D. Vizza, Fabio Naro, Susanna Morano, Francesco Fedele and Andrea Lenzi Elisa Giannetta, Andrea M. Isidori, Nicola Galea, Iacopo Carbone, Elisabetta Mandosi, Carmine Myocardial Tagging A Randomized, Controlled Clinical Trial Using Magnetic Resonance Imaging With Chronic Inhibition of cGMP Phosphodiesterase 5A Improves Diabetic Cardiomyopathy : Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Circulation doi: 10.1161/CIRCULATIONAHA.111.063412 2012;125:2323-2333; originally published online April 11, 2012; Circulation. http://circ.ahajournals.org/content/125/19/2323 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://circ.ahajournals.org/content/suppl/2012/04/11/CIRCULATIONAHA.111.063412.DC1.html Data Supplement (unedited) at: http://circ.ahajournals.org//subscriptions/ is online at: Circulation Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer this process is available in the click Request Permissions in the middle column of the Web page under Services. Further information about Office. Once the online version of the published article for which permission is being requested is located, can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Circulation in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: at ARCURI ATT LISTA on November 12, 2012 http://circ.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

D. Vizza, Fabio Naro, Susanna Morano, Francesco Fedele and Andrea LenziElisa Giannetta, Andrea M. Isidori, Nicola Galea, Iacopo Carbone, Elisabetta Mandosi, Carmine
Myocardial TaggingA Randomized, Controlled Clinical Trial Using Magnetic Resonance Imaging With
Chronic Inhibition of cGMP Phosphodiesterase 5A Improves Diabetic Cardiomyopathy :
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.111.063412
2012;125:2323-2333; originally published online April 11, 2012;Circulation.
http://circ.ahajournals.org/content/125/19/2323World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2012/04/11/CIRCULATIONAHA.111.063412.DC1.htmlData Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

Imaging
Chronic Inhibition of cGMP Phosphodiesterase 5A ImprovesDiabetic Cardiomyopathy
A Randomized, Controlled Clinical Trial Using Magnetic ResonanceImaging With Myocardial Tagging
Elisa Giannetta, MD, PhD*; Andrea M. Isidori, MD, PhD*; Nicola Galea, MD; Iacopo Carbone, MD, PhD;Elisabetta Mandosi, MD, PhD; Carmine D. Vizza, MD, PhD; Fabio Naro, MD, PhD;Susanna Morano, MD, PhD; Francesco Fedele, MD, PhD; Andrea Lenzi, MD, PhD
Background—cGMP phosphodiesterase type 5 protein is upregulated in myocardial hypertrophy. However, it has neverbeen ascertained whether phosphodiesterase type 5 inhibition exerts an antiremodeling effect in nonischemic heartdisease in humans. We explored the cardioreparative properties of a selective phosphodiesterase type 5 inhibitor,sildenafil, in a model of diabetic cardiomyopathy.
Methods and Results—Fifty-nine diabetic men (60.3�7.4 years) with cardiac magnetic resonance imaging consistent withnonischemic, nonfailing diabetic cardiomyopathy (reduced circumferential strain [�], �12.6�3.1%; increased leftventricular [LV] torsion [�], 18.4�4.6°; and increased ratio of LV mass to volume, 2.1�0.5 g/mL) were randomizedto receive sildenafil or placebo (100 mg/d). At baseline, the metabolic indices were correlated with torsion, strain,N-terminal pro–B-type natriuretic peptide, vascular endothelial growth factor, monocyte chemotactic protein-1, andblood pressure. After 3 months, sildenafil produced a significant improvement compared with placebo in LV torsion(��: sildenafil, �3.89�3.11° versus placebo, 2.13�2.35°; P�0.001) and strain (��: sildenafil, �3.30�1.86% versusplacebo, 1.22�1.84%; P�0.001). Sildenafil-induced improvement of LV contraction was accompanied by consistentchanges in chamber geometry and performance, with a 6.5�11% improvement in mass-to-volume ratio over placebo(P�0.021). Monocyte chemotactic protein-1 and transforming growth factor-� were the only markers affected by activetreatment (�monocyte chemotactic protein-1: �75.30�159.28 pg/mL, P�0.032; �transforming growth factor-�:5.26�9.67 ng/mL, P�0.009). No changes were found in endothelial function, afterload, or metabolism.
Conclusions—The early features of diabetic cardiomyopathy are LV concentric hypertrophy associated with alteredmyocardial contraction dynamics. Chronic phosphodiesterase type 5 inhibition, at this stage, has an antiremodelingeffect, resulting in improved cardiac kinetics and circulating markers. This effect is independent of any othervasodilatory or endothelial effects and is apparently exerted through a direct intramyocardial action.
Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00692237.(Circulation. 2012;125:2323-2333.)
Key Words: cardiac magnetic resonance imaging � diabetes mellitus type 2 � diabetic diastolic heart failure� fibrosis � phosphodiesterase inhibitors heart failure
Inhibition of phosphodiesterase type 5 (PDE5) exerts arelaxant effect on the smooth muscle cells of the trabecular
structures of the corpora cavernosa, resulting in improvederections. More recently, PDE5 inhibitors have been claimedto offer cardioprotective effects. In vitro and in vivo studiesin mice have shown that cGMP and its downstream proteinkinase G are signals common to most pathways activated in
cardiac hypertrophy.1 Low levels of PDE5 protein andcGMP-mediated activation of protein kinase G have beenfound in unstimulated hearts.2 However, in isolated mousecardiomyocytes treated with �-agonists2 and in hypertrophichearts,3 PDE5 expression is enhanced.4 These findings sug-gest that cGMP might block hypertrophic signals and thatPDE5 inhibitors might act directly within the cardiomyo-
Received August 30, 2011; accepted March 26, 2012.From the Departments of Experimental Medicine (E.G., A.M.I., A.L.); Radiology, Oncology, and Pathology (N.G., I.C.); Internal Medicine and
Medical Specialties (E.M., S.M.); Cardiovascular and Respiratory Diseases (C.D.V., F.F.); and Anatomy, Histology, Legal Medicine, and LocomotorSystem (F.N.), Sapienza University of Rome, Rome, Italy.
*Drs Giannetta and Isidori contributed equally to this work.The online-only Data Supplement is available with this article at http://circ.ahajournals.org/lookup/suppl/doi:10.1161/CIRCULATIONAHA.111.063412/-/
DC1.Correspondence to Andrea M. Isidori, MD, PhD, Department of Experimental Medicine, Sapienza University of Rome, Viale del Policlinico 155,
00161 Rome, Italy. E-mail [email protected]© 2012 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.111.063412
2323 at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

cytes,3 independently of any concomitant endothelial orvasoactive effects, to regulate myocardial growth andcontractility.5
Clinical Perspective on p 2333In mouse models, chronic PDE5 inhibition reverts the left
ventricular (LV) hypertrophy and fibrosis induced by exper-imental aortic coarctation,3,6 protects against ischemia/reper-fusion injury7 and doxorubicin-induced apoptosis,8 and pre-vents cardiac remodeling in hypertrophic cardiomyopathyinduced by nitric oxide synthase blockers (NG-nitro-L-arginine).9,10 However, although there are abundant experi-mental data in animals, few studies have been conducted inhumans. PDE5 protein expression, which is almost undetect-able in normal right and left ventricles of the human heart, isstrongly upregulated in biopsy samples of the myocardium ofhypertrophied chambers.11 Very recently, a study of patientswith heart failure of various etiologies found that PDE5inhibitors improved LV function and geometry.12
The effects of PDE5 inhibition have never been explored inhumans with nonischemic heart disease. Moreover, the afore-mentioned studies were not designed to distinguish betweenan intrinsic cardiac action and indirect secondary changes dueto PDE5-induced afterload or endothelial or vasodilatoryeffects. For this reason, we conducted a prospective random-ized controlled clinical trial designed to document intrinsiccardiac changes associated with chronic PDE5 inhibition. Thesystolic and diastolic dysfunction characteristic of diabetic
cardiomyopathy in type 2 diabetes mellitus (T2DM) offeredthe ideal model. In diabetic cardiomyopathy, chamber remod-eling may occur independently of ischemic heart disease,hypertension, or other macrovascular complications.13 Beforechamber dilation and failure, the signs of diabetic cardiomy-opathy are a worsening of the cardiac kinetic rate, impairedshortening of cardiac fibers, and an increase in cardiactorsion.13–15 These changes can be accurately measured bycardiac magnetic resonance (CMR) imaging, a reproducible,noninvasive method to assess compensatory ventricular re-modeling and hypertrophy and quantify kinetic parameters byradiofrequency tagging.13,16–18
In the first registered randomized clinical trial designed toinvestigate the putative antiremodeling effect of PDE5 inhib-itors by CMR imaging, we explored the systemic and cardiaceffects of the administration of sildenafil, a potent PDE5inhibitor, at 100 mg/d for 3 months in a large cohort ofpatients with diabetic cardiomyopathy.
Methods
SubjectsEligible men were recruited from the outpatient clinics of PoliclinicoUmberto I, Sapienza University Hospital of Rome between 2008 and2009. The inclusion criteria were as follows: age 35 to 75 years;T2DM �1 year; hemoglobin A1c (HbA1c) �10%; normal bloodpressure (BP) or treated hypertension with achievement of a target of�130/80 mm Hg; and body mass index �40. The exclusion criteriawere as follows: use of exogenous insulin, thiazolidinediones, or
Figure 1. Study flowchart. PDE5i indicates phosphodiesterase type 5 inhibitor; stress-echo, echocardiographic test on cycle ergometer;CMR, cardiac magnetic resonance; 24-hour BP, 24-hour blood pressure monitoring; and FMD, flow-mediated vasodilation.
2324 Circulation May 15, 2012
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

spironolactone; prior or current use of PDE5 inhibitors; substanceabuse; history of cardiovascular disease, proliferative retinopathy, orautonomic neuropathy; symptoms or signs of ischemic heart diseaseduring cardiac evaluations at enrollment (Figure 1; stress ECGand/or 2-dimensional Doppler echocardiography, visit 1; CMRimaging, visit 2); and contraindications to sildenafil use or CMRimaging. Concomitant medications (eg, antihypertensives, statins,oral antidiabetic medications) could not be changed between the 3months before the study and 1 month after its completion. Allsubjects gave their written informed consent. The protocol wasapproved by the hospital ethics committee.
Adverse Events and ComplianceAdverse event reports were collected through monthly follow-upvisits and weekly telephone interviews. Adherence was monitoredthrough a monthly pill count.
Study DesignThis was a randomized, double-blind (subjects/outcome assessors),placebo-controlled study in T2DM patients. All patients were ran-domized to receive 100 mg/d sildenafil (25 mg at 8 AM plus 25 mgat 4 PM plus 50 mg at 10 PM) or placebo in identical-looking capsulesfor 3 months. The allocation list was produced with the use ofdedicated software by permuted-block randomization with 1:1 allo-cation with randomly sized blocks.4–8 Randomization was notstratified. Allocation was blinded by use of anonymous drug vials
with a 4-character alphanumeric code. The sequentially numberedsealed envelopes containing the allocation codes were kept by apharmacist staff member not involved in the study and were given tothe physicians after the informed consent was signed. Codes werebroken and unblinded to patients and care providers 3 months afterthe last patient completion. Blinding was maintained for outcomeassessors (ie, the radiologists involved in CMR image analysis andthe biologists) until the full statistical analysis had been completed.Patients were monitored monthly for the entire study duration (5months; Figure 1). The study was designed, conducted, and moni-tored by the study team without industry support and was conductedin collaboration with the departments of experimental medicine andendocrinology; radiology, oncology, and pathology; cardiovascularand respiratory sciences; and internal medicine and medical special-ties of Policlinico Umberto I, Sapienza University Hospital of Rome.
Diagnostic ProceduresSymptom-limited stress echocardiography (Philips HDI 5000) wasperformed (C.D.V.) at visit 1. CMR imaging studies were performedwith a 1.5-T clinical magnetic resonance imaging system (Avanto,Siemens, Healthcare Solutions, Erlangen, Germany) with an8-element phased-array surface receiver coil and ECG triggering.Scout images were used to determine the cardiac axes. Breath-holdbalanced, steady state free precession (cine magnetic resonance)sequences were taken with a stack of 10 to 12 short-axis slicescovering the whole LV from base to apex for the assessment ofventricular volumes (repetition time/echo time, 5.2/1.2 ms; field ofview, 340–400 mm; matrix, 256�256; slice thickness, 8 mm;interslice gap, 0). A grid generated by saturating orthogonal tags(CMR-tagged imaging; Figure 2A and 2B) was then applied toevaluate myocardial strain and torsion (repetition time/echo time,4.3/2.4 ms; field of view, 340–400 mm; matrix, 187�256; flipangle, 15°; slice thickness, 7 mm; band thickness, 7 mm). Breath-
Figure 2. A and B, Cardiac magnetic resonance–tagged imag-ing of apical left ventricular slice at end-diastole (A) and end-systole (B) with superimposed grid tag used for quantification ofmyocardial torsion and strain. C and D, Harmonic phase torsionanalysis by application of the tracking circle at baseline (C) andapical (D) left ventricle; shown are epicardium (green), mesocar-dium (orange), and endocardium (yellow). Rotation of the linesconnecting the dots (white radius) is plotted over time, assess-ing local myocardial deformation. E and F, Harmonic phasestrain analysis with color map attributed to tissue shortening inmidregion of the left ventricle: note less strain in green (hypoki-netic tissue; E) and better strain in blue (normokinetic tissue; F).
