Original Research Burn injury: economic and social impact on a family S.R. Mashreky a,b, *, A. Rahman a , S.M. Chowdhury a , S. Giashuddin a , L.Svanstro¨m b , T.F. Khan d , R. Cox c , F. Rahman a,b a Centre for Injury Prevention and Research, Bangladesh (CIPRB), Bangladesh b Department of Public Health Science, Karolinska Institutet, Sweden c The Alliance for Safe Children, Thailand d Centre for Medical Education, Bangladesh Received 9 January 2008; received in revised form 15 May 2008; accepted 18 June 2008 Available online 21 August 2008 KEYWORDS Burn; Social; Economic; Consequence; Hospital; Bangladesh Summary Objective: To assess the burden of burn injury in primary and second- ary hospitals in Bangladesh, and how these costs are reflected as social and economic burdens in the community. Study design: Cross-sectional study. Methods: A direct method was adopted to estimate the cost of burn injury, which involved interviewing patients or their attendants. Patient discharge records from 16 district hospitals and 45 Upazila (lower political units) health complexes were used as the main data sources in this study. Discharge records for December 2000 were reviewed for all types (injury and non-injury) of hospital admissions, and dis- charge records for January to December 2000 were reviewed for injury admissions. Hospital emergency departments’ records for December 2000 were reviewed to study emergency injury cases. Patient interviews were conducted between Febru- ary and March 2001 in selected primary and secondary hospitals in Bangladesh. Results: Seven hundred and ninety-one burn patients were admitted in 2000, which constituted 2% of total injury admissions. Hospital records of all types of admission in December 2000 revealed that burn patients represented 1% of the total admissions. The duration of hospital stay was significantly longer for patients with burn injury compared with patients with other injuries or illnesses. The longest hospital stay due to burn injury was 17.34 days, found for children aged 1e4 years. The average patient cost for burn injury was higher than that for other injuries and illnesses. Conclusion: Burn injuries were associated with a longer hospital stay compared with other injuries and illnesses. The management costs of burn injury, even using very incomplete data, were found to be very high in Bangladesh. To reduce this *Corresponding author. Centre for Injury Prevention and Research, Bangladesh (CIPRB), House 226, Lake Road 15, New DOHS Mohakhali, Dhaka 1206, Bangladesh. Tel.: þ880 2 886 1258; fax: þ880 2 886 1499. E-mail address: [email protected] (S.R. Mashreky). 0033-3506/$ - see front matter ª 2008 The Royal Institute of Public Health. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.puhe.2008.06.007 Public Health (2008) 122, 1418e1424 www.elsevierhealth.com/journals/pubh

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

*CorrespondMohakhali, Dha
E-mail addr
0033-3506/$ -doi:10.1016/j.p
Public Health (2008) 122, 1418e1424
www.elsevierhealth.com/journals/pubh
Original Research
Burn injury: economic and social impact ona family
S.R. Mashrekya,b,*, A. Rahmana, S.M. Chowdhurya, S. Giashuddina,L. Svanstromb, T.F. Khand, R. Coxc, F. Rahmana,b
aCentre for Injury Prevention and Research, Bangladesh (CIPRB), BangladeshbDepartment of Public Health Science, Karolinska Institutet, SwedencThe Alliance for Safe Children, ThailanddCentre for Medical Education, Bangladesh
Received 9 January 2008; received in revised form 15 May 2008; accepted 18 June 2008Available online 21 August 2008
KEYWORDSBurn;Social;Economic;Consequence;Hospital;Bangladesh
ing author. Centre forka 1206, Bangladesh. Tess: [email protected]
see front matter ª 200uhe.2008.06.007
Summary Objective: To assess the burden of burn injury in primary and second-ary hospitals in Bangladesh, and how these costs are reflected as social andeconomic burdens in the community.Study design: Cross-sectional study.Methods: A direct method was adopted to estimate the cost of burn injury, whichinvolved interviewing patients or their attendants. Patient discharge records from16 district hospitals and 45 Upazila (lower political units) health complexes wereused as the main data sources in this study. Discharge records for December 2000were reviewed for all types (injury and non-injury) of hospital admissions, and dis-charge records for January to December 2000 were reviewed for injury admissions.Hospital emergency departments’ records for December 2000 were reviewed tostudy emergency injury cases. Patient interviews were conducted between Febru-ary and March 2001 in selected primary and secondary hospitals in Bangladesh.Results: Seven hundred and ninety-one burn patients were admitted in 2000, whichconstituted 2% of total injury admissions. Hospital records of all types of admission inDecember 2000 revealed that burn patients represented 1% of the total admissions.The duration of hospital stay was significantly longer for patients with burn injurycompared with patients with other injuries or illnesses. The longest hospital staydue to burn injury was 17.34 days, found for children aged 1e4 years. The averagepatient cost for burn injury was higher than that for other injuries and illnesses.Conclusion: Burn injuries were associated with a longer hospital stay comparedwith other injuries and illnesses. The management costs of burn injury, even usingvery incomplete data, were found to be very high in Bangladesh. To reduce this
Injury Prevention and Research, Bangladesh (CIPRB), House 226, Lake Road 15, New DOHSel.: þ880 2 886 1258; fax: þ880 2 886 1499.rg (S.R. Mashreky).
