation is an awareness that behaviors that are targetsof treatment may differ in their cognitive underpinnings. For ex-ample, our data indicate that learning new skills is mediated byattention and verbal memory skills. Successful performance ofskills was related to response inhibition, attention, verbal learn-ing ability, conceptual flexibility, verbal intelligence, inferentialreasoning, and verbal fluency. Carrying out routine aspects ofdaily living (e.g., keeping room clean) was related to responsepreparedness and response inhibition skills only. The latter sug-gests that carrying out overlearned, routinized aspects of dailyliving that do not involve social skills may involve primarilylower level skills as opposed to higher cognitive functions suchas verbal learning, verbal fluency, and abstract reasoning. Adap-tation to change in the environment, however, was mediated byconceptual flexibility and learning ability. Similarly, the abilityto change behavior enough to be discharged from a long-termrehabilitation program was related to conceptual flexibility andcontext processing ability.
SILVERSTEIN ET AL. 187

It is clear that cognitive factors are important in the psychi-atric rehabilitation of schizophrenia patients. Moreover, cognitiveabilities can be assessed easily and efficiently upon admission toa psychiatric rehabilitation program. Because cognitive deficitspredict outcome better than symptoms, routine testing of cogni-tive functioning should occur alongside symptom rating proce-dures as part of the ongoing comprehensive assessment ofdisability (3).
Identification of cognitive deficits has direct clinical implica-tions, such as assisting in choosing appropriate therapeuticgroups for patients, and in identifying characteristics that mayindicate the need for individualized cognitive and/or behavioralinterventions. Efforts to improve cognitive skills should focus onthe individual's cognitive deficit profile, as well as his/her treat-ment and discharge goals to choose appropriate strategies thatare tailored to individual needs. For example: 1) if a patient ispreparing to move to a setting where social skills are particularlyimportant (e.g., a group home), and attention is too impaired tocurrently benefit from social skills training, a shaping interven-tion to increase attention span (17) would be appropriate priorto entering the patient in a skills group; and 2) if a patient hassufficient attention and memory skills, but is characterized byperseverative and aggressive tendencies, he/she may benefit frominterventions to promote cognitive flexibility (35), especially if,given the data reported above, they are about to be moved to anew living environment. Awareness of those cognitive functionsthat mediate behaviors that are the target of treatment can leadto the introduction of compensatory or rehabilitative cognitive in-terventions that are most likely to improve specific aspects ofcognitive functioning. This is necessary to maximize the gainsfrom concurrent and future psychiatric rehabilitation interven-tions (16).
ACKNOWLEDGMENTS
This research was supported by a grant from the Scottish RiteBenevolent Foundation's Schizopherenia Research Program,N.M.J., U.S.A., and by contributions from the Committee to Aid
188 PSYCHIATRIC QUARTERLY
Research to End Schizophrenia (CARES). We thank the staff andpatients of the Rochester Psychiatric Center for their cooperationwith this research, and Claries Wallace, Ph.D. for his active col-laborative efforts with the Micro-module Learning Test.
REFERENCES
1. Green MF: What are the functional consequences of neurocognitive deficitsin schizophrenia. American Journal of Psychiatry 153:321-330, 1996.
2. Green MF: Schizophrenia from a neurocognitive perspective. Boston, Allyn& Bacon, 1998.
3. Silverstein SM, Maxey JT, West L: Cognitive and symptom factors relatedto outcome in a partial hospitalization program. Continuum: Developmentsin Ambulatory Health Care 1:251-261, 1994.
4. King HE: Psychomotor aspects of mental disease. Cambridge: Harvard Uni-versity Press, 1954.
5. Zahn TP, Carpenter WT: Effects of short term outcome and clinical im-provement on RT in acute schizophrenia. Journal of Psychiatric Research14:59-68, 1978.
6. Kern RS, Green MF, Satz P:. (1992). Neuropsychological predictors of skillstraining for chronic psychiatric patients. Psychiatry Research 43: 223-230,1992.
7. Silverstein SM, Knight RA, Schwarzkopf, S. B, et al: Configuration and con-text effects in perceptual organization in schizophrenia. Journal of AbnormalPsychology 105:410-420, 1996.
8. Silverstein SM: Simple auditory reaction time task. Unpublished software,University of Rochester, 1993.
9. Nuechterlein KH, Dawson ME, Ventura J, et al: Information processing ab-normalities in the early course of schizophrenia and bipolar disorder. Schizo-phrenia Research 5:195-196, 1991.
10. Silverstein SM, Light GA, Palumbo DR: The Sustained Attention Test: Ameasure of cognitive dysfunction. Computers in Human Behavior: in press.
11. Rey A: L'examen clinique en psychologic. Paris: Presses Universitaires deFrance, 1964.
12. Berg EA: A simple objective test for measuring flexibility in thinking. Jour-nal of General Psychology, 39:15-22, 1948.
