CHAPTER 16 Periodontal Emergencies Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

C HAPTER 16 Periodontal Emergencies Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
Dec 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CHAPTER 16
Periodontal Emergencies
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

INTRODUCTION
Knowledge of emergency situations and treatment assists patients in receiving appropriate care.
To identify these conditions, the dental hygienist must take a careful medical and dental history before beginning any procedure.
2
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TYPES OF ABSCESSES
The three basic types of abscesses are: Periodontal Gingival Periapical
Each type may be acute or chronic. Combination abscesses can also develop.
3
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PERIODONTAL ABSCESSES
A periodontal abscess is a site of inflammation of microbial origin that is associated with accumulations of suppuration or purulence (pus) in the periodontal tissues. The pus is often referred to as exudate or
purulent exudate. Such infections have rapid onset and are
usually characterized by pain, swelling, and discomfort.
The presence of a periodontal abscess does not necessarily mean that the tooth must be extracted.
4
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ACUTE PERIODONTAL ABSCESSES
Acute periodontal abscesses are associated with preexisting periodontal disease.
An acute periodontal abscess forms when a periodontal pocket becomes occluded. An inflammatory reaction then occurs.
The abscess appears as a shiny, red, raised, rounded mass on the gingiva or mucosa.
If the abscess can drain through a sulcus or fistula (opening in the tissue), then the infection stabilizes and is considered to be in a chronic state. 5
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ACUTE PERIODONTAL ABSCESSES (CONT.)
Acute abscesses are demonstrated in the following figure.
6
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ACUTE PERIODONTAL ABSCESSES (CONT.)
The most common symptom is pain. Other symptoms include:
Swelling Deep red to blue discoloration of the tissue Tooth sensitivity to pressure Tooth mobility The tooth feels “high” to the patient
The tooth may become slightly extruded as a result of swelling of the periodontal ligament.
7
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ACUTE PERIODONTAL ABSCESSES (CONT.)
Radiographic images may be used to locate an area of bone loss, which may be the origin of the abscess.
The opening of a fistula or sinus along the lateral aspect of the tooth in the adult dentition is usually indicative of a periodontal abscess. However, the opening may be the result of a
periapical abscess. In primary teeth, a sinus opening on the
lateral aspect of the tooth is usually associated with a periapical abscess. 8
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT CONSIDERATIONS
Treatment of acute periodontal abscesses consists of drainage and the use of antibiotics or antimicrobial agents.
Teeth in the affected area are scaled and root planed, and curettage is performed to remove granulation tissue.
9
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT CONSIDERATIONS (CONT.)
Postoperative instructions include: Resting Drinking fluids Using a warm salt water rinse (1 tsp. of salt in a
glass of warm water) to help reduce swelling Follow-up treatment may involve periodontal
surgery to eliminate the problem.
10
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CHRONIC PERIODONTAL ABSCESSES
Chronic periodontal abscesses resemble acute periodontal abscesses. They may be indistinguishable.
Chronic abscesses are usually painless; they drain into the oral cavity, either through the opening of the pocket or through a sinus tract.
The associated gingival tissue is red and swollen.
As long as the chronic abscess is draining, it is unlikely to be painful; therefore patients tolerate the condition or do not realize that it is occurring.
11
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CHRONIC PERIODONTAL ABSCESSES (CONT.)
A chronic abscess with a sinus tract through the tissue is presented in the following figure.
12
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT CONSIDERATIONS
Treatment of a chronic periodontal abscess is similar to the treatment of an acute periodontal abscess.
Affected teeth are scaled and root planed, curettage is performed, local antimicrobial therapy may be administered, and the patient is scheduled for follow-up care to evaluate the need for further periodontal treatment.
13
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

GINGIVAL ABSCESSES
Gingival abscesses often occur in disease-free areas. They may be related to forceful inclusion of some
foreign object into the area. Most frequently, gingival abscesses are found
on the marginal gingiva and are not associated with any abnormality of the deeper tissues.
14
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

GINGIVAL ABSCESSES (CONT.)
A gingival abscess is demonstrated in the following figure.
15
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