8 The Royal Institute of Public Health. Published by Elsevier Ltd. All rights reserved.

Economic and social impact of burn injury in Bangladesh 1419
economic burden on families, an effective burn prevention programme should bedeveloped.ª 2008 The Royal Institute of Public Health. Published by Elsevier Ltd. All rightsreserved.
Introduction
Worldwide, burns are among the most devastatinginjuries among people of all age groups.1 Globally,in 2000, 238,000 people died due to fire-relatedburns, the majority (95%) of which occurred inlow- and middle-income countries.2 In developingcountries, burns have been found to be a majorcause of injury morbidity, disability and mortality.In Africa and many of the South Asian countries,including India, Pakistan, Nepal, Sri Lanka andAfghanistan, burn injuries have emerged as a majorpublic health issue.3e10 Burns represent a leadingcause of unintentional injury mortality and mor-bidity even in high-income countries.11e14
Acute burn care is a costly service.15 In the USA,the medical costs of primary health care for oneinpatient with burns range from $3000 to $5000/day.16 In the USA, the costs of burn patients werefound to be twice as high as the costs of the aver-age patient in hospital, and they increased ata faster rate.17 In the UK, the average cost peradmitted burn case was found to be approximately$3700,18 and in Israel, the hospitalization cost ofeach burn case was found to be $141,750.19
In developing countries, burns are considered tobe a complicated healthcare problem as carerequires specialized staff and medical technolo-gies that are expensive and not always readilyavailable.20 Burns are associated with longer hos-pital stay, permanent disability and emotionalstress. They represent a serious health problem,especially among economically and socially de-prived populations.21 Burns create an economicburden for the family as they disrupt the abilityof family members to work. The long recoveryperiod and complicated morbidity associatedwith burns add to the high cost of rehabilitation.22
For a low-income country such as Bangladesh, itis very difficult to deal with a large economicburden from a single cause of injury like burns.When making priorities in an injury preventionprogramme, the magnitude of the economic andsocial burden of burns must be determined. Likemany other low-income countries, Bangladeshdoes not have comprehensive and reliable dataabout the costs of burn treatment and the durationof hospital stay.
This study was designed to assess the burden ofburn injury in primary and secondary hospitals inBangladesh, and how these costs are reflected aseconomic burdens in the community.
Findings from this study will help in the planningof hospital management to ensure that limitedresources are utilized in a proper and efficientmanner. Information regarding economic andsocial impact will make policy makers aware ofthe devastating situation resulting from burns. Thisshould ultimately help in the development ofa comprehensive management policy for treatmentof burn injury in Bangladesh, and may possibly haveimplications for other developing countries.
Methods
This was a cross-sectional descriptive study. Datawere obtained from the medical records of se-lected primary and secondary hospitals in Bangla-desh and direct interviews of patients or theirattendants/caregivers.
Secondary hospitals are district hospitals andprimary hospitals are sub-district hospitals. Of the64 district hospitals in Bangladesh, 16 were se-lected at random for this study, and 45 Upazila(lower political level) health complexes wereselected at random from 364 primary care centres.District hospitals have 50e100 beds, and somespecialized treatment facilities, such as generalsurgery, orthopaedics, ophthalmology, internalmedicine, gynaecology and obstetrics, are avail-able. Primary hospitals have 31 beds, and do nothave specialized services. Both inpatient andoutpatient services are available at primaryhospitals, but no surgical procedures requiringgeneral anaesthesia are available. Upazila healthcomplexes are the primary healthcare facilitiescovering an average population of 400,000.
