-
8/12/2019 Carbohydrate 5
1/16
-
8/12/2019 Carbohydrate 5
2/16
The pancreas the gland responsible.
Insulin production and secretion.
Insulin receptors.
Glucose transporters.
Insulin action.
Abnormal carbohydrate metabolism.
-
8/12/2019 Carbohydrate 5
3/16
-
8/12/2019 Carbohydrate 5
4/16
Insulin receptor
The first step in insulin action is the activation of tyrosine kinase of the sub-unit.
Initiate a series of events involving a cascade of phosphorylation-dephosphorylation.
Stimulation of intracellular glucose metabolism.
Initial step is the activation of the glucose transport system.
-
8/12/2019 Carbohydrate 5
5/16
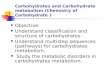
Glucose uptake
GLUT-4 transporter
on cell membraneInsulin
insulin stimulated translocation ofglucose transporters
-
8/12/2019 Carbohydrate 5
6/16
Organ Glucose transporter HK coupler Classification
Brain GLUT1 HK-I Glucose dependent
Erythrocyte GLUT1 HK-I Glucose dependent
Adipocyte GLUT4 HK-II Insulin dependentMuscle GLUT4 HK-II Insulin dependent
Liver GLUT2 HK-IVL Glucose sensor
GK - cell GLUT2 HK-IVB ( glucokinase )Glucose sensor
Gut GLUT3-symporter ---- Sodium dependent
Kidney GLUT3-symporter ---- Sodium dependent
Glucose transporters
-
8/12/2019 Carbohydrate 5
7/16
B cell
High blood
glucose
Insulin
Impaired insulin releaseGlucose
uptake
FFA
FFA
Glucose Metabolism
-
8/12/2019 Carbohydrate 5
8/16
Skeletal
muscle
Brain
Splanchnic
bed
Adipose
tis
sue
Control NIDDM
Gluc
oseuptake(mg/
kg/min)
Insulin resistance is the major
contributor for the pathogenesis
of type 2 diabetes.
Resistance could be at the level
of insulin receptors or post
receptor defect.
Skeletal muscle is the major
contributor to insulin resistance
in patients with type 2 diabetes.
Hepatic glucose production
-
8/12/2019 Carbohydrate 5
9/16
Indogenous glucose
production should
balance with total body
glucose uptake.
Major production come
from glycogenolysis.
Major uptake is through
glucose oxidation.
0
0.5
1
1.5
2
2.5
Endogenous Glucose production Total Body Glucose Uptake
Glycogenolysis
Glycerol (2%)
Pyruvate (1%)
Lactate (16%)
Amino Acids (6%)
Other
Glycolysis
Glucose
Oxidation
Splanchnic
Glucose
Uptake
Hepatic glucose production
-
8/12/2019 Carbohydrate 5
10/16
Glucose
Fatty acid
Citrate
Acetyl CoA
Fatty acid
Glucose
Glucose 6-
Phosphate
Phospho-fructokinase
Frucose 6-
Phosphate
Frucose 1,6-
bisphosphate
Pyruvate
Acetyl CoA
Randle cycle
Glucose metabolism during fast state
Non-diabetic subject:
During an over night
fast liver will supplyenergy from glycogenstore.
Muscle will utilizeenergy from free fatty
acids (FFA) by Randlecycle.
This will decreaseglucose transportthrough cellularmembrane.
-
8/12/2019 Carbohydrate 5
11/16
Fasted state
Fructose 6-Phosphate
Fructose 2,6-bisphosphate
Fructose 1,6-bishosphate
Phosphoenolpyruvate
Oxaloacetate
pyruvate
Fed state
Fructose 6-Phosphate
Fructose 2,6-bisphosphate
Fructose 1,6-bishosphate
Phosphoenolpyruvate
Oxaloacetate
pyruvate
Glucose metabolism during fast and fed state
-
8/12/2019 Carbohydrate 5
12/16
Insulin deficiency
Blood glucose
Insulin resistance
Diabetes Mellitus is a group of metabolic disease characterized
by hyperglycemia resulting from defects in insulin secretion,
insulin action, or both.
The chronic hyperglycemia of diabetes is associated with
log-term damage, dysfunction, and failure of various organs,especially the eyes, Kidneys, nerves, heart, and blood vessels.
Pathogenesis of type 2 Diabetes Mellitus
-
8/12/2019 Carbohydrate 5
13/16
Natural History of Type 2 Diabetes Mellitus
Age 0-5+ 15-40+ 15-60+ 25-70+
Microvascular Complication
IGT Postprandial Fasting
Hyperglycemia Hyperglycemia
Macrovascular Complication
Disability
Insulin resistance
Hyperinsulinemia
HDL cholesterol
Triglyceride
Hypertension
Atherosclerosis
Normo-insulinemia
Retinopathy
Nephropathy
Neuropathy
Hypoinsulinemia
Blindness
Renal Failure
Amputation
IHDStroke
Genetic background for:
Insulin secretion
Insulin sensitivity
complications
Environmental factors:
Nutrition
Obesity
Physical inactivity
Disability
Death
-
8/12/2019 Carbohydrate 5
14/16
Natural History of Type 2 Diabetes Mellitus
Decrease Glucose-induced insulin
secretion
Insulin deficiency
Insulin resistance
Decrease Tissue response to insulin
Genetic
Acquired
GlucotoxicityLipotoxicity
Genetic
Acquired
Obesity
Vo2max
AgeSmoking
Increase Hepaticglucose production
Increase Cellular
glucose uptake
Hyperglycemia
Impaired beta
cell function
Post- receptor
defectDecrease Glucose transport
Decrease Insulin binding
BasalHyperinsulinemia
-
8/12/2019 Carbohydrate 5
15/16
-
8/12/2019 Carbohydrate 5
16/16