13. Zachary RA: Shipley Institute of Living Scale: Revised Manual. WesternPsychological Services: Los Angeles, 1991.
14. Wallace CJ, Liberman RP, MacKain SJ, et al: Effectiveness and replicabilityof modules for teaching social and instrumental skills to the severely men-tally ill. American Journal of Psychiatry 149:654-658, 1992.
15. Silverstein SM, Bowman J, McHugh D: Strategies for hospital-wide dissemi-nation of psychiatric rehabilitation interventions. Psychiatric RehabilitationSkills 2(l):l-24.
16. Silverstein SM, Hitzel H, Schenkel LS: Identifying and addressing cognitivebarriers to rehabilitation readiness. Psychiatric Services 49:34-36, 1998.
SILVERSTEIN ET AL. 189
17. Silverstein SM, Pierce DL, Saytes M, et al: Behavioral treatment of atten-tional dysfunction in chronic, treatment-refractory schizophrenia. Psychiat-ric Quarterly 69:95-105, 1998.
18. Spitzer RL, Williams JEW, Gibbon M, et al: Structured clinical interviewfor DSM-III-R-Patient Edition (SCID-P, Version 1.0). Washington DC: APAPress, 1990.
19. First MB, Spitzer RL, Gibbon M, et al: Structured Clinical Interview forDSM-IV Axis 1 Disorders - Patient Edition (SCID-I/P, Version 2.0). NewYork: Biometrics Research Department, New York State Psychiatric Insti-tute, 1995.
20. Bowen L, Wallace CJ, Glynn SM, Nuechterlein KH, Lutzker JR, KuehnelTG: Schizophrenics' cognitive functioning and performance in interpersonalinteractions and skills training procedures. Journal of Psychiatric Research28:289-301, 1994.
21. Corrigan PW, McCracken S: Interactive Staff Training: Rehabilitation teamsthat work. New York, Plenum, 1997.
22. Wallace CJ: Psychometric properties of the Micro-module Learning Test.Unpublished data UCLA Clinical Research Center for Schizophrenia andPsychiatric Rehabilitation, 1997.
23. Benton AL, Hamsher KD: Multilingual Aphasia Examination. Iowa City:University of Iowa, 1976.
24. Corcoran R, Mercer G, Frith CD: Schizophrenia, symptomatology, and socialinference: Investigating 'theory of mind' in people with schizophrenia.Schizophrenia Research 17:5-13, 1995.
25. Budoff M: Measures for assessing learning potential. In C. S. Lidz (Ed.),Dynamic Assessment. New York: Guilford Press, 1987.
26. Wallace CJ, Boone SE: Cognitive factors in the social skills of schizophrenicpatients. In Theories of Schizophrenia and Psychosis: Nebraska Symposiumon Motivation, 1983. Edited by Spaulding WD, Cole JK. Lincoln: Universityof Nebraska Press, 1984.
27. Cox MD, Leventhal DN: A Multivariate analysis and modification of a pre-attentive perceptual dysfunction in schizophrenia. Journal of Nervous andMental Disease 166:709-718, 1978.
28. Knight RA: Specifying cognitive deficiencies in poor premorbid schizophren-ics. In Progress in Experimental Personality and Psychopathology Research,Vol. 15. Edited by Walker EF, Dworkin RH, Cornblatt, BA. Springer: NewYork.
29. Place EJS, Gilmore GC: Perceptual organization in schizophrenia. Journalof Abnormal Psychology 89: 409-418, 1980.
30. Silverstein SM, Matteson S, Knight RA: Reduced top-down influence inauditory perceptual organization in schizophrenia. Journal of Abnormal Psy-chology 105:663-667, 1996.
31. Knight RA, Silverstein SM: The role of cognitive psychology in guiding re-search on cognitive deficits in schizophrenia. In Experimental Psychopathol-ogy and the Pathogenesis of Schizophrenia. Edited by Lenzenweger M,Dworkin RH. APA Press: Washington DC, 1998.
32. Silverstein SM, Palumbo DR: Nonverbal perceptual organization output dis-ability and schizophrenia spectrum symptomatology. Psychiatry 66:66-81,1995.
33. lacono WG: Psychophysiological markers of psychopathology: A review. Ca-nadian Journal of Psychology 26:96-112, 1985.
190 PSYCHIATRIC QUARTERLY
SILVERSTEIN ET AL.
34. Silverstein SM, Raulin ML, Pristach EA, et al: Perceptual organization andschizotypy. Journal of Abnormal Psychology 101: 265-270, 1992.
35. Spaulding WD, Storms L, Goodrich V, Sullivan M: Applications of experi-mental psychopathology in psychiatric rehabilitation. Schizophrenia Bulletin12:560-577, 1986.
191
Related Documents