Information regarding all admitted (both injuryand non-injury) patients was collected frompatient discharge records for December 2000.Information for injury patients alone was collectedfrom the patient discharge records for January2000 to December 2000. As injury admission isa relatively infrequent event, 1-year dischargerecords were used to obtain an adequate number

1420 S.R. Mashreky et al.
of cases. Information regarding age, sex, cause ofadmission and duration of hospital stay was ob-tained from these records.
Emergency department records were also used tocollect information for injury patients treated inDecember2000. Informationaboutage, sex,diagnosisand management of these patients was obtained.
Face-to-face interviews were conducted be-tween February and March 2001 with injurypatients discharged from the hospitals. Informa-tion was collected from 369 injury patients or theirattendants, representing approximately 6% of thetotal patients discharged during the given periodof time. Patients or their attendants were askedabout socio-economic status, date, time, placeand cause of injury, and their total expenditure onhealth care. To explore the cost of injury, patientsor their attendants were asked ‘How much moneydid you spend for treatment of the injury?’.Parents or caregivers were interviewed in thecase of childhood (<18 years) burns.
There were 16 data collectors and four supervi-sors in this study. All of the data collectors wereuniversity graduates or had reached Masters level indifferent disciplines. Data collectors were trainedextensively on a 5-day training programme, whichplaced special emphasis on how injury cases were tobe identified from hospital records and how othercauses of disease were to be determined. Forquality control, all of the selected hospitals werevisited by members of the research team duringdata collection. Collected data were entered intoEPI 6 software. Statistical Package for Social Sci-ences Version 11.5 was used for data analysis.Descriptive statistics are shown by frequency andproportion. Analysis of variance tests were con-ducted to show the differences in mean duration ofhospital stay between different age groups and fordifferent causes of hospital admission.
Results
The mean age of study participants (both injuryand non-injury) was 27 years [standard deviation(SD) 17.02] and the median age was 26 years. Forinjury patients alone, the mean age was 30.86years (SD 14.06) and the median age was 30 years.For injury patients attending emergency depart-ments, the mean age was 28.78 years (SD 15.13)and the median age was 27 years.
Emergency department findings
In December 2000, 8217 injury patients attendedthe emergency departments in selected hospitals.
Among them, 1.8% had burn injuries. The highestproportion (11%) of patients with burns was seen inchildren aged 1e4 years old; values were 4%, 1.7%and 1.3% among age groups 5e9 years, 11e17 yearsand �18 years, respectively.
Hospital admission and duration of stay
In December 2000, a total of 11,595 patients (bothinjury and non-injury) were admitted to theselected hospitals. Among them, 3828 (33%) weredue to injury. Burns constituted 1% of totaladmissions. A higher proportion of burns patientswere admitted to hospitals compared withpatients with other injuries attending the emer-gency departments; however, this difference wasnot statistically significant. Approximately 48% ofthe burns patients seen in the emergency de-partments needed hospitalization compared with39% of the patients hospitalized due to otherinjuries. The proportion of cases referred tohigher-level hospitals was similar (6%) for bothburns patients and patients with other injuries.The average duration of hospital stay was 6.35days for burns patients, 5.12 days for patients withother injuries and 3.95 days for non- injuredpatients. The duration of hospital stay for burnspatients was significantly higher (P¼ 0.000) thanthat for non-injury cases. The hospital stay forburns patients was also higher than that forpatients with other injuries, but the differencewas not significant.
