CNS UPDATE 1: EMBRYONAL TUMORS Arie Perry, M.D. Director, Neuropathology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CNS UPDATE 1: EMBRYONAL TUMORS
Arie Perry, M.D. Director, Neuropathology

Distribution of Childhood Primary Brain and CNS Tumors by Histology and Age (Ages 0-14) (N = 15,398), CBTRUS Statistical Report: NPCR and SEER, 2006-2010.
Ostrom Q T et al. Neuro Oncol 2013;15:ii1-ii56
© The Centers for Disease Control and Prevention. Published by Oxford University Press on behalf of the Society for Neuro-Oncology in cooperation with the Central Brain Tumor Registry 2013.



“WHO’s Next?”
A Colloquium to Guide Next Steps in
Brain Tumor Classification and
Grading
Sponsored by the
International Society of Neuropathology
Made possible through generous support
from the STOPbraintumors
Foundation
Organizers:
David Louis
Pieter Wesseling
Arie Perry
Program Committee:
Peter Burger
David Ellison
Guido Reifenberger Andreas von Deimling
WHO’s Next meeting, Haarlem/St. Bavo Church, May 1st 2014

School of Medicine
EMBRYONAL CNS TUMORS WHO 2007 SCHEME
• Medulloblastoma
– Classic
– Desmoplastic
– Extensively Nodular
– Large cell/Anaplastic
– Medullo with myogenic differentiation
– Medullo with melanotic differentiation
• Pineoblastoma
• CNS PNET
– Neuroblastoma
– Ganglioneuroblastoma
– Ependymoblastoma
– Medulloepithelioma
• Atypical teratoid / Rhabdoid tumor

School of Medicine
MEDULLOBLASTOMA (WHO IV)
• Children/young adults
• Aggressive natural history
• CSF seeding (“icing” and drop mets)
• 5-year survival: 60-80% with therapy
• Radiation may save patient’s life, but is harmful to the developing CNS
• Favorable and unfavorable variants
• Histogenesis: EGL or SEGM of 4th ventricle

School of Medicine
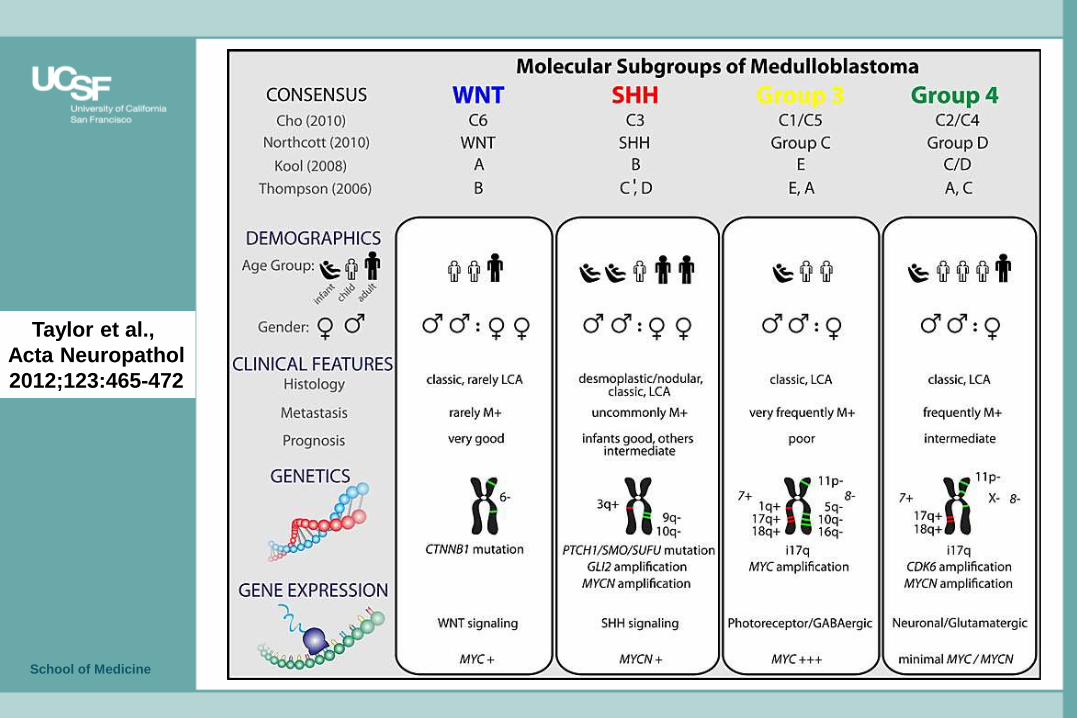
Taylor et al.,
Acta Neuropathol
2012;123:465-472


