CHAPTER 12 Plaque Biofilm and Disease Control for the Periodontal Patient Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

C HAPTER 12 Plaque Biofilm and Disease Control for the Periodontal Patient Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CHAPTER 12
Plaque Biofilm and Disease Controlfor the Periodontal Patient
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

INTRODUCTION
Incorporating individualized plaque control education into periodontal therapy is essential because dental plaque biofilm is the causative agent of gingival and periodontal diseases.
2
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PLAQUE AS A BIOFILMAND AN ETIOLOGIC AGENT
A cause-and-effect relationship exists between bacterial plaque biofilm and gingivitis.
As it ages, supragingival plaque becomes dominated by gram-negative microbial species, which is responsible for the development of a subgingival flora associated with periodontal disease.
Adequate supragingival plaque control when incorporated into periodontal maintenance programs limits periodontal attachment loss in adults. 3
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PLAQUE AS A BIOFILMAND AN ETIOLOGIC AGENT (CONT.)
The following figure demonstrates the effects of plaque accumulation related to gingival inflammation.
4
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
PLAQUE AS A BIOFILMAND AN ETIOLOGIC AGENT (CONT.)
Mature plaque biofilm is a heterogeneous mass with open, fluid-filled channels used for moving nutrients and waste products.
The colonies of bacteria making up the plaque mass facilitate each other’s growth, with the host providing an essential source of nutrients.
Plaque bacteria are a complex group of species that adhere to tooth surfaces in such a way as to limit the diffusion of antimicrobial substances.
5
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

GOALS OF PLAQUE BIOFILM CONTROL FOR PATIENTS WITH PERIODONTAL DISEASE
The goals of plaque biofilm control include: Patient motivation Patient responsibility Managing the complexity of a plaque control
routine Caries control Maintenance of gingival and periodontal health
6
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PATIENT MOTIVATION
Most patients with periodontal disease have poor plaque control.
When teaching proper plaque control, incorporating behavioral techniques is more successful than brushing and flossing instructions alone.
Developing a professional trust and partnership with the patient over time can help facilitate patient adoption of difficult behavioral changes.
7
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PATIENT RESPONSIBILITY
The daily plaque biofilm control program is the responsibility of the patient.
The dental hygienist’s responsibility is to individualize the plaque control program, modify it over time, and present it in such a way that the patient can assist in the long-range outcome of therapy.
8
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

COMPLEXITY OF PLAQUE BIOFILMCONTROL FOR THE PATIENTWITH PERIODONTAL DISEASE
Plaque control for the patient with periodontal disease usually involves far more than simple toothbrushing and dental flossing, as demonstrated in the following figure.
9
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
COMPLEXITY OF PLAQUE BIOFILMCONTROL FOR THE PATIENTWITH PERIODONTAL DISEASE (CONT.)
Significant areas of attachment loss are often associated with disease and can occur as a result of surgery to reduce periodontal pocket depths.
Attachment loss results in the exposure of root anatomy that patients must learn to clean.
10
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

COMPLEXITY OF PLAQUE BIOFILMCONTROL FOR THE PATIENTWITH PERIODONTAL DISEASE (CONT.)
A range of aids, including chemotherapeutic agents, are available to help a patient with plaque control.
Some aids work better for some people than others, some require more dexterity, and some require more patience.
For certain patients, multiple sessions are needed to master the cleaning techniques for their unique periodontal architecture.
11
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CARIES CONTROL
Providing proper oral hygiene instruction for patients with periodontal disease includes the prevention of dental caries.
Teeth that could be maintained for years by treating the periodontal disease can be lost in weeks or months as a result of caries on the root surfaces or in furcation areas.
12
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CARIES CONTROL (CONT.)
Root caries is a great threat to survival of the teeth when attachment loss and recession expose the roots to the oral environment as demonstrated in the following figure.
13
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