GINGIVAL ABSCESSES (CONT.)
The gingival abscess typically appears as a shiny, raised area of acute inflammation that may be painful.
The swelling is usually confined to the marginal gingiva.
A suppurative lesion is usually evident on the gingival tissues.
16
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
GINGIVAL ABSCESSES (CONT.)
Treatment Considerations The gingival abscess must be drained and
irrigated. The dentist or periodontist usually performs the
drainage and irrigation procedures. Warm salt water rinses are recommended for
postoperative therapy. After treatment of the abscess, scaling and
root planing of the teeth is performed. If the reduced lesion is still large, then it may
require excision.17
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ENDODONTIC ABSCESSES
An endodontic abscess is sometimes difficult to distinguish from an acute periodontal abscess. The facial pain and tenderness to the tooth are
similar. An endodontic abscess is the result of
infection through caries, traumatic fracture of the tooth, or trauma from a dental procedure.
In addition, pulpal infection to a tooth can spread to the pulp from an adjacent infected tooth through the lateral canals.
18
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ENDODONTIC ABSCESSES (CONT.)
The endodontic abscess often appears on radiographic images as a rounded radiolucency at the apex of the tooth. In this case, the endodontic abscess may be
correctly termed a periapical abscess. Some abscesses drain through a sinus duct
through the cortical bone, and some drain through the periodontal ligament, making them less identifiable on radiographic images.
Draining endodontic abscesses can resemble acute periodontal abscesses; the symptoms are similar.
19
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ENDODONTIC ABSCESSES (CONT.)
To determine whether an abscess is periodontal or endodontic, consider the following: Approximately 85% of the tooth pain is pulpal
and 15% is periodontal. Many endodontically abscessed teeth test
nonvital. Periapical pain is characterized as sharp, severe,
intermittent, and difficult to localize. Periodontal pain is usually constant, localized,
and less severe.
20
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ENDODONTIC ABSCESSES (CONT.)
Treatment Considerations Treatment of endodontic abscesses requires
endodontic therapy or the extraction of the tooth.
It is extremely important that patients with endodontic lesions receive treatment.
Untreated endodontic abscesses can lead to abscesses of the brain or fasciitis of the neck or chest wall.
These extensions of infection into deeper tissues can be life threatening.
21
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ENDODONTIC ABSCESSES (CONT.)
A treated endodontic lesion is presented in the following figure.
22
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

COMBINATION ABSCESSES
When an abscess spreads from the pulp to the periodontium or from the periodontal pocket to the pulp, it is considered a combination periapical and periodontal abscess.
Combination abscesses have some combination of the signs and symptoms of both types of abscesses and may be difficult to diagnose. Symptoms can be intermittent, causing patients
to delay treatment. These abscesses require extensive therapy
and often result in tooth loss. 23
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

COMBINATION ABSCESSES (CONT.)
The radiographic appearance of a combination abscess is presented in the following figure.
24
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PERICORONITIS Pericoronitis is an abscess associated with
a partially or fully erupted tooth that is covered completely or partially by a flap of tissue called an operculum.
The most commonly affected tooth is the mandibular third molar. Maxillary third molars and other teeth most
distal in the arch are also associated with the condition.
Pericoronitis is generally observed in young adults.
25
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PERICORONITIS (CONT.)
The symptoms of acute pericoronitis are swelling of the operculum and/or other associated gingiva, redness, and extreme pain.
The tissue may be so swollen that it interferes with mastication.
Trismus (muscle spasm) may also occur. The patient may have a fever. Purulent exudate occurs in approximately
one half of the patients with pericoronitis.
26
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PERICORONITIS (CONT.)
Treatment Considerations Initial therapy involves débridement of the
infected area and flushing it with warm water or chlorhexidine.
The patient is instructed to rest, use warm salt water rinses, and drink fluids to avoid dehydration.
Antibiotics may be prescribed if the patient has a fever.
After the acute condition has resolved, the operculum can be surgically removed, if necessary. Extraction of the third molar, which is often only
partially erupted, may be required.
27
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

NECROTIZING ULCERATIVE GINGIVITIS
Necrotizing ulcerative gingivitis (NUG) is an opportunistic infection of the gingiva that is associated with stress, lifestyle, and some chronic illnesses and conditions.
NUG is primarily observed in young adults who are under severe stress and individuals who are immunocompromised.
NUG is not communicable.
28
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

