ORIGINAL ARTICLE Building on safety, feasibility, and acceptability: the impact and cost of community health worker provision of injectable contraception Dawn Chin-Quee, a John Bratt, a Morrisa Malkin, b Mavis Mwale Nduna, c Conrad Otterness, a Lydia Jumbe, d Reuben Kamoto Mbewe e This project in Zambia contributes to our understanding of the impact of community-based provision of injectables on method choice and uptake and of the costs of adding DMPA to an established community- based family planning program. The project also illustrates the importance of involving stakeholders from the outset, analyzing costs relevant to scale up, and engaging in policy change dialogue not at the end, but rather throughout project implementation. ABSTRACT Background: A critical shortage of doctors, nurses, and midwives in many sub-Saharan African countries inhibits efforts to expand access to family planning services, especially in rural areas. One way to fill this gap is for community health workers (CHWs) to provide injectable contraceptives, an intervention for which there is growing evidence and international support. In 2009, with approval from the Government of Zambia (GoZ), FHI 360 collaborated with ChildFund Zambia to design and implement such an intervention as part of its existing CHW family planning program. Methods: The safety of CHW provision of injectable DMPA (depot medroxyprogesterone acetate) was measured by client reports and by a 21-item structured observation checklist. Feasibility and acceptability were measured by interviews with CHWs and a subset of DMPA clients. The impact of adding DMPA to pill and condom provision was assessed by family planning uptake among the clients of trained CHWs from February 2010 to February 2011. Costs were documented using spreadsheets over the period November 2009 to February 2011. Results: Scores were high on all measures of safety, feasibility, and acceptability. Couple-years of protection (CYP, protection from pregnancy for 1 year) was provided to 51 condom clients, 391 pill clients, and 2,206 DMPA clients. Of the 1,739 clients new to family planning, 85% chose injectable DMPA, while 13% chose pills and 2% chose condoms. Continuation rates were also high, at 63% after 1 year as compared with 47% for pill users. Incremental costs per couple- year were US$21.24 if 50% of users continue with CHW-provided DMPA. Conclusion: The study affirms that the provision of injectable contraceptives by CHWs is safe, acceptable, and feasible in the Zambian context, with very high rates of uptake in hard-to-reach areas. High continuation rates among clients mean that costs of the intervention can be low when added to an existing community-based distribution program—a finding that is relevant to program replication (now underway in Zambia). BACKGROUND M any sub-Saharan African (SSA) countries face critical shortages of doctors, nurses, and mid- wives. 1 This deficit inhibits efforts to expand access to family planning services, especially in rural areas, where access to modern contraceptive methods is limited and few trained personnel are available to provide these services. a FHI 360, Division of Health Services Research, Research Triangle Park, NC, USA b FHI 360, Division of Research Utilization, Research Triangle Park, NC, USA c FHI 360, TB CARE I, Lusaka, Zambia d ChildFund Zambia, Lusaka, Zambia e Republic of Zambia Ministry of Health, Lusaka, Zambia Correspondence to Dawn Chin-Quee ([email protected]). Global Health: Science and Practice 2013 | Volume 1 | Number 3 316

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL ARTICLE
Building on safety feasibility and acceptabilitythe impact and cost of community health worker provisionof injectable contraceptionDawn Chin-Queea John Bratta Morrisa Malkinb Mavis Mwale Ndunac Conrad Otternessa
Lydia Jumbed Reuben Kamoto Mbewee
This project in Zambia contributes to our understanding of the impact of community-based provision ofinjectables on method choice and uptake and of the costs of adding DMPA to an established community-based family planning program The project also illustrates the importance of involving stakeholders fromthe outset analyzing costs relevant to scale up and engaging in policy change dialogue not at the end butrather throughout project implementation
ABSTRACTBackground A critical shortage of doctors nurses and midwives in many sub-Saharan African countries inhibitsefforts to expand access to family planning services especially in rural areas One way to fill this gap is forcommunity health workers (CHWs) to provide injectable contraceptives an intervention for which there is growingevidence and international support In 2009 with approval from the Government of Zambia (GoZ) FHI 360collaborated with ChildFund Zambia to design and implement such an intervention as part of its existing CHWfamily planning programMethods The safety of CHW provision of injectable DMPA (depot medroxyprogesterone acetate) was measured byclient reports and by a 21-item structured observation checklist Feasibility and acceptability were measured byinterviews with CHWs and a subset of DMPA clients The impact of adding DMPA to pill and condom provision wasassessed by family planning uptake among the clients of trained CHWs from February 2010 to February 2011 Costswere documented using spreadsheets over the period November 2009 to February 2011Results Scores were high on all measures of safety feasibility and acceptability Couple-years of protection (CYPprotection from pregnancy for 1 year) was provided to 51 condom clients 391 pill clients and 2206 DMPA clients Ofthe 1739 clients new to family planning 85 chose injectable DMPA while 13 chose pills and 2 chose condomsContinuation rates were also high at 63 after 1 year as compared with 47 for pill users Incremental costs per couple-year were US$2124 if 50 of users continue with CHW-provided DMPAConclusion The study affirms that the provision of injectable contraceptives by CHWs is safe acceptable and feasiblein the Zambian context with very high rates of uptake in hard-to-reach areas High continuation rates among clientsmean that costs of the intervention can be low when added to an existing community-based distribution programmdashafinding that is relevant to program replication (now underway in Zambia)
BACKGROUND
M any sub-Saharan African (SSA) countries facecritical shortages of doctors nurses and mid-
wives1 This deficit inhibits efforts to expand access tofamily planning services especially in rural areaswhere access to modern contraceptive methods islimited and few trained personnel are available toprovide these services
a FHI 360 Division of Health Services Research Research Triangle Park NCUSAb FHI 360 Division of Research Utilization Research Triangle Park NC USAc FHI 360 TB CARE I Lusaka Zambiad ChildFund Zambia Lusaka Zambiae Republic of Zambia Ministry of Health Lusaka Zambia
Correspondence to Dawn Chin-Quee (dchin-queefhi360org)
Global Health Science and Practice 2013 | Volume 1 | Number 3 316
Task sharing has been employed as a strategyto address this problem by delegating health caretasks that are usually carried out by doctors andnurses to a lower-level provider who is moreaccessible to the community For example theGovernment of Zimbabwe recently decided toincrease access to antiretroviral treatment (ART)by authorizing trained nurses to prescribe drugsand manage patients in care2
Many countries in SSA deploy lower-levelcadres in different forms as government ornongovernment-affiliated as volunteers or salar-ied workers with limited or wide-rangingresponsibilities to the communities they serveJust in the area of family planning tasksassigned to community health workers (CHWs)can vary For example while CHWs in Rwandaare able to resupply clients with both pills andinjectables only after a clinical evaluation inUganda they are able to initiate and resupplyclients with hormonal methods In EthiopiaCHWs even insert implants3 Thus CHWs canplay an important role in providing familyplanning services Moreover success in UgandaEthiopia and other SSA countries suggests thatthe role of CHWs need no longer be limited todistribution of condoms and oral contraceptivepills or referral to higher-level providers
At a June 2009 technical consultation con-vened by the World Health Organization (WHO)the US Agency for International Development(USAID) and Family Health International (nowFHI 360) 30 technical and program experts from18 countries reviewed evidence and experiencesfrom programs using CHWs to expand access toinjectable contraceptives These experts con-cluded lsquolsquoGiven appropriate and competency-basedtraining CHWs can screen clients effectivelyprovide DMPA (depot medroxyprogesteroneacetate) injections safely and counsel on theside effects appropriately demonstrating compe-tence equivalent to facility-based providers ofprogestin-only injectablesrsquorsquo4 With the conclusionsendorsed by normative bodies such as theInternational Federation of Gynecology andObstetrics the United Nations Population Fundthe International Council of Nurses and USAIDmore countries in SSA initiated pilot studiesbegan implementing scale-up efforts engaged inpolicy change dialogue or realized policy changesthat allow CHWs to provide injectable contra-ceptives
More recently WHO released a set of guide-lines that define health worker roles for maternal
and newborn health These guidelines focus ontask sharing among various cadres of health careproviders to address the critical human resourceshortages in many developing countries Usingthe latest scientific evidence and the Grading ofRecommendations Assessment Development andEvaluation (GRADE) methodology WHOendorsed the lsquolsquoinitiation and maintenance ofinjectable contraceptivesrsquorsquo by lay health workersusing a standard syringe provided that a strongmonitoring and evaluation system is in place5
As of August 2012 13 countries in SSA wereundergoing various stages of rolling out CHWprovision of injectables6 Different paths werefollowed as some governments changed policyfirst and then conducted pilot studies and scaleup while others began with pilots before con-sidering scale up and policy change7 The impactof CHW-provided injectable contraception hasbeen measured in countries such as KenyaMadagascar Malawi Nigeria and Ugandawhere these programs reported expanded accessto family planning services increased uptake offamily planning methods reduced workload inclinics and improved method continuation ratesamong DMPA users89
In Zambia the process to gain approval forCHW provision of DMPA began with a requestfrom the government to conduct a pilot study inhard-to-reach areas where staff turnover alsopresents a significant problem As in other SSAcountries use of family planning services amongrural women in Zambia is relatively low thecontraceptive prevalence rate (CPR) for modernmethods is 37 compared with 48 in urbanareas Similarly unmet need in rural areas is 28(19 spacing 9 limiting) versus 23 (13spacing 10 limiting) in urban areas10 In a July2009 stakeholder meeting to discuss design ofthe pilot study government officials and nationalstakeholders requested measures of programimpact to be included in addition to localconfirmation of the safety feasibility andacceptability of CHW provision of injectablecontraception
With approval from the Government ofZambia (GoZ) FHI 360 collaborated withChildFund Zambia the local affiliate ofChildFund International (formerly ChristianChildrenrsquos Fund) to design and implement anintervention to introduce injectable contracep-tion into ChildFundrsquos existing CHW familyplanning program The ChildFund CHW pro-gram has been in operation since 1987 In
A growing body ofevidence supportsthe provision ofinjectablecontraceptives byCHWs in hard-to-reach areas
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 317
addition to providing family planning servicesChildFund CHWs also deliver health educationon personal hygiene and safe motherhood aswell as sensitize the communitymdashfocusing onmenmdashabout family planning CHWs are bothmen and women with varying levels ofsecondary school education who have beenchosen by community members to provide basicservices at the community level They arevolunteers but receive in-kind remuneration inthe form of materials and equipment (bicyclesraincoats and boots t-shirts bags) and cost-shared animal restocking Their initial familyplanning training conducted over 2 weeks usesthe GoZ curriculum that also includes topics onclientsrsquo rights anatomy and physiology HIVAIDS mode of transmission family life educa-tion male involvement distribution and storageof commodities and more Although they workfor ChildFund these CHWs are affiliated withand supervised by GoZ health center staff (aswell as ChildFund staff) from whom theyobtain family planning commodities and towhom they submit records for inclusion in thedistrict data management system
With ChildFundrsquos assistance we also col-lected information on additional or lsquolsquoincremen-talrsquorsquo costs of adding injectable contraception totheir ongoing CHW provision of condoms andoral contraceptive pills As programs grapple withlimited resources such information is needed toestimate costs of scaling up and to establish thatan intervention provides lsquolsquovalue for moneyrsquorsquoThus this paper not only presents results onthe safety feasibility and acceptability of CHWprovision of DMPA in the Zambian context but italso focuses on the impact and costs of addingDMPA to an established community-basedfamily planning program
The study objectives were to
N Assess CHW ability to provide DMPA injec-tions to clients safely and effectively
N Assess acceptability of and client and CHWsatisfaction with community-based deliveryof DMPA
N Determine the impact of adding DMPA onfamily planning uptake and the proportion ofpill and DMPA users continuing at 6 9 and12 months
N Determine incremental cost per couple-yearof protection (CYP) of adding injectablecontraceptives to the existing CHW program
METHODS
OverviewThe safety of CHW provision of injectableswas measured by DMPA client reports and bya 21-item structured observation checklist(SOC) divided into 2 scales that measuredinfection prevention (11 items) and injectionprocedures (10 items) The SOC was usedduring a clinic-based practicum Feasibilityand acceptability were measured by interviewswith CHWs and a subset of their DMPAclients The impact of adding injectable con-traception to pill and condom provision wasassessed by family planning uptake amongthe clients of trained CHWs from February2010 to February 2011 Costs associated withadding DMPA to CHW-provided family plan-ning services were documented using spread-sheets over the period November 2009 toFebruary 2011
Training and Data CollectionChildFund Zambia selected Mumbwa andLuangwa districtsmdashtwo of ChildFundrsquos hard-to-reach poor communities with limited access tohealth care servicesmdashto participate in the pilotstudy Mumbwa has 34 health centers 8 of whichare in 6 communities served by CHWs involved inthe study Luangwa has 10 health centers andabout 26 health units or health posts 8 of whichhad CHWs involved in the study
Preliminary estimates from Zambiarsquos 2010unpublished census put the population inLuangwa at about 25000 and the 6-communityChildFund catchment area in Mumbwa at about50000 (out of a total district population of218328) The 8 health centers in Mumbwaaffiliated with ChildFund CHWs are staffed by17 providers while the 8 health posts inLuangwa have only 12 staff members reflectinga severe shortage of health care workers AlsoCHWs outnumbered Ministry of Health (MOH)staff in those catchment areas
Forty practicing CHWs (20 from each district)affiliated with the 16 health facilities inMumbwa and Luangwa were trained by mastertrainers from the MOH to safely provide DMPAinjections in addition to the family planningservices they already provided CHWs received5 days of didactic instruction on determiningmethod eligibility (screening) counseling andinformed choice client referral and provision oforal contraceptive pills condoms and DMPA
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 318
CHWs also completed a 2- to 4-week clinic-basedpracticum during which 6 or more DMPAinjections had to be successfully administeredbefore the CHW was allowed to provide injec-tions unsupervised We divided the 21-itemstructured observation checklist used by evalua-tors into its 2 main components and calculated atotal score for safe injections with regard toinfection prevention and to injection procedureEvaluations of the first and last injections givenby each CHW constituted the measures of safety
The training and practicum were conductedon a staggered schedule in Luangwa andMumbwa between December 2009 and January2010 By February 2010 all CHWs were certifiedand their capabilities introduced to their respec-tive communities at an official graduationceremony involving local leaders and ChildFundrepresentatives CHWs were then asked to recordall provision of condoms pills and injectables totheir family planning clients for 13 monthsmdashdistinguishing between new acceptors switchersand continuing users of all methodsmdashusingChildFund Zambiarsquos family planning registermodified to include DMPA
The study teammdashcomprising FHI 360ChildFund Zambia and Ministry of Health staffthe Family Planning Technical Working Group(FPTWG) and other stakeholdersmdashselected thefollowing measures of impact
1 Family planning method uptake (expressedin couple-years of protection or CYPs)
2 Proportion of CHW clients who are newfamily planning and new DMPA acceptors
3 Indicators of family planning method con-tinuation by CHW pill and DMPA clients
4 Comparisons between CYPs provided bystudy CHWs and CYPs recorded by DistrictHealth Offices (DHOs)
