Calcinosis cutis secondary to percutaneous penetration of calcium carbonate in a Dalmatian Manon Paradis and Danny W. Scott A one and one-half-year-old intact female Dalmatian dog was presented to the Small Animal Clinic (SAC) of the Faculte de medecine veterinaire of the University of Montreal with a two-week history of a skin problem. Multifocal erythematous, hyperkerato- tic, flat-topped papules with central crateriform ulcera- tions were present on the thinly-haired skin of the ven- tral abdomen, the inguinal region, and the medial aspect of both hind legs (Figure 1). Solitary ulcerated nodules were present on both left abdominal mam- mary glands. Some of the flat-topped papules had coalesced to form a partially ulcerated plaque in the left inguinal fold (Figure 2). The paws and haired skin were normal. The dog had licked the affected areas frequently, but was otherwise in good health. Physical examination revealed no other abnormali- ties, except for galactostasis that was attributed to Figure 1. Close-up of erythematous papules on the medial thigh. Can Vet J 1989; 30: 57-59 Figure 2. Ulcerated nodules affecting nipples. pseudopregnancy. In fact, the bitch had been in estrus two months previously. One week prior to presenta- tion at the SAC, the skin lesions had been treated without success by another veterinarian with anti- biotics and corticosteroids. Differential diagnoses for the papuloulcerative der- matitis in this dog included: 1) primary irritant contact dermatitis, 2) idiopathic lichenoid dermatitis, 3) mycotic infection (caused by Sporothrix schenkii, Cryptococcus neoformans, or dermatophytes), 4) bacterial infection (staphylococcal folliculitis, atypical mycobacterial granuloma), 5) demodicosis with secondary deep pyoderma, and 6) neoplasia (mast cell tumor or cutaneous lymphosarcoma). A systematic diagnostic approach to define the cause of the dermatological disease included microscopic examination of multiple skin scrapings from affected areas and aseptic collection of representative skin biopsy specimens for fungal and bacteriological cul- ture. Homogenized skin biopsy specimens were plated on dermatophyte test medium, Sabouraud's medium, Can Vet J Volume 30, January 1989 Department of Medicine, Faculty of Veterinary Medicine, University of Montreal, P.O. Box 5000, Saint-Hyacinthe, Quebec J2S 7C6. 57

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Calcinosis cutis secondary to percutaneouspenetration of calcium carbonate in a Dalmatian
Manon Paradis and Danny W. ScottAone and one-half-year-old intact female Dalmatian
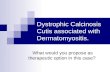
dog was presented to the Small Animal Clinic(SAC) of the Faculte de medecine veterinaire of theUniversity of Montreal with a two-week history of askin problem. Multifocal erythematous, hyperkerato-tic, flat-topped papules with central crateriform ulcera-tions were present on the thinly-haired skin of the ven-tral abdomen, the inguinal region, and the medialaspect of both hind legs (Figure 1). Solitary ulceratednodules were present on both left abdominal mam-mary glands. Some of the flat-topped papules hadcoalesced to form a partially ulcerated plaque in theleft inguinal fold (Figure 2). The paws and haired skinwere normal. The dog had licked the affected areasfrequently, but was otherwise in good health.
Physical examination revealed no other abnormali-ties, except for galactostasis that was attributed to
Figure 1. Close-up of erythematous papules on the medialthigh.
Can Vet J 1989; 30: 57-59
Figure 2. Ulcerated nodules affecting nipples.
pseudopregnancy. In fact, the bitch had been in estrustwo months previously. One week prior to presenta-tion at the SAC, the skin lesions had been treatedwithout success by another veterinarian with anti-biotics and corticosteroids.
Differential diagnoses for the papuloulcerative der-matitis in this dog included:1) primary irritant contact dermatitis,2) idiopathic lichenoid dermatitis,3) mycotic infection (caused by Sporothrix schenkii,
Cryptococcus neoformans, or dermatophytes),4) bacterial infection (staphylococcal folliculitis,
atypical mycobacterial granuloma),5) demodicosis with secondary deep pyoderma, and6) neoplasia (mast cell tumor or cutaneous
lymphosarcoma).A systematic diagnostic approach to define the cause
of the dermatological disease included microscopicexamination of multiple skin scrapings from affectedareas and aseptic collection of representative skinbiopsy specimens for fungal and bacteriological cul-ture. Homogenized skin biopsy specimens were platedon dermatophyte test medium, Sabouraud's medium,
Can Vet J Volume 30, January 1989
Department of Medicine, Faculty of Veterinary Medicine,University of Montreal, P.O. Box 5000, Saint-Hyacinthe,Quebec J2S 7C6.
57

