CLEVELAND ACUTE STROKE EXPERIENCE • Cleveland Health Quality Choice – stroke data collected by trained abstractors since 1991 – IV tPA datapoints added 1996 – disbanded 1998 • Cuyahoga County Operation Stroke 1999 – data collection instrument designed by the Medical Committee and The Stroke Group (ETHOS R ) • grants from Genentech/Astra Zeneca • Cleveland Clinic Health System Stroke QI Program – presented to JCAHO 4/01

CLEVELAND ACUTE STROKE EXPERIENCE Cleveland Health Quality Choice –stroke data collected by trained abstractors since 1991 –IV tPA datapoints added 1996.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CLEVELAND ACUTE STROKE EXPERIENCE
• Cleveland Health Quality Choice– stroke data collected by trained abstractors since 1991– IV tPA datapoints added 1996– disbanded 1998
• Cuyahoga County Operation Stroke 1999– data collection instrument designed by the Medical Committee and
The Stroke Group (ETHOSR)
• grants from Genentech/Astra Zeneca
• Cleveland Clinic Health System Stroke QI Program– presented to JCAHO 4/01
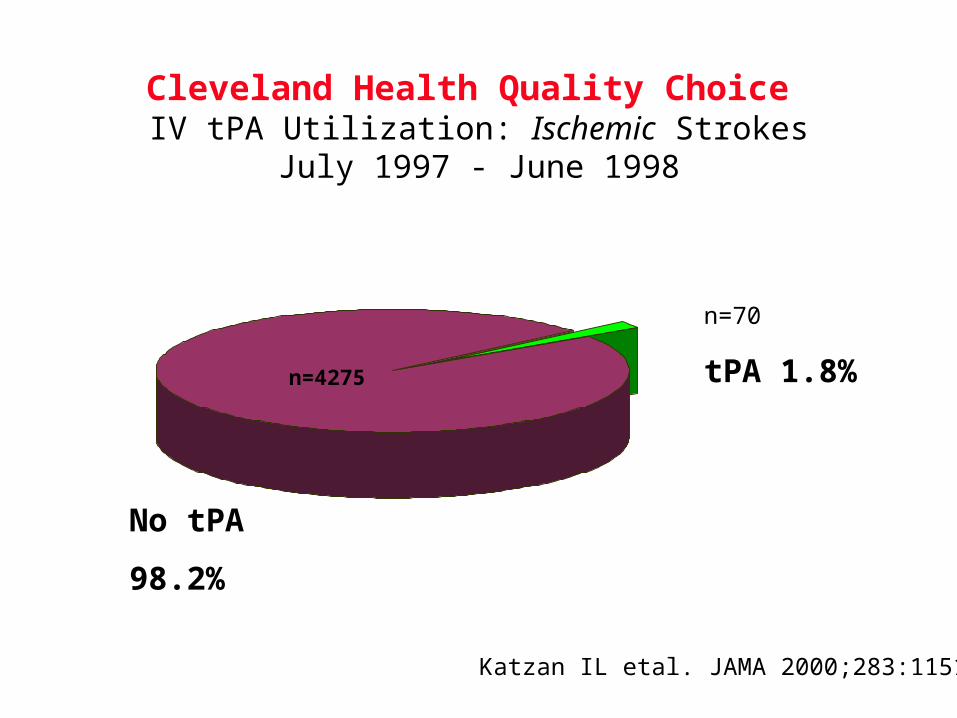
Cleveland Health Quality Choice IV tPA Utilization: Ischemic Strokes
July 1997 - June 1998
n=4275
n=70
tPA 1.8%
No tPA
98.2%
Katzan IL etal. JAMA 2000;283:1151