Table 1. Characteristics of the 59 Randomized Subjects
Characteristic Sildenafil Placebo
No. of patients 30 29
Age, y 60.7�7.6 60.2�8.3
Duration of diabetes mellitus, y 6.7�5.5 6.2�5.7
Body mass index 28.4�4.9 27.9�4.3
HOMA index 6.9�5.6 6.6�5.92
HbA1c, % 7.8�1.3 7.5�1.4
HDL cholesterol, mmol/L 1.1�0.2 1.1�0.3
Triglycerides, mmol/L 1.6�0.9 1.6�1.1
Echo EF, % 55.1�9.7 52.9�9.5
PASP, mm Hg 23.7�4.4 24.2�5.3
Treatment, n (%)
Metformin 26 (85) 21 (74)
Secretagogues 15 (49) 12 (41)
Statins 14 (47) 14 (47)
ACE inhibitors 7 (23) 8 (27)
AT1 blockers 7 (23) 5 (17)
Calcium channel blockers 5 (17) 4 (14)
�-blockers 3 (10) 3 (10)
AT1 blockers�diuretics 4 (13) 3 (10)
Diuretics 1 (3) 1 (3)
Values are mean�SD or number (%). HOMA indicates homeostasis modelassessment; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; echo EF,ejection fraction measured on stress echocardiography; PASP, pulmonaryartery systolic pressure; ACE, angiotensin-converting enzyme; and AT1,angiotensin II type 1.
Giannetta et al Sildenafil Improves Diabetic Cardiomyopathy 2325
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

hold T1-weighted contrast-enhanced inversion-recovery segmentedgradient-echo sequence was performed 10 to 15 minutes after theintravenous injection of contrast agent (0.2 mmol/kg gadolinium-BOPTA; Multihance, Bracco, Milan, Italy) to establish the presence,location, and extent of areas of increased signal intensity (�5 SDabove the normal myocardial signal intensity) due to myocardialregional fibrosis (late gadolinium enhancement imaging). All se-quences were performed in vertical and horizontal long- and short-axis orientations. LV end-diastolic volume (EDV), end-systolicvolume, stroke volume, cardiac output, ejection fraction (EF), andLV mass (LVM) were measured on cine magnetic resonance imagesand indexed to body surface area. Interventricular septum thick-ness and maximum LV transverse diameter were also measured. CMRanalysis was performed independently at visits 2 (time 0) and 5 (�3months) by 2 experienced operators (N.G. and I.C.), who were blindedto the patients’ clinical data.
Ventricular Torsion and StrainCardiac kinetics, deformation, torsion, recoil, and strain were mea-sured by myocardial tagging. Tags are noninvasive markers that areimprinted on CMR slices, producing signals of varying intensity.16,19
Tracking of these signals through the cardiac cycle generates vectorsthat can be used to quantify movement. Radial tag displacement isused to measure torsion, and deformation of the grid pattern is usedto calculate strain (�, %). Tags are applied at end-diastole, andimages are acquired every 40 ms thereafter, triggered by ECG waves(Figure 2C to 2F). Tagged images were processed with the use ofcustom-automated, operator-independent software (Harmonic Phasetechnology, HARP 1.0, Diagnosoft Inc, Palo Alto, CA).
Customization was limited to tracing of the endocardial andepicardial contours on a single reference cardiac phase for each slice.The program automatically generated and applied 24 points for bothcontours and propagated them to all cardiac phases. The angle ofrotation between the base and apex was calculated as the averagerotation of all points in the slice with respect to the LV centroid. Theglobal LV torsion (�, °) was calculated as the difference between thecounterclockwise (positive) rotation at the apex and clockwise
rotation at the base: ���apex��base. The maximum systolic torsion(�max) was calculated as the largest magnitude of � during the cardiaccycle.19,20 The directional reversal of systolic torsion during diastole,recoil (untwisting), was described with the use of the equation recoilrate (RR)�d�ut/dt, defined as the slope of the linear regression ofrecoil versus time during the first 100 ms after peak torsion (withdata from 5 frames). Calculated in this way, the RR was thennormalized for peak torsion as RRnorm�RR/�max (s�1).20 Furtherequations describing torsion and recoil are given in Figure I in theonline-only Data Supplement.
Flow-mediated vasodilation of the brachial artery was performed(E.G.) at visits 2 and 5 with the use of a high-resolution wideband 7-to 12-MHz linear transducer (Philips HDI 5000) according to astandardized protocol.21
We monitored 24-hour BP with a portable device at visits 2 and 5,with BP and heart rate measured every 30 minutes.
Laboratory InvestigationsCirculating markers were recorded as shown in Figure 1. Thefollowing metabolic parameters were assessed at each visit: baselineand postprandial glycemia, insulin, homeostasis model assessmentindex, C-peptide, blood chemistry and lipid profile, HbA1c, esti-mated glomerular filtration rate, 24-hour urinary microalbuminuria,and vital statistics. Cardiac remodeling and inflammatory indices(B-type natriuretic peptide [BNP], pro-BNP, procollagen aminoter-minal propeptide [PINP], transforming growth factor-� [TGF-�],monocyte chemotactic protein-1 [MCP1]) and endothelial functionmarkers (endothelin-1, vascular endothelial growth factor) weremeasured at visits 2, 5, and 6. Serum and plasma specimens werefrozen (�80°C) for subsequent analysis. TGF-�, MCP1,interleukin-6, and vascular endothelial growth factor were assayedwith a quantitative sandwich enzyme immunoassay (Quantikine,R&D Systems, Abingdon, UK). N-terminal pro-BNP (NT-proBNP)was analyzed with the use of an electrochemiluminescence immu-noassay on the Elecsys 1010/2010 system (ECLIA, Roche Diagnos-tics, Basel, Switzerland) (see the online-only Data Supplement forfurther details).
Table 2. Correlation Analysis at Baseline
Variable Midwall Torsion Midwall Strain LVM Index EDV Index Ventricular TD Interventricular Septum Cardiac Index LVM/EDV Ratio
Midwall strain 0.29§; P�0.038
LVM index 0.30§; P�0.040 �0.38; P�0.792
EDV index �0.34§; P�0.040 �0.47*; P�0.001 0.42‡; P�0.002
Ventricular TD �0.36§; P�0.015 �0.41‡; P�0.003 0.34§; P�0.013 0.77*; P�0.001
Interventricular septum 0.54*; P�0.001 0.39‡; P�0.004 0.37‡; P�0.007 �0.27§; P�0.049 �0.26; P�0.059
Cardiac index �0.76; P�0.591 �0.35§; P�0.011 0.31§; P�0.022 0.61*; P�0.001 0.44†; P�0.001 �0.22; P�0.115
LVM/EDV ratio 0.52*; P�0.001 0.49*; P�0.001 0.35‡; P�0.009 �0.62*; P�0.001 �0.47*; P�0.001 0.64*; P�0.001 �0.39‡; P�0.003
EF 0.124; P�0.381 0.10; P�0.500 �0.12; P�0.376 �0.35‡; P�0.009 �0.37‡; P�0.005 �0.04; P�0.788 0.33§; P�0.015 0.11; P�0.426
BMI 0.36‡; P�0.009 0.14; P�0.321 0.27; P�0.052 �0.98; P�0.480 �0.12; P�0.934 0.33§; P�0.013 �0.04; P�0.787 0.52*; P�0.001
HbA1c 0.42‡; P�0.002 0.23; P�0.100 0.32§; P�0.017 �0.11; P�0.410 �0.17; P�0.224 0.39‡; P�0.003 �0.33§; P�0.016 0.43‡; P�0.001
Triglycerides 0.48*; P�0.001 0.46†; P�0.001 0.12; P�0.377 �0.51*; P�0.001 �0.34‡; P�0.010 0.39‡; P�0.003 �0.30§; P�0.028 0.56*; P�0.001
TGF-� 0.06; P�0.648 �0.05; P�0.726 0.13; P�0.339 �0.59; P�0.674 0.10; P�0.500 0.03; P�0.847 0.03; P�0.843 0.15; P�0.267
MCP1 0.51*; P�0.001 0.32§; P�0.029 0.18; P�0.207 �0.19; P�0.177 �0.11; P�0.437 0.18; P�0.192 �0.05; P�0.710 0.34§; P�0.014
NT-proBNP �0.02; P�0.878 �0.08; P�0.569 0.34‡; P�0.010 0.46§; P�0.001 0.39‡; P�0.004 0.17; P�0.205 0.09; P�0.522 �0.18; P�0.191
PINP �0.13; P�0.364 0.03; P�0.040 0.62; P�0.658 �0.17; P�0.224 0.01; P�0.953 �0.07; P�0.605 0.01; P�0.918 0.13; P�0.360
VEGF 0.15; P�0.297 0.27; P�0.053 �0.06; P�0.693 �0.29§; P�0.034 �0.24; P�0.088 0.11; P�0.417 �0.16; P�0.256 0.25; P�0.074
Mean SBP 0.13; P�0.350 0.06; P�0.659 0.57*; P�0.001 0.14; P�0.298 0.03; P�0.843 0.42‡; P�0.002 �0.04; P�0.787 0.33§; P�0.014
Mean DBP 0.05; P�0.736 0.04; P�0.791 0.47*; P�0.001 0.14; P�0.320 0.03; P�0.828 0.35‡; P�0.009 �0.06; P�0.680 0.31§; P�0.020
LVM indicates left ventricular mass; EDV, end-diastolic volume; TD, transverse diameter; EF, ejection fraction; BMI, body mass index; HbA1c, hemoglobin A1c; TGF,transforming growth factor; MCP1, monocyte chemotactic protein-1; NT-proBNP, N-terminal pro–B-type natriuretic peptide; PINP, procollagen aminoterminalpropeptide; VEGF, vascular endothelial growth factor; SBP, systolic blood pressure; and DBP, diastolic blood pressure.
*P�0.0001.†P�0.001.‡P�0.01.§P�0.05.
2326 Circulation May 15, 2012
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

Sample SizeThe primary efficacy outcome was LV torsion angle (�). Wearbitrarily specified a clinically significant change of 3° on CMR,according to previous data on LV � change 12 months after surgicalrepair of aortic stenosis (from 16.6�7.2° to 9.0�3.4°; P�0.05).17,22
An overall sample size of 32 subjects (16 for each group) would thushave provided 90% power to detect the specified minimum detect-able difference at a 2-sided significance level of 0.01. In determiningthe sample size, we assumed that 15% of patients would drop out ofthe study.
Statistical AnalysisContinuous variables are reported as mean�1 SD. All variables weretested for normality. Comparative analysis between groups at base-line and after treatment was performed as appropriate by Student ttest, 2-way repeated-measures ANOVA, and post hoc comparison(Newman-Keuls test) (with similar results). Statistical analyses wereperformed with the use of SPSS for Windows, version 18.0 (SPSS,Inc). All statistical comparisons were performed with 2-tailed sig-nificance tests, with P�0.05 considered statistically significant.
ResultsOne hundred eight diabetic men were screened (Figure 1); 66patients were eligible and enrolled (visit 1). Seven were thenexcluded because of evidence of aneurysm of the ascendingaorta (n�1) on stress echocardiography and of ischemic heartdisease (n�6) on the first CMR image. Fifty-nine patientswere randomized to receive sildenafil (sildenafil group;n�30) or placebo (placebo group; n�29) for 3 months (Table1). Overall, 54 completed the trial. One man withdrew after 2months because of portal vein thrombosis, and 4 withdrew forother reasons (claustrophobia, personal reasons, lost atfollow-up). There were no drug-related adverse events. The
baseline characteristics of the 2 groups, at both randomizationand study completion, were well matched (Table 1).
