Chemoimmunotherapy of Disseminated Malignant Melanoma with OTIC-BCG, Transfer Factor + Melphalan MAX A. SCHWARZ, MB, BS, FRCP,'t JORDAN U. GUTTERMAN, MD, FACP,* MICHAEL A. BURGESS, MD,* LANCE K. HEILBRUN, PHD,* WILLIAM K. MURPHY, MD,* GERALD P. BODEY, MD, FACP,* E. STONE, BS,* V. TURNER-CHISM, BS,* AND EVAN M. HERSH, MD* The experimental synergism of melphalan with DTIC and the ahility of transfer factor to improve immunocompetence were the basis of an attempt to improve therapeutic results in disseminated malig- nant melanoma. Sixty-four evaluable patients with disseminated malignant melanoma were treated in a 21-day cycle as follows: DTIC 250 mg/M2intravenously days 1 to 5, Connaught BCG 6 x 10' organisms on days 7, 12, and 17 by scarification, and transfer factor 1 unit (10:' lymphocytes equivalent, from immunocompetent relatives of patients) subcutaneously on day 12, with or without L-PAM 30 mg/M' on day 1. Twenty-nine patients received L-PAM and 35 did not. Remission rates of 17% and 23%, respectively, occurred in these groups. An additional 15 patients received DTIC-BCG and three doses of transfer factor on days 7, 12, and 17 and had a remission rate of 20%. Remission duration and survival were compared to historical controls of 111 patients treated with DTIC and 89 treated with DTIC-BCG. Median survival on DTIC-BCG-Transfer Factor was seven months compared to four months for DTIC (P = .003) but did not differ from DTIC-BCG. Addition of L P A M did not improve remission duration or survival compared to DTIC-BCG but enhanced myelosuppression and immunosuppression. A 60% increase in delayed type hypersensitivity to recall antigens occurred in this study compared to 34% with DTIC-BCG (P = .005). Prognosis and immunocompetence were not directly related. In summary, in this study, (1) transfer factor therapy did not enhance the clinical effects of DTIC-BCG, although it augmented delayed type hypersensitivity to recall antigens; and (2) L-PAM was not additive to DTIC in the treatment of disseminated malignant melanoma and may have abrogated the effect of immunotherapy . Cancer 45:2506-2515, 1980. I-THOUGH DIMETHYL TRIAZENO imidazole car- A boxamide (DTIC) either alone or in combination with other chemotherapeutic agents is the single most active drug for the treatment of patients with dis- seminated malignant melanoma, response rates are low (14-25%).i.8.2i Rates of complete response of only 5% are observed consistently.x In general, the duration of From the "Department of Developmental Therapeutics and $Biomathematics, The University of Texas System Cancer Center these responses is short with a median survival of all treated patients of only 4.6 In most studies, responding patients survive significantly longer com- pared to non-responders.x*2i Active immunotherapy with Bacillus Calmette- Guerin (BCG) combined with DTIC has resulted in an increased remission rate in metastatic areas regional to BCG vaccination, namely lymph node and cutaneous metastases. The duration of remission, and in particular M. D. Anderson Hospital and Tumor Institute, Houston, Texas. of survival, was significantly longer for patients with CM-57042, Core Grant CA 16672 and Grant CA 14984 from the both non-visceral and visceral metastases treated with National Cancer Institute, National Institutes of Health. U. S. chernoimmunotherapy than for those treated with Supported in part by Contract N01-CB-33888. Contract N01- Public Health Service, Bethesda, Maryland. ment Award (CA 71001 03) from the National Cancer Institute. chemotherapy alone.'" Dr. Gutterman is the recipient of a Research Career Develop- In many ways, DTJC appears to be an ideal drug Dr. Schwarz is the recipient of a Fulbright-Hays Scholarship. to combine with immunotherapy. In contrast to most -- ; Current address: Monash University, Department of Medicine, Monash Medical School. Alfred Hospital, Prahran, Victoria. 3181, chemotherapeutic agents, it is minimally immune- suppressive in man"; in addition, DTIC has been shown Australia. The authors thank Lou Hackenberry, Martha Marshall, Kathy to augment the immunogenicity of tumor cells in Barlogie, and Madeline Cantini for excellent assistance, and Pat Wise for excellent secretarial help. various experimental model systems.:" Finally, there does not appear to be any definite schedule or dose- Accepted for publication June 13, 1979. 0008-543X/80/0515/2506 $1.00 Q American Cancer Society 2506

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chemoimmunotherapy of Disseminated Malignant Melanoma with OTIC-BCG, Transfer Factor + Melphalan
MAX A. SCHWARZ, MB, BS, FRCP,'t JORDAN U. GUTTERMAN, MD, FACP,* MICHAEL A. BURGESS, MD,* LANCE K. HEILBRUN, PHD,* WILLIAM K. MURPHY, MD,* GERALD P. BODEY, MD, FACP,* E. STONE, BS,*
V. TURNER-CHISM, BS,* AND EVAN M. HERSH, MD*
The experimental synergism of melphalan with DTIC and the ahility of transfer factor to improve immunocompetence were the basis of an attempt to improve therapeutic results in disseminated malig- nant melanoma. Sixty-four evaluable patients with disseminated malignant melanoma were treated in a 21-day cycle as follows: DTIC 250 mg/M2 intravenously days 1 to 5 , Connaught BCG 6 x 10' organisms on days 7, 12, and 17 by scarification, and transfer factor 1 unit (10:' lymphocytes equivalent, from immunocompetent relatives of patients) subcutaneously on day 12, with or without L-PAM 30 mg/M' on day 1. Twenty-nine patients received L-PAM and 35 did not. Remission rates of 17% and 23%, respectively, occurred in these groups. An additional 15 patients received DTIC-BCG and three doses of transfer factor on days 7, 12, and 17 and had a remission rate of 20%. Remission duration and survival were compared to historical controls of 11 1 patients treated with DTIC and 89 treated with DTIC-BCG. Median survival on DTIC-BCG-Transfer Factor was seven months compared to four months for DTIC (P = .003) but did not differ from DTIC-BCG. Addition of L P A M did not improve remission duration or survival compared to DTIC-BCG but enhanced myelosuppression and immunosuppression. A 60% increase in delayed type hypersensitivity to recall antigens occurred in this study compared to 34% with DTIC-BCG (P = .005). Prognosis and immunocompetence were not directly related. In summary, in this study, (1) transfer factor therapy did not enhance the clinical effects of DTIC-BCG, although it augmented delayed type hypersensitivity to recall antigens; and (2) L-PAM was not additive to DTIC in the treatment of disseminated malignant melanoma and may have abrogated the effect of immunotherapy .
Cancer 45:2506-2515, 1980.
I-THOUGH DIMETHYL TRIAZENO imidazole car- A boxamide (DTIC) either alone or in combination with other chemotherapeutic agents is the single most active drug for the treatment of patients with dis- seminated malignant melanoma, response rates are low (14-25%).i.8.2i Rates of complete response of only 5% are observed consistently.x In general, the duration of
From the "Department of Developmental Therapeutics and $Biomathematics, The University of Texas System Cancer Center
these responses is short with a median survival of all treated patients of only 4.6 In most studies, responding patients survive significantly longer com- pared to non-responders.x*2i
Active immunotherapy with Bacillus Calmette- Guerin (BCG) combined with DTIC has resulted in an increased remission rate in metastatic areas regional to BCG vaccination, namely lymph node and cutaneous metastases. The duration of remission, and in particular
M. D. Anderson Hospital and Tumor Institute, Houston, Texas. of survival, was significantly longer for patients with CM-57042, Core Grant CA 16672 and Grant CA 14984 from the both non-visceral and visceral metastases treated with National Cancer Institute, National Institutes of Health. U . S. chernoimmunotherapy than for those treated with
Supported in part by Contract N01-CB-33888. Contract N01-
Public Health Service, Bethesda, Maryland.
ment Award (CA 71001 03) from the National Cancer Institute.
chemotherapy alone.'" Dr. Gutterman is the recipient of a Research Career Develop- In many ways, DTJC appears to be an ideal drug Dr. Schwarz is the recipient of a Fulbright-Hays Scholarship. to combine with immunotherapy. In contrast to most - - ; Current address: Monash University, Department of Medicine,
Monash Medical School. Alfred Hospital, Prahran, Victoria. 3181, chemotherapeutic agents, it is minimally immune- suppressive in man"; in addition, DTIC has been shown Australia.
