Clinical Evaluation Dermal Filler 16/2 CRM Gel/CRM Dur/GeneFill Soft Touch/ Hyacorp Lips Version 3.0 CLINICAL EVALUATION CONTENT Clinical Evaluation ............................................................................................................................ 1 Content ............................................................................................................................................. 1 1. General Details........................................................................................................................ 2 2. Description of the device and its intended application.............................................................. 2 3. Intended therapeutic and/or diagnostic indications and claims ................................................ 7 4. Context of the evaluation and choice of clinical data types ..................................................... 10 5. Summary of the clinical data and appraisal ........................................................................... 13 6. Data analysis ......................................................................................................................... 21 6.1. State-of-the-Art ............................................................................................................................................. 21 6.2. Performance ................................................................................................................................................. 25 6.3. Safety .......................................................................................................................................................... 30 6.4. Risk analysis ................................................................................................................................................. 35 7. Post-marked data .................................................................................................................. 36 8. Conclusion ............................................................................................................................ 36 9. References ............................................................................................................................. 37 10. Attachments .......................................................................................................................... 40 _____________________________________________________________________________ 1/40

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
CLINICAL EVALUATION
CONTENT
Clinical Evaluation ............................................................................................................................ 1
Content ............................................................................................................................................. 1
1. General Details ........................................................................................................................ 2
2. Description of the device and its intended application .............................................................. 2
3. Intended therapeutic and/or diagnostic indications and claims ................................................ 7
4. Context of the evaluation and choice of clinical data types ..................................................... 10
5. Summary of the clinical data and appraisal ........................................................................... 13
6. Data analysis ......................................................................................................................... 21
6.1. State-of-the-Art ............................................................................................................................................. 21
6.2. Performance ................................................................................................................................................. 25
6.3. Safety .......................................................................................................................................................... 30
6.4. Risk analysis ................................................................................................................................................. 35
7. Post-marked data .................................................................................................................. 36
8. Conclusion ............................................................................................................................ 36
9. References ............................................................................................................................. 37
10. Attachments .......................................................................................................................... 40
_____________________________________________________________________________
1/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
1. General Details
Manufacturer: BioScience GmbH
Walsmühler Straße 18
19073 Dümmer
Germany
Medical Devices: CRM Gel
CRM Dur
GeneFill Soft Touch
Hyacorp Lips
GMDN-Code: 17876
2. Description of the device and its intended application
Four products with identical composition are marketed by the manufacturer BioScience GmbH
under four different names – CRM Gel, CRM Dur, GeneFill Soft Touch, and Hyacorp Lips.
There are differences between the products under discussion regarding their indications. CRM
Gel, CRM Dur, and GeneFill Soft Touch are indicated for replacement of volume and lost
hyaluronic acid in the facial skin. Hyacorp Lips is specifically indicated for restoration of
volume and contour of the lips.
The products under discussion are clear and viscous gel and are provided in a sterile form. The
products are for single use only and supplied in a syringe with a Luer lock port. The contained
gel consists of cross-linked hyaluronic acid.
The products under discussion are absorbable skin implants with a high level of purity. The
contained hyaluronic acid is of non-animal origin. CRM Gel, CRM Dur, GeneFill Soft Touch,
and Hyacorp Lips products are sterile, apyrogenic, visco-elastic, biologically compatible (non-
immunising, non-inflammatory, non-toxic) gel implants that are insoluble in water and
produced from a hyaluronic acid gained through fermentation.
According to the Medical Device Directive 93/42/EEC, annex IX, rule 8, the products under
discussion are classified as Class III Medical Devices. The products under discussion are
already certified as medical devices and are already marketed in the European Union:
CRM Gel: since 2003
CRM Dur: since 2003
GeneFill Soft Touch: since 2009
Hyacorp Lips: since 2009
_____________________________________________________________________________
2/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
Composition
The products under discussion are composed identically.
1 mL CRM Gel contains:
Hyaluronic acid sodium salt 2.0 mg
Cross-linked Hylan gel 16.0 mg
Sodium chloride 6.9 mg
Water for injection ad 1.0 mL
1 mL CRM Dur contains:
Hyaluronic acid sodium salt 2.0 mg
Cross-linked Hylan gel 16.0 mg
Sodium chloride 6.9 mg
Water for injection ad 1.0 mL
1 mL GeneFill Soft Touch contains:
Hyaluronic acid sodium salt 2.0 mg
Cross-linked Hylan gel 16.0 mg
Sodium chloride 6.9 mg
Water for injection ad 1.0 mL
1 mL Hyacorp Lips contains:
Hyaluronic acid sodium salt 2.0 mg
Cross-linked Hylan gel 16.0 mg
Sodium chloride 6.9 mg
Water for injection ad 2.0 mL
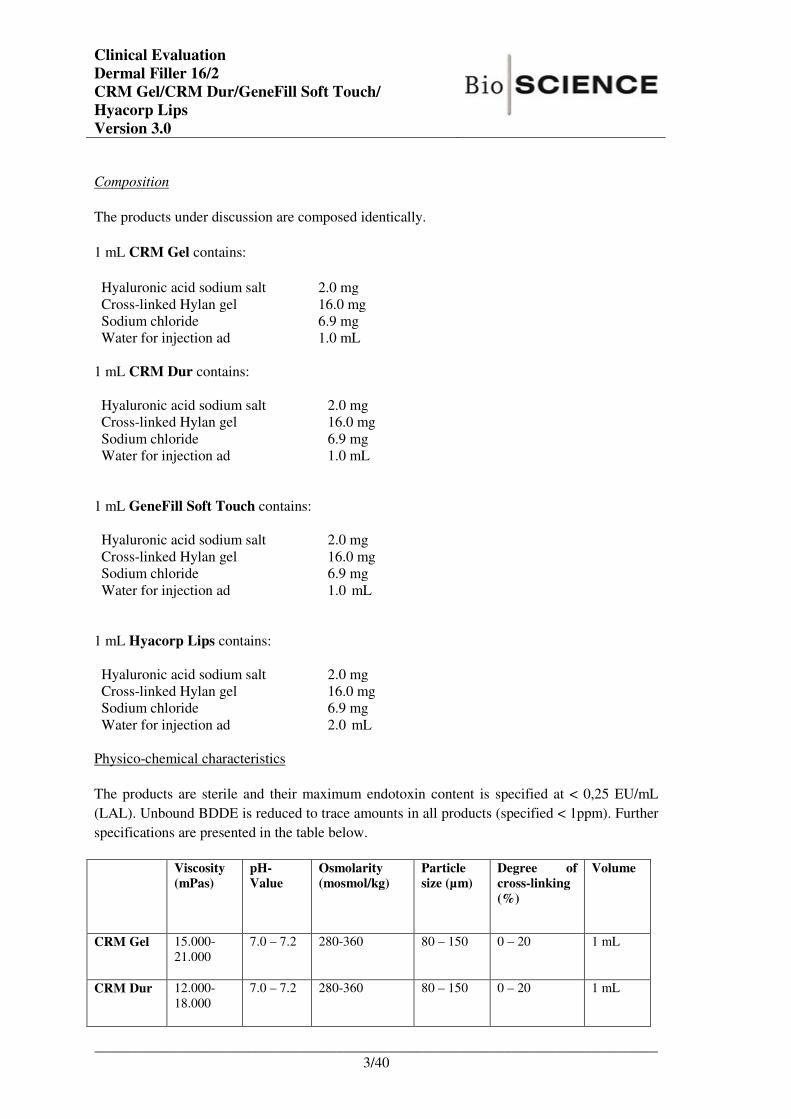
Physico-chemical characteristics
The products are sterile and their maximum endotoxin content is specified at < 0,25 EU/mL
(LAL). Unbound BDDE is reduced to trace amounts in all products (specified < 1ppm). Further
specifications are presented in the table below.
Viscosity (mPas)
pH-Value
Osmolarity (mosmol/kg)
Particle size (µm)
Degree of cross-linking
(%)
Volume
CRM Gel 15.000-
21.000
7.0 – 7.2 280-360
80 – 150 0 – 20 1 mL
CRM Dur 12.000-
18.000
7.0 – 7.2 280-360
80 – 150 0 – 20 1 mL
_____________________________________________________________________________
3/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
GeneFill
Soft Touch
15.000-
21.000
7.0 – 7.2 280-360
80 – 150 0 – 20 1 mL
Hyacorp
Lips
15.000-
21.000
7.0 – 7.2 280-360
80 – 150 0 – 20 1 mL
Hyaluronic acid (HA) is a naturally occurring glycosaminoglycan disaccharide composed of
alternately repeating units of D-glucuronic acid and N-acetyl-D-glucosamine. It is a major
component of the extracellular matrix found in many human tissues, including the skin. In
contrast to other glycosaminoglycans, it occurs free and is not linked to proteins in the dermis.
The highly charged nature of HA renders it soluble and allows it to bind water extensively,
which determines skin viscoelasticity. Hyaluronic acid is chemically, physically and
biologically identical in the tissues of all higher organisms (Kablik, Monheit et al. 2009).
Figure 2-1 Hyaluronic Acid (HA) (Kablik, Monheit et al. 2009)
HA has excellent biocompatibility and affinity for water molecules, but it is a soluble polymer
that is cleared rapidly when injected into normal skin. The two most common functional groups
that can be modified in HA are the carboxylic acid and the hydroxyl group. Cross-linking
strategies attempt to improve biomechanical properties while maintaining biocompatibility and
biological activity. The hyaluronic acid contained in the products under discussion is cross-
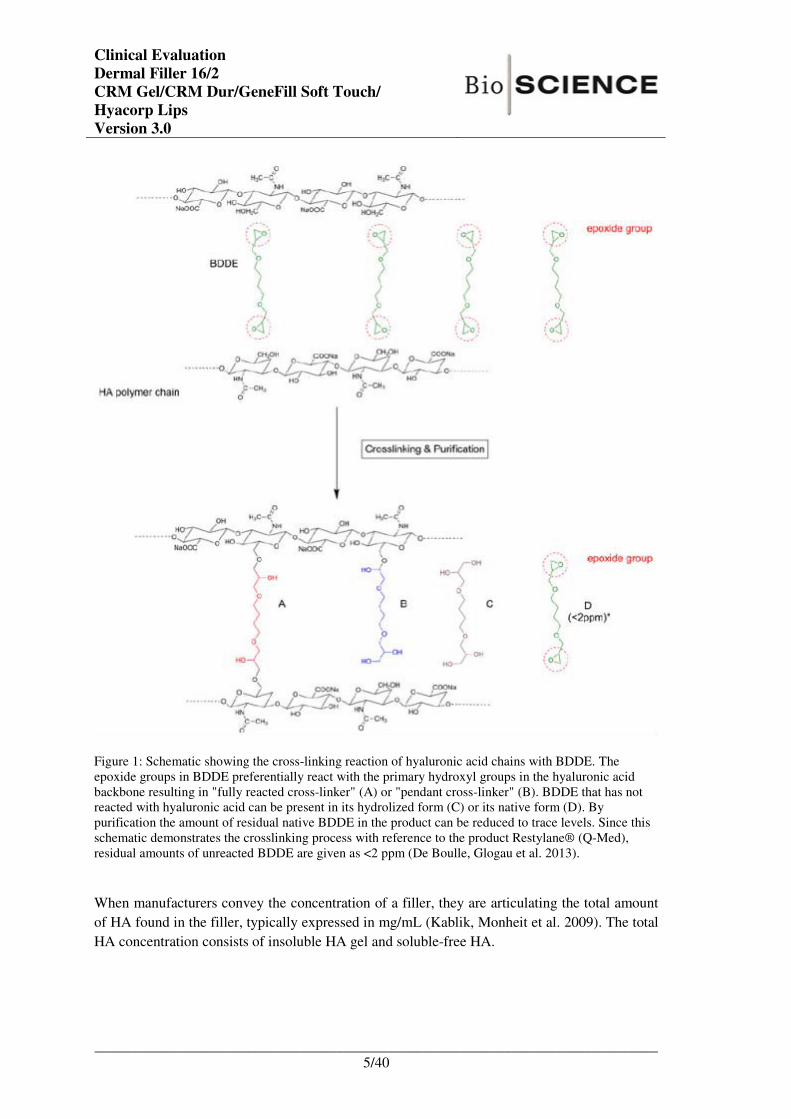
linked using 1,4 butanediol diglycidyl ether (BDDE). By BDDE-crosslinking, the hyaluronic
acid chains are chemically stabilised through permanent epoxidic cross-links. After the cross-
linking process, residual cross-linker is almost completely eliminated (specification: <1 ppm).
Under basic conditions (pH>7) the epoxide groups of BDDE react with primary alcohols in the
backbone of the hyaluronic acid forming ether bond connections and the epoxide groups are
neutralised (figure 2-2).
_____________________________________________________________________________
4/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
Figure 1: Schematic showing the cross-linking reaction of hyaluronic acid chains with BDDE. The
epoxide groups in BDDE preferentially react with the primary hydroxyl groups in the hyaluronic acid
backbone resulting in "fully reacted cross-linker" (A) or "pendant cross-linker" (B). BDDE that has not
reacted with hyaluronic acid can be present in its hydrolized form (C) or its native form (D). By
purification the amount of residual native BDDE in the product can be reduced to trace levels. Since this
schematic demonstrates the crosslinking process with reference to the product Restylane® (Q-Med),
residual amounts of unreacted BDDE are given as <2 ppm (De Boulle, Glogau et al. 2013).
When manufacturers convey the concentration of a filler, they are articulating the total amount
of HA found in the filler, typically expressed in mg/mL (Kablik, Monheit et al. 2009). The total
HA concentration consists of insoluble HA gel and soluble-free HA.