MAINTENANCE OF GINGIVALAND PERIODONTAL HEALTH
Gingival and periodontal health, once restored, cannot be maintained without the active participation and cooperation of the patient in performing daily plaque removal.
Satisfactory treatment outcomes are more likely when patients adopt adequate personal plaque control regimens.
14
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
MECHANICAL PLAQUE REMOVAL
Standard mechanical plaque removal includes a toothbrush, augmented by a device or devices that permit access to interproximal and other
hard-to-reach areas.
15
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TOOTHBRUSHING
The toothbrush is the most widely accepted tool for cleaning the teeth.
Today’s toothbrush is the modern version of the African twig or chew stick, which was a frayed branch used for mechanical cleansing.
Evidence has shown that toothbrushes existed in China as early as 1000 BCE, but the device did not receive wide distribution until the late eighteenth century.
16
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TOOTHBRUSHING (CONT.)
The first brushes were made of hog bristle, often with bone or ivory handles.
The Victorians created elaborate handles, including many made of silver. Consequently, early toothbrushes were
expensive and were often used by the entire family.
In the 1930s, when nylon-bristle brushes were introduced, toothbrushes became affordable for everyone.
17
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TOOTHBRUSHING (CONT.)
Examples of toothbrushes from the late nineteenth and twentieth centuries are demonstrated in the following figure.
18
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TOOTHBRUSHING (CONT.)
Dr. Charles C. Bass proposed the optimal characteristics of toothbrushes.
He studied bristle stiffness, scratching of the gingiva, gingival puncturing, bristle trim, and the presentation of bristles on the brush head.
19
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TOOTHBRUSHING (CONT.)
Since Bass’s time, many toothbrushes have been marketed to the public.
Complex bristle designs and many varieties of handles are available.
One toothbrush may work better than another in the hands of a particular patient, but no evidence demonstrates that one toothbrush design is superior to another.
20
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TOOTHBRUSHING (CONT.)
An example of an unusual toothbrush design with two brush heads in presented in the following figure.
21
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TOOTHBRUSHING METHODS
Several specific toothbrushing techniques include: Scrub Roll Charters Stillman Bass Powered
22
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
SCRUB
Scrub technique: As the simplest brushing technique, the scrub
method consists of merely placing the bristles on the teeth and moving them back and forth or scrubbing.
Nearly anyone, including children, can become adept with the scrub technique.
Extremely vigorous scrubbing, especially with a stiff-bristled brush, can lead to gingival trauma and recession.
23
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ROLL
Steps of the roll technique: Bristles are placed on the gingiva, and then the
handle of the toothbrush is turned to stroke the bristles along the sides of the teeth.
This rolling action is repeated several times in each location, moving around the arches, until all the teeth are brushed on the buccal and lingual surfaces.
The rolling strokes must be performed slowly to ensure that the gingival one third of the teeth are adequately cleaned.
24
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CHARTERS
Steps of the Charters technique: The brush is placed at a 45-degree angle to the
tooth. Bristle ends are pointed away from the gingiva
toward the interproximal surfaces of the teeth, resting on the gingiva.
With a slight rotary motion, pressure is applied to ensure that the bristles go between the teeth.
The brush is lifted and replaced in the same spot, repeating the rotary motion three or four times.
The bristles are also pressed into the occlusal surfaces with a slight rotary motion.
25
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
STILLMAN
Steps of the Stillman technique: Bristles are placed pointing apically but not at
right angles to the gingiva to minimize puncture. Pressure is placed on the bristles, causing them
to flex and the tissue to blanch. This stroke is repeated for all teeth in all areas of
the mouth.The brush is rinsed several times with a salt water and sodium bicarbonate solution.
26
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BASS
Steps of the Bass technique: Bristles of a soft, multitufted toothbrush are
placed at a 45-degree angle to the long axis of the teeth.
The vibratory motion is used to force the bristles into the sulci and between the teeth.
The lingual surfaces of the anterior teeth can be brushed with the heel of the toothbrush and all other areas with the length of the brush head.
The occlusal surfaces are brushed with controlled back-and-forth motions.
27
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BASS (CONT.)
The Bass technique is demonstrated in the following figure.
28
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
POWERED TOOTHBRUSHING
Many people prefer a powered toothbrush, particularly if they have any dexterity problems.
Powered toothbrushes have different types of actions.
The head portion of the brush can be vibrating, oscillating, rotary, or counter rotary, or it can have a sonic vibration feature. All powered toothbrushes have been shown to be
effective when used correctly. 29
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
POWERED TOOTHBRUSHING (CONT.)
Electric toothbrushes with sonic components cause hydrodynamic shearing forces of water that increase penetration of plaque removal onto the proximal surfaces. This type of brush is not a substitute for other
interproximal cleaning devices.
30
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