The authors thank Lou Hackenberry, Martha Marshall, Kathy to augment the immunogenicity of tumor cells in Barlogie, and Madeline Cantini for excellent assistance, and Pat Wise for excellent secretarial help. various experimental model systems.:" Finally, there
does not appear to be any definite schedule or dose- Accepted for publication June 13, 1979.
0008-543X/80/0515/2506 $1.00 Q American Cancer Society
2506

No. 10 CHhMOIMMUNOI H t R A P Y OF DlSSFMINATtD MALIGNANT MELANOMA . .Yci'2bt3(1I.,: ('t (11. 2507
dependent relationship of DTlC to its therapeutic effect.H
There is evidence that the immunocompetence and prognosis of patients with cancer are related." Pre- vious studies have demonstrated that immunocompe- tent melanoma patients receiving immunotherapy had a better prognosis than similarly treated immuno- incompetent patients." These data suggested that immunoincompetent patients may require immune restoration in order to respond to active non-specific immunotherapy with microbial adjuvants and perhaps even to chemotherapy. Transfer factor (TF) is a dialyz- able low molecular weight polypeptide that can be extracted from lymphocytes'" capable of transferring the delayed type hypersensitivity immunity of the donor to a previously non-immunized recipient." This transferred immunity usually persists for 6- 12 months in non-cancer patients.2h Although transfer factor can also convert skin test anergy to reactivity in cancer patients, this systemic immunity is of much shorter d ~ r a t i o n . ~ "
Melphalan (L-PAM) has been extensively used for isolated limb perfusions in the treatment of regional malignant melanoma following primary surgical ther- apy with improved regional control rates.4i The activity of melphalan as a systemic agent in disseminated malignant melanoma is limited, with an overall re- sponse rate of no more than 15% in several older studies.x However, experimental synergism of mel- phalan with DTIC has recently been demonstrated."' This experimental synergism of melphalan with DTIC." and the ability of transfer factor to improve immuno- competence2j were the basis of an attempt to improve the therapeutic results and prognosis in patients with disseminated malignant melanoma.
Patients and Methods Eighty-seven patients with overt disseminated malig-
nant melanoma (Stage IVB)'X were consecutively entered on the study between March 28, 1975 and November 5 , 1975. An additional 7 patients would have been eligible for the study but transfer factor donors were not available for them and they were not treated on this protocol. Of the 87 patients entered on the study, 79 were evaluable, having received an adequate trial of one or more complete courses of chemoimmunotherapy . Of the remaining 8 patients, 4 patients died within the first three weeks and were considered early deaths, and 4 patients had overt cerebral metastases at presentation and were treated with whole brain irradiation, steroids, and DTIC but did not receive BCG or transfer factor therapy.
Prior to the initiation of therapy, patients were evaluated for metastatic disease with the following
' r l B 1 t 1. Summary of Treatment Regimen\'
Entered 87 patients Inevaluable 8 patients Evaluahle 79 patients
/ \ Transfer factor on day 12 of each treatment course
Transfer factor on days 7. I ? , 17 of each treatment course
64 patients
Kdndomire
IA\t 15 evaludble patient5
35 p i t l en t \ 29 patients (DTIC BCG) (DTIC BCG) (DTIC BCG
+ melphalan)
* See text for details.
tests: physical examination, complete blood count, urinalysis, tests of liver and renal function, chest x-ray, liver scan, brain scan, electroencephalogram, and bone marrow biopsy. When specific symptoms indicated, a metastatic bone survey or radiological examination of the gastrointestinal tract or both were performed. Table 1 summarizes patient treatment details.
Sixty-four evaluable patients with disseminated malignant melanoma (Stage IVB) were treated in a 21- day cycle as follows, if blood counts permitted: (1) DTIC 250 mgiM' intravenously days 1 to 5; (2) Con- naught BCG 6 x lox organisms on days 7, 12, and 17 by scarification as previously describedI6; (3) Transfer factor 1 unit ( lo9 lymphocytes equivalent from immu- nocompetent relatives of patients as described below) subcutaneously on day 12; (4) In addition, patients were randomized to either receive or not to receive melphalan (L-PAM) 30 mgiM' on day 1 only. Initially, this was given orally one hour before the first dose of DTIC, but because of moderately severe nausea and vomiting induced by DTIC in a large proportion of patients, L-PAM was subsequently administered intra- venously. Twenty-nine patients received L-PAM and 35 did not. The first 9 patients received melphalan orally: the remaining 20 received it intravenously.
The last 15 evaluable Stage IVB patients received DTIC-BCG as described, but more intensive transfer factor therapy consisting of 1 unit of transfer factor on days 7 , 12, and 17 of each 21-day cycle. This group did not receive melphalan because this randomization was abandoned following preliminary study analysis that suggested patients receiving melphalan did less well.
Chemotherapy dosage was adjusted as follows for patients treated with DTIC-BCG-Tranufer Factor. If myelosuppression did not occur during the initial course, that is, the platelet count remained above
CANCER May I5 1980 Vol. 45
TABLE 2. Clinical Features of 79 Stage IV B Patients with Disseminated Malignant Melanoma Treated with DTIC BCG Transfer Factor ? L-PAM: 89 Treated with DTIC-BCG and 11 1 Treated with DTIC
DTIC DTIC-BCG DTIC-BCG-TF DTIC-BCG-TF + L-PAM Clinical feature (1 11 patients) (89 patients) (50 patients) (29 patients)
Median Age (yrs) Male (5%) Female (%)
Metastasis (%) Non-visceral Visceral Pulmonary Non-pulmonary
Trunk Head and neck Extremities Ocular Unknown
Site of primary tumor (%)
Duration of primary tumor to metastases (%)
<2 yrs 2-5 yrs 2 5 yrs Unknown
Prior chemotherapy (%) Prior immunotherapy (%)
50 (24-75) 53 47
21.6 78.4 31.4 47
33 11 30
26 -
30.5 40.5 12 17
< I < I
51 (25-88) 57 43
27 73 31 42
29 20 25
26 -
33 36 18 13
< I 9
49 (20-74) 55 45
30 70 37 62.8
40 16 30 8 8.5
40 32 24 5.7
6 12
50 (23-77) 66 34
38 62 50 50
44.8 6.9
41.4
6.9 -
41.4 24.1 31.1 3.4
3.4 10.3
100,000, the white cell count was 3000 or higher with a granulocyte count of 1000 or greater, the dose of DTIC was increased to 350 mg/M2/day during the subsequent course. If the white cell count was reduced to below 1000, the granulocyte count to below 500, or the platelet count to below 50,000, DTlC dosage was reduced to 200 mg/M*/day. For patients treated with DTIC-BCG- Transfer Factor and melphalan, if no myelosuppression occurred (as defined above) during the first course of therapy, the same dosage was repeated because of the possibility of cumulative toxicity. If no myelosuppres- sion occurred after the second course, the dose of DTIC was increased to 300 mg/M2/day and the dose of rnelphalan was increased to 35 mg/M2/day during the subsequent course. With severe myelosuppression (as defined above), the dose of DTIC was reduced to
TABLE 3. Response to Chemoimmunotherapy According to Site of Metastasis
DTIC-BCG-TF DTIC DTIC-BCG -C L-PAM
No. of patients 1 1 1 89 Overall response rate (%) 14.4 26.9 Non-visceral (5%) 20.8 54.2 Nodal (%) 18 55 Subcutaneous (%) 28.6 50 Visceral (%) 12.6 16.9 Pulmonary (%) 14.3 17.9 Non-pulmonary (%) 11.5 16.2
Difference between * and + P < 0.025.
