Hobbs, Martin R. Wilkins, Michael A. Gatzoulis and John Wharton Thum, Stephen J. Wort, Elisabeth Bédard, J. Simon R. Gibbs, Johann Bauersachs, Adrian J. Gerhard-Paul Diller, Sven van Eijl, Darlington O. Okonko, Luke S. Howard, Omar Ali, Thomas Idiopathic Pulmonary Arterial Hypertension Circulating Endothelial Progenitor Cells in Patients With Eisenmenger Syndrome and Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2008 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Circulation doi: 10.1161/CIRCULATIONAHA.108.769646 2008;117:3020-3030; originally published online June 2, 2008; Circulation. http://circ.ahajournals.org/content/117/23/3020 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://circ.ahajournals.org/content/suppl/2008/06/03/CIRCULATIONAHA.108.769646.DC1.html Data Supplement (unedited) at: http://circ.ahajournals.org//subscriptions/ is online at: Circulation Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer this process is available in the click Request Permissions in the middle column of the Web page under Services. Further information about Office. Once the online version of the published article for which permission is being requested is located, can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Circulation in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on May 1, 2014 http://circ.ahajournals.org/ Downloaded from by guest on May 1, 2014 http://circ.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Hobbs, Martin R. Wilkins, Michael A. Gatzoulis and John WhartonThum, Stephen J. Wort, Elisabeth Bédard, J. Simon R. Gibbs, Johann Bauersachs, Adrian J.
Gerhard-Paul Diller, Sven van Eijl, Darlington O. Okonko, Luke S. Howard, Omar Ali, ThomasIdiopathic Pulmonary Arterial Hypertension
Circulating Endothelial Progenitor Cells in Patients With Eisenmenger Syndrome and
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2008 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.108.769646
2008;117:3020-3030; originally published online June 2, 2008;Circulation.
http://circ.ahajournals.org/content/117/23/3020World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2008/06/03/CIRCULATIONAHA.108.769646.DC1.htmlData Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from
Circulating Endothelial Progenitor Cells in Patients WithEisenmenger Syndrome and Idiopathic Pulmonary
Arterial HypertensionGerhard-Paul Diller, MD; Sven van Eijl, PhD; Darlington O. Okonko, MRCP;
Luke S. Howard, MRCP; Omar Ali, MRCP; Thomas Thum, MD; Stephen J. Wort, MRCP;Elisabeth Bédard, FRCPC; J. Simon R. Gibbs, FRCP; Johann Bauersachs, MD; Adrian J. Hobbs, PhD;
Martin R. Wilkins, FRCP; Michael A. Gatzoulis, PhD; John Wharton, PhD
Background—Impaired endothelial homeostasis underlies the pathophysiology of pulmonary arterial hypertension (PAH).We speculated that PAH patients are deficient in circulating endothelial progenitor cells (EPCs), potentially contributingto endothelial dysfunction and disease progression.
Methods and Results—We recruited 41 patients with Eisenmenger syndrome (13 with Down syndrome), 55 withidiopathic PAH, and 47 healthy control subjects. Flow cytometry and in vitro assays were used to quantify EPCs andto assess cell function. The number of circulating CD34�, CD34�/AC133�, CD34�/KDR�, and CD34�/AC133�/KDR�
progenitor cells was low in Eisenmenger patients compared with healthy control subjects, and those with Downsyndrome displayed even fewer EPCs. Reductions in EPC numbers correlated with New York Heart Associationfunctional class, 6-minute walk distance, and plasma brain-type natriuretic peptide levels. The capacity of culturedperipheral blood mononuclear cells to form colonies and incorporate into tube-like structures was impaired inEisenmenger patients. Idiopathic PAH patients had reduced numbers of EPCs, and the number of circulating EPCscorrelated with invasive hemodynamic parameters in this cohort. Levels of immune inflammatory markers, cGMP,stable nitric oxide oxidation products, and asymmetric dimethylarginine were abnormal in patients with PAH and related tonumbers of EPCs. Within the idiopathic PAH population, treatment with the phosphodiesterase inhibitor sildenafil wasassociated with a dose-dependent rise in EPC numbers, resulting in levels consistently above those found with other therapies.
Conclusions—Circulating EPC numbers are reduced in 2 well-characterized forms of PAH, which also exhibit raised levelsof inflammatory mediators. Sildenafil treatment may represent a pharmacological means of increasing circulating EPCnumbers long-term. (Circulation. 2008;117:3020-3030.)
Key Words: endothelial progenitor cells � endothelium � heart defects, congenital � hypertension, pulmonary� pulmonary heart disease
Pulmonary arterial hypertension (PAH) is associated withconsiderable morbidity and mortality.1,2 Despite differ-
ences in the cause and rate of progression, the structuralabnormalities found in the pulmonary vasculature of patientswith idiopathic PAH (IPAH) and PAH associated withcongenital heart disease show remarkable similarities. Endo-thelial dysfunction also is an integral feature and an earlyevent in the pathogenesis of both conditions.3,4 Restoration ofnormal endothelial function is the common goal of availabletreatments.4
Clinical Perspective p 3030
Endothelial progenitor cells (EPCs) are mobilized from thebone marrow and contribute to postnatal vasculogenesis andvascular homeostasis, and the number and in vitro function ofcirculating EPCs relate to endothelial function.5–7 Recentstudies suggest that bone marrow–derived EPCs can incor-porate into the pulmonary microvasculature, and augmentingEPC levels by bolus administration may reverse PAH inmonocrotaline-treated rats.8 This work is now being trans-
Received May 14, 2007; accepted March 7, 2008.From the Adult Congenital Heart Centre and Centre for Pulmonary Hypertension, Royal Brompton Hospital, London, UK (G.-P.D., E.B., S.J.W.,
M.A.G.); National Heart and Lung Institute (G.-P.D., D.O.O., J.S.W., M.A.G., J.S.R.G., L.S.H) and Department of Experimental Medicine andToxicology (S.v.E., O.A., M.R.W., J.W.), Imperial College London, London, UK; Julius-Maximilians-Universität, Medizinische Klinik I, Würzburg,Germany (T.T., J.B); National Pulmonary Hypertension Service, Hammersmith Hospital, London, UK (L.S.H., S.R.G.); and Wolfson Institute forBiomedical Research, University College London, London, UK (A.J.H).
The online-only Data Supplement, which consists of Methods and figures, can be found with this article at http://circ.ahajournals.org/cgi/content/full/CIRCULATIONAHA.108.769646/DC1.
Correspondence to Gerhard-Paul Diller, MD, Adult Congenital Heart Centre and Centre for Pulmonary Hypertension, Royal Brompton Hospital,Sydney Street, London SW3 6NP, UK. E-mail [email protected]
© 2008 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.108.769646
3020 by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from
lated in clinical studies,9 but little is known about the baselinenumber and function of circulating EPCs in patients withPAH. We have examined the hypothesis that this endogenousrepair mechanism is impaired and, by implication, insuffi-cient to maintain endothelial function in 2 well-characterizedforms of the disease. We also assessed factors such asinflammatory mediators, nitric oxide metabolites, and asym-metric dimethylarginine (ADMA) known to affect EPCnumbers.
MethodsStudy SubjectsSubjects were recruited from 2 specialist hospitals between July2006 and December 2007. Approval from the local ethics commit-tees was obtained, and all study subjects provided written informedconsent.
Flow Cytometric Detection of Circulating EPCsPeripheral blood mononuclear cells (PBMNCs) were isolated bydensity centrifugation with Vacutainer CPT cell preparation tubes(BD Biosciences, Oxford, UK) or Ficoll-Paque (GE Healthcare LifeSciences, Little Chalfont, UK) according to the manufacturer’sinstructions. EPCs were enumerated using established criteria asCD34� cells coexpressing AC133 and vascular endothelial growthfactor (VEGF) receptor-2 (VEGFR2/fetal liver kinase 1/KDR) orcells coexpressing CD34 and KDR.10,11 We incubated 106 PBMNCswith FITC-labeled monoclonal mouse anti-human CD34 (BD Bio-sciences), PE-labeled monoclonal mouse anti-human AC133 (Milte-nyi Biotec, Surrey, UK), and allophycocyanin-labeled monoclonalmouse anti-human KDR (R&D Systems, Abingdon, UK) antibodiesfor 30 minutes at 4°C according to the manufacturers’ instructions orwith appropriate isotype controls. At least 100 000 events wereacquired in the lymphomonocytic gate using a FACSCalibur cytom-eter (Becton Dickinson, Oxford, UK). The number of progenitorcells was expressed as a percentage of all lymphomonocytic cells.
