145 British Journal of Clinical Psychology (2011), 50, 145–163 C 2010 The British Psychological Society The British Psychological Society www.wileyonlinelibrary.com Clinical correlates of olfactory hallucinations in schizophrenia Robyn Langdon 1, 2,3 ∗ , Jonathan McGuire 1 , Richard Stevenson 4 and Stanley V. Catts 5 1 Macquarie Centre for Cognitive Science, Macquarie University, Sydney, New South Wales, Australia 2 Schizophrenia Research Institute, Sydney, New South Wales, Australia 3 School of Psychiatry, University of New South Wales, Sydney, Australia 4 Psychology Department, Macquarie University, Sydney, New South Wales, Australia 5 Royal Brisbane Hospital, Brisbane, Queensland, Australia Objectives. Olfactory hallucinations (OHs) are underrepresented in conventional clinical instruments, infrequently researched, and poorly understood. To advance understanding of OHs, we examined their past-month prevalence and co-occurring symptoms in two datasets. Design. One dataset comprised categorical codes and was examined using homo- geneity analysis and logistic regression; the other dataset comprised numeric ratings and was examined using principal components analyses and linear regression. Method. The two datasets included: (1) 962 cases with Present State Examination – 9th Edition (PSE-9), codes (recoded present/absent) from the World Health Organiza- tion 10 Country (WHO-10) Study and (2) 265 cases with ratings on Scales for Assessing Positive/Negative Symptoms of Schizophrenia (SAPS/SANS). Two PSE-9 items (external- and self-smells) were recoded into a single OH item to examine consistency with the SAPS/SANS dataset, which contained a single OH item. Results. Prevalence of OHs and hallucinations in other modalities differed according to the WHO-10 international centre. Across centres, OHs were present in 13% of the WHO-10 dataset, similar to the 17% prevalence rate in the SAPS/SANS dataset. Refer- ential/control delusions and other hallucinations (particularly, somatic/tactile/gustatory hallucinations) were significant independent correlates of OHs in both datasets. OHs also co-occurred with social anxiety and depression in the WHO-10 dataset, with self-smells being particularly associated with self-depreciation. ∗ Correspondence should be addressed to A/Professor Robyn Langdon, Macquarie Centre for Cognitive Science, Macquarie University, Sydney, NSW 2109, Australia (e-mail: [email protected]). DOI:10.1348/014466510X500837

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

145
British Journal of Clinical Psychology (2011), 50, 145–163C© 2010 The British Psychological Society
TheBritishPsychologicalSociety
www.wileyonlinelibrary.com
Clinical correlates of olfactory hallucinationsin schizophrenia
Robyn Langdon1,2,3∗, Jonathan McGuire1, Richard Stevenson4
and Stanley V. Catts5
1Macquarie Centre for Cognitive Science, Macquarie University, Sydney,New South Wales, Australia
2Schizophrenia Research Institute, Sydney, New South Wales, Australia3School of Psychiatry, University of New South Wales, Sydney, Australia4Psychology Department, Macquarie University, Sydney, New South Wales,Australia
5Royal Brisbane Hospital, Brisbane, Queensland, Australia
Objectives. Olfactory hallucinations (OHs) are underrepresented in conventionalclinical instruments, infrequently researched, and poorly understood. To advanceunderstanding of OHs, we examined their past-month prevalence and co-occurringsymptoms in two datasets.
Design. One dataset comprised categorical codes and was examined using homo-geneity analysis and logistic regression; the other dataset comprised numeric ratingsand was examined using principal components analyses and linear regression.
Method. The two datasets included: (1) 962 cases with Present State Examination –9th Edition (PSE-9), codes (recoded present/absent) from the World Health Organiza-tion 10 Country (WHO-10) Study and (2) 265 cases with ratings on Scales for AssessingPositive/Negative Symptoms of Schizophrenia (SAPS/SANS). Two PSE-9 items (external-and self-smells) were recoded into a single OH item to examine consistency with theSAPS/SANS dataset, which contained a single OH item.
Results. Prevalence of OHs and hallucinations in other modalities differed accordingto the WHO-10 international centre. Across centres, OHs were present in 13% of theWHO-10 dataset, similar to the 17% prevalence rate in the SAPS/SANS dataset. Refer-ential/control delusions and other hallucinations (particularly, somatic/tactile/gustatoryhallucinations) were significant independent correlates of OHs in both datasets. OHsalso co-occurred with social anxiety and depression in the WHO-10 dataset, withself-smells being particularly associated with self-depreciation.
∗Correspondence should be addressed to A/Professor Robyn Langdon, Macquarie Centre for Cognitive Science, MacquarieUniversity, Sydney, NSW 2109, Australia (e-mail: [email protected]).
DOI:10.1348/014466510X500837

146 Robyn Langdon et al.
Conclusions. Sociocultural factors may modulate the self-reporting and/or detectionof OHs and hallucinations in other modalities. Referential/control delusions promotethe generation and/or maintenance of OHs independent of factors shared with otherhallucinations. OHs and hallucinations of taste, touch, and bodily sensation frequentlyco-occur. Self-smells warrant sensitive probing.
Hallucinations are characteristic of schizophrenia and occur in all modalities. Baethgeet al. (2005) recently examined the past-week prevalence of hallucinations in 4,972hospitalized psychiatric patients and found that hallucinations were most common inthe patients with schizophrenia compared to other psychiatric disorders. Sixty-eightper cent of the schizophrenia patients were hallucinating, as compared to 11–23% ofthe bipolar patients (depending upon the nature of the mood disorder) and 6% of thedepressed patients. Hallucinations were also more severe and less treatment responsivein the schizophrenia patients. Within the hallucinating schizophrenia patients, auditory–verbal hallucinations were the most common, being experienced by 75%, with somatichallucinations the second most common, present in 37%. Visual and olfactory/gustatoryhallucinations were least common, present in only 14 and 18%, respectively. Prevalencerates vary, however, depending upon the sample (e.g., in-patient vs. out-patient andcultural group: Ndetei & Vadher, 1984; Thomas et al., 2007), rating period (e.g., lifetimevs. current) and grouping of modalities, with visual, rather than somatic, hallucinationstypically reported to be the second most common in schizophrenia. Across severalstudies, auditory hallucinations have been estimated in 47–98%, visual hallucinations in14–69%, and other modalities (including somatic, olfactory, and gustatory) in 4–25% ofschizophrenia patients (Bracha, Wolkowitz, Lohr, Karson, & Bigelow, 1989; Goldberg,Klerman, & Cole, 1965; Mueser, Bellack, & Brady, 1990; Murphy, Wittkower, Fried, &Ellenberger, 1963; Ndetei & Vadher, 1984; Suhail & Cochrane, 2002; Thomas et al., 2007;Zarroug, 1975). This study focuses on olfactory hallucinations (OHs: hallucinations ofsmell) for a number of reasons.
OHs are currently underrepresented in conventional clinical instruments, resultingin a general gap in knowledge concerning OHs. Many symptom-rating scales (e.g., thewidely used Positive and Negative Syndrome Scale, PANSS; Kay et al., 1991), rateall hallucinations on a single item; thus, once hallucinations of any modality havebeen identified, typically the more common, auditory hallucinations, further probingof other modalities might not occur. Likewise, in many diagnostic instruments (e.g.,the Structured Clinical Interview for DSM Disorders, SCID; Spitzer, Williams, Gibbon, &First, 1992), auditory and visual hallucinations will be specifically probed, while OHs willbe grouped together with somatic, tactile, or gustatory hallucinations. In 1961, Rubert,Hollender, and Mehrhof cautioned that the presumed rarity of OHs is more apparent thanreal, due in part to the fact that most psychiatrists do not inquire about such experiences.When Rubert and colleagues specifically asked their schizophrenia patients about OHs,they found that 19/24 (79%) unselected, and 11/12 chronic hallucinating (92%), patientsreported experiences of this type. Goodwin and Alderson (1971) similarly reported thatthe apparent prevalence of OHs increases when patients are explicitly asked about theirsmell experiences. In more recent systematic studies, OHs have been reported in upto 35% of patients with schizophrenia, depending upon the sample, rating period, andinstrument (see Table 1)
While OHs in schizophrenia have been conceived traditionally as subordinate to otherhallucinations with regard to their clinical significance (Meats, 1988), these symptoms