79 20.3 38.5* 31.3 50 11.3t 18.2 6.5
200 mg/M2/day and the dose of melphalan was reduced to 20 mg/M2/day during the next course.
Before chemoimmunotherapy , intradermal skin tests with five delayed hypersensitivity antigens (dermato- phytin, varidase, Candida, mumps, PPD) were applied as previously d e ~ c r i b e d . ~ ~ . ' ~ A total of 76 patients was tested. During the first course of therapy, the patients receiving transfer factor only on day 12 had repeat skin tests on days 9, 14, and 20. The patients receiving transfer factor on days 7, 12, and 17 had repeat skin tests on days 6, 9, 14, and 20. Subsequent skin tests were repeated at two- to three-month intervals.
The following criteria of response were employed: complete remission-complete disappearance of all objective and subjective disease manifestations; partial remission-50% or greater reduction in the area of all measurable tumor; stabilization-less than 50% reduc- tion or less than 25% increase in tumor size for at least two months; progression-25% or greater increase in tumor masses or appearance of any new masses; and relapse-reappearance of a tumor mass.
Survival was measured from the onset of treatment to death or date of last follow-up examination. Chemo- immunotherapy was continued for a minimum of two courses unless the patient died, and was stopped only upon evidence of progression.
The results for the 79 evaluable patients with Stage IVB disseminated malignant melanoma were compared to two historical control groups; 89 patients treated

NO. 10 CHEMOIMMUNOTHERAPY OF DISSEMINATED MALIGNANT MELANOMA . Schwurz et al. 2509
with DTTC-BCG and 111 patients treated with DTIC alone, both of which have been reported previou~ly. '~ Table 2 shows that the three groups were comparable in the major features known to be associated with prognosis.
The statistical methods used included the chi-square and Fisher's exact test for testing differences in re- sponse rate and differences in immunological response, a generalized Wilcoxon test with one-tailed analysis for testing differences between remission or survival curves," and the method of Kaplan and Meier for calculating and plotting remission and survival curves.zo
Transfer Fuctor Prepuration
Transfer factor was prepared by a modification of the standard method of Lawrence.24 All centrifugations were IOOOg x 20 minutes; incubations were at 37 C. Sterile technique was adhered to throughout the preparation.
Healthy Australian antigen (HBsAg) negative rela- tives or co-habitants of the patients were tested with the same battery of intradermal tests as used in patient testing and described above.10,42,45 Those who exhibited at least three positive recall skin test reactions ( 2 5 mm at 24 and 48 hours) were selected for leukophoresis on an TBM cell separator to obtain lymphocytes.
After gentle agitation to ensure homogeneity and a 0.5-ml aliquot removed for cell count and differential, the volume of the transfer pack from the leukophoresis procedure was measured, divided into replicate 25 x 150 mm glass tubes, and centrifuged. To hemolyze as many red cells as possible, each pellet was resus- pended in 50 ml ammonium chloride-TRIS buffer (Trisma base; reagent grade, Sigma Chemical Co., St. Louis, MO) and incubated for 15 minutes. The procedure was repeated twice, differing only in a shortened incubation period of 10 minutes. The result- ing leukocyte pellets were combined and washed in 50 ml normal saline. Preservative-free saline for injection, 1 ml per 2 x loJ lymphocytes, was added to resuspend the pellet. The suspension was frozen in an acetone/dry ice bath and thawed at 37 C ten or more times until complete cell disruption was verified microscopically. For each 2 x lo9 lymphocytes orig- inally in the sample, 0.05 mg MgS04 (as a 10% aqueous solution) and 0.5 mg DNase [(Worthington Biochemical Corp., Freehold, NJ, Cat. #DCL115) as 5 mg/ml in sterile saline for injection] were added, and the lysate then incubated for 30 minutes. For in vivo use, the digested leukocyte lysate was dialyzed for 48 hours at 4 C against 100 ml pyrogen-free distilled water and lyophiiized. The lyophilizate was reconstituted to a concentration containing the extract of lo9 lyrnpho-
1 .o
.9
.8
.7
z .6 2 I-
$ .5 0 a n !I
.3
.2
.I
DTlC vs DTIC-BCG p=.OOl DTlC vs DTIC-BCG T F p = . 0 0 3 DTlC vs DTIC-BCG T F LPAM pz.03 DTIC-BCG vs DTIC-BCG TF pr.45 DTIC-BCG vs DTIC-BCG T F LPAM p=.23 DTIC-BCG T F vs OTlC BCG TF LPAM p.29
Total Fail Ill 109 o OTlC Alone 2 89 69 * DTIC-BCG 50 38 DTIC-BCG-TF4B 29 24 A D T I C - L P A M B T F 4 8
0 0 3 6 9 12 15 20 40
MONTHS FIG. 1. Survival of total patients.
cytes per ml of preservative-free saline, filtered through a 0.45-m filter (Millipore Corp.), and aliquoted in single dose vials for storage at -70 C. For clinical use, the transfer factor was thawed at room temperature and injected subcutaneously as 0.5 cc in two separate sites, usually opposite extremities.
Results
Sixty-four evaluable Stage IVB patients were treated with the above outlined chemoimmunotherapeutic regimen and received transfer factor only on day 12. Of the 35 patients who were randomized not to receive L-PAM, there were three complete and five partial remissions for a response rate of 23%. Among the 29 patients who received L-PAM, there were one com- plete and four partial remissions for a response rate of 17%. Overall, combining these two subgroups, there were 13/64 (20.3%) responses with no statistical differ- ence between the groups. Patients with non-visceral (lymph node and subcutaneous) metastases had a response rate of 40% (8/20), which was significantly better than the response rate of 11% (5/44) for patients with visceral metastases ( P < .025). Disease was
25 10 CANCEK May 15 1980 Vol. 45
I I I I I I I I I
0 2 4 6 8 10 12 14 16 18
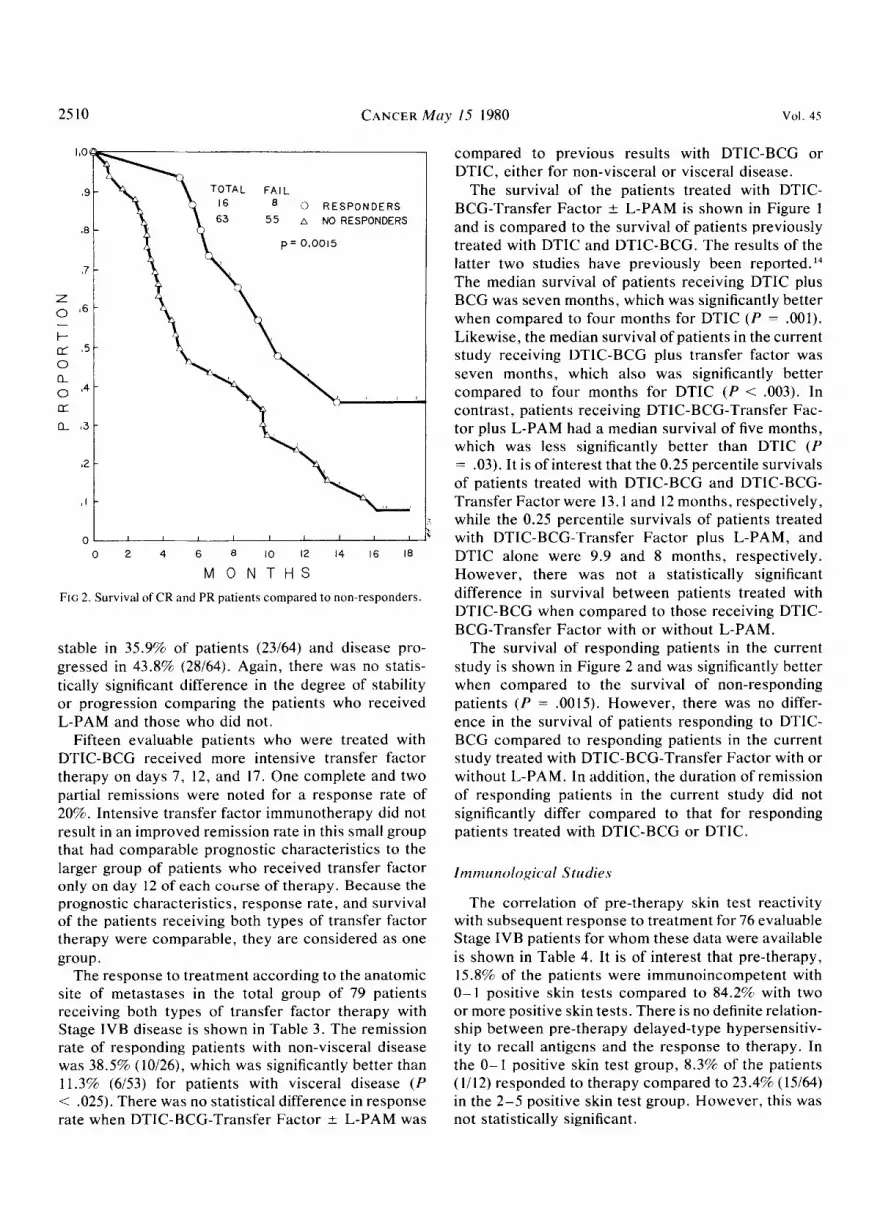
M O N T H S FIG 2. Survival of CR and PR patients compared to non-responders.