_____________________________________________________________________________
5/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
Figure 2-2: Concentration is a measure of the amount of HA in the gel. Given the same degree of
cross-linking, low concentration will result in softer gels (A), whereas higher concentration gels
result in stiffer gels (B) (Kablik, Monheit et al. 2009).
Intended use
The products under evaluation are intended to be implanted into the medium dermal tissue to
supplement the intercellular matrix and the intradermal tissue and to restore lost anatomical
structures of the skin. Its mechanism of action is based on the latest biotechnology in the
production of injectable hyaluronic acid. The product is completely degraded over time.
The products under discussion do not exert any pharmacological, metabolic, or immunological
effects.
_____________________________________________________________________________
6/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
3. Intended therapeutic and/or diagnostic indications and
claims
Application instruction and techniques
The areas to be treated must be marked before treatment begins. A local anaesthetic can be
administered in order to carry out the implant as painlessly as possible. An antibiotic can be
administered at the doctor’s discretion to prevent infection. Remove the syringe from the blister
pack, remove the cap covering the tip of the syringe and fit a suitable sterile needle to the Luer
Lock port.
The implantation technique in terms of the depth of the injection and the amount administered
can vary from case to case and according to the different degrees of augmentation required. The
doctor must select the technique appropriate to the case in hand. The products under evaluation
are injected with the aid of sterile needles. The implantation is effected in the dermis.
Correct only up to 100 % of the volume of augmentation required. Do not carry out
overcorrections. Explanations must be given to the patient before treatment is given about
indications, warnings, intolerances as well as potential side effects and the results to be
expected. The area to be treated must be carefully aseptically prepared before treatment.
Warning: The graduation on the syringe is intended as a guide for users based on the final
volume. It does not perform any measuring function; it merely indicates the amount used in
relation to the nominal volume of 2 ml. The doctor administering treatment should check
visually and by touch that a sufficient amount of the material has been injected.
Indication
CRM Dur
Replaces lost hyaluronic acid in the skin, is used for volume replacement
(filling of folds), superficial folds, periorbital lines, perioral lines.
CRM Gel
CRM Gel is indicated for the restoration of the facial volume and
contour: replaces lost hyaluronic acid in the skin, is used for volume
replacement (filling of folds), medium folds, nasolabial folds, cheek
area, lip augmentation, glabella folds.
Do not inject CRM Gel in the periorbital region (eyelid, crow’s feet,
circles under the eyes)
Genefill Soft Touch
Replaces lost hyaluronic acid in the skin, is used for volume replacement
(filling of folds), superficial folds, periorbital lines, perioral lines.
Hyacorp Lips HYAcorp Lips is intended for the restoration of volume and contour of
the lips.
_____________________________________________________________________________
7/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
The results that can be achieved are dependent on the skin type and the changes requested.
The treatment should be carried out only by doctors with knowledge and experience in the field
of aesthetic treatments.
Contraindications:
The products must not be used in patients who:
- Have a tendency to hypertrophic and keloid scarring
- Have an intolerance towards gram-positive bacteria
- Are prone to active inflammatory or infectious processes
- Are suffering from acute or chronic skin diseases
- Are undergoinhg anti-coagulant therapy
- Have a known allergy against hyaluronic acid
- Are suffering from autoimmune diseases
No clinical data is available on the administration of the product during pregnancy or lactation
or on its ad-ministration to adolescents under 18 years of age. Patients with multiple allergies
should be excluded from treatment.
The use for breast and genital augmentation is contraindicated.
Adverse effects
As with any invasive procedure, treatment with the products under evaluation may also result in
adverse effects. Treatment-related non-allergic reactions may occur such as itching, reddening,
sensitivities and swelling at the puncture site, subcutaneous bleeding or haematoma as well as
hardness or hypersensitivity reactions. In most cases these reactions occur immediately or up to
one week after the injection and usually abate spontaneously within one or two weeks. Delayed
side effects are very rare but can occur later after the injection. Known delayed side effects of
dermal fillers are bacterial infections, biofilm formation, the formation of chronic inflammatory
nodules, reactivation of herpes infections, migration of the filler material, skin necrosis, foreign
body reactions and granuloma formation. The injection technique can cause overcorrections or
bluish discolorations (Tyndall effect). It is essential that side effects are diagnosed by an
experienced doctor and appropriate treatment carried out and monitored.
In order to minimise the risk of side effects from the outset, a thorough anamnesis must be
taken by the doctor carrying out the treatment and the use of a sterile injection technique
rigorously maintained.
Warnings
The products under evaluation must not be injected into blood vessels as this could result in an
occlusion of the vessels and an embolism. The products under evaluation should not be injected
into an area in which a permanent implant has been placed. The products under evaluation
should not be used on or in the vicinity of anatomical sites affected by an active skin disease,
_____________________________________________________________________________
8/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
inflammation or associated conditions. The use of the product in areas that have already been
treated with another augmentation solution is not recommended.
The normal precautionary measures associated with intradermal injections must be observed.
The products under evaluation are intended for injection into the medium dermal tissue. A
technique and injection depth appropriate to the area treated must be chosen. To ensure the
success of the treatment it is crucial that doctors using the product have the relevant expert
knowledge and have undergone special technical training in injection techniques.
In common with all procedures of this type the implantation of The products under evaluation
are associated with the inherent risk of an infection. A thorough anatomical knowledge of the
treatment site is absolutely vital and special care must be exercised if areas are being treated in
the direct vicinity of vulnerable structures such as nerves and vessels.
The doctor carrying out the treatment should be thoroughly conversant with the patient’s
anamnesis. Suitable precautionary measures should be taken in the case of patients suffering
from pre-existing diseases and guidance and explanations should be provided. Patients taking
medication affecting blood clotting, such as aspirins or non-steroidal anti-inflammatory drugs,
will experience, as is the case with any injection, increased bruising or increased bleeding at the
injection site.
The area treated must not be exposed to excessive heat (sun, solarium, laser and IPL) or cold.
Patients should refrain from sporting activities for a few days. The injection area should not be
massaged in the days following the injection and not exposed to excessive pressure.
If the needle is clogged, replace it with a new one. Do not increase the pressure on the piston.
Used syringes needles should be treated as contaminated waste and must be disposed of in
accordance with the generally accepted standards of medical practice.
The products should be stored at room temperature (2°C to 25°C).
_____________________________________________________________________________
9/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
4. Context of the evaluation and choice of clinical data types
The performance and safety of CRM Gel, CRM Dur, GeneFill Soft Touch, and Hyacorp Lips
can be demonstrated based on equivalence to other products and established-use of hyaluronic
acid dermal fillers.
The products under discussion can be regarded as similar to the dermal filler Juvéderm Voluma
(Allergan, Santa Barbara, California USA) regarding their physic-chemical parameters:
Criterion CRM Dur/CRM Gel/GeneFill Soft
Touch/Hyacorp Lips Product Specification
Juvéderm Voluma® VB20A4001
Sterilisation Moist heat Moist heat
Osmolarity 280-360 mosmol/kg 352 mosmol/kg
Viscosity 12.000 - 18.000 mPas
15.000 – 21.000 mPas
21.580 mPas
pH value 7.0 – 7.5 7.2
Quantity of cross-linked HA 16 mg/mL 20 mg/mL
Source HA Fermentation Fermentation
Cross-linker BDDE BDDE
BDDE residuals <0.001 mg/mL (<1ppm) <0.001 mg/mL
Degree of cross-linking 0 – 20% 10.1%
Particle size 80 – 150 µm 149 µm
Slight differences in cross-linked HA content and viscosity are considered to have only minor
influence on the clinical outcome after administration. Juvéderm Voluma is a sterile,
biodegradable, non-pyrogenic, viscoelastic, clear, colorless, homogenised gel implant. It
consists of crosslinked hyaluronic acid (HA) produced by Streptococcus equi bacteria,
formulated to a concentration of 20 mg/mL. Juvéderm Voluma® is intended for deep
(subcutaneous and/or supraperiosteal) injection (see IFU of Juvéderm Voluma®). Therefore,
the following can be concluded: Technical, and biological equivalence of Juvéderm Voluma
and the products under discussion is demonstrated. Since the intended use differs – intradermal
versus subcutaneous/supraperiosteal injection – there is clinical similarity but no equivalence.
However, two important rheological properties of a soft tissue filler gel that can be quantified
are its complex viscosity and its elastic modulus. The elastic modulus of Juvéderm Voluma has
been determined at 499 Pa (data provided by the manufacturer). Sundaram et al analysed the
complex viscosity and elastic moduli of different hyaluronic acid dermal fillers and a calcium
hydroxylapatite filler (Sundaram, Voigts et al. 2010):
_____________________________________________________________________________
10/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
(Sundaram, Voigts et al. 2010)
It can be deduced from the results presented in Sundaram et al that the rheological properties of
Juvéderm Voluma are within the range of other well-established products (Juvéderm Ultra,
Juvéderm Ultra Plus, Restylane, Perlane, and Restylane SubQ).
Restylane SubQ (20 mg/mL BDDE cross-linked hyaluronic acid of non-animal origin) is
intended to be used for facial tissue augmentation. It is recommended to be used for shaping the
contours of the face, e.g. more pronounced cheeks or chin. The depth of injection may vary
from injection into the subcutaneous fatty tissue to supraperiostal administration depending on
the treatment site (see IFU of Restylane SubQ). Thus, as Juvéderm Voluma, clinical
equivalence of Restylane SubQ to the products under discussion is not given.
Restylane is a gel of hyaluronic acid generated by Streptococcus species of bacteria, chemically
crosslinked with BDDE, stabilized and suspended in phosphate buffered saline at pH=7 and
concentration of 20 mg/mL. Restylane is indicated for lip augmentation and for mid-to-deep
dermal implantation for the correction of moderate to severe facial wrinkles and folds, such as
nasolabial folds (see IFU Restylane). The indications of Restylane are equivalent to CRM Gel,
_____________________________________________________________________________
11/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
CRM Dur, and GeneFill Soft Touch, and partly (lip augmentation) to Hyacorp Lips. Thus,
Restylane is considered to be an equivalent product to the products under discussion.
Juvéderm Ultra and Juvéderm Ultra Plus injectable gels are sterile, biodegradable,
nonpyrogenic, viscoelastic, clear, colorless, homogenised gel implants. Juvéderm Ultra (Plus)
injectable gel consists of crosslinked hyaluronic acid produced by Streptococcus equi bacteria,
formulated to a concentration of 24 mg/mL and suspended in a physiologic buffer. Juvéderm
Ultra (Plus) injectable gel is indicated for injection into the mid to deep dermis for correction of
moderate to severe facial wrinkles and folds (such as nasolabial folds) (see IFU Juvéderm
Ultra). Although the HA concentration is higher in Juvéderm Ultra and Juvéderm Ultra Plus
compared with CRM Gel, CRM Dur, and GeneFill Soft Touch, it is regarded as essentially
similar and is therefore taken into consideration as well.
Perlane is a sterile gel of hyaluronic acid generated by Streptococcus species of bacteria,
chemically cross-linked with BDDE, stabilised, and suspended in phosphate buffered saline at
pH 7 and a concentration of 20 mg/mL. This product significantly differs with regard to its
particle size, since is contains the biggest particle size of the presented proucts (the largest
fraction of gel particle size is between 940 and 1090 microns). The particle size is markedly
larger than in the products under discussion, and it is therefore excluded from the evaluation.
Moreover one product is available (Juvéderm Volbella) that is indicated for the treatment of any
fine lines and medium-sized skin depressions due to conditions such as premature aging as well
as for enhancement and pouting of the lips via superficial or middermis injection or lips mucosa
injection. Juvéderm Volbella contains 15 mg/mL BDDE-crosslinked hyaluronic acid (according
to its IFU). Regarding lip augmentation, Juvéderm Volbella is considered equivalent to Hyacorp
Lips.
According to MEDDEV 2.7/1 rev3 evaluation of performance and safety of the products under
discussion based on published data regarding Restylane, Juvéderm Ultra, Juvéderm Ultra Plus,
and Juvéderm Volbella is feasible. Details on the equivalence analysis are provided in
attachment 2.
Therefore, a thorough literature search in established databases is performed to demonstrate the
performance and safety of CRM Gel, CRM Dur, GeneFill Soft Touch, and Hyacorp Lips by
taking products that are regarded as equivalent and the state-of-the-art of dermal fillers into
consideration.