Approximately 9 months into data collectionwe interviewed all CHWs and a subset of theirDMPA clients (n5253) who received their firstinjection from a CHW between February andApril 2010 By then CHWs had performedseveral months of DMPA administration andenough time had elapsed for these initial DMPAusers to receive up to 3 injections from a CHW
ChildFund Zambia also selected 6 maleemployeesmdash3 assigned to each districtmdashto per-sonally retrieve family planning data on amonthly basis from the 40 CHWs These men(given bicycles for transportation) were engagedspecifically to cover the distances to and fromCHWsrsquo homes discuss and verify data with theCHWs and transfer the required informationfrom the family planning register to the dataretrieval form developed for the study This formcollected information on
N Method receivedused on the first visit instudy period
N Whether the client was a continuing user ornew family planning acceptor1
N Previous method used
N Number of pill cycles or condoms distributedand the scheduled re-injection date for DMPAclients over the course of the 13-month datacollection period
The 6 data retrievers received instructionfrom the Lusaka-based project coordinator onuse of the data retrieval form and the familyplanning client register Data retrievers also metwith the project coordinator monthly for the firsthalf of data collection then every 2 to 3 monthsthereafter to verify the accuracy of the informa-tion and to submit CHW family planning uptakedata from February 2010 to February 2011
We also obtained family planning statisticsfor pills condoms and DMPA distribution fromthe District Health Offices in Luangwa andMumbwa for the same 13-month time periodThese statistics reportedly included both healthfacility and CHW provision of family planningmethods All analyses were performed with SAS9211
The training materials used in 2009 can be accessed at httpwwwk4healthorgtoolkitscba2isample-community-health-worker-training-curriculum However the content has since beenupdated to emphasize dual protection to prevent STIsHIV and a13-week DMPA re-injection window Originally the Zambia MOHwas following a 12-week policy The FPTWG comprises all local stakeholders interestedinvolvedin family planning including the Zambia MOH UNFPA WHOUSAID JSI (John Snow Inc) ZISSP (Zambia Integrated SystemsStrengthening Program) Marie Stopes International PPAZ(Planned Parenthood Association of Zambia) CHAZ (ChurchesHealth Association of Zambia) World Vision CDC SFH (Societyfor Family Health) and Boston University CYP is the estimated protection provided by contraceptivemethods during a 1-year period Our estimates were based onUSAID conversion factors for units of condoms (120 per CYP) andpill packs (15 cycles per CYP) distributed and DMPA injectionsreceived (4 doses per CYP) CYPs are not routinely calculated byChildFund and were computed solely to meet the objectives of thestudy
1 During the data collection period no women stopped andrestarted a method after 6 months we did not determine uponrecruitment if continuing users entering the study had restarted amethod after 6 months
Study methodsincluded checkliststo measure safeprovision inter-views with CHWsand clients andcost analyses
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 319
Assessment of Incremental Costs of AddingDMPA to the CHW ProgramThe approach to costing the addition of a healthservice intervention to an existing program is toconcentrate on additional or lsquolsquoincrementalrsquorsquo costsonly since costs of the existing program wouldhave been incurred even without the interven-tion Incremental costs of an intervention can beclassified according to 3 phases 1) planningdesigning the intervention 2) preparing forservice delivery and 3) delivering the new orimproved services Each phase comprises a set ofactivities and each activity uses resources suchas time of trainers and providers and medicalsupplies and equipment When costs are attachedto resources used in the intervention the totalincremental cost of the intervention may becalculated Stakeholders may be more interestedin costs of activities relevant to scaling up givingless emphasis to costs in the planning and designphase In our study these activities included thefollowing
1 The training of trainers (ToT) workshop thattrained 10 trainers of which 4 were used forthe CHW training courses in Luangwa andMumbwa
2 The CHW training consisting of 2 workshopseach of which trained 20 CHWs
3 The CHW practicum which included traineemeal allowances and transport refunds forCHW visits to clinic facilities for mentoringand practice in injection technique
4 Supervision of CHWs which took place in2 stages an intensive initial stage whereinteractions were more frequent and longerin duration and a second phase in whichsupervisors checked in with CHWs duringroutine site visits
5 Overall intervention management byChildFund staff who oversaw all activitiesrelated to the intervention
6 DMPA commodities including vials sy-ringes cotton soap and sharps boxes
We used key informant interviews recordreviews and periodic progress reports to identifyall intervention-related activities and resourcesand we designed Excel-based spreadsheets toorganize information on the costs of theseresources Most costs reflect actual expendituresexcept for personnel costs which were estimatedusing MOH salary scales for positions considered
to be equivalent to those of research and projectstaff who implemented the intervention
Incremental cost per CYP of CHW provisionof DMPA was calculated by dividing the annual-ized incremental cost of the intervention (that iscosts adjusted for the period of the study) by thenumber of CYPs attributable to the CHW inter-vention This indicator provides a sense of thevalue of resources needed to protect 1 couplefrom pregnancy for a year through DMPAprovided by CHWs in ChildFundrsquos program
FHI 360rsquos Protection of Human SubjectsCommittee and ERES Converge Ethical ReviewBoard in Zambia reviewed and approved thisstudy
RESULTS
Safety of DMPA Provision by CHWsOn the 11-item scale on infection preventionprocedures CHWs initially carried out about 9of the items or 82 on average At their finalassessment the average score increased to aperfect 11 or 100 Thus there was improve-ment from the first to the last DMPA injectionevaluated during the practicum but the startingpoint was high to begin with
For the 10-item injection procedure scale theinitial average score was 74 and at finalassessment the score was 96 Again there wasimprovement but it is important to note thatCHWs who scored low in the initial assessmentimproved markedly by the last assessment Thisis captured by the narrowing of the range ofscores from the initial to the final assessmentsfor both infection prevention and injectionprocedure (Figure 1)
Only 6 (2) of the 253 DMPA clientsinterviewed after 9 months of data collectionreported any problems with CHW-providedinjections Three could not describe the problem2 reported pain at the injection site and 1 clientdescribed numbness in the arm There were noreports from clients of abscesses or infectionsDuring monitoring and supervision activitiesconducted by ChildFund throughout the studyperiod CHWs also reported to ChildFund andMOH supervisors that they had not found anyabscesses or infections
Acceptability of Method to ClientsThe acceptability of DMPA and CHW-provisionof the method was ascertained by interviewswith 253 clients
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 320
N 94 were very much satisfied with DMPA asa family planning method
N 93 wanted to get another DMPA injection
N 94 of CBD clients who accepted DMPAbetween February and April 2010 received asecond DMPA injection
N 99 wanted to receive their next injectionfrom a CHW
N 98 were satisfied with the way the CBDagent gave them their injection
N 98 would recommend receiving a DMPAinjection from their CBD agent to a friend
Of the 7 of DMPA users who did not wantanother injection the main reasons mentioned
were desire to have a child (35) side effects orproblems with DMPA use (35) and husbandrsquosdisapproval (18) For the 4 women (16) whocould have but did not receive a second injectionthe reasons were dissatisfaction with side effects(n52) and husbandrsquos disapproval (n52) ThusCHW provision of DMPA and the method itselfproved highly acceptable
In interviews with the 40 CHWs 98reported that it was easy to find women whowere interested in receiving DMPA and 80 feltthat it was easy to gain the confidence of thecommunity in their ability to provide DMPAAlthough 89 said that their workload increaseddue to the addition of DMPA to their familyplanning services they reported that the increasewas acceptable and not a burden
FIGURE 1 Safety of CHW Provision of Injectables
Abbreviations CHW community health worker
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 321
Characteristics of Acceptors and FamilyPlanning UptakeData on family planning method uptake wererecorded for a total 4241 family planning clientsin both districts during the 13-month datacollection period The average age of womenwas 28 with a range of 15 to 53 years Clientshad an average of 36 living children with arange of 0 to 14 children
Based on provision of methods by ChildFundCHWs from February 2010 to February 2011 51condom clients 391 pill clients and 2206 DMPAclients would be protected from pregnancy for 1year Uptake of condoms pills and DMPA wasgreater in Mumbwa than Luangwa as themajority of family planning clients (73) werefrom Mumbwa district the more populous areawith a higher contraceptive prevalence rate (40vs 27)10 In both districts condoms conferredthe fewest CYPs while DMPA conferred the most(Table 1)
With regard to new acceptors 41 of CHWclients during the 13-month period were new tofamily planning In this group of 1739 women85 chose DMPA 13 chose oral contraceptivepills and the remaining 2 chose condoms astheir first family planning method Of thecontinuing users 63 reported using pills 30DMPA 6 condoms and the rest unspecified Ofall the family planning clients in the study 82or 3479 women obtained DMPA from a CHWsome time between February 2010 and February2011 About 20 were continuing clients whowere formerly clinic clients and 24 were formerpill and condom users who switched to CHW-provided DMPA
Continuing Method Use for Pills and DMPATo determine continuing method use we exam-ined data from women who obtained DMPA orpills from CHWs during the study who had theopportunitymdashbased on when they startedmdashtouse DMPA or pills for 6 months 9 months or12 months (Figure 2) Continuation for DMPAusers was always higher than for pill users (usingmutually exclusive groups of women with 6 9and 12 month follow-up data) with a significantdifference noted at the 12-month markmdash63 vs47 (Chi-square P001)
Comparison of District Health OfficeStatistics with CHW Uptake DataFigure 3 compares CYP data from district-levelstatistics (which include both clinic and CHWinputs) with records from the ChildFund ZambiaCHWs participating in Luangwa and Mumbwa Itis clear from the comparison that many morecondoms are provided at the clinic than at thecommunity level while pill and DMPA provisionby the 40 CHWs accounts for about half of theCYPs documented by 34 health centers inMumbwa and 10 in Luangwa
Incremental Cost of Intervention and Per CYPTable 2 reports incremental costs of interventionactivities relevant to future scale up The totalincremental costs were US$37300 (in 2010 dol-lars) while the annualized costs adjust some of thecost items to reflect that their effects would extendbeyond the initial year of the intervention Forexample the ToT workshop produced 10 personscapable of training CHWs to provide DMPA butonly 4 of them participated in the pilot therefore
TABLE 1 Couple-Years of Protection (CYP) by CHW-Provided Methods in Study DistrictsFebruary 2010 to February 2011
Districts
CYP provided by Luangwa Mumbwa Total
Condoms 13 38 51
Oral contraceptive pills 96 295 391
Injectable DMPA 727 1479 2206
Total 836 1812 2648
Source FHI 360 Data Retriever RegistersAbbreviation CHW community health worker DMPA depot medroxyprogesterone acetate
Uptake resultsshowed anoverwhelmingpreference forinjectable DMPAover pills andcondoms
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 322
only 40 of the ToT costs are applicable to the pilotFor both training activities the effects are assumedto last for 2 years (requiring periodic refreshertraining) and so we applied one-half of thetraining cost (including practicum expenses) tothe 1-year period of service delivery in the pilotprogram Other activity costs are unchanged Theestimate of annualized incremental cost (whichalso serves as the numerator of the incrementalcost per CYP ratio) was US$24322
The denominator of the cost per CYP ratioreflects the number of CYPs that can be attributedto the intervention All CYPs (373) from newDMPA acceptors are included along with 20additional CYPs that represent increased contra-ceptive protection contributed by women whoswitched to DMPA from the less effective pills andcondoms The remaining CYPs (1813) can beattributed to the intervention if we assume thatthese continuing users would not have returned tothe clinic for DMPA services Figure 4 shows thecost per CYP that can definitively be attributed toCHW provision (US$6189) and the change in cost
per CYP at different levels of DMPA continuationIf we assume that 50 of existing DMPA userscontinued with their method solely because of theimproved access afforded by CHW provision costper CYP would be lower at US$2124 If all userscontinued because of CHW provision cost per CYPwould be US$1103
DISCUSSION
Safe Feasible and AcceptableThis pilot study contributes to the body ofevidence on CHW provision of injectable contra-ception As detailed in the Results section of thisarticle the findings establish the safety feasi-bility and acceptability of CHWs providingDMPA in the Zambian context
Impact on Method Use and ChoiceThe findings also demonstrate the impact ofproviding DMPA through CHWs on method useand choice namely that a sizable number of womenbecame new acceptors of all the methods provided
FIGURE 2 Continued Use of Methods Obtained From CHWs
Abbreviations DMPA depot medroxyprogesterone acetate
Source FHI 360 Data Retriever Registers
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 323
by CHWs Women were also able to switch to a moredesirable method andor service delivery setting
Other Factors Affecting UptakeThe project cannot take full credit for theincrease in DMPA use in the 2 districts following
initiation of the pilot study since the method wasalso available at 44 health clinics However itwas a noteworthy increase made all the morestriking by the fact that provision by the 40CHWs accounted for more than half of the CYPsreported by the District Health Offices from
FIGURE 3 Couple-Years of Protection (CYP) February 2010 to February 2011
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
TABLE 2 Total and Annualized Incremental Costs of the Intervention (4600 Zambia Kwacha 5US$1)
Intervention Activity Total Cost (US$) Annualized Cost (US$)
Training of trainers (N510) 5103 1021
Training of CHWs (N540) 12964 6482
Practicum expenses 4827 2414
Supervision of CHWs 3334 3334
Overall intervention management 3219 3219
DMPA commodities 7853 7853
Total incremental costa 37300 24322aAs noted these estimates do not include costs of planning and design because these are one-time activities that would notbe repeated in scale upAbbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 324
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327

Task sharing has been employed as a strategyto address this problem by delegating health caretasks that are usually carried out by doctors andnurses to a lower-level provider who is moreaccessible to the community For example theGovernment of Zimbabwe recently decided toincrease access to antiretroviral treatment (ART)by authorizing trained nurses to prescribe drugsand manage patients in care2
Many countries in SSA deploy lower-levelcadres in different forms as government ornongovernment-affiliated as volunteers or salar-ied workers with limited or wide-rangingresponsibilities to the communities they serveJust in the area of family planning tasksassigned to community health workers (CHWs)can vary For example while CHWs in Rwandaare able to resupply clients with both pills andinjectables only after a clinical evaluation inUganda they are able to initiate and resupplyclients with hormonal methods In EthiopiaCHWs even insert implants3 Thus CHWs canplay an important role in providing familyplanning services Moreover success in UgandaEthiopia and other SSA countries suggests thatthe role of CHWs need no longer be limited todistribution of condoms and oral contraceptivepills or referral to higher-level providers
At a June 2009 technical consultation con-vened by the World Health Organization (WHO)the US Agency for International Development(USAID) and Family Health International (nowFHI 360) 30 technical and program experts from18 countries reviewed evidence and experiencesfrom programs using CHWs to expand access toinjectable contraceptives These experts con-cluded lsquolsquoGiven appropriate and competency-basedtraining CHWs can screen clients effectivelyprovide DMPA (depot medroxyprogesteroneacetate) injections safely and counsel on theside effects appropriately demonstrating compe-tence equivalent to facility-based providers ofprogestin-only injectablesrsquorsquo4 With the conclusionsendorsed by normative bodies such as theInternational Federation of Gynecology andObstetrics the United Nations Population Fundthe International Council of Nurses and USAIDmore countries in SSA initiated pilot studiesbegan implementing scale-up efforts engaged inpolicy change dialogue or realized policy changesthat allow CHWs to provide injectable contra-ceptives
More recently WHO released a set of guide-lines that define health worker roles for maternal