Olfactory hallucinations 147
Tabl
e1.
Rec
ent
stud
ies
whi
chre
port
spec
ific
prev
alen
cera
tes
for
OH
sin
psyc
hotic
sam
ples
(gro
uped
bylif
etim
eor
curr
ent-
ratin
gpe
riod
)

148 Robyn Langdon et al.
may be more important than has previously been thought (Mohr, Hubener, & Laska,2002). Phenomenological reports emphasize the negative nature of OHs, with theodours typically described as foul and unpleasant (Meats, 1988), intrusive and distressing(Kopala, Good, & Honer, 1994). OHs might also be indicative of poorer prognosis andmore severe psychopathology (see, e.g., Brill, 1932; Kwapil, Chapman, Chapman, &Miller, 1996; Mohr et al., 2002; Sakel, 1958, for discussion). In support of this latter vieware the findings that premorbid OHs predict later development of schizophrenia andpoorer global adjustment and social position (Kwapil et al., 1996). ‘Other’ hallucinations,which typically include somatic, tactile or gustatory, as well as olfactory, hallucinations,also associate with an earlier age-of-onset (Lewandowski, DePaola, Camsari, Cohen, &Ongur, 2009), which is considered to be indicative of increased illness severity (see,e.g., Brill, 1932; Delisi, 1992; Sakel, 1958). Patients with OHs also lack insight into thesesymptoms (Kopala et al., 1994), and lack of insight is another marker of more severepsychopathology (Carpenter, Straus, & Bartko, 1973) due, in part, to the subsequentinterference with treatment compliance.
OHs might also be informative with regard to current theories of hallucinations inother modalities. There is certainly no evidence that OHs are specifically related tothe olfactory identification deficits that are common in schizophrenia (Hudry, Saoud,d’Amato, Dalery, & Royet, 2002; Moberg et al., 1999). These deficits have been foundto identify ‘ultra-high risk’ young people, who go on to develop schizophrenia, ratherthan other forms of psychosis (Brewer et al., 2003), and first-episode patients, whodevelop a more persistent negative/disorganized (or ‘cognitive deficit’) form of illness(Good, Whitehorn, Rui, Milliken, & Kopala, 2006); however, there is no evidence thatthey associate with OHs (Kopala et al., 1994; Stedman & Clair, 1998). Indeed, whileolfactory identification is generally worse in male compared to female patients, it isfemale patients who are more likely to experience OHs (Kopala et al., 1994; Ndetei &Singh, 1983).
OHs and non-OHs often co-occur suggesting that shared neurobiological/cognitiveprocesses may contribute to the generation of all hallucinations (e.g., John, Khanna,Thennarasu, & Reddy, 2003); however, the extent to which general theories apply toOHs is uncertain. While there is some consensus that metacognitive beliefs, pre-existingschemas, cognitive biases, negative affect, and avoidant safety behaviours contributeto the generation and maintenance of all hallucinations, irrespective of modality, inresponse to intrusive experiences (Bentall, 1990; Campbell & Morrison, 2007; Garety,Kuipers, Fowler, Freeman, & Bebbington, 2001; Lobban, Haddock, Kinderman, &Wells, 2002; Morrison, 2001; Smith et al., 2006), the specific processes by whicholfactory intrusions are generated remain unspecified. Some researchers propose thathallucinations stem from a failure to discriminate imaginings from perceivings (e.g.,Bentall, 1990); however, olfactory imagery is difficult to generate and typically vagueand fleeting, which is at odds with patient reports of vivid, intense OHs. There is also noevidence that olfactory hallucinators have greater olfactory imaging ability (see Stevenson& Case, 2005, for a review). Other researchers propose that hallucinations begin asintrusive, involuntary memories, which are mis-sourced to external reality (Waters,Badcock, Michie, & Maybery, 2006); however, this account seems incompatible withpatient reports of smelling ‘angels’ or ‘aliens’, although OHs of this type may reflectmisinterpretations or elaborations of involuntary, vague olfactory memories, consistentwith the view that affect biases access to, and interpretations of, smell experiences(Ohanyon, 2000). Nevertheless, odour identification ability is not inversely related to thepresence of OHs (Kopala et al., 1994), as might be expected on such an account. Finally,

Olfactory hallucinations 149
the prominent theory that auditory–verbal hallucinations stem from a failure to monitorthe self-generated source of internal ‘self-talk’ (see Seal, Aleman, & McGuire, 2004, for areview) is hardly applicable to OHs.
Against this background, we sought to advance understanding of OHs by examiningtheir prevalence and co-occurring symptoms in two pre-existing datasets, each ofwhich contained unique items for OHs. One dataset came from the World HealthOrganization 10 Country (WHO-10) Study (Jablensky et al., 1992) and focused on first-time clinical presentations. The second dataset came from a series of independent studiesof Australian patients with established schizophrenic illness. If results proved to beconsistent across two such distinct datasets, this would help attest to the reliabilityof findings.
Work, thus far, on clinical and other correlates of OHs is limited. OHs have beenfound to associate with alcohol/drug use, anxiety, depression, organic pathology, andshort sleep duration in the general population (Ohanyon, 2000) and with depressedmood and a subjective change in the sense of smell in schizophrenia (Stedman &Clair, 1998). When OHs have been combined with somatic, tactile, or gustatoryhallucinations, these ‘other’ hallucinations have been found to associate with a historyof depression, family history of mood disorders, and somatic or control delusions(Lewandowski et al., 2009). Mueser et al. (1990) have also found that tactile hallu-cinations co-occur with olfactory and/or gustatory hallucinations, while Meats (1988)suggested that delusional elaborations are particularly common when OHs are present,consistent with Baethge et al.’s (2005) finding that 95.7% of their schizophreniapatients with OHs were delusional, as compared to 83.3% of those with visualhallucinations.
Factor-analytic studies are another potential source of information concerning clinicalcorrelates of OHs. Relevant findings are limited, however. This is because earlier factor-analytic studies focused on global ratings (e.g., for delusions, hallucinations, thoughtdisorder), initially suggesting a two-factor (positive, negative) solution, although a three-factor solution (reality distortion, negative symptoms, disorganization) is generally moreaccepted today (see Blanchard & Cohen, 2006, for a review). More recently, there hasbeen a shift to finer-grained item-based analyses; however, more than 17 studies of thistype have used the PANSS to report a five-factor solution (negative, positive, activation,dysphoric mood, autistic preoccupation: see Emsley, Rabinowitz, & Torreman, 2003, fora review) and, as noted earlier, the PANSS includes a single non-specific hallucinationitem. Other studies, which have included other hallucinations (olfactory, tactile, orgustatory), report mixed results. Peralta and Cuesta (2007) examined current-episodeand lifetime ratings in 660 Spanish in-patients with DSM-IV schizophrenia or related psy-choses. They used the Manual for Assessment and Documentation in Psychopathology
(Guy & Ban, 1982) and reported common factors for current-episode and lifetime ratings,with other hallucinations loading onto a ‘hallucinations/first-rank delusions’ factor.Cardno et al. (1996) used the OPCRIT checklist (McGuffin, Farmer, & Harvey, 1991)with 102 British patients with DSM-III-R schizophrenia and similarly found that otherhallucinations loaded onto a ‘voices and loss-of-boundary delusions’ factor. However,Cardno et al. (1997) used the OPCRIT checklist with 66 British schizophrenia patientsand found, instead, that other hallucinations loaded onto a single-item factor. When theScales for Assessing Positive/Negative Symptoms of Schizophrenia (SAPS/SANS) havebeen used in previous factor-analytic studies, the OH item is often excluded due to lowprevalence rates (see, e.g., Minas et al., 1992; Peralta & Cuesta, 1998; Stuart, Malone,Currie, Klimidis, & Minas, 1995).