At the baseline (visit 2), all patients exhibited CMR-taggedimaging features compatible with cardiac remodeling inducedby nonischemic diabetic cardiomyopathy: increased torsionangle (�: 18.4�4.6°; normal value, �12°), reduced circum-ferential strain (�: �12.6�3.1%; normal value, ��18%),increased LVM index (119.4�25.7 g/m2), low-normal EDVindex (60.2�13.9%), and increased ratio of LVM to EDV(LVM/EDV) (2.07�0.53 g/mL) with normal output (cardiacindex: 2.7�0.6 L/min per square meter; EF: 60.3�9.3%). AllCMR parameters were similar for both groups and wereconsistent with LV concentric hypertrophy.
The baseline correlation analysis is shown in Table 2. Torsionwas correlated with cardiac mass and geometric remodeling:There was a direct correlation with LVM index and interven-tricular septum thickness and an inverse correlation withEDV index and ventricular transverse diameter. Strain wasalso correlated with the cardiac index, whereas neither � nor� was correlated with EF. Cardiac mass, torsion, and strainwere correlated with metabolic impairment (HbA1c, triglyc-erides, and body mass index), whereas BP showed nocorrelation with strain or torsion, confirming that in ourcohort CMR changes were secondary to metabolic impair-ment, independently of hypertension. NT-proBNP was cor-related directly with LVM index and EDV index and indi-rectly with EF but showed no correlation with strain ortorsion. MCP1 was correlated with �, �, metabolic parame-ters, and TGF-� (Figure 3). These correlations demonstratethat CMR kinetic parameters provide sensitive estimates ofcardiac remodeling before chamber dilation or failure. MCP1
Table 2. Continued
EF BMI HbA1c Triglycerides TGF-� MCP1 NT-proBNP PINP VEGF Mean SBP
�0.17; P�0.208
�0.31§; P�0.027 0.32§; P�0.002
�0.11; P�0.431 0.37‡; P�0.005 0.40‡
�0.11; P�0.421 0.22; P�0.105 0.19; P�0.161 0.05; P�0.707
�0.00; P�0.991 0.31§; P�0.026 0.29§; P�0.034 0.55*; P�0.001 0.33§; P�0.016
�0.28§; P�0.037 �0.10; P�0.481 0.13; P�0.337 �0.07; P�0.613 �0.15; P�0.293 �0.02; P�0.888
0.08; P�0.583 0.04; P�0.760 �0.00; P�0.992 �0.22; P�0.119 �0.05; P�0.726 �0.17; P�0.227 �0.17; P�0.209
0.05; P�0.726 0.15; P�0.279 0.06; P�0.671 0.18; P�0.191 0.05; P�0.719 0.04; P�0.788 �016; P�0.251 0.37‡; P�0.008
�0.25; P�0.063 0.23; P�0.093 0.40‡; P�0.001 0.10; P�0.453 0.10; P�0.480 0.10; P�0.456 0.261; P�0.054 0.07; P�0.592 0.04; P�0.760
�0.37‡; P�0.005 0.17; P�0.209 0.23; P�0.084 0.08; P�0.512 0.15; P�0.274 0.00; P�0.999 0.08; P�0.544 0.08; P�0.567 0.42; P�0.767 0.77*; P�0.001
Giannetta et al Sildenafil Improves Diabetic Cardiomyopathy 2327
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from
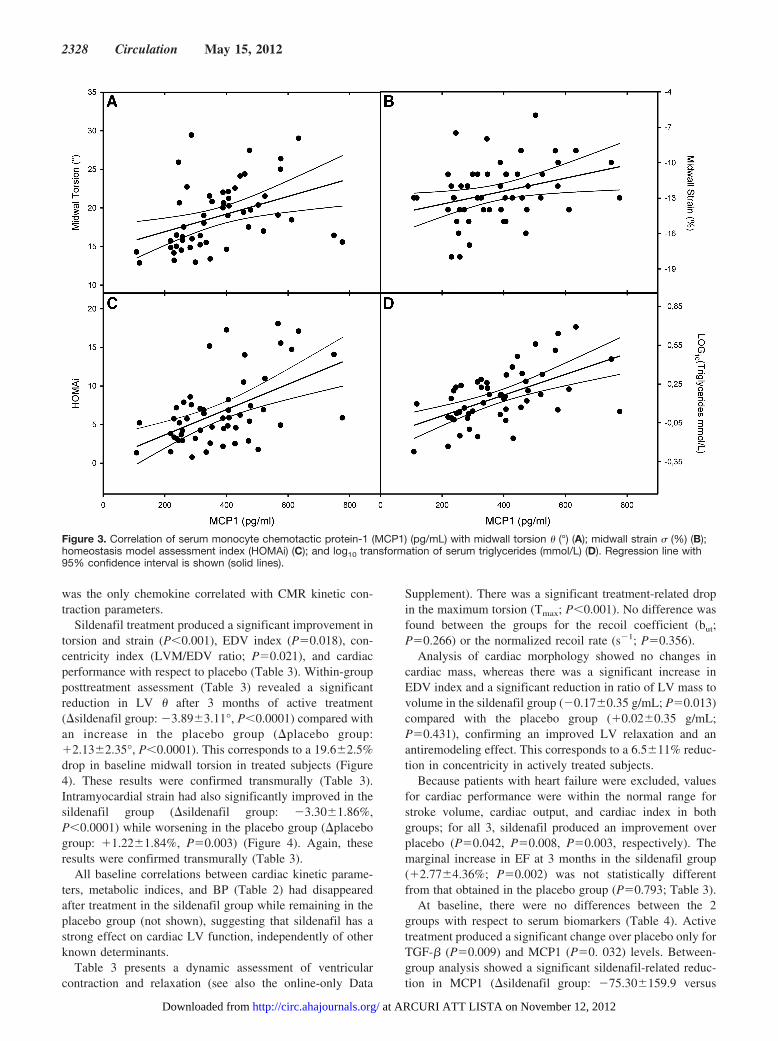
was the only chemokine correlated with CMR kinetic con-traction parameters.
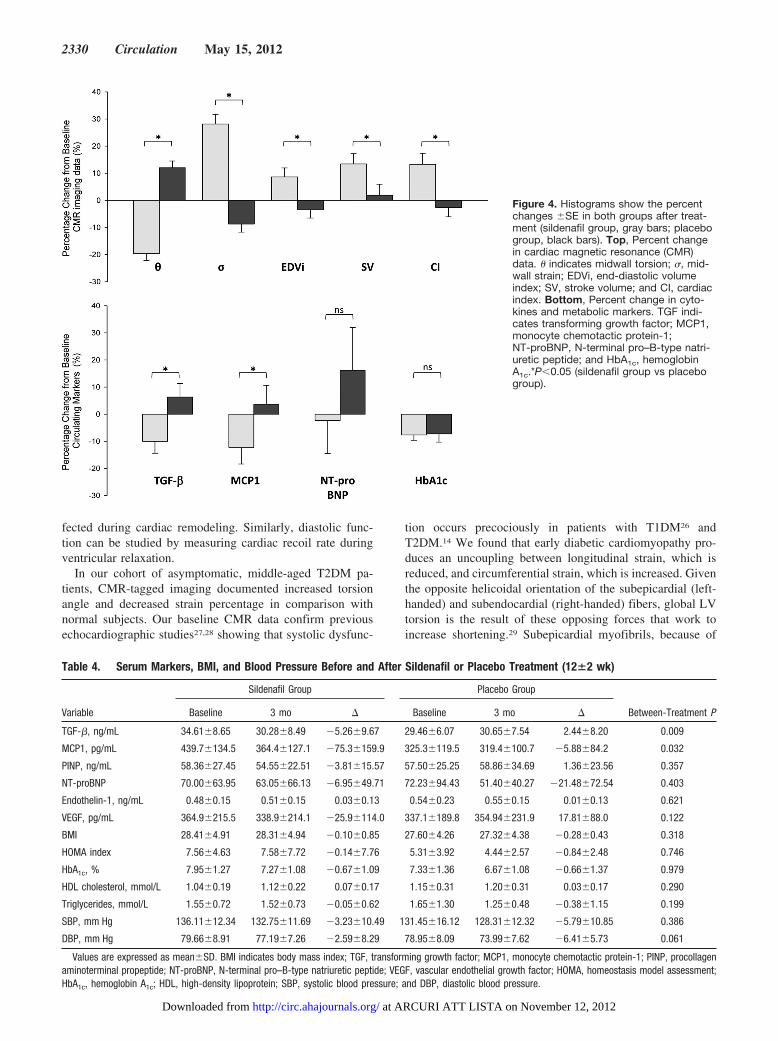
Sildenafil treatment produced a significant improvement intorsion and strain (P�0.001), EDV index (P�0.018), con-centricity index (LVM/EDV ratio; P�0.021), and cardiacperformance with respect to placebo (Table 3). Within-groupposttreatment assessment (Table 3) revealed a significantreduction in LV � after 3 months of active treatment(�sildenafil group: �3.89�3.11°, P�0.0001) compared withan increase in the placebo group (�placebo group:�2.13�2.35°, P�0.0001). This corresponds to a 19.6�2.5%drop in baseline midwall torsion in treated subjects (Figure4). These results were confirmed transmurally (Table 3).Intramyocardial strain had also significantly improved in thesildenafil group (�sildenafil group: �3.30�1.86%,P�0.0001) while worsening in the placebo group (�placebogroup: �1.22�1.84%, P�0.003) (Figure 4). Again, theseresults were confirmed transmurally (Table 3).
All baseline correlations between cardiac kinetic parame-ters, metabolic indices, and BP (Table 2) had disappearedafter treatment in the sildenafil group while remaining in theplacebo group (not shown), suggesting that sildenafil has astrong effect on cardiac LV function, independently of otherknown determinants.
Table 3 presents a dynamic assessment of ventricularcontraction and relaxation (see also the online-only Data
Supplement). There was a significant treatment-related dropin the maximum torsion (Tmax; P�0.001). No difference wasfound between the groups for the recoil coefficient (but;P�0.266) or the normalized recoil rate (s�1; P�0.356).
Analysis of cardiac morphology showed no changes incardiac mass, whereas there was a significant increase inEDV index and a significant reduction in ratio of LV mass tovolume in the sildenafil group (�0.17�0.35 g/mL; P�0.013)compared with the placebo group (�0.02�0.35 g/mL;P�0.431), confirming an improved LV relaxation and anantiremodeling effect. This corresponds to a 6.5�11% reduc-tion in concentricity in actively treated subjects.
Because patients with heart failure were excluded, valuesfor cardiac performance were within the normal range forstroke volume, cardiac output, and cardiac index in bothgroups; for all 3, sildenafil produced an improvement overplacebo (P�0.042, P�0.008, P�0.003, respectively). Themarginal increase in EF at 3 months in the sildenafil group(�2.77�4.36%; P�0.002) was not statistically differentfrom that obtained in the placebo group (P�0.793; Table 3).
At baseline, there were no differences between the 2groups with respect to serum biomarkers (Table 4). Activetreatment produced a significant change over placebo only forTGF-� (P�0.009) and MCP1 (P�0. 032) levels. Between-group analysis showed a significant sildenafil-related reduc-tion in MCP1 (�sildenafil group: �75.30�159.9 versus
Figure 3. Correlation of serum monocyte chemotactic protein-1 (MCP1) (pg/mL) with midwall torsion � (°) (A); midwall strain � (%) (B);homeostasis model assessment index (HOMAi) (C); and log10 transformation of serum triglycerides (mmol/L) (D). Regression line with95% confidence interval is shown (solid lines).
2328 Circulation May 15, 2012
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

placebo group: �5.88�84.2 pg/mL; P�0.032) and TGF-�(�sildenafil group: �5.26�9.67 versus placebo group:2.44�8.20 ng/mL; P�0.009) compared with placebo. Nosignificant changes were found in NT-proBNP, procollagenaminoterminal propeptide, vascular endothelial growth fac-tor, or endothelin-1.
BP monitoring revealed an unexpected lowering of systolicand diastolic 24-hour BP in the placebo group only. Endo-thelial function studies revealed no treatment-related differ-ence in the flow-mediated vasodilation of the brachial artery(data not shown). No differences were found in glycemia,insulin, C-peptide, homeostatic model assessment index, orlipid profile after 3 months of treatment, but HbA1c droppedin both groups (�sildenafil group: �0.67�1.09%, P�0.001;�placebo group: �0.66�1.37%, P�0.048), and high-densitylipoprotein increased over the baseline value in the sildenafilgroup (0.07�0.17 mmol/L; P�0.025) (Table 4). Between-group analysis revealed that there were no treatment-relateddifferences in metabolic parameters.