_____________________________________________________________________________
12/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
5. Summary of the clinical data and appraisal
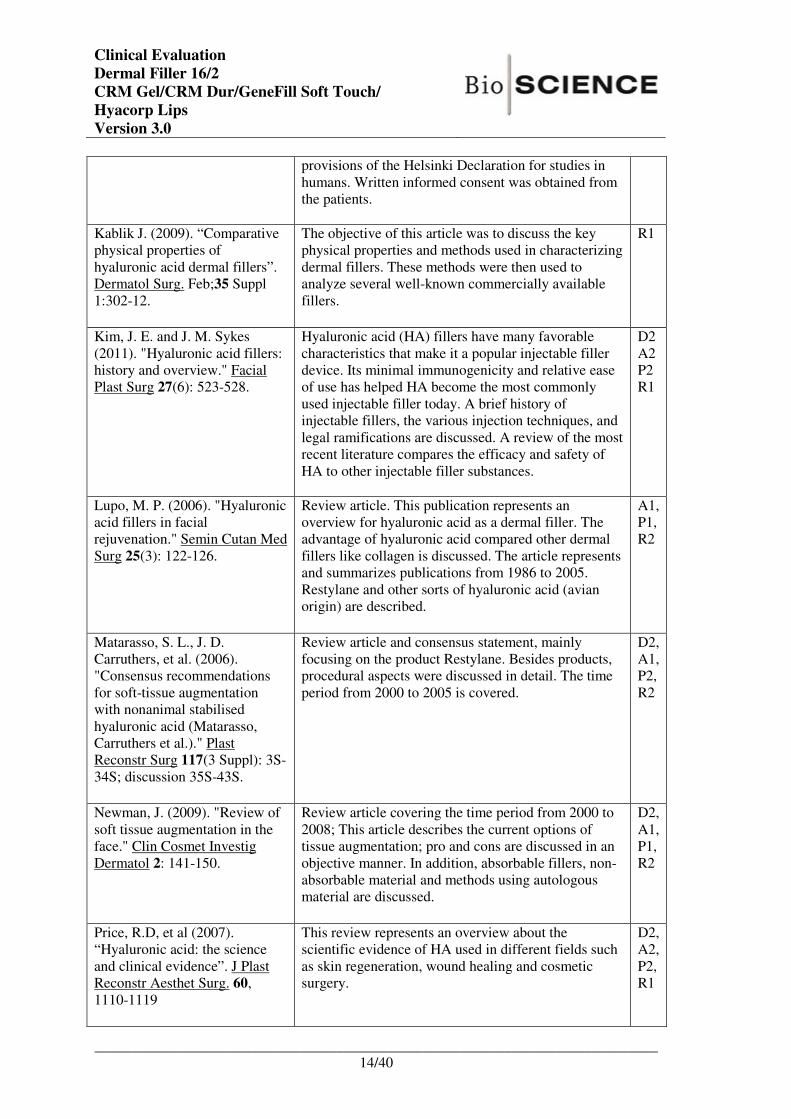
Following publications are regarded to contain sufficient information for a rational and
objective assessment. All articles are relevant for the products under evaluation. The quality of
the data is considered satisfactorily for articles taken into consideration. Protocol of the
literature survey, corresponding results and appraisal criteria are outlined in attachment 1.
The publications are categorised into the following sections: description of state-of-the-art,
demonstration of performance and demonstration of safety.
For description of the current state-of-the-art mainly review articles are assessed. The
performance of Restylane, Juvéderm Ultra, Juvéderm Ultra Plus, and Juvéderm Volbella is
mostly gained from prospective trials providing sufficient information for a detailed assessment.
Although representing a low level of clinical evidence, case reports were evaluated to
investigate rare complications for the use of hyaluronic acid as dermal filler.
The final result of the appraisal of the literature is discussed below:
State-of-the-Art
Baumann, L. S., A. T. Shamban,
et al. (2007). "Comparison of
smooth-gel hyaluronic acid
dermal fillers with cross-linked
bovine collagen: a multicentre,
double-masked, randomised,
within-subject study." Dermatol
Surg 33 Suppl 2: S128-135.
A total of 439 subjects with moderate or severe
nasolabial folds received one of three types of smooth-
gel HA dermal fillers (in one NLF) and cross-linked
bovine collagen (in the other NLF) and were evaluated
for 24 weeks. The study was approved by the relevant
institutional review boards, all subjects signed
informed consent, and the study protocol conformed to
the guidelines of the 1975 Declaration of Helsinki.
D2,
A1,
P1,
R1
Gold, M. (2009). "The science
and art of hyaluronic acid
dermal filler use in esthetic
applications." J Cosmet
Dermatol 8(4): 301-307.
This article provides an overview of the HA fillers,
focusing on interweaving of artistic concepts with
scientific principles of dermal filling.
A1,
P2,
R1
Hoffmann, K. (2009).
"Volumizing effects of a
smooth, highly cohesive,
viscous 20-mg/mL hyaluronic
acid volumizing filler:
prospective European study."
BMC Dermatol 9: 9.
This was a prospective, open-label, nonrandomised
study in which a 20-mg/mL smooth, highly cohesive,
viscous HA volumising filler (Juvéderm™
VOLUMA™, Allergan, Pringy, France) was evaluated
within its indicated use of restoring facial volume. The
study was funded by Allergan, Inc. This Europe-wide
evaluation was conducted under the guidelines of the
World Association of Opinion and Marketing
Research (ESOMAR) to evaluate current usage of the
20mg/mL smooth, cohesive HA volumising filler in
European countries in which the product is CE-
marked or licensed and available. Evaluations took
place within standard practice procedures without the
inclusion of any additional monitoring or diagnostic
procedures. The conduct of the trial complied with the
D2
A1
P1
R2
_____________________________________________________________________________
13/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
provisions of the Helsinki Declaration for studies in
humans. Written informed consent was obtained from
the patients.
Kablik J. (2009). “Comparative
physical properties of
hyaluronic acid dermal fillers”.
Dermatol Surg. Feb;35 Suppl
1:302-12.
The objective of this article was to discuss the key
physical properties and methods used in characterizing
dermal fillers. These methods were then used to
analyze several well-known commercially available
fillers.
R1
Kim, J. E. and J. M. Sykes
(2011). "Hyaluronic acid fillers:
history and overview." Facial
Plast Surg 27(6): 523-528.
Hyaluronic acid (HA) fillers have many favorable
characteristics that make it a popular injectable filler
device. Its minimal immunogenicity and relative ease
of use has helped HA become the most commonly
used injectable filler today. A brief history of
injectable fillers, the various injection techniques, and
legal ramifications are discussed. A review of the most
recent literature compares the efficacy and safety of
HA to other injectable filler substances.
D2
A2
P2
R1
Lupo, M. P. (2006). "Hyaluronic
acid fillers in facial
rejuvenation." Semin Cutan Med
Surg 25(3): 122-126.
Review article. This publication represents an
overview for hyaluronic acid as a dermal filler. The
advantage of hyaluronic acid compared other dermal
fillers like collagen is discussed. The article represents
and summarizes publications from 1986 to 2005.
Restylane and other sorts of hyaluronic acid (avian
origin) are described.
A1,
P1,
R2
Matarasso, S. L., J. D.
Carruthers, et al. (2006).
"Consensus recommendations
for soft-tissue augmentation
with nonanimal stabilised
hyaluronic acid (Matarasso,
Carruthers et al.)." Plast
Reconstr Surg 117(3 Suppl): 3S-
34S; discussion 35S-43S.
Review article and consensus statement, mainly
focusing on the product Restylane. Besides products,
procedural aspects were discussed in detail. The time
period from 2000 to 2005 is covered.
D2,
A1,
P2,
R2
Newman, J. (2009). "Review of
soft tissue augmentation in the
face." Clin Cosmet Investig
Dermatol 2: 141-150.
Review article covering the time period from 2000 to
2008; This article describes the current options of
tissue augmentation; pro and cons are discussed in an
objective manner. In addition, absorbable fillers, non-
absorbable material and methods using autologous
material are discussed.
D2,
A1,
P1,
R2
Price, R.D, et al (2007).
“Hyaluronic acid: the science
and clinical evidence”. J Plast
Reconstr Aesthet Surg. 60,
1110-1119
This review represents an overview about the
scientific evidence of HA used in different fields such
as skin regeneration, wound healing and cosmetic
surgery.
D2,
A2,
P2,
R1
_____________________________________________________________________________
14/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
Rohrich, R. J., A. Ghavami, et
al. (2007). "The role of
hyaluronic acid fillers
(Restylane) in facial cosmetic
surgery: review and technical
considerations." Plast Reconstr
Surg 120(6 Suppl): 41S-54S.
Review article. The product Restylane is described in
detail; procedural aspects are discussed as well. Main
focus of this article is the facial rejuvenation. The
performance of Restylane is shown. Possible
complications and there occurrence are discussed.
A1,
P2,
R1
Smith, K. C. (2008). "Reversible
vs. nonreversible fillers in facial
aesthetics: concerns and
considerations." Dermatol
Online J 14(8): 3.
Review article dealing with hyaluronic acid as dermal
filler in general. History, development and alternatives
in tissue augmentation are presented. The major and
unique advantage of HA fillers, the reversion by
hyaluronidase is outlined.
A2,
P1,
R2
Tezel, A. and G. H. Fredrickson
(2008). "The science of
hyaluronic acid dermal fillers." J
Cosmet Laser Ther 10(1): 35-
42.
The use of injectable materials for soft-tissue
augmentation has been increasing, reflecting the
introduction of new hyaluronic acid based dermal
fillers. Hyaluronic acid dermal fillers vary widely in
their physical and chemical characteristics. This article
explains the basic science of hyaluronic acid and
describes how the physical properties of hyaluronic
dermal fillers may influence clinical outcomes.
D2
A1
P1
R1
Performance
Baumann, L. S., A. T. Shamban,
et al. (2007). "Comparison of
smooth-gel hyaluronic acid
dermal fillers with cross-linked
bovine collagen: a multicentre,
double-masked, randomised,
within-subject study." Dermatol
Surg 33 Suppl 2: S128-135.
The objective of this study was to compare the
effectiveness and safety of smooth-gel HA dermal
fillers with bovine collagen for nasolabial fold
(NLF) correction. Therefore, a total of 439 subjects
with moderate or severe NLFs received one of
three types of smooth-gel HA dermal filler (in one
NLF) and cross-linked bovine collagen (in the
other NLF) and were evaluated for 24 weeks. All
three HA dermal fillers achieved considerably
longer-lasting clinical correction than bovine
collagen; 81 % to 90 % of HA dermal filler-treated
NLFs maintained a clinically significant
improvement from baseline for 6 months. Up to
88 % of subjects preferred the HA dermal fillers
over bovine collagen. All fillers were similarly well
tolerated. In summary, the smooth-gel HA dermal
fillers offer longer-lasting correction than bovine
collagen-which may lessen the frequency that
repeat treatments are needed. Also, they were
preferred by the vast majority of subjects-which
should promote patient satisfaction.
D2,
A1,
P1,
R1
Bogdan Allemann, I. and L.
Baumann (2008). "Hyaluronic
Review article summarising the results of two large
controlled trials performed by Baumann et al
D2,
A1,
_____________________________________________________________________________
15/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
acid gel (Juvederm) preparations
in the treatment of facial
wrinkles and folds." Clin Interv
Aging 3(4): 629-634.
(2007) and Pinsky et al (2007). In summary, the
performance and safety of Juvederm compared to
Zyplast was investigated on 731 subjects.
P1,
R2
Eccleston, D. and D. K. Murphy
(2012). "Juvederm((R)) Volbella
in the perioral area: a 12-month
prospective, multicenter, open-
label study." Clin Cosmet
Investig Dermatol 5: 167-172.
The objective of this prospective, multicenter,
open-label, post market study was to demonstrate
the safety and effectiveness of Juvéderm Volbella
injectable gel for lip enhancement. Ethics
Committee approval was obtained from Sheffield
Research Ethics Committee (Leeds, UK), and the
study was conducted at four European sites (three
in the UK and one in Northern Ireland). The study
was registered at http://www.clinicaltrials.gov
(NCT 01176773), and all subjects provided written
informed consent.
D2
A1
P1
R2
Glogau, R. G., D. Bank, et al.
(2012). "A randomised,
evaluator-blinded, controlled
study of the effectiveness and
safety of small gel particle
hyaluronic acid for lip
augmentation." Dermatol Surg
38(7 Pt 2): 1180-1192.
Eligible patients were adult men and women no
older than 65 seeking lip augmentations at 12
investigational centres A central institutional
review board (Quorum Review IRB, Seattle, WA)
approved the study protocol and documents.
Patients provided written informed consent before
being admitted to the study. The study was
conducted in accordance with the Declaration of
Helsinki and Good Clinical Practice.
D2
A1
P1
R1
Lupo, M. P., S. R. Smith, et al.
(2008). "Effectiveness of
Juvederm Ultra Plus dermal filler
in the treatment of severe
nasolabial folds." Plast Reconstr
Surg 121(1): 289-297.
A multicentre, double-blind, randomised, within-
subject, controlled study was conducted as part of a
submission for approval by the U.S. Food and Drug
Administration. This study compared three
different formulations of Juvederm against bovine
collagen (Zyplast; Allergan). One-third of subjects
were randomly assigned to receive treatment with
Juvederm Ultra Plus, containing 24 mg/ml of cross-
linked hyaluronic acid, in one nasolabial fold and
Zyplast in the other. Results presented here are
limited to those subjects who received Juvederm
Ultra Plus and had severe folds at baseline.
Because of the differences in appearance between
the two products, each study site had two
investigators: a treating investigator who was not
blinded and an evaluating investigator who was. To
maintain this blinding, the evaluating investigator
was not present during treatment every 4 weeks for
up to 24 weeks after the last treatment, subjects
were followed for assessment of nasolabial fold
severity. Follow-up visits for effectiveness
assessments after repeated treatment occurred at 4,
12, and 24 weeks after repeated treatment, and an
amendment to the extended study protocol allowed
even further evaluations at 36 and 48 weeks after
D2
A1
P1
R1
_____________________________________________________________________________
16/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
repeated treatment. The protocols and amendments
were approved by the applicable institutional
review boards, and subjects provided written
informed consent for each study in which they
participated.
Matarasso, S. L., J. D.
Carruthers, et al. (2006).
"Consensus recommendations for
soft-tissue augmentation with
nonanimal stabilised hyaluronic
acid." Plast Reconstr Surg 117(3
Suppl): 3S-34S; discussion 35S-
43S.
Review article and consensus statement, mainly
focusing on the product Restylane. Besides
products, procedural aspects were discussed in
detail. The time period from 2000 to 2005 is
covered.
D2,
A1,
P2,
R2
Morris, C. L., S. S. Stinnett, et al.
(2008). "Patient-preferred sites of
restylane injection in periocular
and facial soft-tissue
augmentation." Ophthal Plast
Reconstr Surg 24(2): 117-121.
The authors respectively reviewed the records 145
patients who received subcutaneous facial
injections of Restylane. Location, amount,
supplemental anaesthetic, injection frequency,
follow-up time, patients’ satisfaction, revision rate,
and adverse reactions were noted and analysed.
D2
A1
P1
R2
Narins, R. S., F. Brandt, et al.