Case et al12 recently reported that PBMNCs coexpressing CD34�/AC133�/KDR� may represent primitive hematopoietic progenitorsand may not relate to colony-forming unit endothelial cells. Incontrast, CD34� cells not expressing the common leukocyte antigen
(CD45) were found to yield colony-forming unit endothelial cells intheir study. Therefore, we also quantified EPCs as lymphomonocyticcells expressing CD34 with low expression of CD45 (PE-labeledmonoclonal mouse anti-human CD45, BD Biosciences) as CD45low/CD34� EPCs in accordance with previous studies.13,14 To accountfor possible differing levels of lymphomonocytic cells in the subjectgroups, EPC levels were corrected for the number of lymphomono-cytic cells and compared with the percentages of EPCs in thelymphomonocytic gate.
Colony-Forming Units, Staining of Cultured Cells,and Incorporation Into Tube-Like StructuresWe assessed the colony-forming and angiogenic capacities of cellsderived from PBMNCs in culture because they have been reported tocorrelate with systemic vascular endothelial dysfunction and prog-nosis in other cardiovascular diseases.15,16 Colony-forming unitswere obtained after 5 days with EndoCult medium (StemCellTechnologies, London, UK).15 Isolated PBMNCs (107 cells per well)also were cultured in fibronectin-coated 6-well plates for 7 days.Adherent cells were counted, and the number that incorporatedhuman umbilical vein endothelial cells (HUVECs) in tube-likestructures was determined as previously described6 (see the online-only Data Supplement).
Plasma AssaysPlasma levels of chemokine (C-C motif) ligand-2 (CCL)-2 (formerlymonocyte chemotactic protein-1), tumor necrosis factor-� (TNF-�),interleukin-6 (IL-6), VEGF, cGMP, C-reactive protein (CRP), andADMA were quantified by use of commercial assays according tothe manufacturer’s instructions (see the online-only DataSupplement).
The combined concentrations (NOx) of plasma nitrite (NO�2) and
nitrate (NO�3), the stable oxidation products of nitric oxide (NO),
were determined with an NO chemiluminescence detector (NOA280, Sievers, Analytix Ltd, Peterlee, UK) as described.17 Plasmasamples were deproteinated by centrifugation in 3-kDa molecularweight cutoff filter units (Ultracel Microcon YM-3, Millipore Ltd,Watford, UK). In addition, a full blood count was made, andbrain-type natriuretic peptide (BNP) levels were measured.
Statistical AnalysisData are expressed as mean�SD or median and interquartile range(IQR). Statistical analysis was performed with the nonparametric
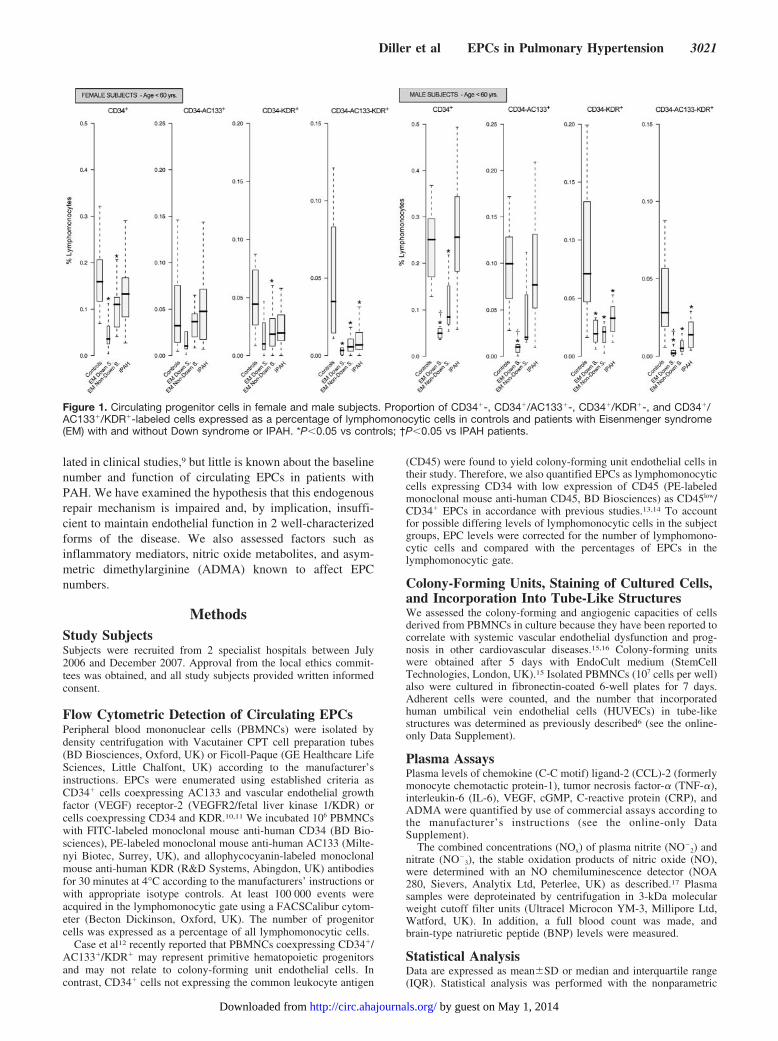
Figure 1. Circulating progenitor cells in female and male subjects. Proportion of CD34�-, CD34�/AC133�-, CD34�/KDR�-, and CD34�/AC133�/KDR�-labeled cells expressed as a percentage of lymphomonocytic cells in controls and patients with Eisenmenger syndrome(EM) with and without Down syndrome or IPAH. *P�0.05 vs controls; †P�0.05 vs IPAH patients.
Diller et al EPCs in Pulmonary Hypertension 3021
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from
Mann-Whitney U test and Spearman’s correlation using R version2.6.1 (R Foundation for Statistical Computing, Vienna Austria) andMedCalc 8.1 (MedCalc Software, Mariakerke, Belgium). Regressionanalyses were performed after variables were log transformed toachieve normal distribution. For all analyses, a 2-sided value ofP�0.05 was considered statistically significant.
The authors had full access to and take full responsibility for theintegrity of the data. All authors have read and agree to themanuscript as written.
ResultsSubjectsFifty-five patients with IPAH (44 female; age, 46�14 years),41 Eisenmenger patients (27 female; age, 37�12 years; 13with Down syndrome), and 47 healthy control subjects (24female; age 36�9 years) were recruited. To account fordifferences in gender distribution between the subject groups,EPC numbers were examined separately in male and femalesubjects. The Eisenmenger population was younger than theIPAH cohort, and patients exhibited secondary erythrocyto-sis, with raised hematocrit and hemoglobin levels and cyano-sis (Table I of the online-only Data Supplement).
EPC NumbersCirculating EPC numbers, as defined by the number ofdouble- (CD34�/KDR�) or triple- (CD34�/AC133�/KDR�)labeled cells, were significantly lower in patients with Eisen-menger syndrome or IPAH regardless of gender (Figure 1).Eisenmenger patients with Down syndrome had the lowestnumber of circulating EPCs. Progenitor cell numbers, definedas single- (CD34�) or double- (CD34�/AC133�) labeledcells, also were lower in the Eisenmenger population com-pared with control and IPAH subjects (Figure 1). Stratifyingsubjects by decades of age revealed that differences in EPCnumbers between patients and control subjects were main-tained throughout all age groups. No significant differences inthe lymphomonocyte cell counts were found between thecohorts (Table I). Correcting EPC numbers (expressed aspercent of lymphomonocytes) for actual lymphomonocyte
cell counts in individual patients did not affect the results ofthe study, confirming that EPC numbers were significantlylower in Eisenmenger and IPAH subjects compared withcontrol subjects (data not shown). In addition, the numbers ofCD45low/CD34� cells were significantly lower in non-Downpatients (0.377% versus 1.073%; P�0.003) and Down pa-tients with Eisenmenger syndrome (0.430% versus 1.073%;P�0.02) compared with those of control subjects. Levels ofCD45low/CD34� cells were not significantly different betweencontrol and IPAH subjects.