150 Robyn Langdon et al.
Three recent factor-analytic studies are of most relevance; each of these studiesincluded a specific OH item and used principal components analysis (PCA). Johnet al. (2003) ran separate PCAs for SAPS and SANS current-episode item ratings for43 neuroleptic naive, recent-onset DSM-IV schizophrenia patients from South India.They reported a five-factor solution for the SAPS, with OHs loading onto the samefactor as auditory and visual hallucinations, as well as delusions with persecutory,referential and somatic themes. In contrast, Arajarvi et al. (2006) examined greatestlifetime SAPS/SANS ratings in a nationwide Finnish sample with established DSM-IV schizophrenia. They reported that OHs loaded no higher than .25 on any factor(this factor included auditory, visual, and somatic hallucinations and persecutory,referential and loss-of-boundary/control delusions). Most recently, McGrath et al. (2009)have examined lifetime ratings (coded present/absent) on the Diagnostic Interviewfor Genetic Studies (DIGS: Nurnberger et al., 1994) for 1,119 patients with DSM-III-R/DSM-IV schizophrenia or schizoaffective disorder. These patients had taken partin studies (1988–2006) for the Epidemiology-Genetics Programme, Johns HopkinsUniversity, Maryland. McGrath and colleagues reported a nine-factor solution withOHs loading onto two factors: (1) an ‘hallucinations’ factor, including auditory, visual,tactile, and OHs, along with catatonia (with OHs having the lowest loading for thehallucinations items, at .33) and (2) a ‘schneiderian first-rank symptoms’ factor, includinghallucinations – somatic (.56), olfactory (.36), and tactile (.35) – along with delusionsof thought insertion, influence, thought withdrawal, thought broadcasting, referenceand guilt, as well as thought echo, primary delusions, and delusional perception(with the loadings ranging from .35 for delusional perception to .67 for thoughtinsertion).
Aims and hypothesesThis study aimed to firstly compare the past-month prevalence of OHs in two distinctclinical samples, one recent-onset, and the other more chronic. Secondly, we aimedto examine clinical correlates of OHs across the two datasets, each of which derivedfrom a different clinical instrument, and each of which contains unique OH items.In accord with previous suggestions that OHs indicate more severe psychopathology(e.g., Brill, 1932; Kwapil et al., 1996; Lewandowski et al., 2009; Sakel, 1958), weexpected OHs to associate with an earlier age-of-onset and more severe negativesymptoms. Given the previous findings of relations between OHs and negative mood(Stedman & Clair, 1998), as well as negative appraisals (Campbell & Morrison, 2007;Garety et al., 2001; Meats, 1988; Morrison, 2001), we also expected OHs to asso-ciate with depression and/or anxiety, particularly in the WHO-10 dataset. Finally,in light of the previous factor-analytic results, we hypothesized that OHs wouldassociate with hallucinations in other modalities, and also delusions, particularly, controldelusions.
Our approach was twofold. Firstly, we used scaling/data reduction techniques oneach dataset, and including the OH item, to identify those symptoms which co-occurwith OHs; in this way, we could examine consistency between our own results andthose of previous studies which have used similar techniques. Secondly, we aimedto extend this line of research by using logistic and linear regression techniques toidentify the best significant independent predictors of OHs. In this way, we hoped togain insights concerning the putative independent factors which might promote thegeneration and/or maintenance of specifically OHs.

Olfactory hallucinations 151
MethodDataset 1The first dataset comprised 962 cases with valid OH ratings from the WHO-10 Study(Jablensky et al., 1992). The data came from centres in Denmark, India, Colombia,Ireland, Nigeria, Japan, the USA, the UK, and Czechoslovakia. Inclusion criteria includedpresence, in the past 12 months, of overt psychotic symptoms and a first-in-lifetimecontact with a ‘helping agency’ in the past 3 months. Exclusion criteria includedorganic cerebral disorder evident (e.g., in either delirium or dementia resulting fromCNS disease/damage or substance abuse). There were 531 males and 431 females, withages ranging from 15 to 54 years and a mean time in psychosis of 31.5 months (SD =35.0).
The PSE-9 was used to assess symptoms over the preceding month. PSE-9 item 68(‘Do you sometimes notice strange smells that other people don’t notice?’) specificallyexcludes self-smells. The item is coded ‘0’ if absent, ‘1’ if there are simple olfactorysmells without delusional elaboration, and ‘2’ if delusional elaboration is present. PSE-9item 69 (‘Do you seem to think that you yourself give off a smell which is noticed?’)targets self-smells. The item is coded ‘0’ if absent, ‘1’ if the patient thinks s/he gives offa smell but is not sure that others have noticed it, and ‘2’ if the patient believes thats/he gives off a smell and that others have noticed it and acts accordingly. Responsesto item 69 are ambiguous as to whether the respondent actually experiences the smellor merely believes that others can smell him/her. However, since one of our aims wasto seek consistency across the PSE-9 and SAPS/SANS datasets, the PSE-9 items 68 and69 were recoded into a single item representing the presence/absence of any reportedsmell. The other PSE-9 items, which comprise a mix of ordinal and categorical codes,were similarly recoded into presence/absence.
Firstly, homogeneity analysis (HOMALS) was used to identify those PSE-9 items whichco-occur with OHs when discriminating between cases. HOMALS is recommendedin preference to PCA when the variables are ordinal or nominal. In accord withrecommended practice (Muelman & Heiser, 1999), we first selected two dimensions andthen explored whether three dimensions might offer better discrimination. Secondly,logistic regression analyses were used to identify the best significant, independentpredictors of presence/absence of OHs. In accord with common practice, we excludedpoorly endorsed items. As per Liddle (1987), PSE-9 items present in fewer than 10% ofcases were excluded. A higher cut-off (e.g., 15%) would have excluded too many PSE-9items, some of which were likely to be of particular interest (e.g., other hallucinations –i.e., somatic/tactile/gustatory). Backwards reduction was used with exclusion set at .05(for the likelihood-ratio statistic). Backwards reduction is recommended for exploratoryanalyses since it minimizes the error term; however, since this is not the mostconservative method, we also followed up these analyses using the more conservative,forward-entry method. Separate analyses were then conducted for external- and self-smells.
Dataset 2The second dataset comprised 265 cases with numeric ratings on the SAPS/SANScollected during clinical interviews conducted by R. L. and S. V. C. The patients werein-patients or out-patients of the Sydney East or Sydney South West Area Health Services(i.e., SEAHS or SSWAHS), or had been recruited via the Australian Schizophrenia ResearchBank (ASRB) Volunteer Register. The clinical interviews were conducted as part of an