(2003). "A randomised, double-
blind, multicentre comparison of
the efficacy and tolerability of
Restylane versus Zyplast for the
correction of nasolabial folds."
Dermatol Surg 29(6): 588-595.
This randomised patient- and evaluator-blinded
study was conducted at six centres in the United
States, and subjects seeking soft tissue
augmentation treatment for correction of bilateral
nasolabial folds were recruited. Outcomes were
evaluated by blinded observer at 2, 4, 6 month after
baseline. The study was performed in accordance to
the Declaration of Helsinki, the ICH guidelines for
Good Clinical Practice.
D2
A1
P1
R1
Philipp-Dormston, W. G., S.
Hilton and M. Nathan (2014). "A
prospective, open-label,
multicenter, observational,
postmarket study of the use of a
15 mg/mL hyaluronic acid
dermal filler in the lips." J
Cosmet Dermatol 13(2): 125-
134.
This one-month, prospective, open-label,
multicenter, observational postmarket study
(clinicaltrials.gov identifier: NCT01629134) was
conducted in two German sites. Eligible subjects
were aged 18 years and older, expressed a desire
and willingness for correction of asymmetry or
enhancement of their lips and could comply with
the study requirements. Each subject signed an
informed consent form and underwent treatment
with the product.
D2
A1
P1
R2
Pinsky, M. A., J. A. Thomas, et
al. (2008). "Juvederm injectable
gel: a multicentre, double-blind,
randomised study of safety and
effectiveness." Aesthet Surg J
28(1): 17-23.
In the multicentre study approved by the Food and
Drug Administration, subjects were randomised to
treatment with Juvéderm Ultra or Ultra Plus in one
nasolabial fold (NLF) and Zyplast collagen in the
other. After optimal correction was achieved
(treatment plus up to 2 touch-ups at 2-week
intervals), effectiveness was assessed on a 5-point
scale through the 6-month study period. An
D2
A1
P1
R1
_____________________________________________________________________________
17/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
additional poststudy visit provided long-term
effectiveness data. Safety was evaluated through
subjects’ daily diaries for 14 days after treatment.
Schweiger, E. S., C. C. Riddle, et
al. (2008). "Successful treatment
with injected hyaluronic acid in a
patient with lip asymmetry after
surgical correction of cleft lip."
Dermatol Surg 34(5): 717-719.
Surgical repair of cleft lip, while correcting
deformity and dysfunction, may leave residual
cosmetic imperfections. The resultant asymmetry
and low volume of the upper lip can be addressed
surgically and via less invasive methods. The
authors present the first reported use of injectable
hyaluronic acid to correct the characteristic lip
asymmetry and poor volume after surgical repair of
a cleft lip.
D2
A1
P2
R2
Smith, S. R., D. Jones, et al.
(2010). "Duration of wrinkle
correction following repeat
treatment with Juvederm
hyaluronic acid fillers." Arch
Dermatol Res 302(10): 757-762.
Upon completion of the pivotal IDE clinical trial
for Juvederm 30, Ultra, and Ultra Plus, five of the
original 11 study sites were selected to participate
in an extended follow- up evaluation. Sites were
selected based on their continued abilities to
participate in the follow-up protocol, their track
record of visit schedule compliance, and the
planned sample size of 150 subjects. No
consideration was given to duration of filler
correction in the selection of sites. Subjects who
were eligible and agreed to participate in the
follow-up study signed an informed consent and
were followed from 4 through 48 weeks after their
repeat treatments. Routine follow-up visits for
effectiveness occurred at 4, 12, and 24 weeks, and
an amendment to the protocol added visits at 36
and 48 weeks after repeat treatment. Safety and
effectiveness were evaluated at each office visit.
D2,
A1,
P1,
R2
Solish, N. and A. Swift (2011).
"An open-label, pilot study to
assess the effectiveness and
safety of hyaluronic acid gel in
the restoration of soft tissue
fullness of the lips." J Drugs
Dermatol 10(2): 145-149.
Investigators treated 21 adults. The primary
efficacy endpoint was an increase in lip fullness at
eight weeks post-treatment. Adverse events were
reported using patient diaries. This study was
approved by the Institutional Review Board
performed in accordance to the Declaration of
Helsinki, and conducted in compliance to good
clinical practice. All patients gave informed
consent to participate.
D2
A1
P1
R2
Wu, Y., et al. (2016). "Clinical
comparison between two
hyaluronic acid-derived fillers in
the treatment of nasolabial folds
in Chinese subjects: BioHyalux
versus Restylane." Arch
Dermatol Res.
This multicenter, double-blinded, randomised,
controlled, non-inferiority study was conducted to
compare the efficacy, tolerability, and durability of
the cosmetic effect of BioHyalux versus Restylane
in correcting nasolabial folds (NLF). Eighty-eight
subjects aged between 18 and 65 years with
moderate or severe NLF (Wrinkle Severity Rating
Scale (WSRS) score of 3 or 4, as evaluated by the
D2
A1
P1
R1
_____________________________________________________________________________
18/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
investigators) were recruited in this study. The
study was approved by a central institutional
review board and conducted at two Chinese
hospitals, in full accordance with the Good Clinical
Practice regulations and guidelines. All subjects
provided a written informed consent.
Safety
Andre, P., N. J. Lowe, et al.
(2005). "Adverse reactions to
dermal fillers: a review of
European experiences." J Cosmet
Laser Ther 7(3-4): 171-176.
This review article summarised publications and
case reports. It described the clinical aspects of
adverse reactions following injections of dermal
filler (absorbable, non biodegradable and
permanent) And provides valid information on
safety of dermal fillers
D2
A2
P1
R1
Artzi, O., et al. (2016). "Resistant
and Recurrent Late Reaction to
Hyaluronic Acid-Based Gel."
Dermatol Surg 42(1): 31-37.
Medical records of 400 patients (360 women and
40 men; average age = 49.6 years) were examined
in this retrospective study. Juvederm Volbellafiller
was injected only into the tear trough area or lips.
Other HA-based products were used in other areas
of the face. Four centers in Israel participated in the
study. Data were collected from patient charts and
through phone call interviews.
D2
A1
P1
R2
Brandt, F., B. Bassichis, et al.
(2011). "Safety and effectiveness
of small and large gel-particle
hyaluronic acid in the correction
of perioral wrinkles." J Drugs
Dermatol 10(9): 982-987.
This open-label, 4-week study at two US centres
evaluated patients who intended to undergo
intradermal injection for correction of perioral
wrinkles and folds. At screening, a 5-grade Wrinkle
Severity Rating Scale (WSRS) was used to
evaluate the baseline appearance of bilateral NLFs,
and a 6-grade Wrinkle Severity (WS) scale was
used to evaluate the appearance of bilateral oral
commissures, marionette lines and upper perioral
rhytides. To qualify, each patient must have had
moderate-to-severe wrinkles at one pair of
marionette lines and upper perioral rhytides. Each
wrinkle was treated to optimal correction with
either SGP-HA or LGP-HA at the discretion of the
treating investigator. All reported local and
systemic adverse events (AEs) were recorded. At
two weeks after treatment or touch-up, the treating
investigator and the patient assessed appearance
using the Global Aesthetic Improvement Scale
(GAIS).
D2
A1
P1
R2
Beasley, K.L. (2009).
“Hyaluronic Acid Fillers: A
comprehensive Review”. Facial
Plast Surg. 25:86-94.
Since 85 % of all dermal filler procedures occurred
with a hyaluronic acid derivate this review
summarised the composition, specific differences
and pivotal clinical studies of all the hyaluronic
acid fillers currently available in the US.
D2,
A1,
P2,
R1
_____________________________________________________________________________
19/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
Eccleston, D. and D. K. Murphy
(2012). "Juvederm((R)) Volbella
in the perioral area: a 12-month
prospective, multicenter, open-
label study." Clin Cosmet
Investig Dermatol 5: 167-172.
The objective of this prospective, multicenter,
open-label, post market study was to demonstrate
the safety and effectiveness of Juvéderm Volbella
injectable gel for lip enhancement. Ethics
Committee approval was obtained from Sheffield
Research Ethics Committee (Leeds, UK), and the
study was conducted at four European sites (three
in the UK and one in Northern Ireland). The study
was registered at http://www.clinicaltrials.gov
(NCT 01176773), and all subjects provided written
informed consent.
D2
A1
P1
R2
Funt, D. and T. Pavicic (2015).
"Dermal fillers in aesthetics: an
overview of adverse events and
treatment approaches." Plast Surg
Nurs 35(1): 13-32.
The objective of this article was to describe
potential adverse events associated with dermal
fillers and to provide structured and clear guidance
on their treatment and avoidance. Reports of
dermal filler complications in the medical literature
were reviewed including those reported for
Restylane for example and, based on the
publications retrieved and the authors’ extensive
experience, recommendations for avoiding and
managing complications are provided.
D2
A1
P1
R1
Gilbert, E., A. Hui et al.
(2012).”The basic science of
dermal fillers: past and present
Part II: adverse effects.” J Drugs
Dermatol 11(9): 1069-1077.
Part I of this article reviews the basic science and
evolution of both historical and contemporary
dermal fillers; Part II examines their adverse
effects.
D2,
A1,
P2,
R2
Hirsch R.J. and Stier M. (2008).
“Complications of soft tissue
augmentation”. J Drugs
Dermatol. Sep; 7(9):841-5.
This article describes a range of complications
resulting from dermal filler injections, reviews key
case studies, and discusses possible treatment
options for adverse effects. While biodegradable
fillers offer the least risk for the patient, location,
allergic reactions, granulomas, necrosis, and
infection are all serious complications that must be
considered before performing soft tissue
augmentation with any approved dermal filler.
D2,
A1,
P2,
R2
Matarasso, S. L., J. D.
Carruthers, et al. (2006).
"Consensus recommendations for
soft-tissue augmentation with
nonanimal stabilised hyaluronic
acid (Matarasso, Carruthers et
al.)." Plast Reconstr Surg 117(3
Suppl): 3S-34S; discussion 35S-
43S.
Review article and consensus statement, mainly
focusing on the product Restylane. Besides
products, procedural aspects were discussed in
detail. The time period from 2000 to 2005 is
covered.
D2,
A1,
P2,
R2
Newman, J. (2009). "Review of
soft tissue augmentation in the
Review article covering the time period from 2000
to 2008. This article compared the current options
D2,
A1,
_____________________________________________________________________________
20/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
face." Clin Cosmet Investig
Dermatol 2: 141-150. of tissue augmentation and discussed the
composition and characteristics of available dermal
fillers.
P1,
R2
Price, R.D, et al (2007).
“Hyaluronic acid: the science and
clinical evidence”. J Plast
Reconstr Aesthet Surg. 60, 1110-
1119
This review represents an overview about the
scientific evidence of HA used in different fields
such as skin regeneration, wound healing and
cosmetic surgery.
D2,
A2,
P2,
R1
Winslow, C. P. (2009). "The
management of dermal filler
complications." Facial Plast Surg
25(2): 124-128.
The purpose of this article is to review the most
commonly encountered complications and
management thereof. Literature published between
2006 and 2008 is taken into consideration.
D2,
A2,
P2,
R1
6. Data analysis
6.1. State-of-the-Art
Pathogenesis
Dermal aging is a consequence of multiple, interacting intrinsic and extrinsic factors. When the
dermis ages, wrinkles, grooves, and ptotic tissue become more and more prominent. Superficial
wrinkles are largely due to photo damage and resulting solar elastosis. This is characterized by
loss of collagen mass in the epidermal–dermal junction and an increased array of elastin whirls
in the deeper dermis. Sun exposure, or photoaging, contributes importantly to the intrinsic
changes associated with aging. Another factor in the appearance of facial aging is the lifelong
activity of the muscles of facial expression, which produces the dynamic and, ultimately, static
facial lines and folds. It has also long been recognized that gravity exerts a toll on the dermal
structures as tissue loses its elasticity and becomes less able to resist stretching (Hoffmann
2009). Grooves appear deeper in the nasolabial and marionette zones with the additional feature
of fat atrophy. As a result of the loss of fat volume, the static suspensory ligaments become
more lax and the face takes on attributes of ptotic jowls, ptotic malar mounds, and nasolabial
folds. Skeletal changes resulting in decreased height of the maxilla and the mandible occur in
the later decades of life (6th–8th decades) and accentuate the above findings. Facial
rejuvenation requires an accurate diagnosis of the above findings, and therapies are directed at
correcting multiple layers. The pillars of dermal rejuvenation: 1) ensuring adequate skeletal
framework and support, 2) tightening and repositioning of the investing musculofascial
aponeurotic system of the face and neck (galea, superficial muscular aponeurotic system, and
platysma), 3) replacement (Newman 2009).
History of dermal fillers
_____________________________________________________________________________
21/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
A major step in the development of injectable fillers occurred in 1981, when bovine collagen
(Zyderm, Zyplast; Inamed Corp., Santa Barbara, CA) became the first FDA-approved injectable
filler for cosmetic use. Zyderm’s smooth flow characteristics made it a popular choice for the
treatment of fine wrinkle lines. But bovine collagen has some notable disadvantages.
Approximately 3 to 3.5 % of the population demonstrate hypersensitivity to bovine collagen,
requiring skin testing prior to injection. Even after an initially negative skin test, 1 % of the
population will still demonstrate hypersensitivity. Other disadvantages include the short
duration of effect and the need for refrigeration of the product. To compound this, bovine
collagen became even less popular during the height of the bovine spongiform encephalopathy
fear. The modern era of injection with synthetic selective bioactive materials began in
December of 2003 with the FDA’s approval of Restylane (Q-Med, Uppsala, Sweden), a
hyaluronic acid (HA) product. Since the introduction of Restylane, various other forms of HA,
like Juvederm (Allergan) have been approved by the FDA for cosmetic use. This has led to a
boom in the popularity of injectable fillers (Kim and Sykes 2011).