Findings from hospital records of admissionsdue to injury from 2000
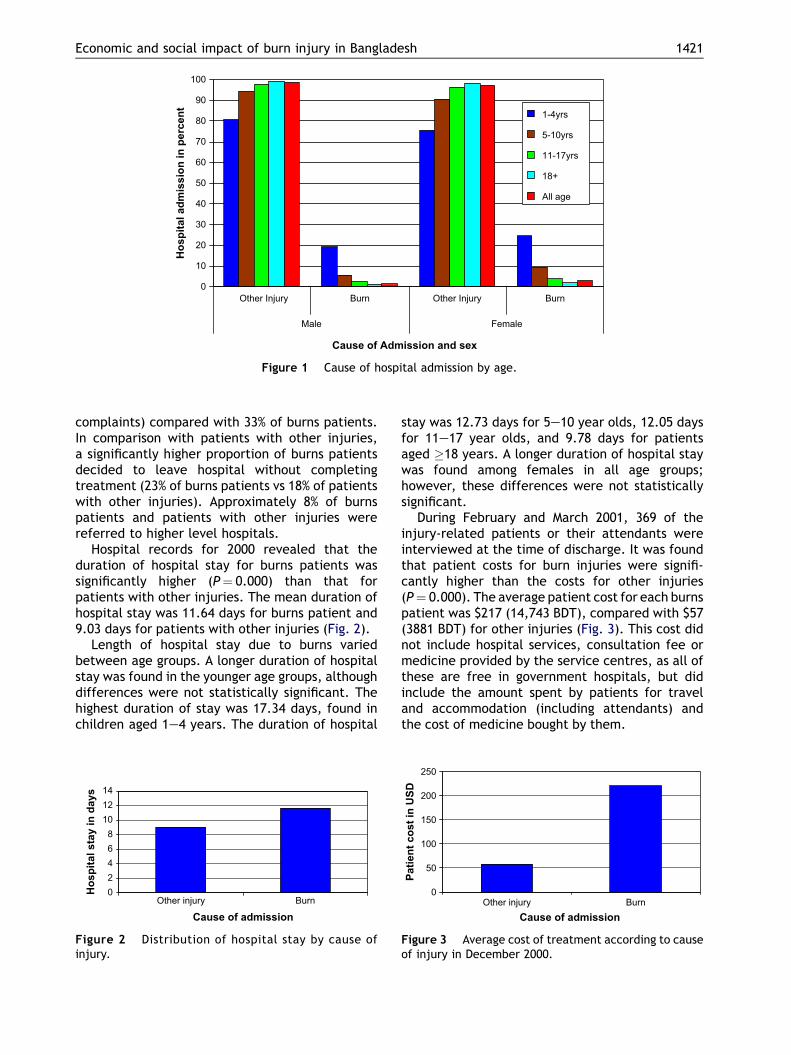
In 2000, a total of 40,375 patients were admittedto the selected hospitals due to injury. Amongthem, 2% (791) were due to burns. Burns admissionwas significantly (P¼ 0.000) higher in younger agegroups. In children aged 1e4 years, approximately22% of the injury-related hospital admissions weredue to burns, compared with only 1.3% in casesaged 18þ years. Admissions due to burn injurieswere more common in females than males in allage groups, but the difference was not statisticallysignificant Fig. 1.
During 2000, hospital records revealed that theoutcomes of management varied according tocause of admission. Treatment outcomes werefound to be significantly (P¼ 0.000) poorer amongburns patient compared with patients admittedwith other injuries. Approximately 41% of patientsadmitted with other injuries left the hospitals ina state of full cure (i.e. left hospital without any
0
10
20
30
40
50
60
70
80
90
100
Other Injury Burn Other Injury Burn
Male Female
Cause of Admission and sex
Ho
sp
ital ad
missio
n in
p
ercen
t
1-4yrs
5-10yrs
11-17yrs
18+
All age
Figure 1 Cause of hospital admission by age.
Economic and social impact of burn injury in Bangladesh 1421
complaints) compared with 33% of burns patients.In comparison with patients with other injuries,a significantly higher proportion of burns patientsdecided to leave hospital without completingtreatment (23% of burns patients vs 18% of patientswith other injuries). Approximately 8% of burnspatients and patients with other injuries werereferred to higher level hospitals.
Hospital records for 2000 revealed that theduration of hospital stay for burns patients wassignificantly higher (P¼ 0.000) than that forpatients with other injuries. The mean duration ofhospital stay was 11.64 days for burns patient and9.03 days for patients with other injuries (Fig. 2).
