498 | SEPTEMBER 2012 | VOLUME 9 www.nature.com/nrclinonc IRCCS MultiMedica, Science and Technology Pole, Via Fantoli 16/15, Milan 20138, Italy (A. Albini). Department of Translational Oncology Research, IRCCS Azienda Ospedaliera Universitaria San Martino—IST—Istituto Nazionale per la Ricerca sul Cancro, Genova 16132, Italy (F. Tosetti). Institute for Advanced Studies, The Angiogenesis Foundation, One Broadway 14 th Floor, Cambridge, MA 02142, USA (V. W. Li, W. W. Li). Department of Biotechnologies and Life Sicences, University of Insubria, Viale Ottorino Rossi 9, Varese 21100, Italy (D. M. Noonan). Correspondence to: A. Albini adriana.albini@ multimedica.it Cancer prevention by targeting angiogenesis Adriana Albini, Francesca Tosetti, Vincent W. Li, Douglas M. Noonan and William W. Li Abstract | Healthy individuals can harbour microscopic tumours and dysplastic foci in different organs in an undetectable and asymptomatic state for many years. These lesions do not progress in the absence of angiogenesis or inflammation. Targeting both processes before clinical manifestation can prevent tumour growth and progression. Angioprevention is a chemoprevention approach that interrupts the formation of new blood vessels when tumour cell foci are in an indolent state. Many efficacious chemopreventive drugs function by preventing angiogenesis in the tumour microenvironment. Blocking the vascularization of incipient tumours should maintain a dormancy state such that neoplasia or cancer exist without disease. The current limitations of antiangiogenic cancer therapy may well be related to the use of antiangiogenic agents too late in the disease course. In this Review, we suggest mechanisms and strategies for using antiangiogenesis agents in a safe, preventive clinical angioprevention setting, proposing different levels of clinical angioprevention according to risk, and indicate potential drugs to be employed at these levels. Finally, angioprevention may go well beyond cancer in the prevention of a range of chronic disorders where angiogenesis is crucial, including different forms of inflammatory or autoimmune diseases, ocular disorders, and neurodegeneration. Albini, A. et al. Nat. Rev. Clin. Oncol. 9, 498–509 (2012); published online 31 July 2012; doi:10.1038/nrclinonc.2012.120 Introduction Cancer has been identified by the United Nations as a non-communicable disease posing a global health threat with considerable economic consequences. 1,2 The cost of cancer care in the USA alone is projected to rise from US$125 billion in 2010 to US$207 billion by 2020. 2 Although great strides have been made in reducing mortality from cardiovascular disease and other non- communicable diseases through preventive efforts, cancer is still usually treated at advanced, often metastatic, disease stages. 3 Screening methods have improved prognosis for some cancers; 4 however, early detection is not yet pos- sible for most malignancies, and the value of screening has been challenged for some tumours. 5 Targeted therapies are emerging as useful therapies, but treating all patients with these costly agents is not economically sustainable. 6,7 As the world population exceeds 7 billion, cancer prevention clearly becomes an urgent goal to pursue. Many cancers can be prevented by lifestyle changes, such as avoiding tobacco use, excessive UV exposure, infectious agents, poor dietary habits and obesity. 8 Behavioural studies suggest that promotion of healthy dietary habits and exercise is only moderately success- ful. 9 Thus, cancer prevention remains a difficult task. Preclinical evidence suggests that cancer prevention is feasible, but for the population at large the question is how. It is estimated that half of men and a third of women will be diagnosed with a cancer in their lifetime. 10 The cancer diagnosis usually comes many years after the transform- ing events that spawned the cancer. Chemoprevention, the pharmacological prevention of cancer, was proposed over three decades ago, 11 but little has been invested to advance this life-saving approach, which should be inexpensive, non-toxic, and suitable for chronic administration. In this Review, we suggest a new consideration: limiting chemo- prevention to tumour cells may be too specific. To be effective, cancer prevention should ideally impact on the organ microenvironment, boosting physiological defences against tumour development. 12 Angiogenesis and angioprevention Angiogenesis and inflammation are two host-dependent and interdependent hallmarks of cancer 13 that have an early permissive role in tumorigenesis (Figure 1). Angio- prevention is the term that we used 10 years ago when we proposed that angiogenesis inhibition was a common target of most cancer chemopreventive drugs. 14 Although epithelial cells that harbour mutations retain distinct, organ-specific phenotypes, endothelial cells are gener- ally untransformed and a common target across many cancers. Increasing evidence supports the angioprevention approach in preclinical models as well as in epidemiological and clinical intervention studies in humans. Judah Folkman first suggested that tumour dormancy could be maintained by preventing neovascularization of microscopic cancers. 15 However, the clinical vali- dation of antiangiogenic therapy was done in the context of metastatic disease. Although antiangiogenic therapy has improved the standard of care for some cancers, its overall clinical benefit is modest for most patients, mainly observed in the form of prolonged progression- free survival. 16,17 In the setting of heavy disease burden, most patients treated with antiangiogenic agents eventu- ally experience disease progression due to evolution of Competing interests The authors declare no competing interests. REVIEWS © 2012 Macmillan Publishers Limited. All rights reserved

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
498 | SEPTEMBER 2012 | VOLUME 9 www.nature.com/nrclinonc
IRCCS MultiMedica, Science and Technology Pole, Via Fantoli 16/15, Milan 20138, Italy (A. Albini). Department of Translational Oncology Research, IRCCS Azienda Ospedaliera Universitaria San Martino—IST—Istituto Nazionale per la Ricerca sul Cancro, Genova 16132, Italy (F. Tosetti). Institute for Advanced Studies, The Angiogenesis Foundation, One Broadway 14th Floor, Cambridge, MA 02142, USA (V. W. Li, W. W. Li). Department of Biotechnologies and Life Sicences, University of Insubria, Viale Ottorino Rossi 9, Varese 21100, Italy (D. M. Noonan).
Correspondence to: A. Albini [email protected]
Cancer prevention by targeting angiogenesisAdriana Albini, Francesca Tosetti, Vincent W. Li, Douglas M. Noonan and William W. Li
Abstract | Healthy individuals can harbour microscopic tumours and dysplastic foci in different organs in an undetectable and asymptomatic state for many years. These lesions do not progress in the absence of angiogenesis or inflammation. Targeting both processes before clinical manifestation can prevent tumour growth and progression. Angioprevention is a chemoprevention approach that interrupts the formation of new blood vessels when tumour cell foci are in an indolent state. Many efficacious chemopreventive drugs function by preventing angiogenesis in the tumour microenvironment. Blocking the vascularization of incipient tumours should maintain a dormancy state such that neoplasia or cancer exist without disease. The current limitations of antiangiogenic cancer therapy may well be related to the use of antiangiogenic agents too late in the disease course. In this Review, we suggest mechanisms and strategies for using antiangiogenesis agents in a safe, preventive clinical angioprevention setting, proposing different levels of clinical angioprevention according to risk, and indicate potential drugs to be employed at these levels. Finally, angioprevention may go well beyond cancer in the prevention of a range of chronic disorders where angiogenesis is crucial, including different forms of inflammatory or autoimmune diseases, ocular disorders, and neurodegeneration.
Albini, A. et al. Nat. Rev. Clin. Oncol. 9, 498–509 (2012); published online 31 July 2012; doi:10.1038/nrclinonc.2012.120
IntroductionCancer has been identified by the United Nations as a non-communicable disease posing a global health threat with considerable economic consequences.1,2 The cost of cancer care in the USA alone is projected to rise from US$125 billion in 2010 to US$207 billion by 2020.2 Although great strides have been made in reducing mortality from cardiovascular disease and other non- communicable diseases through preventive efforts, cancer is still usually treated at advanced, often metastatic, disease stages.3 Screening methods have improved prognosis for some cancers;4 however, early detection is not yet pos-sible for most malignancies, and the value of screening has been challenged for some tumours.5 Targeted therapies are emerging as useful therapies, but treating all patients with these costly agents is not economically sustainable.6,7 As the world population exceeds 7 billion, cancer prevention clearly becomes an urgent goal to pursue.
Many cancers can be prevented by lifestyle changes, such as avoiding tobacco use, excessive UV exposure, infectious agents, poor dietary habits and obesity.8 Behavioural studies suggest that promotion of healthy dietary habits and exercise is only moderately success-ful.9 Thus, cancer prevention remains a difficult task. Preclinical evidence suggests that cancer prevention is feasible, but for the population at large the question is how.
It is estimated that half of men and a third of women will be diagnosed with a cancer in their lifetime.10 The cancer diagnosis usually comes many years after the transform-ing events that spawned the cancer. Chemoprevention, the pharmacological prevention of cancer, was proposed over
three decades ago,11 but little has been invested to advance this life-saving approach, which should be inexpensive, non-toxic, and suitable for chronic administration. In this Review, we suggest a new consideration: limiting chemo-prevention to tumour cells may be too specific. To be effective, cancer prevention should ideally impact on the organ microenvironment, boosting physiological defences against tumour development.12
Angiogenesis and angiopreventionAngiogenesis and inflammation are two host-dependent and interdependent hallmarks of cancer13 that have an early permissive role in tumorigenesis (Figure 1). Angio-prevention is the term that we used 10 years ago when we proposed that angiogenesis inhibition was a common target of most cancer chemopreventive drugs.14 Although epithelial cells that harbour mutations retain distinct, organ-specific phenotypes, endothelial cells are gener-ally untransformed and a common target across many cancers. Increasing evidence supports the angio prevention approach in preclinical models as well as in epidemiological and clinical intervention studies in humans.
Judah Folkman first suggested that tumour dormancy could be maintained by preventing neovascularization of microscopic cancers.15 However, the clinical vali-dation of antiangiogenic therapy was done in the context of metastatic disease. Although antiangiogenic therapy has improved the standard of care for some cancers, its overall clinical benefit is modest for most patients, mainly observed in the form of prolonged progression-free survival.16,17 In the setting of heavy disease burden, most patients treated with antiangiogenic agents eventu-ally experience disease progression due to evolution of
Competing interestsThe authors declare no competing interests.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | SEPTEMBER 2012 | 499
biological escape mechanisms by tumours.18 All these data raise the question: ‘are angiogenesis inhibitors being used in an optimal scenario?’
Angioprevention applies angiogenesis inhibition to predisposing conditions,14 such as chronic inflammation, hyperplastic or preneoplastic lesions, and occult tumours. Angiopreventive drugs are chemopreventive compounds that counteract angiogenesis and/or the underlying inflammation. The goal is to influence the tumour micro-environment so that host defence systems are fortified to more durably suppress the development of clinically detectable tumours. Microscopic foci of transformed cells are very common in healthy individuals. Autopsy studies have shown that approximately 40% of women between 40 and 49 years old have occult breast cancers.19 Similarly, in situ prostate cancer has been detected post-mortem in 24% of men aged 60–70 years.20 Microscopic thyroid cancers are estimated to be present in 98% of indivi duals by the age of 70.21,22 Yet, these cancers are diagnosed in only 2%, 8%, and <0.5%, respectively, in these age groups. The body’s intrinsic ability to prevent tumour angiogenesis is one mechanism by which cancers are maintained in a prolonged dormant state.23 Although it is not known which individuals with occult cancers will go on to develop clinical disease, angioprevention has the potential to avert this fate.