DiscussionThis study characterizes for the first time the early stages ofdiabetic cardiomyopathy, demonstrating that in this cohort ofmen with T2DM, chronic PDE5 inhibition exerts an antire-modeling effect by improving the LVM/EDV ratio andCMR-tagged torsion and strain through an endothelial-independent intramyocardial effect, paralleled by changes ininflammatory serum markers.
Features of Diabetic CardiomyopathyT2DM currently affects �180 million people worldwide. Ofthese, 80% will die of cardiovascular disease.13,23 Diabeticcardiomyopathy progresses from early alteration of myocar-dial interstitium with increased membrane permeability and
preserved cell morphology to subsequent enlargement ofcardiomyocytes with interstitial and perivascular fibrosis.13,24
Geometric ventricular chamber remodeling is initially char-acterized by low-normal EDV index and normal or onlymodestly increased LVM. This is associated with systolic/di-astolic myocardial dysfunction due to passive stiffness andimpaired relaxation.13,23 For these reasons, diabetic cardio-myopathy offers a unique model to explore the potential ofpharmacological targeting of the pathways leading to cardiachypertrophy. We further improved the accuracy of the modelby excluding patients with silent ischemic heart disease,fibrosis, other vascular disorders, or interfering treatments. Ofnote is that 6 of the enrolled patients (9%) had CMR signs ofprevious ischemic disease not otherwise detected on stressechocardiography.
We demonstrated that asymptomatic, “healthy” diabeticpatients exhibit CMR features consistent with advancedremodeling. In particular, concentric hypertrophy (increasedLVM/EDV ratio, with low-normal EDV index)25 appears tocharacterize the early stages of the disease, whereas cardiacperformance remains unaffected.
In our study, cardiac changes were correlated with meta-bolic impairment, indicating that neurohumoral mechanismstriggered by T2DM were responsible for the adaptive changesof the LV (Figure 3). Having confirmed the dependency onthe metabolic disorder, our model of concentric LVH wassuitable to assess whether PDE5 inhibition could work as anantiremodeling drug.
The magnitudes of cardiac axial rotation during ventricularcontraction (torsion [�]) and of fiber shortening along the LVlong axis (strain [�]) are the most sensitive indices of systolicfunction because they are strongly correlated with hypertro-phy and fibrosis.23,26 Both parameters are precociously af-
Table 3. Kinetic, Geometric, and Performance Parameters at Cardiac Magnetic Resonance Assessment After Sildenafil and PlaceboTreatment (12�2 wk)
Variable
Sildenafil Group Placebo Group
Between-Treatment PBaseline 3 mo � Baseline 3 mo �
Midwall torsion, ° 19.74�4.34 15.84�4.21 �3.89�3.11 17.81�4.26 19.95�5.25 2.13�2.35 �0.001
Transmural torsion, ° 8.21�1.91 6.09�1.41 �2.12�1.21 7.47�2.64 8.71�2.52 1.24�1.55 �0.001
Midwall strain, % �11.34�2.70 �14.64�2.37 �3.30�1.86 �13.26�2.45 �12.04�2.64 1.22�1.84 �0.001
Transmural strain, % �11.18�2.56 �14.00�2.46 �2.89�1.65 �12.87�2.43 �11.75�2.48 1.11�2.05 �0.001
Torsion coefficient, Tmax 27.32�7.21 22.67�7.93 �4.64�7.54 25.19�5.92 29.45�8.96 4.26�6.33 �0.001
Recoil coefficient, but 0.18�0.08 0.15�0.07 �0.04�0.06 0.19�0.06 0.18�0.07 �0.008�0.06 0.266
Normalized recoil rate, s�1 5.61�1.97 5.46�2.49 �0.09�1.75 5.79�2.25 4.90�1.98 �0.88�2.04 0.356
LVM index, g/m2 120.7�29.8 120.0�30.2 �0.67�5.07 119.9�21.8 117.8�22.9 �2.03�7.64 0.473
EDV index, mL/m2 57.46�13.68 61.10�11.99 3.64�9.81 63.34�13.66 60.60�14.15 �2.74�9.37 0.018
LVM/EDV, g/mL 2.16�0.51 1.99�0.41 �0.17�0.35 2.01�0.54 2.03�0.55 0.02�0.35 0.021
Ventricular TD, mm 47.30�4.59 47.05�4.51 �0.25�2.20 48.57�4.89 48.84�4.71 0.54�3.04 0.372
Interventricular septum, mm 11.80�1.90 11.55�2.04 �0.17�0.64 11.45�1.61 11.51�1.66 0.04�0.47 0.202
Stroke volume, mL 70.00�18.83 76.83�15.15 6.83�13.64 72.26�13.83 70.63�10.77 �0.35�12.92 0.042
Cardiac output, L/min 5.36�1.26 5.69�1.04 0.36�1.01 5.11�0.93 4.72�0.64 �0.33�0.86 0.008
Cardiac index, L/(min � m2) 2.74�0.61 3.00�0.45 0.27�0.56 2.73�0.60 2.60�0.43 �0.14�0.45 0.003
EF, % 61.59�8.21 64.36�7.14 2.77�4.36 59.11�10.24 62.06�9.85 3.14�5.87 0.793
Values are expressed as mean�SD. LVM indicates left ventricular mass; EDV, end-diastolic volume; TD, transverse diameter; and EF, ejection fraction.
Giannetta et al Sildenafil Improves Diabetic Cardiomyopathy 2329
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from
fected during cardiac remodeling. Similarly, diastolic func-tion can be studied by measuring cardiac recoil rate duringventricular relaxation.
In our cohort of asymptomatic, middle-aged T2DM pa-tients, CMR-tagged imaging documented increased torsionangle and decreased strain percentage in comparison withnormal subjects. Our baseline CMR data confirm previousechocardiographic studies27,28 showing that systolic dysfunc-
tion occurs precociously in patients with T1DM26 andT2DM.14 We found that early diabetic cardiomyopathy pro-duces an uncoupling between longitudinal strain, which isreduced, and circumferential strain, which is increased. Giventhe opposite helicoidal orientation of the subepicardial (left-handed) and subendocardial (right-handed) fibers, global LVtorsion is the result of these opposing forces that work toincrease shortening.29 Subepicardial myofibrils, because of
Figure 4. Histograms show the percentchanges �SE in both groups after treat-ment (sildenafil group, gray bars; placebogroup, black bars). Top, Percent changein cardiac magnetic resonance (CMR)data. � indicates midwall torsion; �, mid-wall strain; EDVi, end-diastolic volumeindex; SV, stroke volume; and CI, cardiacindex. Bottom, Percent change in cyto-kines and metabolic markers. TGF indi-cates transforming growth factor; MCP1,monocyte chemotactic protein-1;NT-proBNP, N-terminal pro–B-type natri-uretic peptide; and HbA1c, hemoglobinA1c.*P�0.05 (sildenafil group vs placebogroup).
Table 4. Serum Markers, BMI, and Blood Pressure Before and After Sildenafil or Placebo Treatment (12�2 wk)
Variable
Sildenafil Group Placebo Group
Between-Treatment PBaseline 3 mo � Baseline 3 mo �
TGF-�, ng/mL 34.61�8.65 30.28�8.49 �5.26�9.67 29.46�6.07 30.65�7.54 2.44�8.20 0.009
MCP1, pg/mL 439.7�134.5 364.4�127.1 �75.3�159.9 325.3�119.5 319.4�100.7 �5.88�84.2 0.032
PINP, ng/mL 58.36�27.45 54.55�22.51 �3.81�15.57 57.50�25.25 58.86�34.69 1.36�23.56 0.357
NT-proBNP 70.00�63.95 63.05�66.13 �6.95�49.71 72.23�94.43 51.40�40.27 �21.48�72.54 0.403
Endothelin-1, ng/mL 0.48�0.15 0.51�0.15 0.03�0.13 0.54�0.23 0.55�0.15 0.01�0.13 0.621
VEGF, pg/mL 364.9�215.5 338.9�214.1 �25.9�114.0 337.1�189.8 354.94�231.9 17.81�88.0 0.122
BMI 28.41�4.91 28.31�4.94 �0.10�0.85 27.60�4.26 27.32�4.38 �0.28�0.43 0.318
HOMA index 7.56�4.63 7.58�7.72 �0.14�7.76 5.31�3.92 4.44�2.57 �0.84�2.48 0.746
HbA1c, % 7.95�1.27 7.27�1.08 �0.67�1.09 7.33�1.36 6.67�1.08 �0.66�1.37 0.979
HDL cholesterol, mmol/L 1.04�0.19 1.12�0.22 0.07�0.17 1.15�0.31 1.20�0.31 0.03�0.17 0.290
Triglycerides, mmol/L 1.55�0.72 1.52�0.73 �0.05�0.62 1.65�1.30 1.25�0.48 �0.38�1.15 0.199
SBP, mm Hg 136.11�12.34 132.75�11.69 �3.23�10.49 131.45�16.12 128.31�12.32 �5.79�10.85 0.386
DBP, mm Hg 79.66�8.91 77.19�7.26 �2.59�8.29 78.95�8.09 73.99�7.62 �6.41�5.73 0.061
Values are expressed as mean�SD. BMI indicates body mass index; TGF, transforming growth factor; MCP1, monocyte chemotactic protein-1; PINP, procollagenaminoterminal propeptide; NT-proBNP, N-terminal pro–B-type natriuretic peptide; VEGF, vascular endothelial growth factor; HOMA, homeostasis model assessment;HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; SBP, systolic blood pressure; and DBP, diastolic blood pressure.
2330 Circulation May 15, 2012
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

their larger radius, produce the dominant force for LVrotation; thus, a dysfunction in the counteracting subendocar-dial action (eg, due to diffuse fibrosis) could lead to increasedtorsion and decreased longitudinal shortening.30 Subendocar-dial dysfunction due to metabolic impairment could explainthe increased torsion paralleling the HbA1c levels found inour patients.
Torsion and strain were altered in the presence of normalEF and controlled BP. We also demonstrated for the first timea correlation between � and MCP1, a serum biomarker ofcardiac fibrosis, suggesting a possible pathogenetic role(Table 2).
Antiremodeling Effects of SildenafilAfter 3 months of sildenafil treatment, we observed a signif-icant improvement in strain and torsion. Analyses of thecardiac kinetics showed that peak torsion was significantlyreduced, tending toward near-normal values, compared withbaseline and the placebo group. PDE5 inhibitor–inducedchanges in cardiac kinetics improved the cardiac geometry, asreflected by the improved ratio of LVM to volume (an indexof LV concentric remodeling) (Figure 4). Cardiac perfor-mance (EF, cardiac output, and cardiac index) also improvedin the sildenafil group. Interestingly, there was a marginalworsening in cardiac dynamics in the placebo group at theend of the study. In this respect, the detrimental progressionof the torsion, without changes in recoil, suggests thatabnormalities in systolic function might be partly indepen-dent of diastolic dysfunction in diabetic cardiomyopathy.27,31
The mechanism by which PDE5 inhibitors may exert sucheffects is under investigation.32 Increased cGMP throughactivation of protein kinase G reduces inotropy, exerting arelaxant effect.5,33,34 However, PDE5 overexpression in hy-pertrophic cardiomyocytes4 reduces cGMP levels and pro-motes remodeling. Sildenafil might stop this loop by inhib-iting cGMP hydrolysis within the cardiomyocytes. However,its effects could also be secondary to vasodilation or anendothelial-mediated effect.
When exploring afterload, we found no significant changesin 24-hour BP in the active treatment group. This is consistentwith our review of randomized clinical trials involvingsildenafil that showed no significant effects on BP even afterhigh doses (Table IV in the online-only Data Supplement). Amarginal reduction in BP35,36 was seen occasionally as anacute effect but diminished with repeated administration.36 Inaddition, all of our patients had normal or well-controlled BP,possibly reducing any mild antihypertensive effect. More-over, the baseline correlation between cardiac kinetics and BP(Table 2) was lost after the perturbation induced by PDE5inhibition. The lack of relationship between the effectsproduced by sildenafil on torsion and the null effect on BPsupport the initial hypothesis of a primary cardiac action,independent of any secondary effect on afterload. Havingexcluded the possibility that improvement in LV dysfunctionis afterload dependent, we explored whether it could be theresult of an endothelial-dependent action. However, nochanges were found in endothelin-1 and vascular endothelialgrowth factor or in flow-mediated vasodilation.