Association Between EPC Numbers andExercise ToleranceWithin the Eisenmenger population, an inverse relationshipwas found between circulating EPC numbers and exercisetolerance as judged by New York Heart Association func-tional class and 6-minute walk distance. EPC numbers weresignificantly higher in Eisenmenger patients in New YorkHeart Association functional class II compared with those inclass III as determined by the number of CD34� (median,0.099 versus 0.062; P�0.03), CD34�/AC133� (median,0.032 versus 0.013; P�0.009), CD34�KDR� (median, 0.029versus 0.012; P�0.02), or CD34�/AC133�/VEGFR2� (me-dian, 0.007 versus 0.002; P�0.008) cells. The number ofCD34�/AC133� cells in Eisenmenger patients also correlateddirectly with 6-minute walk distance (r�0.64, P�0.008) asshown in the online-only Data Supplement. In contrast, EPCnumbers in IPAH patients did not correlate with 6-minutewalk distance and did not vary significantly between NewYork Heart Association classes II, III, and IV (data notshown).
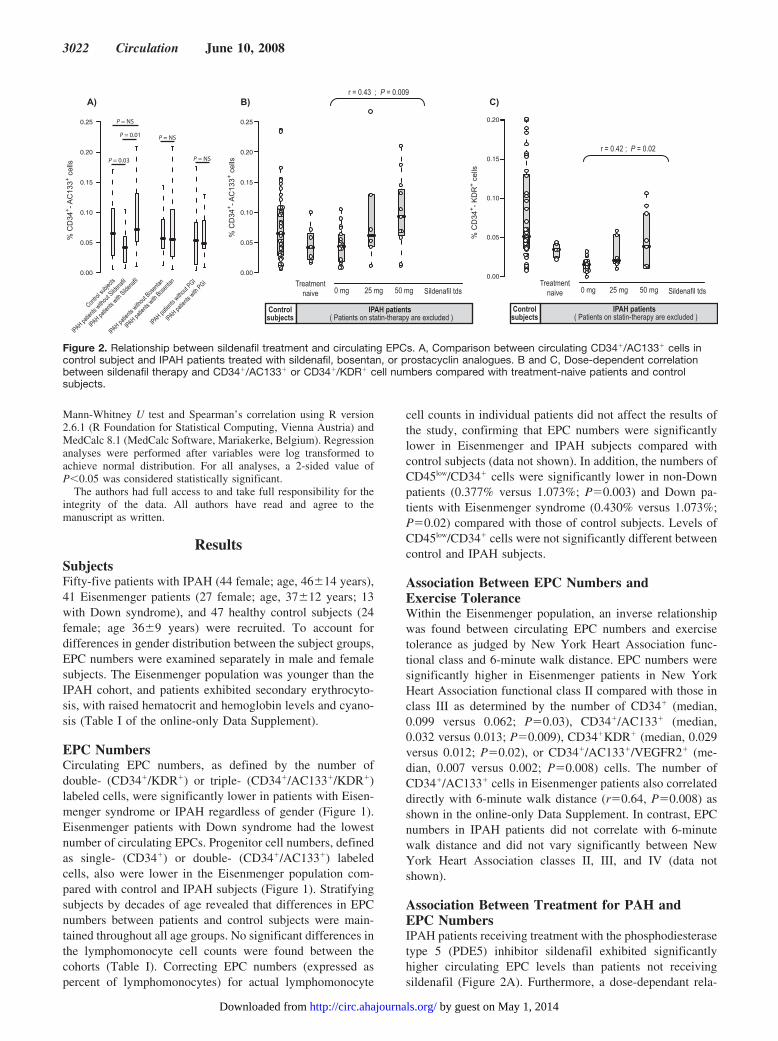
Association Between Treatment for PAH andEPC NumbersIPAH patients receiving treatment with the phosphodiesterasetype 5 (PDE5) inhibitor sildenafil exhibited significantlyhigher circulating EPC levels than patients not receivingsildenafil (Figure 2A). Furthermore, a dose-dependant rela-
% C
D34
+ - AC
133+ c
ells
Control
subjec
ts
IPAH patien
ts witho
ut Silde
nafil
IPAH patien
ts with
Sildenaf
il0.00
0.05
0.10
0.15
0.20
0.25
IPAH patien
ts witho
ut Bose
ntan
IPAH patien
ts with
Bosenta
n
IPAH patien
ts witho
ut PGI
IPAH patien
ts with
PGI
P = NS
P = 0.01
P = 0.03
P = NS
P = NS
% C
D34
+ - AC
133+ c
ells
0.00
0.05
0.10
0.15
0.20
0.25
A) B) C)r = 0.43 ; P = 0.009
Controlsubjects
0 mg 25 mg 50 mg Sildenafil tdsTreatment
naive
IPAH patients( Patients on statin-therapy are excluded )
Controlsubjects
0 mg 25 mg 50 mg Sildenafil tdsTreatment
naive
IPAH patients( Patients on statin-therapy are excluded )
0.00
0.05
0.10
0.15
0.20
r = 0.42 ; P = 0.02
% C
D34
+ - KD
R+ c
ells
Figure 2. Relationship between sildenafil treatment and circulating EPCs. A, Comparison between circulating CD34�/AC133� cells incontrol subject and IPAH patients treated with sildenafil, bosentan, or prostacyclin analogues. B and C, Dose-dependent correlationbetween sildenafil therapy and CD34�/AC133� or CD34�/KDR� cell numbers compared with treatment-naive patients and controlsubjects.
3022 Circulation June 10, 2008
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from
tionship was found between sildenafil exposure and EPCnumber, regardless of the surface markers used (Figure 2Band 2C). In contrast, no significant difference in EPC num-bers was found in IPAH patients treated with bosentan (125mg BD) or other targeted therapies compared with those oftreatment-naive patients and control subjects (Figure 2A).Similarly, no significant difference was found between thenumbers of progenitor cells in Eisenmenger patients treatedwith bosentan and treatment-naive patients (data not shown).Eleven IPAH patients had also taken an HMG-CoA reductaseinhibitor (atorvastatin 20 mg OD, n�1; simvastatin 40 to 80mg OD, n�10). The circulating EPC numbers in this cohortdid not differ significantly from those of control subjects, butthey were nonetheless excluded from the analyses of patientsreceiving sildenafil.
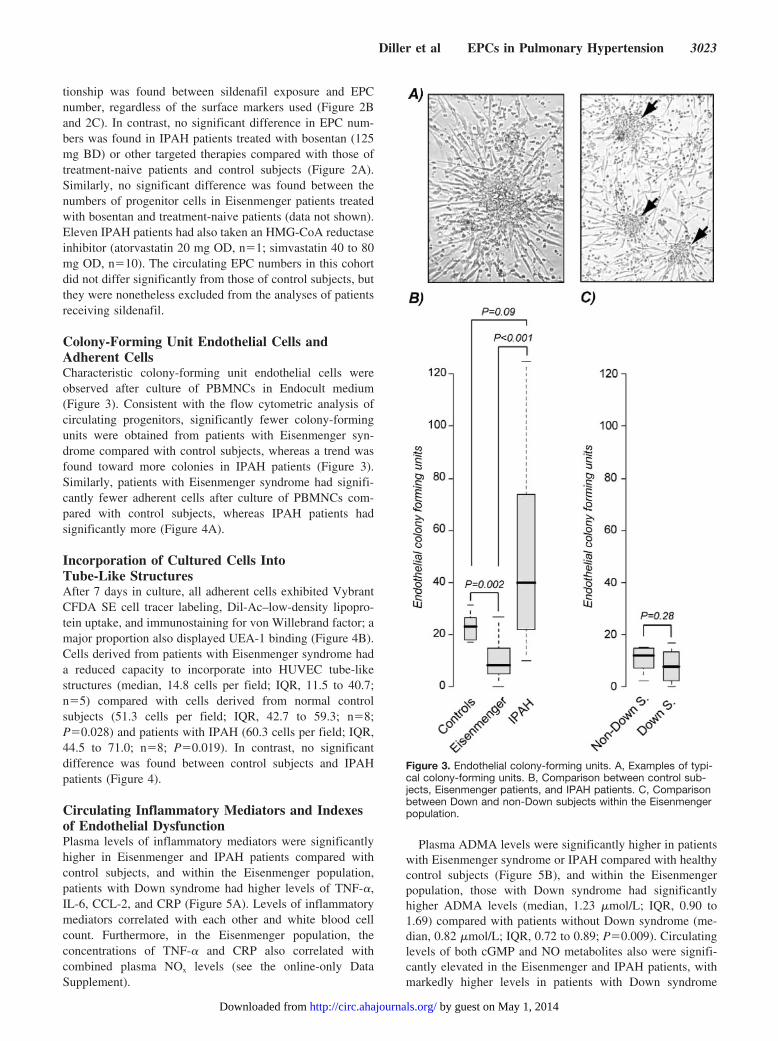
Colony-Forming Unit Endothelial Cells andAdherent CellsCharacteristic colony-forming unit endothelial cells wereobserved after culture of PBMNCs in Endocult medium(Figure 3). Consistent with the flow cytometric analysis ofcirculating progenitors, significantly fewer colony-formingunits were obtained from patients with Eisenmenger syn-drome compared with control subjects, whereas a trend wasfound toward more colonies in IPAH patients (Figure 3).Similarly, patients with Eisenmenger syndrome had signifi-cantly fewer adherent cells after culture of PBMNCs com-pared with control subjects, whereas IPAH patients hadsignificantly more (Figure 4A).