Medulloblastoma
Integrated diagnosis:
Medulloblastoma, histological subtype and molecular subgroup (e.g., Wnt, SHH, non-WNT/non-SHH*), WHO grade IV
Histological classification:
Classic, anaplastic, large cell, desmoplastic/nodular, or medulloblastoma with extensive nodularity
WHO grade:
IV
Molecular information:
MYC amp, NMYC amp, TP53 status, CTNNB1 status, SMO status, PTCH status, i17q, monosomy 6 (list illustrative and not meant to be exhaustive)

School of Medicine
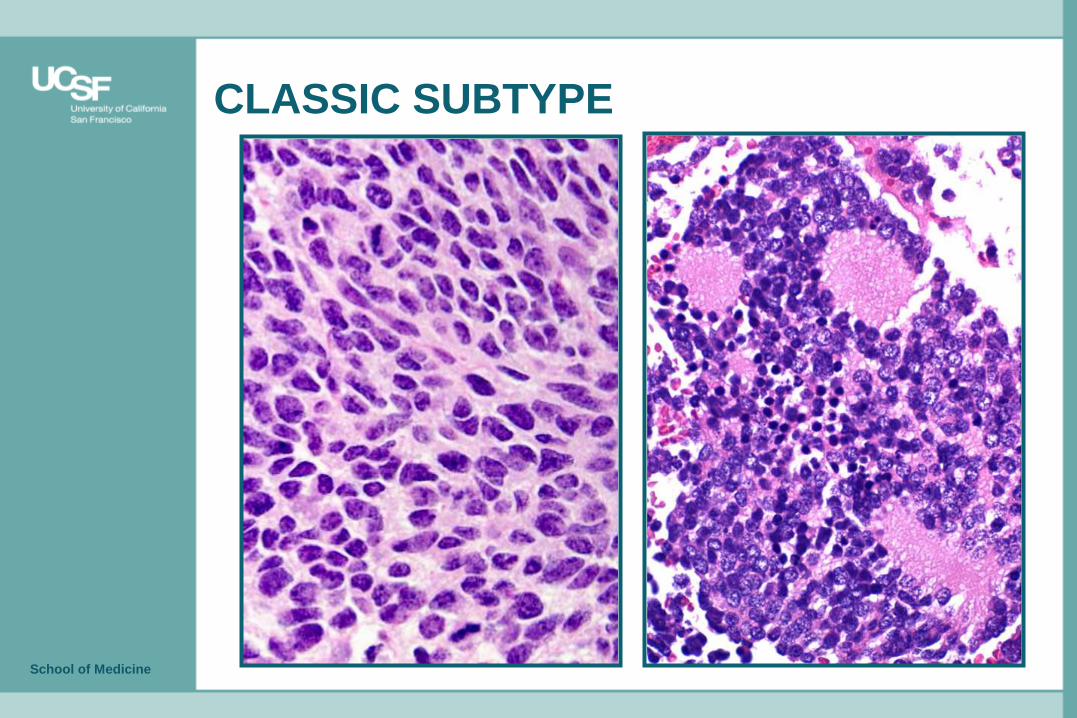
CLASSIC SUBTYPE
School of Medicine
CLASSIC SUBTYPE