Today, a wide range of treatment options are available for managing volume loss in the aging
face, back of the hands and décolleté, including permanent, semi-permanent, and non-
permanent options. A complete aesthetic evaluation of the patient and a thorough understanding
of the patient’s goals and preferences are crucial in any treatment plan. Interventions can
include topical therapy, energy-based therapies, including laser-, radio frequency-, and light
(visible and infrared)-based therapies, surgical procedures, and injectable products, including
neurotoxins such as botulinum toxin type A and fillers (Matarasso, Carruthers et al. 2006).
Epidemiology
As an increasing number of patients seek aesthetic improvement through minimally invasive
procedures, interest in soft tissue augmentation and filling agents is at an all-time high. The
American Society of Plastic Surgeons reported on 13.48 millions of conducted aesthetic
minimally-invasive procedures in the U.S. in 2013 (in contrast to 1.67 millions of aesthetic
surgical procedures). About 2.24 millions of soft tissue filler injections were administered to
patients, of which 1.68 millions were hyaluronic acid injections (numerous different products)
(http://www.plasticsurgery.org/news/plastic-surgery-statistics/2013.html).
Dermal fillers and subcutaneous volume enhancers have enjoyed the greatest degree of
development and differentiation because they are also administered in an office-based setting.
The ideal dermal filler is one that is biocompatible, predictable, adjustable to the anatomy of the
patient, long-lasting, reversible, and natural in appearance, while no single filler possesses all of
these characteristics (Newman 2009). HA fillers are commonly used for wrinkle treatment, fold
filling, and regional volumising.
Treatment Options
Although soft tissue augmentation dates back over a century to when autologous fat was used,
injectable fillers entered mainstream cosmetic medicine when bovine collagen injections were
developed in the 1980s. Autologous fat, once a staple in the filler arena, has been largely
replaced by the new generation of fillers because aesthetic results and duration of benefit after
_____________________________________________________________________________
22/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
fat injection have a degree of variability that is unacceptable to many physicians and their
patients. Reports on the fat-grafting technique are anecdotal and no statistics on the "take" of fat
have been published (Smith 2008).
In general the dermal fillers can be classified in absorbable fillers like collagen or hyaluronic
acid based products, biodegradable microparticle injectable implants (calcium hydroxylapatite
or Poly-L-lactic acid), or non-absorbable fillers containing poly-methylacrylate or silicone.
Injectable microparticles are absorbed much slower than collagen or hyaluronic acid. This fact
is considered as an advantage if compared to absorbable fillers. The disadvantage of these
materials is that the procedure is not reversible; corrections are not possible or even in an
invasive way. With non-absorbable fillers there is only limited experience. Based on the
available literature, the risk of side effects is higher compared to absorbable material (Newman
2009).
Hyaluronic Acid
Hyaluronic acid (HA)-based gels are now the gold standard in dermal fillers, with more
cosmetic procedures in the United States using these fillers than all other fillers combined. The
widespread acceptance of HA fillers is testament to their biocompatibility (unlike protein-based
fillers, they are composed of polysaccharides that exhibit no species specificity), the stability of
their cross-linked HA in vivo (which promotes longevity of clinical improvement), and their
good record of safety and effectiveness in other countries where they have been in use for many
years (Baumann, Shamban et al. 2007).
Hyaluronic acid, or hyaluronan, is a glycosaminoglycan that consists of regularly repeating non-
sulfated disaccharide units of glucuronic acid and N-acetylglucosamine. Hyaluronan is a
naturally occurring biopolymer that exhibits no species or tissue specificity. It is an essential
component of the extracellular matrix of all adult animal tissues and is especially abundant in
early embryos. Hyaluronan normally exists in tissues as a free polymer of linked disaccharide
units and is highly negatively charged. However, in some tissues, such as cartilage and bone,
hyaluronan is bound to large glycoprotein structures or specific cell receptors. In healthy
tissues, the average molecular weight of hyaluronan is 5 to 10 million with up to 25,000
disaccharide units, and the average adult concentration is 200 mg/kg (0.02 %) (Matarasso,
Carruthers et al. 2006, Price, Berry et al. 2007).
A series of chemical modifications and processing steps must be applied to HA to develop
viable formulations for use as dermal fillers. The raw HA polymer used to produce dermal
fillers is usually supplied to the manufacturer in dry powder form. In order to overcome the lack
of persistence of uncross-linked HA, dermal filler manufacturers use crosslinkers. The
crosslinkers bind HA polymer chains to each other, creating a polymer ‘network’ and
transforming the viscous liquid into a gel. The resulting HA gel acts as a single unit, imposing a
physical and chemical barrier to enzymatic and free radical breakdown (Tezel and Fredrickson
2008).
Cross-linked derivatives have been shown to be well tolerated when injected into locations such
as the skin and vocal folds. The use of HA is particularly attractive for soft-tissue augmentation,
_____________________________________________________________________________
23/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
because it is hydrophilic and a normal extracellular component of skin. Factors that impact HA
persistence include HA concentration, percentage of cross-linkage, type of cross-linking, its
fluid retention (i.e. water binding capacity), and injection technique. The two most important
factors are the percentage of cross-linking and the water binding capability of the hyaluronic
gel. If uncross-linked HA is added to water, it produces a highly viscous liquid that would only
last a few days in human skin. For that reason manufacturers use various agents to cross-link
the HA. As a result, the final proportion of cross-linked HA and the degree of cross-linking
impact the physical characteristic of the final product (Newman 2009).
Almost all HA fillers on the world market use 1 of 3 basic cross-linking chemistries. Of these 3,
butanediol diglycidyl ether (BDDE) has by far the longest track record (about 20 years as of
July 2008), and the greatest amount of clinical experience (many millions of patients treated
worldwide including North America) (Smith 2008).
One very important characteristic of HA products is the ability of clinicians to break down the
cross-linking of each product with the use of an enzyme known as hyaluronidase. This enzyme
breaks the cross-links by hydrolysis of the glucosamine and glucornic acid moiety. This result
in the breakage of the cross-links and the three-dimensional structure of HA becomes absorbed
within hours by the surrounding interstitial fluid. One note of caution is the possibility of
allergic reaction with purified bovine testicular hyaluronidase or with preparations that contain
metabisulfite (Newman 2009).
In general clinical trials have documented the safety profile of all forms of HA. Transient and
self-limiting redness and swelling are common following injections of HA and this is due to the
hydrophilic nature of HA. Pain associated with injection may be managed by the use of both
topical and injected anaesthetic agents. Despite adequate anaesthesia, patients can expect
tenderness for 1 to 2 days after injection (Lupo 2006).
Potential adverse reactions are minimal and are mainly injection-related and self-resolving.
These include local bruising, purpura, erythema, and tenderness, itching, and swelling. A major
adverse event that has been reported is hypersensitivity, but true immunoglobulin G- and E-
mediated reactions are rare (Rohrich and Ghavami 2007).
Although no treatment is entirely without risk, the side effect profiles of HAs and other dermal
fillers have been reviewed extensively. HAs in general have demonstrated excellent benefit–risk
profiles. Serious adverse events are rare, and most reactions are transient, injection-site related,
and mild to moderate in severity (Gold 2009).
Manufacturers may provide free HA as a soluble fluid component to the gel to facilitate the
extrusion of the filler through fine-bore needles. This fluid component is often present and
contains unmodified and modified soluble HA that is generated during the manufacturing
process (Kablik, Monheit et al. 2009). Gel hardness or G’ plays an important role in how the
gels must be sized for easy delivery through fine-bore needles.
By virtue of HAs biocompatibility and non-toxicity, it is used in many biomedical fields, such
as ophthalmology, dermatology and rheumatology.
_____________________________________________________________________________
24/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
6.2. Performance
Restylane
Early clinical and efficacy studies of Restylane were reported from Italy and Sweden. In
Sweden, 100 patients were fully assessed following treatment in 285 locations (lips, wrinkles,
folds). The Swedish study reported that, based on physician evaluations, treatment sites
maintained an average of 82 % and 69 % correction (using a visual analogue scale of 0 to
100 %) at 12 and 26 weeks, respectively. In Italy, 158 patients were treated for augmentation
therapy of wrinkles and folds. The Italian study reported that 78 percent of patients maintained
moderate to marked improvement after 8 months, with nasolabial folds and lips sustaining the
best results (Matarasso, Carruthers et al. 2006).
The key active comparator study of Restylane versus Zyplast (bovine collagen; Inamed Aesthet-
ics, Inc., Santa Barbara, Calif.), reported in 2003, provided the basis for the approval of
Restylane use in the United States. The randomised patient- and evaluator-blinded study was
conducted at six centres in the United States, and subjects seeking soft tissue augmentation
treatment for correction of bilateral nasolabial folds were recruited. Each patient received
Restylane in one nasolabial fold and Zyplast on the contra-lateral side of the face. Of 152
subjects who were initially screened, 138 were randomised to study treatment and treated with
both study products (safety population). The intent-to-treat population comprised 137 patients
(128 women and 9 men). Patients ranged in age from 27 to 78 years (mean 54.3) and were
predominantly White (89 %); 59 patients (43.1 %) had previously received collagen injections.
Of this population, 134 patients completed 6 months of follow-up, whereas 4 patients withdrew
from the study prematurely because of consent withdrawal (2), protocol violation (1), or loss to
follow-up (1). Restylane was superior to Zyplast in 56.9 % of patients, whereas Zyplast was
superior to Restylane in 9.5 % of patients (P<0.0001). By this time, 67.2 % of Zyplast-treated
folds had returned to their pre-treatment condition compared with only 29.9 % of Restylane-
treated folds. Likewise, Restylane produced a significantly better (P<0.0001) Global Aesthetic
Improvement Scale (GAIS) rating than Zyplast at all time points after baseline. At 6 months
after baseline, Restylane proved superior to Zyplast in this regard in 62.0 % of patients, whereas
Zyplast was superior to Restylane in 8.0 % of patients (P<0.0001). Patient evaluations of
treatment efficacy were consistent with those of the investigators. After the initial treatment
session, local injection-site reactions (as recorded in patients’ diaries) occurred at 93.5 % of
Restylane- and 90.6 % of Zyplast-treated sites, but these were predominantly mild or moderate
in intensity and short lasting (7 days or less). All delayed-onset reactions (redness was the most
common) were mild or moderate in intensity and resolved within 2 to 3 months without
treatment (Narins, Brandt et al. 2003).
Morris et al retrospectively reviewed the records of 145 consecutive patients who underwent
intradermal and subcutaneous injection of the face with Restylane (0.4 ml or 1 ml) for volume
augmentation and/or to improve rhytid appearance. Patients were treated at Duke University
Eye Centre between February 2005 and March 2006. IRB approval was obtained From
February 2005 to March 2006, 309 Restylane injections were performed on 145 patients (mean,
_____________________________________________________________________________
25/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
2.14 injections/ patient). Gender distribution was 139 female and 6 male, and median age was
53 years (mean, 54 years). There was a median follow-up time of 8 months (mean, 10.4 months;
range, 1–37 months) for all returning patients. Median follow-up time was 11 months (mean, 12
months; range, 1–37 months) for the 75 patients (52 %) who underwent reinjection. Thirty-
seven of 140 patients (26 %) received adjunctive anaesthesia. Injection locations were as
follows: nasolabial folds [72 % (104/145)], melolabial folds [70 % (102/145)], lips [51 %
(74/145)], infraorbital rims [24 % (35/145)], perioral rhytids [24 % (35/145)], glabella [23 %
(34/145)], malar hollows [10 % (14/145)], chin [8 % (12/145)], and other [8 % (12/145)]. The
excellent safety profile of Restylane reported in this study is consistent with its favourable
status when compared with other soft-tissue fillers. Unlike other soft-tissue fillers, its
reversibility with hyaluronidase can help mitigate overcorrection or hypersensitivity. Its
biodegradability and shorter duration compared with more permanent fillers are also favourable
in the setting of an adverse reaction (Morris, Stinnett et al. 2008).
Glogau et al investigated 180 patients in a randomised controlled trial within the indication lip
augmentation. Of 180 patients randomised, 135 received Restylane, and 45 received no
treatment and were included in the ITT population. Eighty patients in the Restylane group
received a touch-up 2 weeks after the first treatment session. One hundred sixteen (86 %) in the
Restylane group and 39 (87 %) in the no-treatment group completed the study. The results of
the current study clearly demonstrated the durability of the augmentation provided by
Restylane. All of the pivotal assessments (live blinded evaluations, unblinded evaluator scoring,
and IPR) showed statistically significant differences in MLFS response between the treatment
group and the control group through 6 months (week 24). The data from the GAIS scoring, on
which patients and physicians noted significant differences at all time points, further
corroborated the persistence of effect. This durability compares favorably with collagen
products (animal and human, no longer available in the United States), which produce results
that last an average of approximately 3 months. Restylane treatment for lip augmentation was
well tolerated. The majority of reported AEs were mild to moderate in severity, anticipated in
their nature (swelling, contusion, pain), and generally resolved promptly. No persistent nodules,
masses, or significant asymmetry were noted during the study. Nearly all (96 %) patients
enrolled in the present study received an anaesthetic during the first Restylane treatment,
including topical, regional, or a combination of both types of anaesthesia. Injecting local
anaesthetic for an infraorbital or submental nerve block can distort anatomic features and
complicate the augmentation procedure (Glogau, Bank et al. 2012).