152 Robyn Langdon et al.
in-house study of the clinical characteristics of patients with schizophrenia presentingfor treatment to the SEAHS and a series of independent studies of social cognitionin schizophrenia (Langdon, Coltheart, & Ward, 2006; Langdon, Coltheart, Ward, &Catts, 2001, 2002; Langdon, Corner, McLaren, Coltheart, & Ward, 2006). Diagnoseswere confirmed using either the SCID (First, Spitzer, Gibbon, & Williams, 1996) orthe Diagnostic Interview for Psychosis (Castle et al., 2006). There were 227 patientswith schizophrenia, 17 with schizophreniform disorder, and 21 with schizoaffectivedisorder. Exclusion criteria included history of head injury, CNS disease, and substanceabuse. There were 171 males and 94 females, with ages ranging from 15 to 60 years anda mean duration of illness of 13.2 years (SD = 9).
The SAPS/SANS, like the PSE-9, were used to rate symptoms over the precedingmonth. While the PSE-9 contains two OH items (external- and self-smells), the SAPScontains a single OH item, item 5 (‘Have you noticed unusual smells that other peopledon’t notice?’, ‘Do you ever notice that your own body has a smell even when you arequite clean?’). This item is scored for severity irrespective of presence or absence ofdelusional elaboration, with scores ranging from ‘0’ (absent) to ‘5’ (severe; i.e., ‘occursalmost daily’).
Similar to our approach with the WHO-10 dataset, we firstly used PCA with theindividual SAPS/SANS items (i.e., excluding global ratings: see Stuart, Pantelis, Klimidis, &Minas, 1999, for discussion of the importance of analysing individual items) to determinewhich items loaded onto the same factor(s) as OHs. While we chose PCA for this datareduction, results of data reduction are typically congruent regardless of the specificmethodology used (Peralta & Cuesta, 2001). As before, poorly endorsed items wereexcluded; in this case, 15% was a more natural cut-off. Five items were thus excluded:delusions of jealousy, thought withdrawal and guilt/sin, thought blocking, and clanging.Consistent with previous PCA studies, components with an eigenvalue greater than onewere considered, and Varimax rotation was used. A second PCA was then conducted,excluding the OH item, as well as the five items listed above, so that linear regressioncould then be employed using the extracted components to predict the severity of OHs.It was necessary to reduce the data in this way, prior to the regression analyses, since thiswas a much smaller dataset. Once again backwards reduction was used, with exclusionset at .05, and then followed up with the forward-entry method. We also used logisticregression with the same components to predict presence/absence of OHs. Scores of‘1’ on the SAPS indicate ‘questionable’. We classified ‘1’ as present in order to be asinclusive as possible and because the presence of mundane OHs (e.g., cooking smells)is often difficult to establish definitively, despite a strong suspicion. Thus, this measureof presence is less stringent than the PSE-9 measure.
ResultsPrevalence and basic demographicsPrevalence rates of OHs differed by WHO-10 international centre, � 2
9 = 79.40, p <
.0005 (see Table 2), as did the prevalence rates for the other modalities: auditory, � 29 =
162.1, p < .0005; visual, � 29 = 121.8, p < .0005; and ‘other’ (somatic/tactile/gustatory),
� 29 = 100.6, p < .0005, although not in the same way (e.g., OHs were less common
in Nigeria, while auditory and visual hallucinations were most common). The genderratio and the mean age-of-onset also differed by WHO-10 centre: � 2
9 = 32.69, p < .0005and Kruskal–Wallis � 2
9 = 71.65, p < .0005, respectively. So, we conducted additionallogistic regression analyses to fit centre, gender and age-of-onset when predicting the

Olfactory hallucinations 153
Table 2. Numbers (% in bracket) coded with hallucinations present according to modality and by centrein the 962 WHO-10 cases
presence/absence of hallucinations in each modality. In all cases, the effect of centreremained significant, with Wald’s F of 50.4, 125.7, 89.4, and 49.9 (for OHs, auditory,visual, and other hallucinations, respectively: all p values < .0005).
Table 3 shows the breakdown of prevalence rates for external- and self-smells, acrosscentre, in the WHO-10 dataset. OHs of smelling one’s own body were less common, beingexperienced by only 5%, with 11% experiencing external smells. The two types of OHswere inter-related; 48% of those who experienced self-smells also experienced externalsmells (vs. 9% of those without self-smells), Somer’s d = .39, p < .0005, and 20% of thosewho experienced external smells also experienced self-smells (vs. 3% of those withoutexternal smells), Somer’s d = .18, p < .0005. Table 3 also contrasts the prevalencerates across the WHO-10 and the SAPS/SANS datasets. Hallucinations (regardless ofmodality) were present in 64 and 57% of the datasets, respectively; this was a non-significant difference, � 2
1 = 1.91, p = .17. The relative prevalence of hallucinations indifferent modalities was also consistent across datasets; auditory hallucinations werethe most common (50–57%), followed by visual and somatic (or other), with OHspresent in a significant minority (13–17%). Prevalence rates for each modality werealso compared across datasets, with the exception of somatic versus other, since thesewere not equivalent. All differences were non-significant, including for OHs, althoughthese appeared slightly more common in the SAPS/SANS dataset, � 2
1 = 3.30, p = .07.
Table 3. Numbers (% in bracket) coded with hallucinations present according to modality across the962 WHO-10 cases and in the SAPS/SANS dataset

154 Robyn Langdon et al.
Females were more likely to experience OHs: 15% of females versus 11% of males inthe WHO-10 dataset, and 21% of females versus 11% of males in the SAPS/SANS dataset.However, these differences were not statistically significant: � 2
1 = 3.37, p = .07; and � 21 =
0.99, p = .32, respectively. Age-of-onset was later, rather than earlier, in those with OHsin the WHO-10 dataset: M = 29.1 years (SD = 12.8) for those with OHs versus M = 26.2years (SD = 10.3) for those without, Mann–Whitney Z = 2.87, p = .004. However, thisrelationship between age-of-onset and OHs was no longer significant when centre andage-of-onset were included in a logistic regression analysis to predict presence/absenceof OHs, Wald’s F = 1.48, p = .22. There was no evidence that age-of-onset differed forthose with OHs (M = 23.3 years, SD = 6.6) versus those without (M = 23.9 years, SD =7) in the SAPS/SANS dataset, Mann–Whitney Z = 0.45, p = .63.
WHO-10 datasetThe HOMALS analyses indicated that three dimensions offered no advantage over two.Items rated as present were clustered together in two main groups. OHs groupedclosest with ‘other’ hallucinations (i.e., somatic/tactile/gustatory: item 70) and delusionsconcerning paranormal phenomena (item 79) and mind control (item 81). Several otherPSE-9 items also appeared in the same quadrant as OHs, although not as close; theseincluded primary delusions (item 82), systematized delusions (item 93), autonomicanxiety due to delusions and/or hallucinations (item 13), and social impairment dueto psychotic condition (item 107).
The logistic regression results were in general accord with the HOMAL results (seeTable 4); other hallucinations and voices were significant independent predictors of OHs,as well as control and referential delusions. The logistic regression results also identifiedsomatic concerns, lack of self-confidence with other people, anxiety, depression, lackof insight, and, to a lesser degree, loss of interest in activities and slowed speech assignificant independent predictors of presence/absence of OHs in this dataset. Fewervariables were significant predictors when the more conservative forward-entry methodwas used.
When external- and self-smells were examined separately, each proved to be the bestpredictor of the other (along with delusional mood for external smells). These separateanalyses also indicated that somatic concerns (e.g., hypochodriasis), depression (e.g., asense of hopelessness), and social difficulties (e.g., social impairment due to psychoticillness) were associated more strongly with self-smells, while referential/control delu-sions and other (somatic/tactile/gustatory) hallucinations were associated more stronglywith external smells.
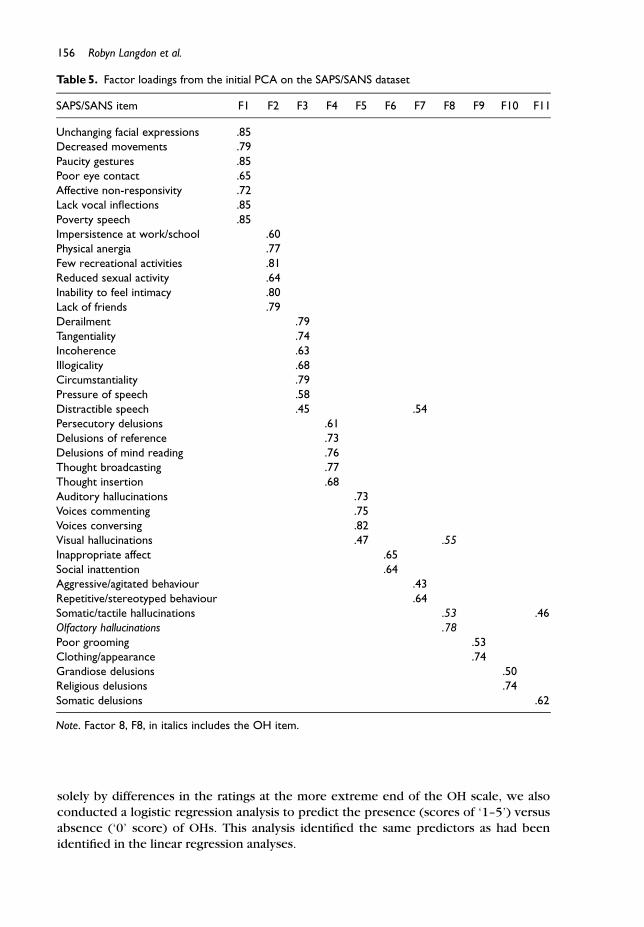
SAPS/SANS datasetThe initial PCA for individual SAPS/SANS items, including the OH item, and excludingpoorly endorsed items, indicated that the data was best characterized by 11 com-ponents (see Table 5, for a summary of loadings). These components comprised oftwo hallucinations factors – one primarily auditory and the other non-auditory (i.e.,somatic, olfactory, visual) – along with nine other factors: flat affect; apathy/anhedonia;referential/persecutory/control delusions; thought disorder; social inappropriateness;bizarre and disorganized behaviour; poor grooming and self-care; grandiose/spiritualdelusions; and somatic concerns (i.e., somatic delusions and somatic hallucinations). Thisnumber of components is not unusual when PCA has been conducted on all SAPS/SANS