WNT MOL SUBTYPE
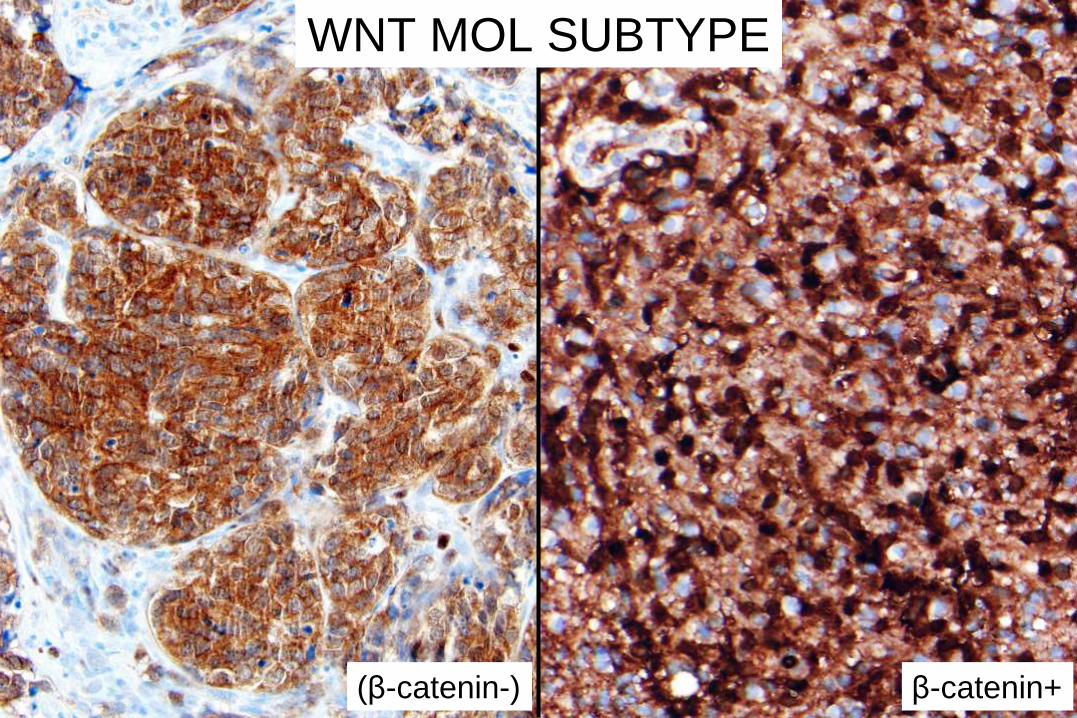
β-catenin+
WNT MOL SUBTYPE
(β-catenin-)
School of Medicine
Taylor et al.,
Acta Neuropathol
2012;123:465-472