Schweiger et al reported on a 21-year-old female was seen in dermatology clinic with the
complaint of lip asymmetry. She reported being born with a unilateral left-sided cleft lip and
cleft palate. From the age of 12 weeks to 20 years, she had received an estimated 12
reconstructive procedures by craniofacial surgeons. She also had received specialized care from
dentists, oral surgeons, and speech pathologists in the past. The patient was successfully treated
with injection of HA (Restylane, Medicis Aesthetics, Scottsdale, AZ). She first underwent an
intraoral miniblock with 0.5 mL of 1 % lidocaine with 1:100,000 epinephrine injected above
each canine in the buccal mucosal groove. A quantity of 0.5 mL of HA was then placed into the
left mucosal body and vermilion. Additional filler was placed at both areas of dimpled
retraction. After the mucosal lip was treated with a goal of 100 % correction, an additional
0.2mL of HA was injected under the left cutaneous upper lip line scar. Clinical improvement
_____________________________________________________________________________
26/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
was noted immediately, as was mild bruising. She returned to clinic 10 days after treatment for
follow-up and was felt to have an excellent cosmetic result. The results lasted approximately 4
months with a gradual decline to baseline. The authors concluded that soft tissue augmentation
using injectable fillers can also be used to address the aesthetic considerations of decreased
upper lip volume and asymmetry (Schweiger, Riddle et al. 2008).
Solish et al describe a prospective pilot study conducted a two centres in Canada with Restylane
hyaluronic acid. 21 adults were enrolled in this study seeking lip augmentation. The finding of
this study suggests the treatment resulted in a clinically significant change in patients’
appearance. Adverse events were reported in five patients during the study, but all of them were
considered to be not related to the study treatment (Solish and Swift 2011).
Wu et al performed a clinical trial in order to compare Restylane with a new HA dermal filler
(BioHyalux). This was a multicenter, double-blinded, randomised, controlled, non-inferiority
clinical trial involving 88 subjects with moderate to severe nasolabial folds. Subjects were
randomised to receive an injection of Restylane in one nasolabial fold and BioHyalux in the
opposite nasolabial fold. The total amount of filler was 0.99 ± 0.27 mL on the BioHyalux side,
and 0.94 ± 0.27 mL on the Restylane side. The outcome was assessed before and right after
injection, and at 1 week, 1, 3, and 6 months. Patients were followed up for 13–15 months to
evaluate the durability and long-term safety. A clinically meaningful response was predefined
as at least one-point improvement on the Wrinkle Severity Rating Scale, which is a five-point
scale. At 6 months, the response rate of BioHyalux was not significantly different to that of
Restylane. At the 13–15 months follow-up, the response rate by investigators was 58.0 % on the
BioHyalux side versus 63.8 % on the Restylane side. The response rate by subjects showed
similar results, which was 56.5 % on the BioHyalux side versus 60.9 % on the Restylane side at
13–15 months. The subjects’ Global Aesthetic Improvement Scale (GAIS) showed that most
subjects felt improvements on both sides of the nasolabial folds at all time points. At 6 months,
100 % reported improvements on both side; at 13–15 months, 60 % of subjects reported
improvements with BioHyalux versus 64 % with Restylane. Adverse events were transient and
predominantly mild or moderate in severity including injection site swelling, pain, itching,
bruising, and tenderness. It can be concluded that both products showed an adequate
performance in this study, with reliable safety (Wu, Sun et al. 2016).
Juvéderm Ultra/Juvéderm Ultra Plus
Pinsky et al investigated the safety and effectiveness of Juvederm dermal fillers compared to
Zyplast® bovine collagen for the correction of nasolabial folds in a multicentre, double-blind,
randomised, within-subject controlled trial. 292 subjects were randomly treated with Juvederm
Ultra or Juvederm Ultra Plus in one nasolabial fold and Zyplast bovine collagen in the other
nasolabial fold. The treating investigators were instructed to fill each nasolabial fold to full
correction (100 % of the defect), but not to overcorrect. A maximum of 3 treatments – first
treatment and up to 2 touch-ups at roughly 2-week intervals – were allowed to achieve optimal
correction. An average injection volume of 1.5 mL (2 syringes) of Juvederm dermal filler was
used for initial treatment and 0.7 mL (1 syringe) for repeat treatment. Nasolabial fold severity
was assessed using the 5-point Wrinkle Assessment Scale (WAS), and a validated photographic
guide. After 6 months subjects showed a clinically significant mean level of improvement for
_____________________________________________________________________________
27/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
the nasolabial folds treated with Juvederm Ultra or Juvederm Ultra Plus, but not for nasolabial
folds treated with Zyplast, supporting the above stated findings by showing a longer longevity
for Juvederm Ultra and Ultra Plus than for Zyplast. The mean level of improvement was still
clinically significant for subjects who returned for a follow-up treatment beyond 9 months, with
the proportion of nasolabial folds still showing clinically significant improvement in 75 % with
Juvederm Ultra and 81 % with Juvederm Ultra Plus. Juvederm Ultra Plus was shown to last
even 12 months or longer. Again, the frequency and severity of treatment site reactions (e.g.,
erythema, indurations, pain, edema, nodule formation, bruising, pruritus, and discoloration)
were mild or moderate and were similar for all fillers. The authors concluded, that due to its
superior longevity, individuals treated with these Juvederm™ dermal fillers may require to
repeat treatments less frequently than those treated with bovine collagen fillers, and that less
product will be needed at repeat treatments (Pinsky, Thomas et al. 2008).
In the pivotal trial that led to FDA approval of Juvederm, Baumann et al (2007) compared the
safety and effectiveness of 3 types of smooth-gel HA dermal fillers vs. cross-linked collagen in
the treatment of NLF in 439 subjects in a multicentre, double-masked, randomised, within-
subject study. The subjects randomly received one of three types of smooth-gel HA dermal
filler in one NLF and cross-linked bovine collagen in the other. The three different smooth-gel
HAs used were Juvederm, Juvederm Ultra, or Juvederm Ultra Plus. The cross-linked bovine
collagen filler used was Zyplast (Allergan, formerly Inamed). The NLFs were to be filled to full
correction (100 % of the defect), and not overcorrected, and a maximum of 3 treatments – first
treatment and up to 2 touch-ups at roughly 2-week intervals – were allowed to achieve optimal
correction. NLF severity was assessed using the 5-point Wrinkle Assessment Scale (WAS),
with 0 = none (no wrinkle); 1 = mild (shallow, just perceptible wrinkle); 2 = moderate
(moderately deep wrinkle); 3 = severe (deep wrinkle, well defined edges but not overlapping); 4
= extreme (very deep wrinkle, redundant fold with overlapping skin). The results showed that
all three dermal fillers proved longer-lasting clinical corrections than bovine collagen. Twenty-
four weeks after the last treatment, 90 % of subjects treated with Juvederm Ultra Plus dermal
filler retained a clinically significant improvement, 88 % treated with Juvederm Ultra and 81 %
with dermal filler. The bovine collagen–treated NLFs showed clearly shorter longevity with
lasting improvement after 24 weeks ranging from 36 % to 45 %. In addition to its superior
longevity, the injection volume for HA dermal fillers proved to be lower (median, 1.6 mL)
compared with bovine collagen (median, 2.0 mL), representing an additional important
advantage for the patient in treatment costs and comfort. The only treatment-related adverse
events observed were localized site reactions in the area of injection, which were mild to
moderate in severity and did not differ between any filler type. In decreasing percentage those
were injection site induration, erythema, edema, pain, nodule formation, bruising, discoloration,
and pruritus; they lasted no more than 7 days. The preferred filler by the patients used was
Juvederm Ultra with 88 %, followed by 84 % for Juvederm Ultra Plus and 78 % for Juvederm;
the majority of subjects preferred HA fillers to the collagen fillers (Baumann, Shamban et al.
2007, Bogdan Allemann and Baumann 2008).
Upon completion of the pivotal IDE clinical trial for Juvederm, Juvederm Ultra, and Juvederm
Ultra Plus, five of the original 11 study sites were selected to participate in an extended follow-
up evaluation. Sites were selected based on their continued abilities to participate in the follow-
up protocol, their track record of visit schedule compliance, and the planned sample size of 150
_____________________________________________________________________________
28/40
Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
subjects. No consideration was given to duration of filler correction in the selection of sites.
Subjects who were eligible and agreed to participate in the follow-up study signed an informed
consent and were followed from 4 through 48 weeks after their repeat treatments. Routine
follow-up visits for effectiveness occurred at 4, 12, and 24 weeks, and an amendment to the
protocol added visits at 36 and 48 weeks after repeat treatment. Safety and effectiveness were
evaluated at each office visit. At the end of the pivotal study, subjects were asked which
treatment they preferred and were subsequently un-blinded. Subjects were offered repeat
treatment of both NLFs with the original Juvederm formulation after the 24-week visit. For this
follow-up study, subjects remained non-randomised and un-blinded. 80 individuals signed
consent forms and enrolled in the follow- up study. The mean improvement in NLF severity
remained clinically significant from 4 weeks after initial treatment through 48 weeks after
repeat treatment. Thus, subjects sustained a total of 18–21 months of wrinkle correction with a
repeat treatment at 6–9 months. Furthermore, a full 78–90% of subjects were responders at 48
weeks post-repeat treatment, and the long-term results showed a smooth, natural looking
wrinkle correction. No serious or unanticipated adverse events were reported. One subject had
positive serum IgG antibody titers at 24 weeks after initial and 4 weeks after repeat treatment,
but no clinical signs or symptoms of hypersensitivity (Smith, Jones et al. 2010).
The results of the above mentioned studies are supported by a recent study by Lupo et al which
compared Juvederm Ultra Plus HA filler with Zyplast bovine collagen in a multicentre, double-
blind, randomised, within-subject, controlled study (Lupo et al 2008). In a split-face mode,
severe NLFs of 87 subjects were treated one side with Juvederm Ultra Plus and the other side
with Zyplast. In the study population all Fitzpatrick skin types were represented, 36% having
darker skin types (Fitzpatrick types IV through VI). Up to two touch-up treatments were
allowed at 2-week intervals. Effectiveness was assessed using the validated, static, 5-point
Wrinkle Assessment Scale (WAS) with a photographic guide. The Juvederm Ultra Plus filler
showed significantly better NLF severity scores compared to Zyplast at each follow-up time
point from 4 to 24 weeks. At 24-week follow-up clinically significant correction of NLF treated
with Juvederm were shown in 96% compared with 41 % Zyderm. The clinical correction with
Juvederm Ultra Plus remained high, whereas the scores for Zyplast nearly returned to baseline
over the period of 24 weeks. At 24 weeks, the mean improvement was still 1.7 with the
Juvederm Ultra Plus product but only 0.5 with bovine collagen. Longevity was shown by
maintenance of the clinical correction for 1 year or more in 81 % of NLFs treated with
Juvederm. The median volume of Juvederm required was 0.7 mL (one syringe), significantly
less than for Zyplast (1.6 mL). For the initial treatment, the median volume of Juvederm Ultra
Plus injected was 2 syringes (1.6 mL), and less than 1 syringe (0.7 mL) for the retreatment at
after 6–9 months. Treatment site reactions were similar for Juvederm Ultra Plus and Zyplast
and were similar to those in the abovementioned trials. As for patient satisfaction, most subjects
preferred Juvederm Ultra Plus (85 %) versus collagen (10 %); 5% showed no preference (Lupo,
Smith et al. 2008).
Juvéderm Volbella
The objective of the prospective, multicenter, open-label, post market study of Ecclestone et al
was to demonstrate the safety and effectiveness of Juvéderm Volbella injectable gel for lip
enhancement. The four investigators enrolled and treated 60 subjects between October 2010 and
_____________________________________________________________________________
29/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
January 2011, and 59 of these subjects (98.3%) completed the study. All of the subjects were
women, and the mean age was 50 years (range, 21–74). Following treatment with Juvéderm
Volbella injectable gel, subjects returned to the clinic for follow-up at 1, 3, 6, 9, and 12 months
after initial treatment. An optional top-up treatment was allowed at 2 weeks. The mean injection
volume was 1.2 mL (range, 0.5–2 mL) for initial treatment and 0.55 mL (range, 0.3–1 mL) for
touch-up treatment. The Month 3 Lip Fullness Score responder rate based on investigator
assessments was 93.2% (P <0.0001). The responder rate over time showed that more than three-
quarters of subjects still had improved lip fullness at month 9 and almost half had improved
fullness at month 12. After treatment, the Lip Fullness Score improved from 1.8 (mild) to 3.0
(moderate). On the 11-point look and feel questionnaire where 0 is lumpy and 10 is smooth,
81.0% of subjects had ratings of 7–10 at Month 1, indicating that they thought their lips felt
smooth. On similar questions at Month 1, 67.2% of subjects reported that their lips felt soft,
91.4% reported their lips felt natural, 91.4% reported their lips looked natural, and 84.5%
reported their lips looked even. High ratings on all of these outcomes were maintained
throughout the course of the study. In terms of overall satisfaction with the effects of treatment,
96.6% of subjects reported being satisfied (scores of 7–10 on the 11-point scale) at Month 1,
and by Month 12 more than 80% of subjects were still satisfied. The mean satisfaction score at
Month 1 was 9.3, and it remained at 9.0 or better at every subsequent visit. The performance of
Juvéderm Volbella for lip augmentation was conclusively demonstrated in this clinical study
(Eccleston and Murphy 2012).
Recently, the performance and safety of Juvéderm Volbella containing lidocaine have been
investigated in 62 patients. In total, 83.6% of the subjects were “Extremely Satisfied”, “Very
Satisfied” or “Satisfied” with the improvement in their lips after the first injection, and the
physicians being “Extremely Satisfied” or “Very Satisfied” with lip improvement in 100% of
the subjects. The high levels of satisfaction may be explained by the natural effect produced by
the treatment: 61.7% of subjects rated the look and feel of their lips as “Extremely Natural” or
“Very Natural” after the first injection, and no subject considered the look and feel to be “Not
Natural” at the follow-up visit. These results are particularly relevant when it is considered that
the majority of subjects (77.4%) had pre-treatment concerns about the possible unnatural look
of their lips following injection. In summary, BDDE-crosslinked HA in an amount of 15
mg/mL has been shown to be effective in lip augmentation (Philipp-Dormston, Hilton et al.