Olfactory hallucinations 155
Table 4. Reduced model predicting presence/absence of OHs (external and/or self-smells) from therecoded PSE-9 ratings (WHO-10 dataset): Variables are ordered by size of Exp. �
ratings at the item level (see, e.g., Peralta & Cuesta, 2001; Stuart et al., 1999). OHs loadedonto the same factor as non-auditory, rather than auditory, hallucinations.
A second PCA was then conducted, prior to the linear regression, and now excludingthe OH item, as well as the poorly endorsed items excluded previously. This PCA pro-duced largely similar results, although the data were now best characterized by a 10-factorsolution: flat affect; apathy/anhedonia; thought disorder; referential/persecutory/controldelusions; grandiose/spiritual delusions; auditory and visual hallucinations (somatichallucinations now only loaded .40 onto this factor); social inappropriateness; bizarreand disorganized behaviour; poor grooming and self-care; and somatic concerns. Thelinear regression using these 10 components then revealed three significant independentpredictors of the OH severity rating, as summarized in Table 6: (1) referential, persecutoryand control delusions; (2) auditory and visual hallucinations; and (3) somatic concerns(i.e., somatic delusions and somatic hallucinations). The backward reduction and forwardentry methods identified the same predictors. To ensure that findings were not driven
156 Robyn Langdon et al.
Table 5. Factor loadings from the initial PCA on the SAPS/SANS dataset
solely by differences in the ratings at the more extreme end of the OH scale, we alsoconducted a logistic regression analysis to predict the presence (scores of ‘1–5’) versusabsence (‘0’ score) of OHs. This analysis identified the same predictors as had beenidentified in the linear regression analyses.

Olfactory hallucinations 157
Table 6. Reduced model predicting severity rating of OHs in the SAPS/SANS dataset
DiscussionThe present study aimed to examine the past-month prevalence of OHs and co-occurring symptoms in two pre-existing datasets. One dataset comprised cases froman international sample of patients who had recently made a first-in-lifetime approachto a clinical service (the WHO-10 Study); and the other dataset comprised cases withestablished schizophrenic illness from a series of independent Australian studies. Thetwo samples were assessed for past-month prevalence of symptoms using the PSE-9 andSAPS, respectively. While the PSE-9 includes two OH items, one for external smells, theother for self-smells, the SAPS includes a single item for external- or self-smells. Resultswere consistent across datasets, in support of the view that the PSE-9 and SAPS OH itemsare indexing the same phenomena, despite that one of the PSE-9 OH items, ‘Delusionthat subject smells’, is ambiguous as to whether the respondent actually experiences thesmell or merely believes that others can smell him/her.
Hallucinations were common in both datasets (57 and 64%, respectively), withthe relative prevalence of hallucinations in different modalities also consistent acrossdatasets, and consistent with previous research; i.e., auditory hallucinations were themost common, followed by visual and somatic, and then other hallucinations. That wefound somatic hallucinations to be the second most common in the SAPS/SANS datasetaccords with the previous findings of Baethge et al. (2005). The past-month prevalenceof OHs (at 13 and 17%, respectively) was also in general accord with much of theprevious research. Previous studies, which have reported higher rates (e.g., 35%: Kopalaet al., 1994; and 26%: Stedman & Clair, 1998), have assessed either lifetime prevalence orpast-month prevalence in patients from a research ward. In contrast, the present studyfocused on past-month prevalence in two datasets derived from patients who had beenrecruited via a variety of service providers and agencies, including a volunteer register.
Examination of the 962 WHO-10 cases revealed that the prevalence of OHs andhallucinations in other modalities differed according to international centre; e.g., visualhallucinations were most common in Nigeria, compared to the other centres, while OHsand other hallucinations were less common. Previous research has similarly suggestedthat visual hallucinations may be more common in non-Western societies (see, e.g.,Zarroug, 1975). Thomas et al. (2007) have also reported that the prevalence ratesof hallucinations can vary according to the patients’ country of origin. For example,these researchers reported that hallucinations, irrespective of modality, were morecommon in their US sample compared to their Indian sample; however, they did notformally compare these rates, since, they argued, the samples were not selected to berepresentative of the two nations. The same point applies to our own findings. In other