and newborn health These guidelines focus ontask sharing among various cadres of health careproviders to address the critical human resourceshortages in many developing countries Usingthe latest scientific evidence and the Grading ofRecommendations Assessment Development andEvaluation (GRADE) methodology WHOendorsed the lsquolsquoinitiation and maintenance ofinjectable contraceptivesrsquorsquo by lay health workersusing a standard syringe provided that a strongmonitoring and evaluation system is in place5
As of August 2012 13 countries in SSA wereundergoing various stages of rolling out CHWprovision of injectables6 Different paths werefollowed as some governments changed policyfirst and then conducted pilot studies and scaleup while others began with pilots before con-sidering scale up and policy change7 The impactof CHW-provided injectable contraception hasbeen measured in countries such as KenyaMadagascar Malawi Nigeria and Ugandawhere these programs reported expanded accessto family planning services increased uptake offamily planning methods reduced workload inclinics and improved method continuation ratesamong DMPA users89
In Zambia the process to gain approval forCHW provision of DMPA began with a requestfrom the government to conduct a pilot study inhard-to-reach areas where staff turnover alsopresents a significant problem As in other SSAcountries use of family planning services amongrural women in Zambia is relatively low thecontraceptive prevalence rate (CPR) for modernmethods is 37 compared with 48 in urbanareas Similarly unmet need in rural areas is 28(19 spacing 9 limiting) versus 23 (13spacing 10 limiting) in urban areas10 In a July2009 stakeholder meeting to discuss design ofthe pilot study government officials and nationalstakeholders requested measures of programimpact to be included in addition to localconfirmation of the safety feasibility andacceptability of CHW provision of injectablecontraception
With approval from the Government ofZambia (GoZ) FHI 360 collaborated withChildFund Zambia the local affiliate ofChildFund International (formerly ChristianChildrenrsquos Fund) to design and implement anintervention to introduce injectable contracep-tion into ChildFundrsquos existing CHW familyplanning program The ChildFund CHW pro-gram has been in operation since 1987 In
A growing body ofevidence supportsthe provision ofinjectablecontraceptives byCHWs in hard-to-reach areas
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 317
addition to providing family planning servicesChildFund CHWs also deliver health educationon personal hygiene and safe motherhood aswell as sensitize the communitymdashfocusing onmenmdashabout family planning CHWs are bothmen and women with varying levels ofsecondary school education who have beenchosen by community members to provide basicservices at the community level They arevolunteers but receive in-kind remuneration inthe form of materials and equipment (bicyclesraincoats and boots t-shirts bags) and cost-shared animal restocking Their initial familyplanning training conducted over 2 weeks usesthe GoZ curriculum that also includes topics onclientsrsquo rights anatomy and physiology HIVAIDS mode of transmission family life educa-tion male involvement distribution and storageof commodities and more Although they workfor ChildFund these CHWs are affiliated withand supervised by GoZ health center staff (aswell as ChildFund staff) from whom theyobtain family planning commodities and towhom they submit records for inclusion in thedistrict data management system
With ChildFundrsquos assistance we also col-lected information on additional or lsquolsquoincremen-talrsquorsquo costs of adding injectable contraception totheir ongoing CHW provision of condoms andoral contraceptive pills As programs grapple withlimited resources such information is needed toestimate costs of scaling up and to establish thatan intervention provides lsquolsquovalue for moneyrsquorsquoThus this paper not only presents results onthe safety feasibility and acceptability of CHWprovision of DMPA in the Zambian context but italso focuses on the impact and costs of addingDMPA to an established community-basedfamily planning program
The study objectives were to
N Assess CHW ability to provide DMPA injec-tions to clients safely and effectively
N Assess acceptability of and client and CHWsatisfaction with community-based deliveryof DMPA
N Determine the impact of adding DMPA onfamily planning uptake and the proportion ofpill and DMPA users continuing at 6 9 and12 months
N Determine incremental cost per couple-yearof protection (CYP) of adding injectablecontraceptives to the existing CHW program
METHODS
OverviewThe safety of CHW provision of injectableswas measured by DMPA client reports and bya 21-item structured observation checklist(SOC) divided into 2 scales that measuredinfection prevention (11 items) and injectionprocedures (10 items) The SOC was usedduring a clinic-based practicum Feasibilityand acceptability were measured by interviewswith CHWs and a subset of their DMPAclients The impact of adding injectable con-traception to pill and condom provision wasassessed by family planning uptake amongthe clients of trained CHWs from February2010 to February 2011 Costs associated withadding DMPA to CHW-provided family plan-ning services were documented using spread-sheets over the period November 2009 toFebruary 2011
Training and Data CollectionChildFund Zambia selected Mumbwa andLuangwa districtsmdashtwo of ChildFundrsquos hard-to-reach poor communities with limited access tohealth care servicesmdashto participate in the pilotstudy Mumbwa has 34 health centers 8 of whichare in 6 communities served by CHWs involved inthe study Luangwa has 10 health centers andabout 26 health units or health posts 8 of whichhad CHWs involved in the study
Preliminary estimates from Zambiarsquos 2010unpublished census put the population inLuangwa at about 25000 and the 6-communityChildFund catchment area in Mumbwa at about50000 (out of a total district population of218328) The 8 health centers in Mumbwaaffiliated with ChildFund CHWs are staffed by17 providers while the 8 health posts inLuangwa have only 12 staff members reflectinga severe shortage of health care workers AlsoCHWs outnumbered Ministry of Health (MOH)staff in those catchment areas
Forty practicing CHWs (20 from each district)affiliated with the 16 health facilities inMumbwa and Luangwa were trained by mastertrainers from the MOH to safely provide DMPAinjections in addition to the family planningservices they already provided CHWs received5 days of didactic instruction on determiningmethod eligibility (screening) counseling andinformed choice client referral and provision oforal contraceptive pills condoms and DMPA
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 318
CHWs also completed a 2- to 4-week clinic-basedpracticum during which 6 or more DMPAinjections had to be successfully administeredbefore the CHW was allowed to provide injec-tions unsupervised We divided the 21-itemstructured observation checklist used by evalua-tors into its 2 main components and calculated atotal score for safe injections with regard toinfection prevention and to injection procedureEvaluations of the first and last injections givenby each CHW constituted the measures of safety
The training and practicum were conductedon a staggered schedule in Luangwa andMumbwa between December 2009 and January2010 By February 2010 all CHWs were certifiedand their capabilities introduced to their respec-tive communities at an official graduationceremony involving local leaders and ChildFundrepresentatives CHWs were then asked to recordall provision of condoms pills and injectables totheir family planning clients for 13 monthsmdashdistinguishing between new acceptors switchersand continuing users of all methodsmdashusingChildFund Zambiarsquos family planning registermodified to include DMPA
The study teammdashcomprising FHI 360ChildFund Zambia and Ministry of Health staffthe Family Planning Technical Working Group(FPTWG) and other stakeholdersmdashselected thefollowing measures of impact
1 Family planning method uptake (expressedin couple-years of protection or CYPs)
2 Proportion of CHW clients who are newfamily planning and new DMPA acceptors
3 Indicators of family planning method con-tinuation by CHW pill and DMPA clients
4 Comparisons between CYPs provided bystudy CHWs and CYPs recorded by DistrictHealth Offices (DHOs)
Approximately 9 months into data collectionwe interviewed all CHWs and a subset of theirDMPA clients (n5253) who received their firstinjection from a CHW between February andApril 2010 By then CHWs had performedseveral months of DMPA administration andenough time had elapsed for these initial DMPAusers to receive up to 3 injections from a CHW
ChildFund Zambia also selected 6 maleemployeesmdash3 assigned to each districtmdashto per-sonally retrieve family planning data on amonthly basis from the 40 CHWs These men(given bicycles for transportation) were engagedspecifically to cover the distances to and fromCHWsrsquo homes discuss and verify data with theCHWs and transfer the required informationfrom the family planning register to the dataretrieval form developed for the study This formcollected information on
N Method receivedused on the first visit instudy period
N Whether the client was a continuing user ornew family planning acceptor1
N Previous method used
N Number of pill cycles or condoms distributedand the scheduled re-injection date for DMPAclients over the course of the 13-month datacollection period
The 6 data retrievers received instructionfrom the Lusaka-based project coordinator onuse of the data retrieval form and the familyplanning client register Data retrievers also metwith the project coordinator monthly for the firsthalf of data collection then every 2 to 3 monthsthereafter to verify the accuracy of the informa-tion and to submit CHW family planning uptakedata from February 2010 to February 2011
We also obtained family planning statisticsfor pills condoms and DMPA distribution fromthe District Health Offices in Luangwa andMumbwa for the same 13-month time periodThese statistics reportedly included both healthfacility and CHW provision of family planningmethods All analyses were performed with SAS9211
The training materials used in 2009 can be accessed at httpwwwk4healthorgtoolkitscba2isample-community-health-worker-training-curriculum However the content has since beenupdated to emphasize dual protection to prevent STIsHIV and a13-week DMPA re-injection window Originally the Zambia MOHwas following a 12-week policy The FPTWG comprises all local stakeholders interestedinvolvedin family planning including the Zambia MOH UNFPA WHOUSAID JSI (John Snow Inc) ZISSP (Zambia Integrated SystemsStrengthening Program) Marie Stopes International PPAZ(Planned Parenthood Association of Zambia) CHAZ (ChurchesHealth Association of Zambia) World Vision CDC SFH (Societyfor Family Health) and Boston University CYP is the estimated protection provided by contraceptivemethods during a 1-year period Our estimates were based onUSAID conversion factors for units of condoms (120 per CYP) andpill packs (15 cycles per CYP) distributed and DMPA injectionsreceived (4 doses per CYP) CYPs are not routinely calculated byChildFund and were computed solely to meet the objectives of thestudy
1 During the data collection period no women stopped andrestarted a method after 6 months we did not determine uponrecruitment if continuing users entering the study had restarted amethod after 6 months
Study methodsincluded checkliststo measure safeprovision inter-views with CHWsand clients andcost analyses
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 319
Assessment of Incremental Costs of AddingDMPA to the CHW ProgramThe approach to costing the addition of a healthservice intervention to an existing program is toconcentrate on additional or lsquolsquoincrementalrsquorsquo costsonly since costs of the existing program wouldhave been incurred even without the interven-tion Incremental costs of an intervention can beclassified according to 3 phases 1) planningdesigning the intervention 2) preparing forservice delivery and 3) delivering the new orimproved services Each phase comprises a set ofactivities and each activity uses resources suchas time of trainers and providers and medicalsupplies and equipment When costs are attachedto resources used in the intervention the totalincremental cost of the intervention may becalculated Stakeholders may be more interestedin costs of activities relevant to scaling up givingless emphasis to costs in the planning and designphase In our study these activities included thefollowing
1 The training of trainers (ToT) workshop thattrained 10 trainers of which 4 were used forthe CHW training courses in Luangwa andMumbwa
2 The CHW training consisting of 2 workshopseach of which trained 20 CHWs
3 The CHW practicum which included traineemeal allowances and transport refunds forCHW visits to clinic facilities for mentoringand practice in injection technique
4 Supervision of CHWs which took place in2 stages an intensive initial stage whereinteractions were more frequent and longerin duration and a second phase in whichsupervisors checked in with CHWs duringroutine site visits
5 Overall intervention management byChildFund staff who oversaw all activitiesrelated to the intervention
6 DMPA commodities including vials sy-ringes cotton soap and sharps boxes
We used key informant interviews recordreviews and periodic progress reports to identifyall intervention-related activities and resourcesand we designed Excel-based spreadsheets toorganize information on the costs of theseresources Most costs reflect actual expendituresexcept for personnel costs which were estimatedusing MOH salary scales for positions considered
to be equivalent to those of research and projectstaff who implemented the intervention
Incremental cost per CYP of CHW provisionof DMPA was calculated by dividing the annual-ized incremental cost of the intervention (that iscosts adjusted for the period of the study) by thenumber of CYPs attributable to the CHW inter-vention This indicator provides a sense of thevalue of resources needed to protect 1 couplefrom pregnancy for a year through DMPAprovided by CHWs in ChildFundrsquos program
FHI 360rsquos Protection of Human SubjectsCommittee and ERES Converge Ethical ReviewBoard in Zambia reviewed and approved thisstudy
RESULTS
Safety of DMPA Provision by CHWsOn the 11-item scale on infection preventionprocedures CHWs initially carried out about 9of the items or 82 on average At their finalassessment the average score increased to aperfect 11 or 100 Thus there was improve-ment from the first to the last DMPA injectionevaluated during the practicum but the startingpoint was high to begin with
For the 10-item injection procedure scale theinitial average score was 74 and at finalassessment the score was 96 Again there wasimprovement but it is important to note thatCHWs who scored low in the initial assessmentimproved markedly by the last assessment Thisis captured by the narrowing of the range ofscores from the initial to the final assessmentsfor both infection prevention and injectionprocedure (Figure 1)
Only 6 (2) of the 253 DMPA clientsinterviewed after 9 months of data collectionreported any problems with CHW-providedinjections Three could not describe the problem2 reported pain at the injection site and 1 clientdescribed numbness in the arm There were noreports from clients of abscesses or infectionsDuring monitoring and supervision activitiesconducted by ChildFund throughout the studyperiod CHWs also reported to ChildFund andMOH supervisors that they had not found anyabscesses or infections
Acceptability of Method to ClientsThe acceptability of DMPA and CHW-provisionof the method was ascertained by interviewswith 253 clients
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 320
N 94 were very much satisfied with DMPA asa family planning method
N 93 wanted to get another DMPA injection
N 94 of CBD clients who accepted DMPAbetween February and April 2010 received asecond DMPA injection
N 99 wanted to receive their next injectionfrom a CHW
N 98 were satisfied with the way the CBDagent gave them their injection
N 98 would recommend receiving a DMPAinjection from their CBD agent to a friend
Of the 7 of DMPA users who did not wantanother injection the main reasons mentioned
were desire to have a child (35) side effects orproblems with DMPA use (35) and husbandrsquosdisapproval (18) For the 4 women (16) whocould have but did not receive a second injectionthe reasons were dissatisfaction with side effects(n52) and husbandrsquos disapproval (n52) ThusCHW provision of DMPA and the method itselfproved highly acceptable
In interviews with the 40 CHWs 98reported that it was easy to find women whowere interested in receiving DMPA and 80 feltthat it was easy to gain the confidence of thecommunity in their ability to provide DMPAAlthough 89 said that their workload increaseddue to the addition of DMPA to their familyplanning services they reported that the increasewas acceptable and not a burden
FIGURE 1 Safety of CHW Provision of Injectables
Abbreviations CHW community health worker
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 321
Characteristics of Acceptors and FamilyPlanning UptakeData on family planning method uptake wererecorded for a total 4241 family planning clientsin both districts during the 13-month datacollection period The average age of womenwas 28 with a range of 15 to 53 years Clientshad an average of 36 living children with arange of 0 to 14 children
Based on provision of methods by ChildFundCHWs from February 2010 to February 2011 51condom clients 391 pill clients and 2206 DMPAclients would be protected from pregnancy for 1year Uptake of condoms pills and DMPA wasgreater in Mumbwa than Luangwa as themajority of family planning clients (73) werefrom Mumbwa district the more populous areawith a higher contraceptive prevalence rate (40vs 27)10 In both districts condoms conferredthe fewest CYPs while DMPA conferred the most(Table 1)