In the context of cancer, immune cells act as Janus-like components: on one side they can destroy cancer cells; on the other side they can promote tumour angiogenesis, growth and dissemination.24–26 The presence of immune cells within tumours has been suggested to contribute to the carcinogenic and metastatic processes,13,27 and to tumour angiogenesis;24–26 their polarization seems to deter-mine clinical outcome. A typical example is macro phages: classically-activated M1 macro phages produce antiangio-genic Th1 cytokines (such as interleukin [IL]-12); by con-trast, tumour-associated macrophages, M2 macrophages, Tie2-expressing macro phages and myeloid-derived sup-pressor cells produce Th2 cytokines, allow tissue recon-struction, growth promotion and angio genesis.28,29 Similar groupings have been proposed for poly morphonuclear neutrophils (PMNs) as either antitumour ‘PMN1’ (or N1) or pro tumour ‘PMN2’ (or N2) subsets that have a direct role in tumour angiogenesis.26,30 Protumour and proangiogenic polarization have been demonstrated for most tumour microenvironment immune cells including dendritic, mast, T and B cells.25,26,28,29,31 Blocking chronic inflam mation can prevent protumour polarization and contribute to angioprevention.
Mechanisms of angiopreventionVascular cell migration and invasionInhibition of proteases involved in the degradation of the vascular basement membrane and extracellular matrix suppresses angiogenesis and metastasis.32 Abnormal matrix remodelling by unchecked protease activity opens the way to sprouting vessels, by breaking the extra-cellular matrix and favouring detachment, attachment and spatial organization of endothelial cells. Targeting this remodelling is one mechanism of action attributed
Key points
■ Angiogenesis and inflammation are host-dependent hallmarks of cancer that can be targeted using prevention approaches long before tumours initiate and progress
■ Several prescription and non-prescription drugs are already available for use in angioprevention, as well as a growing array of nutraceuticals
■ We propose four levels of angioprevention: I for the ‘healthy’ population; II for patients with increased risk of cancer; III for preneoplastic lesions; and IV for prevention of cancer recurrence
■ There are several successes in cancer prevention that demonstrate clinical feasibility and levels of intervention, from no to little to intense physician involvement
■ To avoid toxicity while maintaining efficacy, angioprevention needs to achieve a degree of angiogenesis control that is not excessively suppressive, such that healthy vascular function is maintained
to the antiangiogenic activity of green tea33 through inhi-bition of the matrix metallo proteinases (MMP)-2 and MMP-9. Inhibition of matrix remodelling can occur by direct binding as well as indirect mechanisms including downregulation of proteases and protease stimulators and upregulation of protease inhibitors.34,35 MMP inhibition has a role in the mechanism of action of numerous angio-preventive agents.36,37 Flavonoids such as fisetin, apigenin, and luteolin specifically and dose-dependently antago-nize MMP-9 gene and protein expression in endothelial cells.38 Organosulfur compounds such as sulforaphane and phenethyl isothiocyanate are naturally present in dietary cruciferous vege tables, including broccoli and Brussels sprouts. One key target of phenethyl isothio-cyanate is protein kinase C, which leads to downstream inhibition of MMP-2 and MMP-9.39 Eugenol (4-allyl-2- methoxyphenol), a component of basil, also inhibits angio-genesis through modu lation of MMP-2 and MMP-9; in addition, eugenol acts through modulation of VEGF, its receptor VEGFR-1, tissue inhibitor of metalloproteinases (CSC-21K, also known as TIMP-2) and RECK.40 Other angiopreventive compounds, including hyperforin, cur-cumin, resveratrol, and sili binin, affect metalloproteases and other matrix proteolytic enzymes, thereby impacting on the migration and invasion of endothelial cells.35,41,42
Endogenous angiogenesis inhibitors and hormonesMany endogenous angiogenesis inhibitors reside within the host microenvironment, including thrombospondin-1, platelet factor 4, angiostatin and other plasminogen fragments, endostatin, tumstatin, alphastatin, arresten, canstatin, pigment epithelium-derived factor (PEDF), TIMP-2, ADAM-TS 9 and tetrahydrocortisol as well as some chemokines.43 Induction of these inhibitors by drugs or diet can ‘boost’ innate vascular suppression and curb microscopic tumour growth (Figure 2).43
Interferons (IFN) have long been known to inhibit angio-genesis.44 Imiquimod is a topical immunomodulatory drug that is approved by the FDA for the treatment of actinic keratosis to prevent its progression to skin cancer.45 This agent acts through activation of Toll-like receptor 7 (TLR7) and production of IFN-α, IFN-β, IFN-γ, IL-12 and IL-18;46 repression of MMP activity, and inhibition of tumour angiogenesis.47
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
500 | SEPTEMBER 2012 | VOLUME 9 www.nature.com/nrclinonc
As a preventative agent in women who have had oestro-gen receptor-positive breast cancer, treatment with tamox-ifen reduces the incidence of secondary breast cancer by more than 40%.48 Tamoxifen has antitumour activity independent of its anti-oestrogen action that is associ-ated with endostatin production.49 A clinical study of early stage breast cancer showed that tamoxifen (20 mg/day) significantly increased endostatin levels in breast tissue and abdominal subcutaneous fat by 33%, while simultaneously lowering VEGF and angiogenin levels.50
Endothelial cells are sensitive to the hormonal milieu, such as during the menstrual cycle, and hormonal mimetics and antagonists show antiangiogenic activi-ties.51 A diet high in phytoestrogens, such as genistein and enterolactone, slows breast cancer progression in a fashion similar to tamoxifen,52 with inhibition of pro-inflammatory cytokines IL-1α and IL-1β that promote angiogenesis. Indeed, the phytoestrogens enterolactone, quercetin and curcumin alter oestrogen-dependent transcription of genes in breast cancer cells.53
Inflammation and inflammatory angiogenesisChronic inflammation, which promotes angiogenesis and is linked to the development of 30% of all cancers,25 is a primary target for angioprevention.24,26 Chronic use of anti-inflammatory agents prevents a wide range of human
tumours.54–56 The angiopreventive agent resveratrol reduced neutrophil infiltration in mesenteric lymph nodes and lamina propria in a colon cancer model.57 The signal transducer and activator of transcription (STAT) family member STAT3 is a central signalling hub for immune cells,58 and is often activated in cancer cells, leading to expression of VEGF, IL-10 and IL-6, which in turn upregulates STAT3 signalling in endothelial and immune cell subsets in the tumour microenvironment.58 Several angiopreventive phytochemicals—such as apigenin, luteolin, and myricetin—target the STAT3 pathway,59,60 as well as other key mediators of inflammation, including the NF-κB, PI3K, TNF-α, and HIF-1α pathways.41,61
Cyclooxygenase-2 (COX-2) is another proinflammatory molecule that is overexpressed in many cancers, inclu ding breast, colorectal, lung, and prostate and pre neoplastic lesions, such as ductal carcinoma in situ, cervical intra-epithelial neoplasia, prostatic intraepithelial neoplasia, Barrett’s oesophagus, and actinic keratosis, but is not highly expressed in healthy tissues.62 COX-2 promotes carcinogenesis as well as angiogenesis through both prostaglandin-related and non-prostaglandin-related mechanisms.63 The angiogenic mechanisms include induction of MMP-2 and MMP-9, production of VEGF, bFGF, and PDGF, and enhancement of αvβ3-mediated angiogenesis.62 COX-2 inhibition interferes with these
Clinicallydetectablecancer
Undetectablecancer
Transformationevent
Dormanttumour
Hyperplasticfoci
Years
Weeks
In�ammation
Vascularizedmetastaticcancer
Anti-in�ammation
Angioprevention
Dormancymaintained
Angiogenicswitch
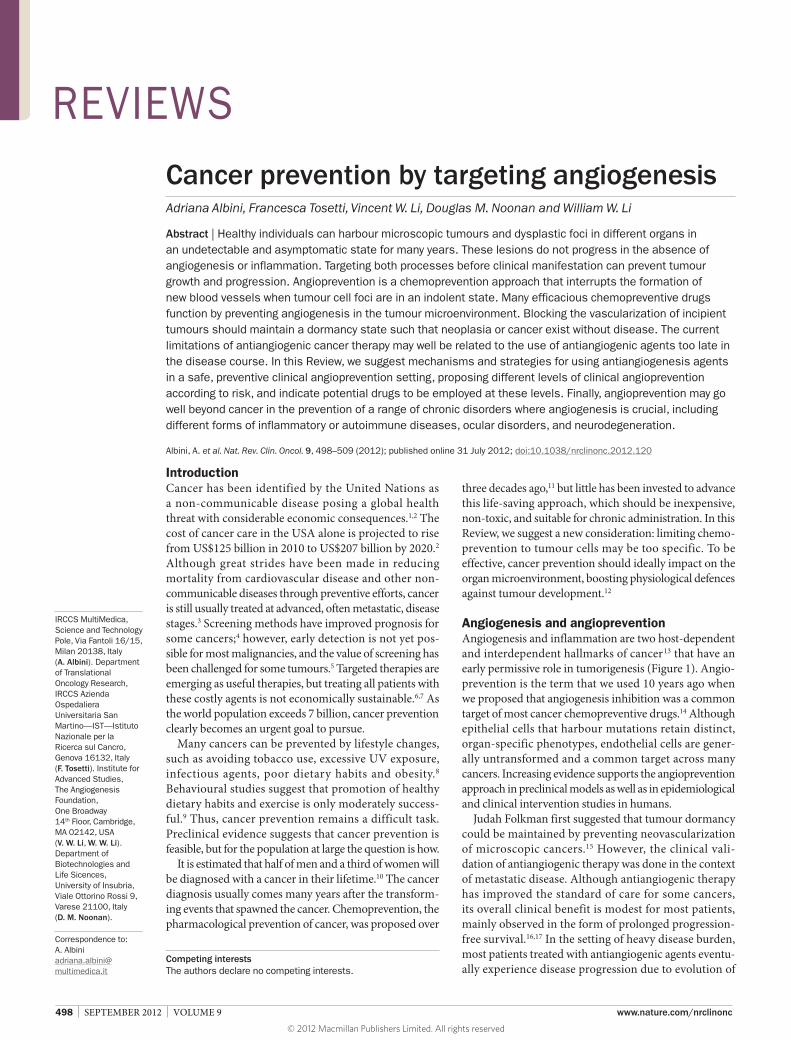
Figure 1 | Timing of angioprevention. After a transformation event, most tumours remain clinically indolent for years if not decades. Only after the angiogenic switch, driven by increasing inflammation, and many subsequent cycles of replication will a tumour become clinically detectable. At this point, it will have extensively progressed, is likely to have disseminated tumour cells and may already be metastatic. Angioprevention, which includes anti-inflammatory antiangiogenic mechanisms, needs to be started when a tumour is a dormant or hyperplastic foci or even before this stage, and sustained to maintain the tumour in this state. The observation that angioprevention efficacy increases as a function of time of application with angioprevention drugs, such as aspirin, is not surprising when seen in this context. These concepts must also be kept in mind when developing clinical trials.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | SEPTEMBER 2012 | 501
events,63 thus aspirin and COX-2 inhibitors are bona fide angiopreventive agents. VEGF, MMPs and NF-κB are also targets of the β-adrenergic receptor blocker propranolol that has been shown to be anti angiogenic, and is clinically active in infantile hemangiomas.64
Apoptosis, autophagy, senescence and stem cellsThe induction of autophagy or forcing activated endo-thelial cells into a quiescent state is also an angio preventive mechanism.65 Among chemopreventive compounds, the phytochemicals sulforaphane66 and resveratrol67 can activate pathways leading to autophagy. Microarray data suggest that some angioprevention agents, such as N-acetyl-cysteine and 9-cis-retinoic acid, induce a molecular profile in endothelial cells similar to that of in vitro senescence.65,68
Beyond microscopic tumours, cancer stem cells (also known as cancer initiating cells) reside in, and are depen-dent on, the tumour microvasculature. Angiogenesis inhibitors have been shown to decrease putative cancer stem cell numbers,69 suggesting that angiopreventive treatments could not only halt tumour growth but might also restrict cancer stem cell expansion.69
Metabolism and caloric restrictionReduction of caloric intake and energy restriction reduces cancer risk.70 Pharmacological metabolism regulators are under investigation for cancer prevention. Agents such as 2-deoxyglucose (2-DG), antidiabetic agents target-ing glucose metabolism (metformin, rosiglitazone and pioglitazone), and histone deacetylase inhibitors, all exhibit antiangiogenic activity.71–73
The mTOR pathway controls protein metabolism in concert with AMPK and Akt; therefore, over-activation of mTOR can induce VEGF-mediated angiogenesis (Figure 3).74 The mTOR inhibitors, rapamycin, sirolimus, temsirolimus and everolimus (rapalogs) are in clinical use based on dual antiangiogenic and antitumour proper-ties.75 Rapalogs are undergoing clinical assessment for the secondary chemoprevention of skin cancer and secon-dary cancers in patients who are immunosuppressed following transplantation.76,77 Metformin, an AMPK stimulator, inhibits mTOR and demonstrates antiangio-genic activity in vitro and in vivo.78–80 Among its unique mechanisms is the upregulation of PEDF, an endogenous angiogenesis inhibitor.81
Redox stress is another key component of oncogenic-induced chronic inflammation.13,25–27 Oxygen radicals can activate endothelial cells and influence cytokine release and vascular permeability.82 Antioxidants are widely pro-posed for cancer prevention,83 and in endothelial cells an antioxidant response may restore redox homeostasis.84 Many angiopreventive agents exert pleiotropic effects by inhibiting angiogenesis and inflammation mediated by redox-sensitive targets, such as NF-κB, Akt, mTOR (Figure 3).85,86 Because energy restriction and metabolic regulation have anti-inflammatory and angiosuppressive consequences,84,87,88 another benefit of angioprevention could be weight control (Box 1).