Incorporation of Cultured Cells IntoTube-Like StructuresAfter 7 days in culture, all adherent cells exhibited VybrantCFDA SE cell tracer labeling, Dil-Ac–low-density lipopro-tein uptake, and immunostaining for von Willebrand factor; amajor proportion also displayed UEA-1 binding (Figure 4B).Cells derived from patients with Eisenmenger syndrome hada reduced capacity to incorporate into HUVEC tube-likestructures (median, 14.8 cells per field; IQR, 11.5 to 40.7;n�5) compared with cells derived from normal controlsubjects (51.3 cells per field; IQR, 42.7 to 59.3; n�8;P�0.028) and patients with IPAH (60.3 cells per field; IQR,44.5 to 71.0; n�8; P�0.019). In contrast, no significantdifference was found between control subjects and IPAHpatients (Figure 4).
Circulating Inflammatory Mediators and Indexesof Endothelial DysfunctionPlasma levels of inflammatory mediators were significantlyhigher in Eisenmenger and IPAH patients compared withcontrol subjects, and within the Eisenmenger population,patients with Down syndrome had higher levels of TNF-�,IL-6, CCL-2, and CRP (Figure 5A). Levels of inflammatorymediators correlated with each other and white blood cellcount. Furthermore, in the Eisenmenger population, theconcentrations of TNF-� and CRP also correlated withcombined plasma NOx levels (see the online-only DataSupplement).
Plasma ADMA levels were significantly higher in patientswith Eisenmenger syndrome or IPAH compared with healthycontrol subjects (Figure 5B), and within the Eisenmengerpopulation, those with Down syndrome had significantlyhigher ADMA levels (median, 1.23 �mol/L; IQR, 0.90 to1.69) compared with patients without Down syndrome (me-dian, 0.82 �mol/L; IQR, 0.72 to 0.89; P�0.009). Circulatinglevels of both cGMP and NO metabolites also were signifi-cantly elevated in the Eisenmenger and IPAH patients, withmarkedly higher levels in patients with Down syndrome
Figure 3. Endothelial colony-forming units. A, Examples of typi-cal colony-forming units. B, Comparison between control sub-jects, Eisenmenger patients, and IPAH patients. C, Comparisonbetween Down and non-Down subjects within the Eisenmengerpopulation.
Diller et al EPCs in Pulmonary Hypertension 3023
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from
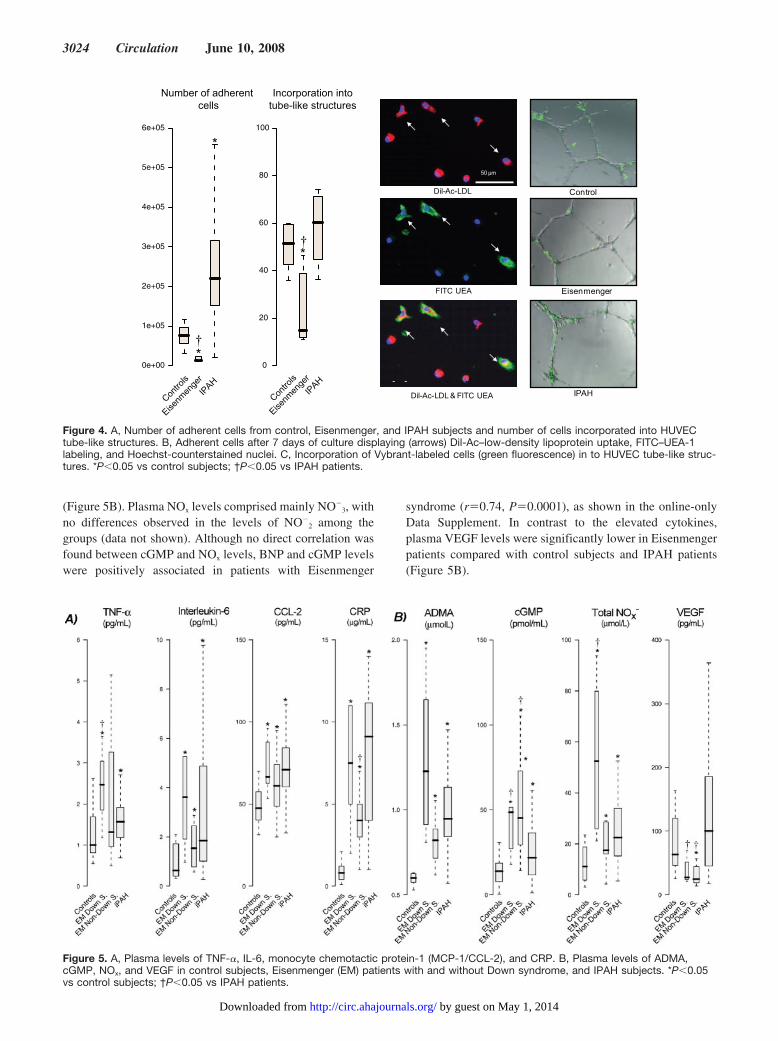
(Figure 5B). Plasma NOx levels comprised mainly NO�3, with
no differences observed in the levels of NO�2 among the
groups (data not shown). Although no direct correlation wasfound between cGMP and NOx levels, BNP and cGMP levelswere positively associated in patients with Eisenmenger
syndrome (r�0.74, P�0.0001), as shown in the online-onlyData Supplement. In contrast to the elevated cytokines,plasma VEGF levels were significantly lower in Eisenmengerpatients compared with control subjects and IPAH patients(Figure 5B).
0
20
40
60
80
100
0e+00
1e+05
2e+05
3e+05
4e+05
5e+05
6e+05
Incorporation intotube-like structures
Number of adherent cells
Contro
lsIP
AH
Eisenm
enge
r
Contro
lsIP
AH
Eisenm
enge
r
*
*
*
†
†
50 µm
FITC-
UEA-1
Dil-
-
Ac-
-
LDL & FITC
-
UEA
-1
Dil--
Ac--
LDL Control
Eisenmenger
IPAH
Figure 4. A, Number of adherent cells from control, Eisenmenger, and IPAH subjects and number of cells incorporated into HUVECtube-like structures. B, Adherent cells after 7 days of culture displaying (arrows) Dil-Ac–low-density lipoprotein uptake, FITC–UEA-1labeling, and Hoechst-counterstained nuclei. C, Incorporation of Vybrant-labeled cells (green fluorescence) in to HUVEC tube-like struc-tures. *P�0.05 vs control subjects; †P�0.05 vs IPAH patients.
Figure 5. A, Plasma levels of TNF-�, IL-6, monocyte chemotactic protein-1 (MCP-1/CCL-2), and CRP. B, Plasma levels of ADMA,cGMP, NOx, and VEGF in control subjects, Eisenmenger (EM) patients with and without Down syndrome, and IPAH subjects. *P�0.05vs control subjects; †P�0.05 vs IPAH patients.