With regard to new acceptors 41 of CHWclients during the 13-month period were new tofamily planning In this group of 1739 women85 chose DMPA 13 chose oral contraceptivepills and the remaining 2 chose condoms astheir first family planning method Of thecontinuing users 63 reported using pills 30DMPA 6 condoms and the rest unspecified Ofall the family planning clients in the study 82or 3479 women obtained DMPA from a CHWsome time between February 2010 and February2011 About 20 were continuing clients whowere formerly clinic clients and 24 were formerpill and condom users who switched to CHW-provided DMPA
Continuing Method Use for Pills and DMPATo determine continuing method use we exam-ined data from women who obtained DMPA orpills from CHWs during the study who had theopportunitymdashbased on when they startedmdashtouse DMPA or pills for 6 months 9 months or12 months (Figure 2) Continuation for DMPAusers was always higher than for pill users (usingmutually exclusive groups of women with 6 9and 12 month follow-up data) with a significantdifference noted at the 12-month markmdash63 vs47 (Chi-square P001)
Comparison of District Health OfficeStatistics with CHW Uptake DataFigure 3 compares CYP data from district-levelstatistics (which include both clinic and CHWinputs) with records from the ChildFund ZambiaCHWs participating in Luangwa and Mumbwa Itis clear from the comparison that many morecondoms are provided at the clinic than at thecommunity level while pill and DMPA provisionby the 40 CHWs accounts for about half of theCYPs documented by 34 health centers inMumbwa and 10 in Luangwa
Incremental Cost of Intervention and Per CYPTable 2 reports incremental costs of interventionactivities relevant to future scale up The totalincremental costs were US$37300 (in 2010 dol-lars) while the annualized costs adjust some of thecost items to reflect that their effects would extendbeyond the initial year of the intervention Forexample the ToT workshop produced 10 personscapable of training CHWs to provide DMPA butonly 4 of them participated in the pilot therefore
TABLE 1 Couple-Years of Protection (CYP) by CHW-Provided Methods in Study DistrictsFebruary 2010 to February 2011
Districts
CYP provided by Luangwa Mumbwa Total
Condoms 13 38 51
Oral contraceptive pills 96 295 391
Injectable DMPA 727 1479 2206
Total 836 1812 2648
Source FHI 360 Data Retriever RegistersAbbreviation CHW community health worker DMPA depot medroxyprogesterone acetate
Uptake resultsshowed anoverwhelmingpreference forinjectable DMPAover pills andcondoms
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 322
only 40 of the ToT costs are applicable to the pilotFor both training activities the effects are assumedto last for 2 years (requiring periodic refreshertraining) and so we applied one-half of thetraining cost (including practicum expenses) tothe 1-year period of service delivery in the pilotprogram Other activity costs are unchanged Theestimate of annualized incremental cost (whichalso serves as the numerator of the incrementalcost per CYP ratio) was US$24322
The denominator of the cost per CYP ratioreflects the number of CYPs that can be attributedto the intervention All CYPs (373) from newDMPA acceptors are included along with 20additional CYPs that represent increased contra-ceptive protection contributed by women whoswitched to DMPA from the less effective pills andcondoms The remaining CYPs (1813) can beattributed to the intervention if we assume thatthese continuing users would not have returned tothe clinic for DMPA services Figure 4 shows thecost per CYP that can definitively be attributed toCHW provision (US$6189) and the change in cost
per CYP at different levels of DMPA continuationIf we assume that 50 of existing DMPA userscontinued with their method solely because of theimproved access afforded by CHW provision costper CYP would be lower at US$2124 If all userscontinued because of CHW provision cost per CYPwould be US$1103
DISCUSSION
Safe Feasible and AcceptableThis pilot study contributes to the body ofevidence on CHW provision of injectable contra-ception As detailed in the Results section of thisarticle the findings establish the safety feasi-bility and acceptability of CHWs providingDMPA in the Zambian context
Impact on Method Use and ChoiceThe findings also demonstrate the impact ofproviding DMPA through CHWs on method useand choice namely that a sizable number of womenbecame new acceptors of all the methods provided
FIGURE 2 Continued Use of Methods Obtained From CHWs
Abbreviations DMPA depot medroxyprogesterone acetate
Source FHI 360 Data Retriever Registers
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 323
by CHWs Women were also able to switch to a moredesirable method andor service delivery setting
Other Factors Affecting UptakeThe project cannot take full credit for theincrease in DMPA use in the 2 districts following
initiation of the pilot study since the method wasalso available at 44 health clinics However itwas a noteworthy increase made all the morestriking by the fact that provision by the 40CHWs accounted for more than half of the CYPsreported by the District Health Offices from
FIGURE 3 Couple-Years of Protection (CYP) February 2010 to February 2011
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
TABLE 2 Total and Annualized Incremental Costs of the Intervention (4600 Zambia Kwacha 5US$1)
Intervention Activity Total Cost (US$) Annualized Cost (US$)
Training of trainers (N510) 5103 1021
Training of CHWs (N540) 12964 6482
Practicum expenses 4827 2414
Supervision of CHWs 3334 3334
Overall intervention management 3219 3219
DMPA commodities 7853 7853
Total incremental costa 37300 24322aAs noted these estimates do not include costs of planning and design because these are one-time activities that would notbe repeated in scale upAbbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 324
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327
addition to providing family planning servicesChildFund CHWs also deliver health educationon personal hygiene and safe motherhood aswell as sensitize the communitymdashfocusing onmenmdashabout family planning CHWs are bothmen and women with varying levels ofsecondary school education who have beenchosen by community members to provide basicservices at the community level They arevolunteers but receive in-kind remuneration inthe form of materials and equipment (bicyclesraincoats and boots t-shirts bags) and cost-shared animal restocking Their initial familyplanning training conducted over 2 weeks usesthe GoZ curriculum that also includes topics onclientsrsquo rights anatomy and physiology HIVAIDS mode of transmission family life educa-tion male involvement distribution and storageof commodities and more Although they workfor ChildFund these CHWs are affiliated withand supervised by GoZ health center staff (aswell as ChildFund staff) from whom theyobtain family planning commodities and towhom they submit records for inclusion in thedistrict data management system
With ChildFundrsquos assistance we also col-lected information on additional or lsquolsquoincremen-talrsquorsquo costs of adding injectable contraception totheir ongoing CHW provision of condoms andoral contraceptive pills As programs grapple withlimited resources such information is needed toestimate costs of scaling up and to establish thatan intervention provides lsquolsquovalue for moneyrsquorsquoThus this paper not only presents results onthe safety feasibility and acceptability of CHWprovision of DMPA in the Zambian context but italso focuses on the impact and costs of addingDMPA to an established community-basedfamily planning program
The study objectives were to
N Assess CHW ability to provide DMPA injec-tions to clients safely and effectively
N Assess acceptability of and client and CHWsatisfaction with community-based deliveryof DMPA
N Determine the impact of adding DMPA onfamily planning uptake and the proportion ofpill and DMPA users continuing at 6 9 and12 months
N Determine incremental cost per couple-yearof protection (CYP) of adding injectablecontraceptives to the existing CHW program
METHODS
OverviewThe safety of CHW provision of injectableswas measured by DMPA client reports and bya 21-item structured observation checklist(SOC) divided into 2 scales that measuredinfection prevention (11 items) and injectionprocedures (10 items) The SOC was usedduring a clinic-based practicum Feasibilityand acceptability were measured by interviewswith CHWs and a subset of their DMPAclients The impact of adding injectable con-traception to pill and condom provision wasassessed by family planning uptake amongthe clients of trained CHWs from February2010 to February 2011 Costs associated withadding DMPA to CHW-provided family plan-ning services were documented using spread-sheets over the period November 2009 toFebruary 2011
Training and Data CollectionChildFund Zambia selected Mumbwa andLuangwa districtsmdashtwo of ChildFundrsquos hard-to-reach poor communities with limited access tohealth care servicesmdashto participate in the pilotstudy Mumbwa has 34 health centers 8 of whichare in 6 communities served by CHWs involved inthe study Luangwa has 10 health centers andabout 26 health units or health posts 8 of whichhad CHWs involved in the study
Preliminary estimates from Zambiarsquos 2010unpublished census put the population inLuangwa at about 25000 and the 6-communityChildFund catchment area in Mumbwa at about50000 (out of a total district population of218328) The 8 health centers in Mumbwaaffiliated with ChildFund CHWs are staffed by17 providers while the 8 health posts inLuangwa have only 12 staff members reflectinga severe shortage of health care workers AlsoCHWs outnumbered Ministry of Health (MOH)staff in those catchment areas
Forty practicing CHWs (20 from each district)affiliated with the 16 health facilities inMumbwa and Luangwa were trained by mastertrainers from the MOH to safely provide DMPAinjections in addition to the family planningservices they already provided CHWs received5 days of didactic instruction on determiningmethod eligibility (screening) counseling andinformed choice client referral and provision oforal contraceptive pills condoms and DMPA
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 318
CHWs also completed a 2- to 4-week clinic-basedpracticum during which 6 or more DMPAinjections had to be successfully administeredbefore the CHW was allowed to provide injec-tions unsupervised We divided the 21-itemstructured observation checklist used by evalua-tors into its 2 main components and calculated atotal score for safe injections with regard toinfection prevention and to injection procedureEvaluations of the first and last injections givenby each CHW constituted the measures of safety
The training and practicum were conductedon a staggered schedule in Luangwa andMumbwa between December 2009 and January2010 By February 2010 all CHWs were certifiedand their capabilities introduced to their respec-tive communities at an official graduationceremony involving local leaders and ChildFundrepresentatives CHWs were then asked to recordall provision of condoms pills and injectables totheir family planning clients for 13 monthsmdashdistinguishing between new acceptors switchersand continuing users of all methodsmdashusingChildFund Zambiarsquos family planning registermodified to include DMPA
The study teammdashcomprising FHI 360ChildFund Zambia and Ministry of Health staffthe Family Planning Technical Working Group(FPTWG) and other stakeholdersmdashselected thefollowing measures of impact
1 Family planning method uptake (expressedin couple-years of protection or CYPs)
2 Proportion of CHW clients who are newfamily planning and new DMPA acceptors
3 Indicators of family planning method con-tinuation by CHW pill and DMPA clients
4 Comparisons between CYPs provided bystudy CHWs and CYPs recorded by DistrictHealth Offices (DHOs)
Approximately 9 months into data collectionwe interviewed all CHWs and a subset of theirDMPA clients (n5253) who received their firstinjection from a CHW between February andApril 2010 By then CHWs had performedseveral months of DMPA administration andenough time had elapsed for these initial DMPAusers to receive up to 3 injections from a CHW
ChildFund Zambia also selected 6 maleemployeesmdash3 assigned to each districtmdashto per-sonally retrieve family planning data on amonthly basis from the 40 CHWs These men(given bicycles for transportation) were engagedspecifically to cover the distances to and fromCHWsrsquo homes discuss and verify data with theCHWs and transfer the required informationfrom the family planning register to the dataretrieval form developed for the study This formcollected information on
N Method receivedused on the first visit instudy period
N Whether the client was a continuing user ornew family planning acceptor1
N Previous method used
N Number of pill cycles or condoms distributedand the scheduled re-injection date for DMPAclients over the course of the 13-month datacollection period
The 6 data retrievers received instructionfrom the Lusaka-based project coordinator onuse of the data retrieval form and the familyplanning client register Data retrievers also metwith the project coordinator monthly for the firsthalf of data collection then every 2 to 3 monthsthereafter to verify the accuracy of the informa-tion and to submit CHW family planning uptakedata from February 2010 to February 2011
We also obtained family planning statisticsfor pills condoms and DMPA distribution fromthe District Health Offices in Luangwa andMumbwa for the same 13-month time periodThese statistics reportedly included both healthfacility and CHW provision of family planningmethods All analyses were performed with SAS9211
The training materials used in 2009 can be accessed at httpwwwk4healthorgtoolkitscba2isample-community-health-worker-training-curriculum However the content has since beenupdated to emphasize dual protection to prevent STIsHIV and a13-week DMPA re-injection window Originally the Zambia MOHwas following a 12-week policy The FPTWG comprises all local stakeholders interestedinvolvedin family planning including the Zambia MOH UNFPA WHOUSAID JSI (John Snow Inc) ZISSP (Zambia Integrated SystemsStrengthening Program) Marie Stopes International PPAZ(Planned Parenthood Association of Zambia) CHAZ (ChurchesHealth Association of Zambia) World Vision CDC SFH (Societyfor Family Health) and Boston University CYP is the estimated protection provided by contraceptivemethods during a 1-year period Our estimates were based onUSAID conversion factors for units of condoms (120 per CYP) andpill packs (15 cycles per CYP) distributed and DMPA injectionsreceived (4 doses per CYP) CYPs are not routinely calculated byChildFund and were computed solely to meet the objectives of thestudy
1 During the data collection period no women stopped andrestarted a method after 6 months we did not determine uponrecruitment if continuing users entering the study had restarted amethod after 6 months
Study methodsincluded checkliststo measure safeprovision inter-views with CHWsand clients andcost analyses
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 319
Assessment of Incremental Costs of AddingDMPA to the CHW ProgramThe approach to costing the addition of a healthservice intervention to an existing program is toconcentrate on additional or lsquolsquoincrementalrsquorsquo costsonly since costs of the existing program wouldhave been incurred even without the interven-tion Incremental costs of an intervention can beclassified according to 3 phases 1) planningdesigning the intervention 2) preparing forservice delivery and 3) delivering the new orimproved services Each phase comprises a set ofactivities and each activity uses resources suchas time of trainers and providers and medicalsupplies and equipment When costs are attachedto resources used in the intervention the totalincremental cost of the intervention may becalculated Stakeholders may be more interestedin costs of activities relevant to scaling up givingless emphasis to costs in the planning and designphase In our study these activities included thefollowing
1 The training of trainers (ToT) workshop thattrained 10 trainers of which 4 were used forthe CHW training courses in Luangwa andMumbwa
2 The CHW training consisting of 2 workshopseach of which trained 20 CHWs
3 The CHW practicum which included traineemeal allowances and transport refunds forCHW visits to clinic facilities for mentoringand practice in injection technique
4 Supervision of CHWs which took place in2 stages an intensive initial stage whereinteractions were more frequent and longerin duration and a second phase in whichsupervisors checked in with CHWs duringroutine site visits
5 Overall intervention management byChildFund staff who oversaw all activitiesrelated to the intervention
6 DMPA commodities including vials sy-ringes cotton soap and sharps boxes
We used key informant interviews recordreviews and periodic progress reports to identifyall intervention-related activities and resourcesand we designed Excel-based spreadsheets toorganize information on the costs of theseresources Most costs reflect actual expendituresexcept for personnel costs which were estimatedusing MOH salary scales for positions considered
to be equivalent to those of research and projectstaff who implemented the intervention
Incremental cost per CYP of CHW provisionof DMPA was calculated by dividing the annual-ized incremental cost of the intervention (that iscosts adjusted for the period of the study) by thenumber of CYPs attributable to the CHW inter-vention This indicator provides a sense of thevalue of resources needed to protect 1 couplefrom pregnancy for a year through DMPAprovided by CHWs in ChildFundrsquos program
FHI 360rsquos Protection of Human SubjectsCommittee and ERES Converge Ethical ReviewBoard in Zambia reviewed and approved thisstudy