To study the molecular signals triggered in the cardiomyo-cytes by PDE5 inhibition, we investigated a large panel ofcardiac biomarkers involved in the pathogenesis and progres-sion of diabetic cardiomyopathy. Interestingly, we found thatsildenafil lowered TGF-� and MCP1 (Figure 4), 2 proinflam-matory molecules involved in LV remodeling and associatedwith myocyte growth and fibrosis.34,37,38 It has been foundrecently that both MCP1 and TGF-� are expressed in skeletalmuscle cells and hypertrophic cardiomyocytes39 (also con-firmed in our own recent study; A.M. Isidori, MD, PhD, et al,unpublished data, 2012), suggesting that the sildenafil-induced changes in these serum markers could be partlyrelated to a direct cardiac effect. This is consistent with recentanimal studies by Kass and colleagues.37 This theory isfurther supported by the direct correlation between MCP1levels and midwall � and � found at the baseline in our studypopulation.40 The reduction in these biomarkers may reflect adeactivation of diabetic cardiomyopathy–triggered fibroticsignals following the increase in intracellular cGMP levels,41
as demonstrated in diabetic nephropathy.42 The secondaryimprovement in profibrotic markers and diastolic compliance(EDV index and LVM/EDV ratio) produced by sildenafilsuggests that improvement in subendocardial fibrosis couldbe a mechanism of action.
Finally, we investigated whether metabolic control wasinvolved in the observed cardiac effects and whether itwas related to PDE5 inhibitor administration. Although therewas a correlation between cardiac kinetics, morphology, andperformance at baseline, this had disappeared after 3 monthsof active treatment.43 Interestingly, we did not observe anychanges in endothelial function. Sildenafil has been found toimprove endothelium-dependent vasodilation in some44,45 butnot all studies.35,46–48 Reports of a positive effect on endo-thelial function mostly involved single-dose trials35,46–48 orstudies of acute effects.49 Most of these studies were per-formed in nondiabetic younger patients or active smokers.50
A possible explanation for the lack of effect on flow-mediated vasodilation is that nitric oxide might make arelatively small contribution to shear stress–induced vasodi-lation in diabetic patients. In this case, our cohort of patientsmight have been less sensitive to the endothelium-relatedeffects of sildenafil.
LimitationsIn contrast with a recent study,12 we were unable to detect anychanges in LVM index and NTpro-BNP levels. For LVMindex, a possible explanation may be the short duration of thetreatment (3 versus 12 months). For NTpro-BNP, the lack ofchange might be due to the inclusion criteria of patientsrecruited at an early stage of disease, when concentric LVhypertrophy has already developed but not yet evolved tosevere eccentric dilation. This is consistent with previousobservations showing that when diabetic cardiomyopathy isnot accompanied by chamber dilation, there is poor correla-tion between cardiac kinetics and NTpro-BNP.27,31 Anotherlimitation of our study was the lack of a quantitative assess-ment of diffuse fibrosis (eg, T1 mapping), which would haveallowed a better estimation of any treatment-related effect
Giannetta et al Sildenafil Improves Diabetic Cardiomyopathy 2331
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from
and may have provided evidence for the suggested antifi-brotic action of sildenafil.9
ConclusionsThis study demonstrated that both systolic and diastolicdysfunction are precocious in diabetic cardiomyopathy andassociated with a compensatory LV concentric remodeling,whereas cardiac performance at rest remains unaffected. Wealso showed that morphological and kinetic impairment arerelated to metabolic status and correlated with circulatingproinflammatory chemokines, especially MCP1 and TGF-�.Dysfunctional LV contraction in diabetic cardiomyopathycan be rapidly improved by chronic PDE5A inhibitionthrough an antiremodeling mechanism independent of vascu-lar, endothelial, or metabolic factors. These findings warrantfurther studies to discover the intramyocardial mechanismsinvolved in the antiremodeling effect of sildenafil, as well aslong-term outcome studies to quantify the risks and benefitsof diabetic cardiomyopathy treatment. Finally, MCP1 couldbe included as a new marker in the follow-up of patients withdiabetic cardiomyopathy, but further mechanistic evidence isnecessary to plan future population studies.
AcknowledgmentsWe would like to thank Dr Carla Di Dato for her help with patients,Alessandra Bachetoni and the staff of the Clinical Pathology andTransplant Laboratory for the cytokine assays, Alberto Isidori formathematical modeling, Gian Luca di Tanna and Matthias Friedrichfor their critical reading of the manuscript, and Marie-Helne Haylesfor revision of the English text.
Sources of FundingThe study was supported by Ministry of Research MIUR grant FIRBNo. RBAP109BLT.
DisclosuresNone.
References1. Tsai EJ, Kass DA. Cyclic GMP signaling in cardiovascular pathophys-
iology and therapeutics. Pharmacol Ther. 2009;122:216–238.2. Takimoto E, Champion HC, Belardi D, Moslehi J, Mongillo M, Mergia
E, Montrose DC, Isoda T, Aufiero K, Zaccolo M, Dostmann WR, SmithCJ, Kass DA. cGMP catabolism by phosphodiesterase 5A regulatescardiac adrenergic stimulation by NOS3-dependent mechanism. Circ Res.2005;96:100–109.
3. Takimoto E, Champion HC, Li M, Belardi D, Ren S, Rodriguez ER,Bedja D, Gabrielson KL, Wang Y, Kass DA. Chronic inhibition of cyclicGMP phosphodiesterase 5A prevents and reverses cardiac hypertrophy.Nat Med. 2005;11:214–222.
4. Zhang M, Koitabashi N, Nagayama T, Rambaran R, Feng N, Takimoto E,Koenke T, O’Rourke B, Champion HC, Crow MT, Kass DA. Expression,activity, and pro-hypertrophic effects of PDE5A in cardiac myocytes.Cell Signal. 2008;20:2231–2236.
5. Kumar P, Francis GS, Tang WH. Phosphodiesterase 5 inhibition in heartfailure: mechanisms and clinical implications. Nat Rev Cardiol. 2009;6:349–355.
6. Nagayama T, Hsu S, Zhang M, Koitabashi N, Bedja D, Gabrielson KL,Takimoto E, Kass DA. Sildenafil stops progressive chamber, cellular, andmolecular remodeling and improves calcium handling and function inhearts with pre-existing advanced hypertrophy caused by pressureoverload. J Am Coll Cardiol. 2009;53:207–215.
7. Salloum F, Yin C, Xi L, Kukreja RC. Sildenafil induces delayed precon-ditioning through inducible nitric oxide synthase–dependent pathway inmouse heart. Circ Res. 2003;92:595–597.
8. Fisher PW, Salloum F, Das A, Hyder H, Kukreja RC.Phosphodiesterase-5 inhibition with sildenafil attenuates cardiomyocyteapoptosis and left ventricular dysfunction in a chronic model of doxo-rubicin cardiotoxicity. Circulation. 2005;111:1601–1610.
9. Ferreira-Melo SE, Yugar-Toledo JC, Coelho OR, De Luca IM, Tanus-Santos JE, Hyslop S, Irigoyen MC, Moreno H Jr. Sildenafil reducescardiovascular remodeling associated with hypertensive cardiomyopathyin NOS inhibitor-treated rats. Eur J Pharmacol. 2006;542:141–147.
10. Rossoni G, Manfredi B, De Gennaro Colonna V, Berti M, Guazzi M,Berti F. Sildenafil reduces L-NAME-induced severe hypertension andworsening of myocardial ischaemia-reperfusion damage in the rat. Br JPharmacol. 2007;150:567–576.
11. Nagendran J, Archer SL, Soliman D, Gurtu V, Moudgil R, Haromy A, StAubin C, Webster L, Rebeyka IM, Ross DB, Light PE, Dyck JR,Michelakis ED. Phosphodiesterase type 5 is highly expressed in thehypertrophied human right ventricle, and acute inhibition of phosphodi-esterase type 5 improves contractility. Circulation. 2007;116:238–248.
12. Guazzi M, Vicenzi M, Arena R, Guazzi MD. PDE5 inhibition withsildenafil improves left ventricular diastolic function, cardiac geometry,and clinical status in patients with stable systolic heart failure: results ofa 1-year, prospective, randomized, placebo-controlled study. Circ HeartFail. 2011;4:8–17.
13. Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy:from the pathophysiology of the cardiac myocytes to current diagnosisand management strategies. Vasc Health Risk Manag. 2010;6:883–903.
14. Fonseca CG, Dissanayake AM, Doughty RN, Whalley GA, Gamble GD,Cowan BR, Occleshaw CJ, Young AA. Three-dimensional assessment ofleft ventricular systolic strain in patients with type 2 diabetes mellitus,diastolic dysfunction, and normal ejection fraction. Am J Cardiol. 2004;94:1391–1395.
15. Feng B, Chen S, Chiu J, George B, Chakrabarti S. Regulation of cardio-myocyte hypertrophy in diabetes at the transcriptional level. Am JPhysiol. 2008;294:E1119–E1126.
16. Dong SJ, Hees PS, Siu CO, Weiss JL, Shapiro EP. MRI assessment of LVrelaxation by untwisting rate: a new isovolumic phase measure of tau.Am J Physiol. 2001;281:H2002–H2009.
17. Biederman RW, Doyle M, Yamrozik J, Williams RB, Rathi VK, Vido D,Caruppannan K, Osman N, Bress V, Rayarao G, Biederman CM, MankadS, Magovern JA, Reichek N. Physiologic compensation is supranormal incompensated aortic stenosis: does it return to normal after aortic valvereplacement or is it blunted by coexistent coronary artery disease? Anintramyocardial magnetic resonance imaging study. Circulation. 2005;112:I429–I436.
18. Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA, FriedrichMG, Ho VB, Jerosch-Herold M, Kramer CM, Manning WJ, Patel M,Pohost GM, Stillman AE, White RD, Woodard PK. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascularmagnetic resonance: a report of the American College of CardiologyFoundation Task Force on Expert Consensus Documents. J Am CollCardiol. 2010;55:2614–2662.
19. Hees PS, Fleg JL, Dong SJ, Shapiro EP. MRI and echocardiographicassessment of the diastolic dysfunction of normal aging: altered LVpressure decline or load? Am J Physiol. 2004;286:H782–H788.
20. Thompson RB, Paterson I, Chow K, Cheng-Baron J, Scott JM, Esch BT,Ennis DB, Haykowsky MJ. Characterization of the relationship betweensystolic shear strain and early diastolic shear strain rates: insights intotorsional recoil. Am J Physiol. 2010;299:H898–H907.
21. Esposito K, Ciotola M, Maiorino MI, Giugliano F, Autorino R, De SM,Jannini E, Lenzi A, Giugliano D. Circulating CD34� KDR� endothelialprogenitor cells correlate with erectile function and endothelial functionin overweight men. J Sex Med. 2009;6:107–114.
22. Sandstede JJ, Johnson T, Harre K, Beer M, Hofmann S, Pabst T, Kenn W,Voelker W, Neubauer S, Hahn D. Cardiac systolic rotation and con-traction before and after valve replacement for aortic stenosis: a myo-cardial tagging study using MR imaging. AJR Am J Roentgenol. 2002;178:953–958.
23. Asghar O, Al-Sunni A, Khavandi K, Khavandi A, Withers S, GreensteinA, Heagerty AM, Malik RA. Diabetic cardiomyopathy. Clin Sci (Lond).2009;116:741–760.
24. Connelly KA, Kelly DJ, Zhang Y, Prior DL, Martin J, Cox AJ, Thai K,Feneley MP, Tsoporis J, White KE, Krum H, Gilbert RE. Functional,structural and molecular aspects of diastolic heart failure in the diabetic(mRen-2)27 rat. Cardiovasc Res. 2007;76:280–291.
25. Khouri MG, Peshock RM, Ayers CR, de Lemos JA, Drazner MH. A4-tiered classification of left ventricular hypertrophy based on left ven-
2332 Circulation May 15, 2012
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

tricular geometry: the Dallas Heart Study. Circ Cardiovasc Imaging.2010;3:164–171.
26. Chung J, Abraszewski P, Yu X, Liu W, Krainik AJ, Ashford M, CaruthersSD, McGill JB, Wickline SA. Paradoxical increase in ventricular torsionand systolic torsion rate in type I diabetic patients under tight glycemiccontrol. J Am Coll Cardiol. 2006;47:384–390.
27. Yu CM, Lin H, Yang H, Kong SL, Zhang Q, Lee SW. Progression ofsystolic abnormalities in patients with “isolated” diastolic heart failureand diastolic dysfunction. Circulation. 2002;105:1195–1201.
28. Fang ZY, Leano R, Marwick TH. Relationship between longitudinal andradial contractility in subclinical diabetic heart disease. Clin Sci (Lond).2004;106:53–60.
29. Torrent-Guasp F, Buckberg GD, Clemente C, Cox JL, Coghlan HC,Gharib M. The structure and function of the helical heart and its buttresswrapping, I: the normal macroscopic structure of the heart. Semin ThoracCardiovasc Surg. 2001;13:301–319.