Angioprevention in the clinicClinically, angioprevention maintains transformed cells in a dormant state and keeps the microenvironment healthy so that transformation is hampered despite
Angioprevention
Monocyte
Microscopic tumour (avascular)Not clinically detectable
Macrophage
Neutrophil
Stimulators Inhibitors
Reducestimulation
Boostinhibition
Endothelium
Normalepithelial cell
Platelet
Fibroblast
Stroma
T cell
VEGFPIGFFGF
PDGFEGF
MMP-2, MMP-9COX-2mTORROS
CaloriesGlucose, fat
pH, oxygen levelsOthers
TSP-1PF-4
AngiostatinEndostatinTumstatin
Interferon α, β, γTIMPsAMPK
Tight junctionsIntegrins (ligated)
Others
0.5 mm3
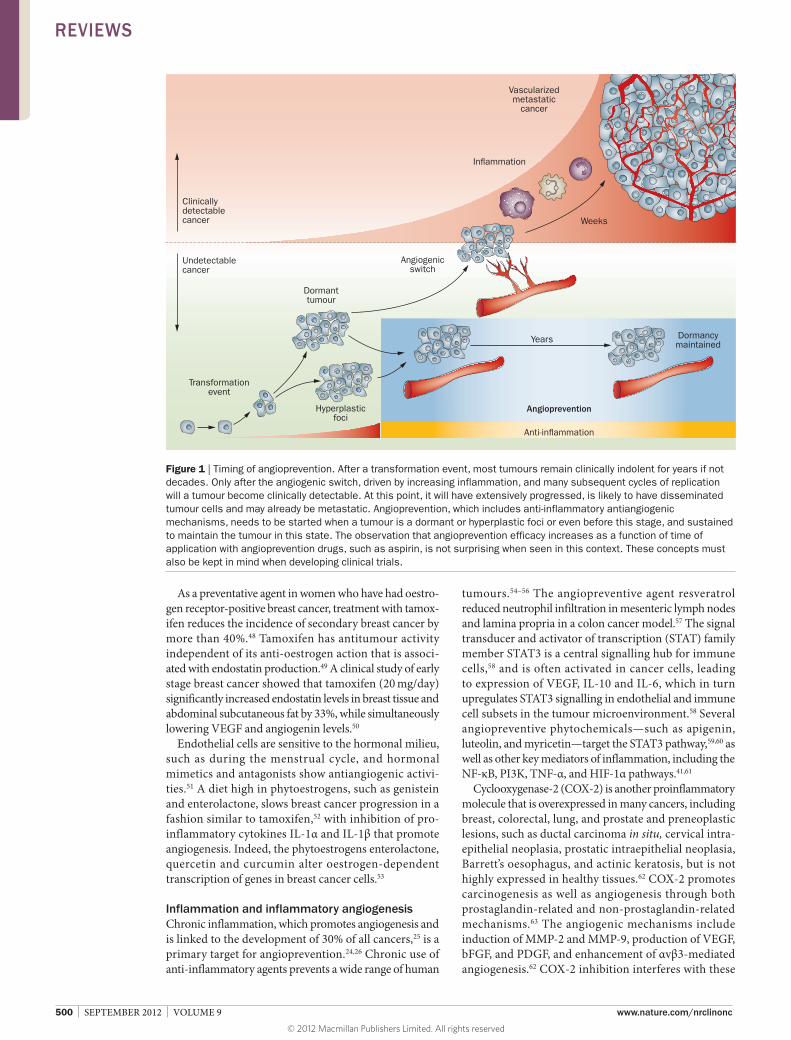
Figure 2 | Angiogenesis is controlled by a balance of endogenous stimulators and inhibitors; in homeostasis, the sum of these effects is null. Stimuli, for example in wound healing, can tip the balance, at first in favour of angiogenesis, where many new vessels are formed, then towards antiangiogenesis, where excess vessels are pruned away. Some angioprevention approaches aim to boost endogenous inhibitor levels and/or lower stimulators. Cell polarization from protumour to antitumour phenotypes, and metabolic repression can also promote a microenvironment resistant to tumour vascularization and tumour expansion. Abbreviations: MMP, matrix metalloproteinase; ROS, reactive oxygen species; TIMP, tissue inhibitor of metalloproteinase.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
502 | SEPTEMBER 2012 | VOLUME 9 www.nature.com/nrclinonc
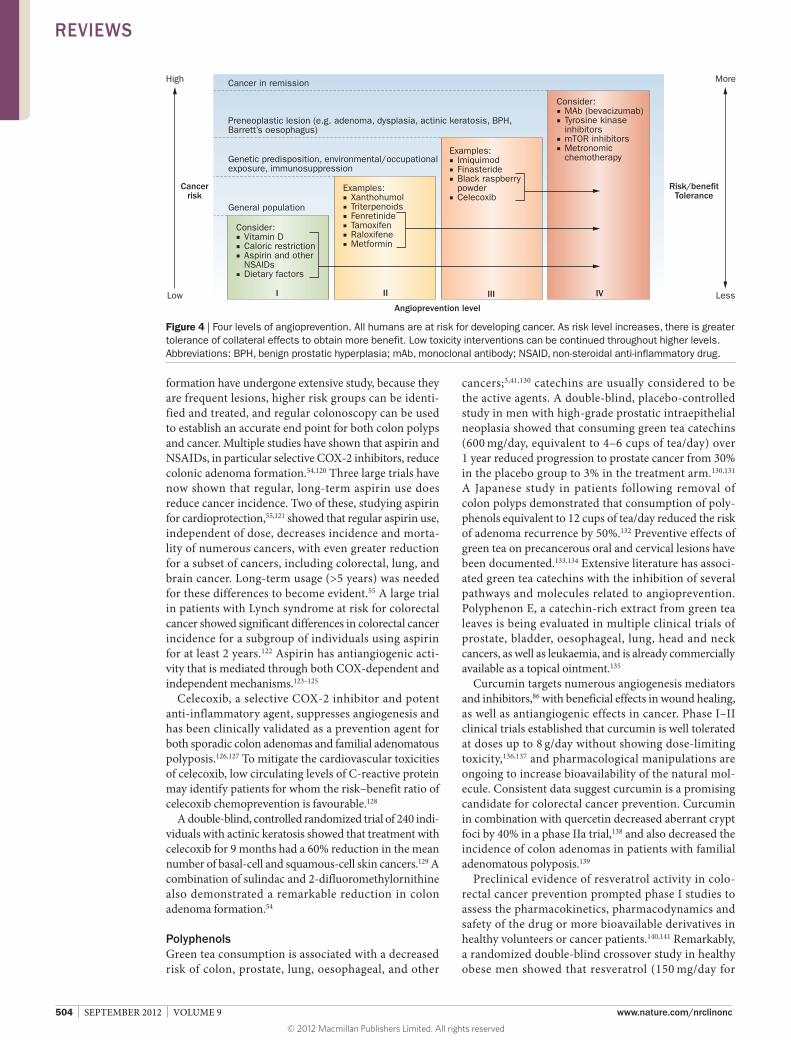
promoting stimuli. We propose four distinct levels of angioprevention (Figure 4).
Level IThis level is aimed at cancer prevention in the general healthy population at ‘lowest’ risk of developing cancer. In these low-risk individuals, intervention must be safe with few, if any, adverse effects. Possible interventions include dietary factors and scientifically supported dietary supple ments, caloric restriction, and aspirin, which is already used to prevent heart attack or stroke. Combinations of drugs or foods and nutritional supple-ments might have synergistic angiopreventive activity.89 For level I angioprevention, regulatory approval might be unnecessary as long as the interventions are safe and suitable for general application.
Level IILevel II angioprevention would be aimed at cancer pre-vention in individuals at moderate-to-high cancer risk. These include healthy persons with genetic abnorma-lities that are associated with a higher cancer risk (for example, BRCA1 and BRCA2 mutations, Li-Fraumeni syndrome and familial adenomatous polyposis), family history (any heritable cancer), occupational or lifestyle exposure (such as asbestos, toxins, tobacco and heavy alcohol consumption), immunosuppression (for example, transplan tation, or HIV) and/or metabolic syndromes
(including diabetes). The higher cancer risk of indivi-duals in this group justifies a higher risk tolerance for the angioprevention agents used than in level I.