Cleveland Health Quality Choice IV tPA Utilization by Hospital
July 1997 - June 199811
5
32 2
12
1
0
2
4
6
8
10
12
0 1 2 4 5 6 9 17
# tPA cases
# H
ospi
tals
Katzan IL etal. JAMA 2000;283:1151
N = 27
(N = 70)
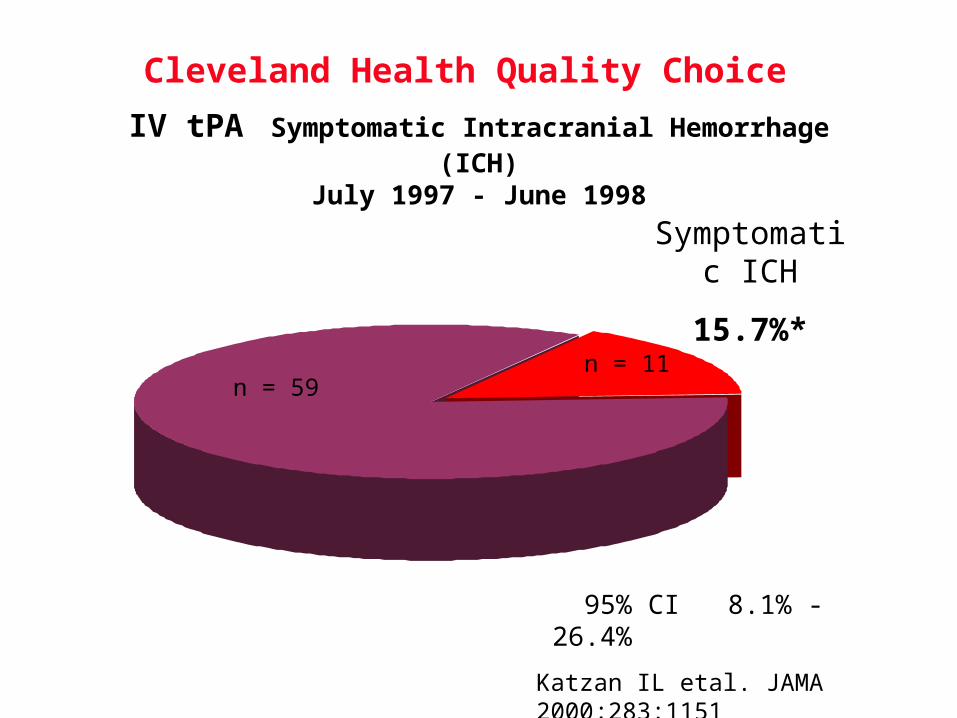
Cleveland Health Quality Choice IV tPA Symptomatic Intracranial Hemorrhage (ICH)
July 1997 - June 1998
n = 59n = 11
Symptomatic ICH
15.7%*
* 95% CI 8.1% - 26.4%
Katzan IL etal. JAMA 2000;283:1151
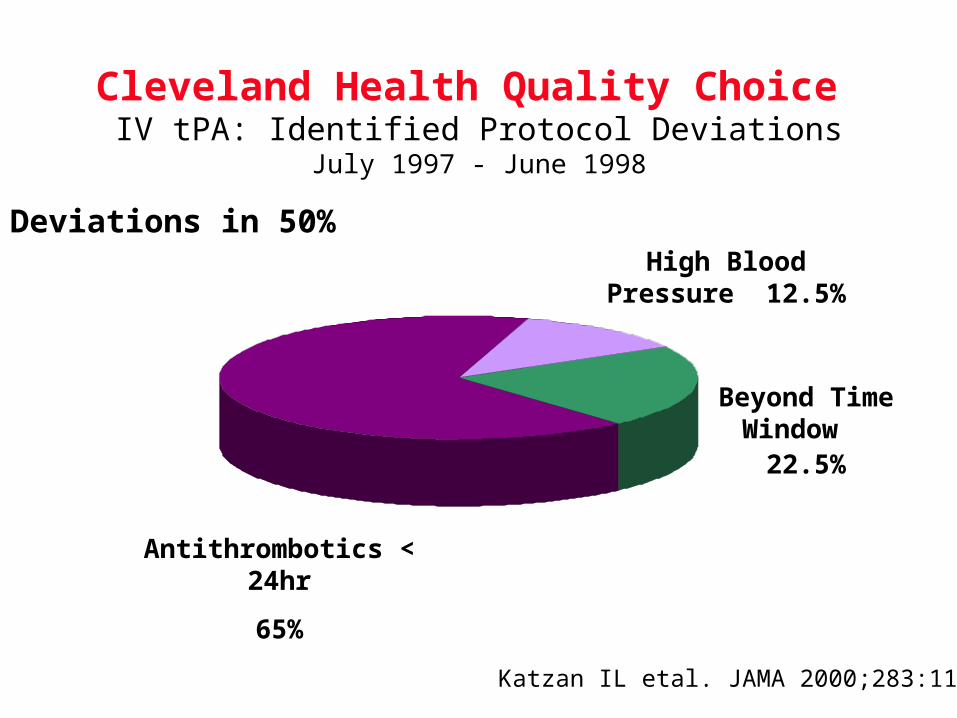
Cleveland Health Quality Choice IV tPA: Identified Protocol Deviations
July 1997 - June 1998
Antithrombotics < 24hr
65%
Beyond Time Window
22.5%
High Blood Pressure 12.5%
Katzan IL etal. JAMA 2000;283:1151
Deviations in 50%