POWERED TOOTHBRUSHING (CONT.)
The following figure demonstrates the placement of the powered toothbrush head on the tooth surface.
31
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
POWERED TOOTHBRUSHING (CONT.) A rotary electric toothbrush designed
specifically for access to proximal areas is also available.
It has shaped tips and can be applied to both the interproximal surfaces when space is sufficient and the gingival margin.
These brush tips have been shown to be as effective in plaque removal and gingivitis reduction as conventional toothbrushing, flossing, and toothpick use for periodontal maintenance.
32
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

RECOMMENDATIONS
Regular toothbrushing, whether with a manual or powered brush, is essential for patients.
The Bass technique is probably most accepted by the dental profession. The vibratory motion of the bristles into the
sulcus is simple to perform and has the greatest cleaning potential at the gingival margin of the teeth.
The technique is adaptable enough to remove plaque biofilm from the complex architecture of severely periodontally damaged dentitions.
33
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
RECOMMENDATIONS (CONT.)
The best brushing technique for each patient must be created with the knowledge of what works with the difficulties the individual patient faces.
Powered toothbrushes are useful and good substitutes for patients who have difficulty brushing or those who simply prefer powered toothbrushes. Evidence indicates modest benefits in plaque
and gingivitis reductions with oscillating-rotating powered brushes. 34
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
INTERPROXIMAL CLEANINGWITH MECHANICAL AIDS
In most cases, toothbrushes do not adequately clean interproximal surfaces.
Interdental cleaning with at least one additional device is necessary for thorough plaque removal.
Interdental plaque biofilm control may be accomplished with several different aids including: Dental floss Interdental brushes Toothpicks
35
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
DENTAL FLOSS
Dental floss is available in a variety of sizes and thicknesses: Waxed, unwaxed, round, flat, thick, thin, tape,
shred-resistant, and fuzzy versions, just to name a few
Floss will clean the interproximal surfaces of the teeth, extending under the gingival margin, where a toothbrush cannot reach.
However, dental floss is likely to miss plaque in root surface grooves and cannot adequately clean furcations.
36
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

DENTAL FLOSS (CONT.)
Flossing Steps Use a piece of floss approximately 18 inches
long. Grasp it firmly with both hands with
approximately 1 inch held between the thumbs and the forefingers.
Insert the floss into the proximal space by working it back and forth, slipping it under the papilla and wrapping it around the tooth.
Use an up-and-down stroke to clean the tooth surface.
Repeat around the mouth, moving along the piece of floss to ensure that a fresh length of the strand can be used to clean the next surface.
37
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

DENTAL FLOSS (CONT.)
Correct flossing is demonstrated in the following figure.
38
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

FLOSS THREADERS
Floss threading is accomplished with a needlelike device called a floss threader or a bridge threader.
The floss is threaded through the eye of the device and then inserted under the contact area of the bridge.
The floss is used to clean around the abutment teeth with an up-and-down motion and under the pontic with a back-and-forth motion.
When flossing is completed, the floss is pulled out to the side. 39
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

FLOSS TOOLS OR AIDS
Many patients have a difficult time learning to floss correctly and give up.
In many cases, the hardest part is holding and manipulating the floss.
Floss tools can help with this problem. Two types of tools are available:
Reusable tools that require the patient to wrap the floss around the device
Single-use disposable tools with prestrung floss
40
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