3024 Circulation June 10, 2008
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from
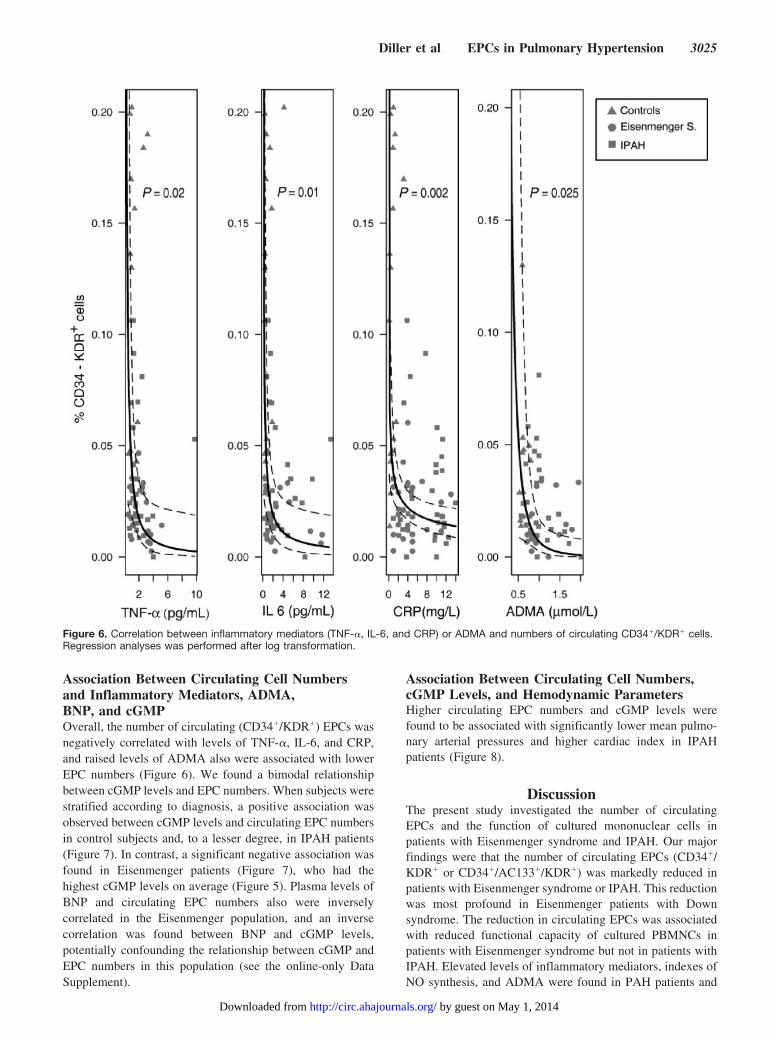
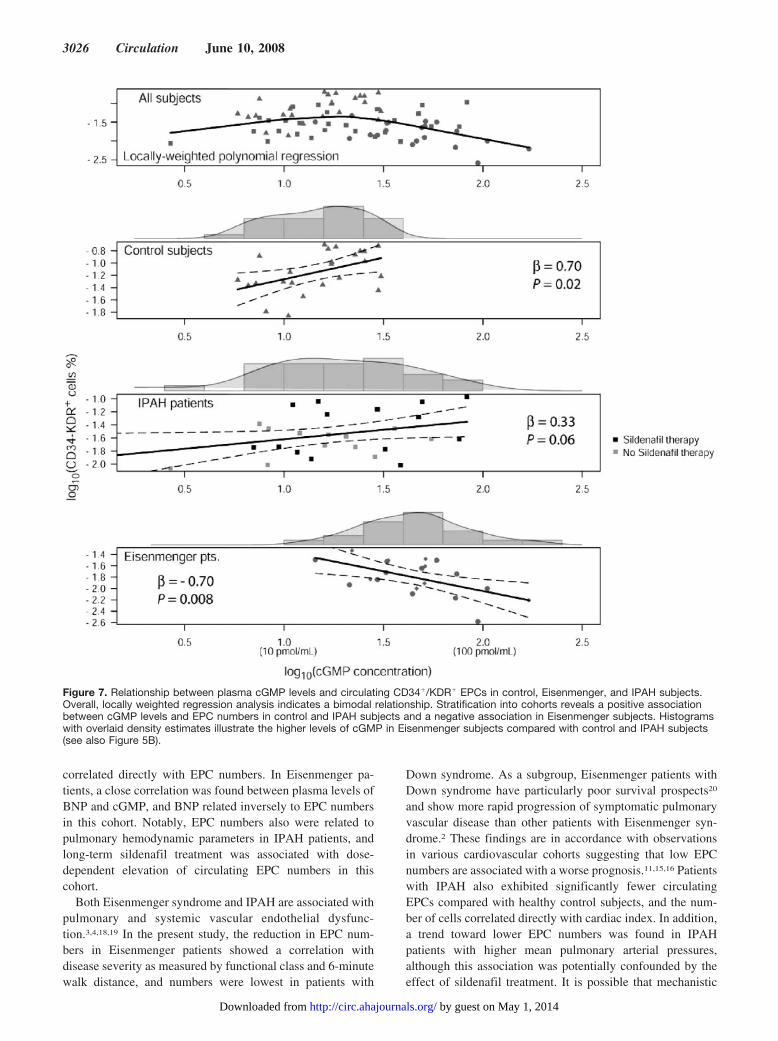
Association Between Circulating Cell Numbersand Inflammatory Mediators, ADMA,BNP, and cGMPOverall, the number of circulating (CD34�/KDR�) EPCs wasnegatively correlated with levels of TNF-�, IL-6, and CRP,and raised levels of ADMA also were associated with lowerEPC numbers (Figure 6). We found a bimodal relationshipbetween cGMP levels and EPC numbers. When subjects werestratified according to diagnosis, a positive association wasobserved between cGMP levels and circulating EPC numbersin control subjects and, to a lesser degree, in IPAH patients(Figure 7). In contrast, a significant negative association wasfound in Eisenmenger patients (Figure 7), who had thehighest cGMP levels on average (Figure 5). Plasma levels ofBNP and circulating EPC numbers also were inverselycorrelated in the Eisenmenger population, and an inversecorrelation was found between BNP and cGMP levels,potentially confounding the relationship between cGMP andEPC numbers in this population (see the online-only DataSupplement).
Association Between Circulating Cell Numbers,cGMP Levels, and Hemodynamic ParametersHigher circulating EPC numbers and cGMP levels werefound to be associated with significantly lower mean pulmo-nary arterial pressures and higher cardiac index in IPAHpatients (Figure 8).
DiscussionThe present study investigated the number of circulatingEPCs and the function of cultured mononuclear cells inpatients with Eisenmenger syndrome and IPAH. Our majorfindings were that the number of circulating EPCs (CD34�/KDR� or CD34�/AC133�/KDR�) was markedly reduced inpatients with Eisenmenger syndrome or IPAH. This reductionwas most profound in Eisenmenger patients with Downsyndrome. The reduction in circulating EPCs was associatedwith reduced functional capacity of cultured PBMNCs inpatients with Eisenmenger syndrome but not in patients withIPAH. Elevated levels of inflammatory mediators, indexes ofNO synthesis, and ADMA were found in PAH patients and
Figure 6. Correlation between inflammatory mediators (TNF-�, IL-6, and CRP) or ADMA and numbers of circulating CD34�/KDR� cells.Regression analyses was performed after log transformation.
Diller et al EPCs in Pulmonary Hypertension 3025
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from
correlated directly with EPC numbers. In Eisenmenger pa-tients, a close correlation was found between plasma levels ofBNP and cGMP, and BNP related inversely to EPC numbersin this cohort. Notably, EPC numbers also were related topulmonary hemodynamic parameters in IPAH patients, andlong-term sildenafil treatment was associated with dose-dependent elevation of circulating EPC numbers in thiscohort.