Metformin is a well-tolerated drug suitable for level II angioprevention90 that is widely prescribed for type 2 diabetes and is potentially also usable for level I angio-prevention. Difluoromethylornithine (an inhibitor of polyamine synthesis) and sulindac,54 fenretinide and hormonal mimetics91 also fall into the level II angio-prevention category. Selected phytocompounds (cur-cumin, hyperforin, xanthohumol, and black raspberry extract) would also be appropriate,3,92 as well as synthetic triterpenoids, such as bardoxolone, which show potent antiangiogenic and anti-inflammatory activity.93–95
Level IIIIndividuals with pre-neoplastic lesions, such as skin actinic keratosis, oral leukoplakia, colon adenomas, cervical dysplasia, prostatic hypertrophy, and Barrett’s oesophagus would be eligible for level III angioprevention strategies. The risk for progression to frank carcinoma warrants a more-aggressive angiopreventive approach, with a greater risk-to-risk-tolerance ratio. A number of prescription drugs with angiogenesis inhibitory proper-ties are available, such as imiquimod (for skin cancer), finasteride (for prostate cancer), and celecoxib (for colon cancer).96 For the latter, cardiac protective treatment is warranted.97
JAK
STAT
Cytokines(e.g. TNF-α)
Cytokine inhibitors Phytochemicals Integrin inhibitors
Fenretinide
Anti-VEGF
TK inhibitorsGenistein
Nucleus Endothelial cell
IntegrinsGrowthfactor
(e.g. VEGF)
VEGF
VEGF
Angiogenesis
NF-κBIKK
IKK
STAT NF-κBCOX-2
MMP
NSAIDs
NSAIDsPhytochemicals
Metformin
FAK
Imiquimod
Cell survival
PI3K
Akt mTOR
AMPK Caloric restrictionMetforminPhytochemicals
Rapalogs(rapamycin,everolimus,temsirolimus)
Phytochemicals
ROS
Sirt1
GSK3β
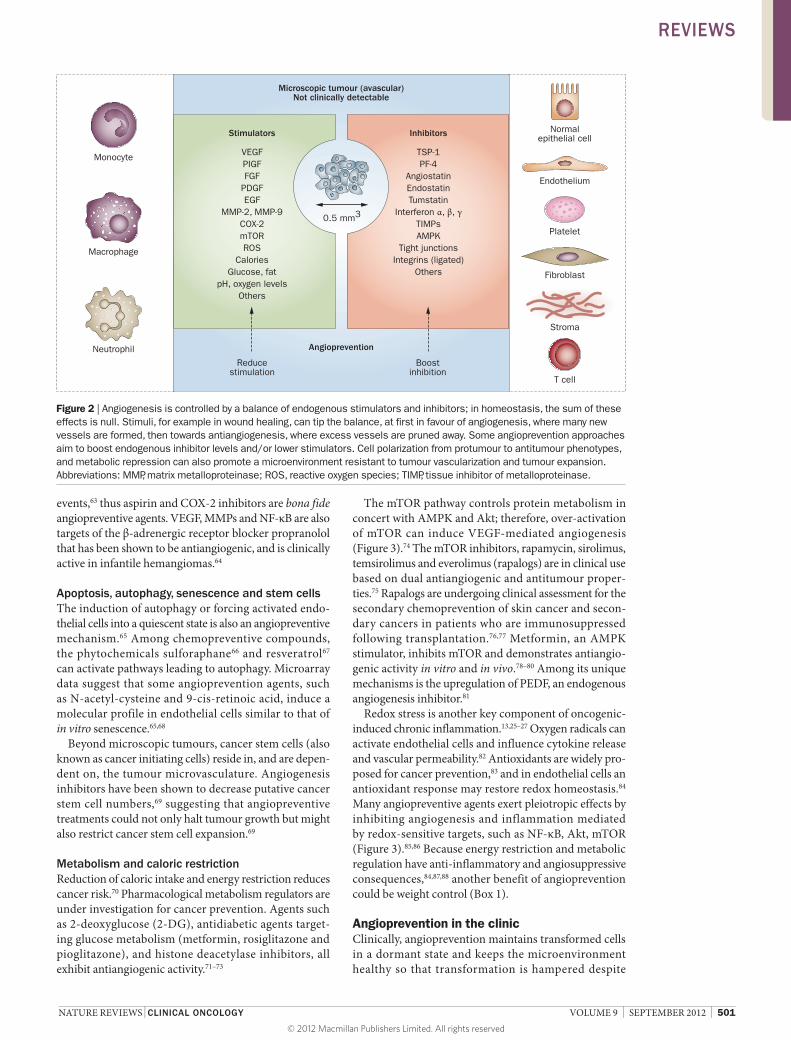
Figure 3 | Selected key signalling pathways that are targets for angioprevention. STAT and NF-κB are closely associated with inflammation and angiogenesis. Agents blocking these pathways in endothelial cells could have angiopreventive activity. Angiopreventive compounds induce both free-radical scavenging or transient reactive oxygen species elevation, evoking antioxidant responses. The identification of molecular targets of angioprevention is important for drug design, for identifying predictive biomarkers, and as a rationale for combinatorial angioprevention. Abbreviations: MMP, matrix metalloproteinase; NSAID, non-steroidal anti-inflammatory drug; ROS, reactive oxygen species; TK, tyrosine kinase; STAT; signal transducer and transcription activator.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | SEPTEMBER 2012 | 503
Level IVLevel IV angioprevention aims to prevent disease recur-rence in patients who have achieved cancer remission. An aggressive and sustained angiopreventive approach is necessary, since tumour cell dissemination is likely to exist.98 Prevention of pathological angiogenesis is of para-mount importance for durable cures. Angiopreventive interventions must potently suppress the ‘soil’ (micro-environment) as described by Steven Paget, so that the ‘seed’ (microscopic metastases) will not thrive.99,100 Level IV therapies include antiangiogenic cancer agents, such as tyrosine kinase inhibitors (axitinib, pazopanib, sorafenib, and sunitinib), mTOR inhibitors (everolimus, and temsirolimus), and certain chemotherapeutic drugs administered at low dose in a ‘metronomic’ schedule.101 Long-term administration of bevacizumab in the adjuvant setting is currently under clinical investigation.102,103
Regulatory issues, biomarker useRegulatory approval of pharmaceuticals for chemo-prevention has proved challenging. Both finasteride and dutasteride have been shown in large clinical trials to decrease risk of prostate cancer by 25–35% in treated healthy men, for example, but both were denied FDA approval for cancer prevention, because of uncertainty for applicability in the general population.104 The dis-covery of biomarkers for microscopic cancers may pave the way for monitoring the impact of angioprevention.105 Recent discoveries of proangiogenesis and antiangio-genesis markers in the platelet proteome reflecting dormant cancers are now being translated to clinical studies.106–108 Several microRNAs are highly expressed during angiogenesis, particularly miR-126 that targets VEGF.109 Effects of phytocompounds on vascular micro-RNAs are coming to light,110 including those with protec-tive effects on endothelial cells.111 MicroRNAs might also be a key source of biomarkers useful in angioprevention and cancer prevention in general.112
Whether regulatory approval is required for clinical application of angioprevention remains an open ques-tion. Dietary and over-the-counter drug angioprevention may not even require physician involvement at level I, while interventions from level II to level IV will need to be prescribed by a clinician.
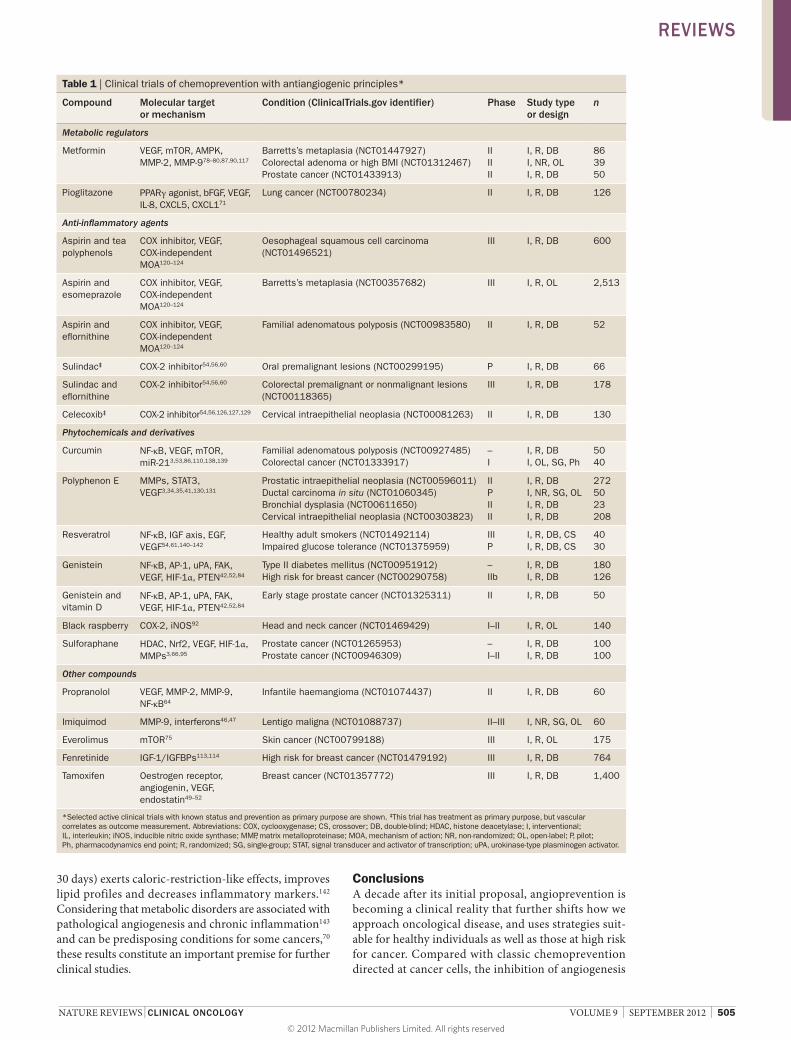
Successful angiopreventionClinical trials that assess antiangiogenesis and angio-prevention as an end point are underway (Table 1), increasing the urgency for identifying biomarkers for angio genesis.17 However, a number of chemo-preventive angiogenesis inhibitory agents have shown clinical efficacy. Here, we describe selected compounds that demonstrate angiopreventive benefits.
FenretinideSeveral retinoids inhibit angiogenesis, including fenre-tinide.113 A multicentre, randomized chemoprevention trial evaluated the effect of fenretinide on the incidence of contra lateral tumours in women with stage I breast cancer, showing a 35% reduction in second breast cancer
incidence in premenopausal women and significantly (95% CI 0.000–0.522; P = 0.0327) lower incidence of ovarian cancer in the fenretinide arm.114 An overall reduc-tion by 17% (hazard ratio [HR] = 0.83; 95% CI 0.67–1.03) in second breast cancer incidence was observed with fen-retinide after 14.6 years of follow up, along with a 38% (HR = 0.63; 95% CI 0.46–0.83) reduction in second breast cancer incidence in premenopausal women,114 reaching 50% (P-age*treatment interaction = 0.023) in women aged 40 years or younger. Fenretinide may be active in BRCA mutation carriers,113 and a randomized prevention trial is underway in women who are at high risk for breast and ovarian cancer.115
MetforminMetformin, widely used as a treatment for type 2 diabetes,116 is well tolerated and associated with limited, transient side effects. Retrospective population studies showed a 21% reduced risk and improved survival for all cancers in patients with type 2 diabetes receiving metformin.117,118 The results were significant even after adjusting for BMI, a cancer risk factor. Conversely, diabetics treated with non-metformin regimens had an increased (1.36–1.42 fold) risk for cancer.117 Another study demonstrated that patients taking metformin experienced a 62% risk reduction for pancreatic cancer.119 Metformin upregu-lates circu lating levels of the antiangiogenic extracellular matrix molecule thrombospondin-1 (TSP-1) in insulin-resistant obese women, likely one protective mechanism of action.87
Aspirin and NSAIDsObservational studies of long-term use of aspirin or NSAIDs revealed a reduced risk of colon, breast, pros-tate and lung cancer.56 Colon cancer and colon polyp
Box 1 | Angioprevention—not only in cancer
Pathological angiogenesis is a common denominator of many disorders,96 suggesting that clinical angioprevention may provide benefits in a wide range of conditions beyond cancer. In contrast to cancer, other pathologies often show more dependence on specific angiogenic pathways, further enhancing targeted drug action; the success of angiogenesis inhibition in the treatment of ‘wet’ age-related macular degeneration (AMD) is an example.145 This can be extended into the angioprevention realm. Epidemiological evidence suggests long-term non-steroidal anti-inflammatory drug (NSAID) use is associated with reduced risk of Alzheimer’s disease, where pathological brain microvessels are characteristic.146,147 The AREDS (Age-related Eye Disease Study) formula supplementation148 might implicate angioprevention in the neovascular form of AMD. Pathological angiogenesis driven by hypoxia and inflammation leads to joint destruction in patients with rheumatoid arthritis,149,150 where angioprevention may avert its progression. Angioprevention could even be used to prevent the growing epidemic of obesity, since controlling angiogenesis regulates adipose mass.151–153 Genetic polymorphisms of VEGF are associated with childhood obesity,154 and human studies have correlated BMI with inflammatory biomarkers (CRP) and angiogenesis (VEGF).143 Green tea intake reduced visceral fat in adults by 6% over 12 weeks in a small, prospective, controlled trial;155 other compounds such as synthetic triterpenoids are showing promise.156 Finally, many angiopreventive compounds, including phytochemicals, are showing protective effects on the cardiovascular system, not only by inhibiting atherosclerosis through suppressing plaque neovascularisation, but also by preventing collateral damage during cancer chemotherapy, while often enhancing efficacy.42 Combinatorial angioprevention regimens are a highly promising but untapped frontier.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
504 | SEPTEMBER 2012 | VOLUME 9 www.nature.com/nrclinonc