30. Cappelli F, Toncelli L, Cappelli B, De LA, Stefani L, Maffulli N, GalantiG. Adaptative or maladaptative hypertrophy, different spatial distributionof myocardial contraction. Clin Physiol Funct Imaging. 2010;30:6–12.
31. Fang ZY, Schull-Meade R, Leano R, Mottram PM, Prins JB, MarwickTH. Screening for heart disease in diabetic subjects. Am Heart J. 2005;149:349–354.
32. Zhang M, Kass DA. Phosphodiesterases and cardiac cGMP: evolvingroles and controversies. Trends Pharmacol Sci. 2011;32:360–365.
33. Pokreisz P, Vandenwijngaert S, Bito V, Van den Bergh A, Lenaerts I,Busch C, Marsboom G, Gheysens O, Vermeersch P, Biesmans L, Liu X,Gillijns H, Pellens M, Van LA, Buys E, Schoonjans L, Vanhaecke J,Verbeken E, Sipido K, Herijgers P, Bloch KD, Janssens SP. Ventricularphosphodiesterase-5 expression is increased in patients with advancedheart failure and contributes to adverse ventricular remodeling aftermyocardial infarction in mice. Circulation. 2009;119:408–416.
34. Zhang M, Takimoto E, Hsu S, Lee DI, Nagayama T, Danner T, Koit-abashi N, Barth AS, Bedja D, Gabrielson KL, Wang Y, Kass DA.Myocardial remodeling is controlled by myocyte-targeted gene regulationof phosphodiesterase type 5. J Am Coll Cardiol. 2010;56:2021–2030.
35. Stirban A, Laude D, Elghozi JL, Sander D, Agelink MW, Hilz MJ,Ziegler D. Acute effects of sildenafil on flow mediated dilatation andcardiovascular autonomic nerve function in type 2 diabetic patients.Diabetes Metab Res Rev. 2009;25:136–143.
36. Oliver JJ, Melville VP, Webb DJ. Effect of regular phosphodiesterasetype 5 inhibition in hypertension. Hypertension. 2006;48:622–627.
37. Koitabashi N, Danner T, Zaiman AL, Pinto YM, Rowell J, Mankowski J,Zhang D, Nakamura T, Takimoto E, Kass DA. Pivotal role of cardio-
myocyte TGF-beta signaling in the murine pathological response tosustained pressure overload. J Clin Invest. 2011;121:2301–2312.
38. Opie LH, Commerford PJ, Gersh BJ, Pfeffer MA. Controversies inventricular remodelling. Lancet. 2006;367:356–367.
39. Seino Y, Ikeda U, Sekiguchi H, Morita M, Konishi K, Kasahara T,Shimada K. Expression of leukocyte chemotactic cytokines in myocardialtissue. Cytokine. 1995;7:301–304.
40. Bishu K, Hamdani N, Mohammed SF, Kruger M, Ohtani T, Ogut O,Brozovich FV, Burnett JC Jr, Linke WA, Redfield MM. Sildenafil andB-type natriuretic peptide acutely phosphorylate titin and improve dia-stolic distensibility in vivo. Circulation. 2011;124:2882–2891.
41. Saura M, Zaragoza C, Herranz B, Griera M, Diez-Marques L,Rodriguez-Puyol D, Rodriguez-Puyol M. Nitric oxide regulates trans-forming growth factor-beta signaling in endothelial cells. Circ Res. 2005;97:1115–1123.
42. Tesch GH, Lim AK. Recent insights into diabetic renal injury from thedb/db mouse model of type 2 diabetic nephropathy. Am J Physiol. 2011;300:F301–F310.
43. Riddle MC. Glycemic control and cardiovascular mortality. Curr OpinEndocrinol Diabetes Obes. 2011;18:104–109.
44. Kimura M, Higashi Y, Hara K, Noma K, Sasaki S, Nakagawa K, Goto C,Oshima T, Yoshizumi M, Chayama K. PDE5 inhibitor sildenafil citrateaugments endothelium-dependent vasodilation in smokers. Hypertension.2003;41:1106–1110.
45. Guazzi M, Samaja M, Arena R, Vicenzi M, Guazzi MD. Long-term useof sildenafil in the therapeutic management of heart failure. J Am CollCardiol. 2007;50:2136–2144.
46. Halcox JP, Nour KR, Zalos G, Mincemoyer RA, Waclawiw M, RiveraCE, Willie G, Ellahham S, Quyyumi AA. The effect of sildenafil onhuman vascular function, platelet activation, and myocardial ischemia.J Am Coll Cardiol. 2002;40:1232–1240.
47. Robinson SD, Ludlam CA, Boon NA, Newby DE. Phosphodiesterasetype 5 inhibition does not reverse endothelial dysfunction in patients withcoronary heart disease. Heart. 2006;92:170–176.
48. Gori T, Sicuro S, Dragoni S, Donati G, Forconi S, Parker JD. Sildenafilprevents endothelial dysfunction induced by ischemia and reperfusion viaopening of adenosine triphosphate–sensitive potassium channels: ahuman in vivo study. Circulation. 2005;111:742–746.
49. Desouza C, Parulkar A, Lumpkin D, Akers D, Fonseca VA. Acute andprolonged effects of sildenafil on brachial artery flow-mediated dilatationin type 2 diabetes. Diabetes Care. 2002;25:1336–1339.
50. Vlachopoulos C, Tsekoura D, Alexopoulos N, Panagiotakos D,Aznaouridis K, Stefanadis C. Type 5 phosphodiesterase inhibition bysildenafil abrogates acute smoking-induced endothelial dysfunction. Am JHypertens. 2004;17:1040–1044.
CLINICAL PERSPECTIVEType 2 diabetes mellitus is associated with cardiac remodeling that may occur independently of ischemic heart disease,hypertension, or macrovascular complications. Cardiac magnetic resonance can be used to measure diabetic cardiomyop-athy, for which there is currently no specific treatment. In vitro studies have shown that phosphodiesterase 5 overexpressionreduces cGMP levels and exacerbates remodeling. Inhibiting cGMP hydrolysis in stimulated cardiomyocytes can preventhypertrophy. We studied the effects of 3-month daily sildenafil treatment (a phosphodiesterase 5A inhibitor) on cardiacremodeling in a cohort of asymptomatic, middle-aged men with type 2 diabetes mellitus. Cardiac magnetic resonanceimaging revealed that diabetic cardiomyopathy in these patients produced an uncoupling in left ventricular contractionbetween longitudinal strain, which is reduced, and cardiac axial rotation, which is increased. We found that long-termsildenafil treatment restored coupling by reducing torsion and improving strain. It also reduced the ratio of left ventricularmass to end-diastolic volume that is increased in the presence of concentric hypertrophy. These data suggest thatphosphodiesterase 5 inhibition could work as an antiremodeling drug by acting directly on cardiac tissue, independentlyof other secondary vascular, endothelial, or metabolic effects. Our findings also have an impact on the clinical monitoringof patients with type 2 diabetes mellitus. We showed that (1) asymptomatic diabetic men may already be undergoingcardiac remodeling; (2) monocyte chemotactic protein-1 [MCP1] could be included as a new potential marker related todiabetic cardiomyopathy evolution; and (3) sildenafil can partially reverse these changes. Large-scale studies are neededto test whether phosphodiesterase 5A inhibition could become a new target for antiremodeling drugs and to discover themolecular pathways affected by this class of drugs.
Giannetta et al Sildenafil Improves Diabetic Cardiomyopathy 2333
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
1
SUPPLEMENTAL MATERIAL
SUPPLEMENTAL METHODS
1. Abbreviations used in the MS
PDE5: Phosphodesterase-type-5; NO: nitric oxide; PKG: protein kinase G.
T2DM: Type 2 diabetes mellitus; HbA1c: glycated hemoglobin HOMAi: homeostatic model assessment index; eGFR:
estimated glomerular filtration rate; TGD: Triglyceride; HDL: High density lipoproteins; BMI: Body mass index; SBP:
Systolic blood pressure; DBP: Diastolic blood pressure.
NT-proBNP: pro-hormone of N-terminal brain natriuretic peptide; P1NP: Pro-collagen 1 N-terminal peptide; TGF-β:
Transforming growth factor-β; MCP1: Monocyte chemotactic protein 1; VEGF: Vascular endothelial growth factor; ET-
1: Endothelin-1.
CMR: Cardiac magnetic resonance imaging; LV: Left ventricle; LVMi: Left ventricular mass index; EDVi: End-diastolic
volume index; ESV: End-systolic volume; SV: Stroke volume; CO: Cardiac output; CI: Cardiac index; EF: Ejection
fraction; : Strain; : Torsion; Ventricular TD: Ventricular transverse diameter; FMD: Flow-mediated vasodilation.
2. LV function during systolic torsion and diastolic recoil
Non-linear regression analysis with dynamic fit was used to identify the best equation describing
torsion during systole and diastole 1,2 for each patient (Sigmaplot 11.0, Systat Software Inc,
Chicago, IL). LV function during systole was defined by the coefficients of a monoexponential rise
to a non-zero asymptote as t(t)=Tmax[1-exp(bt·t)] where t (t) is the instantaneous LV torsion, Tmax
is the asymptotic maximum torsion, and bt is the torsion time constant. All time frames from null to
maximum torsion were fitted into the model. LV function in early diastole was explored by
interpolating the time of decline of Tmax during isovolumetric relaxation. Shapiro and colleagues
have clearly demonstrated a rapid recoil of about 40% of the torsion accumulating during systole.3,4
Therefore all frames within max and max-40% were regressed to a monoexponential decay (with a
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
2
zero-torsion asymptote) as ut(t)=T0exp(-but·t) where ut(t) is the instantaneous LV recoil, T0 is the
initial torsion before the onset of torsion decay, and but is the recoil time constant. Analogously with
the relaxation constant (t), the recoil time constant (but) can be used as an index for LV relaxation.
Figure 1S provides examples of CMR torsion data before (top) and after (bottom) the treatment
period in two random patients, one treated with sildenafil (left) and the other with placebo (right).
The goodness of fit of the monoexponential models (for the entire systole and for isovolumetric
relaxation, defined as 40% reduction in max) was demonstrated by an r2 >0.9 for all sets of data.
Although previous studies showed that the monoexponential fit was poor during the first 10-20 ms
after the peak torsion,5 this was negligible in our group (data not shown) and not relevant to the
analyses of the effects of treatment.