FLOSS TOOLS OR AIDS (CONT.)
Reusable floss tools have a C- or U-shaped working end.
Floss is stretched across the head of the device. C-shaped ends work better in the anterior areas. U-shaped ends work better in the posterior
areas. The floss is inserted interproximally by
moving it back and forth between the contact areas of the teeth.
The cleaning procedure is the same as with finger flossing, wrapping the floss around the tooth and moving it up and down to clean to the tooth surfaces.
41
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
FLOSS TOOLS OR AIDS (CONT.)
Disposable floss tools eliminate the problems of threading and winding floss onto a handle.
The floss is stretched on the working end of the tool in the manufacturing process.
Disposable floss tools are convenient when traveling and for children to use.
42
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
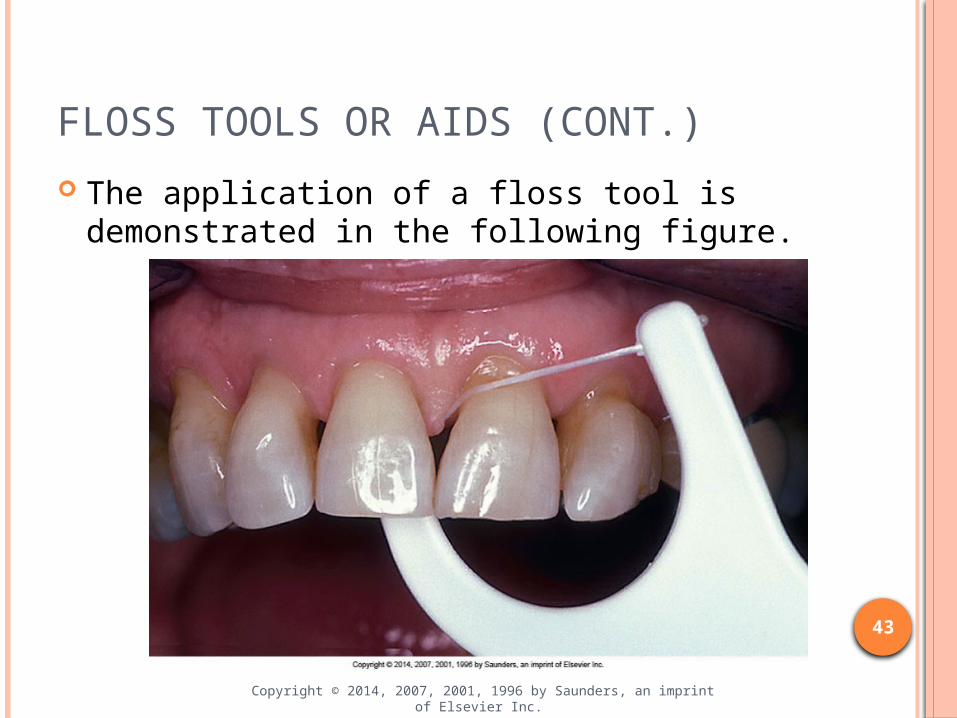
FLOSS TOOLS OR AIDS (CONT.)
The application of a floss tool is demonstrated in the following figure.
43
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
OTHER FLOSSING MATERIALS
Besides dental floss, other materials can be used for flossing. Thicker materials, such as yarn or gauze, can be
used. These materials can be used like dental floss to
clean large interproximal spaces and around abutment teeth.
A number of automatic flossing devices are now available. These have prestrung floss that vibrates or a
wand of flossing material that penetrates between the teeth and vibrates or spins to remove plaque. 44
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
INTERDENTAL BRUSHES
Interdental brushes facilitate the cleaning of proximal root surfaces. They provide improved access into the
developmental grooves and furcations. Interdental brushes are useful for patients
with periodontal disease who have attachment loss, long-exposed root surfaces, and complex root architecture to clean.
45
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

INTERDENTAL BRUSHES (CONT.)
Two types of interdental brush systems are available: A reusable handle with a disposable brush tip An all-in-one disposable brush
Both types are used with an in-and-out brushing stroke from both the buccal and lingual aspects.
Furcation areas may also be large and accessible enough to permit brushing with this device.
46
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