formation have undergone extensive study, because they are frequent lesions, higher risk groups can be identi-fied and treated, and regular colonoscopy can be used to establish an accurate end point for both colon polyps and cancer. Multiple studies have shown that aspirin and NSAIDs, in particular selective COX-2 inhibitors, reduce colonic adenoma formation.54,120 Three large trials have now shown that regular, long-term aspirin use does reduce cancer incidence. Two of these, studying aspirin for cardioprotection,55,121 showed that regular aspirin use, independent of dose, decreases incidence and morta-lity of numerous cancers, with even greater reduction for a subset of cancers, including colorectal, lung, and brain cancer. Long-term usage (>5 years) was needed for these differences to become evident.55 A large trial in patients with Lynch syndrome at risk for colorectal cancer showed significant differences in colorectal cancer incidence for a subgroup of individuals using aspirin for at least 2 years.122 Aspirin has antiangiogenic acti-vity that is mediated through both COX-dependent and independent mechanisms.123–125
Celecoxib, a selective COX-2 inhibitor and potent anti-inflammatory agent, suppresses angiogenesis and has been clinically validated as a prevention agent for both sporadic colon adenomas and familial adenomatous polyposis.126,127 To mitigate the cardiovascular toxicities of celecoxib, low circulating levels of C-reactive protein may identify patients for whom the risk–benefit ratio of celecoxib chemoprevention is favourable.128
A double-blind, controlled randomized trial of 240 indi-viduals with actinic keratosis showed that treatment with celecoxib for 9 months had a 60% reduction in the mean number of basal-cell and squamous-cell skin cancers.129 A combination of sulindac and 2-difluoromethylornithine also demonstrated a remarkable reduction in colon adenoma formation.54
PolyphenolsGreen tea consumption is associated with a decreased risk of colon, prostate, lung, oesophageal, and other
cancers;3,41,130 catechins are usually considered to be the active agents. A double-blind, placebo-controlled study in men with high-grade prostatic intraepithelial neoplasia showed that consuming green tea catechins (600 mg/day, equivalent to 4–6 cups of tea/day) over 1 year reduced progression to prostate cancer from 30% in the placebo group to 3% in the treatment arm.130,131 A Japanese study in patients following removal of colon polyps demonstrated that consumption of poly-phenols equivalent to 12 cups of tea/day reduced the risk of adenoma recurrence by 50%.132 Preventive effects of green tea on precancerous oral and cervical lesions have been documented.133,134 Extensive literature has associ-ated green tea catechins with the inhibition of several pathways and molecules related to angio prevention. Polyphenon E, a catechin-rich extract from green tea leaves is being evaluated in multiple clinical trials of prostate, bladder, oesophageal, lung, head and neck cancers, as well as leukaemia, and is already commercially available as a topical ointment.135
Curcumin targets numerous angiogenesis mediators and inhibitors,86 with beneficial effects in wound healing, as well as antiangiogenic effects in cancer. Phase I–II clinical trials established that curcumin is well tolerated at doses up to 8 g/day without showing dose-limiting toxicity,136,137 and pharmacological manipulations are ongoing to increase bioavailability of the natural mol-ecule. Consistent data suggest curcumin is a promising candidate for colorectal cancer prevention. Curcumin in combination with quercetin decreased aberrant crypt foci by 40% in a phase IIa trial,138 and also decreased the incidence of colon adenomas in patients with familial adenomatous polyposis.139
Preclinical evidence of resveratrol activity in colo-rectal cancer prevention prompted phase I studies to assess the pharmacokinetics, pharmacodynamics and safety of the drug or more bioavailable derivatives in healthy volunteers or cancer patients.140,141 Remarkably, a randomized double-blind crossover study in healthy obese men showed that resveratrol (150 mg/day for
High
Low
Cancerrisk
More
Less
Risk/bene�tTolerance
Angioprevention level
I II III IV
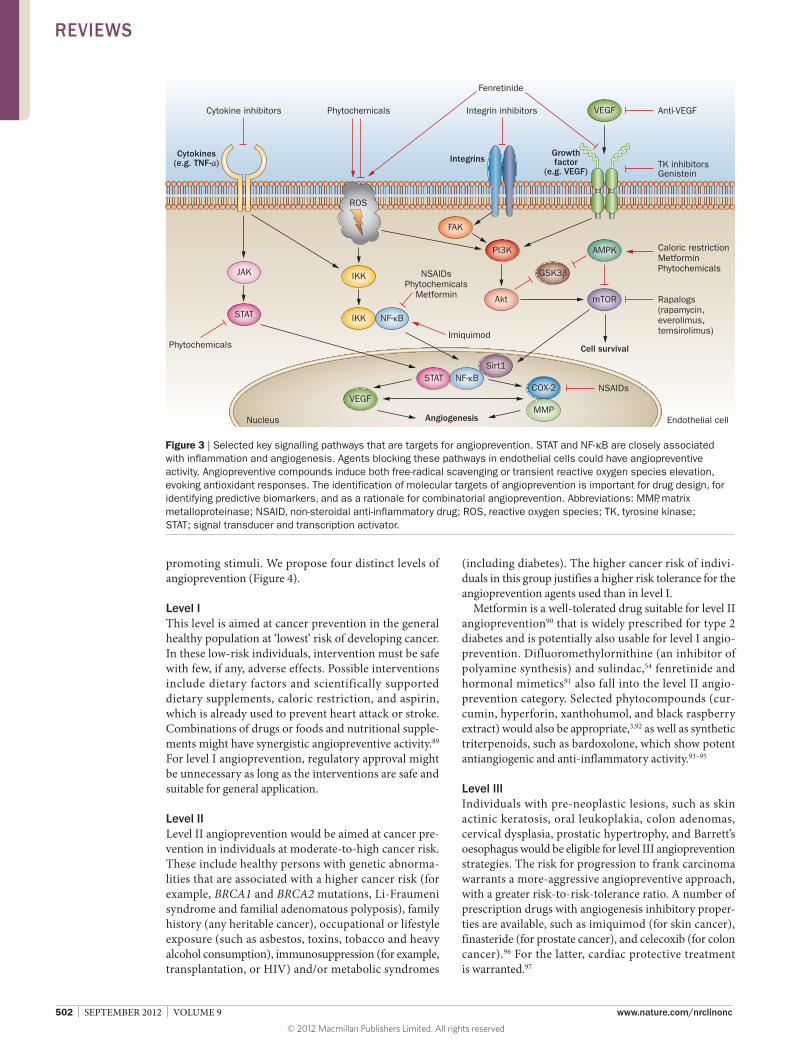
Consider:■ Vitamin D■ Caloric restriction■ Aspirin and other NSAIDs■ Dietary factors
Examples:■ Xanthohumol■ Triterpenoids■ Fenretinide■ Tamoxifen■ Raloxifene■ Metformin
Examples:■ Imiquimod■ Finasteride■ Black raspberry powder■ Celecoxib
Consider:■ MAb (bevacizumab)■ Tyrosine kinase inhibitors■ mTOR inhibitors■ Metronomic chemotherapy
General population
Genetic predisposition, environmental/occupationalexposure, immunosuppression
Preneoplastic lesion (e.g. adenoma, dysplasia, actinic keratosis, BPH,Barrett’s oesophagus)
Cancer in remission
Figure 4 | Four levels of angioprevention. All humans are at risk for developing cancer. As risk level increases, there is greater tolerance of collateral effects to obtain more benefit. Low toxicity interventions can be continued throughout higher levels. Abbreviations: BPH, benign prostatic hyperplasia; mAb, monoclonal antibody; NSAID, non-steroidal anti-inflammatory drug.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | SEPTEMBER 2012 | 505
30 days) exerts caloric-restriction-like effects, improves lipid profiles and decreases inflammatory markers.142 Considering that metabolic disorders are associated with pathological angiogenesis and chronic inflammation143 and can be predisposing conditions for some cancers,70 these results constitute an important premise for further clinical studies.
ConclusionsA decade after its initial proposal, angioprevention is becoming a clinical reality that further shifts how we approach oncological disease, and uses strategies suit-able for healthy individuals as well as those at high risk for cancer. Compared with classic chemoprevention directed at cancer cells, the inhibition of angiogenesis
Table 1 | Clinical trials of chemoprevention with antiangiogenic principles*
Compound Molecular target or mechanism
Condition (ClinicalTrials.gov identifier) Phase Study type or design
n
Metabolic regulators
Metformin VEGF, mTOR, AMPK, MMP-2, MMP-978–80,87,90,117
Barretts’s metaplasia (NCT01447927)Colorectal adenoma or high BMI (NCT01312467)Prostate cancer (NCT01433913)
IIIIII
I, R, DBI, NR, OLI, R, DB
863950
Pioglitazone PPARγ agonist, bFGF, VEGF, IL-8, CXCL5, CXCL171
Lung cancer (NCT00780234) II I, R, DB 126
Anti-inflammatory agents
Aspirin and tea polyphenols
COX inhibitor, VEGF, COX-independent MOA120–124
Oesophageal squamous cell carcinoma (NCT01496521)
III I, R, DB 600
Aspirin and esomeprazole
COX inhibitor, VEGF, COX-independent MOA120–124
Barretts’s metaplasia (NCT00357682) III I, R, OL 2,513
Aspirin and eflornithine
COX inhibitor, VEGF, COX-independent MOA120–124
Familial adenomatous polyposis (NCT00983580) II I, R, DB 52
Sulindac‡ COX-2 inhibitor54,56,60 Oral premalignant lesions (NCT00299195) P I, R, DB 66
Sulindac and eflornithine
COX-2 inhibitor54,56,60 Colorectal premalignant or nonmalignant lesions (NCT00118365)
III I, R, DB 178
Celecoxib‡ COX-2 inhibitor54,56,126,127,129 Cervical intraepithelial neoplasia (NCT00081263) II I, R, DB 130
Phytochemicals and derivatives
Curcumin NF-κB, VEGF, mTOR, miR-213,53,86,110,138,139
Familial adenomatous polyposis (NCT00927485)Colorectal cancer (NCT01333917)
–I
I, R, DBI, OL, SG, Ph
5040
Polyphenon E MMPs, STAT3, VEGF3,34,35,41,130,131
Prostatic intraepithelial neoplasia (NCT00596011)Ductal carcinoma in situ (NCT01060345)Bronchial dysplasia (NCT00611650)Cervical intraepithelial neoplasia (NCT00303823)
IIPIIII
I, R, DBI, NR, SG, OLI, R, DBI, R, DB
2725023208
Resveratrol NF-κB, IGF axis, EGF, VEGF54,61,140–142
Healthy adult smokers (NCT01492114)Impaired glucose tolerance (NCT01375959)
IIIP
I, R, DB, CSI, R, DB, CS
4030
Genistein NF-κB, AP-1, uPA, FAK, VEGF, HIF-1α, PTEN42,52,84
Type II diabetes mellitus (NCT00951912)High risk for breast cancer (NCT00290758)
–IIb
I, R, DBI, R, DB
180126
Genistein and vitamin D
NF-κB, AP-1, uPA, FAK, VEGF, HIF-1α, PTEN42,52,84
Early stage prostate cancer (NCT01325311) II I, R, DB 50
Black raspberry COX-2, iNOS92 Head and neck cancer (NCT01469429) I–II I, R, OL 140
Sulforaphane HDAC, Nrf2, VEGF, HIF-1α, MMPs3,66,95
Prostate cancer (NCT01265953)Prostate cancer (NCT00946309)
–I–II
I, R, DBI, R, DB
100100
Other compounds
Propranolol VEGF, MMP-2, MMP-9, NF-κB64
Infantile haemangioma (NCT01074437) II I, R, DB 60
Imiquimod MMP-9, interferons46,47 Lentigo maligna (NCT01088737) II–III I, NR, SG, OL 60
Everolimus mTOR75 Skin cancer (NCT00799188) III I, R, OL 175
Fenretinide IGF-1/IGFBPs113,114 High risk for breast cancer (NCT01479192) III I, R, DB 764
Tamoxifen Oestrogen receptor, angiogenin, VEGF, endostatin49–52
Breast cancer (NCT01357772) III I, R, DB 1,400
*Selected active clinical trials with known status and prevention as primary purpose are shown. ‡This trial has treatment as primary purpose, but vascular correlates as outcome measurement. Abbreviations: COX, cyclooxygenase; CS, crossover; DB, double-blind; HDAC, histone deacetylase; I, interventional; IL, interleukin; iNOS, inducible nitric oxide synthase; MMP, matrix metalloproteinase; MOA, mechanism of action; NR, non-randomized; OL, open-label; P, pilot; Ph, pharmacodynamics end point; R, randomized; SG, single-group; STAT, signal transducer and activator of transcription; uPA, urokinase-type plasminogen activator.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

506 | SEPTEMBER 2012 | VOLUME 9 www.nature.com/nrclinonc
and inflammation boosts anticancer defence mecha-nisms and provides protection against a broad spectrum of neoplasms.