158 Robyn Langdon et al.
related work, Suhail and Cochrane (2002) have examined medical records to compare thecontent of hallucinations (and delusions) in three schizophrenia groups: White British;Pakistanis living in Britain; and Pakistanis living in Pakistan. They found that the Pakistanisliving in Pakistan revealed more evidence of visual hallucinations and less evidence ofauditory–verbal hallucinations, compared to the other two groups. While acknowledgingthe need for caution when interpreting findings of this type, including our own, suchfindings do nevertheless suggest that sociocultural factors may modulate the estimatedprevalence rates of hallucinations in different modalities. Such effects may reflect eithersocialcultural variation in the self-reporting and/or detection of hallucinations in differentmodalities or socialcultural differences in the actual content of the patients’ hallucinatoryexperiences. The latter might arise, for example, via socialcultural differences in thepatients’ expectations and/or differences in the social and environmental triggers of thepatients’ hallucinatory experiences.
OHs were more common in females than males, although not significantly so,generally consistent with the previous findings of Kopala et al. (1994) and Ndeteiand Singh (1983). Results were non-significant concerning an hypothesized relationshipbetween OHs and more severe psychopathology, whether indexed by earlier age-of-onset or more severe negative symptoms; instead, we found that positive symptomsbetter predicted OHs. In contrast, significant associations were found between OHsand negative mood, in particular, depression and anxiety, in the WHO-10 dataset,consistent with the view that negative mood and negative appraisals associate stronglywith hallucinatory experiences (e.g., Gauntlett-Gilbert & Kuipers, 2005; Kopala et al.,1994).
The initial scaling/data reduction techniques were also consistent across datasets;OHs were found to co-occur with hallucinations in other modalities (particularly,somatic, tactile, and gustatory hallucinations) and referential/control delusions, generallyconsistent with the findings of previous studies which have used techniques of thistype (see, e.g., McGrath et al., 2009). The strong associations found between OHs andsomatic/tactile/gustatory hallucinations also provide support for a number of previousstudies, which have grouped together all hallucinations of this type (e.g., Lewandowskiet al., 2009).
The regression results were likewise consistent across datasets; referential/controldelusions were found to be significant correlates of OHs, independent of the influence ofother hallucinations. Such findings accord with the previous anecdotal reports that OHsare particularly prone to trigger delusional elaborations (e.g., that smells are being forcedupon one, and with some purpose in mind: Meats, 1988). The additional findings (fromthe WHO-10 dataset) that OHs associate with somatic concerns, depression, and anxietyare also worthy of note. These findings go some way to justify the concerns that patientswith OHs feel a societal pressure to keep such experiences to themselves, thus mitigatingagainst any spontaneous self-reporting, as previously cautioned by Meats (1988) andRubert, Hollender, and Mehrhof (1975). The implication here is that conventional clinicalinstruments, which currently lack OH items, need to be augmented with specific OHprobes to provide more reliable and comprehensive clinical assessments. OHs of smellingone’s own body associated most strongly with somatic concerns, depression, and a senseof hopelessness, cautioning that experiences of this type are particularly deleterious tosocial function. They thus warrant probing with great sensitivity, despite that they arerelatively less common.
While auditory and other hallucinations correlated strongly with OHs, suggestingthat some shared processes are involved in both olfactory and non-OHs, the finding that

Olfactory hallucinations 159
referential/control delusions, and specifically somatic/tactile/gustatory hallucinationscontribute independently to the prediction of OHs (i.e., having accounted for otherhallucinations: e.g., auditory–verbal) points to the existence of other processes thatmore specifically promote OHs. These associations were seen whether predicting thepresence or severity of OHs; thus, it seems unlikely that the presence of co-occurringdelusions simply exacerbates the severity of OHs, once these have been generated bymechanisms shared equally with other hallucinations. The absence of obvious perceptualdeficits (e.g., odour identification deficits) in olfactory hallucinators (Kopala et al., 1994;Stedman & Clair, 1998) rules out that these OH-specific processes might involve basicolfactory deficits. We offer three suggestions. The first draws upon the strong associationsobserved between olfactory, tactile, and gustatory hallucinations; our proposal here isthat some OHs might be generated as a sort of tactile ‘sniffing hallucination’ (i.e., anexperience of sniffing in the absence of actual sniffing – hallucinatory sniffs, which leadto olfactory cortical activation and an OH). Our other suggestions focus on delusion-related factors; firstly, we allow that OHs might share common abnormal generatorswith non-OHs (e.g., abnormal involuntary memories), however, OHs, by their nature,may be more prone to threat-related delusional elaborations (see, e.g., Meats, 1988).These delusional elaborations would then feedback to promote the enhanced mainte-nance of olfactory (compared to non-olfactory) hallucinations. Secondly, normal smellexperiences are more elusive than other sensory experiences; as such, perfectly normal(yet vague) smell experiences might be more vulnerable (compared to other sensoryexperiences) to misinterpretations that are fuelled by pre-existing referential/controldelusions. As the current study was cross-sectional, however, and relied upon secondarydata, focused primarily on prevalence, we had no data available to more directly evaluatethese proposals.
In summary, our findings highlight the clinical significance of OHs, despite that thesesymptoms are relatively less common, and underrepresented in conventional ratingscales and diagnostic instruments. Previous phenomenological reports of OHs haveemphasized their intrusive, distressing nature, and their unpleasantness (Kopala et al.,1994; Meats, 1988), consistent with the present study’s findings (across both datasets)that OHs associate strongly with delusions of reference and control, which likely fuel asense of threat and anxiety. The effects of the different international centres in the WHO-10 dataset also caution that the experience of, and/or the detection of, hallucinations maybe nuanced by sociocultural factors. Moreover, the strong associations observed betweenOHs, lack of self-confidence with others, and anxiety also caution that any spontaneousself-reporting of OHs might be self-censored due to a societal pressure to avoid mentionof unpleasant odours. OHs of smelling one’s own body appear particularly deleteriousto social relations and may require sensitive probing. More directed phenomenologicaland longitudinal research is required to further evaluate our proposals concerning thestrong associations observed between OHs, somatic/tactile/gustatory hallucinations andreferential/control delusions.
AcknowledgementsWe wish to thank Professor Assen Jablensky of the Centre for Clinical Research inNeuropsychiatry (CCRN), University of Western Australia, for kindly providing us withaccess to the WHO-10 database, Danny Rock of CCRN for assistance with recoding thePSE-9 ratings, and Dr Alan Taylor, Department of Psychology, Macquarie University, for his

160 Robyn Langdon et al.
invaluable statistical advice. We also thank the ASRB, which is supported by the NationalHealth and Medical Research Council of Australia, the Pratt Foundation, Ramsay Health Care,the Viertel Charitable Foundation, and the Schizophrenia Research Institute, for its assistancein recruiting some of the participants in the SAPS/SANS dataset.
ReferencesArajarvi, R., Varilo, T., Haukka, J., Suvisaari, J., Suokas, J., Juvonen, H., . . . Lonnqvist, J. (2006).
Affective flattening and alogia associate with the familial form of schizophrenia. Psychiatry
Research, 141, 161–172. doi:10.1016/j.psychres.2005.08.008Baethge, C., Baldessarini, R. J., Freudenthal, K., Streeruwitz, A., Bauer, M., & Bschor, T. (2005).
Hallucinations in bipolar disorder: Characteristics and comparison to unipolar depression andschizophrenia. Bipolar Disorders, 7, 136–145. doi:10.1111/j.1399-5618.2004.00175.x
Bentall, R. P. (1990). The illusion of reality: A review and integration of psychological research onhallucinations. Psychological Bulletin, 107, 82–95. doi:10.1037/0033-2909.107.1.82
Blanchard, J. J., & Cohen, A. S. (2006). The structure of negative symptoms within schizophrenia:Implications for assessment. Schizophrenia Bulletin, 32, 238–245. doi:10.1093/schbul/sbj013
Bracha, H. S., Wolkowitz, O. M., Lohr, J. B., Karson, C. N., & Bigelow, L. B. (1989). High prevalenceof visual hallucinations in research subjects with chronic schizophrenia. American Journal of
Psychiatry, 146 , 526–528.Brewer, W. J., Wood, S. J., McGorry, P. D., Francey, S. M., Phillips, L. J., Yung, A. R., . . . Pantelis,
C. (2003). Impairment of olfactory identification ability in individuals at ultra-high risk forpsychosis who later develop schizophrenia. American Journal of Psychiatry, 160, 1790–1794. doi:10.1176/appi.ajp.160.10.1790
Brill, A. A. (1932). The sense of smell in the neuroses and psychoses. Psychoanalytical Quarterly,1, 7–42.
Campbell, M. L. C., & Morrison, A. P. (2007). The role of unhelpful appraisals and behaviours invulnerability to psychotic-like phenomena. Behavioural and Cognitive Psychotherapy, 35,555–567. doi:10.1017/S1352465807003906
Cardno, A. G., Holmans, P. A., Harvey, I., Williams, M. B., Owen, M. J., & McGuffin, P. (1997). Factor-derived subsyndromes of schizophrenia and familial morbid risks. Schizophrenia Research,23, 231–238. doi:10.1016/S0920-9964(96)00093-X
Cardno, A. G., Jones, L. A., Murphy, K. C., Asherson, P., Scott, L. C., Williams, J., . . . McGuffin, P.(1996). Factor analysis of schizophrenic symptoms using the OPCRIT checklist. Schizophrenia
Research, 22, 233–239. doi:10.1016/S0920-9964(96)00060-6Carpenter, W. T., Straus, J. S., & Bartko, J. J. (1973). Flexible system for the diagnosis of
schizophrenia: Report from the WHO International Pilot Study of Schizophrenia. Science,182, 1275–1277. doi:10.1126/science.182.4118.1275
Castle, D. J., Jablensky, A., McGrath, J. J., Carr, V., Morgan, V., Waterreus, A., . . . Farmer, A. (2006).The diagnostic interview for psychoses (DIP): Development, reliability and applications.Psychological Medicine, 36 , 69–80. doi:10.1017/S0033291705005969
Delisi, L. E. (1992). The significance of age of onset for schizophrenia. Schizophrenia Bulletin,18, 209–215.
Emsley, R., Rabinowitz, J., & Torreman, M. (2003). The factor structure for the Positive andNegative Syndrome Scale (PANSS) in recent-onset psychosis. Schizophrenia Research, 61,47–57. doi:10.1016/S0920-9964(02)00302-X
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. (1996). Structured clinical interview for
DSM-IV axis I disorders, clinician version (SCID-CV). Washington, DC: American PsychiatricPress.
Fortuyn, H. A. D., Lappenschaar, G. A., Nienhuis, F. J., Furer, J. W., Hodiamont, P. P.,Rijnders, C. A., . . . Overeem, S. (2009). Psychotic symptoms in narcolepsy: Phenomenol-ogy and a comparison with schizophrenia. General Hospital Psychiatry, 31, 146–154.doi:10.1016/j.genhosppsych.2008.12.002