stable in 35.9% of patients (23164) and disease pro- gressed in 43.8% (28164). Again, there was no statis- tically significant difference in the degree of stability or progression comparing the patients who received L-PAM and those who did not.
Fifteen evaluable patients who were treated with DTIC-BCG received more intensive transfer factor therapy on days 7, 12, and 17. One complete and two partial remissions were noted for a response rate of 20%. Intensive transfer factor immunotherapy did not result in an improved remission rate in this small group that had comparable prognostic characteristics to the larger group of patients who received transfer factor only on day 12 of each course of therapy. Because the prognostic characteristics, response rate, and survival of the patients receiving both types of transfer factor therapy were comparable, they are considered as one group.
The response to treatment according to the anatomic site of metastases in the total group of 79 patients receiving both types of transfer factor therapy with Stage IVB diseare is shown in Table 3 . The remission rate of responding patients with non-visceral disease was 38.5%) (10126), which was significantly better than 11.3% (6153) for patients with visceral disease ( P < .025). There was no statistical difference in response rate when DTIC-BCG-Transfer Factor ;r L-PAM was
compared to previous results with DTIC-BCG or DTIC, either for non-visceral or visceral disease.
The survival of the patients treated with DTIC- BCG-Transfer Factor L L-PAM is shown in Figure 1 and is compared to the survival of patients previously treated with DTIC and DTIC-BCG. The results of the latter two studies have previously been reported.'l The median survival of patients receiving DTIC plus BCG was seven months, which was significantly better when compared to four months for DTIC ( P = .OOlj. Likewise, the median survival of patients in the current study receiving DTIC-BCG plus transfer factor was seven months, which also was significantly better compared to four months for DTIC ( P < .003j. In contrast, patients receiving DTIC-BCG-Transfer Fac- tor plus L-PAM had a median survival of five months, which was less significantly better than DTIC ( P = .03). It is of interest that the 0.25 percentile survivals of patients treated with DTIC-BCG and DTIC-BCG- Transfer Factor were 13.1 and 12 months, respectively, while the 0.25 percentile survivals of patients treated with DTIC-BCG-'Transfer Factor plus L-PAM, and DTIC alone were 9.9 and 8 months, respectively. However, there was not a statistically significant difference in survival between patients treated with DTIC-BCG when compared to those receiving DTIC- BCG-Transfer Factor with or without L-PAM.
The survival of responding patients in the current study i3 shown in Figure 2 and was significantly better when compared to the survival of non-responding patients ( P = ,0015). However, there was no differ- ence in the survival of patients responding to DTIC- BCG cornpared to responding patients in the current study treated with DTIC-BCG-Transfer Factor with or without L-PAM. In addition, the duration of remission of responding patients in the current study did not significantly differ compared to that for responding patients treated with DTIC-BCG or DTIC.
I mm unol ogica 1 S tiidies
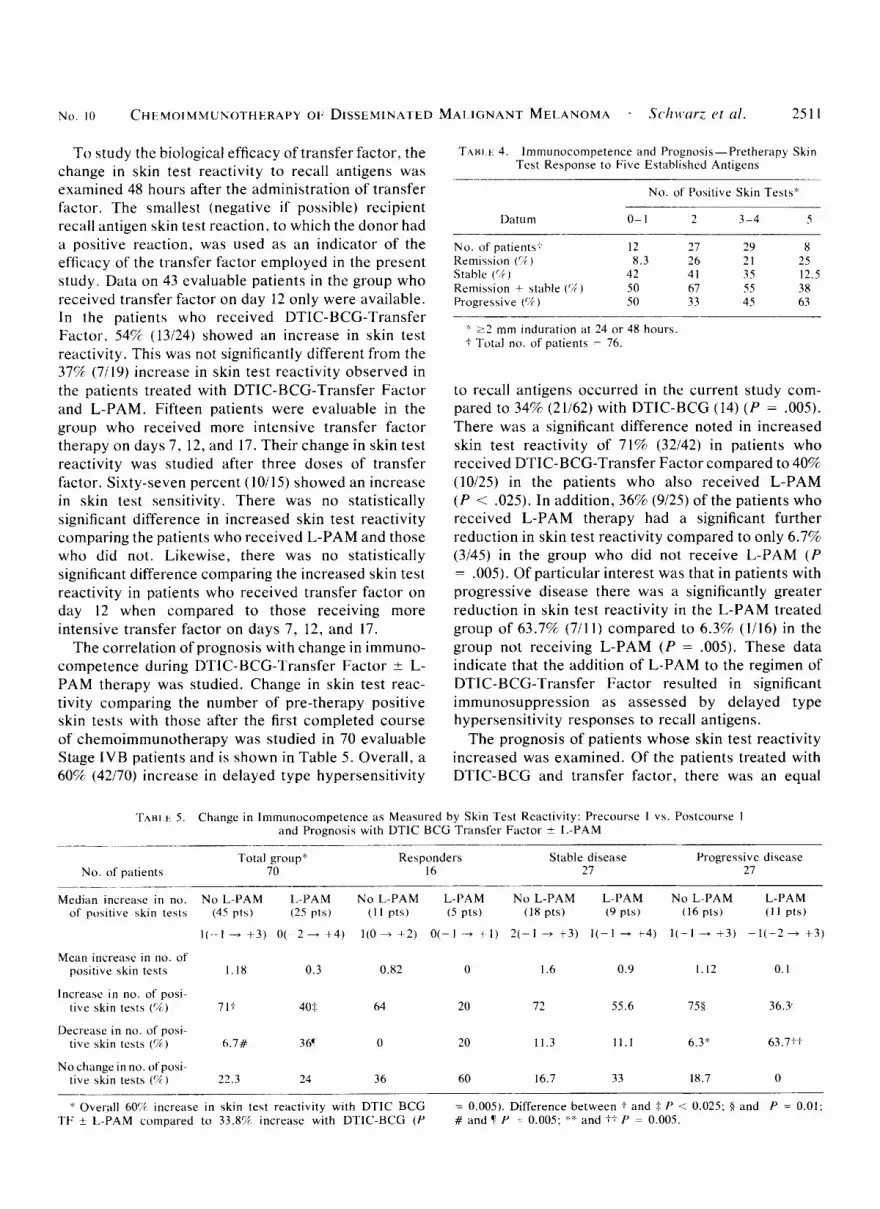
The correlation of pre-therapy skin test reactivity with subsequent response to treatment for 76 evaluable Stage IVB patients for whom these data were available is shown in Table 4. It is of interest that pre-therapy, 15.8% of the patients were immunoincompetent with 0-1 positive skin tests compared to 84.296 with two or more positive skin tests. There is no definite relation- ship between pre-therapy delayed-type hypersensitiv- ity to recall antigens and the response to therapy. In the 0-1 positive skin test group, 8.3% of the patients ( I1 12) responded to therapy compared to 23.4% (15/64) in the 2-5 positive skin test group. However, this was not statistically significant.