RESULTS
Safety of DMPA Provision by CHWsOn the 11-item scale on infection preventionprocedures CHWs initially carried out about 9of the items or 82 on average At their finalassessment the average score increased to aperfect 11 or 100 Thus there was improve-ment from the first to the last DMPA injectionevaluated during the practicum but the startingpoint was high to begin with
For the 10-item injection procedure scale theinitial average score was 74 and at finalassessment the score was 96 Again there wasimprovement but it is important to note thatCHWs who scored low in the initial assessmentimproved markedly by the last assessment Thisis captured by the narrowing of the range ofscores from the initial to the final assessmentsfor both infection prevention and injectionprocedure (Figure 1)
Only 6 (2) of the 253 DMPA clientsinterviewed after 9 months of data collectionreported any problems with CHW-providedinjections Three could not describe the problem2 reported pain at the injection site and 1 clientdescribed numbness in the arm There were noreports from clients of abscesses or infectionsDuring monitoring and supervision activitiesconducted by ChildFund throughout the studyperiod CHWs also reported to ChildFund andMOH supervisors that they had not found anyabscesses or infections
Acceptability of Method to ClientsThe acceptability of DMPA and CHW-provisionof the method was ascertained by interviewswith 253 clients
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 320
N 94 were very much satisfied with DMPA asa family planning method
N 93 wanted to get another DMPA injection
N 94 of CBD clients who accepted DMPAbetween February and April 2010 received asecond DMPA injection
N 99 wanted to receive their next injectionfrom a CHW
N 98 were satisfied with the way the CBDagent gave them their injection
N 98 would recommend receiving a DMPAinjection from their CBD agent to a friend
Of the 7 of DMPA users who did not wantanother injection the main reasons mentioned
were desire to have a child (35) side effects orproblems with DMPA use (35) and husbandrsquosdisapproval (18) For the 4 women (16) whocould have but did not receive a second injectionthe reasons were dissatisfaction with side effects(n52) and husbandrsquos disapproval (n52) ThusCHW provision of DMPA and the method itselfproved highly acceptable
In interviews with the 40 CHWs 98reported that it was easy to find women whowere interested in receiving DMPA and 80 feltthat it was easy to gain the confidence of thecommunity in their ability to provide DMPAAlthough 89 said that their workload increaseddue to the addition of DMPA to their familyplanning services they reported that the increasewas acceptable and not a burden
FIGURE 1 Safety of CHW Provision of Injectables
Abbreviations CHW community health worker
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 321
Characteristics of Acceptors and FamilyPlanning UptakeData on family planning method uptake wererecorded for a total 4241 family planning clientsin both districts during the 13-month datacollection period The average age of womenwas 28 with a range of 15 to 53 years Clientshad an average of 36 living children with arange of 0 to 14 children
Based on provision of methods by ChildFundCHWs from February 2010 to February 2011 51condom clients 391 pill clients and 2206 DMPAclients would be protected from pregnancy for 1year Uptake of condoms pills and DMPA wasgreater in Mumbwa than Luangwa as themajority of family planning clients (73) werefrom Mumbwa district the more populous areawith a higher contraceptive prevalence rate (40vs 27)10 In both districts condoms conferredthe fewest CYPs while DMPA conferred the most(Table 1)
With regard to new acceptors 41 of CHWclients during the 13-month period were new tofamily planning In this group of 1739 women85 chose DMPA 13 chose oral contraceptivepills and the remaining 2 chose condoms astheir first family planning method Of thecontinuing users 63 reported using pills 30DMPA 6 condoms and the rest unspecified Ofall the family planning clients in the study 82or 3479 women obtained DMPA from a CHWsome time between February 2010 and February2011 About 20 were continuing clients whowere formerly clinic clients and 24 were formerpill and condom users who switched to CHW-provided DMPA
Continuing Method Use for Pills and DMPATo determine continuing method use we exam-ined data from women who obtained DMPA orpills from CHWs during the study who had theopportunitymdashbased on when they startedmdashtouse DMPA or pills for 6 months 9 months or12 months (Figure 2) Continuation for DMPAusers was always higher than for pill users (usingmutually exclusive groups of women with 6 9and 12 month follow-up data) with a significantdifference noted at the 12-month markmdash63 vs47 (Chi-square P001)
Comparison of District Health OfficeStatistics with CHW Uptake DataFigure 3 compares CYP data from district-levelstatistics (which include both clinic and CHWinputs) with records from the ChildFund ZambiaCHWs participating in Luangwa and Mumbwa Itis clear from the comparison that many morecondoms are provided at the clinic than at thecommunity level while pill and DMPA provisionby the 40 CHWs accounts for about half of theCYPs documented by 34 health centers inMumbwa and 10 in Luangwa
Incremental Cost of Intervention and Per CYPTable 2 reports incremental costs of interventionactivities relevant to future scale up The totalincremental costs were US$37300 (in 2010 dol-lars) while the annualized costs adjust some of thecost items to reflect that their effects would extendbeyond the initial year of the intervention Forexample the ToT workshop produced 10 personscapable of training CHWs to provide DMPA butonly 4 of them participated in the pilot therefore
TABLE 1 Couple-Years of Protection (CYP) by CHW-Provided Methods in Study DistrictsFebruary 2010 to February 2011
Districts
CYP provided by Luangwa Mumbwa Total
Condoms 13 38 51
Oral contraceptive pills 96 295 391
Injectable DMPA 727 1479 2206
Total 836 1812 2648
Source FHI 360 Data Retriever RegistersAbbreviation CHW community health worker DMPA depot medroxyprogesterone acetate
Uptake resultsshowed anoverwhelmingpreference forinjectable DMPAover pills andcondoms
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 322
only 40 of the ToT costs are applicable to the pilotFor both training activities the effects are assumedto last for 2 years (requiring periodic refreshertraining) and so we applied one-half of thetraining cost (including practicum expenses) tothe 1-year period of service delivery in the pilotprogram Other activity costs are unchanged Theestimate of annualized incremental cost (whichalso serves as the numerator of the incrementalcost per CYP ratio) was US$24322
The denominator of the cost per CYP ratioreflects the number of CYPs that can be attributedto the intervention All CYPs (373) from newDMPA acceptors are included along with 20additional CYPs that represent increased contra-ceptive protection contributed by women whoswitched to DMPA from the less effective pills andcondoms The remaining CYPs (1813) can beattributed to the intervention if we assume thatthese continuing users would not have returned tothe clinic for DMPA services Figure 4 shows thecost per CYP that can definitively be attributed toCHW provision (US$6189) and the change in cost
per CYP at different levels of DMPA continuationIf we assume that 50 of existing DMPA userscontinued with their method solely because of theimproved access afforded by CHW provision costper CYP would be lower at US$2124 If all userscontinued because of CHW provision cost per CYPwould be US$1103
DISCUSSION
Safe Feasible and AcceptableThis pilot study contributes to the body ofevidence on CHW provision of injectable contra-ception As detailed in the Results section of thisarticle the findings establish the safety feasi-bility and acceptability of CHWs providingDMPA in the Zambian context
Impact on Method Use and ChoiceThe findings also demonstrate the impact ofproviding DMPA through CHWs on method useand choice namely that a sizable number of womenbecame new acceptors of all the methods provided
FIGURE 2 Continued Use of Methods Obtained From CHWs
Abbreviations DMPA depot medroxyprogesterone acetate
Source FHI 360 Data Retriever Registers
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 323
by CHWs Women were also able to switch to a moredesirable method andor service delivery setting
Other Factors Affecting UptakeThe project cannot take full credit for theincrease in DMPA use in the 2 districts following
initiation of the pilot study since the method wasalso available at 44 health clinics However itwas a noteworthy increase made all the morestriking by the fact that provision by the 40CHWs accounted for more than half of the CYPsreported by the District Health Offices from
FIGURE 3 Couple-Years of Protection (CYP) February 2010 to February 2011
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
TABLE 2 Total and Annualized Incremental Costs of the Intervention (4600 Zambia Kwacha 5US$1)
Intervention Activity Total Cost (US$) Annualized Cost (US$)
Training of trainers (N510) 5103 1021
Training of CHWs (N540) 12964 6482
Practicum expenses 4827 2414
Supervision of CHWs 3334 3334
Overall intervention management 3219 3219
DMPA commodities 7853 7853
Total incremental costa 37300 24322aAs noted these estimates do not include costs of planning and design because these are one-time activities that would notbe repeated in scale upAbbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 324
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327

CHWs also completed a 2- to 4-week clinic-basedpracticum during which 6 or more DMPAinjections had to be successfully administeredbefore the CHW was allowed to provide injec-tions unsupervised We divided the 21-itemstructured observation checklist used by evalua-tors into its 2 main components and calculated atotal score for safe injections with regard toinfection prevention and to injection procedureEvaluations of the first and last injections givenby each CHW constituted the measures of safety
The training and practicum were conductedon a staggered schedule in Luangwa andMumbwa between December 2009 and January2010 By February 2010 all CHWs were certifiedand their capabilities introduced to their respec-tive communities at an official graduationceremony involving local leaders and ChildFundrepresentatives CHWs were then asked to recordall provision of condoms pills and injectables totheir family planning clients for 13 monthsmdashdistinguishing between new acceptors switchersand continuing users of all methodsmdashusingChildFund Zambiarsquos family planning registermodified to include DMPA
The study teammdashcomprising FHI 360ChildFund Zambia and Ministry of Health staffthe Family Planning Technical Working Group(FPTWG) and other stakeholdersmdashselected thefollowing measures of impact
1 Family planning method uptake (expressedin couple-years of protection or CYPs)
2 Proportion of CHW clients who are newfamily planning and new DMPA acceptors
3 Indicators of family planning method con-tinuation by CHW pill and DMPA clients
4 Comparisons between CYPs provided bystudy CHWs and CYPs recorded by DistrictHealth Offices (DHOs)
Approximately 9 months into data collectionwe interviewed all CHWs and a subset of theirDMPA clients (n5253) who received their firstinjection from a CHW between February andApril 2010 By then CHWs had performedseveral months of DMPA administration andenough time had elapsed for these initial DMPAusers to receive up to 3 injections from a CHW
ChildFund Zambia also selected 6 maleemployeesmdash3 assigned to each districtmdashto per-sonally retrieve family planning data on amonthly basis from the 40 CHWs These men(given bicycles for transportation) were engagedspecifically to cover the distances to and fromCHWsrsquo homes discuss and verify data with theCHWs and transfer the required informationfrom the family planning register to the dataretrieval form developed for the study This formcollected information on
N Method receivedused on the first visit instudy period
N Whether the client was a continuing user ornew family planning acceptor1
N Previous method used
N Number of pill cycles or condoms distributedand the scheduled re-injection date for DMPAclients over the course of the 13-month datacollection period
The 6 data retrievers received instructionfrom the Lusaka-based project coordinator onuse of the data retrieval form and the familyplanning client register Data retrievers also metwith the project coordinator monthly for the firsthalf of data collection then every 2 to 3 monthsthereafter to verify the accuracy of the informa-tion and to submit CHW family planning uptakedata from February 2010 to February 2011
We also obtained family planning statisticsfor pills condoms and DMPA distribution fromthe District Health Offices in Luangwa andMumbwa for the same 13-month time periodThese statistics reportedly included both healthfacility and CHW provision of family planningmethods All analyses were performed with SAS9211
The training materials used in 2009 can be accessed at httpwwwk4healthorgtoolkitscba2isample-community-health-worker-training-curriculum However the content has since beenupdated to emphasize dual protection to prevent STIsHIV and a13-week DMPA re-injection window Originally the Zambia MOHwas following a 12-week policy The FPTWG comprises all local stakeholders interestedinvolvedin family planning including the Zambia MOH UNFPA WHOUSAID JSI (John Snow Inc) ZISSP (Zambia Integrated SystemsStrengthening Program) Marie Stopes International PPAZ(Planned Parenthood Association of Zambia) CHAZ (ChurchesHealth Association of Zambia) World Vision CDC SFH (Societyfor Family Health) and Boston University CYP is the estimated protection provided by contraceptivemethods during a 1-year period Our estimates were based onUSAID conversion factors for units of condoms (120 per CYP) andpill packs (15 cycles per CYP) distributed and DMPA injectionsreceived (4 doses per CYP) CYPs are not routinely calculated byChildFund and were computed solely to meet the objectives of thestudy
1 During the data collection period no women stopped andrestarted a method after 6 months we did not determine uponrecruitment if continuing users entering the study had restarted amethod after 6 months
Study methodsincluded checkliststo measure safeprovision inter-views with CHWsand clients andcost analyses
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 319
Assessment of Incremental Costs of AddingDMPA to the CHW ProgramThe approach to costing the addition of a healthservice intervention to an existing program is toconcentrate on additional or lsquolsquoincrementalrsquorsquo costsonly since costs of the existing program wouldhave been incurred even without the interven-tion Incremental costs of an intervention can beclassified according to 3 phases 1) planningdesigning the intervention 2) preparing forservice delivery and 3) delivering the new orimproved services Each phase comprises a set ofactivities and each activity uses resources suchas time of trainers and providers and medicalsupplies and equipment When costs are attachedto resources used in the intervention the totalincremental cost of the intervention may becalculated Stakeholders may be more interestedin costs of activities relevant to scaling up givingless emphasis to costs in the planning and designphase In our study these activities included thefollowing
1 The training of trainers (ToT) workshop thattrained 10 trainers of which 4 were used forthe CHW training courses in Luangwa andMumbwa
2 The CHW training consisting of 2 workshopseach of which trained 20 CHWs
3 The CHW practicum which included traineemeal allowances and transport refunds forCHW visits to clinic facilities for mentoringand practice in injection technique
4 Supervision of CHWs which took place in2 stages an intensive initial stage whereinteractions were more frequent and longerin duration and a second phase in whichsupervisors checked in with CHWs duringroutine site visits
5 Overall intervention management byChildFund staff who oversaw all activitiesrelated to the intervention
6 DMPA commodities including vials sy-ringes cotton soap and sharps boxes
We used key informant interviews recordreviews and periodic progress reports to identifyall intervention-related activities and resourcesand we designed Excel-based spreadsheets toorganize information on the costs of theseresources Most costs reflect actual expendituresexcept for personnel costs which were estimatedusing MOH salary scales for positions considered
to be equivalent to those of research and projectstaff who implemented the intervention
Incremental cost per CYP of CHW provisionof DMPA was calculated by dividing the annual-ized incremental cost of the intervention (that iscosts adjusted for the period of the study) by thenumber of CYPs attributable to the CHW inter-vention This indicator provides a sense of thevalue of resources needed to protect 1 couplefrom pregnancy for a year through DMPAprovided by CHWs in ChildFundrsquos program
FHI 360rsquos Protection of Human SubjectsCommittee and ERES Converge Ethical ReviewBoard in Zambia reviewed and approved thisstudy
RESULTS
Safety of DMPA Provision by CHWsOn the 11-item scale on infection preventionprocedures CHWs initially carried out about 9of the items or 82 on average At their finalassessment the average score increased to aperfect 11 or 100 Thus there was improve-ment from the first to the last DMPA injectionevaluated during the practicum but the startingpoint was high to begin with
For the 10-item injection procedure scale theinitial average score was 74 and at finalassessment the score was 96 Again there wasimprovement but it is important to note thatCHWs who scored low in the initial assessmentimproved markedly by the last assessment Thisis captured by the narrowing of the range ofscores from the initial to the final assessmentsfor both infection prevention and injectionprocedure (Figure 1)