INTERDENTAL BRUSHES (CONT.)
The following figure demonstrates the adaptation of an interproximal brush to a large embrasure space.
47
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TOOTHPICKS
Toothpicks are a popular interdental cleaning aid but are less effective than floss for interproximal cleaning.
Toothpick tips mounted on a handle are more adaptable. They can be single or double ended.
The tip is placed at the gingival margin and used to trace around the necks of the teeth.
The handle also permits the tip to slip into proximal spaces, furcation areas, subgingival root surfaces, and developmental grooves to rub off biofilm.
48
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TOOTHPICKS (CONT.)
Using a toothpick technique to remove plaque biofilm is demonstrated in the following figure.
49
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TOOTHPICKS (CONT.)
Specially designed triangular toothpicks made of a soft wood, such as balsa, are also available.
These can be placed with the base of the triangle on the gingiva and pushed in and out of large proximal spaces.
They provide good plaque removal on the buccal surfaces but are difficult to apply to the lingual surfaces and the more posterior teeth.
50
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PLASTIC PICKS
Plastic toothpick-like devices are used similar to toothpicks.
They can be rinsed and reused rather than thrown away like wooden picks.
51
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
RUBBER-TIP STIMULATORS
A rubber-tip stimulator is a device with a conical tip made of firm rubber or plastic.
The tip is placed proximally and worked in a small circular motion.
Interdental spaces should be cleaned from both the buccal and lingual surfaces.
In addition, the rubber tip may be adapted and applied to the gingival margins of the teeth and traced along the gumline like a toothpick in a holder.
52
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

RUBBER-TIP STIMULATORS (CONT.)
Application of the rubber-tip stimulator is illustrated in the following figure.
53
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
RECOMMENDATIONS
Interproximal cleaning may require some experimentation to find the best tool or combination of tools.
The importance of mechanical plaque control is to Individualizing the recommendations to meet the needs and abilities of each patient with periodontal disease is very important in mechanical plaque control.
Individualization, working to find the right tools that are easy to use, and reinforcement are the keys to compliance and success with mechanical plaque control. 54
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

IRRIGATION
Supragingival irrigation devices force water between the teeth with a single or multiple jets of pulsed beads of water.
Although the mass of plaque biofilm may be minimally affected, its toxicity may be altered.
For supragingival irrigation, the tip is directed between the teeth at right angles to the interdental papillae and held there for several seconds.
The tip is then moved along the gingival margin to the next proximal area.
The pressure setting on the irrigator may be gradually increased if the tissue condition permits.
55
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

IRRIGATION (CONT.)
Subgingival irrigation can be accomplished using a special soft rubber tip that permits the irrigant to be directed under the gingiva.
The tip is slipped under the gingiva in areas with deep pockets, and the irrigant is flushed into the pockets.
The pressure for the irrigation unit should be set on low.
This technique extends the cleansing action of irrigation beyond the generally accepted 3-mm depth reached with the standard technique.
56
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

RECOMMENDATIONS
Data suggest that supragingival oral irrigation reduces gingivitis and is an acceptable tool to be recommended. Oral irrigation is especially useful for patients
who cannot or will not adopt mechanical devices for interproximal cleaning.
57
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