N o . 10 CHtMOIMMUNOTHERAPY 01. DISSEMINATED MAIUGNANT MELANOMA . S c h ~ u r ~ c t al. 2511
To study the biological efficacy of transfer factor, the change in skin test reactivity to recall antigens was examined 48 hours after the administration of transfer factor. The smallest (negative if possible) recipient recall antigen skin test reaction. to which the donor had a positive reaction. was used as an indicator of the efficacy of the transfer factor employed in the present study. Data on 43 evaluable patients in the group who received transfer factor on day 12 only were available. In the patients who received DTIC-BCG-Transfer Factor, 54% (13124) showed an increase in skin test reactivity. This was not significantly different from the 37% (7119) increase in skin test reactivity observed in the patients treated with DTIC-BCG-Transfer Factor and L-PAM. Fifteen patients were evaluable in the group who received more intensive transfer factor therapy on days 7, 12, and 17. Their change in skin test reactivity was studied after three doses of transfer factor. Sixty-seven percent (10115) showed an increase in skin test sensitivity. There was no statistically significant difference in increased skin test reactivity comparing the patients who received L-PAM and those who did not. Likewise, there was no statistically significant difference comparing the increased skin test reactivity in patients who received transfer factor on day 12 when compared to those receiving more intensive transfer factor on days 7, 12, and 17.
The correlation of prognosis with change in immuno- competence during D'TI(:-BCG-l'rdnsfer Factor ? L- PAM therapy was studied. Change in skin test reac- tivity comparing the number of pre-therapy positive skin tests with those after the first completed course of chemoimmunotherapy was studied in 70 evaluable Stage I V B patients and is shown in Table 5. Overall, a 60% (42170) increase in delayed type hypersensitivity
'I'Af3i.t 4. lmmunocompetence and Prognosis-Pretherapy Skin T a t Response to Five Established Antigens
No. of Positive Skin Teats*
Datum 0- 1 2 3-4 5
No. of patients.;. 12 27 29 8 Remission ( Y ) 8.3 26 21 25 Stable ( C i ) 42 41 35 12.5 Remission ~t stable ( % ) 50 67 5.5 38 Progressive ( V ) 50 33 45 63
' 2 2 mm induration at 24 or 48 hours. f 'rutdl no. of patient? - 76.
to recall antigens occurred in the current study com- pared to 34% (21162) with DTIC-BCG (14) ( P = .005). There was a significant difference noted in increased skin test reactivity of 71% (32142) in patients who received DTIC-BCG-Transfer Factor compared to 40% (10125) in the patients who also received L-PAM (P cz ,025). In addition, 36% (9125) of the patients who received L-PAM therapy had a significant further reduction in skin test reactivity compared to only 6.756 (3145) in the group who did not receive L-PAM (P = .005). Of particular interest was that in patients with progressive disease there was a significantly greater reduction in skin test reactivity in the L-PAM treated group of 63.7% (711 1) compared to 6.3% (1116) in the group not receiving L-PAM (P = .005). These data indicate that the addition of L-PAM to the regimen of DTlC-BCG-Transfer Factor resulted in significant immunosuppression as assessed by delayed type hypersensitivity responses to recall antigens.
The prognosis of patients whose skin test reactivity increased was examined. Of the patients treated with DTIC-BCG and transfer factor, there was an equal
T A H i I, 5. Change in Imrnunocompetence a s Measured by Skin Test Rcactivity: Precoursc 1 vs. Postcourse 1 and Prognosis with DTIC BCG Transfer Factor ? I.-PAM
~ _ _ _ _ ~~ ~ ~ _ _ _ ~ - - . ~
Total group" Responders Stable disease Progrcssive disease No. of patients 70 16 27 27
.- ___.~ ~~~~ ~~~ ~~
Median increase in no. N o L P A M L P A M No L-PAM L-PAM N o L-PAM L-I'AM No L-PAM L-PAM of positive skin tests (45 pts) (25 pts) ( I 1 pts) ( 5 pts) (18 pts) (9 pts) (16 pts) ( 1 1 pts)
I ( - - I - + 3 ) 0( 2 - + 4 ) 1(0+ + 2 ) 0(-I -+ t 1) 2(-1 + t 3 ) I ( - ] - t 4 ) ] ( - I - +3) - l ( - 2 + +3)
Mean increase in no. of positive skin tests 1.18 0.3 0.82 0 1.6 0.9 I . 12 0.1
Increase i n no. of posi- tive skin tests ((k) 71t 40$ 64 20 72 55.6 758 36.3'
Decrease in no. of posi- tive skin tests (74) h.7# 3 6' 0 20 11.3 11.1 6.3* 63.71.;
Noctiangeinno. ofposi- live skin tests (% ) 22.3 24 36 60 16.7 33 18.7 0
'k Overall 60? increase in skin test reactivity with DTIC BCG TF t L-PAM compared to 33.8% increase with D'IlC-BCG ( P
= 0.005). Difference between f and t I' .< 0.025; I and P = 0.01: # and 1' P :- 0.005: e4 and +f P = 0.00.5.