Only 6 (2) of the 253 DMPA clientsinterviewed after 9 months of data collectionreported any problems with CHW-providedinjections Three could not describe the problem2 reported pain at the injection site and 1 clientdescribed numbness in the arm There were noreports from clients of abscesses or infectionsDuring monitoring and supervision activitiesconducted by ChildFund throughout the studyperiod CHWs also reported to ChildFund andMOH supervisors that they had not found anyabscesses or infections
Acceptability of Method to ClientsThe acceptability of DMPA and CHW-provisionof the method was ascertained by interviewswith 253 clients
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 320
N 94 were very much satisfied with DMPA asa family planning method
N 93 wanted to get another DMPA injection
N 94 of CBD clients who accepted DMPAbetween February and April 2010 received asecond DMPA injection
N 99 wanted to receive their next injectionfrom a CHW
N 98 were satisfied with the way the CBDagent gave them their injection
N 98 would recommend receiving a DMPAinjection from their CBD agent to a friend
Of the 7 of DMPA users who did not wantanother injection the main reasons mentioned
were desire to have a child (35) side effects orproblems with DMPA use (35) and husbandrsquosdisapproval (18) For the 4 women (16) whocould have but did not receive a second injectionthe reasons were dissatisfaction with side effects(n52) and husbandrsquos disapproval (n52) ThusCHW provision of DMPA and the method itselfproved highly acceptable
In interviews with the 40 CHWs 98reported that it was easy to find women whowere interested in receiving DMPA and 80 feltthat it was easy to gain the confidence of thecommunity in their ability to provide DMPAAlthough 89 said that their workload increaseddue to the addition of DMPA to their familyplanning services they reported that the increasewas acceptable and not a burden
FIGURE 1 Safety of CHW Provision of Injectables
Abbreviations CHW community health worker
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 321
Characteristics of Acceptors and FamilyPlanning UptakeData on family planning method uptake wererecorded for a total 4241 family planning clientsin both districts during the 13-month datacollection period The average age of womenwas 28 with a range of 15 to 53 years Clientshad an average of 36 living children with arange of 0 to 14 children
Based on provision of methods by ChildFundCHWs from February 2010 to February 2011 51condom clients 391 pill clients and 2206 DMPAclients would be protected from pregnancy for 1year Uptake of condoms pills and DMPA wasgreater in Mumbwa than Luangwa as themajority of family planning clients (73) werefrom Mumbwa district the more populous areawith a higher contraceptive prevalence rate (40vs 27)10 In both districts condoms conferredthe fewest CYPs while DMPA conferred the most(Table 1)
With regard to new acceptors 41 of CHWclients during the 13-month period were new tofamily planning In this group of 1739 women85 chose DMPA 13 chose oral contraceptivepills and the remaining 2 chose condoms astheir first family planning method Of thecontinuing users 63 reported using pills 30DMPA 6 condoms and the rest unspecified Ofall the family planning clients in the study 82or 3479 women obtained DMPA from a CHWsome time between February 2010 and February2011 About 20 were continuing clients whowere formerly clinic clients and 24 were formerpill and condom users who switched to CHW-provided DMPA
Continuing Method Use for Pills and DMPATo determine continuing method use we exam-ined data from women who obtained DMPA orpills from CHWs during the study who had theopportunitymdashbased on when they startedmdashtouse DMPA or pills for 6 months 9 months or12 months (Figure 2) Continuation for DMPAusers was always higher than for pill users (usingmutually exclusive groups of women with 6 9and 12 month follow-up data) with a significantdifference noted at the 12-month markmdash63 vs47 (Chi-square P001)
Comparison of District Health OfficeStatistics with CHW Uptake DataFigure 3 compares CYP data from district-levelstatistics (which include both clinic and CHWinputs) with records from the ChildFund ZambiaCHWs participating in Luangwa and Mumbwa Itis clear from the comparison that many morecondoms are provided at the clinic than at thecommunity level while pill and DMPA provisionby the 40 CHWs accounts for about half of theCYPs documented by 34 health centers inMumbwa and 10 in Luangwa
Incremental Cost of Intervention and Per CYPTable 2 reports incremental costs of interventionactivities relevant to future scale up The totalincremental costs were US$37300 (in 2010 dol-lars) while the annualized costs adjust some of thecost items to reflect that their effects would extendbeyond the initial year of the intervention Forexample the ToT workshop produced 10 personscapable of training CHWs to provide DMPA butonly 4 of them participated in the pilot therefore
TABLE 1 Couple-Years of Protection (CYP) by CHW-Provided Methods in Study DistrictsFebruary 2010 to February 2011
Districts
CYP provided by Luangwa Mumbwa Total
Condoms 13 38 51
Oral contraceptive pills 96 295 391
Injectable DMPA 727 1479 2206
Total 836 1812 2648
Source FHI 360 Data Retriever RegistersAbbreviation CHW community health worker DMPA depot medroxyprogesterone acetate
Uptake resultsshowed anoverwhelmingpreference forinjectable DMPAover pills andcondoms
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 322
only 40 of the ToT costs are applicable to the pilotFor both training activities the effects are assumedto last for 2 years (requiring periodic refreshertraining) and so we applied one-half of thetraining cost (including practicum expenses) tothe 1-year period of service delivery in the pilotprogram Other activity costs are unchanged Theestimate of annualized incremental cost (whichalso serves as the numerator of the incrementalcost per CYP ratio) was US$24322
The denominator of the cost per CYP ratioreflects the number of CYPs that can be attributedto the intervention All CYPs (373) from newDMPA acceptors are included along with 20additional CYPs that represent increased contra-ceptive protection contributed by women whoswitched to DMPA from the less effective pills andcondoms The remaining CYPs (1813) can beattributed to the intervention if we assume thatthese continuing users would not have returned tothe clinic for DMPA services Figure 4 shows thecost per CYP that can definitively be attributed toCHW provision (US$6189) and the change in cost
per CYP at different levels of DMPA continuationIf we assume that 50 of existing DMPA userscontinued with their method solely because of theimproved access afforded by CHW provision costper CYP would be lower at US$2124 If all userscontinued because of CHW provision cost per CYPwould be US$1103
DISCUSSION
Safe Feasible and AcceptableThis pilot study contributes to the body ofevidence on CHW provision of injectable contra-ception As detailed in the Results section of thisarticle the findings establish the safety feasi-bility and acceptability of CHWs providingDMPA in the Zambian context
Impact on Method Use and ChoiceThe findings also demonstrate the impact ofproviding DMPA through CHWs on method useand choice namely that a sizable number of womenbecame new acceptors of all the methods provided
FIGURE 2 Continued Use of Methods Obtained From CHWs
Abbreviations DMPA depot medroxyprogesterone acetate
Source FHI 360 Data Retriever Registers
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 323
by CHWs Women were also able to switch to a moredesirable method andor service delivery setting
Other Factors Affecting UptakeThe project cannot take full credit for theincrease in DMPA use in the 2 districts following
initiation of the pilot study since the method wasalso available at 44 health clinics However itwas a noteworthy increase made all the morestriking by the fact that provision by the 40CHWs accounted for more than half of the CYPsreported by the District Health Offices from
FIGURE 3 Couple-Years of Protection (CYP) February 2010 to February 2011
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
TABLE 2 Total and Annualized Incremental Costs of the Intervention (4600 Zambia Kwacha 5US$1)
Intervention Activity Total Cost (US$) Annualized Cost (US$)
Training of trainers (N510) 5103 1021
Training of CHWs (N540) 12964 6482
Practicum expenses 4827 2414
Supervision of CHWs 3334 3334
Overall intervention management 3219 3219
DMPA commodities 7853 7853
Total incremental costa 37300 24322aAs noted these estimates do not include costs of planning and design because these are one-time activities that would notbe repeated in scale upAbbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 324
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327
Assessment of Incremental Costs of AddingDMPA to the CHW ProgramThe approach to costing the addition of a healthservice intervention to an existing program is toconcentrate on additional or lsquolsquoincrementalrsquorsquo costsonly since costs of the existing program wouldhave been incurred even without the interven-tion Incremental costs of an intervention can beclassified according to 3 phases 1) planningdesigning the intervention 2) preparing forservice delivery and 3) delivering the new orimproved services Each phase comprises a set ofactivities and each activity uses resources suchas time of trainers and providers and medicalsupplies and equipment When costs are attachedto resources used in the intervention the totalincremental cost of the intervention may becalculated Stakeholders may be more interestedin costs of activities relevant to scaling up givingless emphasis to costs in the planning and designphase In our study these activities included thefollowing
1 The training of trainers (ToT) workshop thattrained 10 trainers of which 4 were used forthe CHW training courses in Luangwa andMumbwa
2 The CHW training consisting of 2 workshopseach of which trained 20 CHWs
3 The CHW practicum which included traineemeal allowances and transport refunds forCHW visits to clinic facilities for mentoringand practice in injection technique
4 Supervision of CHWs which took place in2 stages an intensive initial stage whereinteractions were more frequent and longerin duration and a second phase in whichsupervisors checked in with CHWs duringroutine site visits
5 Overall intervention management byChildFund staff who oversaw all activitiesrelated to the intervention
6 DMPA commodities including vials sy-ringes cotton soap and sharps boxes
We used key informant interviews recordreviews and periodic progress reports to identifyall intervention-related activities and resourcesand we designed Excel-based spreadsheets toorganize information on the costs of theseresources Most costs reflect actual expendituresexcept for personnel costs which were estimatedusing MOH salary scales for positions considered
to be equivalent to those of research and projectstaff who implemented the intervention
Incremental cost per CYP of CHW provisionof DMPA was calculated by dividing the annual-ized incremental cost of the intervention (that iscosts adjusted for the period of the study) by thenumber of CYPs attributable to the CHW inter-vention This indicator provides a sense of thevalue of resources needed to protect 1 couplefrom pregnancy for a year through DMPAprovided by CHWs in ChildFundrsquos program
FHI 360rsquos Protection of Human SubjectsCommittee and ERES Converge Ethical ReviewBoard in Zambia reviewed and approved thisstudy
RESULTS
Safety of DMPA Provision by CHWsOn the 11-item scale on infection preventionprocedures CHWs initially carried out about 9of the items or 82 on average At their finalassessment the average score increased to aperfect 11 or 100 Thus there was improve-ment from the first to the last DMPA injectionevaluated during the practicum but the startingpoint was high to begin with
For the 10-item injection procedure scale theinitial average score was 74 and at finalassessment the score was 96 Again there wasimprovement but it is important to note thatCHWs who scored low in the initial assessmentimproved markedly by the last assessment Thisis captured by the narrowing of the range ofscores from the initial to the final assessmentsfor both infection prevention and injectionprocedure (Figure 1)
Only 6 (2) of the 253 DMPA clientsinterviewed after 9 months of data collectionreported any problems with CHW-providedinjections Three could not describe the problem2 reported pain at the injection site and 1 clientdescribed numbness in the arm There were noreports from clients of abscesses or infectionsDuring monitoring and supervision activitiesconducted by ChildFund throughout the studyperiod CHWs also reported to ChildFund andMOH supervisors that they had not found anyabscesses or infections
Acceptability of Method to ClientsThe acceptability of DMPA and CHW-provisionof the method was ascertained by interviewswith 253 clients
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 320
N 94 were very much satisfied with DMPA asa family planning method
N 93 wanted to get another DMPA injection
N 94 of CBD clients who accepted DMPAbetween February and April 2010 received asecond DMPA injection
N 99 wanted to receive their next injectionfrom a CHW
N 98 were satisfied with the way the CBDagent gave them their injection
N 98 would recommend receiving a DMPAinjection from their CBD agent to a friend
Of the 7 of DMPA users who did not wantanother injection the main reasons mentioned
were desire to have a child (35) side effects orproblems with DMPA use (35) and husbandrsquosdisapproval (18) For the 4 women (16) whocould have but did not receive a second injectionthe reasons were dissatisfaction with side effects(n52) and husbandrsquos disapproval (n52) ThusCHW provision of DMPA and the method itselfproved highly acceptable
In interviews with the 40 CHWs 98reported that it was easy to find women whowere interested in receiving DMPA and 80 feltthat it was easy to gain the confidence of thecommunity in their ability to provide DMPAAlthough 89 said that their workload increaseddue to the addition of DMPA to their familyplanning services they reported that the increasewas acceptable and not a burden
FIGURE 1 Safety of CHW Provision of Injectables
Abbreviations CHW community health worker
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 321
Characteristics of Acceptors and FamilyPlanning UptakeData on family planning method uptake wererecorded for a total 4241 family planning clientsin both districts during the 13-month datacollection period The average age of womenwas 28 with a range of 15 to 53 years Clientshad an average of 36 living children with arange of 0 to 14 children
Based on provision of methods by ChildFundCHWs from February 2010 to February 2011 51condom clients 391 pill clients and 2206 DMPAclients would be protected from pregnancy for 1year Uptake of condoms pills and DMPA wasgreater in Mumbwa than Luangwa as themajority of family planning clients (73) werefrom Mumbwa district the more populous areawith a higher contraceptive prevalence rate (40vs 27)10 In both districts condoms conferredthe fewest CYPs while DMPA conferred the most(Table 1)
With regard to new acceptors 41 of CHWclients during the 13-month period were new tofamily planning In this group of 1739 women85 chose DMPA 13 chose oral contraceptivepills and the remaining 2 chose condoms astheir first family planning method Of thecontinuing users 63 reported using pills 30DMPA 6 condoms and the rest unspecified Ofall the family planning clients in the study 82or 3479 women obtained DMPA from a CHWsome time between February 2010 and February2011 About 20 were continuing clients whowere formerly clinic clients and 24 were formerpill and condom users who switched to CHW-provided DMPA
Continuing Method Use for Pills and DMPATo determine continuing method use we exam-ined data from women who obtained DMPA orpills from CHWs during the study who had theopportunitymdashbased on when they startedmdashtouse DMPA or pills for 6 months 9 months or12 months (Figure 2) Continuation for DMPAusers was always higher than for pill users (usingmutually exclusive groups of women with 6 9and 12 month follow-up data) with a significantdifference noted at the 12-month markmdash63 vs47 (Chi-square P001)
Comparison of District Health OfficeStatistics with CHW Uptake DataFigure 3 compares CYP data from district-levelstatistics (which include both clinic and CHWinputs) with records from the ChildFund ZambiaCHWs participating in Luangwa and Mumbwa Itis clear from the comparison that many morecondoms are provided at the clinic than at thecommunity level while pill and DMPA provisionby the 40 CHWs accounts for about half of theCYPs documented by 34 health centers inMumbwa and 10 in Luangwa
Incremental Cost of Intervention and Per CYPTable 2 reports incremental costs of interventionactivities relevant to future scale up The totalincremental costs were US$37300 (in 2010 dol-lars) while the annualized costs adjust some of thecost items to reflect that their effects would extendbeyond the initial year of the intervention Forexample the ToT workshop produced 10 personscapable of training CHWs to provide DMPA butonly 4 of them participated in the pilot therefore
TABLE 1 Couple-Years of Protection (CYP) by CHW-Provided Methods in Study DistrictsFebruary 2010 to February 2011
Districts
CYP provided by Luangwa Mumbwa Total
Condoms 13 38 51
Oral contraceptive pills 96 295 391
Injectable DMPA 727 1479 2206
Total 836 1812 2648
Source FHI 360 Data Retriever RegistersAbbreviation CHW community health worker DMPA depot medroxyprogesterone acetate
Uptake resultsshowed anoverwhelmingpreference forinjectable DMPAover pills andcondoms
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 322