NECROTIZING ULCERATIVE GINGIVITIS (CONT.)
NUG is a recurring disease with a complex bacteriologic structure that consists of a large proportion of spirochetes and gram-negative organisms.
The bacteria invade the tissue and cause the characteristic pseudomembranous appearance of the disease.
Recurrent NUG can result in attachment loss. When NUG reoccurs, the more appropriate
name for the disease is necrotizing ulcerative periodontitis. 29
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CHARACTERISTICS OF NECROTIZING ULCERATIVE GINGIVITIS
Specific clinical characteristics that distinguish NUG from other forms of acute oral infections include the following: Involved papillary gingiva becomes necrotic and
appears cratered or “punched out.” Surface of the gingiva has a pseudomembranous
coating made up of necrotic bacteria and tissue. Gingiva is reddened and painful. Lesions may be localized or generalized. Patients have a strong and offensive breath odor,
described as fetid (fetor oris).
30
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
CHARACTERISTICS OF NECROTIZING ULCERATIVE GINGIVITIS (CONT.)
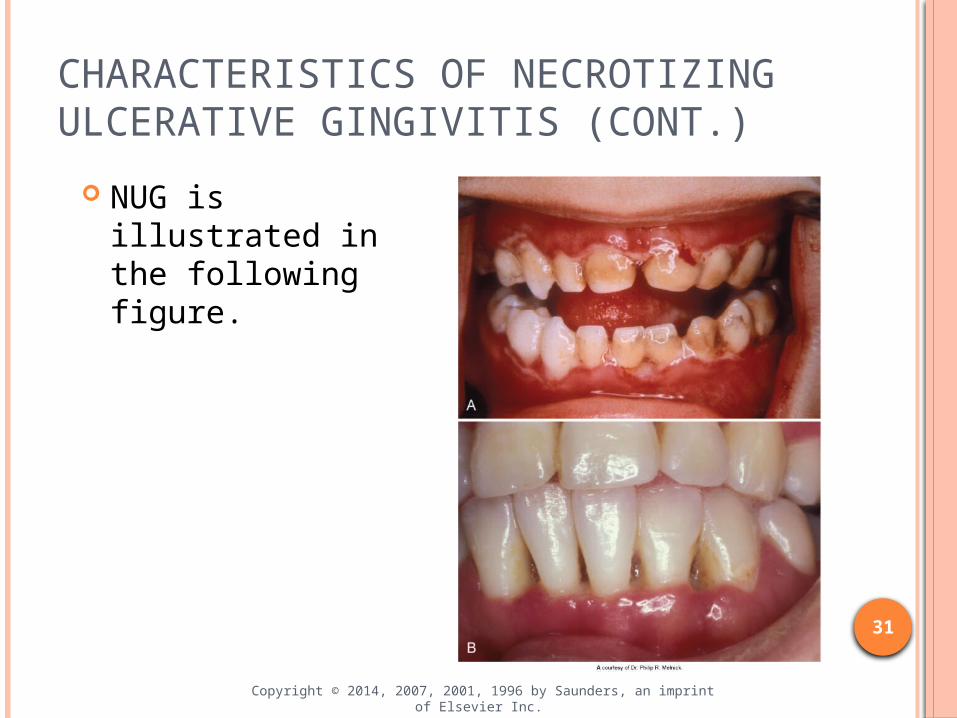
NUG is illustrated in the following figure.
31
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT CONSIDERATIONS
Treatment for NUG requires the following approaches: Alleviation of acute inflammation and treatment
of chronic conditions. Alleviation of systemic symptoms such as fever
and malaise. Correction of conditions that contribute to the
initiation or progress of the disease. The recommended treatment sequence
requires several visits.
32
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT CONSIDERATIONS (CONT.)
The first visit requires a limited amount of débridement, only what the patient can tolerate. The use of ultrasonic instruments and topical or
local anesthetics may be helpful. Subgingival scaling and root planing are
contraindicated; these procedures increase the possibility of extending the infection into deeper tissues and causing bacteremia.
The dentist may prescribe systemic antibiotics if the patient has a fever or lymphadenopathy. 33
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT CONSIDERATIONS (CONT.)
The second treatment visit should occur 1 or 2 days later. Subgingival scaling may be performed if the
patient’s sensitivity permits. The third visit should occur 3 to 5 days after
the first visit to complete débridement. The patient is instructed to rest at home,
drink plenty of fluids, avoid spicy foods, rinse with warm salt water as needed, and refrain from smoking.
After emergency treatment is completed, the dentist or periodontist should evaluate the patient.
34
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ACUTE HERPETIC GINGIVOSTOMATITIS
Acute herpetic gingivostomatitis is the oral manifestation of primary infection with the herpes virus, usually herpes simplex virus I (HSVI).
Acute herpetic gingivostomatitis is now more commonly found in young adults, possibly representing primary infection with genital herpes virus, herpes simplex virus II (HSVII).
This disease is highly infectious. Dental and dental hygiene care should be
postponed until the condition has subsided.35
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ACUTE HERPETIC GINGIVOSTOMATITIS (CONT.)
Acute herpetic gingivostomatitis is commonly associated with symptoms such as fever, malaise, headache, irritability, and lymphadenopathy.
Oral lesions begin as small yellow vesicles that coalesce to form larger round ulcers with gray centers and bright red borders. They may be found on any of the oral mucous
membranes. The patient may have serious, even extreme,
pain. 36
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ACUTE HERPETIC GINGIVOSTOMATITIS (CONT.)
After the primary infection has occurred, the herpes virus travels through the nerves to reside in neuronal ganglia.
There, the virus can become active again and recur most commonly in the form of herpes labialis.
These secondary lesions occur in approximately one third of the world’s population and are triggered by sunlight, trauma, fever, or stress.
37
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ACUTE HERPETIC GINGIVOSTOMATITIS (CONT.)
The following figure demonstrates an example of primary herpetic gingivostomatitis.
38
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT CONSIDERATIONS
Treatment of acute herpetic gingivostomatitis is supportive. The disease runs its course in 7 to 10 days.
The patient should maintain an adequate diet, perform oral hygiene as often as possible, and, if necessary, use over-the-counter topical anesthetics to control the discomfort. For controlled delivery, topical anesthetics can
be swabbed on the lesions rather than rinsed or sprayed.
Chlorhexidine rinses may also be helpful. 39
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TREATMENT CONSIDERATIONS (CONT.)
Herpetic whitlow is the term for the herpetic lesion that occurs most often on the fingers of the dentist or dental hygienist where the inoculation of the herpes virus occurred.
Even if the hygienist has been previously exposed to the herpes virus, the possibility of initiating herpetic whitlow can occur from an inadvertent puncture.
40
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
Related Documents