25 12 CANCER Muy 15 1980 Vol. 45
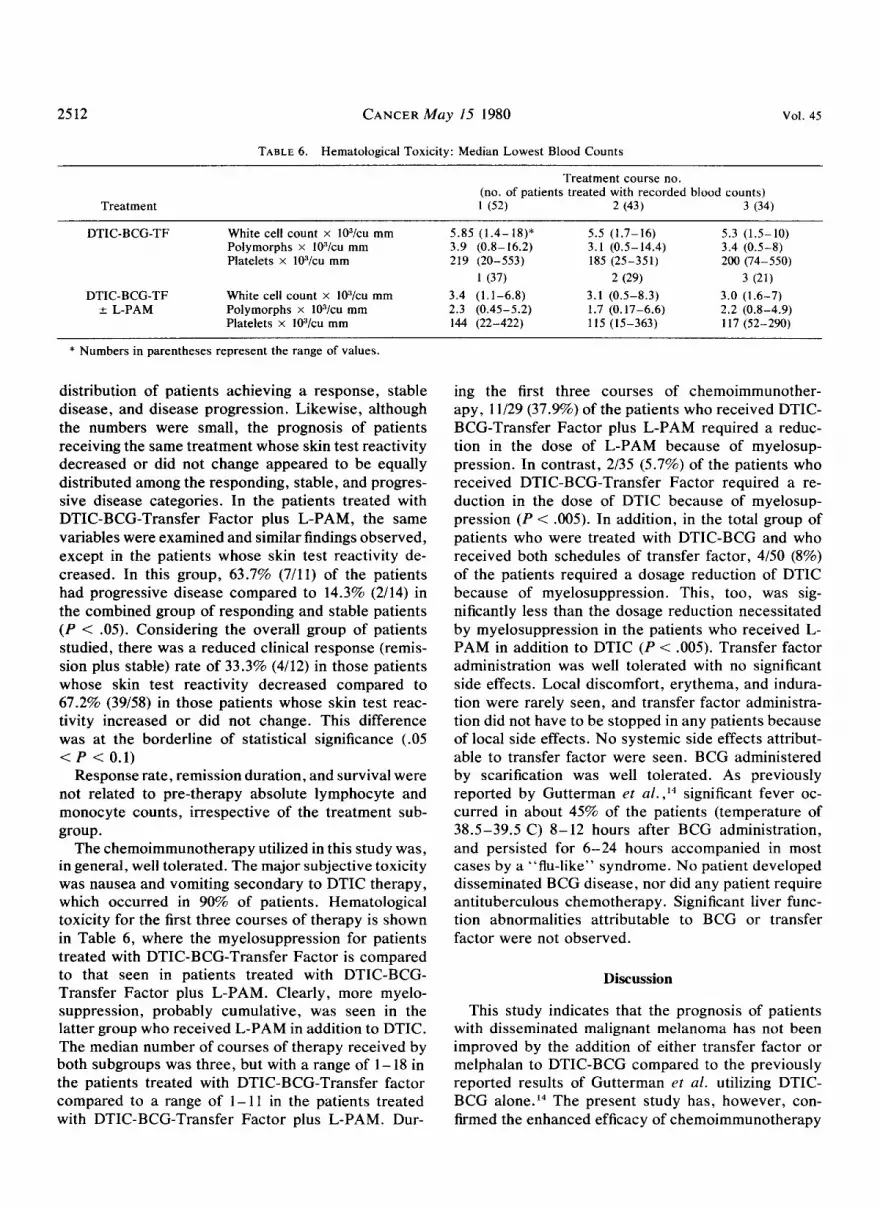
TABLE 6. Hematological Toxicity: Median Lowest Blood Counts
Treatment course no. (no. of patients treated with recorded blood counts)
Treatment 1 (52) 2 (43) 3 (34)
DTIC-BCG-TF White cell count x 103/cu mrn 5.85 (1.4-18)* 5.5 (1.7-16) 5.3 (1.5-10) Polymorphs x I03/cu mm 3.9 (0.8- 16.2) 3.1 (0.5-14.4) 3.4 (0.5-8) Platelets x I03/cu mm 219 (20-553) 185 (25-351) 200 (74-550)
1 (37) 2 (29) 3 (21) DTIC-BCG-TF White cell count x 10J/cu mm 3.4 (1.1-6.8) 3.1 (0.5-8.3) 3.0 (1.6-7)
2 L-PAM Polymorphs x 103/cu mm 2.3 (0.45-5.2) 1.7 (0.17-6.6) 2.2 (0.8-4.9) Platelets x 103/cu mm 144 (22-422) 115 (15-363) 117 (52-290)
* Numbers in parentheses represent the range of values.
distribution of patients achieving a response, stable disease, and disease progression. Likewise, although the numbers were small, the prognosis of patients receiving the same treatment whose skin test reactivity decreased or did not change appeared to be equally distributed among the responding, stable, and progres- sive disease categories. In the patients treated with DTIC-BCG-Transfer Factor plus L-PAM, the same variables were examined and similar findings observed, except in the patients whose skin test reactivity de- creased. In this group, 63.7% (7/11) of the patients had progressive disease compared to 14.3% (2/14) in the combined group of responding and stable patients (P < .05). Considering the overall group of patients studied, there was a reduced clinical response (remis- sion plus stable) rate of 33.3% (4/12) in those patients whose skin test reactivity decreased compared to 67.2% (39/58) in those patients whose skin test reac- tivity increased or did not change. This difference was at the borderline of statistical significance (.05 < P < 0.1)
Response rate, remission duration, and survival were not related to pre-therapy absolute lymphocyte and monocyte counts, irrespective of the treatment sub- group.
The chemoimmunotherapy utilized in this study was, in general, well tolerated. The major subjective toxicity was nausea and vomiting secondary to DTIC therapy, which occurred in 90% of patients. Hematological toxicity for the first three courses of therapy is shown in Table 6, where the myelosuppression for patients treated with DTIC-BCG-Transfer Factor is compared to that seen in patients treated with DTIC-BCG- Transfer Factor plus L-PAM. Clearly, more myelo- suppression, probably cumulative, was seen in the latter group who received L-PAM in addition to DTIC. The median number of courses of therapy received by both subgroups was three, but with a range of 1 - 18 in the patients treated with DTIC-BCG-Transfer factor compared to a range of 1 - 11 in the patients treated with DTIC-BCG-Transfer Factor plus L-PAM. Dur-
ing the first three courses of chemoimmunother- apy, 11/29 (37.9%) of the patients who received DTIC- BCG-Transfer Factor plus L-PAM required a reduc- tion in the dose of L-PAM because of myelosup- pression. In contrast, 2/35 (5.7%) of the patients who received DTIC-BCG-Transfer Factor required a re- duction in the dose of DTIC because of myelosup- pression (P < .005). In addition, in the total group of patients who were treated with DTIC-BCG and who received both schedules of transfer factor, 4/50 (8%) of the patients required a dosage reduction of DTIC because of myelosuppression. This, too, was sig- nificantly less than the dosage reduction necessitated by myelosuppression in the patients who received L- PAM in addition to DTIC (P < .005). Transfer factor administration was well tolerated with no significant side effects. Local discomfort, erythema, and indura- tion were rarely seen, and transfer factor administra- tion did not have to be stopped in any patients because of local side effects. No systemic side effects attribut- able to transfer factor were seen. BCG administered by scarification was well tolerated. As previously reported by Gutterman et ul. , I 4 significant fever oc- curred in about 45% of the patients (temperature of 38.5-39.5 C) 8- 12 hours after BCG administration, and persisted for 6-24 hours accompanied in most cases by a “flu-like’’ syndrome. No patient developed disseminated BCG disease, nor did any patient require antituberculous chemotherapy. Significant liver func- tion abnormalities attributable to BCG or transfer factor were not observed.
Discussion
This study indicates that the prognosis of patients with disseminated malignant melanoma has not been improved by the addition of either transfer factor or melphalan to DTIC-BCG compared to the previously reported results of Gutterman et af. utilizing DTIC- BCG a10ne.I~ The present study has, however, con- firmed the enhanced efficacy of chemoimmunotherapy

NO. 10 CHEMOIMMUNOTHERAPY OF DISSEMINATED MALIGNANT MELANOMA - Schwarz et a / . 25 13
with DTIC-BCG compared to DTIC alone in the management of disseminated malignant melanoma. l4
In particular, the overall survival of patients receiving chemoimmunotherapy was superior to historical controls who received chemotherapy alone accom- panied by a threefold greater response rate to chemo- therapy in metastatic areas regional to BCG immuni- zation, again confirming previously reported re~u1ts.I~ Although Connaught stain BCG was used in this study, the number of viable organisms used were comparable to that used with the Pasteur strain of BCG in the previous study."
Transfer factor was clearly biologically active in significantly augmenting delayed type hypersensitivity to recall antigens (60% increase) over and above that previously seen with BCG alone (34% increase). l4
Clinically, however, this was not correlated with either an increase in systemic or regional response rates or survival advantage compared to that seen previously with DTIC-BCG.l4
The only reliable method to assay for transfer factor activity at the present time remains the effectiveness of systemic transfer of dermal reactivity in man.25,41 In a literature review of transfer factor, Spitler has summarized the results of transfer factor therapy in 109 patients with various malignancie~.~' Data on the conversion of skin test reactivity were available for 22 patients and was seen in 12 patients, namely a 54.5% conversion rate which is similar to that seen in the current study. It has not been possible to assess the relationship of the clinical effectiveness of transfer factor preparations and their effect on lymphocyte transformation in vitro5 or in vivo. 37
Transfer factor in the current study was collected from appropriate donors, namely close relatives and cohabitants of patients. 1"342345 The rationale for this was that Spitler and co-workers have reported that 75% of family members of patients with malignant mela- noma exhibit reactivity to melanoma antigens in at least one of three in vitro tests of cellular imm~ni ty .~ ' In the current study, the potential of transfer factor was examined in a large enough number of patients to conclude that it is not useful to non-specifically aug- ment microbial adjuvant immunotherapy combined with the regimens of chemotherapy employed. This was despite a clearcut enhancement of delayed type hypersensitivity to recall antigens.