only 40 of the ToT costs are applicable to the pilotFor both training activities the effects are assumedto last for 2 years (requiring periodic refreshertraining) and so we applied one-half of thetraining cost (including practicum expenses) tothe 1-year period of service delivery in the pilotprogram Other activity costs are unchanged Theestimate of annualized incremental cost (whichalso serves as the numerator of the incrementalcost per CYP ratio) was US$24322
The denominator of the cost per CYP ratioreflects the number of CYPs that can be attributedto the intervention All CYPs (373) from newDMPA acceptors are included along with 20additional CYPs that represent increased contra-ceptive protection contributed by women whoswitched to DMPA from the less effective pills andcondoms The remaining CYPs (1813) can beattributed to the intervention if we assume thatthese continuing users would not have returned tothe clinic for DMPA services Figure 4 shows thecost per CYP that can definitively be attributed toCHW provision (US$6189) and the change in cost
per CYP at different levels of DMPA continuationIf we assume that 50 of existing DMPA userscontinued with their method solely because of theimproved access afforded by CHW provision costper CYP would be lower at US$2124 If all userscontinued because of CHW provision cost per CYPwould be US$1103
DISCUSSION
Safe Feasible and AcceptableThis pilot study contributes to the body ofevidence on CHW provision of injectable contra-ception As detailed in the Results section of thisarticle the findings establish the safety feasi-bility and acceptability of CHWs providingDMPA in the Zambian context
Impact on Method Use and ChoiceThe findings also demonstrate the impact ofproviding DMPA through CHWs on method useand choice namely that a sizable number of womenbecame new acceptors of all the methods provided
FIGURE 2 Continued Use of Methods Obtained From CHWs
Abbreviations DMPA depot medroxyprogesterone acetate
Source FHI 360 Data Retriever Registers
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 323
by CHWs Women were also able to switch to a moredesirable method andor service delivery setting
Other Factors Affecting UptakeThe project cannot take full credit for theincrease in DMPA use in the 2 districts following
initiation of the pilot study since the method wasalso available at 44 health clinics However itwas a noteworthy increase made all the morestriking by the fact that provision by the 40CHWs accounted for more than half of the CYPsreported by the District Health Offices from
FIGURE 3 Couple-Years of Protection (CYP) February 2010 to February 2011
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
TABLE 2 Total and Annualized Incremental Costs of the Intervention (4600 Zambia Kwacha 5US$1)
Intervention Activity Total Cost (US$) Annualized Cost (US$)
Training of trainers (N510) 5103 1021
Training of CHWs (N540) 12964 6482
Practicum expenses 4827 2414
Supervision of CHWs 3334 3334
Overall intervention management 3219 3219
DMPA commodities 7853 7853
Total incremental costa 37300 24322aAs noted these estimates do not include costs of planning and design because these are one-time activities that would notbe repeated in scale upAbbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 324
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327
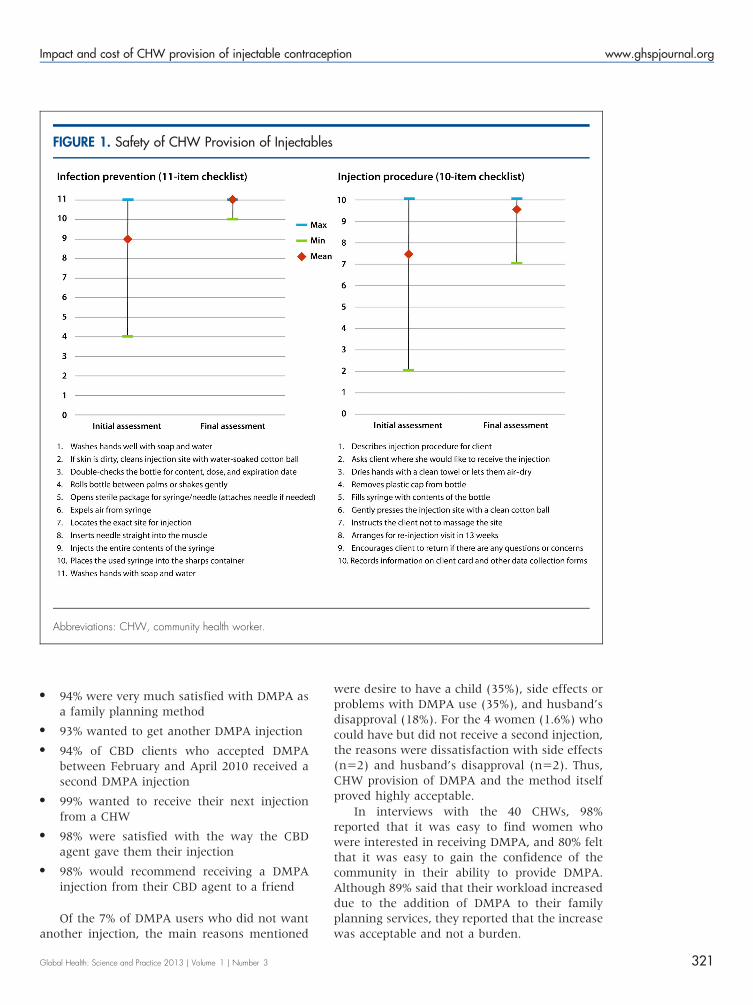
N 94 were very much satisfied with DMPA asa family planning method
N 93 wanted to get another DMPA injection
N 94 of CBD clients who accepted DMPAbetween February and April 2010 received asecond DMPA injection
N 99 wanted to receive their next injectionfrom a CHW
N 98 were satisfied with the way the CBDagent gave them their injection
N 98 would recommend receiving a DMPAinjection from their CBD agent to a friend
Of the 7 of DMPA users who did not wantanother injection the main reasons mentioned
were desire to have a child (35) side effects orproblems with DMPA use (35) and husbandrsquosdisapproval (18) For the 4 women (16) whocould have but did not receive a second injectionthe reasons were dissatisfaction with side effects(n52) and husbandrsquos disapproval (n52) ThusCHW provision of DMPA and the method itselfproved highly acceptable
In interviews with the 40 CHWs 98reported that it was easy to find women whowere interested in receiving DMPA and 80 feltthat it was easy to gain the confidence of thecommunity in their ability to provide DMPAAlthough 89 said that their workload increaseddue to the addition of DMPA to their familyplanning services they reported that the increasewas acceptable and not a burden
FIGURE 1 Safety of CHW Provision of Injectables
Abbreviations CHW community health worker
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 321
Characteristics of Acceptors and FamilyPlanning UptakeData on family planning method uptake wererecorded for a total 4241 family planning clientsin both districts during the 13-month datacollection period The average age of womenwas 28 with a range of 15 to 53 years Clientshad an average of 36 living children with arange of 0 to 14 children
Based on provision of methods by ChildFundCHWs from February 2010 to February 2011 51condom clients 391 pill clients and 2206 DMPAclients would be protected from pregnancy for 1year Uptake of condoms pills and DMPA wasgreater in Mumbwa than Luangwa as themajority of family planning clients (73) werefrom Mumbwa district the more populous areawith a higher contraceptive prevalence rate (40vs 27)10 In both districts condoms conferredthe fewest CYPs while DMPA conferred the most(Table 1)
With regard to new acceptors 41 of CHWclients during the 13-month period were new tofamily planning In this group of 1739 women85 chose DMPA 13 chose oral contraceptivepills and the remaining 2 chose condoms astheir first family planning method Of thecontinuing users 63 reported using pills 30DMPA 6 condoms and the rest unspecified Ofall the family planning clients in the study 82or 3479 women obtained DMPA from a CHWsome time between February 2010 and February2011 About 20 were continuing clients whowere formerly clinic clients and 24 were formerpill and condom users who switched to CHW-provided DMPA
Continuing Method Use for Pills and DMPATo determine continuing method use we exam-ined data from women who obtained DMPA orpills from CHWs during the study who had theopportunitymdashbased on when they startedmdashtouse DMPA or pills for 6 months 9 months or12 months (Figure 2) Continuation for DMPAusers was always higher than for pill users (usingmutually exclusive groups of women with 6 9and 12 month follow-up data) with a significantdifference noted at the 12-month markmdash63 vs47 (Chi-square P001)
Comparison of District Health OfficeStatistics with CHW Uptake DataFigure 3 compares CYP data from district-levelstatistics (which include both clinic and CHWinputs) with records from the ChildFund ZambiaCHWs participating in Luangwa and Mumbwa Itis clear from the comparison that many morecondoms are provided at the clinic than at thecommunity level while pill and DMPA provisionby the 40 CHWs accounts for about half of theCYPs documented by 34 health centers inMumbwa and 10 in Luangwa
Incremental Cost of Intervention and Per CYPTable 2 reports incremental costs of interventionactivities relevant to future scale up The totalincremental costs were US$37300 (in 2010 dol-lars) while the annualized costs adjust some of thecost items to reflect that their effects would extendbeyond the initial year of the intervention Forexample the ToT workshop produced 10 personscapable of training CHWs to provide DMPA butonly 4 of them participated in the pilot therefore
TABLE 1 Couple-Years of Protection (CYP) by CHW-Provided Methods in Study DistrictsFebruary 2010 to February 2011
Districts
CYP provided by Luangwa Mumbwa Total
Condoms 13 38 51
Oral contraceptive pills 96 295 391
Injectable DMPA 727 1479 2206
Total 836 1812 2648
Source FHI 360 Data Retriever RegistersAbbreviation CHW community health worker DMPA depot medroxyprogesterone acetate
Uptake resultsshowed anoverwhelmingpreference forinjectable DMPAover pills andcondoms
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 322
only 40 of the ToT costs are applicable to the pilotFor both training activities the effects are assumedto last for 2 years (requiring periodic refreshertraining) and so we applied one-half of thetraining cost (including practicum expenses) tothe 1-year period of service delivery in the pilotprogram Other activity costs are unchanged Theestimate of annualized incremental cost (whichalso serves as the numerator of the incrementalcost per CYP ratio) was US$24322
The denominator of the cost per CYP ratioreflects the number of CYPs that can be attributedto the intervention All CYPs (373) from newDMPA acceptors are included along with 20additional CYPs that represent increased contra-ceptive protection contributed by women whoswitched to DMPA from the less effective pills andcondoms The remaining CYPs (1813) can beattributed to the intervention if we assume thatthese continuing users would not have returned tothe clinic for DMPA services Figure 4 shows thecost per CYP that can definitively be attributed toCHW provision (US$6189) and the change in cost
per CYP at different levels of DMPA continuationIf we assume that 50 of existing DMPA userscontinued with their method solely because of theimproved access afforded by CHW provision costper CYP would be lower at US$2124 If all userscontinued because of CHW provision cost per CYPwould be US$1103
DISCUSSION
Safe Feasible and AcceptableThis pilot study contributes to the body ofevidence on CHW provision of injectable contra-ception As detailed in the Results section of thisarticle the findings establish the safety feasi-bility and acceptability of CHWs providingDMPA in the Zambian context
Impact on Method Use and ChoiceThe findings also demonstrate the impact ofproviding DMPA through CHWs on method useand choice namely that a sizable number of womenbecame new acceptors of all the methods provided
FIGURE 2 Continued Use of Methods Obtained From CHWs
Abbreviations DMPA depot medroxyprogesterone acetate
Source FHI 360 Data Retriever Registers
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 323
by CHWs Women were also able to switch to a moredesirable method andor service delivery setting
Other Factors Affecting UptakeThe project cannot take full credit for theincrease in DMPA use in the 2 districts following
initiation of the pilot study since the method wasalso available at 44 health clinics However itwas a noteworthy increase made all the morestriking by the fact that provision by the 40CHWs accounted for more than half of the CYPsreported by the District Health Offices from
FIGURE 3 Couple-Years of Protection (CYP) February 2010 to February 2011
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
TABLE 2 Total and Annualized Incremental Costs of the Intervention (4600 Zambia Kwacha 5US$1)
Intervention Activity Total Cost (US$) Annualized Cost (US$)
Training of trainers (N510) 5103 1021
Training of CHWs (N540) 12964 6482
Practicum expenses 4827 2414
Supervision of CHWs 3334 3334
Overall intervention management 3219 3219
DMPA commodities 7853 7853
Total incremental costa 37300 24322aAs noted these estimates do not include costs of planning and design because these are one-time activities that would notbe repeated in scale upAbbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 324
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327
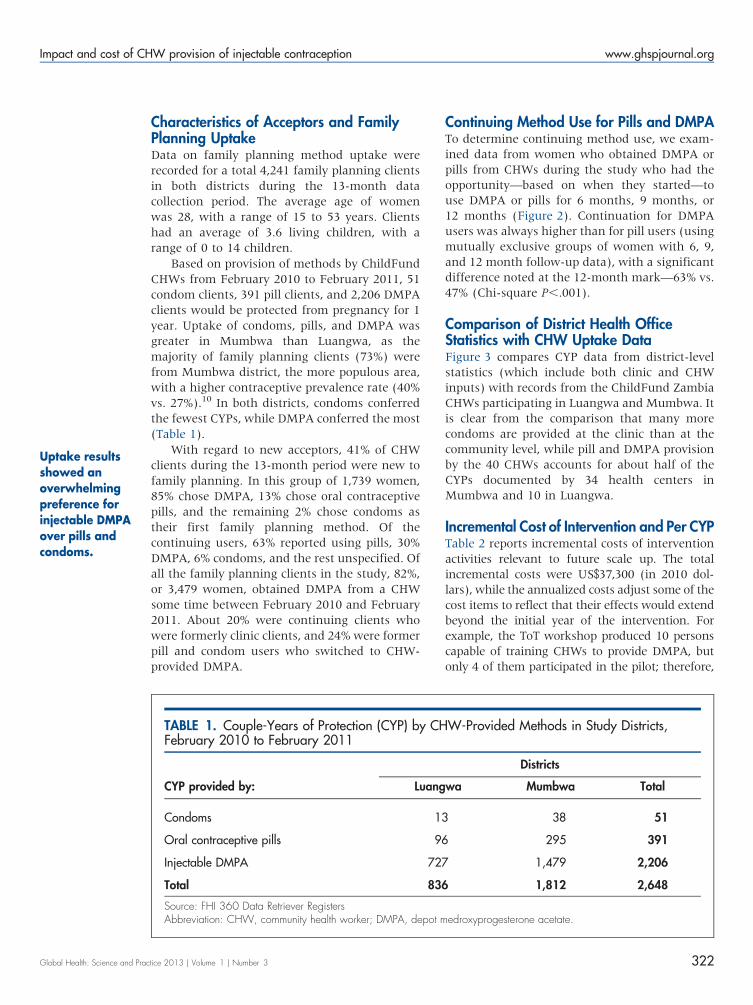
Characteristics of Acceptors and FamilyPlanning UptakeData on family planning method uptake wererecorded for a total 4241 family planning clientsin both districts during the 13-month datacollection period The average age of womenwas 28 with a range of 15 to 53 years Clientshad an average of 36 living children with arange of 0 to 14 children
Based on provision of methods by ChildFundCHWs from February 2010 to February 2011 51condom clients 391 pill clients and 2206 DMPAclients would be protected from pregnancy for 1year Uptake of condoms pills and DMPA wasgreater in Mumbwa than Luangwa as themajority of family planning clients (73) werefrom Mumbwa district the more populous areawith a higher contraceptive prevalence rate (40vs 27)10 In both districts condoms conferredthe fewest CYPs while DMPA conferred the most(Table 1)
With regard to new acceptors 41 of CHWclients during the 13-month period were new tofamily planning In this group of 1739 women85 chose DMPA 13 chose oral contraceptivepills and the remaining 2 chose condoms astheir first family planning method Of thecontinuing users 63 reported using pills 30DMPA 6 condoms and the rest unspecified Ofall the family planning clients in the study 82or 3479 women obtained DMPA from a CHWsome time between February 2010 and February2011 About 20 were continuing clients whowere formerly clinic clients and 24 were formerpill and condom users who switched to CHW-provided DMPA
Continuing Method Use for Pills and DMPATo determine continuing method use we exam-ined data from women who obtained DMPA orpills from CHWs during the study who had theopportunitymdashbased on when they startedmdashtouse DMPA or pills for 6 months 9 months or12 months (Figure 2) Continuation for DMPAusers was always higher than for pill users (usingmutually exclusive groups of women with 6 9and 12 month follow-up data) with a significantdifference noted at the 12-month markmdash63 vs47 (Chi-square P001)
Comparison of District Health OfficeStatistics with CHW Uptake DataFigure 3 compares CYP data from district-levelstatistics (which include both clinic and CHWinputs) with records from the ChildFund ZambiaCHWs participating in Luangwa and Mumbwa Itis clear from the comparison that many morecondoms are provided at the clinic than at thecommunity level while pill and DMPA provisionby the 40 CHWs accounts for about half of theCYPs documented by 34 health centers inMumbwa and 10 in Luangwa
Incremental Cost of Intervention and Per CYPTable 2 reports incremental costs of interventionactivities relevant to future scale up The totalincremental costs were US$37300 (in 2010 dol-lars) while the annualized costs adjust some of thecost items to reflect that their effects would extendbeyond the initial year of the intervention Forexample the ToT workshop produced 10 personscapable of training CHWs to provide DMPA butonly 4 of them participated in the pilot therefore
TABLE 1 Couple-Years of Protection (CYP) by CHW-Provided Methods in Study DistrictsFebruary 2010 to February 2011
Districts
CYP provided by Luangwa Mumbwa Total
Condoms 13 38 51
Oral contraceptive pills 96 295 391
Injectable DMPA 727 1479 2206
Total 836 1812 2648
Source FHI 360 Data Retriever RegistersAbbreviation CHW community health worker DMPA depot medroxyprogesterone acetate
Uptake resultsshowed anoverwhelmingpreference forinjectable DMPAover pills andcondoms
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 322
only 40 of the ToT costs are applicable to the pilotFor both training activities the effects are assumedto last for 2 years (requiring periodic refreshertraining) and so we applied one-half of thetraining cost (including practicum expenses) tothe 1-year period of service delivery in the pilotprogram Other activity costs are unchanged Theestimate of annualized incremental cost (whichalso serves as the numerator of the incrementalcost per CYP ratio) was US$24322
The denominator of the cost per CYP ratioreflects the number of CYPs that can be attributedto the intervention All CYPs (373) from newDMPA acceptors are included along with 20additional CYPs that represent increased contra-ceptive protection contributed by women whoswitched to DMPA from the less effective pills andcondoms The remaining CYPs (1813) can beattributed to the intervention if we assume thatthese continuing users would not have returned tothe clinic for DMPA services Figure 4 shows thecost per CYP that can definitively be attributed toCHW provision (US$6189) and the change in cost
per CYP at different levels of DMPA continuationIf we assume that 50 of existing DMPA userscontinued with their method solely because of theimproved access afforded by CHW provision costper CYP would be lower at US$2124 If all userscontinued because of CHW provision cost per CYPwould be US$1103
DISCUSSION
Safe Feasible and AcceptableThis pilot study contributes to the body ofevidence on CHW provision of injectable contra-ception As detailed in the Results section of thisarticle the findings establish the safety feasi-bility and acceptability of CHWs providingDMPA in the Zambian context
Impact on Method Use and ChoiceThe findings also demonstrate the impact ofproviding DMPA through CHWs on method useand choice namely that a sizable number of womenbecame new acceptors of all the methods provided
FIGURE 2 Continued Use of Methods Obtained From CHWs
Abbreviations DMPA depot medroxyprogesterone acetate
Source FHI 360 Data Retriever Registers
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 323
by CHWs Women were also able to switch to a moredesirable method andor service delivery setting
Other Factors Affecting UptakeThe project cannot take full credit for theincrease in DMPA use in the 2 districts following
initiation of the pilot study since the method wasalso available at 44 health clinics However itwas a noteworthy increase made all the morestriking by the fact that provision by the 40CHWs accounted for more than half of the CYPsreported by the District Health Offices from
FIGURE 3 Couple-Years of Protection (CYP) February 2010 to February 2011
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
TABLE 2 Total and Annualized Incremental Costs of the Intervention (4600 Zambia Kwacha 5US$1)
Intervention Activity Total Cost (US$) Annualized Cost (US$)
Training of trainers (N510) 5103 1021
Training of CHWs (N540) 12964 6482
Practicum expenses 4827 2414
Supervision of CHWs 3334 3334
Overall intervention management 3219 3219
DMPA commodities 7853 7853