RECOMMENDATIONS (CONT.)
Commonly used oral irrigation tips are illustrated in the following figure.
58
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CHEMICAL PLAQUE CONTROL
Chemical agents can assist in plaque control programs, but they are not a substitute for good mechanical oral hygiene practices.
A variety of over-the-counter and prescription agents are available for patients.
Some of these agents can provide significant advantages to patients with periodontal disease.
59
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CHEMICAL PLAQUE CONTROL (CONT.)
Chemical antiplaque agents should demonstrate the following properties: Antiplaque action
Bactericidal (causing cell death) Bacteriostatic (affecting the functioning
of the cells)
Substantivity Ability to adhere to structures in the
oral environment and be released slowly over time
60
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CHEMICAL PLAQUE CONTROL (CONT.)
Chemical antiplaque agents should demonstrate the following properties: (cont.) Low toxicity and nonirritating
Agents must be nontoxic to tissues, allowing them to extend their effects on the bacterial population without damaging host tissues.
Low permeability An effective antiplaque agent must
have low permeability to allow its retention in the oral cavity.
61
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CHLORHEXIDINE
The most effective antibacterial agent available today is chlorhexidine.
Chlorhexidine is sold by prescription as a mouthwash and contains: 0.12% chlorhexidine digluconate 11.6% alcohol
62
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CHLORHEXIDINE (CONT.)
A number of side effects have been reported with the use of chlorhexidine mouthwash: Dark brown staining of the teeth Increased supragingival calculus Reversible desquamation of the oral tissue Altered taste sensations
63
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
CHLORHEXIDINE (CONT.)
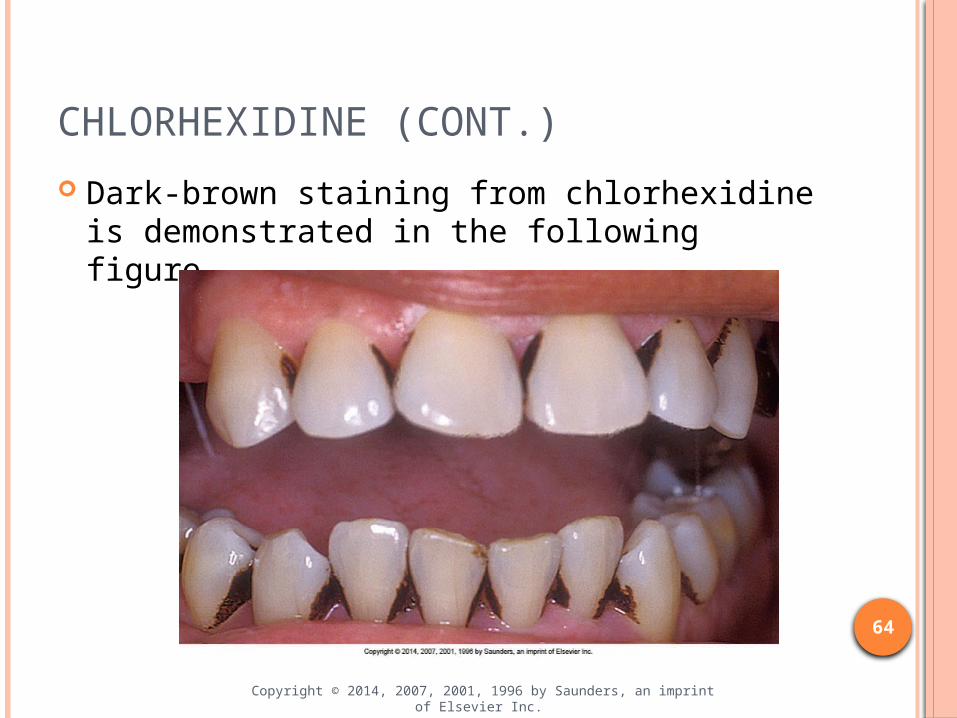
Dark-brown staining from chlorhexidine is demonstrated in the following figure.
64
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
CHLORHEXIDINE (CONT.)
The recommended use of chlorhexidine is full strength (0.12%), twice per day for 30 seconds using 15 ml of the rinse.
Chlorhexidine also reduces gingivitis when used in a 1:1 dilution with water (0.06%) in an oral irrigator for supragingival irrigation once per day.
Chlorhexidine has also been used for subgingival irrigation.
65
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ESSENTIAL-OIL MOUTHWASH (PHENOLIC COMPOUNDS)
Mouthwashes containing essential oils, thymol, eucalyptol, menthol, and methyl-salicylate have been shown to reduce plaque and gingivitis.
These products contain a substantial percentage of alcohol, up to 26.4%, have a strong flavor, and can cause staining.
They are available over the counter and are less costly than chlorhexidine mouthwash.
One product has been on the market for many years and carries the American Dental Association seal verifying that 6-month studies show that it is effective in reducing gingivitis.
66
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ESSENTIAL-OIL MOUTHWASH (PHENOLIC COMPOUNDS) (CONT.)
Triclosan, another phenolic compound, is available without a prescription in toothpaste formulations and has shown promising results as an antiplaque, anticalculus, and antigingivitis agent, especially when combined with other agents.
Triclosan toothpastes with either zinc citrate or a copolymer of methoxyethylene and maleic acid as the active agents have been shown to reduce plaque in numerous studies.
67
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