Length of hospital stay due to burns variedbetween age groups. A longer duration of hospitalstay was found in the younger age groups, althoughdifferences were not statistically significant. Thehighest duration of stay was 17.34 days, found inchildren aged 1e4 years. The duration of hospital
02468
101214
Other injury Burn
Cause of admission
Ho
sp
ital stay in
d
ays
Figure 2 Distribution of hospital stay by cause ofinjury.
stay was 12.73 days for 5e10 year olds, 12.05 daysfor 11e17 year olds, and 9.78 days for patientsaged �18 years. A longer duration of hospital staywas found among females in all age groups;however, these differences were not statisticallysignificant.
During February and March 2001, 369 of theinjury-related patients or their attendants wereinterviewed at the time of discharge. It was foundthat patient costs for burn injuries were signifi-cantly higher than the costs for other injuries(P¼ 0.000). The average patient cost for each burnspatient was $217 (14,743 BDT), compared with $57(3881 BDT) for other injuries (Fig. 3). This cost didnot include hospital services, consultation fee ormedicine provided by the service centres, as all ofthese are free in government hospitals, but didinclude the amount spent by patients for traveland accommodation (including attendants) andthe cost of medicine bought by them.
0
50
100
150
200
250
Other injury BurnCause of admission
Patien
t co
st in
U
SD
Figure 3 Average cost of treatment according to causeof injury in December 2000.

1422 S.R. Mashreky et al.
Discussion
The management of burns is very costly for families.The average cost incurred by families for treatmentof each burns patient was $220, which was approx-imately four times higher than the cost of manage-ment of other injuries. The costs of illness otherthan injuries were not explored in this study, socomparison was not possible. Patient costs of burnsin this study were calculated from the expenditureof the family for the patient to attend primary andsecondary hospitals in Bangladesh. These costs onlyinclude the cost of medicine, transport, food andaccommodation of the patients and their atten-dants. Costs calculated in this study were muchlower than the actual costs, as public hospitalservices were free for the patient and the cost ofprovision of these services was not included in thisstudy. In addition, the national burns unit and othertertiary hospitals were not included in this study.Patient costs of burns management would be muchhigher if tertiary hospitals and the national burnsunit had been included, as specialized hospitals arenormally situated in bigger cities where living costsare higher. In addition, patients with more complexinjuries normally attend tertiary hospitals, result-ing in longer hospital stays and higher costs. Thenational burns unit and other tertiary hospitals werenot included in this study as one of the majorobjectives was to explore the patient burden ofburn injury in primary and secondary hospitals.However, the findings of this study will provideinformation regarding family expenditure fora burns patient.
Although the findings of this study are not directlycomparable to the cost of burns management inother countries, the higher expenditure by familiesof burns victims is consistent with findings in manyother high- and low-income countries.18,26,27 Incomparison with admissions due to other injuriesor illnesses, burns patients stayed in hospital fora longer period. The average duration of hospitalstay for burns patients was 11.65 days, which wassignificantly higher than the duration of stay forany other injury or non-injury cases. Results fromIran and Turkey for burn injuries show similar dura-tions of hospital stay,23,24 and in Papua New Guinea,the duration of hospital stay was 22 days.25 In NewZealand, the duration of hospital stay was 68.7days26; this was much longer as the study was onlyconducted among patients with >30% burns ofbody surface area.
The duration of hospital stay due to burn injurywas highest in the youngest age group. This may bebecause younger children have less perception
about dangerous situations and more limited abil-ities to react promptly and properly to riskysituations.28 This may explain why younger chil-dren get burnt more often and more severely.
Female admissions due to burn injury werehigher in all age groups although the differenceswere not statistically significant. A community-based study on childhood burns in Bangladesh re-vealed that the incidence of burns was higher inyounger boys and older girls.29 Unpublished datafrom the Bangladesh Health and Injury Surveyshowed that the overall incidence of burns washigher in females compared with males, but thesefindings were not statistically significant.30 Femalechildren had to stay in hospital for the longestduration. Higher rates of hospital admission andprolonged hospital stay suggest that females re-ceive more severe burns. In countries like Bangla-desh, girls start cooking or helping their motherswith cooking from a young age, which exposesthem to the risk of injury. This may help to explainthe higher admission rate and longer duration ofhospital stay for females.
The longer duration of hospital stay increasesthe cost of treatment, and longer hospital stay isassociated with complications of morbidity.22 Lon-ger hospital stay places an enormous economicburden on the family, as an adult needs to stayat the hospital with the patient, which ultimatelyamplifies expenditures and inhibits earnings ofother family members.