We propose four levels of angioprevention: level I for the ‘healthy’ population; level II for those with conditions associated with a raised risk of cancer; level III for treat-ment of preneoplastic lesions; and level IV for prevention of recurrence of overt cancer. Angioprevention at levels I and II must be fundamentally non-toxic. Angiogenesis is crucial for wound healing and reproductive function, so angioprevention must be titrated to suppress undesirable angiogenesis, but not subvert healthy endothelial main-tenance or function. We compare this goal of physio-logically compatible angioprevention to the ‘Goldilocks Zone’ concept used by cosmologists seeking planets where life forms may reside.144 The term originated from the fairy tale about a child seeking porridge that is neither too hot nor too cold, but is ‘just right’. Angioprevention needs to achieve a degree of angiogenesis control that is neither over exuberant nor dangerously suppressed, without interfering with the Goldilocks Zone of healthy vascular function. One point that can be made is that many effi-cacious angioprevention drugs have multiple targets, yet do not completely inhibit any single pathway. This may lead to lower toxicity when compared with most potent single-target drugs. Several natural backbones of phyto-chemicals, such as aspirin, have been modified and tested for anticancer or chemopreventive activity. Molecular homologues could be designed from a chemopreventive
backbone to be more antiangiogenic and more suitable as angiopreventives. Synthetic chemistry and mo lecular tailoring may be used to design angiopreventive diet derivatives or pharmaceuticals.
Clinical trials are now underway to test the efficacy of angiopreventive molecules such as curcumin, artemi-sinin, resveratrol, genistein, synthetic triterpenoids, and isothiocyanates in neurological, cardiovascular degener-ative diseases, and cancer at levels III and IV as defined in this article. Given the global health priorities facing socie-ties today, and with the cancer pandemic in our sights, angioprevention and its clinical development is a concept whose time has arrived.
Review criteria
The references selected for this Review were searched in the PubMed database using the terms and Boolean strings: “Angiopreven*”; “(chemopreven* OR cancer prevention) AND (angiogen* AND endothel*)”; “prevention AND inflammation”; “chemoprevention AND microenvironment”; “antiangiogenic therapy AND clinical trials”; “angiogenesis AND biomarkers”; “antiangiogenesis AND resistance”. We also searched for selected articles mentioning “endothel* AND “pathways, ROS, cell death, senescence, miRNA, angiogenic gene expression, endogenous inhibitors, metabolism, caloric restriction, redox, antioxidant response”. We apologize to the many colleagues whose work we could not cite owing to space limitations.
1. Bloom, D. E. et al. The Global Economic Burden of Non-communicable Diseases [online], http://www3.weforum.org/docs/WEF_Harvard_HE_GlobalEconomicBurdenNonCommunicable Diseases_2011.pdf (2011).
2. Mariotto, A. B., Yabroff, K. R., Shao, Y., Feuer, E. J. & Brown, M. L. Projections of the cost of cancer care in the United States: 2010–2020. J. Natl Cancer Inst. 103, 117–128 (2011).
3. Albini, A. & Sporn, M. B. The tumour microenvironment as a target for chemoprevention. Nat. Rev. Cancer 7, 139–147 (2007).
4. Qaseem, A. et al. Screening for colorectal cancer: a guidance statement from the American College of Physicians. Ann. Intern. Med. 156, 378–386 (2012).
5. Nishizawa, S. et al. Prospective evaluation of whole-body cancer screening with multiple modalities including [18F]fluorodeoxyglucose positron emission tomography in a healthy population: a preliminary report. J. Clin. Oncol. 27, 1767–1773 (2009).
6. Shih, Y. C. et al. Economic burden of renal cell carcinoma: part I--an updated review. Pharmacoeconomics 29, 315–329 (2011).
7. Whyte, S., Pandor, A., Stevenson, M. & Rees, A. Bevacizumab in combination with fluoropyrimidine-based chemotherapy for the first-line treatment of metastatic colorectal cancer. Health Technol. Assess. 14, 47–53 (2010).
8. Lippman, S. M. & Hawk, E. T. Cancer prevention: from 1727 to milestones of the past 100 years. Cancer Res. 69, 5269–5284 (2009).
9. Willyard, C. Lifestyle: Breaking the cancer habit. Nature 471, S16–S17 (2011).
10. [No authors listed] Stat bite: Lifetime risk of being diagnosed with cancer. J. Natl Cancer Inst. 95, 1745 (2003).
11. Sporn, M. B. & Newton, D. L. Chemoprevention of cancer with retinoids. Fed. Proc. 38, 2528–2534 (1979).
12. Bissell, M. J. & Hines, W. C. Why don’t we get more cancer? A proposed role of the microenvironment in restraining cancer progression. Nat. Med. 17, 320–329 (2011).
13. Hanahan, D. & Weinberg, R. A. Hallmarks of cancer: the next generation. Cell 144, 646–674 (2011).
14. Tosetti, F., Ferrari, N., De Flora, S. & Albini, A. Angioprevention’: angiogenesis is a common and key target for cancer chemopreventive agents. FASEB J. 16, 2–14 (2002).
15. Folkman, J. Tumor angiogenesis: therapeutic implications. N. Engl. J. Med. 285, 1182–1186 (1971).
16. Ebos, J. M. & Kerbel, R. S. Antiangiogenic therapy: impact on invasion, disease progression, and metastasis. Nat. Rev. Clin. Oncol. 8, 210–221 (2011).
17. Jayson, G. C., Hicklin, D. J. & Ellis, L. M. Antiangiogenic therapy—evolving view based on clinical trial results. Nat. Rev. Clin. Oncol. 9, 297–303 (2012).
18. Ferrara, N. Role of myeloid cells in vascular endothelial growth factor-independent tumor angiogenesis. Curr. Opin. Hematol. 17, 219–224 (2010).
19. Nielsen, M., Thomsen, J. L., Primdahl, S., Dyreborg, U. & Andersen, J. A. Breast cancer and atypia among young and middle-aged women: a study of 110 medicolegal autopsies. Br. J. Cancer 56, 814–819 (1987).
20. Sanchez-Chapado, M., Olmedilla, G., Cabeza, M., Donat, E. & Ruiz, A. Prevalence of prostate cancer and prostatic intraepithelial neoplasia in Caucasian Mediterranean males: an autopsy study. Prostate 54, 238–247 (2003).
21. Black, W. C. & Welch, H. G. Advances in diagnostic imaging and overestimations of disease prevalence and the benefits of therapy. N. Engl. J. Med. 328, 1237–1243 (1993).
22. Harach, H. R., Franssila, K. O. & Wasenius, V. M. Occult papillary carcinoma of the thyroid. A “normal” finding in Finland. A systematic autopsy study. Cancer 56, 531–538 (1985).
23. Folkman, J. & Kalluri, R. Cancer without disease. Nature 427, 787 (2004).
24. Albini, A., Tosetti, F., Benelli, R. & Noonan, D. M. Tumor inflammatory angiogenesis and its chemoprevention. Cancer Res. 65, 10637–10641 (2005).
25. de Visser, K. E., Eichten, A. & Coussens, L. M. Paradoxical roles of the immune system during cancer development. Nat. Rev. Cancer 6, 24–37 (2006).
26. Noonan, D. M., De Lerma Barbaro, A., Vannini, N., Mortara, L. & Albini, A. Inflammation, inflammatory cells and angiogenesis: decisions and indecisions. Cancer Metastasis Rev. 27, 31–40 (2008).
27. Pollard, J. W. Tumour-educated macrophages promote tumour progression and metastasis. Nat. Rev. Cancer 4, 71–78 (2004).
28. Mantovani, A. & Sica, A. Macrophages, innate immunity and cancer: balance, tolerance, and diversity. Curr. Opin. Immunol. 22, 231–237 (2010).
29. Coffelt, S. B. et al. Elusive identities and overlapping phenotypes of proangiogenic myeloid cells in tumors. Am. J. Pathol. 176, 1564–1576 (2010).
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | SEPTEMBER 2012 | 507
30. Fridlender, Z. G. & Albelda, S. M. Tumor-associated neutrophils: friend or foe? Carcinogenesis 33, 949–955 (2012).
31. DeNardo, D. G., Andreu, P. & Coussens, L. M. Interactions between lymphocytes and myeloid cells regulate pro- versus anti-tumor immunity. Cancer Metastasis Rev. 29, 309–316 (2010).
32. Mason, S. D. & Joyce, J. A. Proteolytic networks in cancer. Trends Cell Biol. 21, 228–237 (2011).
33. Cao, Y. & Cao, R. Angiogenesis inhibited by drinking tea. Nature 398, 381 (1999).
34. Garbisa, S. et al. Tumor invasion: molecular shears blunted by green tea. Nat. Med. 5, 1216 (1999).
35. Noonan, D. M., Sogno, I. & Albini, A. in Herbal Medicines: Development and Validation of Plant-derived Medicines for Human Health (eds Bagetta, G., Cosentino, M., Corasaniti, M. T. & Sakurada, S.) 285–306 (CRC Press, Boca Raton, FL, 2011).
36. Albini, A., Indraccolo, S., Noonan, D. M. & Pfeffer, U. Functional genomics of endothelial cells treated with anti-angiogenic or angiopreventive drugs. Clin. Exp. Metastasis 27, 419–439 (2010).
37. Araldi, E. M. et al. Natural and synthetic agents targeting inflammation and angiogenesis for chemoprevention of prostate cancer. Curr. Cancer Drug Targets 8, 146–155 (2008).
38. Tahanian, E., Sanchez, L. A., Shiao, T. C., Roy, R. & Annabi, B. Flavonoids targeting of IκB phosphorylation abrogates carcinogen-induced MMP-9 and COX-2 expression in human brain endothelial cells. Drug Des. Devel. Ther. 5, 299–309 (2011).
39. Yang, M. D. et al. Phenethyl isothiocyanate inhibits migration and invasion of human gastric cancer AGS cells through suppressing MAPK and NF-kappaB signal pathways. Anticancer Res. 30, 2135–2143 (2010).
40. Manikandan, P., Murugan, R. S., Priyadarsini, R. V., Vinothini, G. & Nagini, S. Eugenol induces apoptosis and inhibits invasion and angiogenesis in a rat model of gastric carcinogenesis induced by MNNG. Life Sci. 86, 936–941 (2010).
41. Cao, Y., Cao, R. & Brakenhielm, E. Antiangiogenic mechanisms of diet-derived polyphenols. J. Nutr. Biochem. 13, 380–390 (2002).
42. Ferrari, N. et al. Diet-derived phytochemicals: from cancer chemoprevention to cardio-oncological prevention. Curr. Drug Targets 12, 1909–1924 (2011).