Both Eisenmenger syndrome and IPAH are associated withpulmonary and systemic vascular endothelial dysfunc-tion.3,4,18,19 In the present study, the reduction in EPC num-bers in Eisenmenger patients showed a correlation withdisease severity as measured by functional class and 6-minutewalk distance, and numbers were lowest in patients with
Down syndrome. As a subgroup, Eisenmenger patients withDown syndrome have particularly poor survival prospects20
and show more rapid progression of symptomatic pulmonaryvascular disease than other patients with Eisenmenger syn-drome.2 These findings are in accordance with observationsin various cardiovascular cohorts suggesting that low EPCnumbers are associated with a worse prognosis.11,15,16 Patientswith IPAH also exhibited significantly fewer circulatingEPCs compared with healthy control subjects, and the num-ber of cells correlated directly with cardiac index. In addition,a trend toward lower EPC numbers was found in IPAHpatients with higher mean pulmonary arterial pressures,although this association was potentially confounded by theeffect of sildenafil treatment. It is possible that mechanistic
Figure 7. Relationship between plasma cGMP levels and circulating CD34�/KDR� EPCs in control, Eisenmenger, and IPAH subjects.Overall, locally weighted regression analysis indicates a bimodal relationship. Stratification into cohorts reveals a positive associationbetween cGMP levels and EPC numbers in control and IPAH subjects and a negative association in Eisenmenger subjects. Histogramswith overlaid density estimates illustrate the higher levels of cGMP in Eisenmenger subjects compared with control and IPAH subjects(see also Figure 5B).
3026 Circulation June 10, 2008
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from

differences (eg, involving chronic cyanosis, erythrocytosis,increased blood viscosity, and associated shear stress) be-tween Eisenmenger and IPAH patients have diverse effectson the number of circulating cells and the function of culturedcells.
The mobilization and function of EPCs are thought to becritically dependent on NO.21 We found that the plasmaconcentration of ADMA was raised in both Eisenmenger andIPAH patients, which is in keeping with previous studies.22,23
Although increased ADMA levels are associated with re-duced NO bioavailability, we observed elevated systemiclevels of stable NO oxidation products, which is consistentwith earlier reports of raised nitrate levels in adults andchildren with congenital heart disease.24 A positive correla-tion was found between cGMP levels and EPC numbers incontrol subjects and IPAH patients, yet despite high NOx andcGMP plasma concentrations, circulating EPCs not only weredeficient in Eisenmenger patients but also exhibited a nega-tive association with plasma cGMP levels. Several potentialexplanations exist for this phenomenon, but NO and thenatriuretic peptides are the major factors stimulating cGMPsynthesis in pulmonary vascular tissue.25 In experimentalanimals, increased pulmonary blood flow and associatedpulmonary hypertension are accompanied by raised circulat-ing levels of BNP and cGMP.26 The levels of these 2 factorsalso were closely correlated in patients with Eisenmengersyndrome, potentially obscuring any direct association be-tween NO and cGMP production. Increased circulating in-flammatory mediators also accompanied raised plasma NOx
levels, and cytokine-inducible NO synthase (NOS) expres-sion has been described in pulmonary arteries and cardiactissues of patients with flow-associated pulmonary hyperten-sion and cyanotic congenital heart disease.27,28 This repre-sents a potentially important source of “high-output” NOproduction that may be associated with oxidative stress andthe production of reactive NO species that attenuate themobilization, function, and survival of EPCs.29,30
Increasing evidence indicates that inflammation has a keyrole in the pathogenesis of PAH. As in earlier studies,31–33 we
found evidence of chronic inflammation with raised plasmalevels of the inflammatory mediators TNF-�, IL-6, andCCL-2. Increased pulmonary production of CCL-2 in PAH ispostulated to act as a chemoattractant for circulating mono-cytes,33 whereas both TNF-� and IL-6 have a negative effecton the number and function of EPCs.11,34,35 We also foundthat plasma CRP was elevated and, together with the inflam-matory cytokines, was negatively associated with the numberof circulating EPCs. In this regard, CRP has been found toattenuate endothelial NOS (eNOS) expression and the mobi-lization, differentiation, and survival of EPCs.36,37
An important finding of our study was that IPAH patientstreated with the PDE5 inhibitor sildenafil exhibited a selec-tive and dose-dependent increase in circulating EPCs. Studiesof erectile dysfunction have indicated that short-term andlong-term PDE5 inhibition with vardenafil and tadalafil,respectively, is associated with increased circulating CD34�/AC133� progenitor cells.38,39 Our study, however, is the firstreport of the effects of a PDE5 inhibitor on EPC numbers inpatients with PAH. Given that eNOS is expressed in culturedEPCs40 and that NO released from organic nitrates canaugment circulating EPCs,21,29 it is possible that, unlike othertargeted therapies for PAH, sildenafil stimulates an intrinsicNO-cGMP pathway, thereby augmenting EPC numbers. It isunclear whether the effect of sildenafil confers a therapeuticadvantage, but active interest exists in using bone marrow–derived cells to treat IPAH.8,41,42 Data obtained from exper-imental models suggest that these cells may induce regener-ation of pulmonary perfusion, leading to improvedhemodynamics and survival.8,42 Furthermore, Wang et al9
recently found that the intravenous infusion of culturedautologous cells in IPAH patients was associated with anaugmented 6-minute walk test distance and pulmonary he-modynamics 12 weeks later. Nonetheless, a number ofunanswered questions about this therapeutic approach re-main, and a simpler alternative strategy may be the pharma-cological manipulation of EPCs in vivo.
We undertook a careful characterization of circulatingprogenitor cells using a variety of surface markers.10–14
Figure 8. Correlation between hemody-namic parameters (mean pulmonary arte-rial pressure [PAP] or cardiac index) andcGMP levels or circulating CD34�/KDR�
cells in patients with IPAH. Parameterswere log transformed.
Diller et al EPCs in Pulmonary Hypertension 3027
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from

Adherent PBMNCs, after short-term culture, have beenwidely studied and previously also classified as EPCs, butthey are now considered to be mainly of monocyte origin.43
Despite their distinct phenotypes,12 the colony-forming ca-pacity and in vitro function of cultured PBMNCs have beenrelated to endothelial dysfunction, cardiovascular symptoms,and outcome.15,44 In the present study, in vitro analysis ofPBMNCs revealed differences between patients similar tothose of circulating CD34�/AC133� cells. Thus, although thenumber and in vitro function of cells from IPAH patientswere similar or even greater than in control subjects, bothwere severely impaired in Eisenmenger patients. It is uncer-tain whether therapeutic intervention in PAH patients influ-ences cultured and circulating cells, but components of theNO-cGMP pathway are present in PBMNCs40,45 and PDE5inhibition for erectile dysfunction associated with augmentedfunction of cultured cells.46
Several cytokines and growth factors are implicated in themobilization and homing of EPCs. Although levels of inflam-matory mediators and ADMA were elevated in both forms ofPAH studied, levels of the angiogenic protein VEGF wereselectively reduced in Eisenmenger patients. VEGF is apotent stimulus for mobilizing bone marrow–derived EPCs,47
and lower levels may be important in this patient group.Indeed, it may be interesting to investigate whether animbalance exists between other angiogenic (eg, IL-8) andantiangiogenic factors (eg, endostatin) in different formsof PAH.
Clinical ImplicationsEndothelial dysfunction is a hallmark of PAH, and recentevidence suggests that bone marrow–derived cells participatein postnatal blood vessel repair and neovascularization.8 Therelative deficiency of circulating EPCs in PAH patients maycontribute to the pulmonary vascular pathology, whereaschronic pharmacological augmentation with PDE5 inhibitorscould offer a novel therapeutic strategy. On the other hand,resistance to apoptosis and proliferation of pulmonary vascu-lar endothelial cells are implicated in the progression ofPAH,48 and incorporation of circulating progenitors may haveadverse long-term consequences. Further studies are neededto understand the therapeutic implications of chronic PDE5inhibition on circulating EPCs in PAH.
Study LimitationsOne of the limitations of this study is that it did notinvestigate the dynamics of circulating EPCs and thus cannotreport on whether differences reflect alterations in EPCmobilization, survival, or tissue uptake. Changes in EPCswith time in individual patients would be of interest, partic-ularly when related to clinical status, measures of vascularendothelial function, and the abundance of EPCs in thepulmonary vasculature.
ConclusionsCirculating EPCs are reduced in patients with Eisenmengersyndrome or IPAH. Circulating EPC numbers correlated withlevels of inflammatory mediators, indexes of NO synthesis,and ADMA production and are related to exercise capacity
and central hemodynamic markers. Treatment with sildenafilis associated with a dose-related increase in EPC numbersand may represent a novel pharmacological means of increas-ing circulating EPCs in PAH patients.
AcknowledgmentsWe thank Sharon Meehan and Carl Harries for their invaluableassistance.
Sources of FundingWe are grateful for support from Actelion UK, the British HeartFoundation, the EU Pulmotension project, IZKF Würzburg, and DFG.