Utilizing exclusion chromatography and isoelectric focusing, Burger et al. have isolated a number of subfractions in human transfer factor preparations.' In addition to identifying the particular subfraction responsible for in vivo passive dermal transfer, they have also characterized subfractions with immunosup- pressive activity as assessed by the effects on lympho-
cyte transformation in vitro. Certainly immunosup- pression subsequent to transfer factor therapy has been reported," and it would seem important to screen transfer factor preparations for significant suppressive activity with a view to precluding their use ~linically.~ However, whether transfer factor with suppressive activity in vitrn would be associated with suppression in vivo is not known.s
Brandes et af.* reported incomplete regression of metastatic malignant melanoma in 1 of 2 patients treated with specific transfer factor. Smith et ~ 1 . ~ ~ re- ported clinical benefit in 5 of 10 patients with melanoma and also reported clinical benefit in pa- tients with disseminated malignant melanoma. Vetto et af.45 reported two complete and two partial responses in 11 patients with metastatic malignant melanoma. The duration of response was short in 3 patients with a range of 1-5 months, but one of the two achieving complete remission who had axillary and cerebral metastases maintained the response for 12 months. On the other hand, Grob er ~ 1 . ' ~ observed regression of melanoma in 2 of 6 patients with limited subcutaneous metastatic malignant melanoma treated with combined immunotherapy with transfer factor and BCG. Overall, "clinical benefit" in approximately 30% of patients with malignant melanoma has been reported in the l i terat~re.~' The results of the present study suggest that transfer factor is not additive to DTIC-BCG in the treatment of disseminated malignant melanoma. Clearly, differences in study design preclude strict comparison between our present results and those of other investigators, but our study represents the largest series of patients with disseminated malignant mela- noma who have received transfer factor as part of a uniform chemoimmunotherapy protocol.
Melphalan was not additive to DTIC in the treat- ment of disseminated malignant melanoma. It en- hanced myelosuppression and immunosuppression and may have abrogated the effect of immunotherapy in the group of patients who received it in addition to DTIC-BCG and transfer factor. Certainly, experi- mentally and clinically, successful chemotherapy may depend on concomitant antitumor immunity.fi*2s,33.34.46 The ability of chemotherapeutic agents to abrogate the immune response and even to abolish spontane- ous regression in some instances is also well docu- mented.''Y Alkylating agents in particular have potent immunoregulatory properties which may, to a large extent, determine the effectiveness of the chemo- therapy regimen tested. In general, alkylating agents tend to suppress B-cell function, but their effects on T-cell function are variable depending on the timing of drug administration relative to antigen challenge, the nature of the antigen, and the type of response

2514 CANCER M a y 15 1980 Vol. 45
Radov rt (if. have reported that mel- phalan was able to both favorably and adversely affect the immune factors important for drug-induced regres- sion in a highly immunogenic Murine mammary adeno- carcinoma .:34,:x When given too early, melphalan re- sulted in the abrogation of the host humoral response to the tumor and was associated with poor chemo- therapeutic results and survival. In contrast, treatment three days later was associated with depression of antibody titers only in the minority of animals not re- sponding to the drug and prolongation of the delayed hypersensitivity response in all treated animals. These studies support the observations in the current study that melphalan may be immunosuppressive and that this may exert a deleterious clinical effect. It also high- lights the concept of considering the mode of action of chemotherapeutic agents, their immunosuppressive capabilities, and the crucial factor of the timing of administration of both chemotherapeutic and immuno- therapeutic agents in the planning of chemoimmuno- therapy treatment protocols.
Finally, prognosis and immunocompetence as assessed by delayed type hypersensitivity reactions to recall antigens were not directly related, although there appeared to be a higher progression rate in post- therapy immunoincompetent patients. There was also a suggestion that pre-therapy inmunocompetence was associated with a higher response rate. Contrary to the reports of McKelvey rt d.,'$') there was no relation-, ship between pretherapy absolute lymphocyte counts and subsequent response to therapy.
A crucial question raised by this study is whether there is any direct correlation between the stimulation or augmentation of primary or secondary immune re- sponse to non-specific antigens by irnmunotherapeutic agents such as BCG or transfer factor and their anti- tumor effect. In view of the dissociation between various in \pifro and in vivo tests of immunocompe- tence,'":" there is clearly a need to develop a more meaningful and reliable continuous immunological or serological method of assessment of the effect of irn- mune modulators on the host immune system and to correlate this with their in i>ivo effect on the tumor."6
REFERENCES
I . Bach. J . F.: The mode of action of immunosuppressive agents. Iri Frontiers of Biology, Vol. 41, E. Tatum and A. Newberger, eds. Amsterdam and Oxford. North Hulland Publishing Co., 1975; pp. 173-226.
2. Brandes, I,. J., Galton, D. A. G . , and Wiltshaw, E.: New approach to immunotherapy of melanoma. L c i w c r 2:293-295, 1971.
3 . Bruckner. H. W., Mokyr. M. B . , and Mitchell. M. S . : Effect of DTIC on immunity in patients with malignant melanoma. Cunccr Res. 34:181-183, 1974.
4. Burger, D. R., Nolte, J . E . , Vandenbark, A. A,, and Vetto. R . M.: Biological activity of subfractions of human transfer factor.
It1 'Transfer Factor: Basic Properties and Clinical Applications, M. S. Ascher. C. H. Kirkpatrick. and A. A . Gottlieb. eds. New York. Academic Press. 1976; pp. 323-332.
5 . Burger. D. K.. Vandenbark, A. A , . Finke. P . . Nolte. J . E . , and Vetto. R. M. : Human transfer factor: Effects on lymphocyte transformation. J . / 1 / 1 1 7 2 / 1 t i o 1 . I17:782-788. 1976.
6. Burkitt. D. P. : Host defense mechanisms in Burkitt's lym- phoma and Kaposi's sarcoma. Br. Med. J . 4:424-426. 1970.
7. Carter. S. K., and Friedman, M . A,: 5-(3.3-dimethyl-l-triazeno) imidazole-4-caiboxamide (DTIC. DIC. NSC 45388)-a new anti- tumor agent with activity against malignant melanoma. Eur. J . C'uiir~er 8:85-92, 1972.
8. Comis. R . L.: DTIC (NSC 45388) in malignant melanoma: a perspective. ('n/ircJr Tremt. R e p . 60: 165- 176. 1976.
9. Fefer. A.: Immunotherapy and chemotherapy of nioloney sarcoma virus-induced tumors in mice. Ctitic.rr Rrs. 29:2177-2183, 1969.
10. Fudenberg. H . H., Levin. A. S . . Spitler. I,. E. , Wybran. J.. and Byers, V . : The therapeutic uses of transfer factor. Nosp. Prmc. 9:95- 104, 1974.
11. Gehan. E. A.: A generalized wilcoxon test for comparing arbitrarily singly-censored samples. BiorriefriXn 52:203-223, 1965.
12. Golub, S. H.. O'Connell. 'I'. X. , and Morton. D. I,.: Cor- relation of ir i izivo and in t*i/ro assays of immunocompetence in cancer patients. Cuticer Kes . 38: 1833- 1837. 1974.
13. Grob, P. J . , Franke. C. H., Reyrnond. J. P.. and Frie- Wettstein. M.: Therapeutic use of transfer factor. E w . J . Cli/i. I r i t < e s t 5:33 -45, 1975.