43. Li, W. W., Li, V. W., Hutnik, M. & Chiou, A. S. Tumor angiogenesis as a target for dietary cancer prevention. J. Oncol. 2012, 879623 (2012).
44. Sidky, Y. A. & Borden, E. C. Inhibition of angiogenesis by interferons: effects on tumor- and lymphocyte-induced vascular responses. Cancer Res. 47, 5155–5161 (1987).
45. Li, V. W. & Li, W. W. Antiangiogenesis in the treatment of skin cancer. J. Drugs Dermatol. 7 (Suppl. 1), s17–s24 (2008).
46. Li, V. W., Li, W. W., Talcott, K. E. & Zhai, A. W. Imiquimod as an antiangiogenic agent. J. Drugs Dermatol. 4, 708–717 (2005).
47. Sidbury, R. et al. Topically applied imiquimod inhibits vascular tumor growth in vivo. J. Invest. Dermatol. 121, 1205–1209 (2003).
48. Fisher, B. et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J. Natl Cancer Inst. 90, 1371–1388 (1998).
49. Bendrik, C., Karlsson, L. & Dabrosin, C. Increased endostatin generation and decreased angiogenesis via MMP-9 by tamoxifen in hormone dependent ovarian cancer. Cancer Lett. 292, 32–40 (2010).
50. Aberg, U. W. et al. Tamoxifen and flaxseed alter angiogenesis regulators in normal human breast tissue in vivo. PLoS ONE 6, e25720 (2011).
51. Blackwell, K. L. et al. Tamoxifen inhibits angiogenesis in estrogen receptor-negative animal models. Clin. Cancer Res. 6, 4359–4364 (2000).
52. Lindahl, G., Saarinen, N., Abrahamsson, A. & Dabrosin, C. Tamoxifen, flaxseed, and the lignan enterolactone increase stroma- and cancer cell-derived IL-1Ra and decrease tumor angiogenesis in estrogen-dependent breast cancer. Cancer Res. 71, 51–60 (2011).
53. Bachmeier, B. E. et al. Reference profile correlation reveals estrogen-like trancriptional activity of Curcumin. Cell. Physiol. Biochem. 26, 471–482 (2010).
54. William, W. N. Jr, Heymach, J. V., Kim, E. S. & Lippman, S. M. Molecular targets for cancer chemoprevention. Nat. Rev. Drug Discov. 8, 213–225 (2009).
55. Rothwell, P. M. et al. Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials. Lancet 377, 31–41 (2011).
56. Harris, R. E. Cyclooxygenase-2 (cox-2) blockade in the chemoprevention of cancers of the colon, breast, prostate, and lung. Inflammopharmacology 17, 55–67 (2009).
57. Cui, X. et al. Resveratrol suppresses colitis and colon cancer associated with colitis. Cancer Prev. Res. (Phila.) 3, 549–559 (2010).
58. Yu, H., Pardoll, D. & Jove, R. STATs in cancer inflammation and immunity: a leading role for STAT3. Nat. Rev. Cancer 9, 798–809 (2009).
59. Lamy, S., Akla, N., Ouanouki, A., Lord-Dufour, S. & Beliveau, R. Diet-derived polyphenols inhibit angiogenesis by modulating the interleukin-6/STAT3 pathway. Exp. Cell Res. 318, 1586–1596 (2012).
60. Aggarwal, B. B., Vijayalekshmi, R. V. & Sung, B. Targeting inflammatory pathways for prevention and therapy of cancer: short-term friend, long-term foe. Clin. Cancer Res. 15, 425–430 (2009).
61. Gupta, S. C., Kim, J. H., Prasad, S. & Aggarwal, B. B. Regulation of survival, proliferation, invasion, angiogenesis, and metastasis of tumor cells through modulation of inflammatory pathways by nutraceuticals. Cancer Metastasis Rev. 29, 405–434 (2010).
62. Gately, S. & Li, W. W. Multiple roles of COX-2 in tumor angiogenesis: a target for antiangiogenic therapy. Semin. Oncol. 31, 2–11 (2004).
63. Fosslien, E. Review: molecular pathology of cyclooxygenase-2 in cancer-induced angiogenesis. Ann. Clin. Lab. Sci. 31, 325–348 (2001).
64. Greenberger, S. & Bischoff, J. Infantile Hemangioma-Mechanism(s) of Drug Action on a Vascular Tumor. Cold Spring Harb. Perspect. Med. 1, a006460 (2011).
65. Vannini, N., Pfeffer, U., Lorusso, G., Noonan, D. M. & Albini, A. Endothelial cell aging and apoptosis in prevention and disease: E-selectin expression and modulation as a model. Curr. Pharm. Des. 14, 221–225 (2008).
66. Nishikawa, T. et al. The inhibition of autophagy potentiates anti-angiogenic effects of sulforaphane by inducing apoptosis. Angiogenesis 13, 227–238 (2010).
67. Delmas, D., Solary, E. & Latruffe, N. Resveratrol, a phytochemical inducer of multiple cell death pathways: apoptosis, autophagy and mitotic catastrophe. Curr. Med. Chem. 18, 1100–1121 (2011).
68. Christov, K. T., Shilkaitis, A. L., Kim, E. S., Steele, V. E. & Lubet, R. A. Chemopreventive agents induce a senescence-like phenotype in
rat mammary tumours. Eur. J. Cancer 39, 230–239 (2003).
69. Albini, A., Cesana, E. & Noonan, D. M. Cancer stem cells and the tumor microenvironment: soloists or choral singers. Curr. Pharm. Biotechnol. 12, 171–181 (2011).
70. Hursting, S. D., Smith, S. M., Lashinger, L. M., Harvey, A. E. & Perkins, S. N. Calories and carcinogenesis: lessons learned from 30 years of calorie restriction research. Carcinogenesis 31, 83–89 (2010).
71. Aljada, A., O’Connor, L., Fu, Y. Y. & Mousa, S. A. PPAR gamma ligands, rosiglitazone and pioglitazone, inhibit bFGF- and VEGF-mediated angiogenesis. Angiogenesis 11, 361–367 (2008).
72. Merchan, J. R. et al. Antiangiogenic activity of 2-deoxy-D-glucose. PLoS ONE 5, e13699 (2010).
73. Fraisl, P., Mazzone, M., Schmidt, T. & Carmeliet, P. Regulation of angiogenesis by oxygen and metabolism. Dev. Cell 16, 167–179 (2009).
74. Lee, D. F. et al. IKK beta suppression of TSC1 links inflammation and tumor angiogenesis via the mTOR pathway. Cell 130, 440–455 (2007).
75. Fasolo, A. & Sessa, C. Targeting mTOR pathways in human malignancies. Curr. Pharm. Des. 18, 2766–2777 (2012).
76. US National Library of Medicine. ClinicalTrials.gov [online], http://www.clinicaltrials.gov/ct2/ results?term=temsirolimus+prevention+skin (2012).
77. US National Library of Medicine. ClinicalTrials.gov [online], http://www.clinicaltrials.gov/ct2/ results?term=cancer+AND+angiogenesis+AND+%28rapamycin+OR+sirolimus+OR+ temsirolimus+OR+everolimus%29+ (2012).
78. Phoenix, K. N., Vumbaca, F. & Claffey, K. P. Therapeutic metformin/AMPK activation promotes the angiogenic phenotype in the ERalpha negative MDA-MB-435 breast cancer model. Breast Cancer Res. Treat. 113, 101–111 (2009).
79. Xavier, D. O. et al. Metformin inhibits inflammatory angiogenesis in a murine sponge model. Biomed. Pharmacother. 64, 220–225 (2010).
80. Esfahanian, N. et al. Effect of metformin on the proliferation, migration, and MMP-2 and -9 expression of human umbilical vein endothelial cells. Mol. Med. Report 5, 1068–1074 (2012).
81. Akin, S. et al. Pigment epithelium-derived factor (PEDF) increases in type 2 diabetes after treatment with metformin. Clin. Endocrinol. (Oxf.) http:dx.doi.org/10.1111/ j.1365-2265.2012.04341.x.
82. Alom-Ruiz, S. P., Anilkumar, N. & Shah, A. M. Reactive oxygen species and endothelial activation. Antioxid. Redox Signal. 10, 1089–1100 (2008).
83. De Flora, S. et al. Multiple points of intervention in the prevention of cancer and other mutation-related diseases. Mutat. Res. 480–481, 9–22 (2001).
84. Tosetti, F., Noonan, D. M. & Albini, A. Metabolic regulation and redox activity as mechanisms for angioprevention by dietary phytochemicals. Int. J. Cancer 125, 1997–2003 (2009).
85. Aggarwal, B. B. Targeting inflammation-induced obesity and metabolic diseases by curcumin and other nutraceuticals. Annu. Rev. Nutr. 30, 173–199 (2010).
86. Yadav, V. R. & Aggarwal, B. B. Curcumin: a component of the golden spice, targets multiple angiogenic pathways. Cancer Biol. Ther. 11, 236–241 (2011).
87. Tan, B. K. et al. Metformin decreases angiogenesis via NF-kappaB and Erk1/2/Erk5 pathways by increasing the antiangiogenic thrombospondin-1. Cardiovasc. Res. 83, 566–574 (2009).
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
508 | SEPTEMBER 2012 | VOLUME 9 www.nature.com/nrclinonc
88. De Lorenzo, M. S. et al. Caloric restriction reduces growth of mammary tumors and metastases. Carcinogenesis 32, 1381–1387 (2011).
89. Zhou, J. R., Li, L. & Pan, W. Dietary soy and tea combinations for prevention of breast and prostate cancers by targeting metabolic syndrome elements in mice. Am. J. Clin. Nutr. 86, s882–s888 (2007).
90. Cazzaniga, M., Bonanni, B., Guerrieri-Gonzaga, A. & Decensi, A. Is it time to test metformin in breast cancer clinical trials? Cancer Epidemiol. Biomarkers Prev. 18, 701–705 (2009).
91. Cuzick, J. et al. Preventive therapy for breast cancer: a consensus statement. Lancet Oncol. 12, 496–503 (2011).
92. Mallery, S. R. et al. Topical application of a bioadhesive black raspberry gel modulates gene expression and reduces cyclooxygenase 2 protein in human premalignant oral lesions. Cancer Res. 68, 4945–4957 (2008).
93. Vannini, N. et al. The synthetic oleanane triterpenoid, CDDO-methyl ester, is a potent antiangiogenic agent. Mol. Cancer Ther. 6, 3139–3146 (2007).
94. Kim, E. H. et al. CDDO-methyl ester delays breast cancer development in BRCA1-mutated mice. Cancer Prev. Res. (Phila.) 5, 89–97 (2012).
95. Sporn, M. B. Perspective: The big C - for Chemoprevention. Nature 471, S10–S11 (2011).
96. Li, W., Hutnik, M. & Li, V. in Angiogenesis: Basic Science and Clinical Applications (eds Maragoudakis, M. & Papadimitriou, E.) 377–417 (Research Signpost, Trivandrum, India, 2008).
97. Albini, A. et al. Cardiotoxicity of anticancer drugs: the need for cardio-oncology and cardio-oncological prevention. J. Natl Cancer Inst. 102, 14–25 (2010).
98. Comen, E., Norton, L. & Massague, J. Clinical implications of cancer self-seeding. Nat. Rev. Clin. Oncol. 8, 369–377 (2011).
99. Albini, A. & Noonan, D. M. Angiopoietin2 and tie2: tied to lymphangiogenesis and lung metastasis. New perspectives in antimetastatic antiangiogenic therapy. J. Natl Cancer Inst. 104, 429–431 (2012).
100. Albini, A. & Noonan, D. M. The ‘chemoinvasion’ assay, 25 years and still going strong: the use of reconstituted basement membranes to study cell invasion and angiogenesis. Curr. Opin. Cell. Biol. 22, 677–689 (2010).