DESMOPLASTIC SUBTYPE

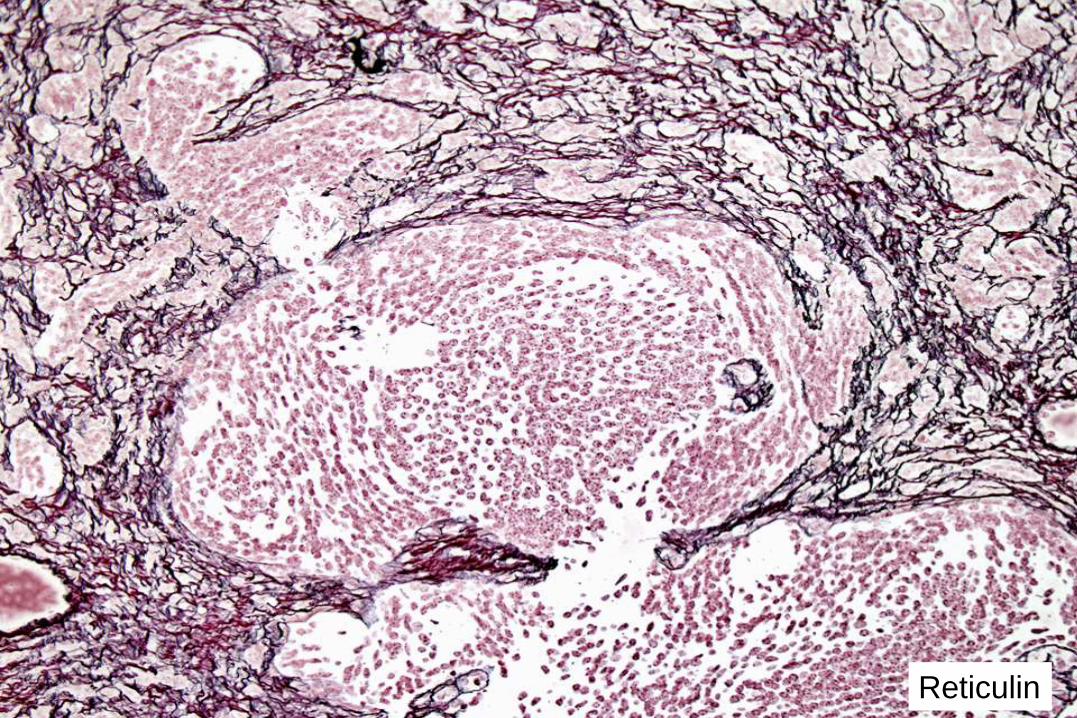
Reticulin

MIB-1 SYN
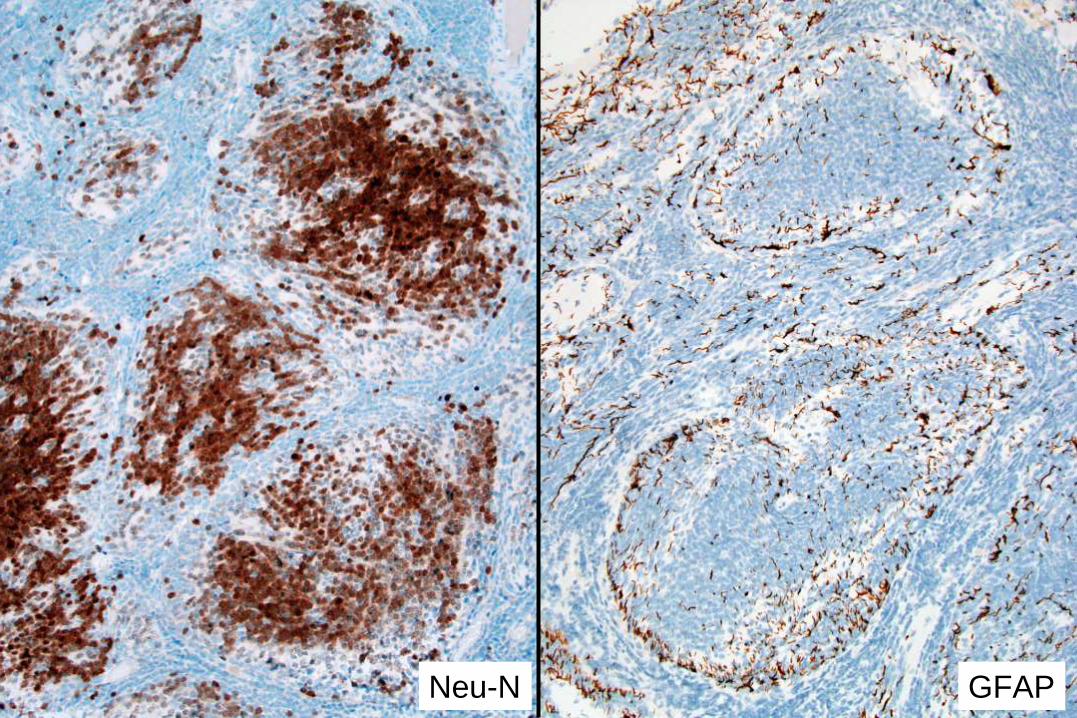
GFAP Neu-N

GAB-1
SHH MOL SUBTYPE

GAB-1
SHH MOL SUBTYPE
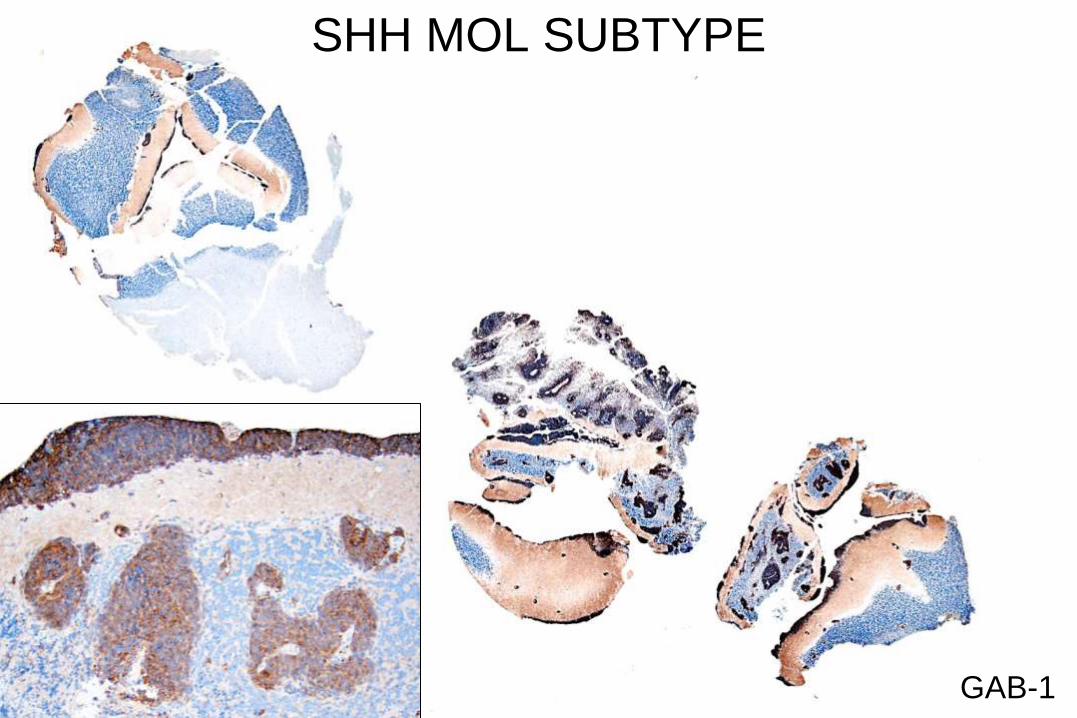