Equation A (torsion): Tt(t)=Tmax[1-exp(bt·t)]
Equation B (recoil): Tut(t)=T0exp(-but·t)
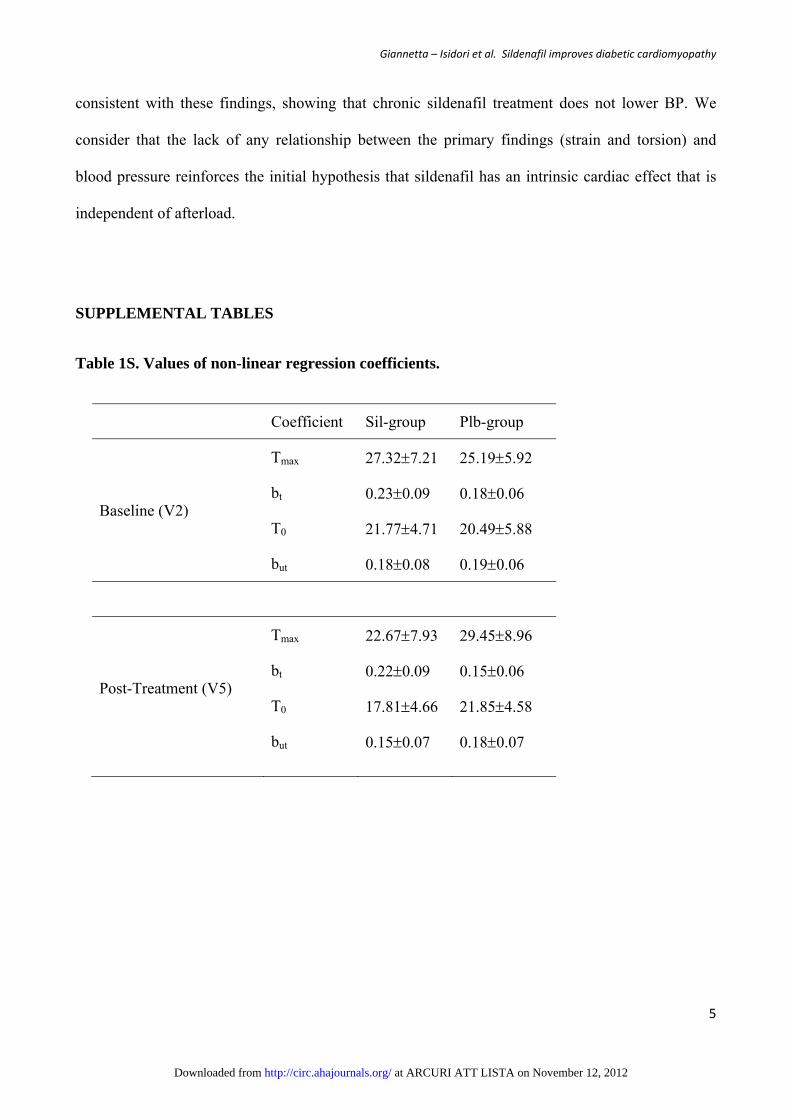
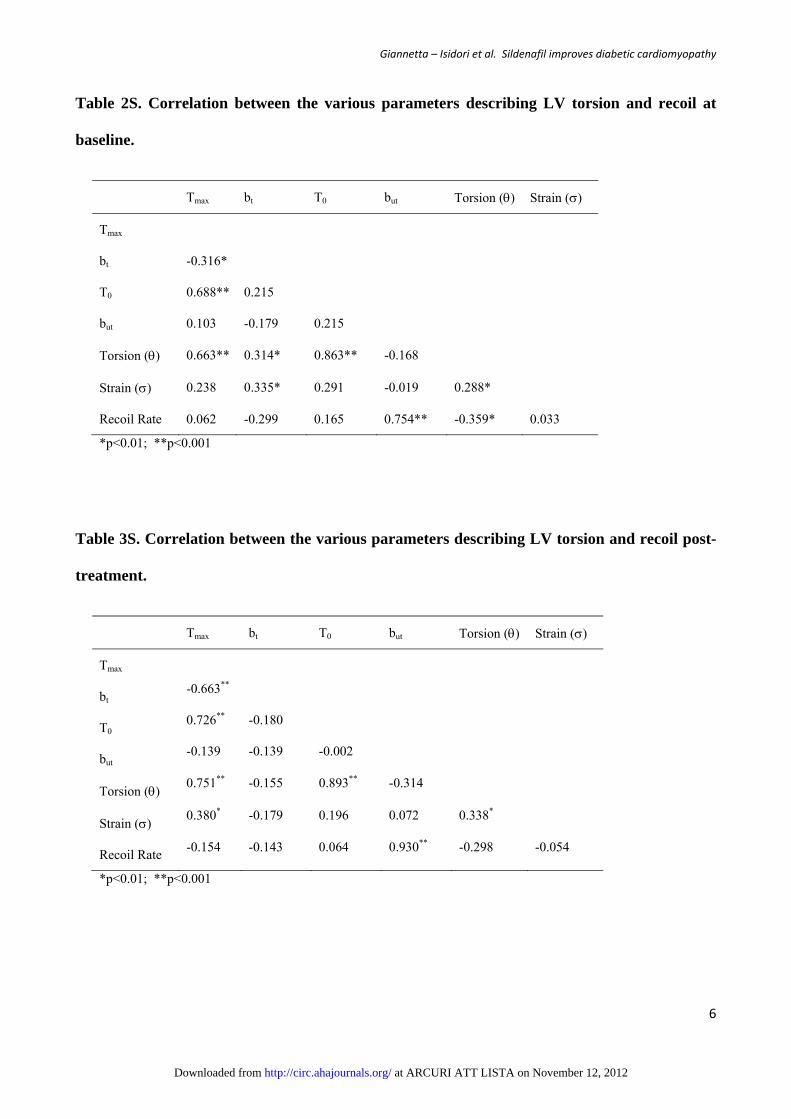
Table 1S reports the complete data for the coefficients.
The advantage of using the coefficients of the monoexponential models rather than absolute
peak/nadir values or velocities is that the b coefficients (bt and but) are constant throughout the
curve (during isovolumetric relaxation). For diastolic function, this enabled the analysis to be
restricted to the early 40% reduction in maximum torsion that occurs at a fixed volume, avoiding
interference from late diastolic filling.3,6 These coefficients, including the asymptotic coefficient
(Tmax) and T0, are also less affected by single frame measurement errors, as they are generated by
interpolation of a minimum of 4 frames during early diastole and 6-10 frames during systolic
torsion. Their accuracy is confirmed by the strong correlation of bt, but, Tmax and T0 with peak
torsion, peak strain and recoil rate measured with traditional formulas both at the baseline and after
treatment (Table 2S and 3S).
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
3
Equation A is also the mathematical solution of the equation describing the Force (Tf) that gives
Torsion () in this model:
Equation (C) Tf = R · + L · (d /dt)
where = angle of torsion (twist)
R · = Torque Spring Return
L · (d/dt) = Viscous Friction
The angle of ventricular torsion measured by MR can therefore be described by the following
equation:
Equation (D) t=Tf/R [1-exp(R/L·t)]
Where Tf/R = Tmax (the asymptotic maximum torsion)
and R/L = bt (the torsion time constant)
Although this is a oversimplified model, Equation D supports the hypothesis that the parameters
describing CMR LV torsion are directly related to contraction and the viscoelasticity of the
myocardium.
3. Laboratory investigations
We measured chemokines reflecting cardiac remodeling: BNP, pro-BNP, PINP, TGF, MCP1; and
endothelial function: IL6; ET1; VEGF. Serum samples obtained at the baseline (time 0) and end
(time + 3 months) visits were analyzed by ELISA. TGF, MCP1, IL6, VEGF were assayed with
quantitative sandwich enzyme immunoassay (Quantikine, R&D Systems, Abingdon, UK). The
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
4
minimum detectable levels were TGF 4.61 pg/ml, MCP1 5 pg/ml, IL6 0.7 pg/ml, VEGF 9 pg/ml.
The mean intra- and inter-assay coefficients of variation (CV) were < 8% and < 10%.
Serum BNP and ET-1 were measured with an enzyme immunoassay kit (Phoenix Pharmaceuticals
Inc., Burlingame, CA). The minimum detectable levels were BNP 0.36 ng/ml and ET1 0.12 ng/ml.
The intra-assay CV was 5-10% and the inter-assay CV <15% for both parameters. Human
Procollagen I N-Terminal Peptide was assayed with ELISA kit (Cusabio Biotech Co., Ltd. Newark,
DE): the minimum detectable level was 4.7 pg/ml, and the intra- and inter-assays CV were <10%.
NT-proBNP was analyzed from serum samples stored at -80°C until analysis by
electrochemiluminescence immunoassay on the Elecsys 1010/2010 System (ECLIA, Roche
Diagnostics, Basel, Switzerland). The functional assay sensitivity (inter-assay CV 20%) was 5.9
pmol/L.
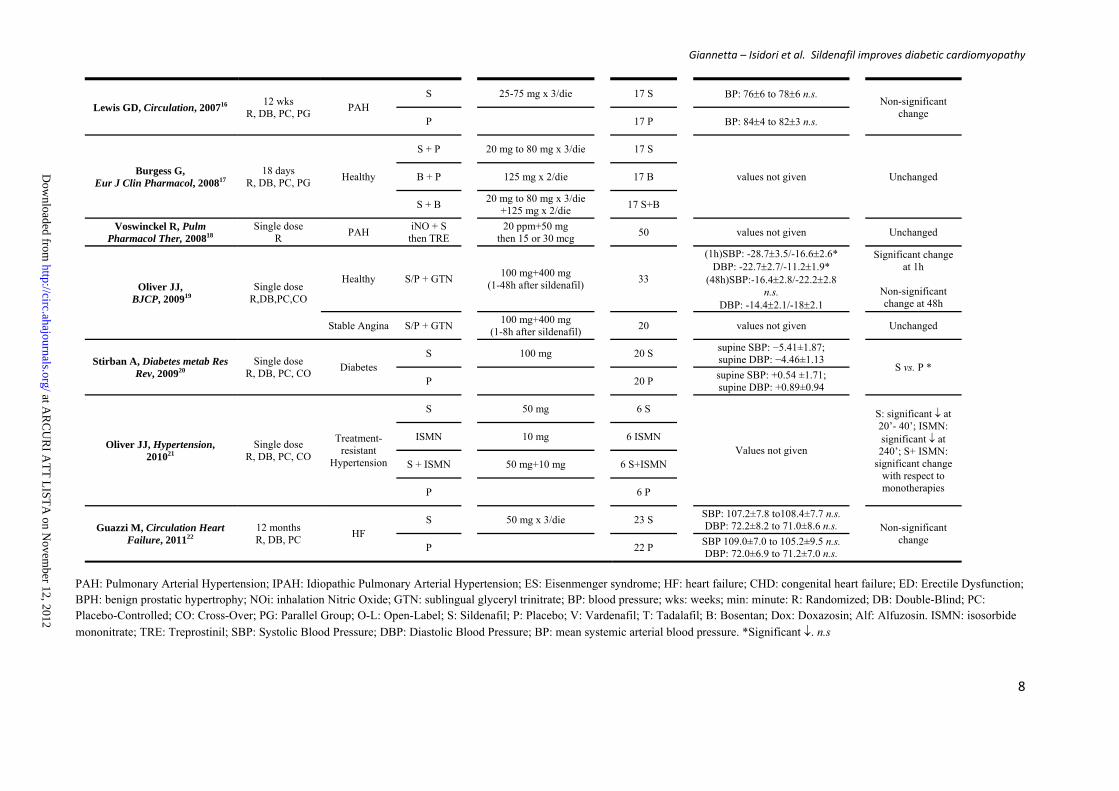
4.Effects of PDE5i on systemic blood pressure (BP)
We performed a systematic review of the literature over the past 10 years for randomized controlled
trials (RCTs) on the use of sildenafil reporting data on BP changes. 16 RCTs were found (Table
4S): 9 (Trial Group A) evaluating the acute effects of sildenafil (from a single-dose administration
to 16 days) and 7 (Trial Group B) using chronic treatment (from 6 weeks to 12 months). The
populations studied included healthy subjects and patients variously affected by pulmonary arterial
hypertension, high blood pressure, diabetes mellitus and heart failure. The results of these trials are
summarized in Table 4S. Overall, 5 of the 9 Group A trials showed an acute antihypertensive effect.
Of note is that no BP change was seen when sildenafil was given to healthy subjects or patients with
controlled hypertension. In the group B trials, higher doses of sildenafil such as those used in
pulmonary hypertension trials produced no change in blood pressure over time. Our results are
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from
Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
5
consistent with these findings, showing that chronic sildenafil treatment does not lower BP. We
consider that the lack of any relationship between the primary findings (strain and torsion) and
blood pressure reinforces the initial hypothesis that sildenafil has an intrinsic cardiac effect that is
independent of afterload.
SUPPLEMENTAL TABLES
Table 1S. Values of non-linear regression coefficients.
Coefficient Sil-group Plb-group
Baseline (V2)
Tmax 27.327.21 25.195.92
bt 0.230.09 0.180.06
T0 21.774.71 20.495.88
but 0.180.08 0.190.06
Post-Treatment (V5)
Tmax 22.677.93 29.458.96
bt 0.220.09 0.150.06
T0 17.814.66 21.854.58
but 0.150.07 0.180.07
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from
Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
6
Table 2S. Correlation between the various parameters describing LV torsion and recoil at
baseline.
Tmax bt T0 but Torsion () Strain ()
Tmax
bt -0.316*
T0 0.688** 0.215
but 0.103 -0.179 0.215
Torsion () 0.663** 0.314* 0.863** -0.168
Strain () 0.238 0.335* 0.291 -0.019 0.288*
Recoil Rate 0.062 -0.299 0.165 0.754** -0.359* 0.033
*p<0.01; **p<0.001
Table 3S. Correlation between the various parameters describing LV torsion and recoil post-
treatment.
Tmax bt T0 but Torsion () Strain ()
Tmax
bt -0.663**
T0 0.726** -0.180
but -0.139 -0.139 -0.002
Torsion () 0.751** -0.155 0.893** -0.314
Strain () 0.380* -0.179 0.196 0.072 0.338*
Recoil Rate -0.154 -0.143 0.064 0.930** -0.298 -0.054
*p<0.01; **p<0.001
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
7
Table 4S. Major RCTs evaluating the effects of sildenafil on systemic blood pressure.
Studies Study Design Condition Treatment
Dose
N° Patients
Systemic Blood Pressure
Results
Zhao L, Circulation, 20017 Single dose R, DB, PC
Healthy S
50 mg
5 S
SBP:1127.1 to10612.6 n.s. DBP: 696.2 to 588.2 n.s.
Non-significant change
P
5 P SBP:1125.9 to11014.4 n.s.
DBP: 675.4 to 598.6 n.s.