2014).
6.3. Safety
Hyaluronic acid
Since HA occurs naturally in the human body, the risk of allergic reactions is very low and thus,
the manufacturers suggest that there is no need for skin testing before. The differences in chain
length molecular weight do not appear to have any clinical significance. Adverse effects related
to HA injection are most commonly localized, immediate, and non-allergic, and include pain,
edema, and ecchymoses. Additional side effects to consider are an angioedema-like swelling
and hypersensitivity as well as the rare rapidly developing bacterial infection acquired
transdermally while injecting (Gilbert, Hui et al. 2012).
_____________________________________________________________________________
30/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
Since HA occurs naturally in the human body, the risk of allergic reactions is very low and thus,
the manufacturers suggest that there is no need for skin testing before. The differences in chain
length molecular weight do not appear to have any clinical significance. Adverse effects related
to HA injection are most commonly localized, immediate, and non-allergic, and include pain,
edema, and ecchymoses. Additional side effects to consider are an angioedema-like swelling
and hypersensitivity as well as the rare rapidly developing bacterial infection acquired
transdermally while injecting (Gilbert, Hui et al. 2012).
In fact, there is a very small amount of proteins which can lead to some hypersensitivity
reactions. Anti-HA antibodies have been demonstrated but the clinical significance is not
exactly known. A retrospective European survey has evaluated the risk of important adverse
reactions with the HA from Q-Med from 1997 to 2001. A total of 4,320 patients were evaluated
and 12,344 syringes were injected. From 1997 to 2001, 34 cases of hypersensitivity are
reported: 16 cases of immediate hypersensitivity and 18 cases of delayed reactions. Global risk
is 0.8 %. Since 2000, the load of proteins of the Q-Med product has decreased, and the
incidence of hypersensitivity reactions has become around 0.6 %. As 50 % of these reactions
are immediate and resolved within less than three weeks, the risk of transient delayed reactions
was around 0.3 % with the old formulations. These are now significantly less frequent (less than
1 in 2000 treatments) with the current Q-Med products. These remain the most used products in
the UK and are very predictable. Sterile abscess and lividoid pattern after intra vascular
injection has been reported. No systemic reactions have been reported. Non-animal HA from
the Q-Med company does not need skin testing. In cases of ‘‘inflammatory’’ reactions, the
histological aspects can be either a moderate lymphocytic infiltrate with some plasma cells in
the dermis and the hypodermis or a lymphocytic infiltrate with macrophages and presence of
foreign body giant cells (Andre, Lowe et al. 2005).
HA dermal fillers as a group are very well tolerated. Infection can occur but is rare.
Hypersensitivity reactions are also uncommon, and may result from reaction to the cross-
linking agent used to stabilize the HA. Occasionally HA can be palpated, or a blue-gray tinge
can be seen in the area of injection. This can be the result of superficial injection allowing more
water binding in the dermis which selectively reflects blue wavelength of light making it appear
darker than the surrounding skin. Solutions to this problem can be addressed by camouflage
with makeup, needle puncture, and massage of excess gel from the dermis or injection of
hyaluronidase. Injection technique can lead to clumping of HA especially in the lips. Massaging
the area immediately following injection is the best way to prevent lumps from persisting. It is
important to have patients understand the expected clinical course of swelling, firmness, and
then softening which typically occurs over the course of 1 week. One of the benefits of using
HA for the less experienced user is the fact that they can be readily broken down by the
hyaluronidase (Newman 2009).
The most frequent types of reactions are needle marks at the site of injection, erythema,
swelling, tenderness, mild pruritus, bruising, and small lumps/bumps. These are generally mild
and are usually transient. These reactions should be discussed in detail with the patient before
treatment so that they are considered expected rather than true complications (Beasley, Weiss et
al. 2009).
_____________________________________________________________________________
31/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
True complications are rarely seen when injecting HAs, but many of these complications
directly correlate with the skill and experience of the physician-injector. These true
complications include injection into or compression of vascular supply, tissue necrosis,
persistent nodule formation, granuloma formation, allergic reaction, infection, and visible blue
hue (Tyndall effect). It has been well documented that nitropaste and hyaluronidase must be
readily available in the physician´s office for the immediate treatment of any vascular
compromise. Hyaluronidase and extrusion techniques are also helpful for treating persistent
nodules and the Tyndall effect (Beasley, Weiss et al. 2009).
The management of dermal filler complications is summarised in an article of C. Winslow.
Bruising is a potential complication to all fillers. The potential to bruise can be affected by
needle size, location of infection, and type of filler. Medication such as aspirin, ibuprofen, or
other anticoagulants may make the patient more susceptible to bruises. Herbal supplements
such as fish oil, glucosamine, or chondroitin can also adversely impact bruising. Swelling is the
most common and ubiquitous complication experienced with fillers. HA fillers are sugar
molecules that bind and hold water and should be expected to cause more swelling than do
other classes of fillers. Post-treatment ice application and elevation of there head may help.
Patient troubled by swelling may benefit from short prednisone taper or antihistamines.
Formation of lumps under the skin can occur due to the consistency of the filler, reaction to the
product, or poor technique. Small lumps resulting from HA injection can easily be treated with
hyaluronidase. Improvement can be seen within hours. The ability to contour the injection site
after injection is unique to HA class and is attractive to many patients. Erythema after injection
is common, especially if massage is performed immediately after filler placement. Some
amount of pain during and after injection is common and can be prevented with topical
numbing and/or nerve blocks administered before injecting the filler. Skin necrosis is a well
known complication that has a predilection for certain “danger zone”. The dorsal nasal artery
may cause compromise of skin at the alar region. Collagen and hyaluronic acid are commonly
injected in the lips. Filler injections in the perioral area can induce cold sore formation by
reactivation of the latent virus. Stress, swelling, and massage may also contribute. Patients with
a strong history of cold sore activation or those who had cold sores with prior injections should
be treated with an antiviral such as acyclovir. Infection is fortunately quite rare after filler
injection in an acutely inflamed area, such as skin with active acneic breakout. Focal or
systemic infections should be considered a contraindication to injection. True allergic reactions
are quite rare with HA. Immediate allergic reactions are manifested by significant swelling,
itching, and pain. Swelling may involve the oral cavity, lips, and tongue, depending on the
severity of reaction and location of injection. Skin testing for HA is not standard or required but
should be considered in atopic individuals. Despite its rare nature, hypersensitivity to HA or its
derivatives of its preparation may still be seen in < 1 % of patients injected. Granulomas
typically appear late, months or years after injection, and remain localized to the injection site.
They are typically soft and dark red or purple. Intralesional steroids remain the mainstay of
granuloma treatment. The most dreaded complication because of its unsightly nature and
permanence, a scar can result from injection or a complication thereof. Treatment of scares
includes intralesional steroid, pulsed dye laser or pulsed light treatments, pressure, and silicone
(Winslow 2009).
_____________________________________________________________________________
32/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
Whilst it is true that HA is tolerated extremely well, it is not uncommon (12 %) to observe
transient erythema and mild swelling. Other documented complications include a case report of
a clinical picture similar to a sterile abscess over injection sites and injections of any form may
trigger sarcoidosis at the injection site, and HA has not escaped. A recent review also quoted an
overall significant complication rate of 1 in 1600 applications. The mild tissue reaction seen
with many injections may, on occasion, be so profound as to elicit a formal inflammatory
response and a range of reactions has been documented, varying from simple hypersensitivity,
to angioedema with positive titres of anti-HA immunoglobulin G and E (Price, Berry et al.
2007).
Depth of dermal filler placement is particularly important in preventing discoloration. Novice
injectors occasionally inject too superficially causing a blue-gray discoloration known as the
Tyndall effect. The Tyndall effect refers to the fact that different wavelengths of light scatter
depending on the size of substances they encounter. According to Rayleigh scattering, for
sufficiently small particles, the amount of light scattered is inversely proportional to the fourth
power of wavelength. For example, blue light is scattered more than red light by a factor of
(700/400) = ~ 10. Thus, within the skin, long red wavelengths penetrate deeper into the tissue
while shorter blue wavelengths are more easily scattered and reflected outwards. The incidence
of the Tyndall effect is most likely to occur if filler meant to be injected deeply is injected too
superficially in the skin. The high-risk areas include the so-called I zone of the central face, (the
nasojugal folds, nasal dorsum, and lip), the infraorbital troughs, and fine superficial lines such
as periorbital and perioral rhytids ("crow's feet" and "pucker lines") (Hirsch and Stier 2008).
A more recent review article also discussed potential complications associated with the use of
dermal fillers. The authors concluded the following: The past decade has seen the arrival of a
host of new soft tissue fillers for facial rejuvenation, which not only remove wrinkles but also
have the ability to restore facial volume to create a balanced, more natural rejuvenated look. To
achieve cosmetically pleasing results, it is essential that those practicing facial rejuvenation
have a thorough understanding of the individual characteristics of available fillers, their
indications, contraindications, benefits and drawbacks, and ways to prevent and avoid potential
complications. Side effects can occur with any dermal filler, but knowledge of the frequency
and potential risk factors is limited. A report from the Injectable Filler Safety Study, which
obtained population-based data on the type and frequency of adverse reactions to injectable
filler substances from dermatologists and plastic surgeons practicing in Berlin, Germany,
confirmed that while adverse reactions are documented with all injectable fillers, time until
reaction and the type of adverse reaction varied between the different fillers. For example,
adverse reactions to biodegradable fillers occurred after a mean (standard deviation) of 4.9 ± 5.8
months, and reactions to nonbiodegradable fillers after 18.3 ± 19.0 months. Adverse events in
patients treated with HA-based fillers (mostly Restylane) were mainly swelling, erythema, and
nodules. Furthermore, as with any procedure that breaks the surface of the skin, dermal filler
injections are associated with a risk of infection. To minimize this risk, sterilising the injection
site with an effective topical disinfectant, carefully removing the needle and syringe from
sterilized individual packaging, wearing gloves throughout the procedure, and ensuring that the
needle is not contaminated during the procedure is important (Funt and Pavicic 2015).
Restylane
_____________________________________________________________________________
33/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
Studies reported injection-related reactions, including redness, swelling, darkening of the
treatment site, and slight pain in about 12 % of patients. Ongoing analysis of the adverse event
databases indicated that in 1999, with an estimated 144,000 patients treated with Restylane,
only one of every 650 (0.15 %) reported redness, swelling, localised granulomatous reactions,
bacterial infection, or acneiform lesions. Delayed implant hypersensitivity reactions were
reported in several case series at low incidences (0.4 to 3.7 %) in early (before mid-1999) non–
United States use of Restylane. In mid 1999, a hyaluronic acid raw material with trace amounts
of protein six times lower than the raw material previously used was introduced. The amount of
protein in the more purified product was reported to be in the range of 13 to 17 mg/ml of
product. In contrast to 1999, reported adverse events were reduced to 0.06 % and
hypersensitivity reactions were reduced to 0.02 % (Matarasso, Carruthers et al. 2006).
Small gel-particle hyaluronic acid (Restylane) and large gel-particle hyaluronic acid (Perlane)
were studied to evaluate their safety for the correction of oral commissures, marionette lines,
upper perioral rhytides and nasolabial folds (NLFs). Twenty patients with a mean age of 59.6
years (range 49 to 65 years) were treated with an average of 5.58 +/-1.15 mL of HA for the
entire perioral area. Treatment areas included NLFs, marionette lines, oral commissures and
perioral rhytides. Eighteen of 20 patients received Restylane and Perlane. The products were
injected into the mid or deep dermis using primarily linear threading and multiple punctate
pools. Patients experienced a total of 66 treatment-emergent adverse events. The reported
events in decreasing order of occurrence were bruising, tenderness, swelling, redness, headache
and discomfort. Bruising was more common in the NLFs and marionette lines than in the oral
commissures and perioral rhytides. Tenderness occurred more often in the perioral rhytides than
in the other areas. The maximum intensity of all adverse events was considered mild. Most
adverse events resolved within seven days, with an average duration of four days. No serious
adverse events occurred during the study. One hundred percent of GAIS evaluations by both
investigators and patients indicated improvement, regardless of filler used or area treated
(Brandt, Bassichis et al. 2011).
Juvéderm Volbella
In the study of Ecclestone et al, Juvéderm Volbella has been revealed to be safe when used for
lip augmentation as intended. There were 34 subjects with 72 adverse events related to the study
injection or device, and the most frequent was injection site bruising (51.7%, 31/60 subjects).
Injection site swelling and lumps each occurred at much lower rates (8.3%, 5/60 subjects), and
all other adverse events occurred in less than 4% of subjects. Three-quarters of the events
(75.0%) were mild, and the remainder (25.0%) were of moderate severity. Two-thirds of the
events (66.7%) resolved within 1 week, and the vast majority resolved without sequelae
(98.6%) and did not require treatment (97.2%). One event of an injection site mass (lump) was
ongoing. There were no severe or serious events related to treatment (Eccleston and Murphy
2012).