14. Gutterman. J. U., Mavligit, G . M., Gottlieb. J . A , , Burgess, M. A, , McBride. C. M., Einhorn. C . . Freireich, E . J . . and Hersh, E. M.: Chemoimmunotherapy of disseminated malignant melanoma with dimethyl triazeno imidazole carboxamide and Bacillus Calrnette- Guerin. M. Etrgf. J . Mcd. 291:592-597, 1974.
15. Gutterman, J . U.. Mavligit. G. M., Kennedy, A , , McBride, C. M.. Burgess. M. A, , and Hersh. E. M.: Immunotherapy for malignant melanoma. In Neoplasms of the Skin and Malignant Melanoma. Chicago, Yearbook Medical Publishers. 1976: pp. 497-531.
16. Gutterman. J. U.. Mavligit, G.. McBride, C., Burgess. M. A, , and Hersh, E. M.: Active immunotherapy with BCG for recurrent malignant melanoma. Laricer 1:1208-3212, 1973.
17. Gutterman. J . , Mavligit. G . , McBride. C. M.. Frei. E.. Ill , Freireich, E. J., and Hersh, E. M.: BCG stimulation of immune responsiveness in patients with malignant melanoma: Preliminary report. Cancer 32:321-327, 1973.
18. Hanna, M. G.. Jr., Peters. L. C.. Gutterman, J . U., and Hersh. E. M.: Evaluation of BCC administered by scarification for immunotherapy of metastatic hepatocarcinoma in the guinea pig. J . Ntrtl. Cancer I w t . 56:1013-1017. 1976.
19. Hersh, E. M., Gutterman, J. U., and Mavligit, G. M.: Cancer and host defense mechanisms. It1 Pathobiology Annual. H. L. Ioachim, ed. New York. Appleton-Century-Crofts, 1975; pp. 133-167.
20. Kaplan, E. I,.. and Meier. P.: Nonparamctric estimation from incomplete observations.J. Am. S / u / . Assoc. 5
21. Kirkpatrick. C. H.: Properties and activ factor. J . Allcrgy Cfiu. I tn /mtnol . 55:41 1-421. 1975.
2 2 . Kirkpatrick, C. H. , and Gallin, J . : Suppression of cellular immune responses following transfer factor: Report of a case. C ' o f l Imt tu t /1o l . 15:470-474, 1975.
23. 1,aGrange. 1'. H., Mackaness, G. B . , and Miller, T. E.: Potentiation of T cell mediated immunity by selective suppression of antibody formation with cyclophosphamide. J . E.up. Med. 139: 1529-1539, 1974.
24. Lawrence, H. S.: The transfer in humans of delayed skin sensitivity to streptococcal M substance and to tuberculin with disrupted leukocytes. J . C ' h . f / i \ , c s r . 34:219-230, 1955.
25. Lawrence. H. S.: Transfer factor. Atli.. 1 n i / ~ n o / . 11:195- 266. 1969.
26. Lawrence, H. S.: Transfer factor and cellular immune de- ficiency disease. N. EtigI. J . Mcd. 283:411-419, 1970.
No. 10 CHEMOIMMUNOTHERAPY OF DISSEMINATED MALIGNANT MELANOMA . SChbisU/'Z P t d. 25 15
27. Luce, J . K.: Chemotherapy of malignant melanoma. Cuncer 30:1604-1615, 1972.
28. Luce, J . K. , McBride, C . M., and Frei, E.. 111: Melanoma. I n Cancer Medicine, J . F. Holland and E. Frei, H I , eds. Phila- delphia, Lea and Febiger, 1973; pp. 1823-1843.
29. Mathe, G., Halle-Pannenko. 0.. and Bourut, C.: Immune manipulation by BCG administered before or after cyclophos- phamide chemoimmunotherapy of L1210 leukemia. Ertr. J . Concer 10:661-666, 1974.
30. McKelvey, E. M. . Luce, J . K . , Vaitkevicius, V. K., Talley, R. W., Bode);, G . P., Lane. M., and Moon. T. E.: Bischloroethyl nitrosourea. vincristine, dimethyl triazeno imidazole carboxamide and chlorpromazine combination chemotherapy in disseminated malignant melanoma. Cancer 39:5- 10. 1977.
31. Mihich, E.: Modification of tumor regression by immuno- logical means. C a r i c . c v RYS. 29:2345-2350, 1969.
32. Montgomery, J . A,: Experimental studies a t southern research institute with DTIC (NSC 45388). Concer Treat. Rrp. 60:125- 134, 1976.
33 . Moore. M . , and Williams, D. E.: Contribution of host im- munity to cyclophosphamide therapy of a chemically-induced murine sarcoma. I n t . J . C o w o r 1 1 :358-368, 1973.
34. Radov, L. A , , Haskill, J . S., and Korn, J. H.: Host immune potentiation of drug responses to a murine mammary adenocar- cinoma. Itit. .I. Cnnccr 17:773-779. 1976.
35. Radov. L . A , , Korn. J . H . , and Haskill, J . S.: Host immune potentiation of drug responses to a murine mammary adenocar- cinoma, 11. Effect of melphalan therapy on the host immune system. Inr. J . CrrncPr 18:630-638, 1976.
36. Schwarz, M . A., Gutterman, J. U . , Hersh, E. M.. Richman, S. P., and Mavligit, G. M. : Immunotherapy and chemoimmuno-
therapy of malignant disease with BCG and nonviable myco- bacterial fractions. World J . Slug. 1 :555-583, 1977.
37. Schwarz, M. A , , Turner-Chism, V., Hersh, E.. and Gutter- man, J . : Unpublished observations.
38. Simmler, M. C . , Rameau, G . , Chou, M. J . , and Mathe, G.: Monitoring of nonspecific cell-mediated immunity in cancer patients. Isr. J . Med. Sci , 12:472-478, 1976.
39. Smith. G. V. , Morse, P. A , , Jr. , Deraps, G . D., Raju, S., and Hardy, J . D.: Immunotherapy of patients with cancer. Srrrgc.vj 74:59-68, 1973.
40. Solowey. A . C., R a p p o r t , F. T., and Lawrence, H. S.: Cellular studies in neoplastic diseases. Irr Histocompatability Testing, E. S. Curtoni, P. L. Mattiuz, and R. M. Tosi, eds. Balti- more, Williams and Wilkins, 1967; pp. 75-78.
41. Spitler, L. E . : Transfer factor. In / . J . Uer/nrrtol . 17:445- 458. 1978.
42. Spitler, L. E . , Levin. A. S.. and Wybran. J . : Combined immunotherapy in malignant melanoma, Regression of metastatic lesions in t w o patients concordant in timing with systemic adminis- tration of transfer factor and Bacillus Calmette-Guerin. Cell. Immrrnol . 2 1 : 1 - 19, 1976.
43. Sugarbaker, E. V . , and McBride, C. M.: Survival and regional disease control after isolation-perfusion for invasivc stage 1 mela- noma of the extremities. Crincer. 37: 188- 198, 1976.
44. Thompson, R. B.: Lymphocyte transfer factor. f 5 r v . J . Clin. B i d . K P S . 16:201-204. 1971.
45. Vetto, R. M. , Burger. D. R.. Nolte, J . E., Vandenbark, A. A., and Baker, H. W.: Transfer factor therapy in patients with cancer. Catic,er 37:90- 97, 1976.
46. Ziegler, J. L.. Morrow, K. H.. Fass, L., Kyalwazi. S. K . , and Carbone, P. P.: Treatment of Burkitt's tumor with cyclophos- phamide. C(i/ic(v 26:474-484, 1970.
Related Documents






![Chemoimmunotherapy versus chemotherapy for metastatic ... · [Intervention Review] Chemoimmunotherapy versus chemotherapy for metastatic malignant melanoma Andre D Sasse 1, Emma C](https://static.cupdf.com/doc/110x72/5ca3dc4888c99374538bc446/chemoimmunotherapy-versus-chemotherapy-for-metastatic-intervention-review.jpg)