Olfactory hallucinations 161
Garety, P. A., Kuipers, E., Fowler, D., Freeman, D., & Bebbington, P. E. (2001). A cogni-tive model of the positive symptoms of psychosis. Psychological Medicine, 31, 189–195.doi:10.1017/S0033291701003312
Gauntlett-Gilbert, J., & Kuipers, E. (2005). Visual hallucinations in psychiatric conditions: Ap-praisals and their relationship to distress. British Journal of Clinical Psychology, 44, 77–87.doi:10.1348/014466504x19451
Goldberg, S. C., Klerman, G. L., & Cole, J. O. (1965). Changes in schizophrenic psychopathologyand ward behaviour as a function of phenothiazine treatment. British Journal of Psychiatry,111, 120–133. doi:10.1192/bjp.111.471.120
Good, K. P., Whitehorn, D., Rui, Q., Milliken, H., & Kopala, L. C. (2006). Olfactory identifi-cation deficits in first-episode psychosis may predict patients at risk for persistent negativeand disorganized or cognitive symptoms. American Journal of Psychiatry, 163, 932–933.doi:10.1176/appi.ajp.163.5.932
Goodwin, D. W., & Alderson, P. (1971). Clinical significance of hallucinations in psychiatricdisorders. Archives of General Psychiatry, 24, 76–80.
Guy, W., & Ban, T. A. (1982). The AMDP system. Manual for the assessment and documentation
in psychopathology. Berlin: Springer.Hudry, J., Saoud, M., d’Amato, T., Dalery, J., & Royet, J. (2002). Ratings of different olfactory
judgements in schizophrenia. Chemical Senses, 27, 407–416. doi:10.1093/chemse/27.5.407Jablensky, A., Sartortius, N., Ernberg, G., Anker, M., Korten, A., Cooper, J. E., . . . Bertelsen, A.
(1992). Schizophrenia: Manifestations, incidence and course in different cultures; A WorldHealth Organisation Ten-Country Study. Psychological Medicine; Monograph Supplement,20, 1–97. doi:10.1017/S0264180100000904
John, J. P., Khanna, S., Thennarasu, K., & Reddy, S. (2003). Exploration of dimensions of psy-chopathology in neuroleptic-naıve patients with recent-onset schizophrenia/schizophreniformdisorder. Psychiatry Research, 121, 11–20. doi:10.1016/S0165-1781(03)00199-9
Kay, S. R., Opler, L. A., Spitzer, R. L., Williams, J. B. W., Fiszbein, A., & Gorelick, A. (1991). SCID-PANSS: Two-tier diagnostic system for psychotic disorders. Comprehensive Psychiatry, 32,355–361. doi:10.1016/0010-440X(91)90085-Q
Kitamura, T., Okazaki, Y., Fujinawa, A., Takayanagi, I., & Kasahara, Y. (1998). Dimen-sions of schizophrenic positive symptoms: An exploratory factor analysis investiga-tion. European Archives of Psychiatry and Clinical Neuroscience, 248, 130–135.doi:10.1007/s004060050029
Kopala, L. C., Good, K. P., & Honer, W. G. (1994). Olfactory hallucinations and olfactory identi-fication ability in patients with schizophrenia and other psychiatric disorders. Schizophrenia
Research, 12, 205–211. doi:10.1016/0920-9964(94)90030-2Kwapil, T. R., Chapman, J. P., Chapman, L. J., & Miller, M. B. (1996). Deviant olfactory experiences
as indicators of risk for psychosis. Schizophrenia Bulletin, 22, 371–382.Langdon, R., Coltheart, M., & Ward, P. (2006). Empathetic perspective-taking is impaired in
schizophrenia: Evidence from a study of emotion attribution and theory of mind. Cognitive
Neuropsychiatry, 11, 133–155. doi:10.1080/13546800444000218Langdon, R., Coltheart, M., Ward, P. B., & Catts, S. V. (2001). Mentalising, executive
planning and disengagement in schizophrenia. Cognitive Neuropsychiatry, 6 , 81–108.doi:10.1080/13546800042000061
Langdon, R., Coltheart, M., Ward, P. B., & Catts, S. V. (2002). Disturbed communication inschizophrenia: The role of poor pragmatics and poor mind-reading. Psychological Medicine,32, 1273–1284. doi:10.1017/S0033291702006396
Langdon, R., Corner, T., McLaren, J., Coltheart, M., & Ward, P. B. (2006). Atten-tional orienting triggered by gaze in schizophrenia. Neuropsychologia, 44, 417–429.doi:10.1016/j.neuropsychologia.2005.05.020
Lewandowski, K. E., DePaola, J., Camsari, G. B., Cohen, B. M., & Ongur, D. (2009). Tactile,olfactory, and gustatory hallucinations in psychotic disorders: A descriptive study. Annals of
the Academy of Medicine, Singapore, 38, 383–387.