DisclosuresThe employer of Dr Diller, Professor Gatzoulis, and Dr Wort(Imperial College London, UK) has received an unrestricted educa-tional grant from Actelion, UK. Dr Diller also has received travelsupport and honoraria from Actelion, UK, Encysive, UK, andSchering, Germany. Professor Wilkins’ employer (Imperial CollegeLondon, UK) has received unrestricted support from Pfizer, UK, andActelion, UK for research studies. He also has received honorariaand travel support from Pfizer, Actelion, GSK, and Encysive, UK.Dr Wharton’s employer (Imperial College London, UK) has receivedunrestricted support from Pfizer, and he has received honoraria andtravel support from Pfizer and Encysive, UK. Dr Bauersachs hasreceived honoraria and grant support for experimental studies fromPfizer, Germany. Dr Gibbs’ and Dr Howard’s institution (Hammer-smith Hospital) has received unrestricted support from Actelion; theyalso have received honoraria and travel support from Actelion,Pfizer, GSK, Schering, and Encysive, UK. The other authors reportno conflicts.
References1. D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH,
Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT.Survival in patients with primary pulmonary hypertension. Resultsfrom a national prospective registry. Ann Intern Med. 1991;115:343–349.
2. Diller GP, Gatzoulis MA. Pulmonary vascular disease in adults withcongenital heart disease. Circulation. 2007;115:1039–1050.
3. Celermajer DS, Cullen S, Deanfield JE. Impairment of endothelium-dependent pulmonary artery relaxation in children with congenital heartdisease and abnormal pulmonary hemodynamics. Circulation. 1993;87:440–446.
4. Haworth SG. Role of the endothelium in pulmonary arterial hypertension.Vascul Pharmacol. 2006;45:317–325.
5. Khakoo AY, Finkel T. Endothelial progenitor cells. Annu Rev Med.2005;56:79–101.
6. Thum T, Tsikas D, Stein S, Schultheiss M, Eigenthaler M, Anker SD,Poole-Wilson PA, Ertl G, Bauersachs J. Suppression of endothelial pro-genitor cells in human coronary artery disease by the endogenous nitricoxide synthase inhibitor asymmetric dimethylarginine. J Am CollCardiol. 2005;46:1693–1701.
7. Shantsila E, Watson T, Lip GY. Endothelial progenitor cells in cardio-vascular disorders. J Am Coll Cardiol. 2007;49:741–752.
8. Zhao YD, Courtman DW, Deng Y, Kugathasan L, Zhang Q, Stewart DJ.Rescue of monocrotaline-induced pulmonary arterial hypertension usingbone marrow-derived endothelial-like progenitor cells: efficacy ofcombined cell and eNOS gene therapy in established disease. Circ Res.2005;96:442–450.
9. Wang XX, Zhang FR, Shang YP, Zhu JH, Xie XD, Tao QM, Zhu JH,Chen JZ. Transplantation of autologous endothelial progenitor cells maybe beneficial in patients with idiopathic pulmonary arterial hypertension:a pilot randomized controlled trial. J Am Coll Cardiol. 2007;49:1566–1571.
10. George J, Shmilovich H, Deutsch V, Miller H, Keren G, Roth A. Com-parative analysis of methods for assessment of circulating endothelialprogenitor cells. Tissue Eng. 2006;12:331–335.
3028 Circulation June 10, 2008
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from
11. Valgimigli M, Rigolin GM, Fucili A, Porta MD, Soukhomovskaia O,Malagutti P, Bugli AM, Bragotti LZ, Francolini G, Mauro E, CastoldiG, Ferrari R. CD34� and endothelial progenitor cells in patients withvarious degrees of congestive heart failure. Circulation. 2004;110:1209 –1212.
12. Case J, Mead LE, Bessler WK, Prater D, White HA, Saadatzadeh MR,Bhavsar JR, Yoder MC, Haneline LS, Ingram DA. HumanCD34�AC133�VEGFR-2� cells are not endothelial progenitor cellsbut distinct, primitive hematopoietic progenitors. Exp Hematol. 2007;35:1109–1118.
13. Kondo T, Hayashi M, Takeshita K, Numaguchi Y, Kobayashi K, Iino S,Inden Y, Murohara T. Smoking cessation rapidly increases circulatingprogenitor cells in peripheral blood in chronic smokers. ArteriosclerThromb Vasc Biol. 2004;24:1442–1447.
14. Numaguchi Y, Sone T, Okumura K, Ishii M, Morita Y, Kubota R,Yokouchi K, Imai H, Harada M, Osanai H, Kondo T, Murohara T. Theimpact of the capability of circulating progenitor cell to differentiate onmyocardial salvage in patients with primary acute myocardial infarction.Circulation. 2006;114:114–119.
15. Hill JM, Zalos G, Halcox JP, Schenke WH, Waclawiw MA, QuyyumiAA, Finkel T. Circulating endothelial progenitor cells, vascular function,and cardiovascular risk. N Engl J Med. 2003;348:593–600.
16. Werner N, Kosiol S, Schiegl T, Ahlers P, Walenta K, Link A, Bohm M,Nickenig G. Circulating endothelial progenitor cells and cardiovascularoutcomes. N Engl J Med. 2005;353:999–1007.
17. Connelly L, Madhani M, Hobbs AJ. Resistance to endotoxic shock inendothelial nitric-oxide synthase (eNOS) knock-out mice: a pro-inflammatory role for eNOS-derived NO in vivo. J Biol Chem. 2005;280:10040–10046.
18. Oechslin E, Kiowski W, Schindler R, Bernheim A, Julius B, Brunner-LaRocca HP. Systemic endothelial dysfunction in adults with cyanoticcongenital heart disease. Circulation. 2005;112:1106–1112.
19. Hughes R, Tong J, Oates C, Lordan J, Corris PA. Evidence for systemicendothelial dysfunction in patients and first-order relatives with pulmo-nary arterial hypertension. Chest. 2005;128(suppl):617S.
20. Yang Q, Rasmussen SA, Friedman JM. Mortality associated with Down’ssyndrome in the USA from 1983 to 1997: a population-based study.Lancet. 2002;359:1019–1025.
21. Aicher A, Heeschen C, Mildner-Rihm C, Urbich C, Ihling C, Technau-Ihling K, Zeiher AM, Dimmeler S. Essential role of endothelial nitricoxide synthase for mobilization of stem and progenitor cells. Nat Med.2003;9:1370–1376.
22. Kielstein JT, Bode-Boger SM, Hesse G, Martens-Lobenhoffer J, TakacsA, Fliser D, Hoeper MM. Asymmetrical dimethylarginine in idiopathicpulmonary arterial hypertension. Arterioscler Thromb Vasc Biol. 2005;25:1414–1418.
23. Gorenflo M, Zheng C, Werle E, Fiehn W, Ulmer HE. Plasma levels ofasymmetrical dimethyl-L-arginine in patients with congenital heartdisease and pulmonary hypertension. J Cardiovasc Pharmacol. 2001;37:489–492.
24. Han TH, Perloff JK, Liao JC. Nitric oxide metabolism in adults withcyanotic congenital heart disease. Am J Cardiol. 2007;99:691–695.
25. Zhao L, Mason NA, Strange JW, Walker H, Wilkins MR. Beneficialeffects of phosphodiesterase 5 inhibition in pulmonary hypertension areinfluenced by natriuretic peptide activity. Circulation. 2003;107:234–237.
26. Oishi P, Sharma S, Grobe A, Azakie A, Harmon C, Johengen MJ, Hsu JH,Fratz S, Black SM, Fineman JR. Alterations in cGMP, soluble guanylatecyclase, phosphodiesterase 5, and B-type natriuretic peptide induced bychronic increased pulmonary blood flow in lambs. Pediatr Pulmonol.2007;42:1057–1071.
27. Ferreiro CR, Chagas AC, Carvalho MH, Dantas AP, Jatene MB, BentoDe Souza LC, Lemos Da Luz P. Influence of hypoxia on nitric oxidesynthase activity and gene expression in children with congenital heartdisease: a novel pathophysiological adaptive mechanism. Circulation.2001;103:2272–2276.
28. Berger RM, Geiger R, Hess J, Bogers AJ, Mooi WJ. Altered arterialexpression patterns of inducible and endothelial nitric oxide synthase inpulmonary plexogenic arteriopathy caused by congenital heart disease.Am J Respir Crit Care Med. 2001;163:1493–1499.