Total incremental costa 37300 24322aAs noted these estimates do not include costs of planning and design because these are one-time activities that would notbe repeated in scale upAbbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 324
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327
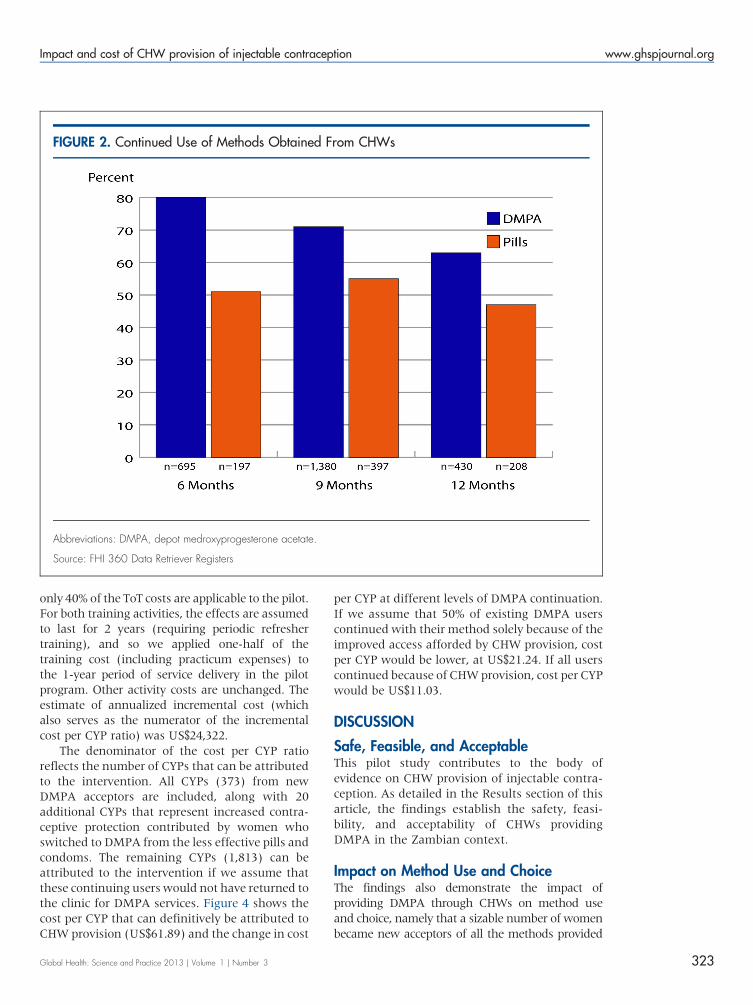
only 40 of the ToT costs are applicable to the pilotFor both training activities the effects are assumedto last for 2 years (requiring periodic refreshertraining) and so we applied one-half of thetraining cost (including practicum expenses) tothe 1-year period of service delivery in the pilotprogram Other activity costs are unchanged Theestimate of annualized incremental cost (whichalso serves as the numerator of the incrementalcost per CYP ratio) was US$24322
The denominator of the cost per CYP ratioreflects the number of CYPs that can be attributedto the intervention All CYPs (373) from newDMPA acceptors are included along with 20additional CYPs that represent increased contra-ceptive protection contributed by women whoswitched to DMPA from the less effective pills andcondoms The remaining CYPs (1813) can beattributed to the intervention if we assume thatthese continuing users would not have returned tothe clinic for DMPA services Figure 4 shows thecost per CYP that can definitively be attributed toCHW provision (US$6189) and the change in cost
per CYP at different levels of DMPA continuationIf we assume that 50 of existing DMPA userscontinued with their method solely because of theimproved access afforded by CHW provision costper CYP would be lower at US$2124 If all userscontinued because of CHW provision cost per CYPwould be US$1103
DISCUSSION
Safe Feasible and AcceptableThis pilot study contributes to the body ofevidence on CHW provision of injectable contra-ception As detailed in the Results section of thisarticle the findings establish the safety feasi-bility and acceptability of CHWs providingDMPA in the Zambian context
Impact on Method Use and ChoiceThe findings also demonstrate the impact ofproviding DMPA through CHWs on method useand choice namely that a sizable number of womenbecame new acceptors of all the methods provided
FIGURE 2 Continued Use of Methods Obtained From CHWs
Abbreviations DMPA depot medroxyprogesterone acetate
Source FHI 360 Data Retriever Registers
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 323
by CHWs Women were also able to switch to a moredesirable method andor service delivery setting
Other Factors Affecting UptakeThe project cannot take full credit for theincrease in DMPA use in the 2 districts following
initiation of the pilot study since the method wasalso available at 44 health clinics However itwas a noteworthy increase made all the morestriking by the fact that provision by the 40CHWs accounted for more than half of the CYPsreported by the District Health Offices from
FIGURE 3 Couple-Years of Protection (CYP) February 2010 to February 2011
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
TABLE 2 Total and Annualized Incremental Costs of the Intervention (4600 Zambia Kwacha 5US$1)
Intervention Activity Total Cost (US$) Annualized Cost (US$)
Training of trainers (N510) 5103 1021
Training of CHWs (N540) 12964 6482
Practicum expenses 4827 2414
Supervision of CHWs 3334 3334
Overall intervention management 3219 3219
DMPA commodities 7853 7853
Total incremental costa 37300 24322aAs noted these estimates do not include costs of planning and design because these are one-time activities that would notbe repeated in scale upAbbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 324
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327
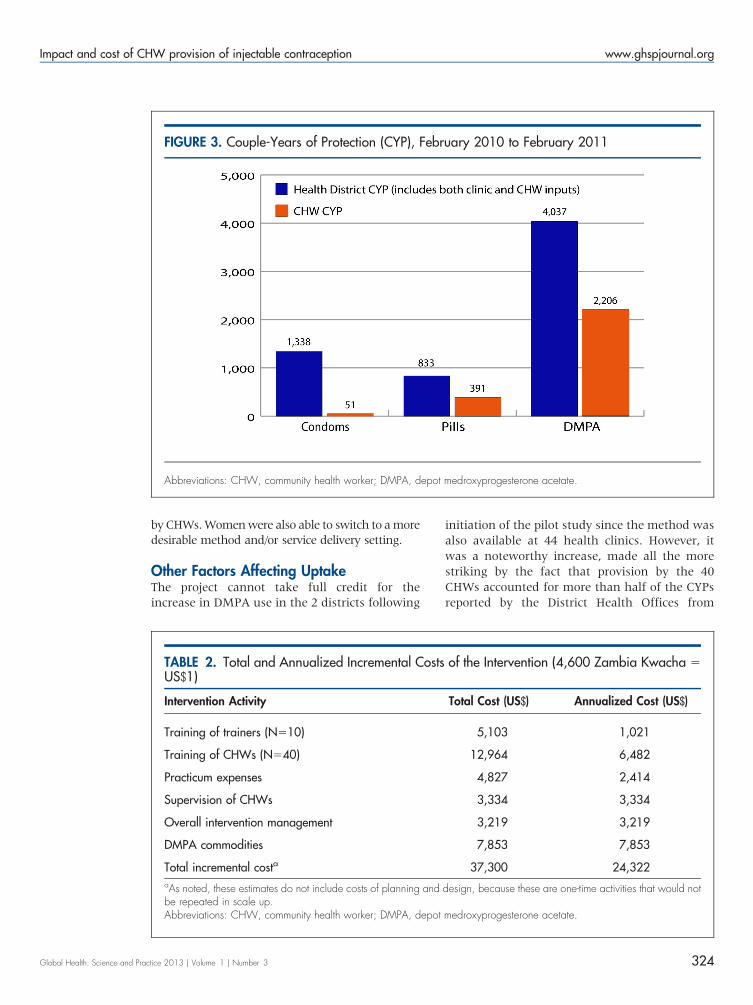
by CHWs Women were also able to switch to a moredesirable method andor service delivery setting
Other Factors Affecting UptakeThe project cannot take full credit for theincrease in DMPA use in the 2 districts following
initiation of the pilot study since the method wasalso available at 44 health clinics However itwas a noteworthy increase made all the morestriking by the fact that provision by the 40CHWs accounted for more than half of the CYPsreported by the District Health Offices from
FIGURE 3 Couple-Years of Protection (CYP) February 2010 to February 2011
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
TABLE 2 Total and Annualized Incremental Costs of the Intervention (4600 Zambia Kwacha 5US$1)
Intervention Activity Total Cost (US$) Annualized Cost (US$)
Training of trainers (N510) 5103 1021
Training of CHWs (N540) 12964 6482
Practicum expenses 4827 2414
Supervision of CHWs 3334 3334
Overall intervention management 3219 3219
DMPA commodities 7853 7853
Total incremental costa 37300 24322aAs noted these estimates do not include costs of planning and design because these are one-time activities that would notbe repeated in scale upAbbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 324
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327
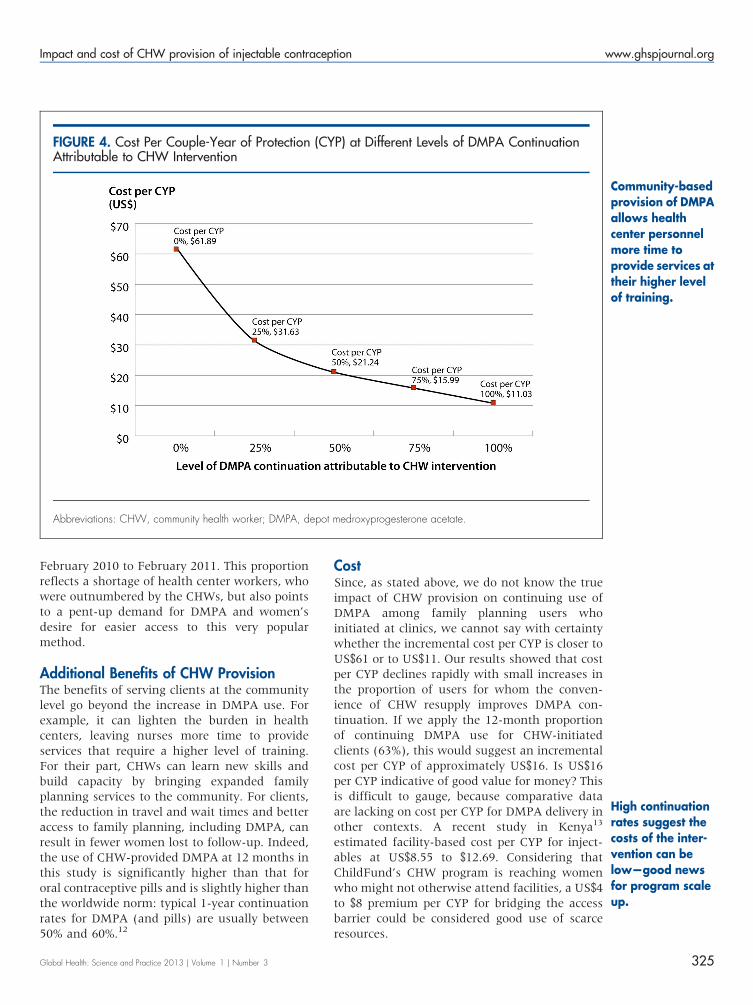
February 2010 to February 2011 This proportionreflects a shortage of health center workers whowere outnumbered by the CHWs but also pointsto a pent-up demand for DMPA and womenrsquosdesire for easier access to this very popularmethod
Additional Benefits of CHW ProvisionThe benefits of serving clients at the communitylevel go beyond the increase in DMPA use Forexample it can lighten the burden in healthcenters leaving nurses more time to provideservices that require a higher level of trainingFor their part CHWs can learn new skills andbuild capacity by bringing expanded familyplanning services to the community For clientsthe reduction in travel and wait times and betteraccess to family planning including DMPA canresult in fewer women lost to follow-up Indeedthe use of CHW-provided DMPA at 12 months inthis study is significantly higher than that fororal contraceptive pills and is slightly higher thanthe worldwide norm typical 1-year continuationrates for DMPA (and pills) are usually between50 and 6012
CostSince as stated above we do not know the trueimpact of CHW provision on continuing use ofDMPA among family planning users whoinitiated at clinics we cannot say with certaintywhether the incremental cost per CYP is closer toUS$61 or to US$11 Our results showed that costper CYP declines rapidly with small increases inthe proportion of users for whom the conven-ience of CHW resupply improves DMPA con-tinuation If we apply the 12-month proportionof continuing DMPA use for CHW-initiatedclients (63) this would suggest an incrementalcost per CYP of approximately US$16 Is US$16per CYP indicative of good value for money Thisis difficult to gauge because comparative dataare lacking on cost per CYP for DMPA delivery inother contexts A recent study in Kenya13
estimated facility-based cost per CYP for inject-ables at US$855 to $1269 Considering thatChildFundrsquos CHW program is reaching womenwho might not otherwise attend facilities a US$4to $8 premium per CYP for bridging the accessbarrier could be considered good use of scarceresources
FIGURE 4 Cost Per Couple-Year of Protection (CYP) at Different Levels of DMPA ContinuationAttributable to CHW Intervention
Abbreviations CHW community health worker DMPA depot medroxyprogesterone acetate
Community-basedprovision of DMPAallows healthcenter personnelmore time toprovide services attheir higher levelof training
High continuationrates suggest thecosts of the inter-vention can belowmdashgood newsfor program scaleup
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 325
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327
BOX From Research to Program Implementation
Strong Stakeholder LeadershipIn May 2011 the Zambian MOH convened a meeting to present the results of the study on the safety feasibility andacceptability of DMPA provision by CHWs to discuss the implications of the results and to chart the way forward TheFPTWG had helped sustain interest in the pilot study by disseminating progress reports acting as liaison between theresearch team and the MOH and helping to reduce obstacles throughout study implementation The MOH agreed tocontinue service delivery in the pilot districts without interruption to revise the National Health Policy to allow provision ofDMPA by CHWs and to develop a lsquolsquoRoad Map for National Scale Uprsquorsquo document lsquolsquoThe Road Maprsquorsquo drafted by the MOHand partners was endorsed by a larger group of stakeholders in October 2011
With support from USAIDZambia preparations for the first phase of scale up began in October 2011 with activitiesbeginning in January 2012 that included continued service delivery in the pilot sites expansion to new sites within the pilotdistricts and expansion to new sites in 1 new district (Nyimba) FHI 360 and ChildFund conducted qualitative andquantitative monitoring and evaluation activities provided technical assistance to the MOH and the Ministry of CommunityDevelopment Maternal amp Child Health and facilitated dialogue among stakeholders regarding the policy change topermit CHWs to administer DMPA In the early scale-up phase 72 CHWs were newly trained to administer DMPA andnow are providing family planning services to their communities
Ministry-level support for scaling up community-based provision of DMPA was very strong in the immediate post-study phaseThis was due in large part to deliberate efforts to engage key stakeholders and influence decision makers from the earliest stagesof the research process in 2009 and to maintain that engagement throughout the entire study Without such concerted efforts toinvolve stakeholders from the beginning of the studymdashand the FPTWGrsquos pivotal role in recommending policy changes and scaleup in Zambiamdashit is unlikely that the translation of this studyrsquos findings into practice would have occurred so rapidly
Study Tour to Sustain MomentumHowever the general elections immediately following the October 2011 stakeholder meeting led to changes in leadershipwithin the MOH and the creation of a new Ministry of Community Development Mother amp Child Health These changesdecelerated the momentum of the early scale-up process FHI 360 ChildFund Zambia and USAIDZambia worked toorient new leadership to the project and cultivate a renewed sense of ownership As part of these efforts a delegation ofZambian stakeholders traveled to Rwanda for a south-to-south tour to observe Rwandarsquos robust community-based familyplanning program and engage with stakeholders around important policy-level and operational issues The study toureffectively improved country-level ownership of the replication process and allowed professional bodies donorsimplementers and key personnel from both ministries to learn from Rwandarsquos experience and develop plans for movingahead with CHW provision of DMPA in Zambia Many stakeholders are strongly advocating a policy change in 2013
Replicability to Other SettingsIt should be noted that this pilot study was implemented within an established CHW program operated by an NGO thatalready had a family planning program in place and with clients who actively sought these services from their CHWs Assuch the intervention was carried out in what could be considered an ideal setting For that reason our positive resultsmay not be replicable to the same degree especially if similar conditions and political will are absent Nevertheless thispilot demonstrated 1) the value of investing in a program where the need for DMPA is ably addressed by a trained cadreof lower-level family planning providers and 2) the successful expansion of CHW provision of DMPA through effectiveand continuous collaboration of research practice and advocacy
Sustaining CommitmentIn Zambia the potential for this practice to be widely replicated and sustainable is increased in part by a resurgent globalinterest in family planning Country-level commitments and support arose out of the highly visible 2012 London Summit onFamily Planning Among them the GoZ pledged to increase contraceptive prevalence through various strategiesincluding reducing barriers to task sharing and doubling budget allocations for family planning Most recently at the 2013Women Deliver conference the First Lady of Zambia Her Excellency Dr Christine Kaseba-Sata emphasized hercommitment to creating a supportive environment for task sharing and ensuring the scale up of CHW provision of familyplanning including DMPA Scale up has already begun in 3 districts with USAIDZambia funding and is expected tocontinue with appropriate adaptations that will facilitate large-scale expansion especially as government ownership andfunding increase
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 326
Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327

Indications of Future DemandProspects for increasing CHW-initiated and resup-plied DMPA in Zambia are very promising (For adescription of the scale-up work already underwayin Zambia see the box) Once the word spread thatcertain CHWs were providing DMPA womenflocked to them for the method includingresidents of Nangoma Mumbwa where thehealth center is affiliated with the CatholicChurch and family planning services are notprovided In Luangwa some women (not includedin our data capture) came to our trained CHWsfrom neighboring Zimbabwe and Mozambiquesince the GoZ provides these services free-of-charge to anyone Therefore it was easy for CHWsto find women who wanted to use DMPA
LIMITATIONS OF THE STUDY
As is often the case family planning statisticsobtained at the district level may be incompletebut to the best of our knowledge all healthcenters in the districts were included Never-theless it is possible that not all clinics and allCHWs reliably and consistently submitted theirmonthly forms to the DHO for the time periodunder study As such the data may under-represent the true contributions of clinics andorCHWs who were not involved in the pilot
Acknowledgments Financial assistance was provided by USAIDunder the terms of Cooperative Agreement GPO-A-OO-O8-OOOO1-OO Program Research for Strengthening Services(PROGRESS)
Competing Interests None declared
REFERENCES1 World Health Organization (WHO) Working together for
health the World Health Report 2006 Geneva WHO 2006Available from httpwwwwhointwhr2006whr06_enpdf
2 Irin PlusNews ZIMBABWE nurses step up to initiate HIVtreatment 2013 [cited 2013 Feb 5] Available from httpwwwplusnewsorgReport96561ZIMBABWE-Nurses-step-up-to-initiate-HIV-treatment
3 Asnake M Henry EG Tilahun Y Oliveras E Addressing unmetneed for long-acting family planning in Ethiopia uptake ofImplanon and characteristics of users Watertown MAPathfinder International 2012 Available from httpwwwpathfinderorgpublications-toolsaddressing-unmet-need-for-Long-Acting-Family-Planning-in-Ethiopiahtml
4 Stanback J Spieler J Shah I Finger WR Community-basedhealth workers can safely and effectively administer injectablecontraceptives conclusions from a technical consultationContraception 201081(3)181ndash4 Epub 2010 Feb 18CrossRef Medline
5 World Health Organization (WHO) WHO recommendationsoptimizing health worker roles to improve access to key maternaland newborn health interventions through task shifting GenevaWHO 2012 Available from httpappswhointirisbitstream106657776419789241504843_engpdf
6 FHI 360 Status of CBA2I in Africa August 2012 K4Health2012 Available from httparchivek4healthorgsitesdefaultfilesCBA2I20Africa20Map_28Aug2012pdf
7 Hoke T Brunie A Krueger K Dreisbach C Akol A Rabenja NLet al Community-based distribution of injectable contraceptivesintroduction strategies in four sub-Saharan African countries IntPerspect Sex Reprod Health 201238(4)2149 Epub 2013 Jan16 CrossRef Medline
8 Malarcher S Meirik O Lebetkin E Shah I Spieler J Stanback JProvision of DMPA by community health workers what theevidence shows Contraception 201183(6)495ndash503 Epub2011 May 17 CrossRef Medline
9 FHI 360 Expanding community-based access to injectablesinitiatives in selected sub-Saharan African countries DurhamNC FHI 360 2012 Available from httparchivek4healthorgsitesdefaultfilesSummary_of_Country_Programs_23March2012_0pdf
10 Zambia Central Statistical Office (CSO) Ministry of Health (MOH)Tropical Diseases Research Centre (TDRC) University of ZambiaMacro International Inc Zambia Demographic and Health Survey2007 Calverton MD USA CSO and Macro International Inc2009 Available from httpwwwmeasuredhscompubspdfFR211FR211[revised-05-12-2009]pdf
11 SAS Institute SAS Release 92 Cary NC SAS Institute 2011
12 Ali MM Cleland J Shah I Causes and consequences ofcontraceptive discontinuation evidence from 60 Demographicand Health Surveys Geneva WHO 2012 Available fromhttpwwwwhointreproductivehealthpublicationsfamily_planning9789241504058enindexhtml
13 USAID Health Policy Initiative The cost of family planning inKenya Washington DC USAID 2010 Available fromhttpwwwhealthpolicyinitiativecomPublicationsDocuments1189_1_1189_1_Kenya_Brief_FINAL_7_12_10_accpdf
______________________________________________________________________Peer Reviewed
Received 2013 Mar 13 Accepted 2013 Jul 5 First Published Online 2013 Oct 9
Cite this article as Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al Building on safety feasibility and acceptabilitythe impact and cost of community health worker provision of injectable contraception Glob Health Sci Pract 20131(3)316-327 httpdxdoiorg109745GHSP-D-13-00025
Chin-Quee D Bratt J Malkin M Nduna MM Otterness C Jumbe L et al This is an open-access article distributed under the terms of theCreative Commons Attribution License which permits unrestricted use distribution and reproduction in any medium provided the original authorand source are properly cited To view a copy of the license visit httpcreativecommonsorglicensesby30______________________________________________________________________
Impact and cost of CHW provision of injectable contraception wwwghspjournalorg
Global Health Science and Practice 2013 | Volume 1 | Number 3 327
Related Documents