Intracranial Hemorrhage after IV tPA
Series # pts Total ICH Sxatic ICH Fatal ICH
NINDS Trial 312 11% 6% 3%
STARS 296 10% 3% n/a
Cologne 100 11% 5% 1%
Multicenter tPA Survey 189 9% 6% 2%
Houston 30 10% 7% 3%
Minnesota 97 13% 9% 6%
Michigan 54 15% 9% n/a
Indianapolis 41 22% 12% 10%
Cleveland 70 22% 16% 9%
Connecticut* 63 17% 6% na

Connecticut IV tPA experience(Bravata DM etal. Arch Intern Med 2002;162:1994)
• Retrospective cohort of 16 community based hospitals 5/96-12/98
• 67% (42/63) major protocol deviations– dosing errors– >3 hours– known increased bleeding risk (eg low platelets)
• Serious extracranial hemorrhage 17% (NINDS 2%)
• In-hospital mortality 31% (NINDS 13%)



Cuyahoga County Operation Stroke Door to Doctor
Median Times
1012
2
10 10 10
20
7
0
5
10
15
20
25
NINDS ALL IV tPA NoExclusions
<2 hr 2-3 hr 3-6 hr >6
Patient population
min
1/00 - 3/01
(N=65) (N=224) (N=253) (N=65)(N=692) (N=101) (N=59)
Katzan IL etal. Stroke 2003 in press

Cuyahoga County Operation Stroke Time to Initiation of CT
Median Times
25
65
20.5
62 68 67.5
108
50
0
20
40
60
80
100
120
NINDS ALL IV tPA NoExclusions
<2 hr 2-3 hr 3-6 hr >6
Patient population
min
1/00 - 3/01
(N=56) (N=241) (N=262) (N=53)(N=671) (N=78) (N=58)
Katzan IL etal. Stroke 2003 in press

Center line = median, box=25-75% quartiles, whiskers=1.5x interquartile range
Katzan IL etal. Stroke 2003 in press
Cuyahoga County Operation Stroke


Cleveland Clinic Health SystemStroke Quality Improvement Program Symptomatic Intracranial Hemorrhage
Symptomatic ICH13.8%*
n=4
No symptomatic ICH86.2%
n=25
*95% CI = 5.5% - 30.6%
7/97-6/98 CHQC



CLEVELAND ACUTE STROKE EXPERIENCE
• Stroke QI requires data– quality of data varies (many hospitals = no data)– multiple barriers must be overcome (behavioral, political, resources)– team building through trust building
• Performance varies widely across hospitals– physicians and hospitals may not like their data– outliers may not mean bad care– community effectiveness may differ from NINDS efficacy
• Protocol deviations are very common – linked with bad outcomes
• Data can change behavior and improve stroke care – community performance improves over time with systematic QI
• Community hospitals can & should give IV tPA IF they are able to demonstrate they know how
Related Documents