Ghofrani HA, J Am Coll Cardiol, 20048
Single dose R
PAH
NOi + S 20-40 ppm +50 mg 19 S BP: -6.9 (-4.5 to -8.8) *
Significant reduction at 120’
NOi + V 20-40 ppm
+10 or 20 mg 7 V (10mg)
9 V (20mg) BP: -6.9 (-17.1 to 1.5)*;
-12.1 (-8.1 to -16.9) *
NOi + T
20-40 ppm +20 or 40 or 60 mg
9 T (20mg) 8 T (40mg) 8 T (60mg)
BP: -6.9 (-0.8 to-16.1) *; -7.3 (-0.9 to-14.4)*; -1.1 (-8.6 to8.5) n.s.
Sastry BKS, JACC, 20049 6 wks
R, DB, CO PAH
S 25-100 mg x 3/die 22 S values not given
Unchanged
P 22 P
Aldashev AA, Thorax, 200510 3 months
R, DB, PC High altitude
PAH
S
25 mg x 3/die
9 S SBP: 12722 to12519;
DBP: 7710 to 787 n.s.
Non-significant change
S
100 mg x 3/die
5 S SBP: 13220to12718;
DBP: 807 to 812 n.s.
P
8 P SBP: 1188to12313;
DBP: 755to756 n.s.
Richalet J-P, Am J Respir Crit Care Med,
200511
6 days R, DB, PC
Healthy (Altitude)
S 40 mg x 3/die 6 S values not given
Unchanged
P 6 P
Wilkins MR, Am J Respir and Crit Care
Med, 200512
16 wks R, DB
PAH and Connective
tissue Disease
S 50 mg x2/die (4 wks),
50mg x3/die (12wks)
13 S SBP:5(-6 to16);
DBP:‐4 (-11 to 2)
Non-significant change
B 62.5mgx2/die (4
wks),125mgx2/die (12wks)
12 B
SBP:-1(-10 to 8); DBP:1 (-8 to 9)
Oliver JJ, Hypertension, 200613
16 days R, DB, PC, CO
Hypertension
S
50 mg x 3/die
22 S SBP: -52;
DBP: -51
S vs. P * P
22 P
SBP:42; DBP:22
Namachivayam P, Am J Respir Crit Care Med, 200614
Single dose R, DB, PC
Ventilated infant
NOi + S 10 ppm + 0.4 mg/kg 15 S BP: 58.711.8 to 56.89.2 n.s. Non-significant change
at 1h and 4h NOi + P 14 P BP: 64.514.0 to 63.313.5 n.s.
Singh TP, Am Heart J, 200615
6 wks R, DB, PC, CO
PAH-ES S
100 mg x 3/die
10 S
(values not given)
Unchanged P
10 P
at AR
CU
RI A
TT
LIST
A on N
ovember 12, 2012
http://circ.ahajournals.org/D
ownloaded from
Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
8
Lewis GD, Circulation, 200716 12 wks
R, DB, PC, PG PAH
S
25-75 mg x 3/die
17 S
BP: 766 to 786 n.s.
Non-significant change
P
17 P
BP: 844 to 823 n.s.
Burgess G, Eur J Clin Pharmacol, 200817
18 days R, DB, PC, PG
Healthy
S + P
20 mg to 80 mg x 3/die
17 S
values not given
Unchanged B + P
125 mg x 2/die
17 B
S + B 20 mg to 80 mg x 3/die
+125 mg x 2/die
17 S+B
Voswinckel R, Pulm Pharmacol Ther, 200818
Single dose R
PAH iNO + S
then TRE 20 ppm+50 mg
then 15 or 30 mcg
50
values not given
Unchanged
Oliver JJ, BJCP, 200919
Single dose R,DB,PC,CO
Healthy S/P + GTN
100 mg+400 mg (1-48h after sildenafil)
33
(1h)SBP: -28.73.5/-16.62.6* DBP: -22.72.7/-11.21.9*
(48h)SBP:-16.42.8/-22.22.8 n.s.
DBP: -14.42.1/-182.1
Significant change at 1h
Non-significant change at 48h
Stable Angina S/P + GTN 100 mg+400 mg
(1-8h after sildenafil)
20
values not given
Unchanged
Stirban A, Diabetes metab Res Rev, 200920
Single dose R, DB, PC, CO
Diabetes S
100 mg
20 S
supine SBP: −5.41±1.87; supine DBP: −4.46±1.13
S vs. P * P
20 P
supine SBP: +0.54 ±1.71; supine DBP: +0.89±0.94
Oliver JJ, Hypertension, 201021
Single dose R, DB, PC, CO
Treatment- resistant
Hypertension
S
50 mg
6 S
Values not given
S: significant at 20’- 40’; ISMN: significant at 240’; S+ ISMN:
significant change with respect to monotherapies
ISMN
10 mg
6 ISMN
S + ISMN
50 mg+10 mg
6 S+ISMN
P
6 P
Guazzi M, Circulation Heart Failure, 201122
12 months R, DB, PC
HF S
50 mg x 3/die
23 S
SBP: 107.2±7.8 to108.4±7.7 n.s. DBP: 72.2±8.2 to 71.0±8.6 n.s.
Non-significant change
P
22 P SBP 109.0±7.0 to 105.2±9.5 n.s.
DBP: 72.0±6.9 to 71.2±7.0 n.s.
PAH: Pulmonary Arterial Hypertension; IPAH: Idiopathic Pulmonary Arterial Hypertension; ES: Eisenmenger syndrome; HF: heart failure; CHD: congenital heart failure; ED: Erectile Dysfunction; BPH: benign prostatic hypertrophy; NOi: inhalation Nitric Oxide; GTN: sublingual glyceryl trinitrate; BP: blood pressure; wks: weeks; min: minute: R: Randomized; DB: Double-Blind; PC: Placebo-Controlled; CO: Cross-Over; PG: Parallel Group; O-L: Open-Label; S: Sildenafil; P: Placebo; V: Vardenafil; T: Tadalafil; B: Bosentan; Dox: Doxazosin; Alf: Alfuzosin. ISMN: isosorbide
mononitrate; TRE: Treprostinil; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; BP: mean systemic arterial blood pressure. *Significant . n.s
at AR
CU
RI A
TT
LIST
A on N
ovember 12, 2012
http://circ.ahajournals.org/D
ownloaded from

Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
9
SUPPLEMENTAL FIGURE
Figure 1S.
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
10
LEGEND TO SUPPLEMENTAL FIGURES
Figure 1S.
Non-linear regression of torsion (systole) and recoil (diastole) in two patients. Dots represent
instant absolute values of torsion during the cardiac cycle (expressed as percentage of systole
duration). The regression line is solid black with 95% CI in blue. Red lines indicate the 95%
prediction band. Left panels show CMR data before (A) and after (C) sildenafil treatment; the
right panels show CMR data before (B) and after (D) placebo. Upper and lower panels are from
the same subject in both treatment groups.
SUPPLEMENTAL REFERENCES
1. Zerhouni EA. Human heart: tagging with MR imaging--a method for noninvasive assessment of myocardial motion. 1988.
2. Axel L. Heart wall motion: improved method of spatial modulation of magnetization for MR imaging. 1989.
3. Dong SJ. MRI assessment of LV relaxation by untwisting rate: a new isovolumic phase measure of tau. 2001.
4. Hees PS, Fleg JL, Dong SJ, Shapiro EP. MRI and echocardiographic assessment of the diastolic dysfunction of normal aging: altered LV pressure decline or load? Am J Physiol Heart Circ Physiol. 2004; 286: H782-H788.
5. Matsubara H. Logistic time constant of isovolumic relaxation pressure-time curve in the canine left ventricle. Better alternative to exponential time constant. 1995.
6. Thompson RB. Characterization of the relationship between systolic shear strain and early diastolic shear strain rates: insights into torsional recoil. 2010.
7. Zhao L, Mason NA, Morrell NW, Kojonazarov B, Sadykov A, Maripov A, Mirrakhimov MM, Aldashev A, Wilkins MR. Sildenafil inhibits hypoxia-induced pulmonary hypertension. Circulation. 2001; 104: 424-428.
8. Ghofrani HA, Voswinckel R, Reichenberger F, Olschewski H, Haredza P, Karadas B, Schermuly RT, Weissmann N, Seeger W, Grimminger F. Differences in hemodynamic and oxygenation responses to three different phosphodiesterase-5 inhibitors in patients with
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from

Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
11
pulmonary arterial hypertension: a randomized prospective study. J Am Coll Cardiol. 2004; 44: 1488-1496.
9. Sastry BK, Narasimhan C, Reddy NK, Raju BS. Clinical efficacy of sildenafil in primary pulmonary hypertension: a randomized, placebo-controlled, double-blind, crossover study. J Am Coll Cardiol. 2004; 43: 1149-1153.
10. Aldashev AA, Kojonazarov BK, Amatov TA, Sooronbaev TM, Mirrakhimov MM, Morrell NW, Wharton J, Wilkins MR. Phosphodiesterase type 5 and high altitude pulmonary hypertension. Thorax. 2005; 60: 683-687.
11. Richalet JP, Gratadour P, Robach P, Pham I, Dechaux M, Joncquiert-Latarjet A, Mollard P, Brugniaux J, Cornolo J. Sildenafil inhibits altitude-induced hypoxemia and pulmonary hypertension. Am J Respir Crit Care Med. 2005; 171: 275-281.
12. Wilkins MR, Paul GA, Strange JW, Tunariu N, Gin-Sing W, Banya WA, Westwood MA, Stefanidis A, Ng LL, Pennell DJ, Mohiaddin RH, Nihoyannopoulos P, Gibbs JS. Sildenafil versus Endothelin Receptor Antagonist for Pulmonary Hypertension (SERAPH) study. Am J Respir Crit Care Med. 2005; 171: 1292-1297.
13. Oliver JJ, Melville VP, Webb DJ. Effect of regular phosphodiesterase type 5 inhibition in hypertension. Hypertension. 2006; 48: 622-627.
14. Namachivayam P, Theilen U, Butt WW, Cooper SM, Penny DJ, Shekerdemian LS. Sildenafil prevents rebound pulmonary hypertension after withdrawal of nitric oxide in children. Am J Respir Crit Care Med. 2006; 174: 1042-1047.
15. Singh TP, Rohit M, Grover A, Malhotra S, Vijayvergiya R. A randomized, placebo-controlled, double-blind, crossover study to evaluate the efficacy of oral sildenafil therapy in severe pulmonary artery hypertension. Am Heart J. 2006; 151: 851-855.
16. Lewis GD, Shah R, Shahzad K, Camuso JM, Pappagianopoulos PP, Hung J, Tawakol A, Gerszten RE, Systrom DM, Bloch KD, Semigran MJ. Sildenafil improves exercise capacity and quality of life in patients with systolic heart failure and secondary pulmonary hypertension. Circulation. 2007; 116: 1555-1562.
17. Burgess G, Hoogkamer H, Collings L, Dingemanse J. Mutual pharmacokinetic interactions between steady-state bosentan and sildenafil. Eur J Clin Pharmacol. 2008; 64: 43-50.
18. Voswinckel R, Reichenberger F, Enke B, Kreckel A, Krick S, Gall H, Schermuly RT, Grimminger F, Rubin LJ, Olschewski H, Seeger W, Ghofrani HA. Acute effects of the combination of sildenafil and inhaled treprostinil on haemodynamics and gas exchange in pulmonary hypertension. Pulm Pharmacol Ther. 2008; 21: 824-832.
19. Oliver JJ, Kerr DM, Webb DJ. Time-dependent interactions of the hypotensive effects of sildenafil citrate and sublingual glyceryl trinitrate. Br J Clin Pharmacol. 2009; 67: 403-412.
20. Stirban A, Laude D, Elghozi JL, Sander D, Agelink MW, Hilz MJ, Ziegler D. Acute effects of sildenafil on flow mediated dilatation and cardiovascular autonomic nerve function in type 2 diabetic patients. Diabetes Metab Res Rev. 2009; 25: 136-143.
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from
Giannetta – Isidori et al. Sildenafil improves diabetic cardiomyopathy
12
21. Oliver JJ, Dear JW, Webb DJ. Clinical potential of combined organic nitrate and phosphodiesterase type 5 inhibitor in treatment-resistant hypertension. Hypertension. 2010; 56: 62-67.
22. Guazzi M, Vicenzi M, Arena R, Guazzi MD. PDE5 inhibition with sildenafil improves left ventricular diastolic function, cardiac geometry, and clinical status in patients with stable systolic heart failure: results of a 1-year, prospective, randomized, placebo-controlled study. Circ Heart Fail. 2011; 4: 8-17.
at ARCURI ATT LISTA on November 12, 2012http://circ.ahajournals.org/Downloaded from
Related Documents