A community-based survey in Bangladesh re-vealed that 173,000 children under 18 years of ageare moderately to severely burned every year.29 If50% of families spend the average cost of treat-ment, the amount will be $18,923,851(1,267,898,000 BDT). The national incidence ofburns and the cost would be much higher whenthe entire Bangladeshi population is considered.For a low-income country like Bangladesh, thiseconomic burden is excruciating.
Over the year, a large proportion (33% of totaladmissions) of hospital beds were occupied bypatients with injuries; consequently, they consti-tute the largest direct cost of medical care. Threepercent of the total injury admissions were due toburns. The percentage of burns admissions com-pared with total hospital admissions was low in thisstudy, but this does not mean that the burden ofburn injuries is low. Burns constitute a longerduration of hospital stay and higher costs of casemanagement. Bangladesh has tertiary hospitalswhere burn management facilities are much betterthan in primary and secondary hospitals, and thereis one burns centre in the capital city, Dhaka.

Economic and social impact of burn injury in Bangladesh 1423
Patients who can afford to do so attend tertiaryhospitals and the national burns centre, as primaryand secondary hospitals cannot manage severe burncases. Severe burns cases are normally referred totertiary hospitals or the burn centre. It was foundthat approximately 8% of burns patients werereferred to the higher level hospitals, and that23% of burns patients decided to leave hospitalthemselves before completion of treatment. Thehigh proportion of patients who decide to leavehospital themselves may be due to the unmanage-able economic burden for poor people. There are noinsurance facilities available to help meet thesecosts. As people cannot afford the cost of treat-ment, they have to accept serious complicationssuch as permanent disability. This social and familyburden should be taken into consideration by publichealth specialists and policy makers.
This study could not explore the treatment costsof non-injury cases, so it was not possible to makecomparisons. In addition, the study did not includecosts accrued in tertiary hospitals or the nationalburns unit, so it did not capture the costs of verysevere burns cases in terms of duration of hospitalstay. It also did not capture the treatment costsmet by the Government in the initial care facili-ties. Therefore, these results must be much lowerthan the actual average costs. Although the find-ings of this study are not directly comparable tothe findings of other countries, they will add to ourunderstanding regarding the burden of burn injuryin other low-income countries.
Conclusion
Burn injury is an important cause of bed occupancyin hospitals. Even using the very incomplete data inthis study, the management costs of burn injurywere found to be very high in Bangladesh. Youngerchildren and females are most likely to experienceburn injury. An effective burn prevention pro-gramme should be developed to reduce this socialand economic burden. Prevention is the paramountintervention in burn management. Understandingrisk factors in low-income countries should beexplored very carefully to assist this process.For example, as female children stay in hospitalfor longer periods, they may represent a target forprevention activities. Proper supervision and someenvironmental modifications at home can reducethe incidence of burn injury among youngchildren. Social mobilization and education canhelp parents to gain knowledge and improvepractices regarding supervision and environmentalmodification.
Timely and proper management is also a veryimportant aspect in reducing mortality anddisability due to burns. Improvement of the treat-ment facilities at primary and secondary servicecentres will help to reduce the duration and cost oftreatment, and will reduce mortality and disability.
Ethical approval
Ethical Review Committee of Institute of Child andMother Health, Dhaka.
Funding
Ministry of Health and Family Welfare, Bangladesh.
Competing interests
None declared.
References
1. Lau YS. An insight into burns in a developing country: a SriLankan experience. Public Health 2006;120:958e65.
2. Peden M, McGee K, Sharma G. The injury chart book:a graphical overview of the global burden of injuries.Geneva: World Health Organization; 2002.
3. Marsh D, Sheikh A, Khalilz A, Kamil S, Zaman JU, Qureshi I,et al. Epidemiology of adults hospitalized with burns inKarachi, Pakistan. Burns 1996;22:225e9.
4. Liu EH, Khatri B, Shakya YM, Richard BM. A 3-year prospec-tive audit of burns patients treated at the Western RegionalHospital of Nepal. Burns 1998;24:129e33.