29. Thum T, Fraccarollo D, Thum S, Schultheiss M, Daiber A, Wenzel P,Munzel T, Ertl G, Bauersachs J. Differential effects of organic nitrates onendothelial progenitor cells are determined by oxidative stress. ArteriosclerThromb Vasc Biol. 2007;27:748–754.
30. DiFabio JM, Thomas GR, Zucco L, Kuliszewski MA, Bennett BM,Kutryk MJ, Parker JD. Nitroglycerin attenuates human endothelial pro-genitor cell differentiation, function, and survival. J Pharmacol Exp Ther.2006;318:117–123.
31. Humbert M, Monti G, Brenot F, Sitbon O, Portier A, Grangeot-Keros L,Duroux P, Galanaud P, Simonneau G, Emilie D. Increased interleukin-1and interleukin-6 serum concentrations in severe primary pulmonaryhypertension. Am J Respir Crit Care Med. 1995;151:1628–1631.
32. Itoh T, Nagaya N, Ishibashi-Ueda H, Kyotani S, Oya H, Sakamaki F, KimuraH, Nakanishi N. Increased plasma monocyte chemoattractant protein-1 levelin idiopathic pulmonary arterial hypertension. Respirology. 2006;11:158–163.
33. Sanchez O, Marcos E, Perros F, Fadel E, Tu L, Humbert M, Dartevelle P,Simonneau G, Adnot S, Eddahibi S. Role of endothelium-derived CCchemokine ligand 2 in idiopathic pulmonary arterial hypertension. Am JRespir Crit Care Med. 2007;176:1041–1047.
34. Herbrig K, Haensel S, Oelschlaegel U, Pistrosch F, Foerster S, PassauerJ. Endothelial dysfunction in patients with rheumatoid arthritis is asso-ciated with a reduced number and impaired function of endothelial pro-genitor cells. Ann Rheum Dis. 2006;65:157–163.
35. Seeger FH, Haendeler J, Walter DH, Rochwalsky U, Reinhold J, UrbichC, Rossig L, Corbaz A, Chvatchko Y, Zeiher AM, Dimmeler S. p38mitogen-activated protein kinase downregulates endothelial progenitorcells. Circulation. 2005;111:1184–1191.
36. Schwartz R, Osborne-Lawrence S, Hahner L, Gibson LL, Gormley AK,Vongpatanasin W, Zhu W, Word RA, Seetharam D, Black S, Samols D,Mineo C, Shaul PW. C-reactive protein downregulates endothelial nosynthase and attenuates reendothelialization in vivo in mice. Circ Res.2007;100:1452–1459.
37. Verma S, Kuliszewski MA, Li S-H, Szmitko PE, Zucco L, Wang C-H,Badiwala MV, Mickle DAG, Weisel RD, Fedak PWM, Stewart DJ,Kutryk MJB. C-reactive protein attenuates endothelial progenitor cellsurvival, differentiation, and function: further evidence of a mechanisticlink between c-reactive protein and cardiovascular disease. Circulation.2004;109:2058–2067.
38. Foresta C, Caretta N, Lana A, De Toni L, Biagioli A, Vinanzi C, FerlinA. Relationship between vascular damage degrees and endothelial pro-genitor cells in patients with erectile dysfunction: effect of vardenafiladministration and PDE5 expression in the bone marrow. Eur Urol.2007;51:1411–1417.
39. Foresta C, Ferlin A, De Toni L, Lana A, Vinanzi C, Galan A, Caretta N.Circulating endothelial progenitor cells and endothelial function afterchronic Tadalafil treatment in subjects with erectile dysfunction. Int JImpot Res. 2006;18:484–488.
40. Hur J, Yoon CH, Kim HS, Choi JH, Kang HJ, Hwang KK, Oh BH, LeeMM, Park YB. Characterization of two types of endothelial progenitorcells and their different contributions to neovasculogenesis. ArteriosclerThromb Vasc Biol. 2004;24:288–293.
41. Stewart DJ, Zhao YD, Courtman DW, Nagaya N, Horio T, Miyatake K,Chiba Y, Kangawa K, Kanda M, Hino J, Harada-Shiba M, Okumura H,Mochizuki N, Mori H, Uematsu M, Fukuyama N, Tabata Y, Nishioka K,Hara H, Asahara T. Cell therapy for pulmonary hypertension: what is thetrue potential of endothelial progenitor cells? Circulation. 2004;109:e172–e173.
42. Nagaya N, Kangawa K, Kanda M, Uematsu M, Horio T, Fukuyama N,Hino J, Harada-Shiba M, Okumura H, Tabata Y, Mochizuki N, ChibaY, Nishioka K, Miyatake K, Asahara T, Hara H, Mori H. Hybridcell-gene therapy for pulmonary hypertension based on phagocytosingaction of endothelial progenitor cells. Circulation. 2003;108:889 – 895.
43. Prater DN, Case J, Ingram DA, Yoder MC. Working hypothesis toredefine endothelial progenitor cells. Leukemia. 2007;21:1141–1149.
44. Asahara T, Murohara T, Sullivan A, Silver M, van der Zee R, Li T,Witzenbichler B, Schatteman G, Isner JM. Isolation of putative progenitorendothelial cells for angiogenesis. Science. 1997;275:964–967.
45. Mateos-Caceres PJ, Garcia-Cardoso J, Lapuente L, Zamorano-Leon JJ,Sacristan D, de Prada TP, Calahorra J, Macaya C, Vela-Navarrete R,Lopez-Farre AJ. Soluble guanylate cyclase beta1-subunit expression isincreased in mononuclear cells from patients with erectile dysfunction. IntJ Impot Res. 2006;18:432–437.
46. Bocchio M, Pelliccione F, Passaquale G, Mihalca R, Necozione S,Desideri G, Francavilla F, Ferri C, Francavilla S. Inhibition of phospho-diesterase type 5 with tadalafil is associated to an improved activity ofcirculating angiogenic cells in men with cardiovascular risk factors anderectile dysfunction. Atherosclerosis. 2008;196:313–319.
Diller et al EPCs in Pulmonary Hypertension 3029
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from

47. Asahara T, Takahashi T, Masuda H, Kalka C, Chen D, Iwaguro H, InaiY, Silver M, Isner JM. VEGF contributes to postnatal neovascular-ization by mobilizing bone marrow-derived endothelial progenitor cells.EMBO J. 1999;18:3964–3972.
48. Levy M, Maurey C, Celermajer DS, Vouhe PR, Danel C, Bonnet D,Israel-Biet D. Impaired apoptosis of pulmonary endothelial cells is asso-ciated with intimal proliferation and irreversibility of pulmonary hyper-tension in congenital heart disease. J Am Coll Cardiol. 2007;49:803–810.
CLINICAL PERSPECTIVEImpaired endothelial homeostasis underlies the pathophysiology of pulmonary arterial hypertension (PAH). We speculatedthat PAH patients are deficient in circulating endothelial progenitor cells (EPCs), potentially contributing to endothelialdysfunction and disease progression. Forty-one patients with Eisenmenger syndrome (13 with Down syndrome), 55 withidiopathic PAH, and 47 healthy control subjects were recruited. The number of EPCs was low in Eisenmenger patientscompared with healthy control subjects, and those with Down syndrome displayed even fewer EPCs. Reductions in EPCnumbers correlated with functional class, 6-minute walk distance, and plasma brain-type natriuretic peptide levels.Idiopathic PAH patients had reduced numbers of EPCs, and the number of circulating EPCs correlated with invasivehemodynamic parameters in this cohort. Levels of immune inflammatory markers, cGMP, stable nitric oxide oxidationproducts, and asymmetric dimethylarginine were abnormal in patients with PAH and related to numbers of EPCs. Withinthe idiopathic PAH population, treatment with the phosphodiesterase inhibitor sildenafil was associated with adose-dependent rise in EPC numbers, resulting in levels consistently above those found with other therapies. In conclusion,circulating EPC numbers are reduced in 2 well-characterized forms of PAH, which also exhibit raised levels ofinflammatory mediators. Sildenafil treatment may represent a pharmacological means of increasing circulating EPCnumbers long-term.
3030 Circulation June 10, 2008
by guest on May 1, 2014http://circ.ahajournals.org/Downloaded from
Related Documents