Figure 3. Skin biopsy. Degeneration and dystropic min-eralization of collagen fibers surrounded by pyogranu-lamatous inflammation (HPS stain).
and blood agar. Other skin biopsy specimens fromrepresentative ulcerated and papular lesions were fixedin 10%o formalin and stained with hematoxylin/phloxin/saffran (HPS) for histological examination. A bloodsample was obtained for CBC.The dog was sent home wearing an Elizabethan col-
lar and was to be given amoxicillin-clavulinic acid,250 mg bid orally, for two weeks, while awaiting thelaboratory results,
Skin scrapings, fungal and bacterial culture, andhematology were all negative or unremarkable. Histo-logical examination of skin biopsies revealed nodularto diffuse pyogranulomatous dermatitis associatedwith collagen degeneration and dystrophic mineraliza-tion (Figures 3 and 4). Epidermal changes varied fromirregular hyperplasia to erosion and ulceration.
Figure 4. Skin biopsy. Amorphous masses of mineral sur-rounded by histiocytes, lymphocytes, plasma cells, neutro-phils, and a multinucleated histocytic giant cell (HPS stain).
The dog was presented for reevaluation 14 dayslater. No improvement was seen following the anti-biotic therapy and application of the Elizabethan col-lar. Galactostasis was no longer present. The ownerwas questioned concerning the dog's possible exposureto calcium-containing substances. Interestingly, theowner was in the landscaping business and frequentlycarried open bags of bone meal in the back of hertruck. The dog could have been in contact with thissubstance on different occasions.
Based on the history of exposure to calcium, thecontact-like distribution of the dermatitis, and thedermatohistopathological findings, a presumptivediagnosis of calcinosis cutis secondary to contact withbone meal was made. The owner was told to preventfurther exposure of her dog to this substance. Ten daysafter the reevaluation, the skin lesions began toimprove. Six weeks later the dermatitis had completelydisappeared. The dog has remained normal for theensuing five months.
Calcinosis cutis has frequently been reported in dogsin association with naturally occurring or iatrogenichyperglucocorticoidism (1). The lesions in this dog,however, were not associated with glucocorticoidexcess. The dog never manifested other signs of hyper-glucocorticoidism, and had not received corticosteroidsprior to the dermatosis.
There have been several reports of calcinosis cutisdue to percutaneous penetration of CaCl2 in humanbeings secondary to contact with dry CaCl2 or strongsolutions of CaCl2 (2,3,5). In some cases, affectedskin had previously been slightly abraded. However,in many instances, affected skin had previously beennormal. The best-documented example is calciumdeposition following electroencephalography. The elec-trode paste used is often rich in calcium chloride, caus-ing local hypercalcemia (3,5).
A presumptive diagnosis of calcinosis cutissecondary to contact with bone meal was made
Accidental exposure of the skin of a dog to a com-mercial hygroscopic landscaping product (77-80%CaCl2), with resultant calcinosis cutis, was reportedrecently (4). Lesions involved glabrous areas of theskin, and were grossly and histologically similar to thelesions in the dog reported here. In addition, theauthors were able to reproduce the lesion in fiveclinically normal dogs by topical application of thelandscaping product. Although we made no attemptto reproduce skin lesions in normal dogs with bonemeal product reported herein, the history of exposure,the distribution of the lesions, and the disappearanceof lesions after avoidance of the suspected causativeagent strongly suggest a cause and effect relationship.Although the precise mechanisms of aberrant min-
eralization in these cases remain unclear, the findingsare consistent with percutaneous, and possibly trans-follicular, penetration of calcium salts into dermal con-nective tissue. An abraded skin surface might havebeen a predisposing factor in the dog reported here,as the owner related that the dog frequently ranthrough fields of grass and sumac bushes.To our knowledge, this is only the second report of
calcinosis cutis secondary to percutaneous penetrationof calcium salts in dogs. This is probably a rare con-dition. However, it could easily go unrecognized orclassified as an idiopathic calcinosis cutis. Whencalcinosis cutis is diagnosed in thinly-haired, contactareas of the skin, the possibility of exposure tocalcium-containing substances should be considered.
Can Vet J Volume 30, January 198958

References1. Muller GH, Kirk KW, Scott DW. Small Animal Dermatology.
3rd ed. Philadelphia: WB Saunders, 1983: 779-780.2. Moschella SL, Hurley HJ. Dermatology. Vol 2. 2nd ed.
Philadelphia: WB Saunders, 1985: 1490-1492.3. Demis DJ. Clinical Dermatology. Vol 2, Unit 12-12. 1987: 1-17.
4. Schick MP, Schick RO, Richardson JA. Calcinosis cutis second-ary to percutaneous penetration of calcium chloride in dogs.J Am Vet Med Assoc 1987; 190: 207-211.
5. Wiley HE III, Eaglestein WE. Calcinosis cutis in children follow-ing electroencephalography. J Am Med Assoc 1979: 242: 455-456.
Can Vet J Volume 30, January 1989 59
Related Documents