Artzi et al reported on a cohort of 400 patients (360 women, average age 49.6 years) who
received Juvéderm Volbella in the tear through area and lips. All patients were injected with
additional HA-based products into other facial areas. The average number of different products
injected to the same patient, in two consecutive sessions, was 2.6. The average amount of fillers
_____________________________________________________________________________
34/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
injected to the same patient in two consecutive sessions was 3.2 mL. The interval between two
sessions ranged from 6 weeks to 6 months. To follow-up the patients after treatment, data were
collected from patient charts and through phone call interviews. Of 400 patients, 17 (4.25%)
developed a cutaneous reaction to the examined filler. In addition to Juvéderm Volbella, 8 of 17
patients (47%) were treated with 1 additional product, 4 (23%) were treated with 2 additional
products, and 5 (29%)with 3 additional products. The cutaneous reaction was observed 8.41
weeks after the injection of Juvéderm Volbella (range: 5–12) and initially manifested with
purplish to brownish discoloration of the skin surrounding the injection site. All affected
individuals were first treated with oral ciprofloxacin for a period of 3 to 4 weeks. In 6 of these
patients, all symptoms and signs receded and did not recur. The 11 remaining patients
developed recurrent episodes of inflammatory reactions. Three patients had only 1 recurrence, 2
patients had 2 recurrences, 2 patients had 3 recurrences, 1 patient had 4 recurrences, 1 patient
had 5 recurrences, and 2 patients had 8 recurrences. Relapses were not always seen at the initial
reaction site. They resolved and recurred in different facial areas, where otherHAfillerswere
previously injected. During analysis of the data, a strong positive association was found
between the number of products injected and the time of full resolution. Furthermore, the total
volume of injected material also correlated with time until resolution. When more than 1 mL of
filler was injected during a session, the median time until resolution was 4.75 months when
compared with 1.5 months, when only 1 mL was injected. The incidence of late-onset adverse
reaction in this study was higher than reported in other studies (Artzi, Loizides et al. 2016). The
reasons are unclear. Importantly, this study revealed that late-onset adverse reactions are of less
severity and duration if the amount of injected HA material is below 1 mL. Thus, for use of
dermal fillers in the facial area, it should be attempted to decrease the amount of injected
material as far as possible.
6.4. Risk analysis
A comprehensive risk analysis for the products under discussion has been performed. Thereby,
potential risks have been addressed and discussed. In the risk analysis, hazards and their clinical
consequences have been characterised according to the putative harm for patients and
probability of occurrence. Risk-diminishing measures have been taken. For more detailed
information, reference is made to the risk management file, which is part of the technical
documentation. From a technical, biological, and clinical point of view, the residual risk for
clinical use of CRM Gel, CRM Dur, GeneFill Soft Touch, and Hyacorp Lips is tolerable after
implementation of risk-minimising measures. There are no inacceptable risks associated with
CRM Gel, CRM Dur, GeneFill Soft Touch, and Hyacorp Lips.
_____________________________________________________________________________
35/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
7. Post-marked data
8. Conclusion
Procedures for facial volume replacement become more and more predominant during the last
two decades.
Cross-linked hyaluronic acid products offer several distinct advantages over permanent filler.
Because HA oocurrs naturally in the human body, its biocompatibility is excellent. Multiple
clinical records confirm the high overall safety profile of BDDE-cross-linked HA fillers. One
great advantage is the possibility to reverse the effects either by hyaluronidase injection or by
removing the HA from the implant site through aspiration. Furthermore, its administration is
minimally-invasive and its performance is well-established for decades.
CRM Gel, CRM Dur, GeneFill Soft Touch, and Hyacorp Lips are regarded to be equivalent to
the currently used and well established products Restylane, Juvéderm Ultra, Juvéderm Ultra
Plus, and Juvéderm Volbella from a technical, biological, and clinical point of view. Therefore
the scientific literature discussing these products was analysed. Restylane, Juvéderm Ultra,
Juvéderm Ultra Plus, and Juvéderm Volbella were investigated in several prospective studies
and case studies. The trials were performed during 2003 to 2014. The performance of of these
products can be assessed as appropriate leading to high satisfaction in patients and physicians.
In summary, performance of Restylane, Juvéderm Ultra, Juvéderm Ultra Plus, and Juvéderm
Volbella has been proven. According to MEDDEV 2.7/1 rev3 and based on the principle of
equivalence, performance of CRM Gel, CRM Dur, GeneFill Soft Touch, and Hyacorp Lips can
be regarded as demonstrated.
Articles related to the safety of hyaluronic acid in general, and especially to the Juvéderm
Volbella and Restylane report only a very low rate of side effects and complications. No
unexpected side effects, complication, or incidents related to these products were reported.
Based on the data provided there are no concerns related to the safety of these products.
Performance and safety of hyaluronic acid have been well supported by additional review
articles issued during the last years.
Product Certified since Units sold in
EU
(until July
2014)
Units sold
outside EU
Serious
adverse events
or incidents
reported
CRM Gel 2003 34614 28232 -
CRM Dur 2003 14052 13134 -
GeneFill Soft
Touch
2009 444 1771 -
Hyacorp Lips 2009 18466 17565 -
_____________________________________________________________________________
36/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
The post market surveillance of CRM Gel, CRM Dur, GeneFill Soft Touch, and Hyacorp Lips
reflect their status of safety reported in scientific literature for the equivalent products
Restylane, Juvéderm Ultra, Juvéderm Ultra Plus, and Juvéderm Volbella. No harm to patients
has been reported during the last years.
In summary hyaluronic acid as filling agent provides a suitable performance and a high safety
in patients. CRM Gel, CRM Dur, GeneFill Soft Touch, and Hyacorp Lips are equivalent to the
well established products Restylane, Juvéderm Ultra, Juvéderm Ultra Plus, and Juvéderm
Volbella. Performance and safety can be demonstrated by these products and by post-market
data on the products under discussion. The benefit-to-risk ratio for clinical use of the products
under discussion within their indications is considered to be positive.
Compiled by Reviewed and approved by
i.DRAS GmbH, 2016-03-10 BioScience GmbH, 2016-03-10
Dr. med. Christian Schübel Kirsten Krollmann
Head Clinical Affairs Product Management
9. References
Andre, P., N. J. Lowe, A. Parc, T. H. Clerici and U. Zimmermann (2005). "Adverse reactions to
dermal fillers: a review of European experiences." J Cosmet Laser Ther 7(3-4): 171-176.
Artzi, O., C. Loizides, I. Verner and M. Landau (2016). "Resistant and Recurrent Late Reaction
to Hyaluronic Acid-Based Gel." Dermatol Surg 42(1): 31-37.
Baumann, L. S., A. T. Shamban, M. P. Lupo, G. D. Monheit, J. A. Thomas, D. K. Murphy, P. S.
Walker and J. v. Z. N. F. S. Group (2007). "Comparison of smooth-gel hyaluronic acid dermal
fillers with cross-linked bovine collagen: a multicenter, double-masked, randomized, within-
subject study." Dermatol Surg 33 Suppl 2: S128-135.
Beasley, K. L., M. A. Weiss and R. A. Weiss (2009). "Hyaluronic acid fillers: a comprehensive
review." Facial Plast Surg 25(2): 86-94.
Bogdan Allemann, I. and L. Baumann (2008). "Hyaluronic acid gel (Juvederm) preparations in
the treatment of facial wrinkles and folds." Clin Interv Aging 3(4): 629-634.
Brandt, F., B. Bassichis, M. Bassichis, C. O'Connell and X. Lin (2011). "Safety and
effectiveness of small and large gel-particle hyaluronic acid in the correction of perioral
wrinkles." J Drugs Dermatol 10(9): 982-987.
_____________________________________________________________________________
37/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
De Boulle, K., R. Glogau, T. Kono, M. Nathan, A. Tezel, J. X. Roca-Martinez, S. Paliwal and
D. Stroumpoulis (2013). "A Review of the Metabolism of 1,4-Butanediol Diglycidyl Ether-
Crosslinked Hyaluronic Acid Dermal Fillers." Dermatol Surg.
Eccleston, D. and D. K. Murphy (2012). "Juvederm((R)) Volbella in the perioral area: a 12-
month prospective, multicenter, open-label study." Clin Cosmet Investig Dermatol 5: 167-172.
Funt, D. and T. Pavicic (2015). "Dermal fillers in aesthetics: an overview of adverse events and
treatment approaches." Plast Surg Nurs 35(1): 13-32.
Gilbert, E., A. Hui, S. Meehan and H. A. Waldorf (2012). "The basic science of dermal fillers:
past and present Part II: adverse effects." J Drugs Dermatol 11(9): 1069-1077.
Gilbert, E., A. Hui and H. A. Waldorf (2012). "The basic science of dermal fillers: past and
present Part I: background and mechanisms of action." J Drugs Dermatol 11(9): 1059-1068.
Glogau, R. G., D. Bank, F. Brandt, S. E. Cox, L. Donofrio, J. Dover, S. Grekin, I. Lawrence, X.
Lin, M. Nestor, A. Shamban, D. Stewart, R. Weiss, R. A. Axford-Gatley, M. J. Theisen and S.
Smith (2012). "A randomized, evaluator-blinded, controlled study of the effectiveness and
safety of small gel particle hyaluronic acid for lip augmentation." Dermatol Surg 38(7 Pt 2):
1180-1192.
Gold, M. (2009). "The science and art of hyaluronic acid dermal filler use in esthetic
applications." J Cosmet Dermatol 8(4): 301-307.
Hirsch, R. J. and M. Stier (2008). "Complications of soft tissue augmentation." J Drugs
Dermatol 7(9): 841-845.
Kablik, J., G. D. Monheit, L. Yu, G. Chang and J. Gershkovich (2009). "Comparative physical
properties of hyaluronic acid dermal fillers." Dermatol Surg 35 Suppl 1: 302-312.
Kim, J. E. and J. M. Sykes (2011). "Hyaluronic acid fillers: history and overview." Facial Plast
Surg 27(6): 523-528.
Lupo, M. P. (2006). "Hyaluronic acid fillers in facial rejuvenation." Semin Cutan Med Surg
25(3): 122-126.
Lupo, M. P., S. R. Smith, J. A. Thomas, D. K. Murphy and F. C. Beddingfield, 3rd (2008).
"Effectiveness of Juvederm Ultra Plus dermal filler in the treatment of severe nasolabial folds."
Plast Reconstr Surg 121(1): 289-297.
Matarasso, S. L., J. D. Carruthers, M. L. Jewell and G. Restylane Consensus (2006).
"Consensus recommendations for soft-tissue augmentation with nonanimal stabilized
hyaluronic acid (Restylane)." Plast Reconstr Surg 117(3 Suppl): 3S-34S; discussion 35S-43S.
Morris, C. L., S. S. Stinnett and J. A. Woodward (2008). "Patient-preferred sites of restylane
injection in periocular and facial soft-tissue augmentation." Ophthal Plast Reconstr Surg 24(2):
117-121.
Narins, R. S., F. Brandt, J. Leyden, Z. P. Lorenc, M. Rubin and S. Smith (2003). "A
randomized, double-blind, multicenter comparison of the efficacy and tolerability of Restylane
versus Zyplast for the correction of nasolabial folds." Dermatol Surg 29(6): 588-595.
_____________________________________________________________________________
38/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
Newman, J. (2009). "Review of soft tissue augmentation in the face." Clin Cosmet Investig
Dermatol 2: 141-150.
Philipp-Dormston, W. G., S. Hilton and M. Nathan (2014). "A prospective, open-label,
multicenter, observational, postmarket study of the use of a 15 mg/mL hyaluronic acid dermal
filler in the lips." J Cosmet Dermatol 13(2): 125-134.
Pinsky, M. A., J. A. Thomas, D. K. Murphy, P. S. Walker and G. Juvederm vs. Zyplast
Nasolabial Fold Study (2008). "Juvederm injectable gel: a multicenter, double-blind,
randomized study of safety and effectiveness." Aesthet Surg J 28(1): 17-23.
Price, R. D., M. G. Berry and H. A. Navsaria (2007). "Hyaluronic acid: the scientific and
clinical evidence." J Plast Reconstr Aesthet Surg 60(10): 1110-1119.
Rohrich, R. J. and A. Ghavami (2007). "The role of hyaluronic acid fillers (Restylane) in facial
cosmetic surgery: review and technical considerations." Plast Reconstr Surg 120(6 suppl): 41S-
54S.
Schweiger, E. S., C. C. Riddle, V. Tonkovic-Capin and D. J. Aires (2008). "Successful
treatment with injected hyaluronic acid in a patient with lip asymmetry after surgical correction
of cleft lip." Dermatol Surg 34(5): 717-719.
Smith, K. C. (2008). "Reversible vs. nonreversible fillers in facial aesthetics: concerns and
considerations." Dermatol Online J 14(8): 3.
Smith, S. R., D. Jones, J. A. Thomas, D. K. Murphy and F. C. Beddingfield, 3rd (2010).
"Duration of wrinkle correction following repeat treatment with Juvederm hyaluronic acid
fillers." Arch Dermatol Res 302(10): 757-762.
Solish, N. and A. Swift (2011). "An open-label, pilot study to assess the effectiveness and
safety of hyaluronic acid gel in the restoration of soft tissue fullness of the lips." J Drugs
Dermatol 10(2): 145-149.
Sundaram, H., B. Voigts, K. Beer and M. Meland (2010). "Comparison of the rheological
properties of viscosity and elasticity in two categories of soft tissue fillers: calcium
hydroxylapatite and hyaluronic acid." Dermatol Surg 36 Suppl 3: 1859-1865.
Tezel, A. and G. H. Fredrickson (2008). "The science of hyaluronic acid dermal fillers." J
Cosmet Laser Ther 10(1): 35-42.
Winslow, C. P. (2009). "The management of dermal filler complications." Facial Plast Surg
25(2): 124-128.
Wu, Y., N. Sun, Y. Xu, H. Liu, S. Zhong, L. Chen and D. Li (2016). "Clinical comparison
between two hyaluronic acid-derived fillers in the treatment of nasolabial folds in Chinese
subjects: BioHyalux versus Restylane." Arch Dermatol Res.
_____________________________________________________________________________
39/40

Clinical Evaluation
Dermal Filler 16/2
CRM Gel/CRM Dur/GeneFill Soft Touch/
Hyacorp Lips
Version 3.0
10. Attachments
Attachment 1 - Literature Search and Outcome
Attachment 2 – Equivalence Analysis
_____________________________________________________________________________
40/40
Related Documents