QUATERNARY AMMONIUM COMPOUNDS
Cetylpyridinium chloride, a quaternary ammonium compound, is the active ingredient in commonly available mouthwashes. Some preparations also contain domiphen
bromide. Their mechanism of action is probably the
ability to increase bacterial cell wall permeability, decrease cell metabolism, and reduce cell attachment to tooth surfaces.
Quaternary ammonium compounds have limited substantivity and are not accepted by the American Dental Association.
68
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
STANNOUS FLUORIDE
Stannous fluoride alters bacterial cell metabolism and cell adhesion properties in addition to reacting with tooth surfaces for caries prevention.
The usual strength for daily home use is 0.4% stannous fluoride delivered in gel or toothpaste form.
Some of the available products carry the American Dental Association seal for caries control. No available products have demonstrated
antigingivitis effects of sufficient quantity or duration to carry an additional seal for gingivitis effects.
69
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
STANNOUS FLUORIDE (CONT.)
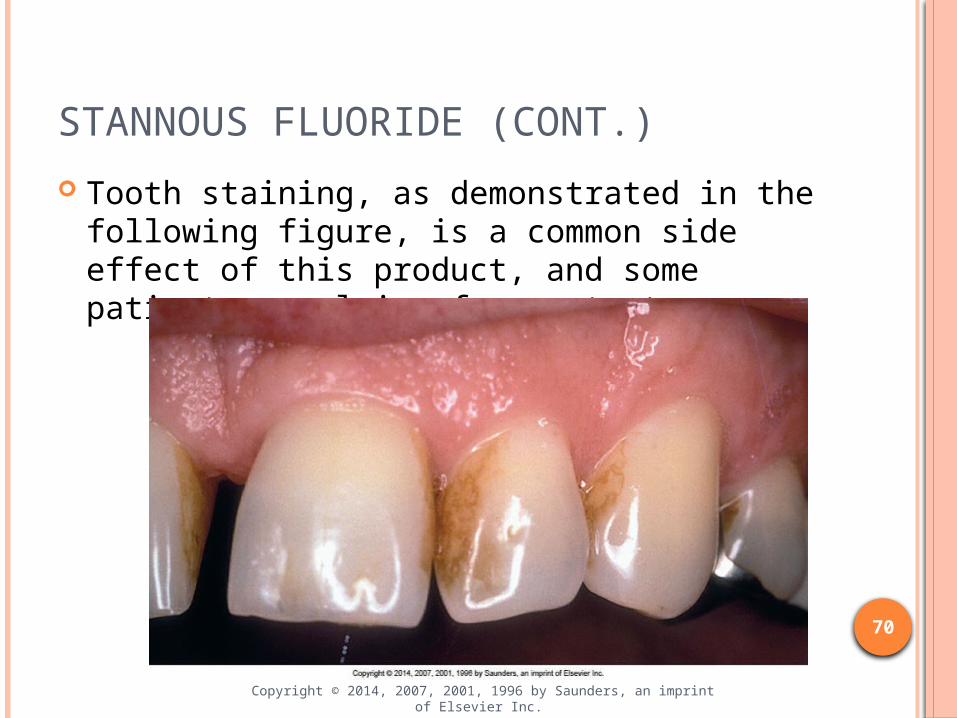
Tooth staining, as demonstrated in the following figure, is a common side effect of this product, and some patients complain of poor taste.
70
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
PROBLEM OF DELIVERY TO THE SITE OF DISEASE
The most meticulous supragingival plaque control does not remove plaque in pockets deeper than approximately 2 mm.
For this reason, lavage, the flushing or irrigating of periodontal pockets, especially with use of an antimicrobial agent, may be used.
Irrigating of periodontal pockets places the antimicrobial agent directly into the site of infection rather than limiting it to supragingival areas.
71
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