101. Pasquier, E., Kavallaris, M. & Andre, N. Metronomic chemotherapy: new rationale for new directions. Nat. Rev. Clin. Oncol. 7, 455–465 (2010).
102. Spigel, D. R. et al. Phase II study of bevacizumab and chemoradiation in the preoperative or adjuvant treatment of patients with stage II/III rectal cancer. Clin. Colorectal Cancer 11, 45–52 (2012).
103. Allegra, C. J. et al. Phase III trial assessing bevacizumab in stages II and III carcinoma of the colon: results of NSABP protocol C-08. J. Clin. Oncol. 29, 11–16 (2011).
104. Jonietz, E. Designing smarter cancer prevention trials. Nature 471, S20–S21 (2011).
105. Sogno, I., Conti, M., Consonni, P., Noonan, D. M. & Albini, A. Surface-activated chemical ionization-electrospray ionization source improves biomarker discovery with mass spectrometry. Rapid Commun. Mass Spectrom. 26, 1213–1218 (2012).
106. Cervi, D. et al. Platelet-associated PF-4 as a biomarker of early tumor growth. Blood 111, 1201–1207 (2008).
107. Italiano, J. E. Jr et al. Angiogenesis is regulated by a novel mechanism: pro- and antiangiogenic proteins are organized into separate platelet
alpha granules and differentially released. Blood 111, 1227–1233 (2008).
108. Peterson, J. E. et al. Normal ranges of angiogenesis regulatory proteins in human platelets. Am. J. Hematol. 85, 487–493 (2010).
109. Fish, J. E. & Srivastava, D. MicroRNAs: opening a new vein in angiogenesis research. Sci. Signal. 2, pe1 (2009).
110. Reuter, S., Gupta, S. C., Park, B., Goel, A. & Aggarwal, B. B. Epigenetic changes induced by curcumin and other natural compounds. Genes Nutr. 6, 93–108 (2011).
111. Noratto, G. D., Angel-Morales, G., Talcott, S. T. & Mertens-Talcott, S. U. Polyphenolics from açai (Euterpe oleracea Mart.) and red muscadine grape (Vitis rotundifolia) protect human umbilical vascular endothelial cells (HUVEC) from glucose- and lipopolysaccharide (LPS)-induced inflammation and target microRNA-126. J. Agric. Food Chem. 59, 7999–8012 (2011).
112. White, N. M. et al. Metastamirs: a stepping stone towards improved cancer management. Nat. Rev. Clin. Oncol. 8, 75–84 (2011).
113. Sogno, I. et al. Angioprevention with fenretinide: targeting angiogenesis in prevention and therapeutic strategies. Crit. Rev. Oncol. Hematol. 75, 2–14 (2010).
114. Veronesi, U. et al. Fifteen-year results of a randomized phase III trial of fenretinide to prevent second breast cancer. Ann. Oncol. 17, 1065–1071 (2006).
115. US National Library of Medicine. ClinicalTrials.gov [online], http://www.clinicaltrials.gov/ct2/ show/NCT01479192 (2011).
116. [No authors listed] Standards of medical care in diabetes—2009. Diabetes Care 32 (Suppl. 1), S13–S61 (2009).
117. Currie, C. J., Poole, C. D. & Gale, E. A. The influence of glucose-lowering therapies on cancer risk in type 2 diabetes. Diabetologia 52, 1766–1777 (2009).
118. Goodwin, P. J. et al. Evaluation of metformin in early breast cancer: a modification of the traditional paradigm for clinical testing of anti-cancer agents. Breast Cancer Res. Treat. 126, 215–220 (2011).
119. Li, D., Yeung, S. C., Hassan, M. M., Konopleva, M. & Abbruzzese, J. L. Antidiabetic therapies affect risk of pancreatic cancer. Gastroenterology 137, 482–488 (2009).
120. Cole, B. F. et al. Aspirin for the chemoprevention of colorectal adenomas: meta-analysis of the randomized trials. J. Natl Cancer Inst. 101, 256–266 (2009).
121. Rothwell, P. M. et al. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet 376, 1741–1750 (2010).
122. Burn, J. et al. Long-term effect of aspirin on cancer risk in carriers of hereditary colorectal cancer: an analysis from the CAPP2 randomised controlled trial. Lancet 378, 2081–2087 (2011).
123. Battinelli, E. M., Markens, B. A. & Italiano, J. E. Jr. Release of angiogenesis regulatory proteins from platelet alpha granules: modulation of physiologic and pathologic angiogenesis. Blood 118, 1359–1369 (2011).
124. Borthwick, G. M. et al. Therapeutic levels of aspirin and salicylate directly inhibit a model of angiogenesis through a Cox-independent mechanism. FASEB J. 20, 2009–2016 (2006).
125. Hawley, S. A. et al. The ancient drug salicylate directly activates AMP-activated protein kinase. Science 336, 918–922 (2012).
126. Lynch, P. M. et al. The safety and efficacy of celecoxib in children with familial adenomatous
polyposis. Am. J. Gastroenterol. 105, 1437–1443 (2010).
127. Bertagnolli, M. M. et al. Five-year efficacy and safety analysis of the Adenoma Prevention with Celecoxib Trial. Cancer Prev. Res. (Phila.) 2, 310–321 (2009).
128. Chan, A. T. et al. C-reactive protein and risk of colorectal adenoma according to celecoxib treatment. Cancer Prev. Res. (Phila.) 4, 1172–1180 (2011).
129. Elmets, C. A. et al. Chemoprevention of nonmelanoma skin cancer with celecoxib: a randomized, double-blind, placebo-controlled trial. J. Natl Cancer Inst. 102, 1835–1844 (2010).
130. Bettuzzi, S. et al. Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia: a preliminary report from a one-year proof-of-principle study. Cancer Res. 66, 1234–1240 (2006).
131. Brausi, M., Rizzi, F. & Bettuzzi, S. Chemoprevention of human prostate cancer by green tea catechins: two years later. A follow-up update. Eur. Urol. 54, 472–473 (2008).
132. Shimizu, M. et al. Green tea extracts for the prevention of metachronous colorectal adenomas: a pilot study. Cancer Epidemiol. Biomarkers Prev. 17, 3020–3025 (2008).
133. Li, N., Sun, Z., Han, C. & Chen, J. The chemopreventive effects of tea on human oral precancerous mucosa lesions. Proc. Soc. Exp. Biol. Med. 220, 218–224 (1999).
134. Ahn, W. S. et al. Protective effects of green tea extracts (polyphenon E and EGCG) on human cervical lesions. Eur. J. Cancer Prev. 12, 383–390 (2003).
135. US National Library of Medicine. ClinicalTrials.gov [online], http://www.clinicaltrials.gov/ct2/ results?term=polyphenon+E+cancer (2012).
136. Cheng, A. L. et al. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res. 21, 2895–2900 (2001).
137. Dhillon, N. et al. Phase II trial of curcumin in patients with advanced pancreatic cancer. Clin. Cancer Res. 14, 4491–4499 (2008).
138. Carroll, R. E. et al. Phase IIa clinical trial of curcumin for the prevention of colorectal neoplasia. Cancer Prev. Res. (Phila.) 4, 354–364 (2011).
139. Cruz-Correa, M. et al. Combination treatment with curcumin and quercetin of adenomas in familial adenomatous polyposis. Clin. Gastroenterol. Hepatol. 4, 1035–1038 (2006).
140. Brown, V. A. et al. Repeat dose study of the cancer chemopreventive agent resveratrol in healthy volunteers: safety, pharmacokinetics, and effect on the insulin-like growth factor axis. Cancer Res. 70, 9003–9011 (2010).
141. Howells, L. M. et al. Phase I randomized, double-blind pilot study of micronized resveratrol (SRT501) in patients with hepatic metastases—safety, pharmacokinetics, and pharmacodynamics. Cancer Prev. Res. (Phila.) 4, 1419–1425 (2011).
142. Timmers, S. et al. Calorie restriction-like effects of 30 days of resveratrol supplementation on energy metabolism and metabolic profile in obese humans. Cell. Metab. 14, 612–622 (2011).
143. Siervo, M. et al. Body mass index is directly associated with biomarkers of angiogenesis and inflammation in children and adolescents. Nutrition 28, 262–266 (2012).
144. Bhattacharjee, Y. Exoplanetary research. A distant glimpse of alien life? Science 333, 930–932 (2011).
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | SEPTEMBER 2012 | 509
145. Lally, D. R., Gerstenblith, A. T. & Regillo, C. D. Preferred therapies for neovascular age-related macular degeneration. Curr. Opin. Ophthalmol. 23, 182–188 (2012).
146. Breitner, J. C. et al. Extended results of the Alzheimer’s disease anti-inflammatory prevention trial. Alzheimers Dement. 7, 402–411 (2011).
147. Desai, B. S., Schneider, J. A., Li, J. L., Carvey, P. M. & Hendey, B. Evidence of angiogenic vessels in Alzheimer’s disease. J. Neural. Transm. 116, 587–597 (2009).
148. Zeng, S., Hernandez, J. & Mullins, R. F. Effects of antioxidant components of AREDS vitamins and zinc ions on endothelial cell activation: implications for macular degeneration. Invest. Ophthalmol. Vis. Sci. 53, 1041–1047 (2012).
149. Konisti, S., Kiriakidis, S. & Paleolog, E. M. Hypoxia--a key regulator of angiogenesis and inflammation in rheumatoid arthritis. Nat. Rev. Rheumatol. 8, 153–162 (2012).
150. Lainer-Carr, D. & Brahn, E. Angiogenesis inhibition as a therapeutic approach for inflammatory synovitis. Nat. Clin. Pract. Rheumatol. 3, 434–442 (2007).
151. Cao, Y. Angiogenesis modulates adipogenesis and obesity. J. Clin. Invest. 117, 2362–2368 (2007).
152. Cao, Y. Adipose tissue angiogenesis as a therapeutic target for obesity and metabolic diseases. Nat. Rev. Drug Discov. 9, 107–115 (2010).
153. Daquinag, A. C., Zhang, Y. & Kolonin, M. G. Vascular targeting of adipose tissue as an anti-obesity approach. Trends Pharmacol. Sci. 32, 300–307 (2011).
154. Belo, V. A. et al. Vascular endothelial growth factor haplotypes associated with childhood obesity. DNA Cell Biol. 30, 709–714 (2011).
155. Zhang, Y. et al. Effects of catechin-enriched green tea beverage on visceral fat loss in adults with a high proportion of visceral fat: a double-blind, placebo-controlled, randomized trial. J. Functional Foods 4, 315–322 (2012).
156. Shin, S. et al. Role of Nrf2 in prevention of high-fat diet-induced obesity by synthetic triterpenoid CDDO-imidazolide. Eur. J. Pharmacol. 620, 138–144 (2009).
AcknowledgementsThe authors would like to thank Diana Saville (Angiogenesis Foundation) for rendering medical graphics. We thank Paola Corradino (MultiMedica IRCCS) for data management, and Alessandra Panvini Rosati (MultiMedica Onlus) and Giuseppe Bertani (IRCCS–Arcispedale Santa Maria Nuova) for administrative assistance. The authors were supported by grants from the AIRC (Associazione Italiana per la Ricerca sul Cancro; IG5968 to D. M. Noolan, IG10228 to A. Albini), the Cariplo Foundation, Progetto Finalizzato of the Ministero della Sanità and by funds from the University of Insubria (fondi di Ateneo) and MultiMedica Onlus. A. Albini is currently Director of Research and Statistics Infrastructure, IRCCS–Arcispedale Santa Maria Nuova (Reggio Emilia-Italy).
Author contributionsAll authors made a substantial contribution to researching and discussing data for this Review, and to writing the manuscript. All authors reviewed and edited the manuscript prior to submission. D. M. Noonan and W. W. Li contributed equally to this article.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
Related Documents