GAB-1
SHH MOL SUBTYPE
School of Medicine
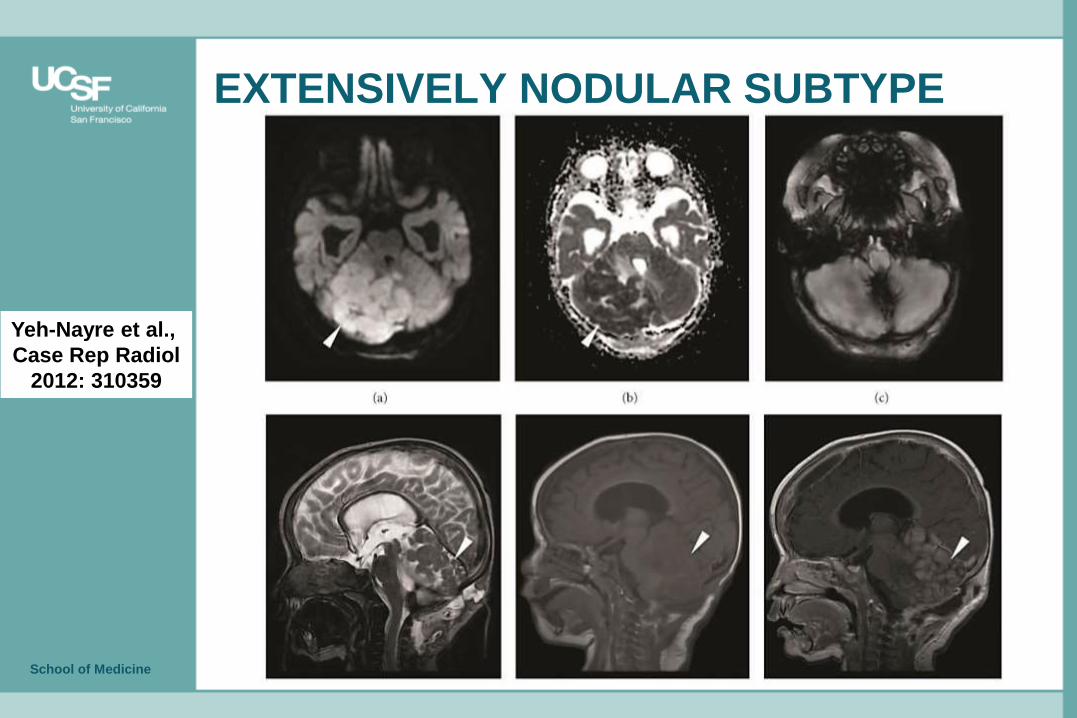
EXTENSIVELY NODULAR SUBTYPE
Yeh-Nayre et al.,
Case Rep Radiol
2012: 310359
Related Documents