SUBGINGIVAL IRRIGATION
Subgingival irrigation can be delivered by powered oral irrigation devices and by blunt needles and syringe systems.
It can be an office procedure performed by the dental hygienist, an at-home procedure performed by the patient, or a combination of the two.
72
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
SUBGINGIVAL IRRIGATION (CONT.)
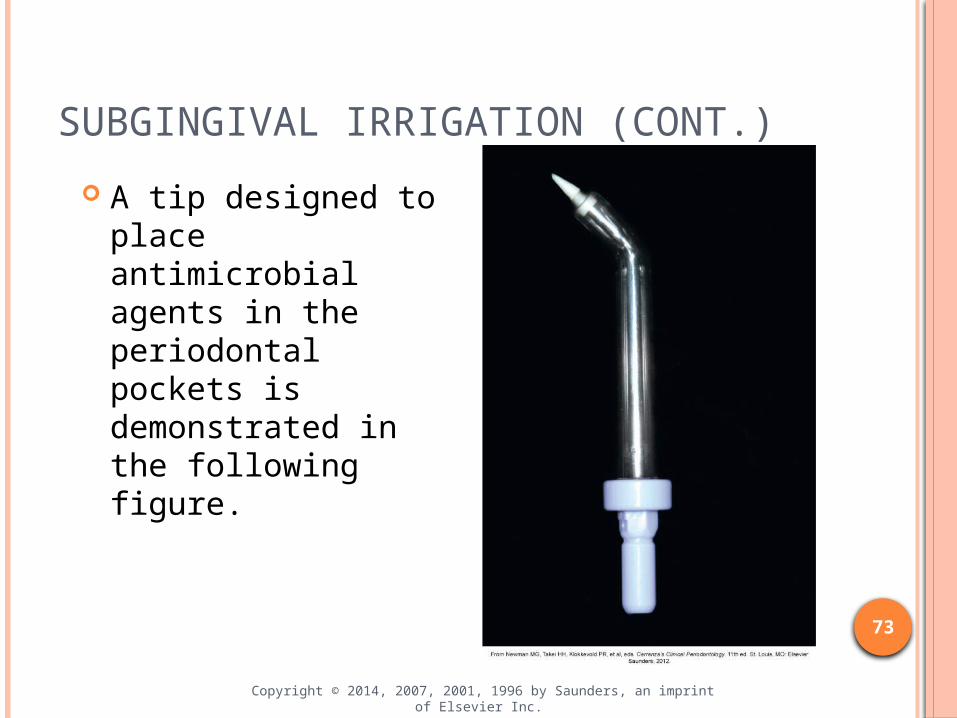
A tip designed to place antimicrobial agents in the periodontal pockets is demonstrated in the following figure.
73
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

OFFICE-APPLIED AGENTS
The dental hygienist can apply antimicrobial agents in the office during or after scaling and root planing procedures.
This procedure is commonly performed with a disposable syringe fitted with a blunt needle or an irrigating pump device with a thin cannula.
Running an antimicrobial irrigant through the ultrasonic tip during scaling can also accomplish the procedure.
Although this procedure is not harmful, its benefit is questionable. 74
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

HOME-APPLIED AGENTS
The use of home-applied agents using and a powered irrigating device on a daily basis has been shown to reduce the number of bleeding sites and the amount of gingivitis.
Evidence suggests that daily irrigation at home has a greater effect than antimicrobial treatment immediately after scaling.
75
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ANTICALCULUS AGENTS
Many toothpastes have active ingredients that are anticalculus agents, meaning they inhibit the formation of new supragingival calculus. These agents are commonly referred to as tartar-
control toothpastes. The active ingredients are soluble
pyrophosphates that inhibit amorphous calcium phosphate from crystallizing into hydroxyapatite, the most common crystal in calculus. Toothpastes containing zinc citrate also retard
calculus formation. 76
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ANTICALCULUS AGENTS (CONT.)
Although forming less supragingival calculus is desirable, the health benefits of anticalculus agents to patients with periodontal disease have not been established.
Plaque biofilm is the etiologic agent in periodontal diseases; supragingival calculus may only represent inconvenience.
77
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
PATIENT MOTIVATION
Changing behavior through patient motivation to institute and continue appropriate oral hygiene procedures is a major challenge in dental hygiene practice.
Knowledge and behavioral changes begin with education provided to patients by the dental hygienist.
The teaching of oral hygiene to achieve plaque biofilm control can be accomplished in a variety of ways.
78
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ROLE OF REINFORCEMENTAND LONG-TERM RAPPORT
The dental hygienist plays the key role in patient education.
The responsibility of the dental hygienist is to assess the individual patient and his or her needs and then educate, customize, motivate, and reinforce the plaque control process for successful periodontal therapy.
Patient education remains primarily a chairside activity in the profession and permits each patient to take responsibility for his or her own oral health.
79
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
Related Documents