5. Ahuja RB, Bhattacharya S. Burns in the developing worldand burn disasters. BMJ 2004;329:447e9.
6. Laloe V. Epidemiology and mortality of burns in a generalhospital of Eastern Sri Lanka. Burns 2002;28:778e81.
7. Razzak JA, Luby SP, Laflamme L, Chotani H. Injuries amongchildren in Karachi, Pakistan e what, where and how. Pub-lic Health 2004;118:114e20.
8. Calder F. Four years of burn injuries in a Red Cross hospitalin Afghanistan. Burns 2002;28:563e8.
9. Nega KE, Lindtjørn B. Epidemiology of burn injuries inMekele Town, Northern Ethiopia: a community based study.Ethiop J Health Dev 2002;16:1e7.
10. Mzezewa S, Jonsson K, Aberg M, Salemar L. A prospectivestudy on the epidemiology of burns in patients admittedto the Harare burn units. Burns 1999;25:499e504.
11. Krug E. Injury surveillance is key to preventing injuries.Lancet 2004;364:1563e6.
12. Rivara FP. Burns: the importance of prevention. Inj Prev2000;6:243e4.
13. Mercier C, Blond MH. Epidemiological survey of childhoodburn injuries in France. Burns 1996;22:29e34.
14. Cronin KJ, Butler PEM, McHugh M, Edwards G. A l-yearprospective study of burns in an Irish paediatric burnsunit. Burns 1996;22:221e4.
15. Takayanagi K, Kawai S, Aoki R. Cost of burn care and impli-cation for efficient care. Clin Perform Qual Health Care1999;7:70e3.

1424 S.R. Mashreky et al.
16. Keswani MH. The 1996 Everett Idris Evans Memorial Lec-ture. The cost of burns and the relevance of prevention.J Burn Care Rehabil 1996;17:485e90.
17. Dimick AR, Potts LH, Charles Jr ED, Wayne J, Reed IM. Thecost of burn care and implications for the future on qualityof care. J Trauma 1986;26:260e6.
18. Griffiths HR, Thornton KL, Clements CM, Burge TS, Kay AR,Young AER. The cost of a hot drink scald. Burns 2006;32:372e4.
19. Eldad A, Stern Z, Sover H, Neuman R, Ben Meir P,Wexler MR. The cost of an extensive burn survival. Burns1993;19:235e8.
20. Lari AR, Panjeshahin MR, Talei AR, Rossignol AMK,Alaghehbandan R. Epidemiology of childhood burn injuriesin Fars Province. Iran J Burn Care Rehabil 2002;23:39e45.
21. Shani E, Ayalon A, Hammad IA, Sikron F. What picture isworth a thousand words? A comparative evaluation ofa burn prevention programme by type of medium in Israel.Health Promot Int 2003;18:369e78.
22. Mandelcorn E, Gomez M, Cartotto RC. Work-related burninjuries in Ontario, Canada: has anything changed in thelast 10 years? Burns 2003;29:469e72.
23. Rouzbahani R, Omranifard M, Rouzbahani A, Barkhordari M.An epidemiological study on burned patients admitted inthe burn hospital in Isfahan Province, Iran in 2002. RawalMed J 2004;29:13e7.
24. Duzgun AP, Senel E, Ozmen MM, Kulacoglu H, Isik Y,Coskun F. Evaluation of the patients admitted to a burncenter in Turkey. Turk J Trauma Emerg Surg 2003;9:250e6.
25. Torova F, Sinha SN. Burn admission to Port Moresby GeneralHospital 1978e1984. Papua New Guinea Med J 1996;39:111e6.
26. Lofts JA. Cost analysis of a major burn. N Z Med J 1991;104:488e90.
27. Sarma BP. Epidemiology and man-days loss in burn injuriesamongst worker in an oil industry. Burns 2001;27:475e80.
28. Bang RL, Ebrahim MK, Sharma PN. Scalds among children inKuwait. Eur J Epidemiol 1997;13:33e9.
29. Mashreky SR, Rahman A, Chowdhury SM, Giashuddin S,Svanstrom L, Linnan M, et al. Epidemiology of childhoodburn: yield of largest community based injury survey in Ban-gladesh. Burns; 2008. doi:10.1016/j.burns.2007.09.009.
30. Bangladesh Health and Injury Survey. Dhaka: Centre forInjury Prevention and Research; 2003. Unpublished.
Available online at www.sciencedirect.com
Related Documents