162 Robyn Langdon et al.
Liddle, P. F. (1987). The symptoms of chronic schizophrenia. A re-examination of the positive–negative dichotomy. British Journal of Psychiatry, 151, 145–151. doi:10.1192/bjp.151.2.145
Lobban, F., Haddock, G., Kinderman, P., & Wells, A. (2002). The role of metacognitivebeliefs in auditory hallucinations. Personality and Individual Differences, 32, 1351–1363.doi:10.1016/S0191-8869(01)00123-4
McGrath, J. A., Avramopoulos, D., Lasseter, V. K., Wolyniec, P. S., Fallin, M. D., Liang, K., . . .Pulver, A. E. (2009). Familiality of novel factorial dimensions of schizophrenia. Archives of
General Psychiatry, 66 , 591–600. doi:10.1001/archgenpsychiatry.2009.56McGuffin, P., Farmer, A. E., & Harvey, I. H. (1991). A polydiagnostic application of operational
criteria in studies of psychotic illness: Development and reliability of the OPCRIT system.Archives of General Psychiatry, 48, 764–770.
Meats, P. (1988). Olfactory hallucinations. British Medical Journal, 296 , 645.doi:10.1136/bmj.296.6622.645
Minas, I. H., Stuart, G. W., Klimidis, S., Jackson, H. J., Singh, B. S., & Copolov, D. (1992). Positiveand negative symptoms in the psychosis: Multidimensional scaling of SAPS and SANS items.Schizophrenia Research, 8, 143–156. doi:10.1016/0920-9964(92)90031-Y
Moberg, P. J., Agrin, R., Gur, R. E., Gur, R. C., Turetsky, B. I., & Doty, R. L. (1999). Olfactory dys-function in schizophrenia: A qualitative and quantitative review. Neuropsychopharmacology,21, 325–340. doi:10.1016/S0893-133X(99)00019-6
Mohr, C., Hubener, F., & Laska, M. (2002). Deviant olfactory experiences, magical ideation, andolfactory sensitivity: A study with healthy German and Japanese subjects. Psychiatry Research,111, 21–33. doi:10.1016/S0165-1781(02)00132-4
Morrison, A. P. (2001). The interpretation of intrusions in psychosis: An integrative cognitiveapproach to hallucinations and delusions. Behavioural and Cognitive Psychotherapy, 29,257–276.
Muelman, J. J., & Heiser, W. J. (1999). SPSS categories 10.0. Chicago, IL: SPSS.Mueser, K. T., Bellack, A. S., & Brady, E. U. (1990). Hallucinations in schizophrenia. Acta
Psychiatrica Scandinavica, 82, 26–29. doi:10.1111/j.1600-0447.1990.tb01350.xMurphy, H. B. M., Wittkower, E. D., Fried, J., & Ellenberger, H. (1963). A cross-cultural survey of
schizophrenic symptomatology. International Journal of Social Psychiatry, 9, 237–249.Ndetei, D. M., & Singh, A. (1983). Hallucinations in Kenyan schizophrenic patients. Acta
Psychiatrica Scandinavica, 67, 144–147. doi:10.1111/j.1600-0447.1983.tb00334.xNdetei, D. M., & Vadher, A. (1984). A comparative cross-cultural study of the frequencies of hallu-
cination in schizophrenia. Acta Psychiatrica Scandinavica, 70, 545–549. doi:10.1111/j.1600-0447.1984.tb01247.x
Nurnberger, J. I., Blehar, M. C., Kaufmann, C. A., York-Cooler, C., Simpson, S. G., Harkavy-Friedman,J., . . . Reich, T. (1994). NIMH genetics initiative. Diagnostic interview for genetic studies:Rationale, unique features, and training. Archives of General Psychiatry, 51, 849–859.
Ohanyon, M. M. (2000). Prevalence of hallucinations and their pathological associations in thegeneral population. Psychiatry Research, 97, 153–164. doi:10.1016/S0165-1781(00)00227-4
Peralta, V., & Cuesta, M. J. (1998). Factor structure and clinical validity of competing models ofpsychotic symptoms in schizophrenia. Biological Psychiatry, 44, 107–114. doi:10.1016/S0006-3223(97)00341-7
Peralta, V., & Cuesta, M. J. (1999). Dimensional structure of psychotic symptoms: An item-levelanalysis of SAPS and SANS symptoms in psychotic disorders. Schizophrenia Research, 38,13–26. doi:10.1016/S0920-9964(99)00003-1
Peralta, V., & Cuesta, M. J. (2001). How many and which are the psychopathological dimensions inschizophrenia? Issues influencing their ascertainment. Schizophrenia Research, 49, 269–285.doi:10.1016/S0920-9964(00)00071-2
Peralta, V., & Cuesta, M. J. (2007). The relationship between syndromes of the psychotic illnessand familial liability to schizophrenia and major mood disorders. Schizophrenia Research, 91,200–209. doi:10.1016/j.schres.2006.12.018

Olfactory hallucinations 163
Rubert, S. L., Hollender, M. H., & Mehrhof, E. G. (1975). Olfactory hallucinations. Archives of
General Psychiatry, 5, 313–318.Sakel, M. (1958). Schizophrenia. New York: Philosophical Libraries.Seal, M. L., Aleman, A., & McGuire, P. K. (2004). Compelling imagery, unanticipated speech and
deceptive memory: Neurocognitive models of auditory verbal hallucinations in schizophrenia.Cognitive Neuropsychiatry, 9, 43–72. doi:10.1080/13546800344000156
Silver, H., David, D., Kaplan, M., Hadjez, J., Tubi, N., Darnel, A., . . . Lererd, B. (1993). Factoranalysis of schizophrenic symptoms and comparison of different rating scales. Schizophrenia
Research, 10, 61–75. doi:10.1016/0920-9964(93)90078-WSmith, B., Fowler, D. G., Freeman, D., Bebbington, P., Bashforth, H., Garety, P., . . .
Kuipers, E. (2006). Emotion and psychosis: Links between depression, self-esteem, negativeschematic beliefs and delusions and hallucinations. Schizophrenia Research, 86 , 181–188.doi:10.1016/j.schres.2006.06.018
Spitzer, R. L., Williams, J. B., Gibbon, M., & First, M. B. (1992). The structured clinical interviewfor DSM-III-R (SCID). I: History, rationale, and description. Archives of General Psychiatry,49, 624–629.
Stedman, T. J., & Clair, A. L. (1998). Neuropsychological, neurological and symptom correlatesof impaired olfactory identification in schizophrenia. Schizophrenia Research, 32, 23–30.doi:10.1016/S0920-9964(98)00021-8
Stevenson, R. J., & Case, T. I. (2005). Olfactory imagery: A review of its phenomenological,experimental and theoretical bases. Psychonomic Bulletin and Review, 12, 244–264.
Stuart, G. W., Malone, V., Currie, J., Klimidis, S., & Minas, I. H. (1995). Positive and negativesymptoms in neuroleptic-free psychotic inpatients. Schizophrenia Research, 16 , 175–188.doi:10.1016/0920-9964(94)00083-K
Stuart, G. W., Pantelis, C., Klimidis, S., & Minas, I. H. (1999). The three-syndrome modelof schizophrenia: Meta-analysis of an artefact. Schizophrenia Research, 39, 233–242.doi:10.1016/S0920-9964(99)00019-5
Suhail, K., & Cochrane, R. (2002). Effect of culture and environment on the phenomenologyof delusions and hallucinations. International Journal of Social Psychiatry, 48, 126–138.doi:10.1177/002076402128783181
Thomas, P., Mathur, P., Gottesman, I. I., Nagpal, R., Nimgaonkar, V. L., & Deshpande, S. N. (2007).Correlates of hallucinations in schizophrenia: A cross-cultural evaluation. Schizophrenia
Research, 92, 41–49. doi:10.1016/j.schres.2007.01.017Waters, F. A. V., Badcock, J. C., Michie, P., & Maybery, M. T. (2006). Auditory hallucinations in
schizophrenia: Intrusive thoughts and forgotten memories. Cognitive Neuropsychiatry, 11,65–83. doi:10.1080/13546800444000191
Zarroug, E. T. (1975). The frequency of visual hallucinations in schizophrenic patients in SaudiArabia. British Journal of Psychiatry, 127, 553–555. doi:10.1192/bjp.127.6.553
Received 26 February 2009; revised version received 19 March 2010
Related Documents











